The musings of a physician who served the community for over six decades
367 Topics
Downtown A discussion about downtown area in Philadelphia and connections from today with its historical past.
West of Broad A collection of articles about the area west of Broad Street, Philadelphia, Pennsylvania.
Delaware (State of) Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Religious Philadelphia William Penn wanted a colony with religious freedom. A considerable number, if not the majority, of American religious denominations were founded in this city. The main misconception about religious Philadelphia is that it is Quaker-dominated. But the broader misconception is that it is not Quaker-dominated.
Particular Sights to See:Center City Taxi drivers tell tourists that Center City is a "shining city on a hill". During the Industrial Era, the city almost urbanized out to the county line, and then retreated. Right now, the urban center is surrounded by a semi-deserted ring of former factories.
Philadelphia's Middle Urban Ring Philadelphia grew rapidly for seventy years after the Civil War, then gradually lost population. Skyscrapers drain population upwards, suburbs beckon outwards. The result: a ring around center city, mixed prosperous and dilapidated. Future in doubt.
Historical Motor Excursion North of Philadelphia The narrow waist of New Jersey was the upper border of William Penn's vast land holdings, and the outer edge of Quaker influence. In 1776-77, Lord Howe made this strip the main highway of his attempt to subjugate the Colonies.
Land Tour Around Delaware Bay Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Tourist Trips Around Philadelphia and the Quaker Colonies The states of Pennsylvania, Delaware, and southern New Jersey all belonged to William Penn the Quaker. He was the largest private landholder in American history. Using explicit directions, comprehensive touring of the Quaker Colonies takes seven full days. Local residents would need a couple dozen one-day trips to get up to speed.
Touring Philadelphia's Western Regions Philadelpia County had two hundred farms in 1950, but is now thickly settled in all directions. Western regions along the Schuylkill are still spread out somewhat; with many historic estates.
Up the King's High Way New Jersey has a narrow waistline, with New York harbor at one end, and Delaware Bay on the other. Traffic and history travelled the Kings Highway along this path between New York and Philadelphia.
Arch Street: from Sixth to Second When the large meeting house at Fourth and Arch was built, many Quakers moved their houses to the area. At that time, "North of Market" implied the Quaker region of town.
Up Market Street to Sixth and Walnut Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Sixth and Walnut over to Broad and Sansom In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
Montgomery and Bucks Counties The Philadelphia metropolitan region has five Pennsylvania counties, four New Jersey counties, one northern county in the state of Delaware. Here are the four Pennsylvania suburban ones.
Northern Overland Escape Path of the Philadelphia Tories 1 of 1 (16) Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
City Hall to Chestnut Hill There are lots of ways to go from City Hall to Chestnut Hill, including the train from Suburban Station, or from 11th and Market. This tour imagines your driving your car out the Ben Franklin Parkway to Kelly Drive, and then up the Wissahickon.
Philadelphia Reflections is a history of the area around Philadelphia, PA
... William Penn's Quaker Colonies
plus medicine, economics and politics ... nearly 4,000 articles in all
Philadelphia Reflections now has a companion tour book! Buy it on Amazon
Philadelphia Revelations
Try the search box to the left if you don't see what you're looking for on this page.
George R. Fisher, III, M.D.
Obituary
George R. Fisher, III, M.D.
Age: 97 of Philadelphia, formerly of Haddonfield
Dr. George Ross Fisher of Philadelphia died on March 9, 2023, surrounded by his loving family.
Born in 1925 in Erie, Pennsylvania, to two teachers, George and Margaret Fisher, he grew up in Pittsburgh, later attending The Lawrenceville School and Yale University (graduating early because of the war). He was very proud of the fact that he was the only person who ever graduated from Yale with a Bachelor of Science in English Literature. He attended Columbia University’s College of Physicians and Surgeons where he met the love of his life, fellow medical student, and future renowned Philadelphia radiologist Mary Stuart Blakely. While dating, they entertained themselves by dressing up in evening attire and crashing fancy Manhattan weddings. They married in 1950 and were each other’s true loves, mutual admirers, and life partners until Mary Stuart passed away in 2006. A Columbia faculty member wrote of him, “This young man’s personality is way off the beaten track, and cannot be evaluated by the customary methods.”
