The musings of a physician who served the community for over six decades
367 Topics
Downtown A discussion about downtown area in Philadelphia and connections from today with its historical past.
West of Broad A collection of articles about the area west of Broad Street, Philadelphia, Pennsylvania.
Delaware (State of) Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Religious Philadelphia William Penn wanted a colony with religious freedom. A considerable number, if not the majority, of American religious denominations were founded in this city. The main misconception about religious Philadelphia is that it is Quaker-dominated. But the broader misconception is that it is not Quaker-dominated.
Particular Sights to See:Center City Taxi drivers tell tourists that Center City is a "shining city on a hill". During the Industrial Era, the city almost urbanized out to the county line, and then retreated. Right now, the urban center is surrounded by a semi-deserted ring of former factories.
Philadelphia's Middle Urban Ring Philadelphia grew rapidly for seventy years after the Civil War, then gradually lost population. Skyscrapers drain population upwards, suburbs beckon outwards. The result: a ring around center city, mixed prosperous and dilapidated. Future in doubt.
Historical Motor Excursion North of Philadelphia The narrow waist of New Jersey was the upper border of William Penn's vast land holdings, and the outer edge of Quaker influence. In 1776-77, Lord Howe made this strip the main highway of his attempt to subjugate the Colonies.
Land Tour Around Delaware Bay Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Tourist Trips Around Philadelphia and the Quaker Colonies The states of Pennsylvania, Delaware, and southern New Jersey all belonged to William Penn the Quaker. He was the largest private landholder in American history. Using explicit directions, comprehensive touring of the Quaker Colonies takes seven full days. Local residents would need a couple dozen one-day trips to get up to speed.
Touring Philadelphia's Western Regions Philadelpia County had two hundred farms in 1950, but is now thickly settled in all directions. Western regions along the Schuylkill are still spread out somewhat; with many historic estates.
Up the King's High Way New Jersey has a narrow waistline, with New York harbor at one end, and Delaware Bay on the other. Traffic and history travelled the Kings Highway along this path between New York and Philadelphia.
Arch Street: from Sixth to Second When the large meeting house at Fourth and Arch was built, many Quakers moved their houses to the area. At that time, "North of Market" implied the Quaker region of town.
Up Market Street to Sixth and Walnut Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Sixth and Walnut over to Broad and Sansom In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
Montgomery and Bucks Counties The Philadelphia metropolitan region has five Pennsylvania counties, four New Jersey counties, one northern county in the state of Delaware. Here are the four Pennsylvania suburban ones.
Northern Overland Escape Path of the Philadelphia Tories 1 of 1 (16) Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
City Hall to Chestnut Hill There are lots of ways to go from City Hall to Chestnut Hill, including the train from Suburban Station, or from 11th and Market. This tour imagines your driving your car out the Ben Franklin Parkway to Kelly Drive, and then up the Wissahickon.
Philadelphia Reflections is a history of the area around Philadelphia, PA
... William Penn's Quaker Colonies
plus medicine, economics and politics ... nearly 4,000 articles in all
Philadelphia Reflections now has a companion tour book! Buy it on Amazon
Philadelphia Revelations
Try the search box to the left if you don't see what you're looking for on this page.
George R. Fisher, III, M.D.
Obituary
George R. Fisher, III, M.D.
Age: 97 of Philadelphia, formerly of Haddonfield
Dr. George Ross Fisher of Philadelphia died on March 9, 2023, surrounded by his loving family.
Born in 1925 in Erie, Pennsylvania, to two teachers, George and Margaret Fisher, he grew up in Pittsburgh, later attending The Lawrenceville School and Yale University (graduating early because of the war). He was very proud of the fact that he was the only person who ever graduated from Yale with a Bachelor of Science in English Literature. He attended Columbia University’s College of Physicians and Surgeons where he met the love of his life, fellow medical student, and future renowned Philadelphia radiologist Mary Stuart Blakely. While dating, they entertained themselves by dressing up in evening attire and crashing fancy Manhattan weddings. They married in 1950 and were each other’s true loves, mutual admirers, and life partners until Mary Stuart passed away in 2006. A Columbia faculty member wrote of him, “This young man’s personality is way off the beaten track, and cannot be evaluated by the customary methods.”
