The musings of a physician who served the community for over six decades
367 Topics
Downtown A discussion about downtown area in Philadelphia and connections from today with its historical past.
West of Broad A collection of articles about the area west of Broad Street, Philadelphia, Pennsylvania.
Delaware (State of) Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Religious Philadelphia William Penn wanted a colony with religious freedom. A considerable number, if not the majority, of American religious denominations were founded in this city. The main misconception about religious Philadelphia is that it is Quaker-dominated. But the broader misconception is that it is not Quaker-dominated.
Particular Sights to See:Center City Taxi drivers tell tourists that Center City is a "shining city on a hill". During the Industrial Era, the city almost urbanized out to the county line, and then retreated. Right now, the urban center is surrounded by a semi-deserted ring of former factories.
Philadelphia's Middle Urban Ring Philadelphia grew rapidly for seventy years after the Civil War, then gradually lost population. Skyscrapers drain population upwards, suburbs beckon outwards. The result: a ring around center city, mixed prosperous and dilapidated. Future in doubt.
Historical Motor Excursion North of Philadelphia The narrow waist of New Jersey was the upper border of William Penn's vast land holdings, and the outer edge of Quaker influence. In 1776-77, Lord Howe made this strip the main highway of his attempt to subjugate the Colonies.
Land Tour Around Delaware Bay Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Tourist Trips Around Philadelphia and the Quaker Colonies The states of Pennsylvania, Delaware, and southern New Jersey all belonged to William Penn the Quaker. He was the largest private landholder in American history. Using explicit directions, comprehensive touring of the Quaker Colonies takes seven full days. Local residents would need a couple dozen one-day trips to get up to speed.
Touring Philadelphia's Western Regions Philadelpia County had two hundred farms in 1950, but is now thickly settled in all directions. Western regions along the Schuylkill are still spread out somewhat; with many historic estates.
Up the King's High Way New Jersey has a narrow waistline, with New York harbor at one end, and Delaware Bay on the other. Traffic and history travelled the Kings Highway along this path between New York and Philadelphia.
Arch Street: from Sixth to Second When the large meeting house at Fourth and Arch was built, many Quakers moved their houses to the area. At that time, "North of Market" implied the Quaker region of town.
Up Market Street to Sixth and Walnut Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Sixth and Walnut over to Broad and Sansom In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
Montgomery and Bucks Counties The Philadelphia metropolitan region has five Pennsylvania counties, four New Jersey counties, one northern county in the state of Delaware. Here are the four Pennsylvania suburban ones.
Northern Overland Escape Path of the Philadelphia Tories 1 of 1 (16) Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
City Hall to Chestnut Hill There are lots of ways to go from City Hall to Chestnut Hill, including the train from Suburban Station, or from 11th and Market. This tour imagines your driving your car out the Ben Franklin Parkway to Kelly Drive, and then up the Wissahickon.
Philadelphia Reflections is a history of the area around Philadelphia, PA
... William Penn's Quaker Colonies
plus medicine, economics and politics ... nearly 4,000 articles in all
Philadelphia Reflections now has a companion tour book! Buy it on Amazon
Philadelphia Revelations
Try the search box to the left if you don't see what you're looking for on this page.
George R. Fisher, III, M.D.
Obituary
George R. Fisher, III, M.D.
Age: 97 of Philadelphia, formerly of Haddonfield
Dr. George Ross Fisher of Philadelphia died on March 9, 2023, surrounded by his loving family.
Born in 1925 in Erie, Pennsylvania, to two teachers, George and Margaret Fisher, he grew up in Pittsburgh, later attending The Lawrenceville School and Yale University (graduating early because of the war). He was very proud of the fact that he was the only person who ever graduated from Yale with a Bachelor of Science in English Literature. He attended Columbia University’s College of Physicians and Surgeons where he met the love of his life, fellow medical student, and future renowned Philadelphia radiologist Mary Stuart Blakely. While dating, they entertained themselves by dressing up in evening attire and crashing fancy Manhattan weddings. They married in 1950 and were each other’s true loves, mutual admirers, and life partners until Mary Stuart passed away in 2006. A Columbia faculty member wrote of him, “This young man’s personality is way off the beaten track, and cannot be evaluated by the customary methods.”
