5 Volumes
Philadelphia Medicine
Several hundred essays on the history and peculiarities of Medicine in Philadelphia, where most of it started.
History: Philadelphia and the Quaker Colonies
Philadelphia and the Quaker Colonies
Medicine
New volume 2012-07-04 13:34:26 description
Health: Philadelphia
New volume 2014-08-04 22:18:40 description
Surviving Strands of Quakerism
Of the original thirteen, there were three Quaker colonies, all founded by William Penn: New Jersey first, Pennsylvania biggest, and Delaware so small Quakerism was overcome by indigenous Dutch and Swedes.
Philadelphia Physicians
Philadelphia dominated the medical profession so long that it's hard to distinguish between local traditions and national ones. The distinctive feature is that in Philadelphia you must be a real doctor before you become a mere specialist.
Nation's First Hospital, 1751-2016

|
| Pennsylvania Hospital |
As commonly stated in medical history circles, the history of the Pennsylvania Hospital is the history of American medicine. The beautiful old original building, with additions attached, still stands where it did in 1755, a great credit to Samuel Rhoads the builder and designer of it. The colonial building on Pine Street stopped housing 150 patients around 1980, supposedly at the demand of the Fire Marshall, although its perpetual fire insurance policy still owes the hospital several thousand dollars a year as an unspent premium dividend. There may have been one small fire during two centuries of use, but its true fire hazard would be difficult to assert. It was just out of date. The original patient areas consisted of long open wards, with forty or so beds lined up behind fluted columns, in four sections on two floors. The pharmacy was on the first floor, the lunatics in the basement, and the operating rooms on the third floor under a domed skylight. It was entirely serviceable in 1948 when I arrived as an intern doctor. Individual privacy was limited to what a curtain between the beds would provide, but on the other hand, it was possible for one nurse to stand at the end of the award and recognize any distress among forty patients immediately. In this trade-off between delicacy and utility, the utility was certain to be preferred by the Quaker founders. Visitors were essentially excluded, and if a patient recovered enough to be unnaturally curious about neighboring patients, well, he had probably recovered enough to go home.
Located between two large rivers, South Philadelphia up to ten blocks away was essentially a swamp until the Civil War. So, there were seasonal epidemics of malaria, yellow fever, typhoid, and poliomyelitis at the hospital until the early twentieth century. Philadelphia was a port city, so sailors brought in cases of venereal disease, scurvy, even an occasional case of anthrax or leprosy. During the Industrial Revolution of the nineteenth century, tuberculosis, rheumatic fever, and diphtheria were part of clinical practice. But underlying the ebb and flow of environmental effects, there was a steady population of illness which did not change a great deal from 1776 to 1948. These patients were all poor, because the rules in Benjamin Franklin's handwriting restricted service to the "sick poor, and only if there is room, for those who can pay." In 1948 there was a poor box for those who might feel grateful, but no credit manager or official payment office. The matter had been considered, but the cost of collection was considered greater than the likely revenue. When Mr. Daniel Gill was offered the position as the hospital's first credit manager, it was suggested that he be given a tenth of what he collected. To his lifelong regret, Dan Gill regretted that he refused an offer that he had felt he could not afford to accept.
So, the wards were filled with victims of the diseases of poverty, punctuated by occasional epidemics of whatever was prevalent. And a second constant feature of the patients was their medical condition forced them to be housed in bed. For centuries, physicians dreaded the news that a new patient was being admitted with "dead legs".
A Toast to Doctor Franklin

|
| Benjamin Franklin |
Benjamin Franklin's formal education ended with the second grade, but he must now be acknowledged as one of the most erudite men of his age. He liked to be called Doctor Franklin, although he had no medical training. He was given an honorary degree of Master of Arts by Harvard and Yale, and honorary doctorates by St.Andrew and Oxford. It is unfortunate that in our day, an honorary degree has degraded to something colleges give to wealthy alumni, or visiting politicians, or some celebrity who will fill the seats at an otherwise boring commencement ceremony. In Franklin's day, an honorary degree was awarded for significant achievements. It was far more prestigious than an earned degree, which merely signified adequate preparation for potential later achievement.
And then, there is another subtlety of academic jostling. Physicians generally want to be addressed as Doctor, as a way of emphasizing that theirs is the older of the two learned professions. A good many PhDs respond by rejecting the title, as a way of sniffing they have no need to be impostors. In England, moreover, surgeons deliberately renounce the title, for reasons they will have to explain themselves. Franklin turned this credential foolishness on its head. Having gone no further than the second grade, he invented bifocal glasses. He invented the rubber catheter. He founded the first hospital in the country, the Pennsylvania Hospital, and he donated the books for it to create the first medical library in the country. Until the Civil war, that particular library was the largest medical library in America. Franklin wrote extensively about gout, the causes of lead poisoning and the origins of the common cold. By inventing bar soap, it could be claimed he saved more lives from the infectious disease than antibiotics have. It would be hard to find anyone with either an M.D. degree or a Ph.D. degree, then or now, who displayed such impressive scientific medical credentials, without earning -- any credentials at all.
Dr. Cadwalader's Hat

|
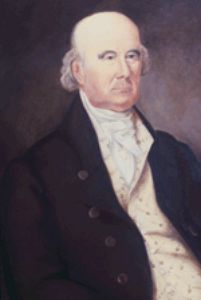
| Dr. Thomas Cadwalader |
The early Quakers disapproved of having their pictures painted, even refused to have their names on their tombstones. Consequently, relatively few portraits of early Quakers can be found, and it might, therefore, seem surprising to see a picture of Dr. Thomas Cadwalader hanging on the wall at the Pennsylvania Hospital. A plaque relates that it was donated by a descendant in 1895. Another descendant recently explained that the branch of the family which continued to be Quaker spells the name, Cadwallader. Dr. Cadwalader of the painting, famous for presiding over Philadelphia's uproar about the Tea Act, was then selected to hear out the tea rioters because of his reputation for fairness and remains famous even today for his unvarying courtesy.

|
| Pennsylvania Hospital |
In one of the editions of Some Account of the Pennsylvania Hospital, I believe the one by Morton, there is a story about him. It seems there was a sailor in a bar on Eighth Street, who announced to the assemblage that he was going to go out the swinging doors of the taproom and shoot the first man he met. So out he went, and the first man he met was Dr. Cadwalader. The kindly old gentleman smiled, took off his hat, and said, "Good Morning, Sir". And so, as the story goes, the sailor proceeded to shoot the second man he met. A more precise rendition of this story comes down in the Cadwalader family that the event in the story really took place in Center Square, where City Hall now stands, but which in colonial times was a favored place for hunting. A man named Brulumann was walking in the park with a gun, which Dr. Cadwalader took as a sign of a hunter. In fact, Brulumann was despondent and had decided to kill himself, but lacking the courage to do so, had decided to kill the next man he met and then be hanged for murder. Dr. Cadwalader's courteous greeting, doffing his hat and all, befuddled Brulumann who went into Center House Tavern and killed someone else; he was indeed hanged for the deed.
I was standing at the foot of the staircase of the Pennsylvania Hospital, chatting to a young woman who from her tailored suit was obviously an administrator. I pointed out the Amity Button, and told her its story, along with the story of Jack Gallagher, whom I knew well, bouncing an empty beer keg all the way down to the Great Court from the top floor in the 1930s, which was then being used as housing for the resident physicians. Since the young woman administrator was obviously beginning to regard me like the Ancient Mariner, I thought one last story about courtesy was in order. So I told her about Dr. Cadwalader and the shooting.
"Well," she said, "The moral of that story obviously is that you should always wear a hat." There then is no point to further conversation, I left.
July 4, 1776: Patients in the Pennsylvania Hospital on Independence Day
According to the records of the Pennsylvania Hospital, the following 48 persons were patients in the hospital on July 4, 1776:
| Richard Brinkinshire (Admitted 11/15/1775) | John Ridgeway (Admitted 12/26/1775) |
| James Chartier (Admitted 1/6/1776) | patient (Admitted 1/6/1776) |
| patient (Admitted 1/20/1776) | patient (Admitted 1/20/1776) |
| Mary Yell (Admitted 2/7/1776l) | John Beckworth (Admitted 2/7/1776) |
| Bart. McCarty (Admitted 2/10/1776) | John King (Admitted 2/10/1776) |
| Robert Alden (Admitted 2/17/1776) | William Patterson (Admitted 3/6/1776) |
| Elizabeth Hanna (Admitted 3/9/1776) | John McMahon (Admitted 3/13/1776) |
| Mary Burgess (Admitted 3/23/1776) | Mary Anderson (Admitted 4/10/1776) |
| John Hatfield (Admitted 4/15/1776) | Eliza Haighn (Admitted 4/17/1776) |
| Charles Whitford (Admitted 4/24/1776) | patient (Admitted 5/8/1776) |
| Susanna Carrington (Admitted 5/8/1776) | patient (Admitted 5/8/1776) |
| William Johnson (Admitted 5/13/1776) | Lazarus Chesterfield (Admitted 5/22/1776) |
| Mary Spieckel (Admitted 5/22/1776l) | William Edwards (Admitted 5/22/1776) |
| patient (Admitted 5/23/1776, Lunatic) | Jane White (Admitted 5/25/1776) |
| Charles McGillop (Admitted 5/29/1776) | ---Fitzgerald (Admitted 6/1/1776) |
| Michael Rowe (Admitted 6/6/1776) | patient (Admitted 6/6/1776) |
| John Hughes (Admitted 6/12/1776) | Joseph Smith (Admitted 6/15/1776) |
| Esther Munro Lunda (Admitted 6/15/1776) | Mathew Coope (Admitted 6/19/1776) |
| Anne Patterson (Admitted 6/19/1776) | Thomas Savoury (Admitted 6/20/1776) |
| Rebecca Winter (Admitted 6/26/1776) | Elizabeth Manning (Admitted 6/26/1776) |
| Negro (Admitted 6/24/1776) | Elex. Scanvay (Admitted 6/24/1776) |
| Fanny Stewart (Admitted 6/24/1776) | Peter Barber (Admitted 6/29/1776) |
| Catherine Campbell (Admitted 6/29/1776) | Ann McGlauklin (Admitted 7/3/1776) |
| Elizabeth Lindsay (Admitted 7/3/1776) | Ann Jones (Admitted 7/3/1776) |
The records indicate the following diseases were the reason for admission of those patients. Although in Colonial times there was no medical delicacy to avoid offending readers, present privacy standards require that we strip the diagnoses from the name of the patient and list them independently. There is some overlap, sometimes making it difficult to judge which disorder caused the admission.
- Sore, poisoned or ulcerated legs: 16 cases
- Lunacy, mind or head disorders: 10 cases
- Syphilis: 7 cases
- Fever and Rheumatic fever: 7 cases
- Dropsy: 5 cases
- Gunshot: 4 cases
- Diabetes: 1
- Blindness with clear pupil: 1
- Spitting blood: 1 case
- Dislocated arm: 1 case
- Inflammation of face: 1 case
- Scurvy: 1 case
- broken arm: 1 case
The following physicians were elected at the Managers Meeting dated 5/13/1776:
- Dr. Thomas Bond
- Dr. Thomas Cadwalader
- Dr. John Redman
- Dr. William Shippen
- Dr. Adam Kuhn
- Dr. John Morgan
America's First Medical Interne, Jacob Ehrenzeller
This Indenture Witnesseth, That Jacob Ehrenzeller, son of Jacob Ehrenzeller of the City of Philadelphia hath put himself, and by these presents, with consent of his said father, doth voluntarily, and of his own free Will and Accord, put himself Apprentice to the Managers of the Pennsylvania Hospital to learn the Art, Trade and Mystery, and after the Manner of an Apprentice to serve the said managers from the Day of the Date hereof, for and during, to the full End and Term of five years and three months next ensuing. During all of that Term, the said Apprentice his said Master faithfully shall serve, his Secrets keep, his lawful Commands every where readily obey. He shall do no Damage to his said Master, nor see it to be done by others, without letting or giving Notice thereof to his said Master. He shall not waste his said Master's Goods, nor lend them unlawfully to any. He shall not commit Fornication, nor contract Matrimony within the said Term.
He shall not play at Cards, Dice or any other unlawful Game, whereby his said Master may have Damage. With his own Goods, nor the Goods of others, without license from his said Master, he shall neither buy nor sell. He shall not absent himself Day nor Night from his said Master's Service without his leave: nor haunt Ale-houses, Taverns or Playhouses; but in all Things behave himself as a faithful Apprentice ought to do, during the said Term. And the said Master shall use the utmost of his Endeavor to teach or cause to be taught or instructed the said Apprentice in the Trade or Mystery of an Apothecary. And procure and provide for him sufficient Meat, Drink, washing Cloths and Lodging fitting for an Apprentice, during the said Term of five years and three months.
And for the true Performance of all and singular the Covenants and Agreements aforesaid, the said Parties bind themselves each unto the other, firmly by these Presents. IN WITNESS whereof, the said Parties have interchangeably set their Hands and Seals hereunto. Dated the first Day of June in the thirteenth year of the Reign of our Sovereign Lord George the third, King of Great-Britain, etc, Annoque Domini, One Thousand Seven Hundred and Seventy Three.
Signed and Delivered in the Presence of Jacob Ehrenzeller, Jacob Ehrenzeller Sr, Sam V. Coates
* * * *
|
| Jacob Ehrenzeller |
The Ex-residents Association of the Pennsylvania Hospital became active early in the Nineteenth century, and naturally concerned itself with just who was the first interne or resident of the hospital. It seemed probable that the first interne of the Pennsylvania Hospital would also be the first interne in America. When this indenture was discovered in the archives, Ehrenzeller became a likely candidate, although being apprenticed as an Apothecary did raise some questions. Nor did Ehrenzeller perform his indenture after the completion of medical school, as is now the custom; the first resident physician in that sense was Caspar Wister, in 1812. However, in colonial times most physicians did not go to medical school at all, qualifying as practitioners by working in the offices of practicing physicians, just as lawyers did for a much longer time. The argument is somewhat complicated by the existence of a medical school, the College of Philadelphia, created in 1765, and the fact that the upper crust of colonial medicine had gone to medical school in Edinburgh. That group of seven physicians with degrees gathered themselves together (in 1787) as the College of Physicians of Philadelphia, which still exists as the nation's oldest medical organization.
Dorothy I. Lansing MD, then the clerk of the Section on History of the College of Physicians of Philadelphia, interested herself in these issues, and privately published a pamphlet about it. The argument for regarding Ehrenzeller as an interned physician revolves around the fact that his father had gone to medical school in Europe, and was regarded as a physician even though he made his living by operating a tavern after he came to Philadelphia. Furthermore, the 16 year-old Ehrenzeller found his apprenticeship disrupted by the Revolutionary War, particularly the occupation of Philadelphia in 1777 by British troops who used the hospital for their wounded. Nevertheless, young Ehrenzeller served as a surgeon at the battle of Monmouth (June 28, 1778). Among the minute books of the Board of Managers of the Pennsylvania Hospital was discovered a minute of June 26, 1773 with the terms that Jacob Ehrenzeller, Jr. "shall have leave at his own or his Father's expense to attend the lectures of the Medical Professors out of the Hospital during the last two years of his apprenticeship; to attend the Surgical Operations and Lectures in the Hospital free of any expense; and that the Apothecary for the time being shall duly instruct him in Physic and Surgery." Dr. Lansing concluded that this was "a unique concurrent internship: apothecary apprentice cum medical student arrangement that no doubt suffered innumerable changes due to wartime problems; Jacob Ehrenzeller was awarded a certificate of medical competency. The College of Philadelphia medical school having ceased to exist because of the war, he obtained no degree in medicine."
Dr. Lansing found even stronger evidence of his physician rather than apothecary status in the fact that immediately after the war he established a practice in Goshen, Chester County. While it was customary for practicing physicians of the time to support themselves as schoolteachers, storekeepers or bankers, Ehrenzeller was able to live exclusively on his income as a physician. Indeed, after his death in July 18, 1838, his estate was one of wealth. It seems unlikely that an apothecary masquerading as a physician would have flourished in those competitive times, and on this basis it is concluded that he came as close as the times permitted to the description of an interned hospital physician. The Ex-residents Society of the Pennsylvania Hospital was satisfied enough to declare Ehrenzeller to have been its first interne. And invites the rest of the nation's medical community to examine whether anyone else might have been better qualified to have that title earlier.
The Kappa Lambda Society of Hippocrates
Philosophical Hall
February 5th 1835, 3 1/2 PM
A special meeting of the Kappa Lambda was convened this afternoon by order of the President, Dr. Otto, at the request of Drs. Bache, Bond, and Wood for the purpose of settling and closing the concerns of the institution ....
Resolved that the Secretary be requested to transfer to the College of Physicians, for safe keeping, With the consent of that body, Journal of Proceedings and other manuscript documents of the Kappa Lambda Society to be deposited in the Archives of the College ....
Philosophical Hall
February l Sth 1835, 3 1/2 PM
.... Resolved that from and after the termination of this meeting the Kappa Lambda Society of Philadelphia be held to be dissolved.
Resolved that the foregoing minutes of the present meeting be now read, which being done, they are unanimously approved.
On Motion adjourned sine die.
Henry Bond, Secy,
WITH these resolutions, the Philadelphia branch of the Kappa Lambda Society of Hippocrates transferred its organizational records to the College of Physicians of Philadelphia and then dissolved itself.
What was the Kappa Lambda Society of Hippocrates?
- An elitist clique dedicated to the advancement of its membership?
- A secret fraternal order?
- A scientific society that published one of America's most important medical journals?
- A society for the moral reform of medicine?
- A society for reviving the Hippocratic Oath?
- A society dedicated to the replacement of Hippocratic ethics with Thomas Percival's code of medical ethics?
- A medical society that served as the prototype for the American Medical Association?
- A failure from which the founders of the AMA learned how not to organize a national medical organization?
|
|
Seal of the Philadelphia chapter of the Kappa Lambda Society |
The answer that seems to emerge from the books, ledgers, and correspondence that the Philadelphia branch of Kappa Lambda transferred to the College of Physicians of Philadelphia 1835 is that the Philadelphia chapter was all of the above. Yet the only three scholars who have written about the society -- Chauncey Leake (1922), Lee Van Antwerp (l945), Philip van Ingen (1945) -- have tended to view it as only some of the above, casting Kappa Lambda as either "elf" or more commonly, as Van Antwerp marks, as an "ogre".
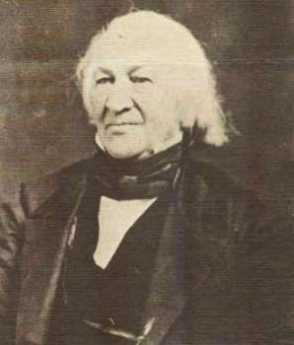
|
| Samuel Jackson, M.D. |
The Kappa Lambda Society began as a secret fraternal order whose members swore a version of the Hippocratic Oath, pledged to upload the honor of the medical profession, and promised to keep the existence of the society a secret. The earliest known records of the society are from Lexington, Kentucky, and date from 1820. But, as Van Ingen has suggested, the history of society is considerably older. What appears to have happened in Lexington was that, in 1820, Dr. Samuel Brown (1769-1830), as professor of medicine, became head of the local chapter of Kappa Lambda. Under his leadership, this chapter committed itself to the moral reform of American medicine and took as its objective the idea of having American doctors pledge themselves to adhere to the code of conduct that Dr. Thomas Percival (1740-1804) had published in 1803 under the title Medical Ethics. To implement these reforms the Lexington chapter of the Kappa Lambda Society of Hippocrates published the first American edition of Percival's code of ethics, Extracts from Medical Ethics or A Code of Institutes and Precepts, Adapted to the Professional Conducts of Physicians & Surgeons in Private or General Practice (1821),and sought to establish new chapters of Kappa Lambda, whose members would pledge to adhere to the standards of conduct delineated in Percival's code.
When Dr. Brown went forth to spread the new Perivalean gospel, he found willing adherents in Philadelphia, where Samuel Jackson and seven other physicians (Franklin Bache, J.H.Gordon, Thomas Harris, Thomas T. Hewson, Hugh L. Hodge, Charlie D. Meigs, and Rene' La Roche)agreed to found a chapter. The Philadelphia constitution required all members to adhere to Percival's code of medical ethics and designated several members as "Guardians" with "the duty of preserving concord among all the members of the society, by arbitrating in all disputes referred to them, and prescribing the kind of reparation to be made .... (and) report(ing) ... whatever they may deem derogatory to its dignity and usefulness, in the misconduct of its members." The Philadelphia chapter of Kappa Lambda was thus to be a self-policing medical community that would abide by laws (stated in Percival's Medical Ethics) and that had guardians to police and enforce these laws.
Philadelphia may have been the only chapter of Kappa Lambda to take Dr. Brown's commitment to a self-policing moral community seriously. His ideas had been awkwardly juxtaposed on top of the original conception of Kappa Lambda as a secret fraternal order. The Philadelphia struggled with this fundamental tension in drafting their constitution. At the core of the old fraternal order was a secret oath passed down from society to society. Philadelphians were initiated into the society with the following oath:
You (swear/affirm) that you will endeavor to exalt the character of the Medical Profession by a life of virtue and honor--that you will keep the secrets, guard the reputations and advance the interest of the Society and of each of its members; and that you will never encourage anyone to devote himself to the Study of Medicine whose leaning, talents, and honorable qualities are not such as to render him respectable in his Profession, and worthy to be distinguished as a member of this society.
Whatever the original intent of this oath, its fraternal aspects--"advanc[ing] the interests ... of each of (the) members" and excluded from the profession, or at least from its higher ranks, anyone insufficiently virtuous, honorable, learned, or talented to be elected to Kappa Lambda--seem more prominent than its moral commitments.
Each chapter, moreover, was free to develop its own initiation ceremony. The Philadelphians used the ceremony to put a reformist spin on the oath. The following words were to be pronounced by Philadelphia initiates immediately after they read the oath:
The venerable Hippocrates of Cos may be considered as the remote founder of this society and the considered as the remote founder of this Society and the {oath/affirmation} which you have taken is in substance the same as that administered to its members. The influence of this society on the morals and professional demeanor of the physicians of that period is attested to by the most respectable authorities.
Believing that the state of the Profession in this country so imperiously calls for reformation & knowing that we have not that rank and influence in the community, to which as members of a liberal profession we are entitled, we have determined under a solemn sense of duty to associate on just principles for the purpose of elevating the character of our Vocation.
In other words, the oath was simply a ritual reminder of a historical reform movement. One could no longer reform medicine by excluding the unworthy, however, because "unworthy brethren" had already been admitted to the profession and had “humbled†the profession through their “sinister conduct.†The Problem facing the new Hippocrates, the Kappa Lambda, was reforming an already corrupt profession that problem could only b resolved by teaching the profession t associate on "just principles"(i.e., Percival's principles of Medical Ethics).
The need for "just" and benevolent principles of association is restated in the Preamble to the Philadelphia chapter's constitution, to which very member affixed their signature upon joining the organization.
As the bonds of all associations and confederacies by which their parts are firmly and permanently linked together, must be the eternal principles of benevolence and justice-we the undersigned-professing to follow implicitly, desirous of rigidly applying, these principles to our particular situation; uninfluenced by motive of personal ambition, disclaiming any right or wish to infringe on social compact, assume any power, delegate any authority which is incompatible with the religion we profess, the laws of our country or the fair and honourable advancement of our fellow citizen:--do hereby unite and pledge ourselves to be governed by the following constitution, and the laws which may afterwards be framed under it. Nor can we ever be unmindful, that our present efforts, directed to the support of the dignity, and extension of the usefulness of the medical profession, will more readily meet with their successful fulfillment in the encouragement of virtue and science, the pure lights of which must eventually dispel the mists of immorality and ignorance. To this end, we are to engraft medical ethics on moral precept, and sedulously cherish that friendly feeling and courteous conduct, in our professional and social intercourse, which can alone confer happiness on individuals, and promote the welfare of mankind.
With the words "uninfluenced by personal ambition ... [and] disclaiming any right or wish to infringe on ... the fair and honourable advancement of our fellow citizens" the Philadelphia chapter explicitly annulled the self-serving clauses of the traditional Kappa Lambda oath; indeed, by "engraft[ing Percival's] medical ethics on [Hippocratic] moral precept," they had effectively consigned the oath to a purely ceremonial function. The Philadelphia was thus continuing along the path taken by Samuel Brown (who beamed upon the Philadelphia branch and lauded its work), converting a vaguely Hippocratic elitist fraternal order into a society seriously committed to reforming American medicine.
The Philadelphia broke entirely new ground on another issue. Citizens of a city that was the center of the American science, the Philadelphia quite naturally wedded the two distinct ideas of scientific and moral reform into a single progressive union: pledging themselves to "the encouragement" of both "virtue and science" and to dispelling "the mists" of both "immorality and ignorance." Article V of the Philadelphia chapter's constitution made it morally obligatory for "Every member ... to contribute any practical fact, discovery, or view, which, in his opinion, will tend to the improvement of the profession, and the amelioration of the condition of the sick and infirm."
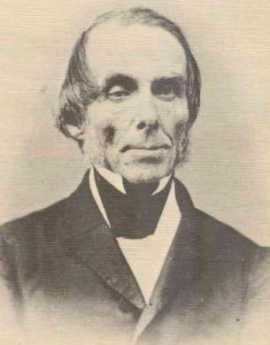
|
| John Bell, M.D. |
Such statements must have been intuitively obvious to the founding members of the Philadelphia chapter. When Samuel Jackson(l787-1872), who is generally credited with writing the constitution, formed the chapter in 1822, he was already professor of material medical at the Philadelphia College of Pharmacy and a member of the American Philosophical Society; by the time the constitution was formally enacted in 1825, he had become professor of the institutes of medicine at the University of Pennsylvania. A year later Franklin Bache (1792-1864) became a professor of chemistry at the Franklin Institute. Similar career patterns are evident in most of the other founding members; Hugh L. Hodge(l836-1881) was a lecturer on the principles of Surgery at the Medical Institute of Philadelphia, and went on to become a professor of obstetrics at the University of Pennsylvania; Charles D. Meigs (1792-1869 had been a member of the Academy of Natural Sciences of Philadelphia, became a member of the American Philosophical Society, and went on to become a professor of obstetrics at the Jefferson Medical College; Rene' la Roche(1795-1872) was a member of the Academy of Natural Sciences and, shortly after the constitution was approved, became a member of the American Philosophical Society.
The Philadelphia' fervor to reform medicine and to advance medical science clashed with the secret fraternal inclinations of traditional Kappa Lambda chapters. First, there was the issue of Percival's Medical Ethics. In 1823, following the precedent set by Dr. Brown, the Philadelphians published 500 copies of a newly revised editions of Percival' code, sending them to older chapters in Baltimore, Lexington, and New York, and distributing three copies to each member of the Philadelphia chapter(who appear to have used the extra copies to recruit new members). A new member, John Bell (1796-1872), was instructed to publish a copy of the Philadelphia edition of Extracts from the Medical Ethics of Percival in the National Gazette. He would later chair a subcommittee that revised and published yet another edition of the Extracts in 1826. As a member of a society committed to abiding by Percival's code, dedicated to disseminating its ideals, and seeking to recruit like-minded physicians, the Philadelphians thought it was perfectly natural to continuously revise and publish new editions of Percival. Yet publication was a disturbingly public activity for a supposedly secret society like Kappa Lambda.
Even more disturbing to the already established non-reform chapters of Kappa Lambda was the Philadelphia chapter's attempt to encourage scientific research by American physicians through The North American Medical and Surgical Journal. A regularly published journal was an event more public enterprise than the sporadic publication of revised editions of Percival's code. The New York chapter was instantly hostile to the idea, demanding that the existence of the Kappa Lambda society be kept secret. The District of Columbia chapter was concerned with the question of secrecy and wrote to the Philadelphia chapter to "ascertain particularly" whether in light of the "Journal which is to be proposed ... you intend to make public the existence of the KL societies generally." The journal's editors (Drs. Hodge, Bache, Meigs, Benjamin Homer Coates, and LaRoche) did not initially acknowledge the relationship between the journal and society. In February 1827, however, Dr. Meigs proposed that the Philadelphia chapter rescind its pledge of secrecy. The proposition was formally accepted by the membership in June. In meantime, the editors of The North American Medical and Surgical Journal announced that the Journal was supported by the Kappa Lambda Society.
Removing the Philadelphia Chapter from behind the shroud of secrecy was problematic. The older fraternal societies had never accepted Dr. Brown's reformist agenda and resisted it at every tum. A move vexatious challenge to publicity was the central reformist tenet of voluntary self-policing. It was one thing for members to volunteer to submit their personal and professional conduct to the private scrutiny and possible censure of their peers within the confidential confines of a secret society, it was quite another to voluntarily expose themselves to possible public censure. It took over two years to settle this question, when, in 1830, it was decided that all meetings would be opened to the public--except those involving inquiries into the conduct of the membership. This compromise in place, it was officially decided in June 1830 to announce the existence of the Philadelphia chapter of Kappa Lambda. By this time, however, the tide of public opinion had begun to tum against Kappa Lambda; all chapters were swamped in the backwash of a scandal over the conduct of the older non-reform New York chapter.
An anonymous letter to the Medical Society of the State of New York had revealed not only the existence of a "Secret Medical Association" operating in city , but the content of its secret oath, and the names of all its members--which included all the attending physicians and surgeons at the New York City Dispensary, the New York Hospital( except for one, ) and the Lying-in Hospital (except for two). The simple fact that a preponderance of members in the upper echelons of New York were members of a secret society prompted suspicions of favoritism. The Medical Society convened a Special Committee to Investigate a Secret Medical Association. The secret oath of the New York chapter of Kappa Lambda (a pre-reform chapter, founded around 1819) confirmed the Special Committee's worst suspicions.
I-do solemnly promise, that by all proper means, J will promote the professional respectability and welfare of the members of this association and vindicate their characters when unjustly assailed, and that J will not demand any pecuniary acknowledgment for such instruction as it may be convenient for me to afford to the son of an indigent member, as may be in the opinion of the society qualified by his previous educations, and talents, and moral character, to become a respectable and useful member of the profession, but I will afford such instruction gratuitously, in conjunction with the members of the society.
This oath, the Special Committee observed, acknowledge that the members of the society were pledged "to promote the professional respectability and welfare ... of each other." Moreover, when the Special Committee asked the members of the New York chapter what they had done as an Association for the cause of science and the honor of the profession, the New Yorkers could not cite any significant achievements. Consequently, on the evidence of the oath and the pattern of appointments at New York hospitals, the Special Committee concluded that members of Kappa Lambda had in fact created "an unjust monopoly of the emoluments and honors of the profession.: They had evoked the name "Hippocrates" simply to put a patina of honor and a veneer of venerability on the shameless pursuit of personal advantage. The Special Committee reprimanded all members of "the Secret Association" and advised any man of character to resign.