After training at the Pennsylvania Hospital in Philadelphia where he was Chief Resident in Medicine, and spending a year at the NIH, he opened a practice in Endocrinology on Spruce Street where he practiced for sixty years. He also consulted regularly for the employees of Strawbridge and Clothier as well as the Hospital for the Mentally Retarded at Stockley, Delaware. He was beloved by his patients, his guiding philosophy being the adage, “Listen to your patient – he’s telling you his diagnosis.” His patients also told him their stories which gave him an education in all things Philadelphia, the city he passionately loved and which he went on to chronicle in this online blog. Many of these blogs were adapted into a history-oriented tour book, Philadelphia Revelations: Twenty Tours of the Delaware Valley.
He was a true Renaissance Man, interested in everything and everyone, remembering everything he read or heard in complete detail, and endowed with a penetrating intellect which cut to the heart of whatever was being discussed, whether it be medicine, history, literature, economics, investments, politics, science or even lawn care for his home in Haddonfield, NJ where he and his wife raised their four children. He was an “early adopter.” Memories of his children from the 1960s include being taken to visit his colleagues working on the UNIVAC computer at Penn; the air-mail version of the London Economist on the dining room table; and his work on developing a proprietary medical office software using Fortran. His dedication to patients and to his profession extended to his many years representing Pennsylvania to the American Medical Association.
After retiring from his practice in 2003, he started his pioneering “just-in-time” Ross & Perry publishing company, which printed more than 300 new and reprint titles, ranging from Flight Manual for the SR-71 Blackbird Spy Plane (his best seller!) to Terse Verse, a collection of a hundred mostly humorous haikus. He authored four books. In 2013 at age 88, he ran as a Republican for New Jersey Assemblyman for the 6th district (he lost).
A gregarious extrovert, he loved meeting his fellow Philadelphians well into his nineties at the Shakespeare Society, the Global Interdependence Center, the College of Physicians, the Right Angle Club, the Union League, the Haddonfield 65 Club, and the Franklin Inn. He faithfully attended Quaker Meeting in Haddonfield NJ for over 60 years. Later in life he was fortunate to be joined in his life, travels, and adventures by his dear friend Dr. Janice Gordon.
He passed away peacefully, held in the Light and surrounded by his family as they sang to him and read aloud the love letters that he and his wife penned throughout their courtship. In addition to his children – George, Miriam, Margaret, and Stuart – he leaves his three children-in-law, eight grandchildren, three great-grandchildren, and his younger brother, John.
A memorial service, followed by a reception, will be held at the Friends Meeting in Haddonfield New Jersey on April 1 at one in the afternoon. Memorial contributions may be sent to Haddonfield Friends Meeting, 47 Friends Avenue, Haddonfield, NJ 08033.
We are about to look at a remarkable
a fourteen-block stretch of street, with several unifying historical
themes, but there is one notable feature which stands by itself. The PSFS
building is now the site of a luxury hotel, but it once
housed the Philadelphia
Savings Fund Society, the oldest savings bank in the country,
having been founded in 1816. Setting aside the place of this
the institution in American finance, and passing quickly by the deplorable
end of it with swashbuckling corsairs in three-piece suits, 1929
the building itself remains so remarkable that the hotel still displays the
PSFS sign on its top. The imagination of the architects was so advanced
that a building constructed seventy-five years ago looks as though it
might have been completed yesterday. The Smithsonian Institution
conducts annual five-day tours of Chicago to look at a skyscraper
architecture, but hardly anything on that tour compares with the PSFS
building. From time to time, someone digs up old newspaper clippings
from the 1930s to show how the PSFS was ridiculed for its odd-looking
the building, but anyhow this is certainly one example of how the Avante
the guard got it right.
