6 Volumes
Philadelphia Medicine
Several hundred essays on the history and peculiarities of Medicine in Philadelphia, where most of it started.
Sociology: Philadelphia and the Quaker Colonies
The early Philadelphia had many faces, its people were varied and interesting; its history turbulent and of lasting importance.
Medicine
New volume 2012-07-04 13:34:26 description
Health: Philadelphia
New volume 2014-08-04 22:18:40 description
Pre-Revolutionary Ben Franklin
Poor Richard was able to retire at the age of 42, and spent the rest of his life as a rich man, dying at the age of 82 with an eye-popping estate.
Surviving Strands of Quakerism
Of the original thirteen, there were three Quaker colonies, all founded by William Penn: New Jersey first, Pennsylvania biggest, and Delaware so small Quakerism was overcome by indigenous Dutch and Swedes.
Philadelphia Medicine
The first hospital, the first medical school, the first medical society, and abundant Civil War casualties, all combined to establish the most important medical center in the country. It's still the second largest industry in the city.
Nation's First Hospital, 1751-2016

|
| Pennsylvania Hospital |
As commonly stated in medical history circles, the history of the Pennsylvania Hospital is the history of American medicine. The beautiful old original building, with additions attached, still stands where it did in 1755, a great credit to Samuel Rhoads the builder and designer of it. The colonial building on Pine Street stopped housing 150 patients around 1980, supposedly at the demand of the Fire Marshall, although its perpetual fire insurance policy still owes the hospital several thousand dollars a year as an unspent premium dividend. There may have been one small fire during two centuries of use, but its true fire hazard would be difficult to assert. It was just out of date. The original patient areas consisted of long open wards, with forty or so beds lined up behind fluted columns, in four sections on two floors. The pharmacy was on the first floor, the lunatics in the basement, and the operating rooms on the third floor under a domed skylight. It was entirely serviceable in 1948 when I arrived as an intern doctor. Individual privacy was limited to what a curtain between the beds would provide, but on the other hand, it was possible for one nurse to stand at the end of the award and recognize any distress among forty patients immediately. In this trade-off between delicacy and utility, the utility was certain to be preferred by the Quaker founders. Visitors were essentially excluded, and if a patient recovered enough to be unnaturally curious about neighboring patients, well, he had probably recovered enough to go home.
Located between two large rivers, South Philadelphia up to ten blocks away was essentially a swamp until the Civil War. So, there were seasonal epidemics of malaria, yellow fever, typhoid, and poliomyelitis at the hospital until the early twentieth century. Philadelphia was a port city, so sailors brought in cases of venereal disease, scurvy, even an occasional case of anthrax or leprosy. During the Industrial Revolution of the nineteenth century, tuberculosis, rheumatic fever, and diphtheria were part of clinical practice. But underlying the ebb and flow of environmental effects, there was a steady population of illness which did not change a great deal from 1776 to 1948. These patients were all poor, because the rules in Benjamin Franklin's handwriting restricted service to the "sick poor, and only if there is room, for those who can pay." In 1948 there was a poor box for those who might feel grateful, but no credit manager or official payment office. The matter had been considered, but the cost of collection was considered greater than the likely revenue. When Mr. Daniel Gill was offered the position as the hospital's first credit manager, it was suggested that he be given a tenth of what he collected. To his lifelong regret, Dan Gill regretted that he refused an offer that he had felt he could not afford to accept.
So, the wards were filled with victims of the diseases of poverty, punctuated by occasional epidemics of whatever was prevalent. And a second constant feature of the patients was their medical condition forced them to be housed in bed. For centuries, physicians dreaded the news that a new patient was being admitted with "dead legs".
Franklin Crown Soap

|
| Benjamin Franklin |
It's easy to make soap, but hard to make good soap. You just boil animal fat with wood ashes, and you get soft soap. Softsoap was sold by the barrel in the Colonies. Hard soap is made by adding salt to the mix, allowing it to be sold by the bar. The trick to all this is to know how long to boil it, how much ash of what kind, and how much salt. If you get it wrong it will be too soft or too hard, and if you have too much lye from the ashes, it will burn your skin when you wash with it. Most people made their own soap in the colonies, so they often got it wrong, because they didn't exactly know what they were doing. What they were doing was called Saponification, after the old Roman hill of Sapo. The legend is that burnt animal sacrifices in the Temple at the top of the hill would wash down and help the washerwomen in the river below get their clothes clean. The point of all this is that Josiah Franklin, the father of Benjamin and sixteen other children, was a candle maker and a soap boiler. Somehow he got the recipe right, particularly the part about adding salt, and made famously fine bars of soap with a crown stamped on them -- Crown soap. The formula was a strict family secret, the source of family discord when one sister let it out.
The point which needs reflection is that nobody in Franklin's family ever heard of potassium hydroxide, saponification, triglycerides or fatty acids. The process of achieving fame throughout the colonies -- for making a product everyone could make haphazardly -- must have involved a careful series of experiments with different fats, tallows and lards, with different amounts of ashes of various trees, and different amounts of salt. When you got it right it worked consistently, but it would have been necessary to make many experiments to get it right. To avoid repeating the same mistakes, it would be necessary to keep careful records. In other words, little Benjamin must have observed a great many examples of experimental chemistry which made him a chemist fit to talk with Lavoisier and Priestly on equal terms, even though he quit school after the second grade. His childhood was one long demonstration of a motto of Claude Bernard: "Experiment first, a theory later."
Pembertons
|
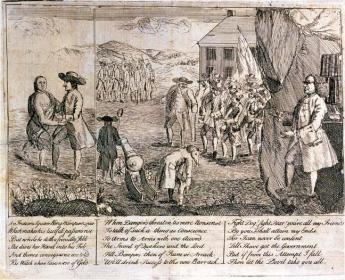
| Israel Pemberton, Ben Franklin satire l |
Ralph Pemberton was an English Quaker well before 1650; he may have been a Quaker before William Penn was one. As an old man, he accompanied his son Phineas to Pennsylvania in 1682. They established a farm on the banks of Delaware in Bucks County called Grove Place, and Phineas soon became one of the chief men in the colony. In the next generation, Israel Pemberton became one of the best educated, richest merchants in the colony. But it was Israel's son also called Israel, who earned the title of King of the Quakers. He was one of the founding Managers of the Pennsylvania Hospital along with Benjamin Franklin and one of his brothers, James Pemberton, and was a generous philanthropist and leader of a number of other civic organizations. Just exactly what provoked his famous political disputes with Franklin is not clear, but he was a leading friend of the Indians, whom Franklin never much liked. Israel Pemberton strongly and effectively argued William Penn's policy of friendship with the Indians, particularly insisting that sales of land to colonists should be prevented until there was a clear agreement with the Indians about the ownership. Unfortunately, pressures built up as Europeans immigrated faster than this policy could accommodate smoothly, and Franklin mostly sided with the impatient immigrants -- and squatters. This disagreement came to a head in 1756 when Pemberton negotiated a treaty of peace with the Indians at a conference at Easton. Although this treaty seemed to settle matters, it came against a background of the descendants of William Penn abandoning Quakerism. They, however, remained the proprietary owners of the Province with a more narrow focus on speeding up land sales to maximize their investment. Much of the internal dynamics of these quarrels before the Revolutionary War remain unclear and possibly somewhat misrepresented.