|
| Title Page of Volume I |
Prior to June 1830 the Philadelphia chapter of Kappa Lambda had been doing quite well. Beginning with a small group of eight initiates, it had rapidly enrolled many prominent physicians, ultimately initiating ninety-eight members--with seventy dues-paying members residing in Philadelphia. The North American Medical and Surgical Journal was generally regarded as one of America's leading medical periodicals. Meetings were well attended; some drew crowds of over forty members. Yet, after word of the Special Committee report reached Philadelphia, attendance fell below the minimal quorum required by Kappa Lambda's Constitution. The Only meeting that had a quorum large enough to conduct business was that of 5 February 1835, when ten members assembled to dissolve the chapter. Samuel Jackson resigned on the first word of the scandal, but many members simply ceased to pay their dues. Without the membership dues to sustain it, The North American Medical and Surgical Journal was discontinued.
It mattered little that no one had ever accused the members of the Philadelphia chapter of monopolizing emoluments and honors; it mattered even less than the Philadelphia chapter's constitution forbade favoritism concerning any member, or that it had tried to become a public society, or even that, in striking contrast to the New York chapter, it had made contributions to medical science by publishing a major medical journal and Percival's Medical Ethics. The Philadelphia chapter was still a society, and the Special Committee had argued that secrecy corrupted any society, no matter how noble its initial intent. The stigma attached to Kappa Lambda was so deep that as late as 1858, when the New York chapter of Kappa Lambda sent an openly-declared member as its representative to a national meeting of the AMA, his credentials were rejected.
The Story of Kappa is more than a quaint tale, for as Chauncey Leake has correctly observed: "the same forces[that] were at work in establishing the American Medical Association in 1847, and in passing its elaborate code of ethics." The Philadelphia "forces" exerted their influence at the end of a national medical convention that had been convened in New York in 1846 to set national standards for medical education. After two days of discussions, the conferees were unable to reach any consensus. The Meeting was about to dissolve in failure when hoping to salvage something from the failed convention, Isaac Hayes(l796-1879), former secretary of the Philadelphia chapter of Kappa Lambda, proposed that the convention reconvenes in Philadelphia the next year to create a national medical society dedicated to reforming American medicine--ethically as well as educationally. The convention delegates endorsed Dr. Hays' proposal and put him in charge of making arrangements for the 1847 Philadelphia convention. They also established a committee to draft national code of medical ethics. Chairing this committee was John Bell, who had chaired the 1826 Kappa Lambda Committee to revise Percival's Medical Ethics; Dr. Hays, who had been secretary and editor for the 1826 Kappa Lambda committee, played the same role for the 1846 code-drafting committee, The third Philadelphian on this committee, Governor Emerson (1796-1874), was also an alumnus of the Philadelphia chapter of Kappa Lambda.
The American Medical Association and its code of ethics were, as Leake suggests, an extension of the ideas and ideas that originated in the Philadelphia chapter of Kappa Lambda. Yet the failure of Kappa Lambda had taught the Philadelphians some important lessons. Kappa Lambda had been secret, fraternal, and exclusive; by contrast, the AMA was to be public, political, and inclusive--a grand public alliance of all the forces of reform and of all the hospitals, medical schools, and medical societies in America. Kappa Lambda had been founded on a gentlemanly version of the Hippocratic Oath. Chastened by their experience with corrupt versions of the Oath, the former Kappa Lambda eschewed any mention of Hippocrates of his oath in AMA Code of Ethics. The new AMA Code of Ethics, like the old Kappa Lambda code, was based on Percival ethics that called 0 physicians "to obey the calls of the sick," to treat every patient skillfully, attentively, faithfully, tenderly, but firmly while tempering medical authority with a spirit of equality. Moreover, "every case committed to the charge of a physician" would "be treated with attention, steadiness, and humanity"; every patient would be entitled to confidentially, delicacy and discretion. Yet the new AMA code of ethics required even more of physicians that the older Percival codes: having once been crucified on charges on selfishness and monopolization, the former Kappa Lambdans obligated physicians to self-sacrifice on behalf of their patients and the public. They required physicians to recognize "poverty ... as presenting valid claims for gratuitous services," and to pledge that "when pestilence prevails" it is their "duty to face the danger, and to continue their labors for the alleviation of suffering, even at the jeopardy of their own lives. "
The grand moral vision of the former Kappa Lambda energized the American Medical Association and made it the preeminent moral and political voice of American medicine. In the twentieth century, as the Kappa Lambda's reformist vision lost its vigor, the tale of Kappa Lambda became the stuff of scholarly debate=most scholars have tended to dismiss it as an idiosyncratic and ultimately unimportant chapter in the history of American medicine. Yet it seemed to me, as I surveyed the records that the Kappa Lambdans had turned over to the College of Physicians of Philadelphia, that 1997 was an appropriate time to reassess its legacy. For in wrestling with the task of developing formal standards of medical ethics that could serve as the basic of professional self-policing, in obligating American physicians to serve the interests of the public as well as their willingness to put the care of their patients ahead of their own financial interests and physical safety, the Kappa Lambda had formulated very high ideals for American medicine. Looking back on these ideals on the sesquicentennial of the founding of the American Medical Association and its Code of Ethics one is still struck by the grandeur of their moral vision--and also by the thought that the prominent role ethics still plays in American medicine is ultimately the heritage of the Philadelphia chapter of Kappa Lambda.
Robert Baker, Ph.D.
Union College, New York
Lumpers In Constant Combat With Splitters
|
| James Boswell's Book |
Some colleges produce managers by teaching management theory, but in certain Ivy League colleges it is thought to be more useful to teach how to dominate a committee, eventually perhaps a board of directors, or a board of trustees. The handbook of instruction is James Boswell's Life of Johnson which is a rather large book of verbatim notes that Boswell took of his many lunches at a London club in the 18th Century. Boswell was a quiet mouse privileged to sit in the company of the great Dr. Samuel Johnson, surrounded by the most eminent intellects of the Enlightenment. Boswell carefully manages the background of each episode, describing the issue and the various arguments, and then -- Sam Johnson's booming voice settles the matter. After he speaks, the meeting is over.

|
| Dr. Samuel Johnson |
"Why, sir", says Johnson, and then look out for the one-liner to follow. We get the impression that Dr. Johnson used that "Sir" signal to indicate he had enough of these dumb arguments, and soon would come the growled epigram that scatters any token resistance. Boswell may have neglected to record instances where the great Johnson was defeated in debate, who knows. We are left with the distinct impression that if you engaged in lunch table conversation with Sam, you were almost certain to lose. So that's what Ivy League students are being taught: how to win a debate at a committee meeting, in the expectation they would spend much of their lives in committees, boards, and even cabinets. That's how the English-speaking world gets its work done and its decisions made. That's what lunches at the Franklin Inn Club, or the club tables of the Union League, are trying to do for the education of neophytes.
As the goggle-eyed student of the great Chauncey Tinker, who gave young Pottle his start in life, it was an awesome performance for me to watch. But the rules of this game never became entirely clear to me, I'm afraid, until the other evening when I listened to Peter Nowell describe in a half-dozen brief paragraphs how he had revolutionized prevailing theories of the cause of cancer. The Franklin Institute then followed the award ceremony by putting on an all-day symposium of notables who run elaborate enterprises in cancer research, essentially funded by the National Institutes of Health, your tax dollars at work again. Last year, the NIH dispensed thirty billion -- you heard me -- dollars in research grants to internationally known research entrepreneurs, and if you can stay awake during their talks, there must be something the matter with you. So far as I could see, they were painstakingly describing every grain of sand on the beach, whereas Peter Nowell made the whole beach electric and clear in ten minutes. Essentially, he was saying that each patient's cancer is caused by a long chain of events, starting with a single mutation within a single cell. All the other cancer cells of a patient are descendants of that first one, which triggered the cascade of chemical events now repeated by the descendants. To stop the process, you probably only have to find a way to break the chain at one vulnerable point. Then you have a cure, without necessarily understanding every other link in the chain.
Peter Nowell described himself as a "lumper", admitting that most scientists are "splitters". A splitter quite reasonably attacks a complex problem by isolating one small piece of it at a time; that's really a pretty good way to address overwhelming complexity when you encounter it. But you can be sure that people of that mindset should not be found in a President's cabinet, deciding how to save the world from impending disaster. Whether by their own genetic predisposition or as a result of peer pressure in their profession, they are habitual splitters. And it suddenly occurred to me why Sam Johnson's one-liners always won the argument; he was a lumper. Usually right, sometimes wrong, never in doubt. Witty as a Frenchman, but as quick as a rattlesnake. Cordial, perhaps, unless you disagreed with him.
We need more lumpers. If they get that way from the likes of Chauncey Tinker, we need to print more copies of The Life of Johnson. If they are born that way, maybe we need a breeding farm for lumpers, which is what the Assembly Ball amounts to. But don't get me wrong, we need more splitters, too. They just have to learn their place at the table.
A Toast To Silas Weir Mitchell, MD
|
| Silas Weir Mitchell |
Silas Weir Mitchell lived to be an old man during the Nineteenth Century when it was unusual to get very old. He was an important part of both the Philadelphia medical scene and the literary one. He became known as the Father of American Neurology as a published studies of nerve injuries caused by the Civil War. He published about 150 scientific papers, including famous investigations of the neurological effects of rattlesnake venom. His most famous medical treatment was the "rest cure" for hysteria, while his most enduring scientific discovery was the phenomenon of causalgia. He despised Freud, and psychonanalysis. No doubt the feeling was mutual, but the passage of time has tended to favor Mitchell more than Freud. The central role of sex is the essence of Freud's viewpoint, while Mitchell is summarized in the remark that, "those who do not know sick women, do not know women."Struggling medical students can take heart from the well-documented fact that Mitchell applied to the Pennsylvania Hospital for an internship, and was rejected. Upset by the experience, he toured Europe for a year and applied again. He was again rejected. He later applied for the faculty at Jefferson and was rejected, but his reaction to that was one of rage and vengeance. Just what these two episodes out of Philadelphia medical politics really mean, remains to be clarified by Mitchell's biographers.

|
| Franklin Inn |
Mitchell's second career was literary, publishing 12 novels and 5 books of poetry. He is honored as the founder of the Franklin Inn Club, for century home to every important literary figure in Philadelphia. It is striking that he selected Benjamin Franklin as the guiding star of the Inn since Franklin similarly was eminent in both science and culture, and an ornament to conversation and society. In a pacifist Quaker City, both men approved of combat, and his novel about Hugh Wynne stresses that his hero was a "Free Quaker, meaning one who fought in the Revolution. Because of his strong Republican views, he was never made a professor at the local medical school.

|
| College of Physicians |
Mitchell's patient Andrew Carnegie donated the funds to build a new building for the College of Physicians when Mitchell was its President. When Mitchell was president of the Franklin Inn, Carnegie wrote him, asking for suggestions about donating a small sum, say five or ten million, and asking where it should go. That was the Inn's big chance, all right, but somehow it failed the test. Mitchell suggested that the money be given to raise the salaries of college professors, thus perhaps suggesting that this veteran of many academic revolts did eventually soften his views.
Eakins and Doctors

|
| The Gross Clinic |
A Christmas visitor from New York announced he read in the New York newspapers that Philadelphia's mayor had just rescued a painting called The Gross Clinic, for the city of Philadelphia. The Philadelphia physicians who heard this version of events from an outsider reacted frostily, grumpily, and in stone silence. To them, the mayor was just grandstanding again, and whatever the New York newspaper reporters may have thought they were saying was anybody's conjecture.
Thomas Eakins is known to have painted the portraits of eighteen Philadelphia physicians. Several of these portraits have been highly praised and richly appraised, seen in the art world as part of a larger depiction of Philadelphia itself in the days of its Nineteenth-century eminence. That's quite different from its colonial eminence, with George Washington, Ben Franklin, the Declaration and all that. And of course entirely different from its present overshadowed status, compared with that overpriced Disneyland eighty miles to the North. Eakins depicted the rowers on the Schuylkill, and the respectable folks of the professions, every scene reeking with Victorian reminders. It's a little hard to imagine any big-city mayor of the present century in that environment. Indeed, it is hard to imagine most contemporary Americans in a Victorian environment -- except in Philadelphia, Boston, and perhaps Baltimore. So, Mayor Street can be forgiven for not knowing exactly what stance to take, and was not alone in that condition.
S. Weir Mitchell, for example, became known as the father of neurology as a result of his studies and descriptions of wartime nerve injuries. But the repair of injuries is a surgical art, and many novel procedures were invented and even perfected, many textbooks were written. Amphitheaters were constructed around the operating tables, for students and medical visitors to watch the famous masters at work.
In The Gross Clinic, we see the flamboyant surgeon in the pit of his amphitheater at Jefferson Hospital, in the background we see anesthesia being administered. Up until the invention of anesthesia, the most prized quality in a surgeon was speed. With whiskey for the patient and several attendants to hold him down, the surgeon had one or two minutes to do his job; no patient could stand much more than that. After the introduction of anesthesia, it might overwhelm newcomers to observe leisurely nonchalance, but in truth, the patient felt nothing, so the surgeon could safely pause and lecture to his nauseated admirers.
|
| Operating Amphitheater |
What made an operation dangerous was not its duration, but the subsequent complications of wound infection. By 1876, Eakins could have had no idea that Pasteur and Lister were going to address that issue in four or five years, making operations safe as well as painless. But his depiction of a surgeon with bloody bare hands, standing in Victorian formal street clothes, gives the most dramatic possible emphasis in the painting to the two most important scientific advances of the century. Modern medical students spend days or weeks learning the ceremonial of the five-minute scrubbing of hands with a stiff and somewhat painful brush, the elaborate robing of the high priest in a sterile gown by a nurse attendant, hands held high. The rubber gloves, the mystery of a face mask and cap. In some schools, the drill is to cover the hands of a neophyte with charcoal dust, blindfold him, and insist that he scrub off every speck of dirt that he cannot see before he is admitted to the operating theater for the first time. If he brushes some object in passing, he is banished to the scrub room to start over. So the Gross Clinic has an impact on everyone who sees the surgeon in street clothes, but it is trivial compared with the impact that painting has on every medical student who has been forced to learn the stern modern ritual. For at least fifty years, that painting hung on the wall facing the main entrance to the medical school, where every student had to pass it every day. To every graduate, the lack of clean surgical technique by the famous man was a wrenching sermon on every doctor's risk of trying his utmost to do his best, but doing the wrong thing.
That painting, hanging quite high, was rather cleverly displayed to the public through a large window above the door. With clever lighting, every layman who walked along busy Walnut Street could see it, too, and it became a part of Philadelphia. That was a feature the medical community barely noticed, but it was probably the main reason for public uproar when a billionaire heiress offered the school $68 million to take the painting to Arkansas. The painting was not just an icon for the medical profession, it had become a central part of Philadelphia. Philadelphia wanted to keep that painting for a variety of reasons, and one of the main ones was probably a sense of shame that we were so poor we had to sell our family heirlooms to hill-billies.
The doctors didn't pay much attention to that. They were mad, plenty mad, that a Philadelphia board of trustees would appoint a president from elsewhere who would give any consideration at all to such an impertinent offer.
Link to:Medical Club of Philadelphia
This concludes the general topic Medicine in Philadelphia. The more specific topic area of the Medical Club of Philadelphia (founded 1892 and still operating) can be reached by clicking on the title below. It's large, so wait a moment for it to come up:
» Click here for THE MEDICAL CLUB OF PHILADELPHIA «
Medical Club of Philadelphia, Appendix B, Membership
The Club grew robustly to the point where it attained a total of 1.393 members 1924 (In 1911 it had a thousand members compared to a total of forty thousand in the American Medical Association.) Exact figures are not available for all years. Some totals were taken from Annual Reports, but these figures are distorted by the fact that for many decades they continued to count persons who were two years delinquent in dues, as members. In some cases, they also counted applicants who had not paid any dues or admission fees. It was not until the 1970s that dues were collected before applicants were elected to membership.
For some years numbers were computed from records of dues & initiation fees paid. In other cases, where members were elected late in the year, their dues were credited both to the year paid and following year. Financial records are not available for some years, and in others, there simply are no records from which figures can be computed.
1893 570
1899 230
1900 313
1901 365
1902 460
1903 570
1904 644
1905 614
1906 640
1907 799
1908 846
1909 928
1910 931
1911 998
1912 1,010
1913 999
1914 1,042
1915
1916 1,107
1917 1,121
1918 1,067
1919 1,190
1920 1,211
1921 1,235
1922 1,205
1923
1924 1,393
1925 1,362
1926 1,359
1927 1,258
1928 1,329
1929 1,288
1930 1,348
1931 1,247
1932 1,159
1933 1,079
1934 982
1935 936
1936 910
1937 868
1938 821
1939 854
1940 860
1941 870
1942 767
1943 749
1944 748
1945 752
1946 765
1947 792
1948 990
1949 1,007
1950 965 (Dues increased
1951 942 from $5 to $10)
1952 958
1953 936
1954 924
1955 880
1956 876
1957 857
1958 800
1959 802
1960 799
1961 756
1962 724
1963 728
1964 703
1965 696
1966 684
1967 679
1968 671
1969 674
1970 654
1971 619
1972 629
1973 590
1974
1975 669
1976 555
1977 446 (Dues increased
1978 410 to $25)
1979 410
1980 412
1981 379
1982 387
1983 398
1984 329 (Dues increased
1985 409 to $35)
1986 390
1897 397
1988 387
1989 400
1990 398
1991 388
Appendix D, Presidents of the Club
Presidents of the Medical Club
*1892-4 John H.W. Chestnut, M.D.
*1895-6 Hobart A. Hare,M.D.
*1897-8 John H. Musser,M.D.
*1899-0 James M. Anders,M.D.
*1901-2 Edward L.Duer, M.D.
*1903-4 Edward E. Montgomery, M.D.
*1905-6 Roland G. Curtin, M.D.
*1907 L.Webster Fox, M.D.
*1908 George McClellan, M.D.
*1909 Wharton Sinker, M.D.
*1910 James B. Walker, M.D.
*1911 William L. Rodman, M.D.
*1912 S. Lewis Ziegler, M.D.
*1913 James C. Wilson, M.D.
*1914 Samuel D. Risley, M.D.
*1915 McCluney Radcliffe, M.D.
*1916 Judson Daland, M.D.
*1917 Charles K.Mills, M.D.
*1918 Albert P. Brubaker, M.D.
*1919 G. Oram Ring, M.D.
*1920 Francis X. Dercum, M.D.
*1921 Barton C. Hurst, M.D.
*1922 Ernest Laplace, M.D.
*1923 John B. Clark, M.D.
*1924 William D. Robinson, M.D.
*1925 Charles W. Burr, M.D.
*1926 Wilmer Krusen, M.D.
*1927 J. Torrance Rugh, M.D.
*1928 Orlando H. Petty, M.D.
*1929 J. Norman Henry, M.D.
*1930 John M. Fisher, M.D.
*1931 Frank C. Hammond, M.D.
*1932 Isador P. Strittmatter, M.D.
*1933 George M. Piersol, M.D.
*1934 Charles A. E. Codman, M.D.
*1935 Edward J. Klopp, M.D.
*1936 Paul J. Pontius, M.D.
*1937 Frederick S. Baldi, M.D.
*1938 John D. Mclean, M.D.
*1939 Henry B. Kobler, M.D.
*1940 Milton F. Percival, M.D.
*1941 W.Burrill Odenatt, M.D.
*1942 Walt P. Conaway, M.D.
*1943 Wayne P. Killian, M.D.
*1944 William Bates, M.D.
*1945 Bernard P. Widmann, M.D.
*1946 J. Allan Bertolet, M.D.
*1947 Edgar S. Buyers, M.D.
*1948 Joseph W. Post, M.D.
*1949 Eugene P. Pendergrass, M.D.
*1950 Joseph C. Birdsall, M.D.
*1951 Francis F. Borzall, M.D.
*1952 Myer Solis-Cohen, M.D.
*1953 Sameul G. Shepherd, M.D.
*1954 Theodore R. Fetter, M.D.
*1955 Francis G. Harrison, Sr., M.D.
*1956 George E. Pfahler, M.D.
*1957 Edward A. Bortz, M.D.
*1958 William A. Lell, M.D.
*1959 George E. Cormeny, M.D.
*1960 J. Rudolph Jaeger, M.D.
*1961 Jacob H. Vastine, M.D.
*1962 Joseph M. Kuder, M.D.
*1963 Henry S. Bourland, M.D.
*1964 Francis G. Harrison, Jr., M.D.
1965 Thomas M. Birdsall, M.D.
1966 George P. Keefer, M.D.
1967 Frederick Murtagh, M.D.
1968 Robert E. Booth, M.D.
*1969 Frederic H. Leavitt, M.D.
*1970 Paul J. Poinsard, M.D.
*1971 Elmer L. Grimes, M.D.
1972 Edmond Preston,III, M.D.
*1973 N. Henry Moss, M.D.
1974 Richard C. Putnam, M.D
1975 Federick P. Sutliff, M.D.
1976 H. Keith Fischer,M.D.
1977 H. Craig Bell, M.D.
1978 Thomas B. Mervine, M.D.
1979 F. Peter Kohler, M.D.
1980 Goerge E. Ehrlich, M.D.
1981 Robert D. Harwick, M.D.
*1982 Stewart McCracken, M.D.
1983 Joseph A. Wagner, M.D.
1984 Edward J. Resnick, M.D.
1985 Eugene B. Rex, M.D.
1986 John A. Koltes, M.D.
1987 James C. Hutchison, M.D.
1988 Timothy J. Michals, M.D.
1989 Joseph W. Sokolowski, M.D.
1990 Herminio Muniz, M.D.
1991 F. Douglas Raymond, Jr., M.D.
1992 Raymond Q. Seyler, M.D.
A Toast To J. William White, MD
JWilliam White left a legacy to the Franklin Inn, the income from which was to pay for an annual dinner, with all the trimmings. Good as its word, the Inn holds the J. William White dinner every year on Benjamin Franklin's birthday, although inflation and fluctuations of the stock market require it to make a modest charge for attendance. White also created the J. William White Professorship in Surgery at the University of Pennsylvania, a chair which was once occupied by Jonathan Rhoads.