After training at the Pennsylvania Hospital in Philadelphia where he was Chief Resident in Medicine, and spending a year at the NIH, he opened a practice in Endocrinology on Spruce Street where he practiced for sixty years. He also consulted regularly for the employees of Strawbridge and Clothier as well as the Hospital for the Mentally Retarded at Stockley, Delaware. He was beloved by his patients, his guiding philosophy being the adage, “Listen to your patient – he’s telling you his diagnosis.” His patients also told him their stories which gave him an education in all things Philadelphia, the city he passionately loved and which he went on to chronicle in this online blog. Many of these blogs were adapted into a history-oriented tour book, Philadelphia Revelations: Twenty Tours of the Delaware Valley.
He was a true Renaissance Man, interested in everything and everyone, remembering everything he read or heard in complete detail, and endowed with a penetrating intellect which cut to the heart of whatever was being discussed, whether it be medicine, history, literature, economics, investments, politics, science or even lawn care for his home in Haddonfield, NJ where he and his wife raised their four children. He was an “early adopter.” Memories of his children from the 1960s include being taken to visit his colleagues working on the UNIVAC computer at Penn; the air-mail version of the London Economist on the dining room table; and his work on developing a proprietary medical office software using Fortran. His dedication to patients and to his profession extended to his many years representing Pennsylvania to the American Medical Association.
After retiring from his practice in 2003, he started his pioneering “just-in-time” Ross & Perry publishing company, which printed more than 300 new and reprint titles, ranging from Flight Manual for the SR-71 Blackbird Spy Plane (his best seller!) to Terse Verse, a collection of a hundred mostly humorous haikus. He authored four books. In 2013 at age 88, he ran as a Republican for New Jersey Assemblyman for the 6th district (he lost).
A gregarious extrovert, he loved meeting his fellow Philadelphians well into his nineties at the Shakespeare Society, the Global Interdependence Center, the College of Physicians, the Right Angle Club, the Union League, the Haddonfield 65 Club, and the Franklin Inn. He faithfully attended Quaker Meeting in Haddonfield NJ for over 60 years. Later in life he was fortunate to be joined in his life, travels, and adventures by his dear friend Dr. Janice Gordon.
He passed away peacefully, held in the Light and surrounded by his family as they sang to him and read aloud the love letters that he and his wife penned throughout their courtship. In addition to his children – George, Miriam, Margaret, and Stuart – he leaves his three children-in-law, eight grandchildren, three great-grandchildren, and his younger brother, John.
A memorial service, followed by a reception, will be held at the Friends Meeting in Haddonfield New Jersey on April 1 at one in the afternoon. Memorial contributions may be sent to Haddonfield Friends Meeting, 47 Friends Avenue, Haddonfield, NJ 08033.
In 1747, Benjamin Franklin had a life-transforming experience, acting quite unlike his character before, or later. At that time, Old Europe was engaged in some distant tribal skirmishing which has come to be known as King George's War. King George II, that is, under whose rule Franklin in 1751 inscribed on the cornerstone of the Pennsylvania Hospital that Pennsylvania was flourishing, "for he sought the happiness of his people."
The cornerstone of the Pennsylvania Hospital inscribed by Franklin.
Those distant commotions suddenly developed a harsh reality for the little pacifist sanctuaries on the Delaware River, when French and Spanish privateers suddenly raided and destroyed settlements on Delaware Bay. The Quaker Assemblies and their absentee Proprietor merely dithered and huddled in the face of what impended as a totally unexpected threat of annihilation of the pacifist colonies. It probably only seemed natural for the owner of the largest newspaper in the colony to publish a pamphlet called "Plain Truth," urging the inhabitants to rally to their own defense, and pressure their government to lead them. The Quaker leaders were in fact unable to readjust a lifetime of pacifist belief in a few days of an emergency, and the English Proprietor, then Thomas Penn, was far too remote to take active charge of matters. So, Franklin gave speeches, also an unfamiliar role for him, and finally brought out a detailed proposal for the creation of a Pennsylvania Militia. Ten thousand volunteers promptly signed up, elected Franklin as their Colonel; but he declined, and served as a common soldier.