After training at the Pennsylvania Hospital in Philadelphia where he was Chief Resident in Medicine, and spending a year at the NIH, he opened a practice in Endocrinology on Spruce Street where he practiced for sixty years. He also consulted regularly for the employees of Strawbridge and Clothier as well as the Hospital for the Mentally Retarded at Stockley, Delaware. He was beloved by his patients, his guiding philosophy being the adage, “Listen to your patient – he’s telling you his diagnosis.” His patients also told him their stories which gave him an education in all things Philadelphia, the city he passionately loved and which he went on to chronicle in this online blog. Many of these blogs were adapted into a history-oriented tour book, Philadelphia Revelations: Twenty Tours of the Delaware Valley.
He was a true Renaissance Man, interested in everything and everyone, remembering everything he read or heard in complete detail, and endowed with a penetrating intellect which cut to the heart of whatever was being discussed, whether it be medicine, history, literature, economics, investments, politics, science or even lawn care for his home in Haddonfield, NJ where he and his wife raised their four children. He was an “early adopter.” Memories of his children from the 1960s include being taken to visit his colleagues working on the UNIVAC computer at Penn; the air-mail version of the London Economist on the dining room table; and his work on developing a proprietary medical office software using Fortran. His dedication to patients and to his profession extended to his many years representing Pennsylvania to the American Medical Association.
After retiring from his practice in 2003, he started his pioneering “just-in-time” Ross & Perry publishing company, which printed more than 300 new and reprint titles, ranging from Flight Manual for the SR-71 Blackbird Spy Plane (his best seller!) to Terse Verse, a collection of a hundred mostly humorous haikus. He authored four books. In 2013 at age 88, he ran as a Republican for New Jersey Assemblyman for the 6th district (he lost).
A gregarious extrovert, he loved meeting his fellow Philadelphians well into his nineties at the Shakespeare Society, the Global Interdependence Center, the College of Physicians, the Right Angle Club, the Union League, the Haddonfield 65 Club, and the Franklin Inn. He faithfully attended Quaker Meeting in Haddonfield NJ for over 60 years. Later in life he was fortunate to be joined in his life, travels, and adventures by his dear friend Dr. Janice Gordon.
He passed away peacefully, held in the Light and surrounded by his family as they sang to him and read aloud the love letters that he and his wife penned throughout their courtship. In addition to his children – George, Miriam, Margaret, and Stuart – he leaves his three children-in-law, eight grandchildren, three great-grandchildren, and his younger brother, John.
A memorial service, followed by a reception, will be held at the Friends Meeting in Haddonfield New Jersey on April 1 at one in the afternoon. Memorial contributions may be sent to Haddonfield Friends Meeting, 47 Friends Avenue, Haddonfield, NJ 08033.
Charles Wilson Peale (1741-1827)
The Artist in His Museum
1822, Oil on canvas (The Joseph Harrison Jr. Collection)
Courtesy of the Pennsylvania Academy of
Fine Arts.
all of the red brick buildings on Independence Square look as though they were part of Independence Hall, but there is one exception. The building facing Fifth Street is Philosophical Hall, one of the four buildings of the American Philosophical Society. Right now, Philosophical Hall is used as a museum. It could be called the first museum in America, but not the oldest, because it had interruptions and different proprietorships. Charles Wilson Peale started his museum of curiosities there and then moved it to the second floor of Independence Hall, where he painted the famous portrait of himself holding up the curtain. In recent years, Philosophical Hall has again become a museum, holding treasures and curiosities belonging to the Philosophical Society itself. The docent is pleased to alternate between calling it America's new oldest museum, and America's oldest new museum. And, yes, the newell post has an Amity Button.