|
| Shenandoah Valley |
When the Revolution came, Pemberton viewed it with disfavor, mostly for pacifist rather than purely Tory reasons. Feelings ran high since the Pembertons were influential citizens with the potential to dissuade wavering neighbors, which made it difficult to tolerate them as invisible bystanders. However that may be, the three Pemberton brothers and twenty other wealthy and influential Quakers were arrested and, without hearing or trial, thrown in the back of an oxcart and sent into exile in Virginia for eight months. Their journey was a curious one, along a trail up the Schuylkill to the ford at Pottstown, and then down the Shenandoah Valley, an area in which they were well known and highly respected, greeted with great sympathy as they traveled. Isaac's brother John, who had spent several years as a missionary, died during this exile.
|
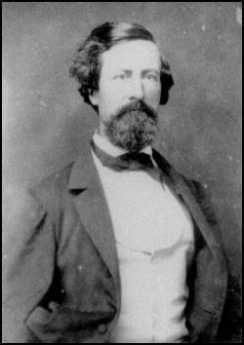
| John Clifford Pemberton |
In some ways, the most curiously notable Pemberton was John Clifford Pemberton, who applied to West Point on his own initiative and was appointed by Andrew Jackson who had been a friend of his father. In itself, it is curious that so combative a person and so vigorous an enemy of the Indians -- as Jackson certainly was -- would have Quaker friendships. But he did not misjudge John Clifford, who became a diligent professional warrior for his country in a number of military incidents with the Indians, the Mexicans, and the Canadians, rising to the rank of captain in the regular Army at the opening of the Civil War. In spite of personal efforts by General Winfield Scott to dissuade him, he resigned his commission and volunteered in the Confederate army. He was quickly promoted to major, then a brigadier general and eventually to Lieutenant General. As such, he was the commanding Confederate officer at the fifty-day siege of Vicksburg where he was finally forced to surrender to Grant's army. In a prisoner exchange, he was returned to the Confederate side, which they had no openings for Lieutenant Generals. He resigned and re-enlisted as a common soldier, but was quickly promoted to the rank of Colonel, in charge of the artillery at the final siege of Richmond. After the war, he became a farmer in Warrenton, Virginia, but was visiting at the family home in Penllyn when he died in 1881. John Clifford Pemberton, the highest-ranking general on the grounds, lies buried in Laurel Hill cemetery right next to Israel Pemberton. In some sort of triumph of the South, he here out-ranks George Gordon Meade, the hero of Gettysburg. Just how his pacifist family reconciled itself to his heroism can only be imagined.
A Toast to Doctor Franklin
|
|
| Benjamin Franklin |
Benjamin Franklin's formal education ended with the second grade, but he must now be acknowledged as one of the most erudite men of his age. He liked to be called Doctor Franklin, although he had no medical training. He was given an honorary degree of Master of Arts by Harvard and Yale, and honorary doctorates by St.Andrew and Oxford. It is unfortunate that in our day, an honorary degree has degraded to something colleges give to wealthy alumni, or visiting politicians, or some celebrity who will fill the seats at an otherwise boring commencement ceremony. In Franklin's day, an honorary degree was awarded for significant achievements. It was far more prestigious than an earned degree, which merely signified adequate preparation for potential later achievement.
And then, there is another subtlety of academic jostling. Physicians generally want to be addressed as Doctor, as a way of emphasizing that theirs is the older of the two learned professions. A good many PhDs respond by rejecting the title, as a way of sniffing they have no need to be impostors. In England, moreover, surgeons deliberately renounce the title, for reasons they will have to explain themselves. Franklin turned this credential foolishness on its head. Having gone no further than the second grade, he invented bifocal glasses. He invented the rubber catheter. He founded the first hospital in the country, the Pennsylvania Hospital, and he donated the books for it to create the first medical library in the country. Until the Civil war, that particular library was the largest medical library in America. Franklin wrote extensively about gout, the causes of lead poisoning and the origins of the common cold. By inventing bar soap, it could be claimed he saved more lives from the infectious disease than antibiotics have. It would be hard to find anyone with either an M.D. degree or a Ph.D. degree, then or now, who displayed such impressive scientific medical credentials, without earning -- any credentials at all.
July 4, 1776: Patients in the Pennsylvania Hospital on Independence Day
According to the records of the Pennsylvania Hospital, the following 48 persons were patients in the hospital on July 4, 1776:
| Richard Brinkinshire (Admitted 11/15/1775) | John Ridgeway (Admitted 12/26/1775) |
| James Chartier (Admitted 1/6/1776) | patient (Admitted 1/6/1776) |
| patient (Admitted 1/20/1776) | patient (Admitted 1/20/1776) |
| Mary Yell (Admitted 2/7/1776l) | John Beckworth (Admitted 2/7/1776) |
| Bart. McCarty (Admitted 2/10/1776) | John King (Admitted 2/10/1776) |
| Robert Alden (Admitted 2/17/1776) | William Patterson (Admitted 3/6/1776) |
| Elizabeth Hanna (Admitted 3/9/1776) | John McMahon (Admitted 3/13/1776) |
| Mary Burgess (Admitted 3/23/1776) | Mary Anderson (Admitted 4/10/1776) |
| John Hatfield (Admitted 4/15/1776) | Eliza Haighn (Admitted 4/17/1776) |
| Charles Whitford (Admitted 4/24/1776) | patient (Admitted 5/8/1776) |
| Susanna Carrington (Admitted 5/8/1776) | patient (Admitted 5/8/1776) |
| William Johnson (Admitted 5/13/1776) | Lazarus Chesterfield (Admitted 5/22/1776) |
| Mary Spieckel (Admitted 5/22/1776l) | William Edwards (Admitted 5/22/1776) |
| patient (Admitted 5/23/1776, Lunatic) | Jane White (Admitted 5/25/1776) |
| Charles McGillop (Admitted 5/29/1776) | ---Fitzgerald (Admitted 6/1/1776) |
| Michael Rowe (Admitted 6/6/1776) | patient (Admitted 6/6/1776) |
| John Hughes (Admitted 6/12/1776) | Joseph Smith (Admitted 6/15/1776) |
| Esther Munro Lunda (Admitted 6/15/1776) | Mathew Coope (Admitted 6/19/1776) |
| Anne Patterson (Admitted 6/19/1776) | Thomas Savoury (Admitted 6/20/1776) |
| Rebecca Winter (Admitted 6/26/1776) | Elizabeth Manning (Admitted 6/26/1776) |
| Negro (Admitted 6/24/1776) | Elex. Scanvay (Admitted 6/24/1776) |
| Fanny Stewart (Admitted 6/24/1776) | Peter Barber (Admitted 6/29/1776) |
| Catherine Campbell (Admitted 6/29/1776) | Ann McGlauklin (Admitted 7/3/1776) |
| Elizabeth Lindsay (Admitted 7/3/1776) | Ann Jones (Admitted 7/3/1776) |
The records indicate the following diseases were the reason for admission of those patients. Although in Colonial times there was no medical delicacy to avoid offending readers, present privacy standards require that we strip the diagnoses from the name of the patient and list them independently. There is some overlap, sometimes making it difficult to judge which disorder caused the admission.
- Sore, poisoned or ulcerated legs: 16 cases
- Lunacy, mind or head disorders: 10 cases
- Syphilis: 7 cases
- Fever and Rheumatic fever: 7 cases
- Dropsy: 5 cases
- Gunshot: 4 cases
- Diabetes: 1
- Blindness with clear pupil: 1
- Spitting blood: 1 case
- Dislocated arm: 1 case
- Inflammation of face: 1 case
- Scurvy: 1 case
- broken arm: 1 case
The following physicians were elected at the Managers Meeting dated 5/13/1776:
- Dr. Thomas Bond
- Dr. Thomas Cadwalader
- Dr. John Redman
- Dr. William Shippen
- Dr. Adam Kuhn
- Dr. John Morgan
The First and Oldest Hospital in America

|
| South East Prospect of Pennsylvania Hospital |
There is a painting of the region around 8th and Spruce Streets in the 1750s, depicting a pasture, with cows, and three or four buildings between 8th and 13th Streets. When the Pennsylvania Hospital moved there in 1755 from its temporary location in a house located a block from Independence Hall, there were complaints that it was now located so far out in the woods that it was difficult and dangerous to go there. Still another description of the area is evoked by the provision which the Penn family placed in the deed of gift of the land, strictly forbidding the use of the land as a tannery. Tanneries have always been notorious for giving off noxious odors, so most people wanted them to be somewhere else, anywhere else. In any event, the main activity of Penn's "green country town" at that time was concentrated closer to the Delaware River, and the nation's first hospital was definitely placed in the outskirts. Two blocks further West the almshouse was already in place, but not much else. We are told that Benjamin Franklin had flown his Famous Kite at 9th and Chestnut, using a barn there to store his materials. It might be recalled that the population of Philadelphia, although the second largest English-speaking city in the world, was only about twenty-five thousand inhabitants at the time of the Revolution, and in 1751 was even smaller.
In any event, the first and oldest hospital in America was built on 8th Street between Spruce and Pine, and the Eighteenth Century buildings on Pine Street still present a breathtaking view at any season, but particularly in May when the azaleas are in bloom, and fragrance from the flowering magnolias fills the evening atmosphere for blocks around. Although some people today mistake the Pennsylvania Hospital for a state hospital, it was founded in the reign of George II, decades before there was such a thing as the State of Pennsylvania. The Cornerstone was laid by Benjamin Franklin, with full Masonic rites. Most doctors regard a hospital as a mere workshop, but the affection with which many Pennsylvania physicians regarded their special hospital is indicated by the number who have requested that their ashes be buried in the garden.
For two hundred years, beginning with the first American resident physician Jacob Ehrenzeller, the interns and residents were paid no salary, so they had to live on the grounds. An Internet was just that, interned within the four walls for at least two years. Because the resident physicians had no money, they stayed in the hospital at night and on weekends, playing cards and swapping stories. The hospital was home for them, as it was for the student nurses, likewise unpaid but more strictly confined and supervised. This penury seemed acceptable because the patients were mostly charity ward patients, otherwise unable to pay for their own care. Ehrenzeller finished his medical apprenticeship and went to practice for many decades in the farm country of Chester County, but gradually upper-class Philadelphia moved from 4th Street westward to and beyond the hospital, and two of the richest men in American history, Morris and Biddle, had houses within a block of the hospital, although Morris never lived in his house, having more pressing matters in debtor's prison. Therefore, later resident physicians at the hospital had the potential of setting up a private practice in the area and becoming society doctors as well as academically prominent ones. Being a charity hospital in a rich neighborhood created the potential for volunteer work by the town aristocrats and large bequests for charity. The British housed their wounded in the hospital during the Revolutionary War and shot deserters against the red brick wall of the small cemetery to the north. A century later, there were a couple of dozen rooms for private patients in the hospital for the convenience of the doctors and the neighbors, but everyone else was a charity patient. And a century after that, the hospital still did not have an accounting department to collect bills and tended to regard people who asked for a bill as a nuisance. Benjamin Franklin is regarded as the Founder of the hospital, and his autobiography famously describes how he fast-talked the legislature into matching the donations of the public, not mentioning to them that he had already collected enough promises to see the project through. This seems in character; Franklin's biographer Edmond Morgan summed up that, "Franklin doesn't tell us everything, but what he does tell us, is straight." The idea for the hospital was that of Dr. Thomas Bond, whose house is now a bed and breakfast on Second Street, but it was characteristic of Franklin to be the secretary of the first board of managers of the hospital. In Quaker tradition, the clerk of a meeting is the person who really runs the show. It thus comes about that the minutes of the founding board were recorded in Franklin's own handwriting, among them the purpose of the institution, which is to care for the Sick Poor, and if there is room, for Those Who can pay. This tradition and this method of operation continued until the advent in 1965 of Medicare when charity care was displaced by concepts which the nation had decided were better. The Pennsylvania Hospital was not only the first hospital but for many decades it was the only hospital in America. Its traditions, sometimes quaint and sometimes glorious, cast a long shadow on American medicine.
REFERENCES
| America's First Hospital: The Pennsylvania Hospital 1751-1841 William Henry Williams Ph.D. ISBN-10: 0910702020 | Amazon |
Pennsylvania Prison Society