At the far Eastern end of Market Street, right in the middle of the
street once stood a head house, which in this case was called the
market terminal building
. In those days, street markets were mostly a line
of sheds and carts down the middle of a wide street, but usually there
was a substantial masonry building at the head of the market, where
money was counted and more easily guarded. An example of a restored
ahead house can today be found at Second and Pine, although that market
("Newmarket") was less for groceries than for upscale shops. The market
on Market Street started at the river and worked West with the
advancing city limits, making it understandable that buildings which
lined that broad avenue gradually converted to shops, and then stores.
The grandest of the department stores on Market Street was, of course, John Wanamaker's,
all the way to City Hall, built on the site of Pennsylvania
Railroad's freight terminal (the passenger terminal was on the West
side of City Hall). In the late Nineteenth Century, the Pennsylvania
Railroad and the Reading Railroads terminated at this point, so
rail traffic flowing east merged with ocean and river traffic flowing
west. Well into the Twentieth Century, a dozen major department stores
and hundreds of specialty stores lined the street, with trolley cars,
buses, and subway traffic taking over for horse-drawn drainage. The
the pinnacle of this process was the corner of Eighth and Market, where
four department stores stood, one on each corner, and underneath them
three subway systems intersected. The Reading terminal market is
Philadelphia's last remnant of this almost medieval shopping concept,
although the Italian street markets of South Philadelphia display a
more authentic chaos. Street markets, followed by shops, overwhelmed by
department stores showed a regular succession up Market Street, and
when commerce disappeared, it all turned into a wide avenue from City
Hall to River, leaving few colonial traces.
The history of Market Street is the history of the Reading Terminal
Market. Farmers and local artisans thronged to sell their wares in
sheds put up in the middle of the wide street, traditionally called
"shambles" after the similar areas in York, England. Gradually, elegant
stores were built on the street, and upscale competitors began to be
uncomfortable with the mess and disorder of the shambles down the
center of the street. By 1859 the power structure had changed, and the
upscale merchants on the sidewalks got a law passed, forbidding
shambles. After the expected uproar, the farmers and other shambles
merchants got organized, and built a Farmers Market on the North side
of 12th and Market Relative peace and commercial
tranquility then prevailed until the Reading Railroad employed power
politics and the right of eminent domain to displace the Farmer's
Marketplace with a downtown railroad terminal that was an architectural
marvel for its time, with the farmers displaced to the rear in the
Reading Terminal Market, opening in 1893. Bassett's, the ice cream
maker, is the only merchant continuously in business there since it
opened, but several other vendors are nearly as old. The farmers market
persisted in that form for a century until the City built a convention
center next door. As a result, the quaint old farmers market became a
tourist attraction, with over 90,000 visitors a week. That's fine if
you are selling sandwiches and souvenirs, but it crowds out meat and
produces and thereby creates a problem. If the tourist attraction gets
too popular, it drives out everything which made it a tourist
attraction; so rules had to be made and enforced, limiting the number
of restaurants, but encouraging Pennsylvania Dutch farmers. Competition
and innovation are the lifeblood of commercial real estate, but they
are always noisy processes. The history of the street is the history of
clamor and jostling, eventually dying out to the point where everyone
is regretful and nostalgic for a revival of clamor.
When you take the ferry across the mouth of Delaware Bay from Lewes to Cape May, you are out of sight of land for half an hour. But the Army Corps of Engineers have thoroughly dredged it out. By contrast, when Henry Hudson first discovered the river while searching for a Northwest passage to the Indies, it was so full of snags and shoals that he just gave up and sailed on to what is now New York harbor. So, for centuries the river pilots were an essential part of ocean commerce to Philadelphia. As you might well imagine, the earliest pilots were members of local Indian tribes. Eventually, a proud colony of professional pilots grew up at Lewes, Delaware. Since radio communication is a comparatively recent development in this ancient trade, they had to devise ways for an incoming ship to select a pilot, and establish rules to be enforced by the Port Wardens about how to go about it.