|
| William J White MD |
These trust-fund memorials do little to convey the wild and glamorous image of Bill White. White was a member of the First City Troop and fought the last known honest-to-goodness duel on Philadelphia's field of honor (in the accidental "wedge" of disputed land between Delaware and Pennsylvania). The right and wrong of the argument about wearing the City Troop uniform are in dispute, but the details boiled down to White at the critical moment raising his gun to the sky and firing at the stars. That it was not a meaningless gesture was then brought out by his opponent ( a fellow Trooper named Adams) taking slow and deadly aim -- but missing him.
White was an academic in the sense that he was the first, unpaid, Professor of Physical Culture at the University of Pennsylvania. Active in the Mask and Wig Club, he was a chief surgeon at Philadelphia General Hospital, chief surgeon to the Philadelphia Police, and chief surgeon to the Pennsylvania Rail Road. He is the surgeon actually operating in Thomas Eakins' Agnew Clinic, while Agnew himself stands as the "rainmaker", to use a term from legal circles. He was Chairman of the Fairmount Park Commission, and numerous other positions where political contact was more important than surgical skill. When World War I came along, he was off to France with the University of Pennsylvania Hospital Unit, writing two books with Theodore Roosevelt. Although his friendship with Henry James suggests greater literary talent, he was supportive of Adams' transfer of citizenship in protest of America's staying out of World War I; but nonetheless, Roosevelt published more than thirty books. What emerges from the history of Bill White is flamboyance and lots and lots of unfettered energy. He might feel a little out of place at one of his endowed dinners today, but he was probably always a little out of place in any company -- and didn't care a whit.
REFERENCES
| Philadelphia Gentlemen: The Making of a National Upper Class: E. Digby Baltzell ISBN-13: 978-0887387890 | Amazon |
Victor Rambo, Indian Eye Surgeon
|
| Apostle of Sight |
There have been at least twelve documented generations of the Rambo family in Philadelphia. Historical justification can be found for the idea that this was the first family to settle within what are now the city limits. Victor Clough Rambo MD was an unpaid intern at the Pennsylvania Hospital in 1927; you will find his nameplate on the wall.
Victor early made up his mind that he was going to go where he could do the most good. Considerable thought led him to learn how to extract cataracts, and go to India to extract as many as he could. from time to time, he would return to America to visit family, and to give some speeches to raise money for his project.
The builders of our enormously costly hospital castles might give some thought to the fact that Victor did most of his surgery in tents. His system was to send out teams to the next two villages, whenever he was, with the news, "Bring in your blind people, the eye doctor is coming." When he then arrived, he set about operating on cataracts from dawn to dusk, in a country where the supply of cataracts was essentially unlimited. There was no time to operate on the comparatively minor visual disturbances so commonly treated in America today; he had to concentrate on people who were really blind, and in both eyes.
He wrote a book about his experiences, and perhaps there you could find data to calculate the number of people who were restored to a useful existence by his efforts. Surely, it was thousands. He just kept going at it, and when he died he was a very old man.
Emperor's Doctor

|
| Kitamura |
As told by one of his fellow interns who is now a very old man, Kitamura was one of the best interns the Pennsylvania Hospital ever had; diligent, dependable, intelligent and infinitely polite. He married one of the hospital's nurses, and they tended to keep to themselves, especially in 1941, as war clouds began to gather. About two months before Pearl Harbor, both of them mysteriously disappeared. Kimura's wife later wrote one of her friends that they were in Japan. After the war, it was learned that she had been placed in a concentration camp as an enemy alien, and when released, had divorced him.
Still later, it was learned that Kimura had a distinguished medical career in Japan. He kept up a minimal sort of correspondence with his old intern pals, inviting them to visit if they were ever in Japan.
In 1985 one of them did so, going to the largest hospital in Tokyo to inquire. Great silence ensued; unfortunately, the revered and distinguished physician had recently died. You knew, of course, that he was the Emperor's personal physician.
Discipline for the Disciple

|
I.S.Ravdin was President Eisenhower's surgeon; Chick Koop was President Reagan's Surgeon General. Both of them were overshadowed by Jonathan Rhoads. Even in a physical sense, this was true. Rhoads was a foot taller than almost anyone. Big bones, too.
{kind=link}
During the Second World War, Ravdin led almost every doctor in the University of Pennsylvania off to some military hospital unit or other, and in fact, the 900-bed hospital in Philadelphia was left with only two surgeons, Koop and Rhoads, ineligible for military service because of previous tuberculosis. Koop was a first-year resident in training, so for practical purposes, Rhoads was the only surgeon. Even after eliminating purely elective or optional surgery, the workload was staggering, and the number of operations was prodigious.
Rhoads devised a system. The young trainee, Koop, would do the time-consuming work of opening the belly wall and Rhoads would then do the internal surgery, following which Koop would close the wound while Rhoads was operating on another patient. As Koop told the story at Rhoads' 90th birthday celebration, one day a patient was to have his gall bladder removed. Rhoads told him to open the wound, first, the skin, then the fascial layer, then the peritoneum, while he was finishing up with another patient in another room. At that point, Rhoads felt he would be able to come in and remove the gall bladder. Most gall blabbers are firmly attached to the nearby liver, and must be shaved loose before it is possible to put a clamp around the base to remove them.
{kind=link}
{kind=link}
On this day, two things were different. Rhoads was delayed in the other room because of some complication, and Koop was just standing around waiting. The other thing that was different was that this particular gall bladder was not attached to the liver at all, but was just flopping around in the belly. When Rhoads continued to be delayed, Koop just went ahead and clipped off the gall bladder; more time elapsed. So he carefully sewed up the peritoneal layer, then the fascial layer, then the skin, stitch by stitch. He was standing there pretty pleased with himself when the doors finally banged open and Rhoads came charging into the operating room.
Koop offered some explanation in a faltering way, but Rhoads did not say a word. A large elbow on a huge arm silently but forcefully brushed Koop off to one side in a single movement. Rhoads then took out each stitch in the skin, then the stitches in the fascia, then the stitches in the peritoneum. He peered into the cavity, inspected the former bed of the gall bladder. Finding things in good order, he then resutured the peritoneum, then the fascia, then the skin. Without a word, he then strode from the room, leaving the future Surgeon General never to forget the lesson he had been taught.
Mind Your Manners

|
| Hoeffel |
In 1948 I was an intern at the old Pennsylvania Hospital, assigned for a while to the accident room. One of the accident-room duties of an intern is to sew up cuts and lacerations that arrive unexpectedly, but some lacerations can be out of your pay-grade and you have to call for help. On the evening in question, the victim had been so thoroughly slashed up that I had to call the chief surgical resident, Dr. Joseph Hoeffel. Hoeffel was big, tall, loud and self-assured, and swept majestically into the accident room with a little fellow trailing him. This follower seemed less than four feet tall but very quick and shifty. He didn't walk so much as he scuttled. Hoeffel bellowed, "Get out here!" and the gnome vanished.
While Joe was examining the laceration problem, the little fellow slipped through a different door to see what was going on. Most of us had the impression this guy might well be the one who inflicted the cuts, but in any event, he didn't belong where he was. "I told you to get out of here, and stay out," bellowed our surgeon. Again the scuttler scuttled away, while Hoeffel put on a sterile gown, sterile rubber gloves, mask, cap, and the whole ceremonial costume. He prepared to do his work, stamping out disease among the sick and injured, when a fist started at the floor. The little guy had slipped into the operating area once more, and soon the fist on the floor quickly flew in a wide arc, ending up on Hoeffel's jaw.
Hoeffel tumbled head over heels across the room, ending up in a corner. I don't think he was knocked out, but he was certainly dazed. The nurses called the police, who made a tumult of their own arriving to do battle. But the little fellow was gone, never to be seen again.
Fifty years later, I had occasion to preside over a meeting of the Right Angle Club, where
Hoeffel's son, the former congressman and current deputy member of the Pennsylvania Governor's cabinet, was the featured speaker. He looked remarkably like his father. I had to wonder if his father's lesson in diplomacy had made any notable effect on his progeny.
Funny Toes: A Physician Viewpoint

|
| Webbed Toes |
It probably took me twenty years to notice that, unlike most people, I had an incomplete separation of my second and third toes. I thought my toes were like everybody else's, but once you start peeking, you see that webbed toes are not normal, although they are not really rare, either. After another thirty years, it became apparent that most of my numerous descendants had the same kind of toe; it was obviously an inherited condition. When the family clan gathered at the beach, it was a source of mild amusement, possibly even a little pride. A few weeks ago, I happened to mention the matter at a party, whereupon another doctor promptly pulled off his shoes and socks, and revealed fused or webbed toes of a much more striking sort than mine; obviously, he was proud of it, too. He is of an old, old Philadelphia family that owns one of the oldest, if not the oldest, a house in Germantown. His family, too, is stigmatized in the same way only more so. In Philadelphia, when you are proud of your family, you are really, really, proud of it.

|
| Ainhum |
Which brings me back to my days as an intern in the accident room of the Pennsylvania Hospital. When there is a sudden crowd of emergencies in an emergency department, the nurses get all of them undressed, put in a hospital gown, and instructed to wait for the doctor behind a curtain that doesn't quite reach the floor. For some reason, as a medical student, I had been particularly struck by a photograph in a textbook of an inherited disorder said to have been first noted on a slave ship; the disease in the native language was named Ainhum. For reasons obscure, a tight little band appears at the base of the fifth, or little, too. It gets slowly tighter over a period of months, and eventually, the little toe falls off. That's all there is to Aihnum, and all that was known about it. So, imagine my surprise and delight to walk past a row of naked feet sticking out below curtains -- and there was my first and last case of Aihnum.
I summoned my colleagues, and the visiting medical students from both Jefferson and Penn who at that time shared training in our accident room. I raced off to my room to get a camera to record this momentous event. An elderly staff physician, either Tom McMillan or Charles Hatfield, wandered past and was invited to share the excitement. Well, he says, I saw one of those forty years ago, it looked just like that; old Doctor Norris showed it to me when I was an intern. Much murmuring ensued but abruptly stopped when the patient himself rose up and started putting on his clothes. He was going home, but why? "Well," he growled, "I came here because my back hurts, and all you people do is look at my toes!" He said he was going over to the Jefferson Hospital to get proper treatment, and I guess he did.
And finally, there is Morton's Toe. Or perhaps more properly, Mortons' Toes. There were in fact two Doctor Mortons, one of them at Columbia College of Physicians and Surgeons where I went to school, and the other at the Pennsylvania Hospital where I interned. In New York, Morton's Toe refers to a painful callous, or neuroma, that forms on the bottom of the victim's big toe. In Philadelphia, such an answer would get a failing grade, because the Philadelphia Morton had noticed that some people have a big toe that is shorter than the other toes, instead of being bigger as the term would suggest was proper. The tricky thing about this relatively harmless variant is that the big toe is actually not short at all. The foot bone, or metatarsal, is short, so the toe of normal length sits back farther on the foot and just looks shorter. The main significance is for shoe salesmen since the shoe needs to be long enough to avoid crushing the other toes.
So now, you readers who were not lucky enough to go to medical school can get a feeling for what it seems like to be a doctor. The other significant shared bond within the fraternity is a sense of outrage at the way health insurance companies drag their feet paying doctors, but that's not limited to feet..
Albert C. Barnes, M.D.
A private investor has the general goal of accumulating enough wealth so, come what may, there will be a little left when he dies. If he has dependents or heirs, he needs somewhat more. Either way, he is not planning for perpetuity or thinking in astronomical time periods. Albert C. Barnes (1872-1951) had to switch his investment goals, in the 1920s, from investing for a comfortable retirement to investing for a perpetual art foundation. Perpetual.
|
| A bottle of Argyrol |
Having graduated from medical school (University of Pennsylvania) in 1902, and then writing a doctoral thesis in chemistry and pharmacology at the Universities of Berlin and Heidelberg, Barnes invented a patent medicine that quickly made him rich. Argyrol was a mildly effective silver-containing antiseptic with the unfortunate tendency to turn its users permanently slate-gray. The advent of antibiotics has since made Argyrol almost sound like quackery, but it was effective enough at the time to require factories in America, Europe, and Australia, and Barnes became immensely rich with it. The American Medical Association strongly disapproves of physicians who patent remedies, so Barnes was never held in high regard by his colleagues; but it could well be argued that he had as much training as a chemist as a physician, and spent his entire professional life as a chemist, manufacturer, and investor.

|
| The Barnes Gallery |
Barnes was eccentric, all right, but on Wall Street, the saying goes, "What everyone knows, isn't worth knowing." Guided by that principle, in 1929 he sold his company at the very peak of market euphoria, getting out of common stocks at the top of the market. It is small wonder that he soon instructed his Foundation to invest its endowment entirely in bonds. During the 1930s, commodities were extremely cheap because no one had any money. Barnes, of course, had a potful of money and bought hundreds, even thousands, of artworks very cheaply. He also bought 137 acres of Chester County, PA, real estate, and a 12-acre arboretum in Merion Township on the Main Line. Although he is famous for acquiring hundreds of French Impressionist paintings with the advice of Gertrude Stein and her brother Leo, he also bought great quantities of Greek and Roman classical art, African art, and the art of the Pennsylvania German community. He picked up a notable collection of metallic art objects. Most of these "losers" are down in the basement because he had so many Renoirs, Matisse, and Picasso (some of them may be worth $200 million apiece) that the upstairs galleries were pretty well stuffed with them. Viewed from the perspective of an investor with a goal of perpetuity, of course, the things in the basement just happen to be temporarily out of fashion, just like those bonds in the portfolio.
|
| A view inside the Barnes gallery |
Since the Foundation is currently strapped for ready cash, Judge Stanley Ott of the Montgomery County Orphans Court is now being urged to allow the Foundation to break Barnes' will in some way or other. Move the museum to downtown Philadelphia where it can attract more paying visitors. Sell some of that land. Sell some of those paintings in the cellar. Fire some of those employees. But all of these suggestions are short-term solutions, which may injure the long term. Everybody has an idea of what Barnes the rich eccentric would have done if he were alive to do it, but I suspect he would have rejected the whole lot. Barnes the shrewd investor would have taken the most expensive painting off the wall, and sold it to the highest bidder. Buy low, sell high, and the niceties of non-profit professionals are damned. Barnes wasn't in love with one single painting, or one particular school of painterly interpretation, he was in love with Art.
Investment theory has improved in the past fifty years; there have even been some Nobel prizes awarded for new insights. But it still isn't possible to put an investment portfolio on autopilot for perpetuity. Every museum, university, and the foundation has the same problem, with the result that the landscape is littered with the bones of perpetual organizations destroyed by following a fixed formula. With the singular success that Barnes displayed, it isn't surprising that he went a little too far with instructing his successor trustees in what to invest in. Never sell the paintings or the real estate, avoid the common stock, were ideas that worked brilliantly, and may even work most of the time. But sooner or later, the institution will be endangered by following them too literally. Somebody has to have some flexibility. But there is something else that is inevitable, too. Sooner or later, whether it takes fifty years or five hundred years, sooner or later someone will be given the responsibility and the necessary flexibility -- but will try to run off with the boodle, for himself. The balance between necessary prudence and necessary flexibility is impossible to maintain forever, and the Judge will surely have a hard time deciding what Barnes would have decided.
The Barnes Foundation: Comments on the Economics of Art (2)
In 1951, Albert C. Barnes' legacy included Jerome's Epistle to Paulinus from the Gutenberg Bible education centered on a notable collection of illustrative artworks, housed in a museum of his own general design for the purpose. He left a multi-million dollar endowment to support his rather detailed and, in the opinion of many, somewhat eccentric intentions. It was his money, however, so his word was final. The institution was fairly mature, having previously been in operation under his direct control for twenty-five years.
Since the Foundation trustees are now before the Orphans Court pleading for permission to modify Dr. Barnes' instructions in order to avoid financial collapse, skepticism is inevitable. Obviously, the successor trustees must explain their expenses. But quite a plausible case can be made that the true cause of this disaster is inherent in the huge windfall growth in value of the paintings. In short, growth in value of the fine art may have outstripped the growth of the resources set aside for maintenance.

|
| Johann Gutenberg, creator of mass produced books, died in poverty |
Let's make a benchmark of the Gutenberg Bible, where incomplete copies are currently selling for $100,000 a page and complete copies are estimated to be worth $100 million apiece. Dealers maintain the Gutenberg is increasing in value at 20% a year, but growth seems closer to 9% a year if you go back to 1951. What's really relevant here is the growth in cost to ensure, protect, dehumidify, display and make it available to scholars, if not the public. It seems safe to guess these maintenance costs have grown more rapidly than the investment growth of the endowment, which is surely closer to 4% than 20%. The imbalance is even greater if you remember that some investment income is spent every year, while the worth of the fine art just grows and grows. Regardless of the true numbers, if the cost of maintaining the art does grow even slightly faster than the endowment, the dilemma the Barnes is now facing will eventually face any museum. New sources of revenue, either from the government or from public admissions, eventually becomes necessary if the priceless art remains on display. It is displaying these things that cost money; burying them under an Aztec mound or a German salt mine shelters them from the problem. In the case of Alfred Barnes, it is not completely certain that he wanted them displayed.
There is also the issue of quirky fluctuations in the market for fine art. The 22 known perfect copies of Gutenberg, Bibles have been around for almost five hundred years, and it is safe to say their value is enduring. The 180 paintings by Renoir now owned by the Barnes may prove to be Gutenberg Bibles or they may prove to be a passing fad, but it is pretty hard to believe that one of them will always be worth two Gutenbergs. Since there is a pretty fair chance that we are currently seeing a value bubble in French Impressionist painting, it is questionably prudent to shipwreck the whole Barnes Foundation, the School, or Albert C. Barnes basic intent, by resisting the sale of even one of the more overpriced examples in the collection at the top of the market.
That's one side of it. Another consideration is that Barnes himself did considerable merger negotiation with other museums, and may have been unexpectedly killed in an auto accident before he turned over all his cards in that particular poker game. It's asking a lot of the poor judge to overturn the clear and largely unmistakable language of Barnes will in favor of theories about what Barnes was really really thinking when he wrote it. If the judge is feeling adventurous, it's probably more satisfying to all parties if he sets forth a new legal doctrine, reflecting the inevitable disparity between the cost of displaying fine art to the public, and providing a perpetual endowment to do so.
Harry C. Bishop 1921-2009