|
| Duke of York |
William Penn, who spent considerable time in British prisons, established a penal code for his new colony which largely swept away the draconian punishments established by the code of the Duke of York. Until as late as 1780, jails were mainly confinement hotels for debtors, prisoners awaiting trial, and witnesses. For actual punishment, the methods were execution and flogging. Penn's Code for Pennsylvania restricted execution to the crime of murder, and flogging to sexual offenses; everything else was punished by fines and imprisonment. Hidden in this code, of course, was the need to invent and construct prisons to service the imprisonment. It would take over a century to address this need, and Philadelphia still has not completely caught up with the need for more prison cells. Without a prison system, the Penn code was impractical, and the colonial penal code retrogressed toward floggings, pillories, and hangings after Penn's death.
|
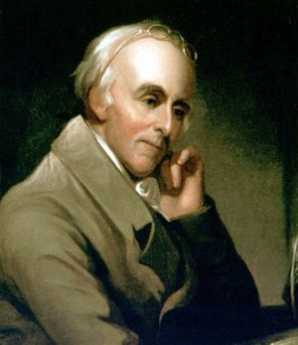
| Dr. Benjamin Rush |
In colonial Philadelphia, the main prison was on Walnut Street, with sixteen cells. A neighboring Quaker, Richard Wistar, started a soup kitchen in his own home, taking the soup over to prisoners. By 1773, he had established the Pennsylvania Society for Assisting Distressed Prisoners, which was unfortunately disbanded by the occupying British Army in 1777. In 1783, Dr. Benjamin Rush with the assistance of Benjamin Franklin, Bishop White, and the Vaux family, founded the Philadelphia Society for Alleviating the Miseries of Public Prisons, which after a century changed its name to the Pennsylvania Prison Society. The Prison Society believes it is the oldest continuous non-profit society in America.

|
| Eastern State Penitentiary |
The Prison Society has had several major changes in direction. The original concept was to substitute public labor for imprisonment, a less costly arrangement than imprisonment while avoiding a return to floggings and dismemberment. However, the degrading sight of prisoners in chain gangs caused a public outcry, and the approach was abandoned. In the spirit of the French and American revolutions, loss of liberty was seen as the greatest punishment conceivable. Added to this was the Quaker concept of inspiring remorse through silent meditation, and the eventual outcome was the construction of the Eastern State Penitentiary on what was then called Cherry Hill. In 1823, it was ominous that Eastern State Penitentiary was the largest structure in America. Although the concept was widely admired and imitated, the prolix Charles Dickens took a violent dislike to the idea of never talking to anyone, and led a reversion away from penitentiaries back to simple prisons. In the days before Alzheimers and schizophrenia were well characterized, the spectacle of massive recidivism was added to the rumor that protracted solitude led to insanity.

|
| Catherine Wise |
From Catherine Wise the Communications Director of the Pennsylvania Prison Society, the Right Angle Club recently learned that the current evolution of the American penal system has led to a steady state, but a troubled one. There are 2.2 million inmates in American prisons today, more than any other nation including Russia and China. Of these, 75,000 are confined in Pennsylvania, 9,000 in Philadelphia. Recidivism is 67%, the cost is $31,000 per year per inmate, the majority of inmates have been involved with illicit drugs, a growing number are infected with HIV and Hepatitis C, mental illness runs around 20%. The cost of incarceration is growing faster than the cost of either education or healthcare for the community. Prison overcrowding is extremely serious, the programs for managing parole and integration back into society are weak and underfunded. Eighty percent of the inmates are non-white, most prisons are located in remote regions too far for easy visiting, medical care in prison would not seem at all acceptable in general society. The Prison Society has no difficulty finding projects which are urgently needed. Just for an example, take the peculiar prison statistics; it really seems improbable that only 9,000 of the 75,000 Pennsylvania prisoners are in Philadelphia. Then reflect, NIMBY, that no one wants a prison or its visitors near his home, except areas of rural poverty welcome the employment a prison brings. Reflect for a moment that "jails" are paid for by local county taxes and contain prisoners with less than two years to serve. "Prisons" are paid for with state taxes, and contain those sentenced to longer than two years. Finally, add the fact that nonvoting Philadelphia prisoners in rural prisons are counted by the census as residents of the rural area for the purpose of distributing legislative and congressional seats. The rural politicians love the system, the urban neighbors love to be rid of the prison environment, but the prisoner families can't visit the prisoner. Who cares? Who even notices?
During the first World War, Quaker interest in prison matters was greatly stimulated by the imprisonment of many Quaker conscientious objectors to the wartime draft; since that time prison conditions have again become a central interest of the religion. It's hard to prove but is confidently asserted, that violence and mistreatment of prisoners are appreciably less in Pennsylvania than the rest of the country, California for example. In any event, The Pennsylvania Prison Society is a particularly effective advocate for humane treatment because of credibility achieved over two centuries, with newspaper editors on its board, and sympathetic affiliations with the legislative judicial committees. It knows what it is talking about, as a result of over 5000 annual prison visitations, and it has served the prison administrative corps by performing volunteer work, accepting contracts for parole projects, arranging bus trips for prisoner families to remote prisons, and working for improved funding for prisons. At the moment, there are six highly imaginative bills before the Pennsylvania Legislature, devised and researched by this outside organization with credibility, and political clout. Although the Society takes an occasional contract for a project, it is itself entirely funded by outside contributions, and because of occasional adversarial situations, asks for no funds from the state. Even the contract funds have been questioned, and are only accepted when the working relationships fostered are more useful for the prisoner clients than any co-option which might result.
One final word about medical care in prison. It's not as good as medical care for non-prisoners, and unfortunately it probably never can be. The remote rural location of prisons makes it difficult to obtain physicians and nurses, regardless of wage levels. It's dangerous to be around prisoners, as any guard will tell you, and it's more dangerous to be in control of narcotics amidst a population of addicted convicts. Malingering is nearly universal, both to obtain desired drugs and to spend "easy time" in the infirmary. Many prison escapes are engineered around the necessarily weakened security of the medical system. The prison budgeting system has all the rigidity and weaknesses of any governmental medical system, and in this case, it's run far out of sight of the public. Even the bureaucrats in charge are victimized by other bureaucrats. The average duration of incarceration in Pennsylvania is longer than in most other states; the prisons have to keep mental patients because the mental hospitals have all been closed. Fifty years ago, when there was no place to put a non-criminal with tuberculosis, he was put in jail. The parole system is underfunded, there is not nearly enough community support to absorb ex-con. Behind all this is a shortage of prison facilities. The legislature has got itself into a position that if it moved more prisoners into the outside, more prisoners would just fill the vacancies, costs would go up, and things wouldn't look much better. Only after the backlogs have been absorbed, would there be much visible effect.
Germantown Nurses the Yellow Fever, 1793

|
| Yellow Fever, Phila |
The French Revolution continued from 1789 to 1799 and created the opportunity for a second revolution in the New World which a second overstretched European country would lose. The slaves of Haiti just about exterminated the white settlers, except for the few who escaped, taking Yellow Fever and Dengue with them. Both diseases are mosquito-borne, so they flare up in the summer and die down in the winter, although the Philadelphians who welcomed the exiles didn't know that. Yellow Fever in Philadelphia was bad in 1793, came back annually for three more years, and flared up once again in 1798. It could be easily observed to be more frequent in the lowlands, absent in the hills. Seasonal, it reached a peak in October, disappeared after the first frost. In the early fall, people died a horrible yellow death, jaundiced and bilious.
|
|
| Dr. Rush |
The Yellow Fever epidemic had a profound effect on many things. It was one of the major reasons the nation's capital did not remain in Philadelphia. It made the reputation of Dr. Benjamin Rush who announced a highly unfortunate treatment -- bleeding the victims -- thus provoking numerous anti-scientific medical doctrines based on the relative superiority of doing nothing at all. In Latin, Galen had capsulized the doctrine of Hippocrates in the "Epidemics" as premium non-nocere ("At least do no harm.") It took a full century for American scientific medicine to recover from this blow to its reputation. Whatever criticism Rush may deserve for his Yellow Fever blunder, it definitely is not true that he was a scientific lemon. Medical students are regularly surprised to learn that he is the physician who first identified and described the tropical disease of Dengue, or "break-bone fever", which was a somewhat less noticed feature among the Haiti exiles in Philadelphia. In still other scientific circles, Benjamin Rush is often referred to as the "Father of American Psychiatry". He was one of the founders of the College of Physicians of Philadelphia, the oldest medical society in North America. Medical colleagues who today scoff at the yellow fever episode seem to forget that Rush stayed behind to tend the sick during a devastating epidemic, while many of his more cautious colleagues fled for their lives. An unhesitating signer of the Declaration of Independence, whatever Rush did, he did courageously. Non-academic physicians have sarcastically referred to this episode ever since, as proving that "some people" think it is "better to publish than to perish".
One very good non-medical thing the Yellow Fever epidemic accomplished was to put an abrupt end to the torch-light parades of window-breaking rioters agitating, with Jefferson's approval, for an American version of the guillotine and the terror. Federalists like John Adams and William Bingham never forgave Jefferson or his admirers for this, so the class warfare movement might likely have got much worse if everyone had not suddenly dropped tools, and headed for the hilly safety of Germantown.
The President of the new republic, George Washington, was in Mt. Vernon in the summer of 1793, wondering what to do about the Yellow Fever epidemic, and particularly uncertain what the Constitution empowered him to do. He finally decided to rent rooms in Germantown and called a cabinet meeting there. His first rooms were rented from Frederick Herman, a pastor of the Reformed Church and teacher at the Union School, although he later moved to 5442 Germantown Ave, the home of Col. Franks. Jefferson chose to room at the King of Prussia Tavern.
During this time, Germantown was the seat of the nation's government. As was fervently hoped for, the cases of yellow fever stopped appearing in late October, and eventually, it seemed safe to convene Congress in Philadelphia as originally scheduled, on December 2.
Although Germantown was badly shaken by the experience, it was a heady experience to be the nation's capital. Meanwhile, a great many rich, powerful and important people had come to see what a nice place it was. Germantown then entered the second period of growth and flourishing. Walking around Germantown today is like wandering through the ruins of the Roman forum, silently tolerant of visitors who would have never dared approach it in its heyday.
REFERENCES
| Benjamin Rush: A Discourse delivered before the College of Physicians of Philadelphia: Thomas A. Horrocks ASIN: B0006FCBXS | Amazon |
| Bring Out Your Dead: The Great Plague Of Yellow Fever In Philadelphia In 1793: J.H. Powell ISBN-13: 978-1436715881 | Amazon |
| Germantown and the Germans: An Exhibition from the Collection of the Library Company of Philadelphia: Edwin, II Wolf ISBN-13: 978-0914076728 | Amazon |
Dr. Cadwalader's Hat