In the mid-Eighteenth Century, the system was to hang a black ball from the Cape Henlopen lighthouse whenever a ship was sighted. Little companies of ten or fifteen pilots would then jump into very fast schooners designed for the purpose, and race to be first out to the ladder hanging from the incoming ship's side. The rule was, the first to arrive and present his certificate got the job. Tony Junker, an actively practicing Philadelphia architect has immersed himself in tales and adventures among the pilots, and Tunnell's Boys is an exciting new novel about this dangerous, wet and uncomfortable, profession.
We talk high finance here, so perhaps a simple story from Wall Street is needed to introduce the topic to a non-Wall Street audience. Following the 1929 crash, and consequent to the Glass Steagall Act, Morgan Stanley was the only American investment bank in existence. It was the first of a new kind, but barely in existence, doing something like $300,000 worth of business in 1933. As finance adjusted to the new ground rules, Morgan Stanley grew in size, commonly referred to as the "White Shoe" investment bank. That term was an allusion to the Ivy League background of its partners, who came from colleges which affected white buckskin shoes among their more elite students. It also referred to the fact that almost all Morgan Stanley partners were pretty rich and fairly young, entirely able to live by a code of behavior which might be summarized as, "We don't find it necessary to cheat."
Buried within that motto was the idea that Morgan Stanley was as good as its word, and tried very hard to avoid doing business with anybody who did cheat. In a business where a great deal of business was transacted too quickly for written contracts or vetting by law firms, that meant a lot.
<
Morgan Stanley soon climbed to the top of a very tough heap and stayed there for fifty years. Many of its partners were millionaires in their twenties, but so what, they were mostly pretty rich before they joined the firm. The company ran as a partnership, with the capital they leveraged coming from the personal fortunes of the partners. Under these circumstances, it is not surprising many partners retired in their forties, taking their enhanced capital with them. The Glass-Steagall Act (now being imitated by the Volcker Rule within the Dodd-Frank Law) made it illegal for a depository bank to be under the same roof with an investment bank. Much of the capital in the pre-1929 days had been supplied by the deposits in the depository bank, but Glass Steagall cut that off when it created depository insurance, on the theory that deposit insurance was a Federal gift, and its "moral hazard" should not flow through to the speculation of investment banking.
That comment was tinged with populism, with the dubious implication that those who are two generations off the farm are less likely to cheat than those who are five generations off the farm. So the depository bank of Morgan Guaranty has split away from the investment bank of Morgan Stanley, which was the three-step process by which Morgan Stanley eventually grew so big it could no longer be sustained by leveraging the personal wealth of its partners.
Buy And Sell
Eventually, the pressure to raise money by selling stock to the public could no longer be resisted. The rich partners became even richer by selling their company's stock on the stock exchange, the company did grow enormously, and a lot of new stockholders got rich, too. Unfortunately, when you sell a stock you also sell voting rights, so the sale transferred voting control of the company to the new stock purchasers. It did not take many years before the white shoe atmosphere was a thing of the past, along with the discipline that the atmosphere imposed on the rest of corporate America. When the 2008 crash came along, there was enough questionable behavior on Wall Street to justify a populist President of the United States to tolerate, or even encourage, a witch hunt of Wall Street bankers for ruining the country.
Even so brilliant an economist as Paul Volcker has encouraged the idea that separating the two forms of banks was an unmitigated blessing which must be restored, while in fact it is only justified by the gift of Federal Deposit Insurance to the depository arm, not the Investment Banking Arm. It seems only a matter of time before there will be agitation to extend the insurance to the investment arm so we will be chasing our own tail, of extending insurance to encourage risk-taking, instead of using demand deposits to do so. And thus inviting another crash.
I'm sorry, Paul, but there is a reversed way to describe it. The small investors demanded the entitlement of risk-free investing, protected by deposit insurance. And they declared this insurance was a special entitlement to which wealthy players were ineligible. When small punters go broke, it is a tragedy. When big players go broke, it serves them right for being so greedy.