Benjamin Franklin in 1767.
Against naval attack, the Militia needed cannon, which did not exist in the colony. So Franklin organized a lottery, raised three thousand pounds, and tried to buy cannon from Governor Clinton of New York. New York declined to sell, and so Franklin led a delegation to New York to negotiate. The negotiations largely consisted of getting Governor Clinton drunk and convivial, but they were successful, the artillery was shipped off to Philadelphia. Although they were undoubtedly grateful to Franklin for saving the day, this entirely extra-legal recruitment of an army badly rattled the Quakers and their Proprietor, since it demonstrated the ineffectiveness of their governance at a time of obvious crisis, and might ultimately have led to their overthrow. Franklin's heroic behavior seemed so threatening to Thomas Penn that he described him as "a dangerous man," acting like "the Tribune of the People."
When the underlying commotion in Old Europe subsided, the threat to the colonies disappeared, so the Militia disbanded in a year. Franklin seemed to be just as uncomfortable with his unaccustomed role as the governing leaders were, and he hardly ever mentioned it again. However, this is the sort of reflex leadership which makes political careers, and it surely influenced his decision to retire from business in 1748, run for election to the Assembly, and live like a gentleman. Seven years later, during the French and Indian War, he had become the chosen leader of the Pennsylvania Assembly, had much longer to think through what he was doing, and had learned how to organize a war. By that time, as the saying goes, he knew who he was. He was a man whose silent memories could flashback to that time when a bald fat printer stepped out of the crowd, saying "Follow me," and ten thousand men with muskets did so.
MEETING OF THE SHAKSPERE SOCIETY OF PHILADELPHIA
AT THE FRANKLIN INN CLUB, FEBRUARY 5, 2003
Dean Wagner in the chair. Other members present: Bartlett, Binnion, Bornemann, Cramer, Di Stefano, Dupee, Fallon, Fisher, Frye, Griffin, Hopkinson, Ingersoll, Lehmann, Madeira, O' Malley, Peck, Warden, Wheeler.
Members are grateful to Messrs. Friedman, Pope, and Madeira for hosting the 2003 Annual Dinner on the Bard's birthday, Wednesday, April 23 The probable site will be the Awbury Arboretum in Germantown.
Dr. Orville "Pete" Horwitz, a longtime member of this Society, died on January 28 at the age of 93. A memorial service will be held on February 7 at eleven AM at the Church of the Redeemer in Bryn Mawr. Senior members recalled that Dr. Horwitz had loved the Society and had attended meetings faithfully for many years. He was a veteran of the Battle of Midway, and during his Navy service in World War Two, he was awarded the Bronze Star with two oak leaf clusters. He went on to a distinguished career as a cardiologist and medical scholar in Philadelphia. He is survived by his wife of almost seventy years, Natalie, a niece of John Foster Dulles. Members grinned at memories of Dr. Horwitz's vigorous role in an annual competition among men's clubs from New York, Boston, and Philadelphia to decide whose members could tell the funniest off-color stories. Dr. Horwitz starred in this competition, borrowing stories from his Trenton barber.
Mr. Dupee recently visited our senior member, Mr. Foulke, in Florida, and brings Mr. Foulke's cordial greetings to all Society members. Mr. Dupee also reported that he has arranged, on behalf of the annual Shakspere competition among local high schools students, for Society members Fallon and Peck to play a role this year. All twenty-eight of the young people competing will be presented with copies of Dr. Fallon's recently published reader's guide to Shakspere's plays. Dr. Peck will be one of the judges of this year's contest, to be held at the Walnut Street Theater on President's Day, February 17, from 9:00 AM through the afternoon. Each of the young people, winners of contests at their respective schools, will recite a passage of some twenty lines from one of the Bard's plays, and one of Shakspere's sonnets. The winner here goes on to competition among regional winners in New York City.