|
| Harry C. Bishop |
Harry C. Bishop, M.D., a pediatric surgeon known throughout the medical world, died suddenly of heart failure at his home in Haverford on May 9, 2009, at the age of 88. He was one of the originators of the specialty of pediatric surgery and pioneered many techniques for operating on newborns and very small children.
After graduating from Dartmouth in 1943 and thereafter from the Harvard Medical School and serving as a major in the U.S. Army Medical Corps in Wyoming and Kansas, he completed several surgical residencies. In 1954 he came to Philadelphia from Boston's Children's Hospital to join C. Everett Koop, M.D. at Philadelphia Children's Hospital. Over the years, Dr. Koop and Harry partnered in the development of new techniques to correct potentially fatal abnormalities in newborns. In retrospect, Harry estimated that he had operated on over 9,000 children. He was Professor of Surgery at the University of Pennsylvania and the author of 78 publications. His reputation was worldwide, and he lectured in many countries, being elected to the British Pediatric Society and the German Pediatric Society.
After retirement, Harry joined the Right Angle Club and served on the Board of Control until 2008. He greatly enjoyed the Friday luncheons at the Racquet Club as well as the special holiday events throughout the year at the Union League, the Downtown Club, the Corinthian Yacht Club, and the trip to the battleship New Jersey, among others. Having spent his professional career engrossed in medicine, he particularly appreciated the insights he gained from the varied topics of discussion stimulated by the speakers and subsequently in conversations with fellow members of diverse backgrounds and activities.
Harry was in every sense a family man, devoted to his wife, the former Deborah Dilworth Newbold, and liked nothing better than spending time with his daughter, two sons, brother, and sister, often in boats or ships.
Sailing was one of Harry's greatest pleasures. As long as he was on the water, he was happy to be on all kinds of vessels, yachts or commercial cruise ships. He went on many cruises and was the joint owner of yachts in the Chesapeake and the Caribbean, the Caribbean yacht appropriately christened "Heaven." The cool and calm demeanor that he was known for in the operating room was reflected in his capacity as Captain no matter what the weather, which endeared him to his many friends who served as crew.
A kind and thoughtful man of many interests, Harry was always engaged in one or more continuing "projects," from fashioning boat models to repairing screens at my summer camp in Maine. He was a skilled electrician as well as a plumber, as some of us have gratefully learned in emergencies of sorts at one time or another.
All of us who have had the rewarding pleasure of Harry's company will greatly miss his sense of humor and friendly interest in the companionship of friends in the Right Angle Club.
Dick Palmer
Philadelphia Chromosome
Every Spring for the last 185 years, the Franklin Institute has honored the most distinguished scientists alive; Franklin would certainly be proud of the Institute named after him. In recent years, many awards were combined into two categories, the Bower Awards and the Benjamin Franklin gold medals. Unlike the Nobel Prize, the Franklin Institute Medals are not given for eminence in a designated field of science, but rather are given out by a hard-working committee of scientists who ask themselves What are the really hottest scientific fields at present, and then ask panels of international referees Who is most eminent in that field? The awards thus effectively avoid fields that are temporarily stale and static, by being unrestricted in advance to particular fields. The approach of searching for the greatest minds rather than greatest achievement may well lead to the same award, but the method of choice seems more harmonious with the spirit of Benjamin Franklin, who not only excelled in the field of electricity but actually invented that whole field. The subtle shift in emphasis seems to have been well received; this year's Awards Banquet was over-subscribed before the invitations were printed, and a capacity audience of 800 attended a superb reception, dinner and audio-visualized live ceremony. Actually, the ceremony extends for a whole week, with scientific symposia and in-person meetings with high school students designed to interest them in science.
This year eleven scientists, the most prominent of whom were Bill Gates and Peter Nowell, received the medals. We'll get to Bill Gates in a while; for the present, let's concentrate on Peter Nowell, who invented the Philadelphia Chromosome. What's that?
|
| The Philadelphia Chromosome |
Well, from 1921 to 1955, it was generally held that people, members of the human race, contained 48 chromosomes in every cell in their bodies. The chromosomes were thought to contain the genetic code governing our biological construction, explaining the difference between us and fruit flies, which for example only have four chromosomes per cell. After painstakingly examining the appearance of the chromosomes in different people and in cancer cells, it was then generally held that cancers never seemed to have any genetic abnormality. After all, the chromosomes of cancer cells looked exactly like those in normal tissue: Forty-eight chromosomes, never differing in cancers, so go look somewhere else for the cause of cancer. Unfortunately, the state of scientific development fifty years ago can be summarized by noting that about that time it then became established we really only had 46 chromosomes, not 48. As for cancer, the M.D. pathologist Peter Nowell, then noticed in 1956 that a patient with chronic myelogenous leukemia had an extra translocation on one particular chromosome, giving it a funny shape. This translocation was furthermore present in every single other leukemic cell suggesting that one cell had somehow undergone a single mutant change, and all the rest were its descendants. At least in CML (chronic myelogenous leukemia), it suddenly looked as though the cause had been found since the further study revealed the same was true of just about everyone who had CML. At first, it was felt that while maybe the cause of this particular type of cancer had been found, every other cancer might still be caused by something else. Not so. From believing no cancers were genetic in origin, Peter Nowell started us on the path of now being confident all cancers have a genetic cause.
|
| Dr. Peter Nowell |
How could we all have been so wrong; can't scientists even count up to 46? No, as a matter of fact, in 1955 it was pretty hard. If we couldn't even tell how many of them were there, it's obvious the comment they all looked alike wasn't worth very much. As Peter shyly admits, his discovery was a result of being trained as a physician rather than as a life scientist; he knew what leukemia looked like, but at that time he didn't know very much about chromosomes. It happens chromosomes spend most of their lives expanded into tiny filaments too small to examine under the microscope. But as they enter the stage of cell division called metaphase, those filaments shorten and thicken up, becoming a lot easier to examine. As a pathologist, Peter didn't bother to stain his slides in dilute salt solution, but just washed them in tap water. The tap water had caused the cells to swell up and burst; those that happened to be in metaphase dumped their stubby chromosomes out where they could be stained and looked at. Simple. Doesn't everyone wash slides in tap water?
So fifty years ago, the general question of what causes cancer finally narrowed down to the right sort of specific question. Thousands of scientists, spending billions of dollars from the National Institutes of Health, sharpened the focus of their search considerably. It certainly looks as though someone is going to carry the search the final step, pretty soon. However, the fact that fifty years of intensive study still hasn't quite found the answer is an illustration of how fiendishly difficult the search really is. Each year that might have been spent futilely avoiding genetic searches would have added one year more before the answer was finally found. By the way, why is it called the Philadelphia Chromosome? In 1955 it had been decided by the scientific community that every genetic abnormality would be named after the city in which it was discovered. Dr. Peter C. Nowell of the University of Pennsylvania and the late Dr. David Hungerford of the Fox Chase Cancer Center were the joint discoverers, so obviously it was entirely a Philadelphia discovery; at that time it had been made a custom that genetic abnormalities were named after the city where they had been first found.
It would be a mistake to conclude that nothing new has been discovered in half a century of research. It has been established that not only Myelocytic Leukemia but essentially every cancer starts with some genetic abnormality, which triggers the expression of "mini RNA". These abnormalities then apparently express a cancer-producing action by triggering an abnormal factor in the cell signaling system, called tyrosine kinase. Drugs with the effect of paralyzing that enzyme have been found to be curative in 95% of cases of chronic myelogenous leukemia, and some other forms of lymphoma. We're certainly getting closer, step by unexpected step, to the answer. In fact, we may be getting even closer to a point where drug research can jump to seeking cures without precisely defining how the cancer was caused. After all, if cancer is caused by a chain of cellular events, it may not matter where you break the chain. That realization appeared with, first aspirin and then the statin drugs, for treating heart attacks and strokes, even though we are still not completely clear about how atherosclerosis is produced. Meanwhile, the death rate from hardened arteries has dropped by half.
It wouldn't be right to omit mention of Peter Nowell's Quaker heritage. Although he isn't a Quaker, his mother was a Matlack, a direct descendant of Timothy Matlack, the Haddonfield Quaker who was the scribe for the first writing of the Declaration of Independence. Sitting in silent Quaker meeting, polishing and simplifying one's message before delivering it, is very good training for a habit of simple, direct thought. As Dr. Nowell phrases it, he is a chronic "lumper" of ideas, when so many scientists are content to be "splitters". Splitting complexity into its essential components is a useful approach. But somewhere, someone has to get to the heart of the matter.
Kenneth Gordon, MD, Hero of Valley Forge

|
| Valley Forge |
There's no statue of Ken Gordon at Valley Forge National Park, although it would be appropriate. No building is named after him; it's probable he isn't even eligible to be buried there. But there would be no park to visit at Valley Forge without his strenuous exertions.
One day, Ken's seventh-grade daughter came home from school with the news that the father of one of her classmates said that Valley Forge Park was going to be turned into a high-rise development. That's known as hearsay, and lots of things you hear in seventh grade are best ignored. But this happened to be substantially true. At that time, the Park was owned by the Commonwealth of Pennsylvania, and Governor Shapp was finding the upkeep on the Park was an expense he needed to reduce. The historic area had two components, the headquarters area, and the encampment area. One part would become high-rise development and the other would become a Veteran's Administration cemetery. Although any form of rezoning has the familiar sound of politics to it, Dr. Gordon (a child psychiatrist) had the impression that Sharp was mostly interested in reducing state expenses, and had no particular objection to some better use of the historic area. At any rate, when Gordon went to see him, he said that he would agree to a historic park if Gordon could raise the money somehow. The Federal Government seemed a likely place to start.
Well, the sympathetic civil servants at the National Park Service told him how it was going to be. You get the consent of the local Congressman (Dick Schulze) and it will happen. If you don't get his consent, it won't happen. It seemed a simple thing to visit that Congressman, persuade him of the value of the idea, and it would be all done; who could refuse? After the manner of politicians, Schulze never did refuse, but somehow never got around to agreeing, either. It takes a little time to learn the political game, but after a reasonable time, the National Park employees told Gordon he was licked. Too bad, give up.
He didn't give up, he went to see his Senators, at that time Scott and Clark. They instantly thought it was a splendid idea, and instead of going pleasantly limp, they sent Citizen Gordon over to see Senator Johnson of Louisiana, the chairman of a relevant committee. Johnson also thought it was a great idea, and called out, "Get me a bill writer!" A bill writer is usually a government lawyer, tasked with listening to some citizen's idea and translating it into that strange language of laws -- section 8(34), sub-chapter X is hereby changed to, et cetera. Bill writers have to be pretty good at it, or otherwise, they will misunderstand the intent of the original idea, modified by the personal spin of the committee chairman, the comments of the authorizing committee, and later bargains struck in the House-Senate conference committee. Having negotiated all those hurdles, a bill has to be written in such a prescribed manner that it won't be found to have multiple loopholes when it later reaches the courts in a dispute. A good deal of the time of our courts is taken up with making sense of some careless wording by bill writers. That's what is known as the "Intent of Congress", an ingredient that may or may not survive the whole process.

|
| Dick Schulze |
Ken Gordon had to go through this process, including testimony at hearings, for three separate congressional committees. To get everybody's attention, he organized several hundred supporters to write letters and get petitions signed by several thousand voters. These supporters, in turn, influenced the media and started a lot of what is known as buzz. All of this is an awful lot of work, but there is one thing about this case that can make us all proud. Not once did a politician suggest a campaign contribution was essential in this matter.
In time, ownership of the Park did in fact migrate from the Commonwealth to the U.S. Department of the Interior, hence to the National Parks Service. Everyone agrees it has been well managed, and increasing droves of visitors come here every year. It is now clearly a national treasure. Unfortunately, the encampment area got away and has been commercially developed, although not nearly as high-rise as originally contemplated. Along the way, many discouraging words were spoken about the futility of fighting against such odds. The outcome, however, is the embodiment of two slogans, the first by Ronald Reagan. "It's amazing what can be accomplished, if you don't care who gets the credit for it." The other slogan is older, and Quaker. All you need, to accomplish anything, is leadership. And leadership -- is one person.
One day Ken Gordon, the very busy doctor, was asked how much of his time was taken by this effort. His answer was, ten hours a week, every week for five years.
Community Volunteers in Medicine

|
| Comm Volu In Medicine |
Mary Wirshup has a very different medical background from mine, but she's my kind of doctor. I couldn't help wishing, as she addressed our urban luncheon club, there could be thousands more like her, even while understanding more fully than she seems to, the reasons why doctors are driven from her behavior model. As we parted, it felt like saying a last goodbye to the Spartans marching to Thermopylae.
As 46,000 medically uninsured persons in Chester County get sickness and injuries, they know that a Federal Law prohibits a hospital accident room from refusing to see them, so ways are found to shunt patients to the CVIM free clinic, run by volunteers. This law is, in turn, a response to a government-created situation where a hospital which "accepts" patients must keep them. Any economics teacher can tell you that supply/demand issues are best addressed by price adjustment, so price controls in whatever guise lead to shortages. I must say I have little sympathy with the devious strategies which hospitals often employ to disguise their rejection of uninsured patients. At the same time, I know a lifeboat will sink if too many climbs aboard. Nevertheless, the semantic switch from lack of insurance to lack of care implies that only more insurance can surmount the barriers to care, which is absurd. For one thing, I know too many hospital administrators who are paid a million dollars a year, and one who is paid two million. And at least two health insurance executives are in the newspapers with a net worth over a billion -- yes, that's billion with a b. We have reached a point where reducing all physician income to zero would only reduce "healthcare" costs by 10%. As I look at Dr. Wirshup's modest clothing I can only surmise she plans to continue her modest living until she is 80 years old, after which her savings might see her out. Squeezing physician reimbursement is not intended to save significant money, nor intended to restore physician incomes to more equitable levels. It is intended to address the oversupply of physicians without confronting either the universities or the foreign trained lobby.
The elite tranche of medical schools do their part to relieve physician oversupply without reducing class size, through the encouragement of their students to go into research. I was well along at the National Institutes of Health before I finally decided I had not gone into medical school with that goal, and returned to teaching and patient care in a more satisfying model not too different from CVIM's obviously Pennsylvania Dutch spirit. The Amish at the far western end of Chester County reject the whole idea of insurance; their most characteristic statement is "Don't send me no bills." That attitude is rather a contrast with the shiny housing and automobiles in the Silicon Valley developments of Southern Chester County, or even with some rather bewildered Quaker farm families scattered over the rest of the county next to the horsey set. Chester County is America.
On Second Street in Society Hill, next to the park where William Penn's house stood and a few feet from Bookbinders, is the house of Dr. Thomas Bond. Bond conceived the idea of building the first hospital in America and with Franklin's publicity machine succeeded in getting it built, to care for the "sick poor". Dr. Bond started a second enduring tradition as well. When the Legislature expressed doubt that the institution was sustainable, he pledged to convince the local medical profession to serve the poor without charge. Some of the legislators who voted for the measure did so in the belief that charity care would never appear so the gesture would be without cost. The physicians did indeed come forward, in sufficient numbers to run many institutions for two hundred years. In 1965 health insurance made its national appearance and has regarded the benchmark low costs of charity care as a threat, ever since.
Hospital Elevators

|
| Modern, High-Speed Elevator |
Elevators are a problem for any architect in any building, because they are expensive in a number of ways. If the building is no more than four stories high, it can manage to have hydraulic elevators, quite sturdy and comparatively inexpensive, but agonizingly slow. Taller buildings need high-speed electric versions, but the elevator itself is not the most expensive part. More important is that every elevator bores a hole in every floor, more elevators bore more holes, and the usable floor space on each floor is reduced. Further, the mechanical stress is mostly on the doors on each floor, which open and close hundreds of times each day, rather than the lifting engine of the cab. Elevators which seem to be breaking down continually, are mostly in need of new doors. In building a hospital, the architect confers closely with the administrator until the place is built and then the architect leaves. The administrator may leave soon afterward, too, because the hospital personnel who use the new building soon discover that when pennies were pinched, the result was fewer elevators. There's no right answer to this problem; nobody is ever satisfied.
|
| Waiting for the Elevator |
The surgeons long ago learned to cope with the problem by beginning their day before everyone else arrives. If the elevator comes immediately after being summoned and skips all intervening floors to the surgeon's destination, it can save at least a half hour of his time to make rounds at 5 AM. Multiply that imposed delay on hundreds or thousands of hospital employees, and it is possible to conjecture that hospital employees generally only work a 7-hour day, and spend the 8th hour waiting for the elevator. Whatever the actual calculation, it is a cost seldom actually calculated into the equation of constraining the installation of elevators because of cost considerations. Unwelcome crowding is a social cost, too. Bereaved relatives coming down in the elevator must meet students of various disciplines going up the elevator holding coffee cups and chattering. And all ranks and conditions must crowd into the unyielding back of the elevator when the door opens to confront a hospital bed with an afflicted patient aboard, surrounded by a team of attendants in pajamas, holding up bottles and tubes. Attempts are usually made to assign separate elevators for patients and/or equipment, but the attendants soon find out about elevators that save time, flocking to them in spite of signs, threats, administrative letters of admonishment, and dreary staff meetings. It is easy to identify new staff; they are the people who take elevators down. Everyone else learns to go to the top floor and walk down the stairwells. Outta my way!

|
| Harry Gold |
So, hospital elevators evoke recollections. Mine include the many times I rode up beside a sullen teenager named Harry Gold, who was going to the chemistry department of the old Philadelphia General Hospital. If we ever exchanged a word I don't remember it, so I have to regret that I missed out on striking up an acquaintance with a real, convicted Soviet spy, the one who passed hydrogen bomb secrets to those Rosenbergs who went to the electric chair protesting their innocence. Something to tell my grandchildren I guess.
On another occasion, Dr. John Y. Templeton was standing impatiently for an elevator at Jefferson Hospital. John was a brilliant surgeon from Virginia, one of the inventors of the heart-lung machine, and also one of the quickest, most irreverent wits in Medicine. The door of the elevator opened, to reveal a completely crowded crowd of assorted folk, with a Doctor Zimskind standing in the front. Templeton's southern accent boomed out, "Going down?" "Going dow-un?" Lost in thought, Zimskind had trouble finding his voice and simply poked his index finger skyward two or three times. To which, Templeton shouted out, "The same to you, Dr. Zimskind. But are you going dow-un?"
And, much earlier when I was a resident wearing a long white coat, accompanied by a jolly sort named Carroll who wore the same, we got on an elevator which was empty except for a surgical resident wearing his particular uniform of a short white coat covering his green surgical pajamas. We had gossiped earlier about this surgeon, who had returned for training after some harrowing experiences in the Normandy beachhead. He was a mean, silent, sort, but Carroll was an irrepressible joker. "Well," sez Carroll, "I hear you carry a gun around with you. Do you carry it into the operating room?" To this, the surgical resident opened his jacket and, so help me, pulled out a pistol from his belt. "When I was in Germany," he murmured, "I killed lots of better men than you are." Under the circumstances, there was little more to be said, and we stopped breathing just to be sure. Those Jefferson elevators are awfully slow to reach the next floor.
And finally, there was Herman, who ran the hydraulic elevator in the original old building of the Pennsylvania Hospital. Herman the German we called him, although his accent was probably Central European. This elevator was an antique, with a big iron steering wheel that Herman turned to release the oil or water or whatever pumped the excruciatingly slow cage up two floors. There, for our contemplation, was America's first building of the first hospital, with the first operating room on the top floor. For more than a century, orderlies had to carry stretchers up and down the stairs with the apprehensive surgical patients, and then this marvel of a hydraulic thing was installed to great admiration. It has long been replaced with a fancy new self-service elevator. But so have the patients been replaced; one hundred sixty patient beds entirely replaced by administrators.
Atlantic City, Brigantine and the N.I.H.

|
| Dr. William Osler |
It would only be honest to say that Atlantic City was a rundown mess after World War II, cheap, sleasey and dispirited. But for academic medicine during a period of thirty or forty years, one small nook of A.C. was the most exciting place in the whole world. Only during several days at the beginning of May, however. The reason it was so attractive to scientists was that beach hotels were cheap and dilapidated; Atlantic City probably contained the worst on the East Coast. The Haddon Hall was an exception, rather elegant and far too expensive for most physicians in training; research is a young doctor's game. The medical profession's annual beauty contest for medical research was headquartered in Haddon Hall next door to the Steel Pier, surrounded by hundreds of cheap lesser hotels. The professors all stayed at Haddon Hall, but few others could afford it. Indeed, resident physicians from Philadelphia mostly found it cheaper to commute from home for ninety minutes than to stay overnight, residents and fellows from more distant cities stayed in the dumpy hotels. Nobody in that age group had much money to spend, so the commuting Philadelphians didn't miss out on much nightlife at the shore by going home every night.

|
| New Atlantic City Skyline |
Before the spring meetings got popular after World War II, a hundred members of the most elite society of academic research professors on the East Coast assembled in Haddon Hall, all of them quite able to afford to stay in the headquarters hotel. This had been going on since William Osler founded it in 1885, at first in Washington, and then migrating to Atlantic City. As medical research began to flourish, the society grew a little, but at a pace too slow to keep up with the growth of medical scientists, so a second group of "Young Turks" formed a competitive society which met the next day, and ultimately a third group, the "Young Squirts", felt excluded by the old has-beens, and met on the third day of what eventually turned into a week-long parade of scientific presentations, each ten or twelve minutes long, starting before normal breakfast time, lasting until 10 PM, with occasional breaks. That is to say, the medical papers that everybody wanted to hear grew from thirty or forty a year to nearly a thousand. If a young fellow did well, the older professors would notice, and he would get employment offers. That kept the eminent older doctors around for the whole session and provided an informal ranking of the worth of the program. Everybody wanted to advance up the ranks of prestige, and this system roughly sorted them out. However, it was an exhausting experience just to sit through all that and listen; the old professors tended to drop out and go home a little early. No matter how many outstanding papers were clamoring to be heard, no one could endure more than a week of straining for attention. It was strictly forbidden to present a paper which had been published or presented anywhere else, so it was usually difficult to guess in advance whether a paper was likely to be exciting. You could go home early if you wanted to, but at the risk of missing the real blockbuster of the year, tucked away on the program with a bewildering scientific title. The younger wise-apples had a formula, that if one paper in three was outstanding, you were having a good meeting; you just had to grit your teeth and try to stay awake during the other two-thirds. Still, that got to mean that the reward for pursuing this grinding ordeal was to go home after learning about three hundred outstanding scientific advances that no one else knew about; knowing three hundred cutting-edge things that other doctors didn't know really did put you well ahead of the pack. Keep that up for ten or twenty years, and notable differences among colleagues would relentlessly emerge.
|
| Old Steel Pier |
From the lounge of the Haddon Hall, with non-members forced to stand in the back, the meeting moved to the 2000-seat movie theater in the Steel Pier, at about 1950. Things then came to equilibrium; the movie theater was never completely full. We were told there were seven or eight even larger auditoriums on the Steel Pier, but it was never necessary to move to them. The first four years I attended these sessions I was being paid no salary at all, and most of my contemporaries were only getting token amounts beyond room and board. The eminent professors who were real members of the top society would find their way to front-row seats where they could ask questions, having had a chat with colleagues at breakfast in the Haddon Hall. But they had once been impecunious, too, and wore their brand-new Ivy League plaid jackets rather uncomfortably. Doctors who (gasp) worked for drug companies also gave signs of affluence, but they tended to drift over to the barber shop and have a shoeshine, where they picked up the gossip for their employers. Over a period of fifty years, I can recall first hearing of the wonders of several new antibiotics, a strange chemical called cortisone which seemed to cure rheumatoid arthritis, the introduction of the birth-control pill, the introduction of polio vaccine, the first drugs in the treatment of tuberculosis, and a vast array of novel explanations for disease phenomena that had seemed mysterious for centuries. In those days, a year without a new medical miracle was a very lean year, indeed. During this interval, the basis for curing at least thirty common diseases was first presented at the Spring Meetings in A.C., and since then medical practice looks nothing like it did in 1947.
Gradually the audience changed, too. At first, the people presenting papers came from at most ten medical schools, and mutterings of discrimination could be heard. In fact, it was plainly true, because only about ten schools had any extra money to fund research. When this news reached the U.S. Senators from the Mid and Far West, federal research money started to be spread around more evenly, just like the distribution of Senators. It was the appointment of one of the members of the original small nest of clubs to the Directorship of the N.I.H., the National Institutes of Health in Bethesda, Maryland, which really got the research spigot to flow. The point man was James Shannon, who knew what was what in cutting-edge research, and he sat there in the audience making up his mind who was who. For all the time of his directorship and for long afterward, he enforced, really enforced, the rule of "no political influence in research grants". Lots of congressmen came to the N.I.H. with the news that their relatives had such-and-such a disease, and so they thought more money should be diverted to research in that area. Nothing doing. Shannon held the keys to the kingdom, and he knew it. He had a deft feel for how much money the research industry could usefully absorb, and then he went to Congress and demanded it. The purity of this process has frayed at the edges somewhat as the amounts of money grew to what is now thirty billions of dollars a year. Most experiments, unfortunately, fumble or fail, so a lot of money gets spent on blind alleys before someone gets it right. It takes a tough-as-nails idealist like Jim Shannon to survive the temptations of an N.I.H. Director, and among the temptations is just to give up and give out money indiscriminately to people who want to count all the grains of sand on the beach. If your idea was a good one, you got all the money you could possibly spend; if the idea was mediocre, in those days you got nothing at all. On the other hand, the estimation of overhead costs is something other mortals can quibble about. Shannon demanded and got about a third of the grant money to be given to the medical school administrations. That was barely enough in a research establishment emerging from the Depression of the 30s, and the World War. However, now that the pipeline is filled, it is increasingly doubtful that ten billion a year needs to go to administrators; the bean-counters took over, and the results are more open to criticism. After all, after someone finds a cheap cure for cancer, some disadvantages of perpetuating an aging retiree population start to emerge and may outweigh the arguments for spending quite so much doing it. That may well be what the advisors to President Obama are growling at, but for now, the example of his nose poked into the hornet's nest of favoring research for certain population (voter?) groups will restrain others who were once inclined to agree. After cancer is cured, perhaps then everything will seem different.
|
| Dr. James Augustine Shannon |
Well, let's tell one story out of many that could be told. Around 1965 there were two competitive polio vaccines rumored to be in the pipeline. Jonas Salk had an injection method, and Albert Sabin had an oral vaccine. Anyone who had watched children run shrieking from a needle knew that Sabin had the preferred method, but Salk got to Atlantic City two years earlier than Sabin. The auditorium was filled with rumors of very dubious precision to the effect that Salk had used unfair methods to get to the stage of public announcement. For example, it was growled he gave the vaccine to the Russians to test, but they were afraid of it and gave it to the Poles. Regardless of such scurrilous gossip, which is here repeated only to show how hysteria can occasionally agitate even scientists when Salk gave his paper at the Steel Pier, the standing ovation was thunderous. And so, as the meeting broke for dinner the crowds migrated over to a huge seafood restaurant named Hackney's and watched the new scientific hero get a little tipsy in public. That seemed to revive the rumors which became even less factual. But there is no doubt that by the time Sabin stood at the same podium and gave his presentation of the oral vaccine, the crowd had switched to his side, the ovations were unlike anything the scientists had ever heard. Anyway, as emotions now settle down in retrospection, we are all pretty happy that polio is nearly eradicated from all but a few corners of the earth, and these two men are both responsible for it. But so is Jim Shannon responsible for it, and he never got the ovations he deserved.
|
| Mr. Peanut |
When the gambling casinos came to A.C. the cheap boarding houses were swept away, doctors in the research were incidentally better paid, and the Spring Meetings migrated back to Washington. The dumps on the beach have been replaced by gleaming multistory hotels, the place looks much more prosperous. Doctors are in a position to know about the drug and alcohol addiction, the venereal disease and crime among the casino employees, and the personal tragedies among the gamblers. But anybody can see the new buildings and clean streets. When a group of eight of us took a nostalgic trip to revisit the place, no doctor even mentioned the idea of going in to drink and gamble -- even the suggestion was preposterous. So we wandered over to Brigantine where there appears to be a large retirement community, where gambling and drinking seem equally unlikely. The elementary school in which we heard a talk about the old days was splendid beyond anything I remember in an elementary school. Among the audience, the questions revealed there were many former employees of the old A.C., people who ran shops to sell salt water taffy, fudge and the like to crowds on the boardwalk. Some of them may have once driven Jitney buses or pushed sightseeing wheelchairs. But not one of them showed the slightest sign of recognizing that on the first weekend in May, every year, a crowd of nerdy-looking serious fellows would move into familiar boarding houses for a few days, remaining mostly invisible during daylight hours. That was the academic doctor crowd if anyone had bothered to ask, pouring into the Steel Pier movie theater, having the time of their lives listening to medical history being made. After a week they all went home, and nobody in A.C., later Brigantine, paid any attention to any of it. After all, A.C. is about salt water taffy, right?
Avian Footnote
Waldo E. Nelson was a much revered professor of Pediatrics at Temple University School of Medicine for several decades. He was the original source of fame for St. Christopher's Hospital for Children, a powerful and revered teacher, and has recently been mentioned as the "Father of Pediatrics." He died in 1997 at the age of 98.