No matter. The point of the story is not the value of Glass Steagall, but rather the enormous power of Wall Street, to force a partnership to become a stockholder company, even so, might a company as the House of Morgan. Because I have become persuaded, and hope to persuade the public, that this is the main mechanism which humbled Philadelphia, from being the mightiest industrial engine in the world, in less than twenty years. Like the perfect storm, it took three other forces to make it quite so violent, and quite so swift. They were the first World War, the 1929 stock market crash, and Prohibition. The central operational lever of force was exerted by converting industrial corporations, from partnerships into stockholder corporations. That was the tool which destroyed the old Philadelphia. The other three forces simply made it happen in certain ways and at certain times.
Gasoline
Converting partnership or family businesses into stockholder organizations was a universal outcome of both World Wars, all over the world. The phenomenon can be looked at as one way of extracting frozen wealth to pay war debts. It is accompanied by an increase in national indebtedness, so it makes civilizations less stable. Scraps of partnership control do continue to persist in remote developing countries, and in tiny principalities like Luxembourg, but it seems only a matter of time before the public buys them out. The only major developed country to retain family control of businesses in Germany. Apparently, it was intentional, based on the inheritance laws. Tightly held countries are more commonly tightly held together by force, as in Russia, Saudi Arabia, and Monaco, usually because of a monopoly grip on oil or other natural resources. But even those governments could probably be toppled, except for fear of ensuing chaos, just as did happen to many former dictatorships, and was a source of fear in Philadelphia. A case can be made for populism if it is kept small and under control. Hardly any case at all can be made for chaos.
Brewerytown Map
For those of us who love Philadelphia and wonder what happened to it, let me point out three defining local peculiarities. Prohibition was more of a factor than we like to think because Philadelphia's Tenderloin was the former Brewerytown, filled with Beer Gardens, refrigeration plants (Lager beer is brewed in the cold) and beer distributors. The passage of the Volstead Act suddenly transformed the largest alcohol-production center in the country into the largest alcohol-consuming area, from River to River, from Franklin Square to the Schuylkill.
It was concentrated in the Brewerytown by being illegal, and somewhat secret. Brewerytown soon turned into the Tenderloin, and the Tenderloin into Skid Row, cutting off North Philadelphia from law and order, but in time it was alarming in a different way to see speakeasies spread into other sections of the city. Much as it tried, even the Mafia couldn't control the influx of amateur criminals, when the Tenderloin essentially cut the city in half.
When the great migration from the South occurred after WW II, the immigrants turned North Philadelphia into a slum. Cutting I76 along the same center-city lines helped shrivel North Philadelphia and hustle its flight to the suburbs. Some misadventures of Philco and Ford, Baldwin and Stetson hastened the process and may have caused some of it.
Pennsylvania Railroad
America grew into a mighty industrial nation as a result of becoming the Arsenal of Freedom in the Civil War and two World Wars. The nation needed to expand its industrial base from the essential monopoly corridor of the Pennsylvania Railroad, and it had the money to do so. The land was cheaper elsewhere, labor was nonunion elsewhere, and air conditioning made the South bearable. Wall Street saw an enormous opportunity to buy stock from the family partners of Philadelphia industries, and sell it again to the world. These new owners had no interest in preserving lovable Philadelphia; they wanted to reap the harvest of expanding what we had, to the rest of the country, maybe even the rest of the world.
Once a spiral like this gets started, it runs by itself. The owners of the mansions on the hills, proprietors of what were big businesses by Victorian standards, sold their partnerships, their children were converted into coupon clippers, and their grandchildren into trust-fund babies. If you really have nothing much to do, why not do it in California next to the beaches? Hollywood made trust fund babies seem glamorous on the Main Line, just as Madison Avenue had once made patriots on the left bank seem fatally attractive. Those movies and novels made somebody pretty rich, but whoever it was, doesn't live here, anymore.