American Philosophical Society
Patents were established by the Constitution when it was a piece of parchment lying on a table fifty feet away from here, and the early patent office required the submission of a working model of every application for patent. After a while, that got to be a lot of working models lying around, and many of the more interesting ones are on display in the museum. Like the model of Fitch's first steamboat or the gadget Jefferson used, to make simultaneous copies of documents he was writing. That's right near the Gilbert Stuart copy of Washington's portrait, and von Neumann's first algorithm to be stored in his stored program machine, or computer, and Neil Armstrong's speech on the moon, concerning one step for mankind and all. It's a splendid museum, full of the real stuff, in a handsome Georgian building with sparkling immaculate marble staircases.
John Fitch received a US Patent for the Steamboat August 26, 1791
In the Eighteenth Century, Natural Philosophy was what we now call science. That's why PhDs get a degree of Doctor of Philosophy when they study chemistry and physics. The idea for forming a scientific society in America apparently originated with John Bartram. As so often happens, the originator couldn't quite get it established and had to call on Ben Franklin that impression of publicity, to get it off the ground. To be fair about it, Franklin was probably the more distinguished scientist of the two. To be even more fair about it, the organization struggled a bit until Thomas Jefferson (that's the one who was President of the United States) gave it a real publicity shove. During the depths of the 1930s depression, one of the members left it several million dollars with the stipulation that the investments should focus on common stock. Since buying stock in 1935 was widely regarded as about the stupidest thing an investor could do, this little episode reinforced a strong impression that membership in the APS is given to people who are very smart, not merely famous. The four buildings, the many fellowships, and the big endowment were largely made possible by this contraries investment decision.
There are eight hundred members, of whom 93 have won Nobel Prizes. Over the years, two hundred members have been awarded Nobel Prizes, but you must remember that the organization existed for 150 years before there was such a prize. Several U.S. Supreme Court justices are members and lots and lots of people who are famous. The docent comments that they look pretty much like everyone else. There's a rumor that Bill Gates turned down the offer of membership, so now we will just see. He's young enough to have several decades' opportunity to reconsider an offer, although the APS might just be old enough to lack interest in any second chances.
The European financial system consists of one monetary policy, set by the European Central Bank, but twelve (soon to be twenty-five) fiscal policies, set by the various governments. This was once thought to represent a major difference from the American Federal Reserve, but in fact, it hardly matters. Our fifty component states are not permitted to run deficits, but our federal government runs deficits, plenty of them, and it turns out to make little practical difference if a Central Bank must float bonds to pay for a deficit arriving in one envelope or twelve. What matters is the size of the total. From that starting point, the central bank struggles to modify matters to restrain inflation, or combat unemployment. The main tool at the bank's disposal relates to the fact that governments no longer fear to print more money than they can redeem in gold. They print money, all right, but the spigot is now turned down when inflation begins to appear. In theory, at least, inflation is not possible if the central bank is able to maintain this policy. Of course, if money created in the past comes flooding in from abroad or out of mattresses, there might be a problem. Central bankers seem like terribly powerful people until you count up the people they can't control. The first is the politicians who create those deficits.
European politicians believe their constituents prize security above all else, a condition known as socialism. High taxes, high unemployment, and slow economic growth are considered more tolerable in Europe than sacrificing pensions, health care, and other features of the social safety net; out of this come government deficits, then maybe inflation. The central bank is told to make the best of it.
Recently, however, long-term interest rates have failed to rise in response to rising deficits, and speculation abounds as to why that should be so. It creates uneasiness to hear that the finances of the world are simply a "conundrum". And finally, foreigners will flee from an inflated currency, eventually triggering a devaluation. A few years ago, Argentina refused to devalue, but the result was a devastating recession when their foreign trading partners refused to deal with an unrealistic currency.