|
| Saint Christopher Hospital |
Everyone admitted he was a demanding task-master, to the point of eccentricity. That's a quality almost essential in any editor of a multi-author textbook because authors regularly procrastinate in submitting their contributions, while publishers have rigid deadlines and no patience at all with editors who ask to extend them. The central element in Nelson's fame was his 1600-page textbook of Pediatrics, with more authors than it is reasonable to count in the decades it was published and re-published, eventually establishing itself as the standard work in the field. Nelson applied discipline to his resident physicians, too. One former resident recently recalled his forbidding a husband and wife resident pair to eat lunch together in the hospital cafeteria. Not in my hospital, you won't.
What his family life was like is not reported, but it can easily be imagined that he had rebellious children. One day he instructed his daughter to prepare a complete index of the textbook for the next edition. Apparently there was some resistance, eventually quashed. And to emphasize how unlikely it was that anyone would read an index very carefully, the book went through editing and proof-reading, and was in the bookstores for several months before anyone noticed the entry tucked away under "Birds".
BIRDS, For the. page 1-1650.
House that Love Built: Ronald McDonald of Philadelphia
Kim Hill had the misfortune to develop leukemia, but the great luck to have Fred Hill of the Philadelphia Eagles football team for a father. Driven by gratitude for the treatment at St. Christopher's Hospital for Children

|
| Audrey Evans |
Fred demanded to be told what he could do and was referred to Dr. Audrey Evans. This world-famous pediatric oncologist was well known for her philanthropic activities and had frequently expressed the need for a temporary residence for families of children needing protracted medical treatments. Young children have young parents, whose savings are soon exhausted by travel, hotel and other non-insured costs related to a seriously sick child. The Hills had just been through such an experience and grasped the problem immediately, adding to it the discomfort and loneliness of families in such a situation. Fred Hill quickly enlisted the enthusiastic support of the whole professional football organization, and Jim Murray the Eagles' general manager recruited Don Tuckerman from their advertising agency, who got to Ed Rensi, the regional manager of McDonald's. Together, they got the project financed and started with a seven-bed facility near Children's Hospital of Philadelphia.

|
| Fred Hall |
In 25 years, the Philadelphia Ronald McDonald House has grown to a capacity of 44 families, in a century-old mansion at 39th and Chestnut Streets filled with Mercer tiles and the like. The operation uses eighteen volunteers at all times, runs two jitney buses, and is one huge teeming family home for people confronting a common issue, supporting each other through a wrenching emotional experience. Although it actually costs about $65 a day per family, the charge is $15 and over half of the clients cannot afford even that. Although an effort is made to have family cooking, the McDonald's restaurant chain supplies 20% of the budget along with generous help with exigencies and in-kind assistance with such things as clowns for the entertainment program, birthdays and the like. Although McDonalds's is probably the world's premier franchising corporation, every one of the 300 worldwide Ronald McDonald Houses is an independent local organization, run without a central headquarters or any sort of standards-setting and the like. Every one of the other 299 Houses got the idea from Philadelphia but proceeds in its own way. Philadelphia created it, but Philadelphia does not own the idea.
In this connection, it is probably worth reflecting on the history of this topic. When Benjamin Franklin and Dr. Thomas Bond started the Pennsylvania Hospital in 1751 at Eighth and Spruce Streets, it was the custom to be diagnosed, treated, be born and to die in your own house. The unique perception behind the nation's first hospital was that poor people generally did not have home facilities that were adequate to support home care. In Franklin's own handwriting the purpose of the Pennsylvania Hospital was stated to be "for the sick poor, and if there is room, for those who can pay." It was understood that poor sick people needed a place to take care of them, not merely for their surgery and overwhelming illness,
<but for convalescence and rehabilitation as well. Two centuries later, in the first thrill of founding the Medicare and Medicaid programs, it was imagined that things would remain exactly the same, only paid for by the Government. But after four or five years, it became abundantly clear that it was far too expensive to use hospitals in that way. The very act of federally paying for the program undermined its volunteer spirit, raised its mandated standards, and made it financially unsustainable. And so, although the 1965 Amendments to the Social Security Act insisted, and still pretend, that no change was to be made to the delivery of care, the delivery of care simply had to be changed. Not only was domiciliary and custodial care to be excluded, but heroic efforts were to be made to reduce the length of stay in the hospital to what would once have been regarded as special intensive care. In effect, if a type of service could normally be handled at home by non-indigent people, it was to be prohibited for everybody. Since the cost of care in hospital has continued to escalate far in excess of the cost of living, it seems unlikely we will ever go back to the days of rest and in-hospital recuperation.
So, just as Dr. Bond recognized the problem and went to Ben Franklin to handle the philanthropy, Dr. Evans had the idea and Fred Hill made it work. Around the Ronald McDonald house, the idea is frequently heard expressed that every hospital needs such a place nearby, for people of all ages. Perhaps that is workable, but it offhand seems more likely that Retirement Villages, so-called CCRC, will be called on to supply this badly needed service, at least for senior citizens. And that what we now call hospitals will evolve into the scientific "focused factories" so popular in the minds at the Harvard Business School.
Contemporary Germantown
The Strittmatter Award is the most prestigious honor given by the Philadelphia County Medical Society and is named after a famous and revered physician who was President of the society in the 1920s. There is usually a dinner given before the award ceremony, where all of the prior recipients of the award show up to welcome to this year's new honoree.

|
| Bockus |
This is the reason that Henry Bockus and Jonathan Rhoads were sitting at the same table, some time around 1975. Bockus had written a famous multi-volume textbook of gastroenterology which had an unusually long run because it was published before World War II and had no competition during the War or for several years afterward; to a generation of physicians, his name was almost synonymous with gastroenterology. In addition, he was a gifted speaker, quite capable of keeping an audience on the edge of their chairs, even though after the speech it might be difficult to recall just what he had said. On this particular evening, the silver-haired oracle might have been just a wee bit tipsy.
Jonathan Rhoads had likewise written a textbook, about Surgery, and had similarly been president of dozens of national and international surgical societies. He devised a technique of feeding patients intravenously which has been the standard for many decades, and in his spare time had been a member of the Philadelphia School Board, a dominant trustee of Bryn Mawr and Haverford Colleges, and the provost of the University of Pennsylvania. Not the medical school, the whole university, and is said to have been one of the best provosts of the University of Pennsylvania ever had. When he was President of the American Philosophical Society, he engineered its endowment from three million to ten times that amount. For all these accomplishments, he was a man of few words, unusual courtesy -- and a huge appetite in keeping with his rather huge farmboy physical stature. On the evening in question, he was busy shoveling food.
"Hey, Rhoads, wherrseriland?". Jonathan's eyes rose to the questioner, but he kept his head bowed over his plate.
"HeyRhoads, Westland?" The surgeon put down his fork and asked, "What are you talking about?"
"Well," said Bockus, "Every famous surgeon I know, has a house on an island, somewhere. Where's your island?
"Germantown," replied Rhoads, and returned attention to his dinner.
Furniture for the Horse Country

|
| Douglas Mooberry |
Low-end furniture for America is now mostly made in China, and seldom made of wood. Truly American cabinet making tends to be high-end, and high priced. That tendency goes to some sort of extreme around Unionville in Chester County, where a 25-year old company named Kinloch Woodworking holds pride of place. The owner, D. Douglas Mooberry, picked the name Kinloch at random from a map of Scotland, but his selection of southern Chester County was not an accident. The influence of nearby Winterthur has infused that whole region with an interest in fine furniture craftsmanship, and museums like the Chester County Museum and others throughout the nearby Pennsylvania Dutch country provide an ample source of authentic pieces to serve as examples. There's one other factor at work. As Doug Mooberry quickly noticed, people with money usually have lots of it. There really is a market for $28,000 tall case clocks, $18,000 highboys, and $12,000 tables -- if you can convince people in Chester County you are really good.
Although this 12-person company repairs antique pieces, it does not make exact reproductions. It produces new pieces in the old style of the region, based on careful analysis and evaluation of museum pieces from earlier times. Kinloch once aspired to equal the quality of the early artisans, but now aspires to surpass them in quality of materials and workmanship. The more conventional stance of fine artists is to attempt to excel in today's current style, whatever that may be, probably "post-modern". Kinloch artists, however, choose to excel in the style of a long-past era, taking care not to claim the product is antique. Artisans grow up in cooperative clusters; there's a world-famous veneer company nearby and a pretty good hardware company, although the best craftsmen of furniture hardware are still found in England.

|
| Chippendale Table |
The characteristic style of Chester County furniture in the Eighteenth Century was a mixture of two neighboring cultures, Queen Anne, Chippendale, ball and claw Georgian style of Philadelphia; and the "line and berry" inlay style of the Pennsylvania Germans. If carefully executed, this hybrid style can be very pleasing, and you had better believe it requires painstaking craftsmanship. Others will have to explain the significance or symbolism of intersecting hemi-circles in the lines, and the inlaid wood hemispheres, the berries, at the end of the lines. But the technical difficulty of laying strips of 1/16 inch wood in curved grooves only a thousandth of an inch wider, or the matching of 3/8th-inch wood hemispheres into hemispheric holes gouged out of the main piece -- making the surfaces of the inlays perfectly smooth -- is immediately obvious to anyone who ever tried to whittle. Ultimately, however, true artistry lies in combining two unrelated styles without producing an aesthetic clash. By the way, you would be wise to wax such furniture once a year.
The factory is on Buck and Doe Run Road, and here's another culture clash. At one time, Lammot du Pont cobbled a 9000-acre estate out of several little country villages. In 1945 it was sold to the Kleberg family of Texas, the owners of the King Ranch. Robert Kleberg was an admiring friend of Sam Rayburn but treated the oafish Lyndon Johnson as his personal political gofer. From 1945 to 1984 Buck and Doe was used as one of several remote feedlots for Texas Longhorns bred to Guernseys, the so-called Santa Gertrudis breed. Originally, Texas cattle were seasonally driven to Montana for fattening, then on to railheads for the stockyards. As farmers began to build fences interfering with the long drive over the prairies, it became cheaper to fatten cattle closer to the markets. So satellite feedlots like Buck and Doe Run were developed. You can pack more cattle in a rail car when they are younger and smaller, and advantage can be taken of price swings by suppliers who are close to the market. In this case, the markets were in Baltimore. Since the King Ranch is larger than the state of Rhode Island, such 9000-acre farms were pretty small operations in the view of the Texas Klebergs, an opinion they did not trouble to conceal from the irritated local gentry. The point was even driven home in high society circles by holding large parties at Buck and Doe Run, allowing guests to wander around the roads, unable to find the house of their host even though they had been on his property for most of an hour. In 1984 the Buck and Doe was sold to Art DeLeo, who is busily converting it into a nature conservancy.
Baruch Blumberg, Renaissance Man
|
|
| College of Physicians |
Baruch Blumberg may be an octogenarian, but he radiates vigor and good health; his current intellectual interests are invariably on the cutting edge. He currently serves as the president of the American Philosophical Society, was for five years the Master of Balliol College at Oxford, was the Director of Astrobiology at NASA -- all of them after he had won the Nobel Prize in Medicine, and retired from his laboratory. He likes to run and bicycle, with a long history of disconcerting the populace of China, India, and Africa with early morning forays. His undergraduate major was physics, with graduate work in mathematics. He went to medical school at his father's suggestion.
|
| Hepatitis B |
The Nobel Prize was awarded for the discovery of the Hepatitis B virus, for which he developed a highly successful vaccine. It has been estimated that there are 375 million people in the world infected with this virus, and it leads in time to liver cancer, the most common form of cancer in Asia. If you set about to stamp out disease and save lives, it's advantageous to do it with an extremely prevalent disease. And then there are some surprising side-benefits. For some reason, women who are infected with Hepatitis B produce a disproportionately large number of male offspring, so that vast immunization programs in Asia are now starting to result in a larger proportion of females in the population. The lack of female children in Asian families has long been attributed to selective abortion, so it's satisfying to see an abatement of that particular slander.

|
| Baruch Blumberg |
Blumberg has twice been invited to deliver a lecture to the College of Physicians of Philadelphia. The first was a description of the problems of space travel. The second was a discussion of current trends in medical genetics. It seems that gene mutations only occasionally cause disease directly. The much more important genetic factor in disease affects the ability of some people to resist particular diseases and makes others more likely to be a victim. Hepatitis B? Well, that's so yesterday.
Nobel Prize: Michael Brown, MD

|
| Michael Brown |
The College of Physicians of Philadelphia annually sponsors a lecture by a winner of the Nobel Prize in Medicine or Physiology. There is never any doubt of the high quality of any such lecture, but it does add an element of local pride whenever the Nobel Laureate comes from Philadelphia, as he did this year. Michael S. Brown, MD graduated from Cheltenham high school in 1958, received a B.A. from the University of Pennsylvania in 1962, and his M.D. degree in 1966. Nineteen years later, he was awarded the Nobel Prize in Medicine for his work in describing the cholesterol pathways, and the human defects in it which lead to heart attacks, strokes and other consequences of atherosclerosis. Almost immediately, Japanese investigators found the so-called stain drugs being produced by relatives of the penicillin mold for no, particularly obvious purpose. The patents have not yet expired on most of these drugs, but many millions of people have already been spared death or disability from hardening of the arteries, the commonest killer in modern life.
The speaker, now a gastroenterologist practicing in Texas, chose to organize his talk around the manner in which biochemical discoveries are currently being made. Physicians in medical research endure news media presentations, usually in silence, of scientific research performed by basic scientists with Ph.D. degrees, with MDs then merely dispensing the drugs. It sometimes happens that way, but in general, the basic scientist is too highly focused on the techniques of the scientific cutting edge to be well positioned to see the direction that should be taken next. The physician-scientist, on the other hand, is aching to find a solution to current problems, but often lacks the necessary technical skills to perform the experiment. James Shannon, one of the early directors of the National Institutes of Health, recognized this mutual deficiency was impairing progress and set about establishing training programs for cross-fertilization between the scientific approaches. Dr. Brown was one of the early trainees of that program, and now describes its glories, going from the patient bedside to the scientific laboratory bench, and then back to the bedside to test the results. Competition has morphed into collaboration.
Some day, someone will conduct a study of Nobel Laureates, seeking out the traits which characterize them. The next step after that would probably be cloning them, although public opinion will first have to catch up with that thought. From an observers point of view, Nobel prize winners all seem gifted with the ability to give a logical, entertaining and succinct description of a complicated matter. Almost all of them are located in very large research environments, where news of small scientific discoveries in obscure scientific journals is quickly picked up by a hundred eyeballs, filtered for the benefit of the local enthusiast of the topic, and often fitted together with something which that enthusiast has discovered but not published, or published too recently to be well known. Research is not just expert marksmanship, it is marksmanship within a boiling cauldron of undigested facts. One other thing about Nobel Laureates: as a group, they tend to drive over the speed limit, even when going to the local supermarket.
Anyway, it's really nice to take the statin drug and watch your cholesterol go down, secure in the knowledge that invisibly your longevity is improved. There's just nothing more attractive than having more longevity. At least, it's hard to imagine what would ever replace it in attractiveness.
National Business Coalition on Health

|
| NCOH |
In 1992 the National Business Coalition for Health was just forming at a convention in Chicago. Before I really understood what it was all about, I agreed to their flattering invitation to be the keynote speaker at the kick-off luncheon. Who suggested my name was and is a mystery to me, and I arrived in Chicago with very little idea what they wanted to hear. However, it followed the familiar pattern of inviting the speakers to stay overnight at the hotel on the evening before the meeting began and to meet for drinks at the bar with the organizing leaders. I had enough experience with public speaking to know I could learn the general slant of the thing at such an informal party and adjust the speech to the audience to whatever degree seemed needed. Among the people scattered around at tables was Harry Schwartz, who was also there to give them a speech. Harry had been on the editorial board of the New York Times for many years and was known to be generally quite favorable to physicians. We had both written books about medical care, The Hospital That Ate Chicago in my case, and The Case for American Medicine, in his. We liked each other immediately and fell into an animated cocktail conversation that would eventually be renewed every six months at the American Medical Association House of Delegates meetings, where I was a delegate and he covered the topic for various news media. As we chuckled together about one anecdote or another of medical politics, the bar gradually emptied out. It soon became clear that all the other cronies had wandered off to dinner together, so we ordered dinner on the house, neither one of us have learned just what we were there to talk about. It really didn't bother either one of us very much, since from long experience we could tell some jokes and make it up as we went along. I knew what I wanted to tell businessmen, so it was just a matter of finding a way to lead into it.
The speech seemed to go well. There were several hundred, perhaps even a thousand in attendance, quite convivial and prosperous. As executives usually do, they looked younger than you might expect from the titles on their name tags; they laughed at the appropriate points and applauded at the end. In other words, I went home from Chicago with no more idea what this organization was up to than I had before I came. At the very least, it is clear they were forming a national organization of businesses, with constituent representatives largely drawn from Departments of Human Resources. They wanted to speak for American Business with a more or less unified voice, and the topic seemed to be health care. Although fate had put me into the debate at the very earliest moment at Wills Eye Hospital, this convocation of extroverted Republicans seemed to know a lot more than I did about what was secretly afoot among the Democrats in Washington.
This Chicago tea party did one other thing for me. Many months later, when the editors of USAToday were in search of an editorial page writer who was both a physician and opposed to the Clinton Health Proposal, they called Harry Schwartz. And he suggested to me. They ultimately ended up with a Medical Editorial Advisory Board of five members, at least three of whom were far to the left of me. At the New York Times, of course, Harry Schwartz was considerably more outnumbered than I was. After it was over, Harry and I used to joke that both sides were fairly evenly matched.
Picking Up the Usual Suspects
The federal government directly controls about half of health care spending and makes rules affecting most of the rest.

|
| Claude Rain |
Every group or business which receives some of this money is alert not to lose it. Many other groups are alert for openings to get more of it. All employ sentries in Washington. False alarms are frequent, stealth attacks are a constant threat, constituents paying the bills demand immediate reassurances. Members of Congress seldom initiate a disturbance unless someone from inside an industry brings it to them. Consequently, when proposals do surface and seem to be serious, the question to be immediately answered is -- who's behind this? If you know who starts something, you can readily imagine the motive, assess the political strength, decide how to respond. With what little was generally known about the Clinton Health Care Plan of 1993, it was easy to imagine a host of people with some motive, but very hard to say who was actually pushing one. Must be a Democrat, obviously, but not immediately obvious which of several possibilities was the real agitator.
Health insurance companies would always seem likely to have proposals about national health insurance. Blue Cross dominates the market in large geographical markets, mainly East Coast, and would seem fearful to lose that dominance in a major upheaval. But other market areas of the country are dominated by commercial insurance companies who might seek to upend the Blue Cross monopoly, but whose form of business would be even more seriously threatened by health insurance innovations. Most commercial health insurance was written by large life insurance companies who regard health insurance as a small sideline for the convenience of their industrial customers. Blue Cross was somewhat more comfortable with government work, particularly since the 1965 Medicare and Medicaid programs were patterned after them. However, Blue Cross was non-profit, thus lacking in incentives, and historically controlled by health care providers. That is, Blue Cross was formed by and dominated by the hospital associations, and Blue Shield was formed by and dominated by medical societies. Since doctors and hospitals were very prompt in announcing their deep concerns and uncertainties about the Clinton Plan, Blue Organizations seemed unlikely to make daring proposals so likely to provoke trouble at home.
Not that some doctors and some hospitals didn't try to see what might be made of this opportunity. At the American Medical Association, certain leaders known to have Blue Shield involvement offered conciliatory remarks about waiting for further details before taking a stance but were abruptly halted by a general opinion that things had apparently already gone too far for substantive negotiation. Much the same thing occurred at the Hospital Association; the winners had too much to lose, the losers had too little influence to matter, and nobody stepped up to claim an inside track. Hospital trustees didn't know what was going on, strongly suspected something was going on and didn't like either situation. If the doctors got mad enough at a hospital, they could ruin it, and if hospitals got mad enough at Blue Cross, it too was ruined. The main strength behind the Blue Cross monopoly position was the secret discount provided to them by hospitals, which was refused to competitor insurance companies but could easily be extended in the interest of fairness. If need be. The commercial competitors wanted that discount much more than they wanted new insurance models.
There is one subset of doctors and hospitals that might be suspected of generating a sweeping revision of the medical system -- academia. Medical schools think of themselves as the appropriate source of vision about the profession they are training, and they run large prestigious hospitals. Their heavy dependence on government research grants, teaching subsidies, and tuition support programs puts them in constant contact with Washington bureaucracy and politics; propinquity is a great match-maker. Their style of salaried faculty creates estrangement from making a living by being paid fees for specified services, and they are reasonably comfortable with the flaws and techniques of professional promotion within a large organization. So, a slogan which has been attributed to Wilbur Cohen himself does not greatly jar on their ears. The author of the Medicare Act is said to have announced that the entire medical system of America could be accommodated by thirty or forty Mayo Clinics. Twist that just a little, and you are imagining he said forty or fifty medical school teaching hospitals. The briefest contemplation and rebuttal will knock down that proposal, such as pointing out that we have several times that many teaching hospitals at present without achieving anything like the nation-wide coverage envisioned. After absorbing the administrative chaos of readjusting to that model, you would confront the old repeated history of grossly overestimating, and then grossly underestimating, the future manpower needs of a medical system in the process of constant scientific turmoil. Suppose you built the fifty Mayo Clinics and found you needed two hundred? Suppose you built two hundred and found you needed seventy? And then, finally, remember that each big city could expect to contain one of these organizations, but the fewer of them there are, the longer the distance everyone else would have to travel to get to them. No one has even ventured to speculate how you could go about doing such a thing, let alone doing it three or four times to get it right. But, but. The infeasibility of academia at the center of medical care delivery does not eliminate the possibility that the idea underlying the Clinton Health Plan may have originated in academia, or that academia might support some similar proposal with something else at its center.
Since it was soon clear that the traditional "players" in the health policy arena were unlikely to be sponsoring some self-serving policy that might masquerade as the Clinton Health Plan, the search went on. There were a number of professional groups within the medical community who had traditionally chafed at the domination of the hierarchy by physician leadership. Nurses, hospital administrators, pharmaceutical companies, druggists, corporate human resources officers, public health officials, social workers, biology teachers all represented groups who derived status with the public by displaying inside knowledge of medicine. But all of them fell silent when a physician entered the room, and tended to shift their emphasis to faults of the "system" or the "industry". Their Washington representatives placed their emphasis on changes in the existing system which might elevate the prestige and income of the members and were particularly vigilant for system modifications intended for other purposes which might nevertheless create advantageous loopholes for the members. All of this is normal striving in the good ole' American way, a polite variant of the mixture of bellicosity and restraint usually seen in the Union movement. These people wanted to improve their income and working conditions but were ultimately quite hesitant about radical proposals that might sink the ship. A quick survey showed they were not supporting any particular reform project, even though they could be counted on to support any reform project. Furthermore, they consistently injured their political strength by extending beyond economic goals to issues like radical feminism in the case of nurses, or direct advertising to the public as in the case of the drug companies, or practicing medicine without a license in the case of limited-license practitioners. These people had votes, influence, and lobbyists, but they did not have a national project for health care reform of their own devising, and they surely were not the people behind the Clinton Plan.
During the six months before The Plan was presented to Congress and the Public, a White House task force said to consist of five hundred secret members was meeting under the direction of President Clinton's wife Hillary. No doubt part of their purpose was to give Hillary a public platform on which to show her stuff, with the idea of someday succeeding her husband as President sort of in the back of her mind. But most of it was also quite practical; somebody had to figure out what this proposal was going to be, and newly elected Bill had to spend most of his time learning how to run the rest of the country. Buried in here was an efficiency principle too; the staff members of every important congressman and senator were involved in the process, making the deals and surfacing the political angles before things had to come down to votes and filibusters. Meanwhile, the rest of the country had to wait outside closed doors, fed by rumors and spin.
How well I remember one public seminar on the subject during this period of suspense. The audience was filled with people thought to be influential with the public, the usual suspects in that sense, too. Representatives of various interest groups were seated up front at a table, and for some reason, I had been picked to represent doctors. Next to me was a druggist who had made a billion dollars starting an HMO; it was intriguing to watch how many well-dressed women with no interest in health care paraded up to the table to show their stuff to the billionaire, while we waited for the meeting to begin. All of the usual suspects of Philadelphia medical care were at the table, each of us wondering what the other was going to say. When some last Very Important Person had wandered in and taken a seat, it was time to begin. The moderator told a funny story or two, and then asked each one of us what we thought of the Clinton Health Plan. One by one, to the utter amazement of us all, we each explained how we were opposed to it.
So obviously this proposal was not coming from the usual agitators. But, remember, somebody was surely behind it. Before we take a stab at that mystery, let's humanize the usual suspects by describing a few of them.
Hold the Presses