|
| Dr. Thomas Cadwalader |
The early Quakers disapproved of having their pictures painted, even refused to have their names on their tombstones. Consequently, relatively few portraits of early Quakers can be found, and it might, therefore, seem surprising to see a picture of Dr. Thomas Cadwalader hanging on the wall at the Pennsylvania Hospital. A plaque relates that it was donated by a descendant in 1895. Another descendant recently explained that the branch of the family which continued to be Quaker spells the name, Cadwallader. Dr. Cadwalader of the painting, famous for presiding over Philadelphia's uproar about the Tea Act, was then selected to hear out the tea rioters because of his reputation for fairness and remains famous even today for his unvarying courtesy.

|
| Pennsylvania Hospital |
In one of the editions of Some Account of the Pennsylvania Hospital, I believe the one by Morton, there is a story about him. It seems there was a sailor in a bar on Eighth Street, who announced to the assemblage that he was going to go out the swinging doors of the taproom and shoot the first man he met. So out he went, and the first man he met was Dr. Cadwalader. The kindly old gentleman smiled, took off his hat, and said, "Good Morning, Sir". And so, as the story goes, the sailor proceeded to shoot the second man he met. A more precise rendition of this story comes down in the Cadwalader family that the event in the story really took place in Center Square, where City Hall now stands, but which in colonial times was a favored place for hunting. A man named Brulumann was walking in the park with a gun, which Dr. Cadwalader took as a sign of a hunter. In fact, Brulumann was despondent and had decided to kill himself, but lacking the courage to do so, had decided to kill the next man he met and then be hanged for murder. Dr. Cadwalader's courteous greeting, doffing his hat and all, befuddled Brulumann who went into Center House Tavern and killed someone else; he was indeed hanged for the deed.
I was standing at the foot of the staircase of the Pennsylvania Hospital, chatting to a young woman who from her tailored suit was obviously an administrator. I pointed out the Amity Button, and told her its story, along with the story of Jack Gallagher, whom I knew well, bouncing an empty beer keg all the way down to the Great Court from the top floor in the 1930s, which was then being used as housing for the resident physicians. Since the young woman administrator was obviously beginning to regard me like the Ancient Mariner, I thought one last story about courtesy was in order. So I told her about Dr. Cadwalader and the shooting.
"Well," she said, "The moral of that story obviously is that you should always wear a hat." There then is no point to further conversation, I left.
College of Physicians of Philadelphia

|
| College of Physicians of Philadelphia |
The College of Physicians of Philadelphia is the oldest medical organization in America, or even the Western Hemisphere, having been founded in 1787, the year of the Constitutional Convention. The CPP, located on 22nd Street near Market, is not to be confused with the American College of Physicians (a much more recent organization, formed in 1923 and located at Fifth and Arch Streets). The term "Physician" was then much more specific, and Philip Syng Physick, now known as the father of American Surgery was not considered eligible for membership because he was a surgeon, not a physician.
The general idea of the founding of the College seems to have been to focus on the physicians who had attended medical school (usually in Edinburgh), as distinguished from the general run of a physician at the time, who had merely served an apprenticeship. The first medical school, at the University of Pennsylvania (then at Ninth and Walnut Streets, but now at 36th and Spruce) caused the College of Physicians to turn away from pedagogy to the direction of setting standards and providing a forum for the "better sort" of the profession to be self-governing. At one point, there was even a real possibility that the College of Physicians of Philadelphia would become the credentialing agency for the whole country, but licensing took the direction of state boards during the Nineteenth Century. Every book and journal must have a Library of Congress number. The Transactions of the College of Physicians of Philadelphia has a Library of Congress number, all right. Number one. Jonathan Rhoads, the giant of 20th Century surgery and the only person to be president of the College twice, once remarked that being first may not be terribly important in the greater scheme of things, but -- it's awfully hard to imitate.
The College was a very strong guiding force in the development of a system of medical ethics for the profession. A curious false turn was taken in the direction of Lambda Chi, a secret society of physicians for the purpose of invisibly policing medical conduct, but the College soon recognized this was the wrong direction to take, and eventually, it assumed the lead in forming the American Medical Association in 1848. The portrait of Chapman, the first President of the AMA, hangs above the mantle in the fellows' reception room, the original minutes and rolls of the delegates are found in the library. Half a dozen presidents of the College were also presidents of the AMA, but for some curious reason the College never became the local branch of the AMA, reserving that for the State and Pennsylvania County Medical Societies.
Every year a number of the most distinguished physicians in the world address the College, and an annual lecture by a Nobel Prize winner has been established. The College had the largest medical library in the country until recently, and it is still one of the largest. The present building is a Carnegie Library, in a sense. Andrew Carnegie was a patient of S. Weir Mitchell at the time Mitchell was president of the College and donated a large sum for a new building. The present elegant marble and the walnut-paneled structure was built in 1905, fairly recent by Philadelphia standards but nevertheless a national landmark.
With all this dignity, history and tradition, it likely comes as a surprise to learn that the College building has sixty thousand paid visitors each year. The source of this popularity is a combination of medical exhibits for the public, and the Mutter Museum. In the late Nineteenth Century Thomas Dent Mutter gave his large personal collection of anatomical specimens to the College for a museum in the style of the medieval European medical schools, where the students could learn from specimens on display because anatomical dissection was discouraged if not forbidden, and Kodachrome slides had not been invented. Mutter's collection is a combination of believe-it-or-not "freaks", anthropological studies of human variations, and a museum of medical history. The former curator, Gretchen Worden, has produced an illustrated book of the exhibits which quickly sold out and must be reprinted, and a yearly illustrated calendar which is quite popular. The doctors are a little bemused by the popularity of this material with the public, but tolerant.
Among the odd features of this collection is the brain of Sir William Osler, the giant of modern medical education. Osler belonged to a club of people who had such a high opinion of their own genius they pledged to donate their brains after death to the collection of specimens, in the hope that eventually science would be able to determine the anatomical source of their talents. Most people today are a little staggered at the arrogance of such an idea, so widely at variance with the concept that all men are created equal. Albert Einstein is another acknowledged genius whose brain is still floating in a pickle jar, waiting for its unique properties to be discerned. Presumably, time will eventually tell whether even the greatest intellects suffer from unconquerable hubris, or whether the envious rest of us must adapt to the consensus of political correctness, just to avoid facing the reality of our own inferiority.
Joseph Priestley, Shaker and Mover
|
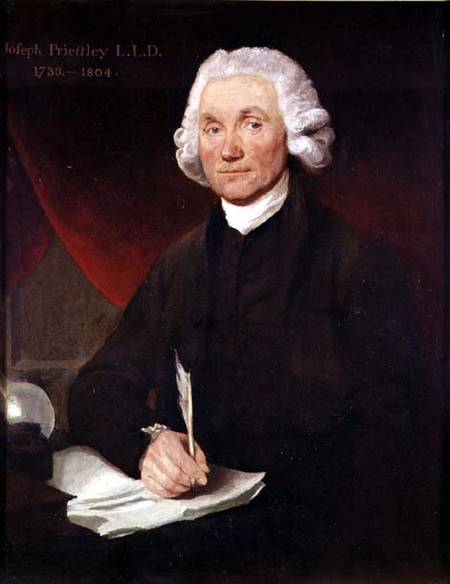
| Priestley |
Joseph Priestley, sometimes also spelled Priestly, is surely one of the more undeservedly neglected men of history. He has been called, with justice, the Father of the Science of Chemistry. He might also be called with equal justice, the father of the First Unitarian Church . The First Unitarian Church of Philadelphia, at 21st and Walnut, is the first and oldest Unitarian church and was indeed started at the urging of Priestley, whose principal residence was in Northumberland PA, at the confluence of the West and North Branches of the Susquehanna. Priestly wrote a scholarly work on the teachings of Jesus, which so captivated Thomas Jefferson that Jefferson wrote him the outline of another book that needed writing. Apparently, Priestley didn't have time, so in 1803 Jefferson wrote it himself, in the four languages he was fluent in, English, French, Latin, and Greek. Although those were simpler times, there have been few if any others who have told a President of the United States that he was just too busy to respond to a presidential request, particularly when the President could then find he had time to do it himself.
Priestley's theological teachings were based on scientific reasoning. They were highly controversial views, to say the least. He rejected the concept of a Trinity (he was a Calvinist minister, mind you), the divinity of Christ, and the immortality of the soul. Essentially, he rejected the concept of an immortal soul on the reasoning that perceptions and thought were functions of material structures in the human brain (Edmund O. Wilson's idea of Consilience is largely similar), and therefore will not outlive the cerebral tissue which produced them. In 1791, mobs burned his house in Birmingham, England, his patronage was revoked, and he hastily emigrated to Philadelphia. It isn't hard to see why these ideas were particularly unpopular with the Anglican church, which is probably the main reason England made him into a non-person, and his scientific ideas were denigrated as the product of other people.
That's too bad because he really was a scientist of immense importance. As a young man, he encountered Benjamin Franklin in England and was certainly a man after Franklin's heart. He noticed funny things about gases that rose from swamps and over mercury salts, and Franklin encouraged him to systematize and analyze his observations into theory. Although he called it anti-phlogiston, he had discovered oxygen. And then hydrogen, and nitrous oxide, and sulfur dioxide, and hydrochloric acid. Priestley really was the first organized and coherent scientific chemist, the Father of Chemistry. Franklin, Lavoisier, and Priestley became scientific friends, and enthusiastically exchanged ideas and observations, eventually leading to Lavoisier's fundamental principle: Matter is neither created nor destroyed, it only changes its form. In the end, it made no difference; Priestly had offended some pretty large religions, and nothing he did in chemistry was going to get much attention. Perceiving the value of the land at the confluence of rivers, he made his home for the last ten years of his life in Northumberland, Pennsylvania, now three hours drive Northwest, somehow managing to maintain an active scientific, political and theological influence worldwide. Visiting this rather sumptuous estate in a little river town is well worth a tourist visit. He died in 1804, just after his friend and kindred-religionist Thomas Jefferson became President of the United States.
Priestley's life can be summarized in one of his own most quoted remarks. "In completing one discovery we never fail to get an imperfect knowledge of others of which we could have no idea before so that we cannot solve one doubt without creating several new ones."
REFERENCES
| The Invention of Air: A Story of Science, Faith, Revolution,and The Birth of America, Steven Johnson ISBN: 978-1-59448-852-8 | Amazon |
Abortion
The official position of the Pennsylvania Medical Society on the topic of abortion is, we have no position on abortion. I ought to know because I was the author of this position, proposed at a moment when the PA Medical House of Delegates was obviously going nowhere. After two hours of angry debate, we had to stop before we split into two warring medical societies. The Pennsylvania delegation to the AMA was then obliged to hold the same no-position on a national level. As I recall, our position was likewise greeted by the AMA House of Delegates with great relief, and word quickly circulated in the corridors that Pennsylvania had a position everyone could endorse for the good of the organization. For several years, this no-position position was widely referred to whenever the topic threatened to arise. It almost invariably stopped the discussion in its tracks, as it was intended to do. In going back over the minutes, it would appear the AMA never actually voted to adopt a no-position motion, a discovery that surprised but did not change the basic determination to let the rest of the nation settle this. We were going to stay out of it.