A government which refuses to respond to these "signals" from the bond market and foreigners, will be forced to take some undesirable actions. In Europe, it is to oppose globalization of the economy, thereby hurting everybody but especially poor nations. And the internal European unemployment is shifted as much as possible onto the backs of immigrants, even migrants from within the European community. Take that far enough, and you get serious threats to world peace. Even within the European community, many of the policies which protect the welfare state will consciously injure their own economic growth. Reform is resisted.
Many needed reforms are obvious to policymakers in Europe, and the American example would often seem to be convincing. But it isn't, because Europeans terrified of losing their welfare state recognize that the American model includes a large amount of contempt for socialism, no matter how otherwise successful it is. The interesting thing has been that the Scandinavian countries have an equally extensive welfare safety net, but have nevertheless prospered by adopting free-market reforms. There are signs that this experience is beginning to convince Europeans it is possible to work their way out of the dilemmas.
After his talk, which avoided mention of many of these concerns in the mind of his audience, Governor Noyer was even more charming in cocktail-party mode, but one thing made his face turn beet red. When asked what the John Jay letter was all about, he had to admit he hadn't the foggiest. It was just something hanging on his wall that seemed appropriate for a trip to Philadelphia.
My wife once remarked that having children was like making pancakes; just throw the first two away. But she only had four children, her grandmother had ten. Her daughters had two. Increased education makes childhood longer, while improved health lengthens retirement. The working period, age 25-65, however, has already extended its borders, pretty much to the limit. Ben Franklin's crusade to use healthcare to put sick people back to work, has been superseded for lack of orphans and invalids. In the past fifty years, miscarriage changed from passing nuisance into a devastating disaster because waiting to have the first child is largely an athletic event. In the future, population unbalancing will mostly depend on more retirees. There's a big economic effect. Neither children nor retirees earn very much, so the wealth of the country comes from ages 25-65, which must support everybody else. Countermovements seem remarkably feeble. The pressure to retire later in life is voiced but not much acted upon while starting work younger must contend with the publicity that more education increases lifetime income. It is too early to know how realistic it would be to shorten school vacations or to pack more education into shorter time at school, with electronic teaching.
In a simpler age, parents supported their children and their aging parents. It was unusual for women to earn very much, so marriage contracts enforced a support requirement. While the employment of women broadened the base of earnings, weakening the marriage institution threatened the retirement security of unmarried women. The political reaction to these changes has been a tendency to substitute government support and retirement programs for the family-based support system. Our national commitment to equal justice has had a tendency to make the new government system more expensive than the old family one. It once seemed just and natural for the wife of an impoverished man to be impoverished, but now the standard has moved to equality of treatment. In all classes of life, there is a tendency for discordance between males and females. The poor single woman gets more money, the poor single male probably gets less. The prosperous single woman gets less that she has been accustomed to, the prosperous single male is probably better off. It is too early to know how the new legislative climate will affect homosexuals. There is little doubt these changes will affect political attitudes of almost all demographic groups, but great uncertainty about the degree and direction.
Nothing makes it likely there can be much change in the dependence of the whole system on financial transfers from working groups to non-working ones. However, the system of collecting in the form of taxes and disbursing in the form of subsidies is both inefficient and disagreeable. A particularly inefficient way to accomplish this response to a weakened family structure is found in health insurance, now representing close to 18% of Gross Domestic Product (GDP). If we are to take money from younger people and transfer it to older ones, we should be collecting investment income on the decades-long interval. This is a continuous process, not a one-off transfer, and the amounts involved are seriously large. While the issue is the same for Social Security as it is for Medicare, it is easier to see how it came about in Medicare. In any new program, there is usually a transition problem to be financed, quite often by phasing it in. In the case of Medicare, the choice was made to facilitate passage of the legislation by employing "Pay as you go". In this system, the early recipients receive full benefits without paying anything toward them and are paid by the contributions of the new younger beneficiaries who will not need benefits for many decades. In other words, the system functions on the cash flow of the system instead of on funded reserves. Its great danger lies in the possibility that some generation (in this case the Baby Boomers) will eventually create a beneficiary class too large to be supported by smaller later generations. This pitfall has received much attention, but unfortunately, very little attention has been given to the problem mentioned earlier: no interest or investment income is derived from funded reserves, as is quite common in whole-life life insurance.