|
| Stop the Presses |
At USAToday, techniques are astounding. After getting an 800-word piece, an editor by phone will suggest cuts to 300 words; the piece is always improved. Last-minute speed, trying to watch television, is unbelievable. On one occasion, after a medical meeting in Kansas City, watching a baseball game go into extra innings I fell asleep with the game undecided. The next morning a newspaper was pushed under my door. It was USAToday, not only carrying the final score but a full story, under a color photo of the winning play. Just consider the precision Chicago reporting, Washington DC editing, Kansas City printing and local delivery that took place in seven hours. By contrast in book publishing, a full year often intervenes between manuscript submission and actual bookstore sales.
So on a certain Monday night, the editor called. The Senate Majority Leader, George Mitchell, finally was to unveil the Clinton Health Proposal tomorrow morning. Would I please submit an editorial to run in the morning paper; he would supply the title. It was to be called, What Should Congress Do Now? and the deadline was 7 PM tonight. My watch read 5:30 PM.
Well, what fun. After a few minutes of stumbling around, I resolved to build the editorial around the theme, Don't Make Things Worse. It then seemed natural to allude to similar proposals gone famously wrong, define some predictable traps, and end up with Hippocrates. Over and over it is thundered at medical students: Primum non nocere. First do no harm. It all came together in my head, and I sat at the typewriter to bang it out. But when I came to that last sentence, pleading at least do no harm, I was hit by terrible doubt.
That phrase comes to us in Latin, and Hippocrates was a Greek, living at least five hundred years before the Roman Empire. Famous though the saying is, it wasn't (then) in Bartlett's Quotations, or Roget's Thesaurus, or anything else I could lay my hands on in what was, after all, a medical office. It was 6:50 PM. I called a learned friend from his dinner-table, and he agreed it was a strange business, looked at a couple of books, couldn't help, sorry. So, I drew a deep breath, said the Hell with it, typed in, "As Hippocrates said, At Least Do No Harm," and shoved it into the fax machine. The next morning it appeared, next to two million copies of my photo; so at least the editor seemed to like it. Some friends soon called to say that Senators Dole and Moynihan had adopted the line on the noon and six o'clock news, each attributing it to Hippocrates. No matter what happened to the Clinton Health Plan, it looked to me as though I would be forever guilty of supplying the world with a highly quotable misquotation.
Since then, with more time to do a proper search, I'm unfortunately still uncertain. William Safire at the New York Times, was intrigued but could only refer me to a nice lady at the Library of Congress who was a crony. She tried to help but was stumped. Some Hippocrates scholars at the Library of the Philadelphia College of Physicians were able to find a reference in The Epidemics which seems to say what we are looking for, and that reference has tardily crept into Bartlett's latest edition. Some people think Galen really wrote it, which might account for the Latin; but even that is unsatisfying to scholars. Somebody or other took that phrase, whether written by Hippocrates or not and pounded it over and over until it became a medical student incantation. Even if Hippocrates actually did express that sentiment in passing, it doesn't come through as a really important statement, and there isn't much evidence that his students were repeating it over and over as the words of the master.
My present suspicion is that vague rumors about Samuel Hahnemann, the father of Homeopathy having a hand in promoting the slogan during the Nineteenth century, may have some underlying substance. Homeopathy was a belief system which emphasized the prescribing of infinitely minute doses of medicines. It had a flurry in the 19th Century when conventional Medicine was reeling from excesses of bleeding and purging, which surely did a lot of harm to victims of, say, Yellow Fever. The acrimony even spilled over into the emotionalism of the abortion debate, because laws prohibiting abortion had been sponsored by the allopathic American Medical Association. The verbal warfare between doctors of Homeopathy and "Allopathy" was bitter beyond describing. Although conventional medical care finally got its feet on the ground, and homeopathy is now pretty much a historical relic, the homeopaths did have that big strong point. Doing nothing is clearly better than doing something harmful. Nobody takes Latin, much, anymore. So the modern medical way of saying the same thing has come to be, "The hardest thing to do, is to do nothing". This way of stating the same idea is widely believed to have been offered by William Osler, but after all the controversy about Primam non-nocere , I am now reluctant to be too sure about anything in this area.
Nowheres-ville

|
| Jacob S. Hacker |
In more recent writings, Jacob S. Hacker seems obsessed with social inequality, but while he was a graduate student he wrote an excellent and objective book, The Road to Nowhere containing unique insights into the politics of the Clinton Health Plan of 1993. After that hubby was over, he interviewed most of the important actors in that drama, at least those active in the liberal politics of it, and they talked freely. Like the rest of us, he was unable to identify let alone talk with the leaders of big business, who are of course still pursuing their original goals. What emerges does sound roughly accurate; Hillary Clinton and Ira Magaziner designated to find out what this health business was all about; solicit every proposal on the mind of political, particularly congressional, allies; gather and examine all the useful ideas in circulation in academia and the insurance community; and negotiate possible solutions with a surprising new ally, the big corporate employers. A huge semi-secret task force was then assembled to exchange ideas, discard really bad ideas, and work the proposal into legislative form. There would be internal inconsistencies and conflicts but no matter.

|
| William Clinton |
Congress would work it out, differing versions would appear in House and Senate bills, and President Clinton himself would eventually be able to intervene when things got to the House-Senate Conference committee. Since the Clintons really had no pre-conceived ideas on this complicated topic, the will of the people would emerge from a huge debate, and the will of the people would prevail.
That's one version. The other way to picture this circus would be that a highly skilled politician would offer everybody a chance to propose pet projects, and those who failed adversary process would be obligated to support the ones who did prevail. Trade-offs would be made, as needed, and the political ringmaster in the White House would have the final say.
But the final version was the one that came through to the public and the leaders of big business. You weren't going to know what the plan was all about until it was too late to do anything but accept it after a big sales talk full of snake oil. Big business, which had a serious interest in a particular outcome, also had an army of experienced Washington lobbyists. These people were aware of the unpredictable quirks of the house-senate conference system, were completely confident that the membership of that committee would be stacked in favor of a particular outcome, and knew that a congressional staff with agendas different from those of business would, in the end, be perfectly capable of stealing the show. For major employers, that settled it.
Big business had been wavering about whether to go ahead with their own plans, anyway. They had listened politely and carefully to what the government wished for its own insurance plans, Medicare and Medicaid, and were probably willing to agree. But as matters approached a unified approach, too many things surfaced they didn't like, and too much chance the decisions would go against their wishes. There was too much to lose, too little to gain, and well, we're sorry, we can't go along. This or something rather like it seems to have been the final outcome. The press had been furious about exclusion from major news items, coupled with annoyance at the favoritism toward Mr. Weinstein of the New York Times. The whole medical industry was jittery about exclusion from consultation or even notice; the insurance industry was pretty comfortable with the status quo; the public was in a state of utter confusion After the main partner dropped out, the proposal never even came up for a vote in Congress.
What To Do If You Have a Heart Attack

|
| No Ambulance, But Faster |
On a pleasant Spring Sunday some time ago, I was at home, doing nothing in particular, when I suddenly experienced severe, crushing pain deep inside my chest. No doubt in my mind what that meant, so I quickly took an aspirin and looked at the clock: 6:50 PM, daylight time. Out the window to my right, my neighbors were having a yard party, so I walked thirty feet over to them. Side-stepping the big Hollywood hello, I told my neighbor I was having a heart attack and would please like a fast trip to the hospital. There was some talk of calling an ambulance, but that was brushed aside. No time.

|
| E-Z Pass Speeds the Trip |
Neighbor Charlie took the wheel, a friend got in the back seat, and off we went, fast. About that time, I started to sweat, just like they say in books, but to my surprise only after two or three minutes of the pain. The pain continued unchanged. Luckily, on Sunday evening, traffic was light. Down the main road to Benjamin Franklin Bridge, through the gate with E-Z Pass, over the bridge, turn left. I asked the man in the back to call the Emergency Room on his cell phone to tell them I was coming in, please get the cardiac intervention team to come to meet me at the hospital in a few minutes. We made one wrong turn on a one-way street, adding three blocks to the ride. I knew better but didn't feel equal to protesting. We were soon at the right door, and then into the reception area of the Emergency Department. This area is almost brand new; the first time I had been there. But I had been all over that hospital every day for years at a time, and for two years had been the Physician in charge of the Emergency Room, myself.
|
| Electrocardiogram |
I didn't recognize the nice lady at the desk, who wanted to know my next of kin, Medicare number, other insurance coverage, the color of my eyes, the name of my dog. My companions are very large fellows, and I was about to tell them to be polite, but if necessary knock her down, when actually I said the magic words,"Severe chest pain". That was part of her standard protocol, apparently, since I was immediately ushered onto a stretcher through a side door, had an electrocardiogram, watched the resident pick up the phone to call the cardiac team. Then I waved off somebody's informed consent speech to the effect that I didn't just consent to, but in fact, demanded an angioplasty. My clothes were taken away, intravenous lines were placed, ice-cold antiseptics were swabbed around. I was shaved in a business-like way in what the lady cutely called a Mohawk. The surgeon appeared, started his own informed consent speech which was waved off. The locks on the wheels were kicked loose, the stretcher started for the elevator, surrounded by scrambling attendants holding bottles. When we came to rest under a big light in some ceiling, I looked at the large wall clock. It was 7:20 PM. That was exactly thirty minutes after the pain began.
|
| Cardiac Catheter |
I was more or less awake during the whole procedure, getting to watch the dark black line of the catheter moving around on the scope beside me. I didn't know this particular surgeon, but it was obvious he was good. Usually, you can watch the catheter tip advance, then pull back, try again, pull back, try again and hit an obstacle. This evening I had the joy of watching a virtuoso performance, with the catheter smoothly advancing to its destination, twist and come to rest. Black dye squirted out, outlining the artery and its branches. The electrocardiogram correctly predicted the obstruction in the right anterior descending artery, and to general relief, the other atrerieswere "clean".
Probably because I got there so fast, plus swallowing an aspirin at home and chewing several in the Emergency Room, no clot had formed around the obstruction, which apparently was caused by a plaque of cholesterol with a split in it occluding the wall of the artery by bulging into the lumen. There seemed to be no clot behind the plaque or in front of it. The catheter had a stent over the balloon tip, which is to say it contained what amounted to braided chicken wire. The whole contraption gets opened up by inflating the balloon, then deflating and withdrawing it, which allows the artery to be held open by the unfolded chicken wire which remains in place. With the early versions of stents, fibrous scar tissue would grow over the chicken wire and block up the artery a few weeks later. Hence, the stent was coated with a chemical which prevents fibrosis. Unfortunately, this chemical also retards the growth of cells which line an artery on the inside, so coated chicken wire provokes clots. While I was still in the operating room, the solemn incantation was begun: I must take an anti-clotting drug every single day for a whole year, and if I missed a single pill, I could immediately die. I was to hear this incantation twenty times, so I guess they really mean it.
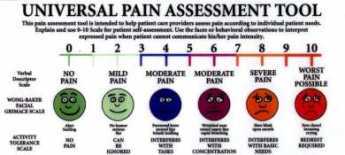
|
| On a scale from 1-10, how bad is it? |
Well, I was asked to call out a number from one to ten, indicating severity of chest pain. It had been "three" when I got to the operating room, even though it had begun as a "seven", and rose to "seven" several times during the procedure. Seven was my own invention; if I had to ask for pain-killer it was going to be an eight and would get to nine if I had to cry out. It never got worse than seven. When they pulled the catheter out of my groin, it was zero. It has stayed zero ever since.
It was a cause of some interest that my enzymes never rose. When heart muscle is injured, characteristic enzymes leak out and appear in blood tests; you can more or less measure the extent of the damage by the level it reaches. I had reached the emergency room so quickly the enzymes had not had a chance to rise. And the artery was re-opened so soon, they never did rise. For the first time in my life, my blood pressure was 250, so I guess I wasn't as calm as I let on. Somewhere during the procedure, the sweating stopped.

|
| Severe chest pain |
So, off to the cardiac care ward, where the custom is for each attendant to write his or her name on a whiteboard, while the date and time are prominently displayed for continuing orientation. They give you a phone so you can call your nurse, but my suggestion is to offer earplugs to drown out the continuous chatter at the desk. A patient of mine once called it the Racket Club. The food is, well, hospital food. Protocol says it should have no salt. I discovered that breakfast arrives on the dot at 9 AM, supper on the dot at 5 PM, lunch somewhere in between. I believe I understand the reasoning. Two days of this, and I'm discharged. Nothing to it, if you get there fast. Let me repeat, if you get there fast.
Since this light-hearted day trip is in sharp contrast with the six weeks of strict bed rest so routine in the days of my internship, not to mention the considerable mortality and disability that prevailed until quite recently, it justifies some reflection. As a medical student, I knew Andre Cournand and Dickenson Richards, who perfected the cardiac catheter. They were awarded Nobel Prizes, as was Michael Brown, who invented the statin drugs to lower cholesterol. Affable and modest men, they have saved millions of lives, now including mine. Or at least they did so, with the assistance of thousands of other doctors who perfected one by one the details of the little minute we danced in the operating room, each adding some little refinement, or eliminating some little hindrance to success. But, doggone it, you have got to get to the hospital fast.

|
| Helicopter Dreams |
To do that, you have to give it some thought in advance; some community organization would also be useful. In my case, waiting for an ambulance would have slowed me down. Not everybody can live within a few minutes fast drive of a hospital, and not all hospitals are equipped to handle such cases. The range of effective rescue could be extended with helicopters, but you have to give some thought to where you would have to drive to find a place for a helicopter to land. Philadelphia is almost unique in having the largest evacuation company in the world, headquartered in Trevose, but it would take a lot of negotiation to arrange a system for the whole Philadelphia area. It just happens my oldest son was helicoptered off a mountain in Nepal this year (by an affiliate of this company), but his helicopter almost ran out of gas. These things can be done, and yearly evacuation insurance is about $200 a year, anywhere in the world. But it would take an awful lot of community planning and argue -- and maybe suing -- to make it happen. Is it worth it? Sure, but a little hard thought in advance might offer better solutions for most people.
Madeira Party 2009

|
| Madeira Wine class= |
The hundred years war, the thirty years war, the seven years war, and other European disagreements made it difficult to import wine to England, turning the wine import trade to Portugal. Port wine was, of course, prominent, but the best wine of all came from the Portuguese colony of Madeira. The island of Madeira is closer to Africa than to Portugal, so the triangular slave trade made it easy to import Madeira wine to the British colonies in America. The eastern seaboard of America had no grape culture of any note, so the beverage trade centered on rum, whiskey, beer, and Madeira. George Washington is widely reported to have had half a bottle of Madeira every day for lunch, for example.
|
|
| S. Weir Mitchell. Mitchell |
The other evening at the Franklin Inn Club, a traditional Philadelphia Madeira party filled the hall, and the membership was brought up to date on some of the traditions and finer points of the occasion. In the first place, the Franklin Inn was founded by S. Weir Mitchell. Mitchell, in his spare time as Father of Neurology, had written a short story called The Madeira Party which worked in a large number of details about what was what about Madeira, ending with ribald tipsiness. Nathan Steven, a well-known wine authority, instructed the group in the various types of grape and vintage, and other members who have summered in Madeira related current conditions. Because the volcanic island is a favorite place for visitors, particularly Englishmen, real estate is at such a premium that most vineyards have only one or two acres of grapes. The wineries whose names are on the bottles pick up the crop from these local growers and take it on from there. This seems as good as any other explanation for the current high prices of the wine. However, a century ago a disease wiped out the French and Portuguese vineyards, who were forced to beg back some exported grapevines from California to get back in business. So, one wonders about the scarcity claim.

|
| Madeira in a barrels |
It is related that a number of cargoes of Madeira, particularly those of John Hancock of Boston were caught being smuggled to the colonies, and got returned. It was discovered that the taste of the wine was greatly improved by the tumult so that each vintner experimented with various methods of agitating and heating the wine to produce a particular brand. Madeira, like sherry, is a fortified wine, with various proportions of grain alcohol and brandy added in secret formulas. On one point there is general agreement, that if fortified wines are aged for long enough periods, eventually they all taste alike. There thus has emerged a tricky business of aging the wine long enough for the vintage of the wine to match the age or anniversary of the person being honored by the gift. Fifty years is the tricky goal; it's the most popular gift, but perilously close to the point where you can't tell if it is sherry or Madeira. There are four main varieties of Madeira (brand names are something else), getting progressively sweeter, darker colored and more expensive as they age. Malmsey, in a barrel of which Shakspere portrayed the royal princes being drowned, is claimed to be the very best. Some people regard it as too sweet, however. At proper Madeira party, each variety is served with a different course of terrapin or whatever. The President of the Franklin Inn read off the instructions for cooking the traditional first course of jellied boiled boar's head, and the guests agreed that modern tastes called for a substitute. After the reading of Mitchell's short story, the group added a new tradition of singing Flanders and Swann's ribald song, "Have Some Madeira, m'dear".
Chuck Barber, the current President of the Green Tree Insurance Company, added an entirely new historical slant. The Insurance Company is well known for having the best dinner in town at its meetings since directors of insurance companies don't do much. At the dinner in 1799, the news was brought in that George Washington had just died. A member rose to propose what has become an annual toast in Madeira, "To President Washington!" In time, S. Weir Mitchell became a member of the board, and the famous short story was the outcome which firmly fixed the rules of the Philadelphia Madeira Party. Bill Madeira was called on to verify this history, but he protested that his family name was derived from the wine, not the other way around.
It seems appropriate to add another historical note. Benjamin Franklin, after whom the club is named, suffered severely from gout. Although some sort of association with liquor had been mentioned as far back as Hippocrates, Franklin's powers of observation and his fame as a scientist placed him in a position to make it an irrefutable doctrine that gout was a medical penalty for drinking liquor. It was, of course, Madeira that old Ben was drinking, and it was the rule that Madeira was transported in lead-lined kegs. The Green Tree has some of the old kegs if you doubt it. Franklin's observation was acute, but what he was reporting was the effect of the lead poisoning, not of the wine.
Equal Pay for Equal Work

|
| American Medical Association |
The House of Delegates of the American Medical Association holds a five day convention twice a year. The meetings last from 7 in the morning until midnight, although the main sessions in the auditorium only last eight hours a day for three days. The rest of the time is consumed with meals, committee meetings, geographical caucuses, and even cocktail parties. Newcomers often object to the numerous parties until they come to see that these are merely committee meetings in a different form, with different subsets of the organization picking up the necessary costs. This group of workaholics has to vote on several hundred issues each session, and most Delegates have little advance opinion when they enter the headquarters hotel on the first day. But after meeting with their specialty in one committee, and members of their geographical region in another, and members of their medical school alumni association in yet another, and with issue-oriented groups, political allies, and other layers of an overlapping matrix day after day -- by the time the vote is actually called for, most Delegates could safely predict the correct outcome with very few exceptions. The AMA works at its similar job with far greater intensity than Congress does because Congress has all year to do it, while the doctors have to go home to make a living. Don't worry about the parties, they are really working sessions for everyone except rank newcomers, outsiders, visitors, and wives. What is perhaps more worrisome is the rare occasion when just about every delegate arrives with one opinion and is persuaded by the leadership to adopt the reverse. That can only happen if new information is suddenly revealed, with little time to check its accuracy.
There are usually fifteen or so parties every night, hosted by large state delegations, large specialty assemblies, and coalitions of smaller groups. Fifteen drinks a night would be quite a bit for most folks, and some newcomers are duped into trying to be polite about it. The rest of us take the proffered drink, walk over to a nearby plant stand and dump it. I hate to think of how many potted palms I have fried that way. Each delegation has its own system of organizing these minutes, and I'll try to describe the Pennsylvania system.
Nobody will come to your party if you don't go to theirs, so we make a list and divide the group into those who "travel" to the parties of other states, and those who remain to host our own party, "at the door". Everyone is expected to wear a name tag, containing your name in large type underneath which is your caucus designation, in my case "Pennsylvania". The older members instruct the newer ones to put the name tag just under their right shoulder. That way, you can seem to be looking at the hand you are shaking while freshening your recollection of who in the world you are meeting. You can, of course, do anything you please, but time is short for the transaction of a lot of business, and it's just easier to do routine things the regulation way, and get on with it.
On the evening in question, I was "at the door". The formula, repeated many times, was to extend a hand of greeting and recite, "Welcome to Pennsylvania. Are you looking for some friend in particular? Let me see that you have a drink. Come on in and meet my fellow delegate, Scotty Donaldson." You can shepherd a lot of people more or less gracefully if you reduce the formalities to a routine. After several people had been brought in under the tent, a man with highly polished shoes came up, wearing a name tag that said, "Blue Cross of America". He was greeted, his hand pumped, a drink procured, and was introduced to Scotty, our most famous extrovert. I quickly turned to the next person at the door.
Well, this lady was six inches taller than I am, and fifty pounds lighter. She wore a name tag, identifying her as President of some Nurses Association, "Welcome to Pennsylvania! Is there someone from Pennsylvania you know or would like to meet? Can I......" The apparition didn't even look at me as she brushed past through the door. Heading straight for the gentleman from Blue Cross, she poked her index finger into his chest, stopped him in mid-sentence as he talked to Scotty.
"What I want to know, " she announced to this startled man, "Is when are you people in Blue Cross going to pay nurses as much as you pay doctors?" And here I must admit I have to give this guy credit for unperturbability.
"Well, madam," he said cheerfully, "I think that's going to be quite some time."
Health Maintenance Organizations (HMO)