The Right Angle Club was once again honored by a recent talk by Tony Junker, the novelist, retired architect, Center City resident -- and now the leader in an effort to start a Peace Museum. He's a Quaker, as Philadelphians would easily guess, and a charming peace advocate. He tells us his specialty while a practicing architect, was designing museums, so the whole thing starts to fit together. The museum is still in the planning stages, hoping to raise two million dollars as start-up money. Needless to say, Philadelphia has a long history of Quaker advocacy for Peace. It is not saying too much to suppose William Penn designed his whole colony as a peace demonstration. And Tony began his talk by noting that in England, Penn's father remains much better known than his son.
William senior conquered the island of Jamaica and gave it to King Charles, in return for which the King repaid his debt by giving the admiral's son Pennsylvania. On his deathbed, the Admiral beseeched his king to look after his rebellious and somewhat disobedient son; this was King Charles' way of doing it. By the way, he had distinguished himself with successful administration of New Jersey before the King gave him Pennsylvania, and acquired what is now the state of Delaware, somewhat later. With these three states, he became the largest private landowner in our history -- ever. He makes the Klebergs of the King Ranch look pretty paltry by comparison, and indeed Charles even offered to make him a vassal king. Young William, however, told him that really wasn't the idea, at all. Young Penn sold land to his suspicious co-religionists, and in order to facilitate the sales, drew up a document called, Concessions and Agreements , which was in considerable part a model for America's Constitution. It can be found in the Archives of the State of New Jersey, in Trenton.
The Peace Museum
The Peace Museum is projected to open in a few years; it would be a great mistake to underestimate Tony's ability to get it started. Since his retirement, he has founded a Quaker retirement community on Front Street which is already in existence. It's open to non-Quakers of course, and there are quite a few Quaker retirement villages in the suburbs. But Philadelphia is returning to Center City, and the need for a retirement home has often been expressed but never implemented until Tony came along. Early Quakers lived in caves along the banks of the Delaware River, just about where the retirement village is situated, and Quaker settlement later concentrated along Arch Street. Arch Street, by the way, really had an arch. Evidently, the river was once much deeper and somewhat wider, so it had one embankment which began at Front Street and a lower one on Water Street. So as the town grew, it was natural to undercut a tunnel with an arch bearing Front Street. Many houses eventually had one door on Water Street and another door on Front Street, higher up. Relics of Quaker settlement can still be noticed on Arch Street, cut off by the Benjamin Franklin Parkway slanting Northward. Front and Arch was the location for the main anchorage in those days, and the London Tavern at Front and Market was the main hangout of sailors off the ships nearby, a rich source of gossip and the origin of a number of rebellious episodes. The Fifteenth Street Meetinghouse now seems to be the most westward sign of this Quaker settlement, but Isaac Sharpless bought the land of Friends Select School further west and shared the land between Friends Select and his high-rise headquarters of what was the Pennwalt headquarters. If you are planning a Quaker museum in Center City, you can find plenty of choices to be called historic Quaker property, along Arch Street. The still earlier Quaker settlements around Dock Creek, beginning at about Spruce Street, have long been outgrown and abandoned.
Unfortunately, although we experienced long periods of Peace during the Nineteenth Century, it must be admitted that Penn's hope for an example of peaceful existence to the rest the world, would have to be called a failure. We have had several major foreign wars during the Twenty-first century, and show every sign of preparing for more. The Quakers literally owned a major portion of the American colonies and withdrew from politics rather than vote for war taxes in the Revolutionary War. While the example of courageous conscientious objection had its impact, it also developed an image of martyrdom which the rest of the world declines to imitate. Friends are perfectly capable of forming their own opinions, but it might be suggested to them that more of their efforts would be successful if somehow they made more publicity of their successes.