Nor should it happen, if the price to be paid is to have the Federal Government become the largest owner of common stock control of the private sector. That would be a very large step in the direction of government ownership of the means of production, otherwise known as Communism. With present artificially suppressed interest rates, the investment return available to governments is so small it could well be counter-productive. Borrowing from yourself is a useless exercise, and if confined to government bonds, puts the nation in a vulnerable position with potentially hostile foreign nations, or even supra-national organizations like the UN, who could one day have an agenda we consider hostile, under the control of a unicameral body dominated by one-state, one-vote system. No matter how it is arranged, it involves a loss of sovereignty for an unacceptably large part of our economy, eventually leading to a total loss of sovereignty. This transfer of funds from young to old must remain in private hands, with individual voters retaining control of it. Unfortunately, a great many intended beneficiaries are incapable of managing their own affairs, so there is a significant agency risk. That's a nice way of saying that a great many people have been cheated by friends and relatives they unwisely trusted, and there is every reason to look an offended politician straight in the eye and say, "I'm sorry, but I don't trust you." Unfortunately, this commonly results in the ones you can trust, charging an exorbitant fee for the simple role of being trustworthy. This is not a new problem. The only solution is to have at least two systems at the same time: a Prudential group of experts with themselves much to lose from being exposed as less than perfect, giving oversight to at least five competitive funds. How you chose the funds, and how you choose the expert overseers, are crucial.
If you want to live on City Line Avenue, safely in Montgomery County, you put your entrance on Latches Lane, which is parallel to City Line. It used to be said that the Barnes Foundation was next to Episcopal Academy, but that has moved further West, and St. Joseph's University now owns the property. When St. Joseph's decides what to do with the land, we can possibly describe a better landmark. The Barnes Foundation has always faced away from Philadelphia and is a little hard to find, all of which may have something to do with Dr. Barnes' strong dislike of the City.
The Barnes Museum
When you go there now, the old Museum is still there, but already showing signs of neglect. The house the Barnes family lived in is still, right next door. But it's harder to move an Arboretum than a group of paintings, so the Arboretum School, which was Mrs. Barnes' hobby, is still at the same place, likely to stay awhile. It's still a very nice place to visit, especially right at Labor Day when the very large Franklinia Trees are in full bloom. Like all Franklinia trees, these are direct descendants of the only example John Bartram was able to find, in Georgia or anywhere else.
Medicinal Garden
We're going to have to leave the decision to former Governor Rendell, about what you do with an empty museum since he is said to have had a lot to do with making it that way. We came to see the Arboretum.
The first thing which strikes you is that many of the big old trees are much older than the Barnes Foundation would have been. The brochure helpfully explains that a 19th Century tree fancier started it in 1880, and the Barnes acquired it in 1922. That still wouldn't account for a massive tree which is lying on the ground all cut up, opposite the Medicinal Garden. The base of the tree must be three or more hundred years old, so perhaps there was a grove of old oaks, just over the line of William Penn's city, which every owner tended carefully until the bugs got it. There are a considerable number of Chinese trees that look about right for 1880, but without a guide, it's pretty conjectural.
Japanese Beetle
Ever since someone imported the Japanese beetle along with some plants, to Moorestown, New Jersey, there have been laws prohibiting the importation of plants from abroad, but there must be some regulatory rigamarole which allows museums to do it. Korea and Japan are at the same latitude as Philadelphia, and the glaciers spared some ancient dinosaur food in those regions, so quite a few strange plants have come here from that source. Since the Barnes is a school, and since it only has a few acres, many if not most of the specimens in the gardens are one or two of a kind. That either means they have a feeder garden somewhere to store backups or a good relationship with government officials. Like all Arboretums, it attracts insects, so be prepared to do some swatting if you go. The school is said to be outstanding and quite conveniently located, but even just a stroll around is quite a nice way to spend a Sunday afternoon.