|
| HMO |
It's an ancient wrangle whether a manufacturer should actually own its suppliers or the reverse; or instead whether it's healthier for industry components to stand at arm's length from each other. At issue is not only what is best, but what is fair. If industry mergers seem sufficiently unfair, it will be proposed they should be illegal. That's the main substance of a lot of antitrust argument. Unfortunately, what is valid in good times may be reversed in a downturn. A prosperous supplier of materials often acts as a "cash cow", saving a merged enterprise from bankruptcy. Unfortunately, within a different economic climate one badly failing supplier can bring down the whole merged enterprise. There's also organizational friction; a temporarily prosperous unit may get to thinking it should boss the less prosperous units around. At the very least, the cash cow resists the use of its cash reserves to help "losers". Several centuries of experience have thus left a minefield of old laws, traditions, and ingrained prejudice to undermine any broad standards for what is best. In no field is this truer than the Medical Industry.
Eighty years ago in Houston, the first Blue Cross health insurance company was started for a single group of school teachers to pay for service in a single hospital. That expanded to other subscribers and other hospitals, soon making it more workable for insurance, subscribers, and hospitals to stand at arm's length, allowing for a variety of local combinations. During World War II, combat in the Pacific led shipyards to be built on the West Coast, but westward migration of steelworkers was hampered by lack of local medical facilities for them and their families. Taking advantage of the loophole provided in the wartime wage and price controls, Kaiser Industries attracted medical personnel by building hospitals, paying salaries, and offering physicians ready-made medical practices. Because of various licensing laws, Kaiser's medical enterprise was divided into two corporations, Kaiser and Permanente, so a specialized corporation within the Kaiser-Permanente Foundation could accommodate the licensed practitioners. The salaried nature of the physician organization immediately caused trouble with local fee-for-service practitioners, who were thus excluded from a large population in their neighborhood when they could not readily adjust to varying mixtures of the two payment methods. Their reaction, led by an obstetrician in Stockton, California, was also to organize dual-corporation structures which were exclusively fee-for-service. Because Kaiser had a Foundation, they also called their organizations Foundations for Medical Care. Then, as now, it proved difficult to run a practice with two different reimbursement philosophies in the same waiting room; in time, friction between the two styles tended to increase as doctors who were more comfortable with each style tended to segregate themselves. Since offers of salaries are more immediately attractive to newly-trained physicians, they flocked to California to serve the steelworkers who were in need of doctors. Fee for service, on the other hand, allowed the gradual assembly of a more durable practice composed of patients who could test what they liked before making a permanent allegiance. Essentially, the transients went to Kaiser, more permanent settlers used fee-for-service.
Thus, it came about that several models for health care reform were tested in a few smallish towns of central California. These demonstration experiments may perhaps not meet everyone's standard for scientific purity, but at least they were public examples with the dumber features knocked away. They certainly provided a laboratory where ideas could develop about topics that otherwise were merely opinions and unsupported conjecture. The Foundations demonstrated that physician-dominated organizations could contain costs and maintain quality in a satisfactory way; there had previously been doubted about their ability to contain cost. The Kaiser organization showed that salaried practice performed acceptably as well, both to most staff physicians and to a majority of the patients; there had been doubt about the willingness of the public to limit choices to a panel of assigned physicians, mostly young and usually from elsewhere. Finally, the two systems seemed to be able to live together more or less peacefully; indeed, the California public seemed reassured that two systems apparently kept each other in check.
The first main difference rested on the system of quality control. The local Foundations developed review systems based on peer review and peer pressure; these worked remarkably well, particularly in constraining non-physician costs like pharmacy, tests, and hospitalizations. Cost and quality control in the Kaiser system was more rule-bound and quicker to apply discipline, kept within bounds however by the ability of both patients and staff to jump ship for the other system. Aside from professional peer review, the Kaiser system experimented with owning hospitals, laboratories, pharmacies. Here, the experience directly paralleled the experience of manufacturing industry with its suppliers; when reimbursement was generous suppliers generated welcome revenue. When reimbursement was constrained and substandard, ancillary service losses were unwelcome. Taken overall, the Houston experience was repeated, that ownership of such facilities was mostly a headache. Indeed, subsequent experience has shown the two systems usually co-exist nicely within independent ancillary facilities.
The Stockton, or Foundation for Medical Care, approach grew popular in the West. The variant which grew up in Utah was locally popular and attracted the attention of Senator Wallace Bennett. The Bennett Amendment to the Medicare Act then picked out the peer review system as the secret of success and set up a nationwide system of Professional Standards Review Organizations (PSRO) to conduct peer review of Medicare and Medicaid patients. The drawing of boundaries around these organizations was the most difficult part, and sometimes the boundaries were inept. Rural districts were adamant that the standards of big-city medical schools were not to be applied to their scattered resources, and urban areas saw themselves as ancient Rome surrounded by hostile tribes. Although these difficulties were foreseen, it is not always possible to draw a line that will separate the cultures, particularly where the outward migration of suburban housing was more rapid than the construction of suburban medical facilities, leaving the medical culture unstable. The PSRO system was quite successful in many areas but caused trouble in others that were not adequately addressed. The central concept of the review system was that the doctors who worked together could quite readily identify the outliers, and better than anyone else could judge whether the local situation was justified. True, some practitioner might try to abuse the system to the disadvantage of his competitor, so no adverse decision was final until there had been an opportunity for outside appeal. There might even be a few circumstances requiring a still higher appeal. The system was new and untried, but it produced eminently satisfactory results from the point of view of the Federal Government paying the bills. As former President of one of the largest PSROs in the country, I will assert that there was remarkably little friction or resistance in the medical community. My very good friend, the President of the New York City PSRO says much the same, and most people would say that if you can carry off a new system in New York without a lot of argument, it must work pretty smoothly. The Government wanted to eliminate unnecessary Medicare costs, particularly in hospitals, and it wanted to maintain peace with the medical profession. Hospital costs are obscured by the wide gap between posted charges and true underlying costs, compounded by disagreement about the proper assignment of overhead charges. Charges were not the assignment of the PSRO, utilization was. Days of hospitalization per thousand enrollees fell from roughly 1000 days per thousand to roughly 200 days per thousand, and that satisfies me at least that we were doing our job; physician peer review was doable.
It is likely, however, that peer review was much more apt to produce friction in rural districts. Philadelphia has had more than a hundred hospitals for more than a century. Birds of a feather tend to flock, so the sorting-out process was already far advanced by the application of constrained referrals to practitioners who failed local standards. Mixing members of different hospital staffs on appeals committees was easy in the big cities, and the naturally censorious tendencies of many physicians could be safely counted on to produce adversary balance. Most committees seemed visibly pleased, even relieved, to discover generally good quality in their competitors' practices. However, in the much smaller and more scattered institutions in the nation's regions with low population density, these informal arrangements cannot stretch as well. When there is only one specialist in a field, for example, it is sometimes hard to know whether he is a good one or not, but always easy to say whether you like him or not. Where the population thins out, much greater wisdom is required to make judgments, the number of close cases is greater, and the limited supply of judicious reviewers is similarly stretched. At least that is my surmise, based on knowing the background of most of the AMA delegates who eventually voted 105-96 to condemn the program in a standing vote. The result was the Dornenberger Amendment, which much weakened the system when instead it should have triggered a more profound analysis and reconsideration.
Perhaps we spend too much time here describing a technical process. It is, however, at the heart of what makes the Foundation approach (sometimes called IPA or Independent Practice Association) superior to the HMO. It is now perfectly clear that both doctors and patients vastly prefer the IPA approach to the HMO, and any reasonable politician would jump at it. But there is one fear, summarized by the slogan that the Fox is guarding the Henhouse. In both systems, an attempt is made to combine insurance with the delivery of health care. In the IPA, the physicians are taking the financial risk that aggregate income will exceed aggregate costs; it's a risk contract. In the case of an HMO, the employer or the government is taking the financial risk and therefore wants to control it. If revenue is good, the doctors will prosper in an IPA; the insurance company intermediary will prosper in an HMO. Doctors will care about that little difference, but why should the rest of the country care?
Because the prospect is overwhelmingly likely that future revenues will be constricted until something hurts, and when you starve with a tiger, the tiger starves last. In the case of an HMO, the insurance middlemen will starve last, and the quality of health care will starve fairly early. That's an unwise design. When we get to the point where Congress cuts the budget and watches to see what happens, Congress will cut it some more if nothing bad happens; it will back off only if something bad happens, so something bad is certain to happen. In designing the system, you need to design the internal review authority so it will cut the waste, inefficiency, and luxury first. The reviewer, no matter who it is, will cut himself last, so you need to arrange the incentives for waste to be cut before the reviewer suffers, and quality of care only after the reviewer has suffered. If you wonder why a whole lot of special interests hate physician-dominated review systems, a short answer will be found in this synopsis. A special exception must be devised for rural health systems, which do have a unique problem.
To return to the well-worn slogan about foxes and henhouses, we have overlooked the central question. Who's the fox, and who is the hen?
Block Captains

|
| Ed Asner |
A block captain is not a ward leader, at least not most of the time. The block leaders of Philadelphia are mostly self-appointed, de facto captains, and yes, they are mostly middle-aged black ladies. Their attitude is that politicians are there to serve the community, not the other way around. At a recent meeting, the leader of the Block Captain's Association called out to the nodding, approving group, "Call your councilman. We elect those people, put 'em to work!"
This enthusiastic group of several hundred grass-roots leaders meets several times a year in, of all places, the hallowed auditorium of the Philadelphia County Medical Society, but doctors are not running this show. Nor is the City Health Department, nor the Department of Streets, nor the various mental health and social service agencies that send representatives. The federal government expressed considerable gratitude in being able to address this group because their new Medicare prescription card was so terribly hard to explain (i.e. it was terribly hard to understand). The genius of the block captain movement is that it appoints leaders to understand what the establishment is trying to say, and then figures out a way to say it. You can make free flu shots available, even take them to the home or workplace, but most people won't accept them unless it is explained by someone they trust. Dead birds don't spread disease, mosquitoes do, but that really sounds a little unlikely. To believe that, you first need the word of a respected local leader. The U.S. Army is built around its sergeants, in the same way. That's in fact how things work at every social level, but in Philadelphia's black communities, it is finally becoming organized. For example, they like pamphlets. Pamphlets are what give sergeants credibility back in the neighborhood.
Success has a thousand fathers, failure is an orphan, so it's now hard to know who started this. Eve Asner, the sister of Ed Asner the movie star, can claim credit for starting a group called Philadelphia More Beautiful, dedicated to cleaning up the messes of the slums, and applying social pressures of a loud and effective sort to irresponsible neighbors. And then, along came the Deputy Health Commissioner Larry Robinson with HEAT. During a hot summer, it was possible for a hundred children and old folks to die of heat prostration because they were confused by dehydration and did things which made matters worse for themselves. The block captains were ideally situated to know who was in danger, who hadn't appeared outside in a day or two, and thus who might need to be forced to drink water or go to an air-conditioned movie. Training the block captains to recognize the signs of trouble fit nicely into the Health Department's ability to measure results with computers. Last year, only seven people died of heat prostration, and everybody knows whose block they lived in.
The Medical Society pays for everybody's lunch at the block captain's meeting, and it is a calculated policy. Every doctor knows how useless it is to talk in terms of calories, carbohydrates, high unsaturated fat content, and water-soluble vitamins. Pamphlets help, but what really works is to serve the block captains a lunch and tell them, now this is what we're talking about. Heaven only knows how that gets translated back in the neighborhood, but surely the first step is to give the block captain an unmistakable message. The Medicare bureaucrat looked visibly relieved when her painfully convoluted explanation of the Medicare prescription card was reduced to about two sentences by questioners in the audience: If you have Medicaid coverage, forget it. If you don't, that card's worth about $600. And this here pamphlet proves I know what I'm talking about.
There did not seem to be a scrap of ideology or power hunger or self-serving -- the usual hallmarks of politics as we commonly observe it. The over-riding principle on which these highly disparate groups are operating together is, pick a problem, and solve it.
Three-Mile Island

|
| Three Mile Island |
On a mud flat of the Susquehanna River called Three Mile Island, a nuclear energy plant had been built around 1970. The mud flat was in front of the entrance of the Swatara Creek, where Middletown the first town in the County had been laid out in 1732. Later on, the town of Harrisburg became the capital city of Pennsylvania, located a few miles north of the Swatara Creek at what had been called Harris's Ferry, later Harrisburg. For quite a while, Middletown and Hummelstown, also on the Swatara Creek, were the two main towns in the area, but the location of the state capital attracted railroads and steel mills to Harrisburg. One of its main claims to fame was that Confederate General Robert E. Lee was thought to have it as his primary objective for invading the North, frustrated in this goal of course by his defeat at the battle of Gettysburg. Meanwhile, Middletown has declined to a small country town and was therefore originally glad to have the industry of electricity generation located next to it. It's true the huge cooling towers loomed ominously, and huge plumes of evaporated water rose in clouds to be seen for miles. But Middletown slowly took on the look of a refurbished 18th Century town, fancy new restaurants and all, prosperous and waiting to be discovered as a tourist attraction. Maybe in time, it would be the next Williamsburg.
|
| The China Syndrome |
On March 28, 1979, some valve got stuck within Reactor Number Two. The plant had two reactors, each with a spare cooling tower so it looked as though there were four nuclear plants instead of two. Warning lights and whistles went off, and it is easy to imagine a general panic within the operators of the plant, especially since a popular movie, The China Syndrome had just been issued two weeks earlier, depicting an imaginary implosion of a similar nuclear plant with famous movie actresses running around screaming. It took about five days for the plant operators to make a preliminary assessment of the TMI situation, which did not seem as bad as it might have been. It would take six months to reach a final evaluation of just what had gone wrong, and why. In the meantime, almost anyone could say or imagine almost anything; no one could prove they were wrong. The local citizens held a referendum; they wanted all of the facility to be closed, permanently. Secretary of Health Gordon MacLeod wanted a somewhat more reasonable thing, which was large supplies of sodium iodide pills to be distributed to the populace to prevent the radioactive iodine content of escaped gases from being attracted to the thyroid glands of the population, especially children and child-bearing mothers. Unfortunately, he took the unforgivable step of criticizing the state government for not having stock-piled the pills, and the Governor fired him, thus demonstrating strong decisive action in an emergency. The news media were equally at sea because this was big news. When all was finally said and done, there was no evidence that anyone was injured as a result of the accident. More than thirty years later, there is still no sign that anyone was ever hurt.
|
| Hiroshima Explosion |
We might not have been so lucky, of course. When the Russian plant at Chernobyl had a worse accident in 1986, literally thousands of Ukrainians were sickened, and the death rate was appreciable. In Japan, the victims of the Hiroshima explosion were closely followed for many years, and the incidence of cancer of the thyroid among the survivors was truly frightening. However, after more decades elapsed, it was possible to determine that the overall death rate from thyroid cancer was not increased, suggesting these new cancers were not particularly malignant. But in a different set of circumstances, when the Chinese set off their tests of nuclear weapons, it became clear that these tests were followed in a few years by a world-wide epidemic of Hashimoto's Disease of the thyroid. Radioactivity in mushroom clouds is mainly radioactive iodine, with a half-life of seven days. Unfortunately, the clouds sail around the earth, eventually settling into the dirt on the ground. Grass grows there, and cows eat the grass. By this time, the radioactivity is much diminished, but the digestive systems of cows concentrate this weak radioactive iodine, which then gets into milk in a more active form. The kids drink milk and get Hashimoto's disease. Whether they will later get thyroid cancer and die of it remains unknown, but possibly not, in view of the Hiroshima experience. So, amidst a welter of conflicting evidence, it is still possible to say almost anything about nuclear power risks without fear of provable contradiction. It is only safe to repeat that radioactive iodine exposure doesn't do anyone any good.
Unfortunately, thirty years after the accident, we now all understand it would be a good thing to develop energy independence from Middle East sources; but we remain unsure just how unsafe we are willing to become in order to re-adopt nuclear energy. Since the accident at Three Mile Island, our government has made it impossible for a single atomic plant to be built in America. And the politicians are surely right about frightening public opinion on the topic. Just look at pretty little Middletown: it's moving toward becoming a dilapidated ghost town.
Without claiming any expertise in atomic energy production, it is possible to quote others to the effect that the hesitation of the politicians is no longer focused on the danger that a plant will explode. Rather, the real dispute is about the disposal of nuclear waste. No one wants it nearby. The French have built nearly sixty plants in the thirty years we have hesitated; how do the French dispose of nuclear waste? The answer seems to be that waste disposal is not a problem with the French methodology, but a new problem surfaces that the French approach generates a type of waste which is much easier for an undeveloped country to deploy as material for atomic bombs. So, the rumor commonly circulating is that this is really the main practical objection to constructing nuclear energy plants in the French style. As is true for the entire nuclear topic, the rumors outrun the evidence.
Governor Keith's House
Route 611 begins at Philadelphia's City Hall and goes due north, headed for the Delaware Water Gap. In 1717 Lieutenant Governor Sir William Keith had decided he needed a summer residence to compliment his in-town establishment on Second Street, and acquired the 1200 acres of land of Samuel Carpenter on Easton Road, now Route 611. Sam had been entrusted with 2000 pounds against a possible French invasion, which Keith transferred to himself by taking Carpenter's land in lieu of it. The ethics of everybody in this transaction are now a little murky. The selected farm area was cool and tranquil, with creeks and level land, so a suitable three-story mansion was built of local stone, with outbuildings. A large mushroom-shaped rock was carved, polished and set on a pedestal beside the house. Tradition has it that Governor Keith asked servants and slaves to lift the stone as a test of physical strength. Keith had several negro slaves, eight or ten indentured servants, and others who were simply hired help for a rather large farm. Criticism was heard for the elaborate luxury of a mansion fifteen miles from town which it took five or six hours to reach.
Governor Keith was an interesting person. He inherited a Scottish baronetcy from his father and is the only Governor of Pennsylvania with a claim to noble blood. His finances were meager, however, and his life was a succession of efforts to advance his own wealth and position, which he regularly consumed with high living. He involved himself in coups and rebellions in Scotland, probably out of expectation of reward from the exiled King James. Efforts at court were finally rewarded by Queen Anne making him Surveyor-General of English land from Pennsylvania to Jamaica, but only after his nearly being hanged for treason for suspected efforts on behalf of the exiled former King James. Keith lost this essentially tax-collector position which he had performed creditably when the Hanoverian King George I took over the throne. After William Penn encountered difficulties which returned him to England, he and the Penn family were in need of an administrator in America, and Keith was at pains to ingratiate himself with Hannah Penn after William suffered several strokes from which he was to die in 1718. Most who met him felt that Keith was charming, although some regarded him as a charming rogue; he succeeded in ingratiating himself to the Penns and was appointed Lieutenant Governor of Pennsylvania in 1716, incurring substantial debts to transfer his family to America in style. After taking office, he wasted no time starting schemes and devices to enrich himself, while at the same time pursuing a populist political style which involved him in more or less constant controversy. There are many echoes in his career of that enduring subsequent conflict in America between creditors and debtors; as probably the most indebted man in Pennsylvania, his populism was highly troubling to conservative Quaker farmers. He pushed hard for paper currency, always popular among debtors, and probably sought to soften the feelings of the Quakers by pushing hard for the replacement of legally binding oaths with secular "affirmations". By doing so, however, Keith infuriated the vestry of Christ Church, representing widely held Anglican support for requiring oaths. Keith's pandering to differing viewpoints succeeded in infuriating James Logan, the secretary of the Penn proprietorship, into setting sail for England to seek Keith's removal from office. Logan only returned with a letter of admonishment from Hannah Penn, and controversy continued to simmer. Reduced to its essentials, a case can be made that Keith behaved like an unrestrained modern machine politician exploiting every opportunity he could find.

However, certain things can be said in Keith's defense. There is no doubt the Quaker farmers were hypersensitive about the display of wealth which a Scottish baronet would find quite appropriate for a man in his station. His mansion, for example, would barely qualify today as a five-bedroom house in the suburbs, and it is a little quaint to recall that generations of Penrose's and Strawbridge's subsequently lived on the property quite proudly, or even defiantly in view of their ample means. Paper money is indeed always the favorite of debtors who seek to dishonor their debts, but the colonies in Keith's times were suffering from a severe lack of space which can now be explained as the consequence of colonial terms of trade but which at that time was a severe economic hardship. His efforts to stop the practice of executing debtors may well have been made with his own indebtedness in the back of his mind, but still, it seems like a step in the right direction. Even the inventory of his property probably exaggerates the ostentation of his lifestyle. True, he had 144 chairs in the house, but the shortage of currency at that time had converted chairs into a form of exchangeable value, employed by almost every shopkeeper. Land was similarly used as a form of currency, although here most people would raise their eyebrows at a governor accumulating in eight years a list of property including not only this country estate and the downtown house in Society Hill, but a dozen rather large estates in other colonies, and a particularly troublesome investment in a copper mine on the west side of the Susquehanna. To some degree, Keith was a good Governor but was forced into a number of conflicts between the wishes of the settlers and the best interest of the Penn proprietors. Three thousand miles from the Court of St. James, he would scarcely be expected to display universal agility in shifting allegiance between the Stuart Kings, Queen Anne and the Hanoverian King George I, not to mention the Penn family and the settlers on their land. Keith did maintain reasonable stability in the colony while seeming to undermine the best interests of the Penn family. He was said to have made shrewd business decisions for the whole region converting surplus grain into malt at a time of money shortages in the colony, even though it particularly profited his own acreage. In some ways, his reputation remains chiefly tarnished by his treatment of Benjamin Franklin. Encouraging Franklin to go to England to buy some printing equipment, Keith promised letters of credit for what was presumably intended as a joint venture. The letters were never forthcoming, Franklin was stranded for months in England without means to return home. Franklin got his revenge years later in his autobiography. This was not the only example of Franklin nursing a grudge for decades. Poor Keith returned to England to defend himself against dismissal by the Penns because of all the turmoil and factionalism, but essentially never got another job and died in debtors prison. During that time he published extensively about current affairs and economics, but the value of that writing is now difficult to judge.

|
| Horsham Friends Meeting |
After Keith returned to England in 1726, presumably to defend his interests and possibly to evade his creditors, the mansion and estate on County Line Road was sold to Keith's son in law, Dr. Thomas Graeme who was a physician at the founding of the Pennsylvania Hospital in 1751 and evidently had become quite prosperous. Graeme paneled the interior of the mansion in high Georgian style, revised the floor plan, generally making the place elegant. Records of how the region between the counties became named Graeme Park, but presumably Graeme would now put up no objection to it. A second house on the property was home to several generations of Penrose's and Strawbridge's; the Strawbridge family donated the estate as a park. Governor Keith having left his wife forever to her distress alone, fathered two illegitimate children in England, making his prevailing emotions subject to uncertainty.
Around the corner, so to speak, on Route 611 the Horsham Friends Meeting is built of the same sort of stonework, with dates which suggest the meeting itself was present well before Keith appeared on the scene, and the string of similar but tavern-like buildings along 611 suggest the highway to Easton was a busy one even at an early time. Increasing traffic and construction carry an ominous prediction that growth of the area will eventually swallow both Graeme Park and Horsham Meeting in a sea of subdivisions and industrial parks. Placing a turnpike entrance nearby almost certainly hastened that fate.
Lazaretto

|
| David Barnes |
DAVID Barnes, professor at the University of Pennsylvania, kindly visited the Right Angle Club with an interesting talk about the Lazaretto, the oldest quarantine station in the Western hemisphere, and the sixth oldest in the world. It was built in 1800 responding to the Yellow Fever epidemic of 1793, followed by those of 1797, 1798, 1799, 1820, 1853, and 1870. If an incoming ship had a case of Yellow Fever on board, the patient was institutionalized at the Lazaretto and the ship captain had to pay for the care until the patient recovered, or until he didn't. Since we now know that Yellow Fever is transmitted by mosquito bites, it probably didn't do much good, and by locating the Lazaretto in a swamp, it may actually have promoted the spread of the disease. It thus fits into the story of Dr. Benjamin Rush hastening the death of his Yellow Fever patients by bleeding them of several pints of blood, as well as the construction of the Philadelphia Water Works to purify the drinking water, which we can now she had nothing to do with the disease, either. However, the waterworks were a marvel of engineering and must have saved many lives from Typhoid Fever. As recently as 1970, I can remember cases of anthrax being brought to the port on Pakistani ships, so quarantining and quarantine stations are useful ideas, some of the time.