|
| Roe vs. Wade |
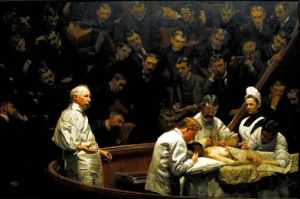
Because, one hundred forty years earlier, we started it. If you actually read Justice Blackmun's opinion for the majority in Roe v. Wade, as very few agitated proponents seem to have done, the original medical origin is clearly laid out. Blackmun had been a lawyer for the Mayo Clinic before his appointment to the Supreme Court, acquiring unusual medical resources and experiences for a lawyer. Now prepare for a logical leap, to the The Gross Clinic, Thomas Eakins masterpiece painting of Philadelphia's pre-eminent surgeon in a black frock coat, holding a dripping crimson scalpel in his bare hand, encapsulates the original situation. Note carefully that anesthesia is being given to the patient, but the surgeon is not wearing a cap, mask, gown, or rubber gloves.

|
| Gross Clinic |
In 1850 medical science had progressed into a forty-year time window when anesthesia made abortions painless, but Pasteur had still not identified bacteria, and Lister had not devised a way to cope with them. Abortions, common in ancient Greece but forbidden by Hippocrates, suddenly were widely demanded by 19th Century women in a situation when their judgment was vulnerable. Abortions were easy to do, all right, but women died like flies from the resulting infections, and the American Medical Association was distraught about it. The Oath of Hippocrates was brought forward to emphasize its prohibition of abortion, and the performance was made unethical for a member of the Association, sufficient cause to warrant expulsion. When that proved inadequate, the delegates agreed to go to their local state legislatures and seek legislation prohibiting the performance of abortion by anyone, member or non-member of the Association. These laws were quickly passed, and it was the Texas version which was overturned by Roe v. Wade as an unconstitutional denial of privacy. Roe was a pseudonym for the patient, and Wade was then Attorney General of Texas, the officer charged with enforcing Texas law. By 1900 abortions became both easy and safe for the mother, and by 1911 the AMA had reversed its position. The scientific surgical situation is well illustrated by a later famous painting about Philadelphia surgery by Thomas Eakins, the Agnew Clinic, in which the surgical team is portrayed in its modern costume of sterile gowns and rubber gloves. But it didn't matter since by that time various churches had hardened their doctrines. Religious leaders and their constituent politicians simply no longer cared what the medical profession thought about it. For at least the following century, ideological combatants were plainly only interested in whether physician opinion might advance one side or the other of their argument with useful official statements. Our real position, if anyone cares, is that we started out seeking protection for the safety of the mother, but the issue got twisted by others into disputes about the welfare of the unborn fetus.
|
| Agnew Clinic |
Since this is the case, there plainly may be a reason for state legislatures to reconsider the state laws they passed in the 19th Century, during that forty-year window of time when the scientific facts were in transition. But when a leap is made by the appointed referees of the federal government to overturn state laws, even about a basically medical issue, there has to be some legal reason to intervene; a medical reason somehow doesn't count. Justice Blackmun's discovery of an unnoticed right to "privacy" in the Constitution, where the word does not appear, is just too hard for us non-lawyers to deal with. Suppose we leave the fine points of the Bill of Rights to those constitutional lawyers. What's at stake here, among other things, of course, is whether the Federal Courts are justified in overturning well-intentioned state laws which had served well for at least fifty years -- simply out of impatience with the sluggishness and political timidness of state legislatures to revise obsolete laws. That's unbalancing the Constitution for a comparatively minor cause. Even major cause is something we have agreed to adjust in other ways, by amendment, not judicial opinion. And that's my opinion, having comparatively little to do with abortion.
Old Blockley (P.G.H.)