At first, the British Empire wasn't even British, it was English. English history, English religion, English unification, even English court intrigue, and gossip. When Sir Francis Drake brought home the Spanish gold, it was welcome enough, but it was just part of the English Revolution, on its way to becoming the British Empire. English settlers were just a curiosity, like the "Indians" they brought home. England was Ben Franklin's idea of home, left behind by his prosperous family because of largely religious quarrels. The silk-dye Franklins, by the way, had to start over at the bottom in Boston because Cotton Mather's crowd wouldn't accept their money, or see their side of a silly English religious quarrel. England was, in fact, everybody's home, intellectually, although that was fast coming to an end. Because of the plague and the fire, lots of things were coming to an end, and lots of other things were just starting. For now, the important thing was they were people of former substance, wide acquaintance, and thoroughly English. Whiggish and out of favor perhaps, but not seriously in rebellion.
When they got to America, the whole Franklin family was rambunctious and supported itself with sister Jane's invention of bar soap, her father's candle-making shop, and brother James' printer shop. They got in trouble somewhat with a straight-laced community, but most of their troubles would be called "scrapes" and "quarrels" of a family trying to re-establish itself in new circumstances. When he got to Philadelphia, Benjamin repeated the performance. Arriving at a strange town as a penniless teenager, he turned a print-shop into a chain of newspapers and was ready to retire to his hobbies and politics at the age of 42. Along the way, he learned to keep his mouth shut.
Franklin was not an aristocrat, but there were scarcely any aristocrats who did not seek him out. In spite of writing one of the most famous autobiographies in America, few people could be certain of his religion, his marital status, his politics. He was definitely not a Quaker, but for a while, he led the Quaker faction. He never went past the second grade, but would have won a Nobel prize if there had been such a thing, and financed his own research. He spent eighteen years living in London, inventing a musical instrument which pleased Mozart, and regularly visiting Parliament. When the King's Saint Paul Cathedral was struck by lightning, the King sought his advice. When King George III rejected this advice, the personal quarrel turned him into a personal enemy of the King. As a consequence, he finally turned rebel, joined the Continental Congress, and eventually helped write the American Constitution. At the Albany Conference of 1754, he had proposed a Union of the Thirteen Colonies and lived to see it a reality in 1789. But in spite of that, it took a personal confrontation with King George III to convince him Independence was a good idea. In spite of his greatly praised autobiography, no one suspected it of him. No one seems to have known.
109 Volumes
Philadephia: America's Capital, 1774-1800 The Continental Congress met in Philadelphia from 1774 to 1788. Next, the new republic had its capital here from 1790 to 1800. Thoroughly Quaker Philadelphia was in the center of the founding twenty-five years when, and where, the enduring political institutions of America emerged.
Philadelphia: Decline and Fall (1900-2060) The world's richest industrial city in 1900, was defeated and dejected by 1950. Why? Digby Baltzell blamed it on the Quakers. Others blame the Erie Canal, and Andrew Jackson, or maybe Martin van Buren. Some say the city-county consolidation of 1858. Others blame the unions. We rather favor the decline of family business and the rise of the modern corporation in its place.

 Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.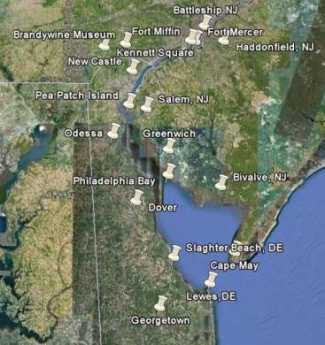 Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it! Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it. In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions. Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.