|
| Philadelphia Lazaretto |
The first Lazaretto was built on the Aegean Sea at Venice, around 1450. There is some dispute about the name, which is said to come from the patron saint of lepers, St. Lazarus. The followers of St. Nazareth maintain the present name is a corruption of Nazaretto however, since St. Lazarus was the name of the church on the island where it stands. It seems most likely that the original Venetian quarantine hospital was responding to the plague, which would have benefitted greatly from isolation, although the rats and mice probably quickly found a way around their problem. Benjamin Rush thought that Yellow Fever was transmitted by the overpowering stench of rotting coffee beans, which is quite wrong as Walter Reed later showed, but at least it would lead to the idea that quarantine might be useful. Historically, the rumors and suppositions about this matter were useful to the Virginia delegates to the Constitutional Convention, who used it to promote their campaign to move the national capital to Washington, D.C.
The Schuylkill empties into the Delaware River at a sharp bend in Delaware, which slows the river and causes silt to be dumped there. William Penn had earlier decided to locate his new colony at Chester, just below the bend. However, he soon saw that it was more defensible to locate Philadelphia on the upstream side of the mud flats, as it proved to be in the Revolutionary War. Fort Mifflin was located just above the mud flats and could be kept supplied by flatboats coming down the Schuylkill from Valley Forge and Reading, the arsenal city of the Revolution. On Benjamin Franklin's suggestion, the channels between the mud flats were blocked by the chevaux de fries, underwater spiked contraptions which were much like the blockages to the entrance of parking lots. On the Jersey side of Delaware was Ft. Mercer at what is now called National Park. It was a formidable defense which almost ended the War by starving the British troops who had occupied Philadelphia from the rear via Germantown but were long unable to get past Fort Mifflin with their fleet, coming upriver. Most of South Philadelphia was a swamp, and there are many reports of flocks of swans paddling around the entrance of the Schuylkill. Hog Island became a shipyard, then a Naval Base. And then the airport was built on the mudflats, pretty much-obliterating everything else. There is the talk of making this area into the main intermodal transportation hub of the east coast, since ocean shipping, air transport, interstate highways, and railroad are all crowded together, quite close to the urban centers.
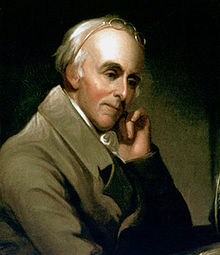
|
| Benjamin Rush |
Benjamin Rush, a signer of the Declaration of Independence, was still active at the Pennsylvania Hospital in 1800. It was still the only general hospital in America and the model for much of subsequent American medicine. One striking memento of that connection at the Lazaretto is the cupola on the center building, which is very similar to the cupulas on the roof of the building at 8th and Spruce Streets. The brickwork is also Flemish bond. The ten-acre site of the Lazaretto is very accessible, except perhaps for the suspicious Tinicum Township police. However, it has long been a tradition to have a banquet and picnic at the Lazaretto at the beginning and end of the quarantine season, roughly June 1, and October 1. Yellow Fever shots are not required.
Psychiatry: Last Cow in Philadelphia
The present problem with PSYCHIATRY can be summarized as follows: At the suggestion of the American Hospital Association, Congress introduced the DRG system of paying for inpatients by diagnosis, rather than itemized services. It worked well except for psychiatry, where the diagnosis usually implies little relation to the later costs it generates, so an exception was made. The dual system of payment created loopholes which unfortunately overpaid psychiatric hospitals and were described as exploitation. Congress over-reacted in a way that was unsustainable, and essentially all of the psychiatric hospitals of the nation were forced to close. This is not a history for anyone to be proud of, and the lack of outcry is also a disappointment. However, after twenty years without reform, evidently, nothing is going to be done without an outcry.CONVENE BLUE RIBBON COMMISSION TO REPAIR PSYCHIATRIC INPATIENT CARE. The 1983 BRA switched hospital inpatient reimbursement to payment by diagnosis (DRG). Abuse of the psychiatric exclusion then led to "corrective" legislation which has essentially reduced American's psychiatric inpatient care to an underfunded national disappointment. The problem is not an easy one, so a commission should devise a workable methodology for psychiatric hospitals, relying neither on present approaches nor on DRG. But overpayment is a better outcome than no care at all. Homeless people sleeping in cardboard boxes on downtown steam grates are the consequence any visitor to the area can observe at night after the commuters go home. Psychiatric social workers readily recognize their daytime patients in the boxes.
* * * * *

|
| Daniel Blain, M.D. |
Daniel Blain, M.D. (1898-1981) was just about the most important psychiatrist in America. He was the Physician in Chief of the Institute of the Pennsylvania Hospital at 49th and Market, the first and in many ways the most prestigious psychiatric hospital before it was closed. Before that, he was the first Medical Director of the American Psychiatric Association, itself the first (1844) medical society in America. His fame rested on organizing the disorganized psychiatry of the Veteran's Administration into a chain of advanced "Dean's Hospitals", a huge and very important achievement. Before that, he had achieved considerable fame as the man who took the dilapidated State Psychiatric Hospitals with a reputation as "snake pits" and made them a respectable part of the medical community. And before that, he had been born in China as the son of missionaries. As a matter of fact, even before that, he was a descendant of General Mercer of Revolutionary War fame.
Dan was an outstanding example of the peculiar fact that Psychiatry was dominated by social upper crust psychiatrists in Philadelphia for a very long time. In fact, Benjamin Rush of the 8th Street branch of the Pennsylvania Hospital is known in some circles as the "Father of Psychiatry", while in other circles he is known for signing the Declaration of Independence. That isn't true in other cities, and it definitely isn't true in New York City, where the psychoanalytic school of Sigmund Freud took that city by storm, and essentially drove every other school of psychiatric thought out of town, out of medical schools, out of psychiatric hospitals. The famous sixteen-year psychoanalysis of Woody Allen is an example of the extremes of that fad. Every profession has petty civil wars of that sort, best left undiscussed in public. But in the case of psychiatry, it was indirectly a material contributor to the present disappearance of inpatient psychiatry, and the related appearance of lots of homeless people on steam grates. Let me give a biased view of what is a massive human tragedy, which someone else can "rectify" if he chooses.
|
| APA |
It starts with a Budget Reconciliation Act of the 1980s, which brought us the DRG (Diagnosis-related) system of paying for hospitalized patients. The idea was that appendicitis resulted in essentially 7 days in the hospital, give or take a couple of days, and the bills for admission for appendectomy were for more or less the same amount. If you had fifty or a hundred cases a year in your hospital, the high bills balanced the low bills, and the overall hospital reimbursement was essentially the same without itemizing the bandages and whatnot. Congress bought this package, and after it got going, just about all hospital bills were reimbursed at one of three hundred prices, the cost to the government was the same, and there was a whole lot less bookkeeping and accounting cost. It was a success, except for a few cases where the costs did not closely line up with the diagnosis, and psychiatric hospitals were where they concentrated. So, psychiatric hospitals were excluded, and psychiatric bills skyrocketed. This experience has been carelessly cited as an example of the evils of payment by service ("fee for service"), when in fact the duration of psychiatric hospitalization is related to features of the condition, like danger of suicide, rather than the diagnosis itself. Psychiatric leadership at the time contained many in a subset of physicians who did not think much of inpatient psychiatry in the first place and even less of lobbying, and they underestimated the severity of the assault on the specialty. Apparently, no workable formula for pricing inpatient psychiatry has since been brought forward to be approved by a Congress which is more accustomed to getting its lobbying in the form of one-liners. And would you believe it, psychiatric inpatient care soon disappeared.

|
| Pennsylvania Hospital |
That's right, if someone in your family needs psychiatric hospitalization, I wouldn't know where to tell them to get it -- at any price. From considerably overpaying for psychiatry inpatients to paying scarcely anything for them, this little change of the regulations caused every psychiatric hospital I know of by name, to close. It helped balance some state budgets, but it also was a considerable factor in filling the steam grates of American cities with people who sleep on cardboard boxes. And what it illustrates is that this is what political society always seemed to do, before Dan Blain and a small group of upper-crust psychiatrists were temporarily able to shame them into something better. In fact, if there is any tattered remnant of good inpatient psychiatric care left in America today, it is in the Veterans Hospitals that Dan was able to straighten out.
Dan Blain will probably eventually be bypassed as a curiosity, like his wife. She was a Wister Logan Blain, descended from families who ruled Philadelphia a hundred years before even General Mercer came along. So the Blain couple lived on an enormous farm plot, centered at 20th and Olney right next to LaSalle University, which is built on their property. It also contains the Peale House, where Charles Willson Peale lived as the elected president of the rebel faction of the American Revolution. Peale didn't know what he was supposed to do, so he resigned and painted portraits of people. The Blains enjoyed keeping a cow on their land, the last cow in Philadelphia, and the LaSalle students enjoyed stealing the cow and leaving it on the top floor of a dormitory, for laughs. Meanwhile, the Blain couple had cocktail parties on their front porch for visiting dignitaries. They usually wore blue jeans, and Mrs. Blain, the absolute Queen of Philadelphia society, was occasionally observed to pour vodka into her glass of beer. That sort of background may well have been useful when psychiatry needed to be built up and humanized, but it became a liability when the rest of inpatient psychiatry failed to appreciate what was knocking on its door.
Barnes Arboretum

|
| The Barnes Foundation |
If you want to live on City Line Avenue, safely in Montgomery County, you put your entrance on Latches Lane, which is parallel to City Line. It used to be said that the Barnes Foundation was next to Episcopal Academy, but that has moved further West, and St. Joseph's University now owns the property. When St. Joseph's decides what to do with the land, we can possibly describe a better landmark. The Barnes Foundation has always faced away from Philadelphia and is a little hard to find, all of which may have something to do with Dr. Barnes' strong dislike of the City.

|
| The Barnes Museum |
When you go there now, the old Museum is still there, but already showing signs of neglect. The house the Barnes family lived in is still, right next door. But it's harder to move an Arboretum than a group of paintings, so the Arboretum School, which was Mrs. Barnes' hobby, is still at the same place, likely to stay awhile. It's still a very nice place to visit, especially right at Labor Day when the very large Franklinia Trees are in full bloom. Like all Franklinia trees, these are direct descendants of the only example John Bartram was able to find, in Georgia or anywhere else.

|
| Medicinal Garden |
We're going to have to leave the decision to former Governor Rendell, about what you do with an empty museum since he is said to have had a lot to do with making it that way. We came to see the Arboretum.
The first thing which strikes you is that many of the big old trees are much older than the Barnes Foundation would have been. The brochure helpfully explains that a 19th Century tree fancier started it in 1880, and the Barnes acquired it in 1922. That still wouldn't account for a massive tree which is lying on the ground all cut up, opposite the Medicinal Garden. The base of the tree must be three or more hundred years old, so perhaps there was a grove of old oaks, just over the line of William Penn's city, which every owner tended carefully until the bugs got it. There are a considerable number of Chinese trees that look about right for 1880, but without a guide, it's pretty conjectural.

|
| Japanese Beetle |
Ever since someone imported the Japanese beetle along with some plants, to Moorestown, New Jersey, there have been laws prohibiting the importation of plants from abroad, but there must be some regulatory rigamarole which allows museums to do it. Korea and Japan are at the same latitude as Philadelphia, and the glaciers spared some ancient dinosaur food in those regions, so quite a few strange plants have come here from that source. Since the Barnes is a school, and since it only has a few acres, many if not most of the specimens in the gardens are one or two of a kind. That either means they have a feeder garden somewhere to store backups or a good relationship with government officials. Like all Arboretums, it attracts insects, so be prepared to do some swatting if you go. The school is said to be outstanding and quite conveniently located, but even just a stroll around is quite a nice way to spend a Sunday afternoon.
Specialized Surgeons

|
| Regina E. Herzlinger |
Local attitudes always somewhat persist among migrants from home. What's distinctive about the Philadelphia diaspora is how unconscious most of them are about still carrying the hometown mark. Philadelphia leaves a prominent birthmark, but it's sort of back between your shoulder blades and you forget it's there. What occasions this observation is a Christmas call from a prominent California surgeon who was once my roommate, back in the days when residents were actually resident in the hospital. More than fifty years ago Bill Doane also served as best man at my wedding. Our conversation turned to clots in the lung, and he related a story. He had once fixed a hernia for a 22-year old girl in the days when it was customary to keep hernia cases in bed for a while. Getting out of bed for the first time, she coughed and turned blue, suddenly on the edge of death. Taken back to the operating room, her chest was opened, and Bill removed a clot which was essentially a cast of the blood vessels of one entire lung. As surgeons like to say, she then did very well.
One doctor can tell such a story to another doctor in four sentences, while lay people who overhear it miss the whole point. The fact is, not one surgeon in ten thousand today could carry this off. Nowadays we train thoracic surgeons to open the lungs; they never repair hernias. Conversely, we train hernia surgeons to fix a dozen hernias daily through a little telescope; they never open a patient's chest. So it is hard to imagine many contemporary surgeons who could recognize this disastrous complication of hernia repair, then fix it themselves in time to rescue the patient. Although this disheartening decline into repetitive super specialties has been forty years in the making, it has been recently popularized with the general public by Regina E. Herzlinger, a Harvard business professor. Writing books and speaking to businessmen groups, she has popularized the proposal to outsource the general hospital into what she calls "focused factories." She rightly characterizes the medical profession as reluctant. She's a nice person, and undoubtedly sincerely believes focused factories will save money, improve quality. But we must not let this idea take hold.

|
| Pennsylvania Hospital |
Specialty hospitals have actually been given more than a fair trial. About a hundred years ago, the landscape was peppered with casualty hospitals, receiving hospitals, stomach hospitals, skin and cancer hospitals, lying-in hospitals, contagious disease hospitals, and a dozen other medical specialty boutiques. With a few notable exceptions, they all failed for the same reason. Sooner or later they found they could not adequately service their specialty without the backup of a full hospital service. Children's hospitals do thrive, but they have patients who are generally of the wrong physical size to fit adult hospital facilities and equipment. There are plenty of things to regret about general hospitals' design, but the inescapable fact is they all must have a very wide range of services to perform any mission, no matter how discrete. It would be still better if the doctors had an equally wide range of skills in their own heads, but the avalanche of innovation and lawsuits has forced sub-specialization, compartmentalizing, and narrowness of viewpoint. Circumstances have forced the profession to hunker down, but that trend must be resisted, not celebrated.
The instant and successful repair of pulmonary embolism make a dramatic illustration, but the reasons for broad medical training are more extensive than that. In the first place, it is much cheaper to use the generalist office than to bounce people to a gastroenterologist for heartburn, a psychiatrist for anxiety, and a dermatologist for pimples. The American employer community is desperate for a way to reduce its burden of employee health costs, and flocks back to their nurturing business schools for advice. They would do better to seek repeal of the tax dodges which tempted them into their present muddle, of course. But in any event, they must be persuaded to recall the disaster of managed care and at least, avoid meddling in hospital design.
That's the cost issue, where specialization surely raises costs. Constant repetition of the same procedure seems superior to first-time fumbling, although it is questionable how long it takes a well-trained surgeon to pick up a new procedure and do it well. But for this system to work, the referring physicians need to be more skillful, not less, in choosing a good one to refer to. There's just nothing like the experience of working for a few weeks in the specialty as a rotating intern, to tell you what to look for and what to avoid. If every doctor in a hospital is making a dozen internal referrals a day, the cumulative effect on the quality of the whole institution is dramatic -- when they have had sufficient past involvement in the specialties to which they now only refer patients. Some specialists will become popular and rich; others will sulk around unnoticed for a while, then go elsewhere. This process, of course, occurs everywhere; what's institutionally distinct is the culture underlying the standards for preferences.
We'll talk later about the Doane brothers of Bucks County, who were judged to be too handsome to hang. Right now, the point of this story can be summarized by the old Pennsylvania Hospital adage, that you must first be a good doctor before you can be a good specialist. Not only was the Pennsylvania Hospital the first in the nation. For sixty years it was the only hospital in the nation, and for decades after that, it was the only hospital in Pennsylvania. In medical history circles, it is said that the history of American medicine, is the history of the Pennsylvania Hospital.
| Posted by: Janet | May 8, 2013 10:37 PM |
| Posted by: Oklahoma doctor INTEGRIS Baptist | Jan 23, 2013 12:19 PM |
47 Blogs
Nation's First Hospital, 1751-2016
The nation's oldest hospital changed more from 1948 to 2016 than it did from July 4. 1776 to 1948.
A Toast to Doctor Franklin
The Franklin Inn annually toasts three doctors. Even though Ben never went past second grade, his medical contributions are the most illustrious of the three. One of the most remarkable men who ever lived.
Dr. Cadwalader's Hat
Sometimes it's hard for others to understand what makes Quakers tick.
July 4, 1776: Patients in the Pennsylvania Hospital on Independence Day
Patients in Pennsylvania Hospital on Independence Day, 1776.
America's First Medical Interne, Jacob Ehrenzeller
The contract between the Pennsylvania Hospital and its resident physicians in 1773 has seemed a little quaint, but only since 1965, when Medicare made it possible to pay them.
The Kappa Lambda Society of Hippocrates
The Secret Origins of the American Medical Association
Lumpers In Constant Combat With Splitters
 The home dinner table is no longer the place most families teach the rules of conduct to each other, probably because of the invasion of homes by television. But there are places where friendly debate is still conducted and social issues are settled. In Philadelphia, newcomers are still taught what's what, in this manner.
The home dinner table is no longer the place most families teach the rules of conduct to each other, probably because of the invasion of homes by television. But there are places where friendly debate is still conducted and social issues are settled. In Philadelphia, newcomers are still taught what's what, in this manner.
A Toast To Silas Weir Mitchell, MD
Philadelphia medical scene, and the literary one.
Eakins and Doctors
Philadelphia's art world joined its medical world in reacting fiercely to Jefferson Medical College's sale of the best painting by the best artist of Philadelphia's Nineteenth century.
Link to:Medical Club of Philadelphia
In 1992, it's Executive Director summarized the century-long history of this last surviving club of physicians, devoted exclusively to non-medical affairs.
Medical Club of Philadelphia, Appendix B, Membership
..... Recruitment of membership was an instantaneous success during the Gilded Age and rose to a peak in the early years of the Great Depression of the 1930s. After that, interest in membership steadily declined. Excursions on private trains and dinners with the U.S. President were no longer within their means.
Recruitment of membership was an instantaneous success during the Gilded Age and rose to a peak in the early years of the Great Depression of the 1930s. After that, interest in membership steadily declined. Excursions on private trains and dinners with the U.S. President were no longer within their means.
Appendix D, Presidents of the Club
.... Although some of these names seem unfamiliar to the modern public, rest assured they were widely considered the cream of the crop by the profession, at the time.
A Toast To J. William White, MD
Franklin Inn holds the J. William White dinner every year on Benjamin Franklin's birthday. A surgeon, author, politician, athlete, cavalryman, and duelist, Bill was a real Philadelphia gentleman.
Victor Rambo, Indian Eye Surgeon
A twelfth-generation Philadelphian devoted his life to restoring eyesight to thousands of poor people in India.
Emperor's Doctor
Almost trapped by the events at Pearl Harbor of which he had advance knowledge, this Pennsylvania Hospital intern rose to the top of Japanese medicine.
Discipline for the Disciple
America
Mind Your Manners
The surgeon father of a local congressman once learned a hard lesson.
Funny Toes: A Physician Viewpoint
Most people either ignore funny toes, or hide them in their shoes. Here are one doctor's idle thoughts about them.
Albert C. Barnes, M.D.
Impressionist paintings grew more valuable, faster than the patron's endowment for their maintenance.
The Barnes Foundation: Comments on the Economics of Art (2)
Well chosen fine art will appreciate in value over time. If a museum's endowment doesn't grow at the same rate to maintain it, eventually some of the art will have to be sold.
Harry C. Bishop 1921-2009
The Right Angle Club of Philadelphia mourns the loss of a valued member.
Philadelphia Chromosome
Just about everybody has 46 chromosomes in every cell in the body. Some people have more than that: they have the Philadelphia Chromosome.
Kenneth Gordon, MD, Hero of Valley Forge
This soft-spoken child psychiatrist was mainly responsible for keeping real estate developers from building houses all over the Valley Forge encampment.
Community Volunteers in Medicine
A little group of medical volunteers in Pennsylvania's Chester County may not understand the underlying issues very well, but they just pitch in and do what they can about the medically underserved.
Hospital Elevators
There are never enough elevators in any hospital; all ranks and classes meet in them; they are forever breaking down.
Atlantic City, Brigantine and the N.I.H.
Great scientists in crowds look and act pretty much like everyone else.
Avian Footnote
Compiling the index of a book is a tedious, difficult, and unrewarded task.
House that Love Built: Ronald McDonald of Philadelphia
The idea of a temporary residence for patients and their families near a children's hospital came from Dr. Audrey Evans of Philadelphia. Initial fundraising was driven by Fred Hill of the Philadelphia Eagles. In 25 years, over three hundred others in 26 nations have independently taken up the idea.
Contemporary Germantown
"Well," said Bockus, "Every famous surgeon I know, has a house on an island, somewhere. Where's your island?".
Furniture for the Horse Country
Fine art is generally the product of rich people demanding something special from a nearby artisan community. Furniture making in Chester County is sort of like that.
Baruch Blumberg, Renaissance Man
Winners of a Nobel Prize are sometimes strange birds. The majority are charming and affable. But Baruch Blumberg has the unusual distinction of being a rollicking extrovert.
Nobel Prize: Michael Brown, MD
A locally trained Philadelphia physician has won the Nobel Prize in Medicine for saving millions of lives with the "statin" drugs.
National Business Coalition on Health
The NCOH was founded in 1992, at the time of the Clinton Health Plan. The national body is headquartered in Washington, coordinating seventy or so state and local coalitions of businesses that are paying for employee health care.
Picking Up the Usual Suspects
When the U.S. President plans to change health care, everyone involved in healthcare gets excited. Some want to resist change, some want to exploit it, but everyone wants to have influence.
Hold the Presses
The Clinton Health Plan was dead on arrival, but the media didn't know that.
Nowheres-ville
 After the Clinton Health Plan faded, but before new ones emerged, participants thought it safe to talk to graduate students studying the event. What emerges is a picture of big business pulling the plug.
After the Clinton Health Plan faded, but before new ones emerged, participants thought it safe to talk to graduate students studying the event. What emerges is a picture of big business pulling the plug.
What To Do If You Have a Heart Attack
 In May, I had a coronary occlusion, and a fast trip to the Pennsylvania Hospital. Cardiac catheterization opened the artery with a stent before there was time for infarction.
In May, I had a coronary occlusion, and a fast trip to the Pennsylvania Hospital. Cardiac catheterization opened the artery with a stent before there was time for infarction.
Madeira Party 2009
In Colonial America, Madeira was what the upper crust drank.
Equal Pay for Equal Work
Sometimes the representatives of political interest groups try, just a little too hard.
Health Maintenance Organizations (HMO)
Paul Ellwood gets credit for inventing the term HMO, and for selling a version of it to large employers, as well as the Clinton Administration. It's been a bumpy ride.
Block Captains
A remarkable group of volunteers look out for their neighbors.
Three-Mile Island
An ominous-looking nuclear energy plant developed some sort of difficulty, a few miles from the State Capital of Harrisburg. The direct effects were minor, but the political and psychological ones have endured for half a century.
Governor Keith's House
 Just off Route 611 adjoining the Willow Grove Air Station, and on the County Line Road between Montgomery and Bucks County, is the summer estate of Sir William Keith, Lieutenant Governor of Pennsylvania from 1717 to 1726. Well worth a visit. Locally, it is called Graeme Park.
Just off Route 611 adjoining the Willow Grove Air Station, and on the County Line Road between Montgomery and Bucks County, is the summer estate of Sir William Keith, Lieutenant Governor of Pennsylvania from 1717 to 1726. Well worth a visit. Locally, it is called Graeme Park.
Lazaretto
The oldest quarantine station in the Western hemisphere is located next to the airport on Tinicum Island, quite easily visited by car. It dates from Philadelphia's famous Yellow Fever epidemics of 1793.
Psychiatry: Last Cow in Philadelphia
Daniel Blain, just about the most famous psychiatrist in America, lived at 20th and Olney, West. Not only was that the place he lived, but he also kept a cow there. And this was within living memory.
Barnes Arboretum
The Barnes impressionistic art has moved to the Parkway in Philadelphia, where Dr. Barnes said he never wanted it to be, But the Arboretum remains on Latches Lane in Merion, just across City Line Avenue, next to where Episcopal Academy used to be, and now is occupied by St. Joseph's.
Specialized Surgeons
Specialty hospitals have actually been given more than a fair try. About a hundred years ago, the landscape was peppered with casualty hospitals, receiving hospitals, stomach hospitals, skin and cancer hospitals, lying-in hospitals, contagious disease hospitals, and a dozen other medical specialty boutiques.