Whiskey Rebellion
George Washington, for example, was effective in keeping us out of foreign entanglement, in large part by the fact that he was a famous athlete and a successful warrior. His example for the country was in effect, "If you are strong, people leave you alone." He was surely successful in achieving a peaceful settlement of the Whiskey Rebellion by saddling up his horse and riding at the head of 10,000 troops in a threatening manner. Later in his presidential administration, he was surely more effective in dealing with European powers because of his former military reputation than he would have been without it. His second inaugural address was in effect a plea that good things could emerge from self-interest: Honesty is the best policy. There's a primitive quality to this appeal, reminding his countrymen they are more likely to get rich if they were honest, than if they were dishonest. Purists may squirm at the undertones of this motto, but surely it was effective with his countrymen. And three-quarters of the world's population might still be better off if they adopted a motto which falls just a little short of being altruistic.
Let's see how short and succinct we can make it. Our task is to take the maximum amount of savings we could possibly ask the public to accumulate, invest it more or less on autopilot, and see if it can generate enough money to pay for what we assume will be health costs a century from now. Some would say that's a fool's errand, but let's see what we can do.
We start with an assumption the average person can save $3350 per year from age 21 to age 66; that's $150,750, total, the most anyone can invest in an HSA. The actuaries at Michigan Blue Cross, verified by Medicare, estimate average lifetime healthcare costs to be $350,000. Some people state you can stop talking, right there, because that's too much money. Please be patient, we will address indigency later. For simplicity, we wish to reduce the question to whether we could turn $150,750 into $350,000 in forty-five years with compound interest at reasonable rates. The answer is yes. We can't predict whether those future predictions of costs are accurate, but if accurate, they can be achieved. We assume two things:
Long Term Strategies
Indigents. We assume there will be no more indigents than at present. Can the government afford to subsidize them in this model? The answer is Yes, but its present commitment is in another direction, so it isn't entirely likely, very soon.
Outliving Your Income. We assume some people will use up their savings. If the average life expectancy, which is now 83, holds its present course, we assume this model can cope with it, even if the average life expectancy grows to be 93 in the next century. The arithmetic is quite favorable, but unfortunately, we don't know what new costs will be added in the meantime. Assuming there are some, we aren't counting them, so predictions about the future all contain this flaw.
We assume some other things, mentioned as we go along, essentially coming to the conclusion the model will produce a result which falls between the top and bottom curves in the graph. Please note the narrow range of variation in the early years and the widening upward range in later years. In particular, notice how a 3% (inflation) rate tends to stay flat well past any reasonable life expectancy, while more likely, investment income returns start to rise at age 60, and even sooner as the rate approaches 9% net of inflation. That seems to be a "sweet spot" the economy has discovered for itself in two hundred years of exploration.
We assume the equity stock market will follow the paths it followed since the Industrial Revolution. That is, it will produce an average of 12% gross return, with 3% of that eaten up by inflation, or 9% net of inflation. We then estimate our present conservative projections at producing at least 6.5% after costs, out of the remaining 9%. Dismissing inflation, we assume the stock market will operate between a 2% real return, and 9.5% real after inflation, leaving a 3.5% "cushion" for contingencies. When the Industrial Revolution ends, these basics may also change. We have a decade or so to try to get the investor's returns up closer to 8% safe level. And meanwhile, we must try to remain prepared for a bleak and bad depression, a "black swan", on average every 28 years, but individually unpredictable. In the meantime, we aspire eventually to pay for 100% of healthcare expenses, but promise to pay only a quarter of that. And finally, we assume medical care will change so much during the next century, that our calculations will need to be totally revised, long before then, with a so-called mid-course correction. With the understanding, that anything which pushes outside of the accompanying graph will have an obvious explanation, we assume future managers will make appropriate adjustments.
Single Premium Investment/Look carefully at the graph. It makes an unfamiliar assumption. It assumes a newborn baby started a Health Savings Account at birth, deposited $500 in it, and didn't touch the account again until he died. It is our assumption the average person could do that, perhaps with a stretch, and our further assumption that the government could do the same for indigent babies. There are times when neither the government nor many middle-class people could manage the necessary expenditures, but we set the value of $500 at birth as an extreme limit of what we think they both could do, on average most of the time. It's a number which is easily changed if the economy varies from our projection.