Members voted on whether they favored allowing women to be eligible for membership in the Society. Several members not present had already expressed their opinions to the Secretary or the Dean. Dean Wagner announced that the final tally was eighteen votes in the affirmative, thirteen in the negative, and nine active members not voting. The motion was therefore defeated since it did not receive the support of three-quarters of those voting. Women guests are of course always welcome. A couple of members commented that we have no rules either welcoming or rejecting the candidacy of women to be members of the Society. Presumably, anyone proposed as a member, according to whatever criteria we decide on following in the future, is eligible for election. The Bartlett Committee will shortly make recommendations as to what these criteria should be.
We elected to membership in the Society Mr. Jonathan Schmalzbach, proposed as a candidate by Mr. Lehmann. We will welcome another dinner visit in the near future by Mr. Ake's friend Michael Mabry, who visited us twice in October.
We completed our reading of The Two Gentlemen of Verona in short order. We noted in Act Four that the disguised Julia analyzes her feelings about her perfidious lover Proteus at some length; she prefigures articulate psychologists of love in Shakspere's later and better romantic plays. Julia and Silvia are by far the most vigorous and strong-minded characters in this weak play, suggesting Rosalind and Juliet and Viola and Olivia, and even, perhaps, Desdemona, in later masterpieces about conflicted love. In Act Five, we visit the forest, so often a symbolically important setting for scenes in the Bard's plays of love, as in Midsummer Night's Dream and As You Like It. Strong emotions cause turmoil but are reordered after threats to lovers' happiness.
WE MEET NEXT ON FEBRUARY 19, 2003, WHEN WE WILL BEGIN READING THE TAMING OF THE SHREW.
On the eve of the Constitutional Convention, the nation was unhappy, confused, and dissatisfied; this wasn't what a victory was supposed to feel like. George Washington wanted a country to be proud of, big enough to discourage enemies, otherwise free of policing, regulation, or monarchy. Eight years of war had taught him it wasn't easy to have both liberty and discipline at the same time. Perhaps America was more unusually blessed, however, defended from invasion by oceans and wilderness, and from greed by a continent of natural resources. If order and justice could be organized, perhaps this by itself would enlist the loyalty of that mixture of classes and nationalities then flocking to our shores. Several important writers were having a strong influence on the era we now call the Enlightenment; David Hume and Adam Smith in Scotland, Edward Gibbon in England, Voltaire and Diderot in France, even Catherine the Great of Russia, with a thousand others including Benjamin Franklin and Robert Morris. Although Washington probably hadn't read them, Adam Smith's The Wealth of Nations showed unvarnished new ways of looking at commerce and politics, while Gibbon's The Decline and Fall of the Roman Empire showed what could happen if idealism gets neglected. Both books were published in the portentous year of 1776, describing many difficulties, but always suggesting problems could somehow be solved. There were plenty of ideas in circulation, but there was no plan.
It must have become obvious to Washington well before the Battle of Yorktown, that the Revolutionary War would not leave us with our problems solved. There was one brief moment as the British Army was withdrawing from Philadelphia in 1778 which seemingly justified boasts our troops had licked 'em. Just after the surrender of a whole British Army at the Battle of Saratoga, the British were also retreating from Philadelphia, and the Lord North offered generous peace terms through the Earl of Carlisle. No doubt the British public was restless after the Burgoyne defeat and the French alliance with America. Because the Carlisle episode is much more familiar in England than in America, perhaps it was a feint or a maneuver to embarrass the Earl of Carlisle or possibly just an exploration of the true state of affairs which were rumored about across a wide ocean. At any event, Gouverneur Morris was the visible American actor in this puzzling episode, but he must have been acting in concert with others. Lord North offered to give us our own elected parliament within a commonwealth; taxation with representation, no less. Morris seems to have dismissed this offer with contempt. But six more years of devastation ensued, surely convincing Washington that bitter defeat was still possible. That reality was concealed behind the graciousness of the French in allowing us to claim American troops had defeated the British at Yorktown. In fact, the preponderance of troop casualties, naval vessels and strategy had been French. The money had been mostly French as well. If that debt nearly bankrupted France, what might it have done to America?