|
| Old Blockley |
For a long time, the Philadelphia General Hospital was the largest hospital in town, even growing briefly to seven thousand patients during the Civil War, but leveling off at about three thousand at the beginning of the Twentieth Century. At the end of World War II, it had shrunk to about 1500 beds, but it was Medicare and Medicaid in 1965 which finally did it in. By 1977 it was costing the City of Philadelphia about five million dollars a year beyond its revenues to run the place with only 300 patients, while the running expenses of the local private hospitals were actually less, per patient. Titles XVIII(Medicare) and XVIV(Medicaid) of the Social Security act constituted Lyndon Johnson's Great Society, and in effect they made every patient at PGH resemble a walking government check in the mind of hospital administrators. The local hospital association made the argument to the Mayor Rizzo that everybody would be better off if the hospital closed and those government checks were directed to the local voluntary institutions. After a few years, the federal government inevitably squeezed the generosity out of the bargain they would of course now like to abandon. But that's the way it goes. PGH is gone and it isn't coming back. The eighteen acres in Blockley Township, now West Philadelphia, were given to the University of Pennsylvania next door, and gigantic amounts of federal money were contributed to the building of skyscrapers replacements for the original PGH. Ironically, the two hundred children's beds now on the location are fewer in numbers than the three hundred adults once considered too uneconomically few to maintain, and the cost per day of hospitalization is roughly ten times the PGH cost which had been described as unsupportable. The rest of the real estate is built up with buildings involved in medical research, which is also an activity dedicated to working for its own extinction. Discovering a cheap cure for cancer would quickly create a need to fill the vacancies with something else. No one regrets this system of creative destruction, but everyone should regret the diminution of the spirit of local philanthropy which underlay it.
PGH was one of a dozen or so big-city charity hospitals, like Bellevue in New York, Charity in New Orleans, or Cook County Hospital in Chicago. Of these hospitals, PGH had surely been the best, and at the turn of the Twentieth Century a Mayor's commission issued a report about the place which began, "Philadelphia can surely be proud...." Having worked in Bellevue and having visited most of the rest, I can testify that was likely true. When PGH was finally torn down, the walls and floors had such substantial construction that changing the wiring and plumbing to some other purpose had become almost impossible. The PGH nurses were famous for running. Although the alcoholic and drug-addicted patients might be called the dregs of society, the alacrity of the student nurses in running them bedpans or answering other calls, was spectacular to watch. When a doctor came on the floor, they jumped to their feet and were usually ready with the patient's charts, unmasked. Unlike Bellevue, where the floors were creaky and wooden, the open wards at PGH were spacious, clean, well maintained and equipped. At Bellevue, the forty-bed wards were crowded with sixty or seventy patients, so close together you could almost roll from one end of the room to the other without touching the floor. I can remember seeing one seventeen-year-old Bellevue student nurse tending such award at night alone, the intern sharpening needles, and the medical resident developing electrocardiograms in the darkroom. None of this would have seemed acceptable at PGH.
|
| Dr. William Osler |
Old Blockley was the place where modern systems of medical education originated. Up until William Osler came to Philadelphia, medical education mostly consisted of attending eight hours of lectures a day. Osler had an electrifying personality and wandered among the sick at PGH with a train of students following him. He is much quoted, and once suggested his obituary ought to read, "Here lies the man who took the students into the wards." A somewhat more elegant statement of the value of the practical experience was included in his dedication speech at the Boston Library: "To treat patients without books is to sail an uncharted sea. To read books without seeing patients is never to go to sea at all. Osler was somewhat underappreciated during his time in Philadelphia and went on to found the medical school at Johns Hopkins in Baltimore. Nevertheless, the main reason he later left John Hopkins and went to Oxford was his dismay at the adoption of the "full-time" system, which is to say the faculty stopped having a private practice of their own to act as a gold standard for their research and teaching. When all is said and done, there are some areas of discomfort in the transition of students from observers to actors. The PGH system of learning surgery was commonly reduced to a slogan, "See one, do one, teach one,"; things have progressed to the point where it is probably right for the public to insist on greater supervision and control than the old almshouse provided.
The disappearance of old Blockley ended a controversy, or even something of a mystery, about which was the oldest hospital in America, PGH or the Pennsylvania Hospital at 8th and Spruce. There had been an infirmary in Old almshouse at Eleventh Street, and there is no doubt the almshouse was there first. PGH grew out of the almshouse. However, there were many comments at the time of the founding of the Pennsylvania Hospital that it was now the first; that's a strange thing to say when the almshouse was three blocks away. Social historians need to look into the mindset of colonial America, which seems to have included the distinction between the worthy poor and the unworthy poor. Somehow, the founding principal of the Pennsylvania Hospital was to get people back to work who were capable of productive work, possibly even paying for itself in that way. In their minds, apparently just giving solace and help to those who were down and out was not quite the same thing.
A Toast To Silas Weir Mitchell, MD
|
| Silas Weir Mitchell |
Silas Weir Mitchell lived to be an old man during the Nineteenth Century when it was unusual to get very old. He was an important part of both the Philadelphia medical scene and the literary one. He became known as the Father of American Neurology as a published studies of nerve injuries caused by the Civil War. He published about 150 scientific papers, including famous investigations of the neurological effects of rattlesnake venom. His most famous medical treatment was the "rest cure" for hysteria, while his most enduring scientific discovery was the phenomenon of causalgia. He despised Freud, and psychonanalysis. No doubt the feeling was mutual, but the passage of time has tended to favor Mitchell more than Freud. The central role of sex is the essence of Freud's viewpoint, while Mitchell is summarized in the remark that, "those who do not know sick women, do not know women."Struggling medical students can take heart from the well-documented fact that Mitchell applied to the Pennsylvania Hospital for an internship, and was rejected. Upset by the experience, he toured Europe for a year and applied again. He was again rejected. He later applied for the faculty at Jefferson and was rejected, but his reaction to that was one of rage and vengeance. Just what these two episodes out of Philadelphia medical politics really mean, remains to be clarified by Mitchell's biographers.

|
| Franklin Inn |
Mitchell's second career was literary, publishing 12 novels and 5 books of poetry. He is honored as the founder of the Franklin Inn Club, for century home to every important literary figure in Philadelphia. It is striking that he selected Benjamin Franklin as the guiding star of the Inn since Franklin similarly was eminent in both science and culture, and an ornament to conversation and society. In a pacifist Quaker City, both men approved of combat, and his novel about Hugh Wynne stresses that his hero was a "Free Quaker, meaning one who fought in the Revolution. Because of his strong Republican views, he was never made a professor at the local medical school.

|
| College of Physicians |
Mitchell's patient Andrew Carnegie donated the funds to build a new building for the College of Physicians when Mitchell was its President. When Mitchell was president of the Franklin Inn, Carnegie wrote him, asking for suggestions about donating a small sum, say five or ten million, and asking where it should go. That was the Inn's big chance, all right, but somehow it failed the test. Mitchell suggested that the money be given to raise the salaries of college professors, thus perhaps suggesting that this veteran of many academic revolts did eventually soften his views.
Eakins and Doctors
|
|
| The Gross Clinic |
A Christmas visitor from New York announced he read in the New York newspapers that Philadelphia's mayor had just rescued a painting called The Gross Clinic, for the city of Philadelphia. The Philadelphia physicians who heard this version of events from an outsider reacted frostily, grumpily, and in stone silence. To them, the mayor was just grandstanding again, and whatever the New York newspaper reporters may have thought they were saying was anybody's conjecture.
Thomas Eakins is known to have painted the portraits of eighteen Philadelphia physicians. Several of these portraits have been highly praised and richly appraised, seen in the art world as part of a larger depiction of Philadelphia itself in the days of its Nineteenth-century eminence. That's quite different from its colonial eminence, with George Washington, Ben Franklin, the Declaration and all that. And of course entirely different from its present overshadowed status, compared with that overpriced Disneyland eighty miles to the North. Eakins depicted the rowers on the Schuylkill, and the respectable folks of the professions, every scene reeking with Victorian reminders. It's a little hard to imagine any big-city mayor of the present century in that environment. Indeed, it is hard to imagine most contemporary Americans in a Victorian environment -- except in Philadelphia, Boston, and perhaps Baltimore. So, Mayor Street can be forgiven for not knowing exactly what stance to take, and was not alone in that condition.
S. Weir Mitchell, for example, became known as the father of neurology as a result of his studies and descriptions of wartime nerve injuries. But the repair of injuries is a surgical art, and many novel procedures were invented and even perfected, many textbooks were written. Amphitheaters were constructed around the operating tables, for students and medical visitors to watch the famous masters at work.
In The Gross Clinic, we see the flamboyant surgeon in the pit of his amphitheater at Jefferson Hospital, in the background we see anesthesia being administered. Up until the invention of anesthesia, the most prized quality in a surgeon was speed. With whiskey for the patient and several attendants to hold him down, the surgeon had one or two minutes to do his job; no patient could stand much more than that. After the introduction of anesthesia, it might overwhelm newcomers to observe leisurely nonchalance, but in truth, the patient felt nothing, so the surgeon could safely pause and lecture to his nauseated admirers.
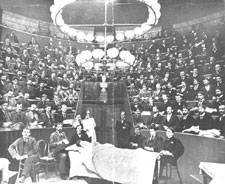
|
| Operating Amphitheater |
What made an operation dangerous was not its duration, but the subsequent complications of wound infection. By 1876, Eakins could have had no idea that Pasteur and Lister were going to address that issue in four or five years, making operations safe as well as painless. But his depiction of a surgeon with bloody bare hands, standing in Victorian formal street clothes, gives the most dramatic possible emphasis in the painting to the two most important scientific advances of the century. Modern medical students spend days or weeks learning the ceremonial of the five-minute scrubbing of hands with a stiff and somewhat painful brush, the elaborate robing of the high priest in a sterile gown by a nurse attendant, hands held high. The rubber gloves, the mystery of a face mask and cap. In some schools, the drill is to cover the hands of a neophyte with charcoal dust, blindfold him, and insist that he scrub off every speck of dirt that he cannot see before he is admitted to the operating theater for the first time. If he brushes some object in passing, he is banished to the scrub room to start over. So the Gross Clinic has an impact on everyone who sees the surgeon in street clothes, but it is trivial compared with the impact that painting has on every medical student who has been forced to learn the stern modern ritual. For at least fifty years, that painting hung on the wall facing the main entrance to the medical school, where every student had to pass it every day. To every graduate, the lack of clean surgical technique by the famous man was a wrenching sermon on every doctor's risk of trying his utmost to do his best, but doing the wrong thing.
That painting, hanging quite high, was rather cleverly displayed to the public through a large window above the door. With clever lighting, every layman who walked along busy Walnut Street could see it, too, and it became a part of Philadelphia. That was a feature the medical community barely noticed, but it was probably the main reason for public uproar when a billionaire heiress offered the school $68 million to take the painting to Arkansas. The painting was not just an icon for the medical profession, it had become a central part of Philadelphia. Philadelphia wanted to keep that painting for a variety of reasons, and one of the main ones was probably a sense of shame that we were so poor we had to sell our family heirlooms to hill-billies.
The doctors didn't pay much attention to that. They were mad, plenty mad, that a Philadelphia board of trustees would appoint a president from elsewhere who would give any consideration at all to such an impertinent offer.
Emperor's Doctor