Let's dramatize the point we're making on a totally different scale, by temporarily appointing Warren Buffett as its role model. According to a story in the Wall Street Journal by columnist Morgan Housel, this is the way the best investor in history made his money. At the age of eighty-four, his personal wealth was $73 billion. Of that, he made $70 billion after the age of sixty. Some might retort, the trick is to make the first $3 billion by the age of sixty, but a more civil underlying moral is that compound interest really starts to work toward the end of life.
Just take another look at that graph; the particular power of compound interest works as efficiently with $500 as with $3 billion. It starts earlier with higher interest rates, in this case, age 40 at 12%, compared with age 85 at 5%, Mr. Buffett's numbers. Obviously, it pays to start early and to get higher interest rates if you can do it safely. And conversely, it's a bad idea to spend or squander your savings while you are young. Our preferred method is to raise the interest rate by reducing the attrition of middle-men, in the approach mentioned earlier. You might not reach 12%, but you have a fair chance of reaching 9% if you allow yourself fifteen years to work on it. In the meantime, be satisfied with less than 100% coverage by this method.
More seriously, why else did we pick this way to depict the future? Because at age 66, when Medicare takes over, all of the plausible curves have reached a point where they could match Medicare's expenditures, indefinitely. If Medicare went broke, or was otherwise unacceptable for some reason, liquifying the account would produce a sum matching Medicare's present rate of expenditure. And finally, the numbers become so astronomical at the far end, it seems entirely reasonable to transfer part of the account to a grandchild's account. That trick alone should greatly reduce the problem, and add 21 years for compound interest to do it. As we will see in a coming section, paying childhood health expenses in advance solves some otherwise difficult issues.
109 Volumes
Philadephia: America's Capital, 1774-1800 The Continental Congress met in Philadelphia from 1774 to 1788. Next, the new republic had its capital here from 1790 to 1800. Thoroughly Quaker Philadelphia was in the center of the founding twenty-five years when, and where, the enduring political institutions of America emerged.
Philadelphia: Decline and Fall (1900-2060) The world's richest industrial city in 1900, was defeated and dejected by 1950. Why? Digby Baltzell blamed it on the Quakers. Others blame the Erie Canal, and Andrew Jackson, or maybe Martin van Buren. Some say the city-county consolidation of 1858. Others blame the unions. We rather favor the decline of family business and the rise of the modern corporation in its place.

 Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.
Originally the "lower counties" of Pennsylvania, and thus one of three Quaker colonies founded by William Penn, Delaware has developed its own set of traditions and history.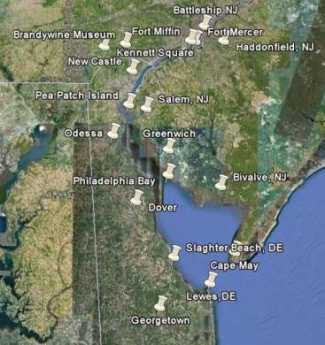 Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it!
Start in Philadelphia, take two days to tour around Delaware Bay. Down the New Jersey side to Cape May, ferry over to Lewes, tour up to Dover and New Castle, visit Winterthur, Longwood Gardens, Brandywine Battlefield and art museum, then back to Philadelphia. Try it! Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it.
Millions of eye patients have been asked to read the passage from Franklin's autobiography, "I walked up Market Street, etc." which is commonly printed on eye-test cards. Here's your chance to do it. In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions.
In 1751, the Pennsylvania Hospital at 8th and Spruce was 'way out in the country. Now it is in the center of a city, but the area still remains dominated by medical institutions. Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.
Grievances provoking the American Revolutionary War left many Philadelphians unprovoked. Loyalists often fled to Canada, especially Kingston, Ontario. Decades later the flow of dissidents reversed, Canadian anti-royalists taking refuge south of the border.