Washington had been an outstanding athlete, soldier, and farmer, but his many travels about the colonies convinced him something more than leadership was needed. You just can't defeat a powerful enemy with short enlistments which give soldiers a legal right to go home on the eve of battle, and no way for the central command to extend the enlistments. To this, Robert Morris added that you can't buy gunpowder without the central power to levy taxes to pay for them. Morris warned him more was needed than a confederation so big others would leave it alone. Even temporary power wasn't enough. National disorganization had been just as bad after the Revolution as before. By 1787, Washington concluded the states just would not surrender power to a central national government unless the people forced them to give it up, and after a brief patriotic fervor, the people mostly wanted to go home for spring plowing. Peacetime also demonstrated another discouraging truth: meaningful improvement of the existing order meant the whole previous leadership class might leave public service to less qualified leaders, watching peace attract mediocrity to political office. Prominent men in the community gathered in a Constitutional Convention recognized the advantages of Union and devising peaceful ways to maintain it. After that transient moment when the memory of the war was fresh, politics could return to the mediocrities of a political class. That's not exactly what is now meant by "We, the People", but it might have to serve. In Washington's view, the voice of the people usually echoed along the lines of Tell us what good it would do to upset the Articles of Confederation, otherwise leave them alone. If you propose the general shape of a new central government, first tell us what it can do better than the states. And then show us how to make dubious state politicians agree to it. The accents of hesitation and defeat echo powerfully.
The hideous French Revolution was soon to demonstrate how unwise it was to look for short-cuts; we need a republic, not a stampeded democracy. George Washington was unsure just what was needed, but he knew a few basic things with certainty. America needed a bargain which everyone was expected to keep. A stronger central government should be provided for, and make it difficult to dissolve.
In 1920, the University of Pennsylvania graduated 34 students with B.A. degrees, and 134 with M.D. degrees. Today, the campus is a little self-contained city of 50,000 inhabitants. The transformation of the campus during that period is an outward expression of revolutionary expansion of the student body, involving demolitions, restorations, new construction. And the nearly constant shortage of parking space.
David Hollenberg
David Hollenberg, the University Architect, recently gave the Franklin Inn Club an interesting description of the University from the point of view of bricks and mortar. Since almost every building on the campus is undergoing or plans to undergo a major building project, he had a lot of material to cover. The disappearance of the railroad-based industrial area of West Philadelphia has been an economic problem for the city, but of course, this abundance of vacant land has created a major opportunity for the University of Pennsylvania. One reflection of this abundance is the opportunity to become the developer for much of the whole region around the campus, working with private developers who wish to be in the University area, and are therefore willing to coordinate their plans with those of the University. It's a remarkable opportunity. Since it comes at the time of a major economic downturn, one can only hope that the University does not impoverish itself taking advantage of this good luck.
Jonathan E. Rhoads
As the graduation statistics illustrate, not so long ago the University was largely a medical school, with appendages. There are rumors of considerable friction from time to time, between the President of the University and the Dean of the Medical School as to who was boss; it is easy to imagine the trustees swinging from one side to the other. The most notable Provost of the University in modern times was Jonathan Rhoads, who also happened to be Professor of Surgery. If you know Quakers, you know that disputes were seldom rancorous. And if you know Jonathan, you know he almost always won the disputes.
Cira Center
While today, the dominant change is caused by the Cira Center buildings and the acquisition of the former Post Office building, it is well to keep in mind that the new Cancer Center is a billion-dollar project. A great deal of the medical school expansion is centered on burgeoning research, particularly in molecular biology, largely financed by the National Institutes of Health. While the leaders of the NIH have long struggled with Congress to keep politics out of both the administration and the substance of research, it seems to old-timers that the politicians are slowly winning. Senator Specter's seniority on the Appropriations Committee may have had as much to do with the prosperity of West Philadelphia, as the quality of research, however eminent. We are about to find out, and if things go hard with us in favor of say Chicago, it could be a wrenching experience. Most of those research buildings cost more to heat, air-condition, insure and clean than the entire tuition base of the students; and they wouldn't be good for much if you tried to sell them.