|
| Kitamura |
As told by one of his fellow interns who is now a very old man, Kitamura was one of the best interns the Pennsylvania Hospital ever had; diligent, dependable, intelligent and infinitely polite. He married one of the hospital's nurses, and they tended to keep to themselves, especially in 1941, as war clouds began to gather. About two months before Pearl Harbor, both of them mysteriously disappeared. Kimura's wife later wrote one of her friends that they were in Japan. After the war, it was learned that she had been placed in a concentration camp as an enemy alien, and when released, had divorced him.
Still later, it was learned that Kimura had a distinguished medical career in Japan. He kept up a minimal sort of correspondence with his old intern pals, inviting them to visit if they were ever in Japan.
In 1985 one of them did so, going to the largest hospital in Tokyo to inquire. Great silence ensued; unfortunately, the revered and distinguished physician had recently died. You knew, of course, that he was the Emperor's personal physician.
Discipline for the Disciple

|
I.S.Ravdin was President Eisenhower's surgeon; Chick Koop was President Reagan's Surgeon General. Both of them were overshadowed by Jonathan Rhoads. Even in a physical sense, this was true. Rhoads was a foot taller than almost anyone. Big bones, too.
During the Second World War, Ravdin led almost every doctor in the University of Pennsylvania off to some military hospital unit or other, and in fact, the 900-bed hospital in Philadelphia was left with only two surgeons, Koop and Rhoads, ineligible for military service because of previous tuberculosis. Koop was a first-year resident in training, so for practical purposes, Rhoads was the only surgeon. Even after eliminating purely elective or optional surgery, the workload was staggering, and the number of operations was prodigious.
Rhoads devised a system. The young trainee, Koop, would do the time-consuming work of opening the belly wall and Rhoads would then do the internal surgery, following which Koop would close the wound while Rhoads was operating on another patient. As Koop told the story at Rhoads' 90th birthday celebration, one day a patient was to have his gall bladder removed. Rhoads told him to open the wound, first, the skin, then the fascial layer, then the peritoneum, while he was finishing up with another patient in another room. At that point, Rhoads felt he would be able to come in and remove the gall bladder. Most gall blabbers are firmly attached to the nearby liver, and must be shaved loose before it is possible to put a clamp around the base to remove them.
On this day, two things were different. Rhoads was delayed in the other room because of some complication, and Koop was just standing around waiting. The other thing that was different was that this particular gall bladder was not attached to the liver at all, but was just flopping around in the belly. When Rhoads continued to be delayed, Koop just went ahead and clipped off the gall bladder; more time elapsed. So he carefully sewed up the peritoneal layer, then the fascial layer, then the skin, stitch by stitch. He was standing there pretty pleased with himself when the doors finally banged open and Rhoads came charging into the operating room.
Koop offered some explanation in a faltering way, but Rhoads did not say a word. A large elbow on a huge arm silently but forcefully brushed Koop off to one side in a single movement. Rhoads then took out each stitch in the skin, then the stitches in the fascia, then the stitches in the peritoneum. He peered into the cavity, inspected the former bed of the gall bladder. Finding things in good order, he then resutured the peritoneum, then the fascia, then the skin. Without a word, he then strode from the room, leaving the future Surgeon General never to forget the lesson he had been taught.
Goat Head Merchant
|
| Bellvue Hospital |
In 1948, one of the Internet physicians at Bellevue Hospital contracted tuberculosis. The senior medical students at Columbia were asked to volunteer to take his place, and for a month I did so. Since I knew I was soon going to Philadelphia to the Internet at the Pennsylvania Hospital, my interest was particularly taken by an old Bowery bum who was talking about untaxed liquor. In New York at that time, it was common for Skid Row denizens to drink the wood alcohol in Sterno, called "squeeze" because it could be extracted from the waxy contents of a Sterno can by wrapping it in cheesecloth or a handkerchief and squeezing out the juice. Another favorite was "Smoke", which was typically a mixture of automobile radiator fluid and other sundry handy ingredients. My new best friend at Bellevue was just recovering from the effects of such recreation, and was in a mood of "never again". He observed that "When I get out of the Bell View, I'm going to get on a bus and go down to Philly. They've got a drink there called Goat Head, and, man, is it ever smooth."
The Chief Resident of the Pennsylvania Hospital was happy to tell me what Goat Head was. It was bootleg liquor, made in the Pine Barrens of New Jersey. Bags of cane sugar were fermented and distilled through coils of copper tubing, obtained from old hot-water heaters. The smooth stuff that so intrigued the bums of Bellevue was what was otherwise known as "White Lightning". It was then sold in the alleys near South Street by "Goat Head Merchants", who carried a suitcase full of small bottles, sold for about 25 cents a bottle. They say that during the Depression, Goat Head was sold out of an open bucket, at 10 cents a dipperful. One of the Goat Head Merchants used the Accident Room of the hospital as his family doctor, let us call him Walter Apple.
One day, Walter had a heart attack and was brought in on a stretcher, in considerable pain. I had just completed an electrocardiogram on him, when the pain disappeared. A few weeks later, he had completely recovered and was going home. Every time I came anywhere near him, he announced to everyone in the vicinity that I was the best doctor in the world, having cured his heart attack by giving him the "wire treatment".
As he gathered up his belongings to go home, he apologized that he was not going to be able to pay his bill. He had once known Dillinger and all those other big shots wore a diamond stick-pin and drove a Duesenberg car. But now he was broke.
But grateful, too. So, if ever there came a time when I encountered someone unpleasant, who needed "pushing' around" -- just you call on Walter Apple, and Walter would be glad to pay off his debt.
Lin
Lindley B. Reagan, M.D.
July 16, 1918 -- September 10, 1995

|
| Lindley B. Reagan, M.D |
The first and oldest hospital in America, the Pennsylvania Hospital at 8th and Spruce Streets, always had a strong Quaker flavor but a unique medical tradition as well. Since it was the only American hospital for decades, later becoming the home hospital of the first medical school in the country, it impressed its ideals and traditions on the whole of American medicine. However, it imposed so many difficult demands on its trainees that a century or more of an evolving profession simply moved away from copying it. It was, in 1960, the last hospital in the country to begin paying its resident physicians anything at all, one of the last privately controlled American hospital to adopt a billing and accounting department, and one of the last if not the last to regard a handful of private beds as merely a convenience for the patients of the staff physicians. In 1970 its method of maintaining inventory was to notice that the supplies on the shelf were running low, and ordering some more. It was founded in Benjamin Franklin's words, for the "sick poor, and if there is room, for those who can pay," and could only survive into the late 20th Century through private donations and the freely contributed services of the doctors, student nurses and administration. No amount of money could induce people to work as hard as they worked. You might say this was the only aspect of Medieval monasteries which Philadelphia Quakers thought worthy of imitating.
Somewhere in this set of ideas was the treasured concept of a rotating internship, preferably two years long, prior to entering specialty training through a residency. In 19th Century Vienna, it was a matter of rule that an intern was just that, physically confined within the walls for the term of service, and a resident was just that, someone who lived on the campus. The Pennsylvania Hospital had no such rule, but since it paid the doctors nothing for five or six years of eighty-hour weeks, their poverty forced them to satisfy the Viennese rules by default. Entertainment was bridge or poker in the intern quarters, conversational chit-chat was a description of bizarre cases or peculiar patients, a weekend "off-call" was a good time to catch up on correspondence. There were student nurses around, of course, but the matron was a pretty no-nonsense chaperon. Every class of interns contained one or two millionaires by inheritance, but peer pressure made them nearly indistinguishable in the daily routines. Aristocrats' main value to the resident physician community was their access to the ruling families in the city, and hence to the governance of the hospital, in case governance should occasionally abuse the vulnerability of the trainees.
I find in retirement that most of my colleagues are now willing to tell stories of the "old days" which they were unwilling to tell at the time. Over several glasses of the finest single-malt in a walnut-paneled club, one such story recently surfaced. It concerned Lin.
Lin was a member of an old Quaker family, surprising everybody during the Second World War by volunteering as a junior physician in the Navy. He was assigned to a marine regiment in the Pacific Theater and went through some of the most murderous fightings on Iwo Jima and Guadalcanal. Our grapevine reported that the enlisted Marines in his outfit absolutely worshipped him, and I easily believe there was a lot of quiet heroism behind that gossip. He told me he had decided to become an internist while in the Pacific, but somehow only a surgical residency was available when the War was over, so he took it. He was probably the best internist on the staff, and it showed in his conduct of surgery, where it sometimes matters more what you decide to cut than what you cut. He always looked exhausted, but never hesitated to drive himself another hour when the situation demanded it. One day, he had to excuse himself from an operation, an almost unheard-of event, and testing his own urine, found it loaded with sugar. So, the soft-spoken Quaker internist who was primarily doing surgery had to add the burden of insulin injections to his load. If he ever complained about that or any other thing, no one could remember hearing it.
At about the third glass of single malt, the story came out. My old friend, like the rest of us, had to spend a year as a surgical intern during the two-year rotating internship; he hated surgery and didn't mind telling the world. At the moment in question, he was the assistant at some neck surgery, with Lin performing the actual surgery. He was told to take a long pair of scissors and cut off the excess strands of sutures after Lin tied the knots; that was known as trimming the ligatures. They were working deep in the crevices of the patient's neck. Lin held up the loose ends of the knot and ordered, "Cut". My friend inserted the long scissors into the hole and snipped -- accidentally cutting right through the jugular vein.
As would be expected, a fountain of blood came up out of the hole, and Lin stopped it by putting his thumb on the cut ends of the vein. "Well," said Lin, "I guess we'll have to fix that." And did.
With tears in his eyes, my octogenarian friend cried out to the startled clubroom. "God bless you. God bless you, Lin."
Perhaps the point isn't clear to those who didn't go through the process, so let's be more explicit. Both my friend and I worshipped Lin, as a person, a teacher, and a surgeon. He was the perfect agent for his patients, without the tiniest trace of conflict of interest, income-maximizing or whatnot. He was as technically skillful as it is useful to be, but he was the thinking man's surgeon as well as the utterly faithful servant of the best interests of the humblest patient. He was, in the opinion of his closest professional associates, the best surgeon in the world. In need of surgery ourselves, all of us would have flown the Atlantic to have him operate on us. For reasons of his own, he was to spend the forty years of his professional life in a small country town with a small hospital, scarcely a famous surgeon but a beloved one to his community. Over the past sixty years, I have had a number of opportunities to know many surgeons who would be in contention for the title of the best surgeon in the world. Some have written books, some have struggled successfully upward through vicious competition, some of them would be called "Rainmakers" if the research world followed the pattern of lawyers and architects. One or two have won Nobel Prizes for surgical innovations, but that's different from being the best surgeon around. The best surgeon in the world was Lin, faithfully plying his trade in a little town that could not possibly know how lucky they were.
Mind Your Manners