The University is almost unique in being located on contiguous land, near existing public transportation, and occupying substantial old structures capable of renovation to new purposes. Mr. Hollenberg was asked whether it was cheaper to grow like this within a city, or whether it is cheaper to plant a totally new university in several open corn fields, as we often see happen. While this is a hard question to answer, and depends to some extent on the type of architect in charge, it is his view that big-city restoration is a considerably cheaper way to expand than building from scratch on open land, although if you are starting the institution itself from scratch, there isn't much choice but the cornfield.
And then, there is the ancient argument between academics and bricks and mortar. Development officers agree that it is easier to raise donations when you can name a building for the donor; grand visions for new frontiers of teaching are a much harder sell. So a question does hang over this expansion, however exciting, whether the endowment will keep up with the structures, once the excitement of physical expansion dies down. These are definitely things to worry about, but right now you seize the opportunities as they go past, leaving integration to your successors to figure out.
Having since my return from France demolished the three houses in Market Street, between Third and Fourth Streets, fronting my dwelling-house, and erected two new and larger ones on the ground, and having also erected another house on the lot which formerly was the passage to my dwelling, and also a printing-office between my dwelling and the front houses; now I do give and devise my said dwelling-house, wherein I now live, my said three new houses, my printing- office and the lots of ground thereto belonging; also my small lot and house in Sixth Street, which I bought off the widow Henmarsh; also my pasture-ground which I have in Hickory Lane, with the buildings thereon; also my house and lot on the North side of Market Street, now occupied by Mary Jacobs, together with two houses and lots behind the same, and fronting on Pewter-Platter Alley; also my lot of ground in Arch Street, opposite the church-burying ground, with the buildings thereon erected; also all my silver plate, pictures, and household goods, of every kind, now in my said dwelling-place, to my daughter, Sarah Bache, and to her husband, Richard Bache, to hold to them for and during their natural lives, and the life of the longest liver of them, and from and after the decease of the survivor of them, I do give, devise, and bequeath to all children already born, or to be born of my said daughter, and to their heirs and assigns forever, as tenants in common, and not as joint tenants.
................
All the lands near Ohio, and the lots near the center of Philadelphia, which I lately purchased of the State, I give to my son-in-law, Richard Bache, his heirs and assigns forever;
................
To my son, William Franklin, late Governor of the Jerseys, I give and devise all the lands I hold or have a right to, in the province of Nova Scotia, to hold to him, his heirs, and assigns forever.
.................
I give and devise to my dear sister, Jane Mecom, a house and lot I have in Unity Street, Boston, now or late under the care of Mr. Jonathan Williams, to her and to her heirs and assigns forever.
..................
Since my will was made I have bought some more city lots, near the center part of the estate of Joseph Dean. I would have them go with the other lots, disposed of in my will, and I do give the same to my Son-in-law, Richard Bache, to his heirs and assigns forever.
109 Volumes
Philadephia: America's Capital, 1774-1800 The Continental Congress met in Philadelphia from 1774 to 1788. Next, the new republic had its capital here from 1790 to 1800. Thoroughly Quaker Philadelphia was in the center of the founding twenty-five years when, and where, the enduring political institutions of America emerged.
Philadelphia: Decline and Fall (1900-2060) The world's richest industrial city in 1900, was defeated and dejected by 1950. Why? Digby Baltzell blamed it on the Quakers. Others blame the Erie Canal, and Andrew Jackson, or maybe Martin van Buren. Some say the city-county consolidation of 1858. Others blame the unions. We rather favor the decline of family business and the rise of the modern corporation in its place.

 Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.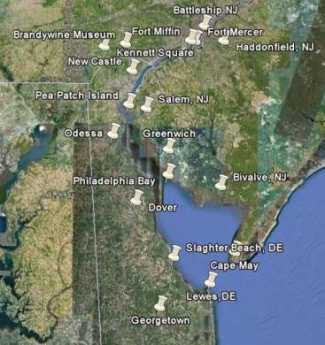 Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it! Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it. In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions. Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.