|
| Hoeffel |
In 1948 I was an intern at the old Pennsylvania Hospital, assigned for a while to the accident room. One of the accident-room duties of an intern is to sew up cuts and lacerations that arrive unexpectedly, but some lacerations can be out of your pay-grade and you have to call for help. On the evening in question, the victim had been so thoroughly slashed up that I had to call the chief surgical resident, Dr. Joseph Hoeffel. Hoeffel was big, tall, loud and self-assured, and swept majestically into the accident room with a little fellow trailing him. This follower seemed less than four feet tall but very quick and shifty. He didn't walk so much as he scuttled. Hoeffel bellowed, "Get out here!" and the gnome vanished.
While Joe was examining the laceration problem, the little fellow slipped through a different door to see what was going on. Most of us had the impression this guy might well be the one who inflicted the cuts, but in any event, he didn't belong where he was. "I told you to get out of here, and stay out," bellowed our surgeon. Again the scuttler scuttled away, while Hoeffel put on a sterile gown, sterile rubber gloves, mask, cap, and the whole ceremonial costume. He prepared to do his work, stamping out disease among the sick and injured, when a fist started at the floor. The little guy had slipped into the operating area once more, and soon the fist on the floor quickly flew in a wide arc, ending up on Hoeffel's jaw.
Hoeffel tumbled head over heels across the room, ending up in a corner. I don't think he was knocked out, but he was certainly dazed. The nurses called the police, who made a tumult of their own arriving to do battle. But the little fellow was gone, never to be seen again.
Fifty years later, I had occasion to preside over a meeting of the Right Angle Club, where
Hoeffel's son, the former congressman and current deputy member of the Pennsylvania Governor's cabinet, was the featured speaker. He looked remarkably like his father. I had to wonder if his father's lesson in diplomacy had made any notable effect on his progeny.
Funny Toes: A Physician Viewpoint

|
| Webbed Toes |
It probably took me twenty years to notice that, unlike most people, I had an incomplete separation of my second and third toes. I thought my toes were like everybody else's, but once you start peeking, you see that webbed toes are not normal, although they are not really rare, either. After another thirty years, it became apparent that most of my numerous descendants had the same kind of toe; it was obviously an inherited condition. When the family clan gathered at the beach, it was a source of mild amusement, possibly even a little pride. A few weeks ago, I happened to mention the matter at a party, whereupon another doctor promptly pulled off his shoes and socks, and revealed fused or webbed toes of a much more striking sort than mine; obviously, he was proud of it, too. He is of an old, old Philadelphia family that owns one of the oldest, if not the oldest, a house in Germantown. His family, too, is stigmatized in the same way only more so. In Philadelphia, when you are proud of your family, you are really, really, proud of it.

|
| Ainhum |
Which brings me back to my days as an intern in the accident room of the Pennsylvania Hospital. When there is a sudden crowd of emergencies in an emergency department, the nurses get all of them undressed, put in a hospital gown, and instructed to wait for the doctor behind a curtain that doesn't quite reach the floor. For some reason, as a medical student, I had been particularly struck by a photograph in a textbook of an inherited disorder said to have been first noted on a slave ship; the disease in the native language was named Ainhum. For reasons obscure, a tight little band appears at the base of the fifth, or little, too. It gets slowly tighter over a period of months, and eventually, the little toe falls off. That's all there is to Aihnum, and all that was known about it. So, imagine my surprise and delight to walk past a row of naked feet sticking out below curtains -- and there was my first and last case of Aihnum.
I summoned my colleagues, and the visiting medical students from both Jefferson and Penn who at that time shared training in our accident room. I raced off to my room to get a camera to record this momentous event. An elderly staff physician, either Tom McMillan or Charles Hatfield, wandered past and was invited to share the excitement. Well, he says, I saw one of those forty years ago, it looked just like that; old Doctor Norris showed it to me when I was an intern. Much murmuring ensued but abruptly stopped when the patient himself rose up and started putting on his clothes. He was going home, but why? "Well," he growled, "I came here because my back hurts, and all you people do is look at my toes!" He said he was going over to the Jefferson Hospital to get proper treatment, and I guess he did.
And finally, there is Morton's Toe. Or perhaps more properly, Mortons' Toes. There were in fact two Doctor Mortons, one of them at Columbia College of Physicians and Surgeons where I went to school, and the other at the Pennsylvania Hospital where I interned. In New York, Morton's Toe refers to a painful callous, or neuroma, that forms on the bottom of the victim's big toe. In Philadelphia, such an answer would get a failing grade, because the Philadelphia Morton had noticed that some people have a big toe that is shorter than the other toes, instead of being bigger as the term would suggest was proper. The tricky thing about this relatively harmless variant is that the big toe is actually not short at all. The foot bone, or metatarsal, is short, so the toe of normal length sits back farther on the foot and just looks shorter. The main significance is for shoe salesmen since the shoe needs to be long enough to avoid crushing the other toes.
So now, you readers who were not lucky enough to go to medical school can get a feeling for what it seems like to be a doctor. The other significant shared bond within the fraternity is a sense of outrage at the way health insurance companies drag their feet paying doctors, but that's not limited to feet..
A Toast To J. William White, MD
JWilliam White left a legacy to the Franklin Inn, the income from which was to pay for an annual dinner, with all the trimmings. Good as its word, the Inn holds the J. William White dinner every year on Benjamin Franklin's birthday, although inflation and fluctuations of the stock market require it to make a modest charge for attendance. White also created the J. William White Professorship in Surgery at the University of Pennsylvania, a chair which was once occupied by Jonathan Rhoads.

|
| William J White MD |
These trust-fund memorials do little to convey the wild and glamorous image of Bill White. White was a member of the First City Troop and fought the last known honest-to-goodness duel on Philadelphia's field of honor (in the accidental "wedge" of disputed land between Delaware and Pennsylvania). The right and wrong of the argument about wearing the City Troop uniform are in dispute, but the details boiled down to White at the critical moment raising his gun to the sky and firing at the stars. That it was not a meaningless gesture was then brought out by his opponent ( a fellow Trooper named Adams) taking slow and deadly aim -- but missing him.
White was an academic in the sense that he was the first, unpaid, Professor of Physical Culture at the University of Pennsylvania. Active in the Mask and Wig Club, he was a chief surgeon at Philadelphia General Hospital, chief surgeon to the Philadelphia Police, and chief surgeon to the Pennsylvania Rail Road. He is the surgeon actually operating in Thomas Eakins' Agnew Clinic, while Agnew himself stands as the "rainmaker", to use a term from legal circles. He was Chairman of the Fairmount Park Commission, and numerous other positions where political contact was more important than surgical skill. When World War I came along, he was off to France with the University of Pennsylvania Hospital Unit, writing two books with Theodore Roosevelt. Although his friendship with Henry James suggests greater literary talent, he was supportive of Adams' transfer of citizenship in protest of America's staying out of World War I; but nonetheless, Roosevelt published more than thirty books. What emerges from the history of Bill White is flamboyance and lots and lots of unfettered energy. He might feel a little out of place at one of his endowed dinners today, but he was probably always a little out of place in any company -- and didn't care a whit.
REFERENCES
| Philadelphia Gentlemen: The Making of a National Upper Class: E. Digby Baltzell ISBN-13: 978-0887387890 | Amazon |
Yet Another Toast to Dr. J. William White
|
|
| Dr. J. William White |
Who was Dr. J. William White, and why do we drink a toast to him every year at our Annual Meeting?
I will answer my second question first: Dr. J. William White died on April 24, 1916, leaving a Will that he finally signed only on March 24 of that year. The Will, drafted by John G. Johnson, the most famous Philadelphia lawyer of that time, runs to 26 pages and disposes of an estate of $868,176.05,--which was real money in 1916.
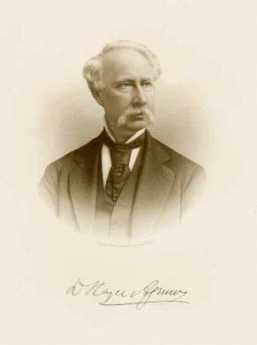
|
| Dr. David Hayes Agnew |
Item 17 of that Will reads as follows: "I give to the Franklin Inn Club of Philadelphia five of its bonds of $100 each to me belonging.
IN ADDITION TO THIS, I give to said Club the sum of $5,000 to be invested by the Directors of the Club, with the approval of the majority of the membership, and the income to be expensed in such way as will best subserve the interests of the Club and conduce to its perpetuation.
I will be glad if, in doing this, they can assure the occasional remembrance of my name. The Club has been of me the source of so much pleasure and happiness that I feel that I owe it something in return."
Well, I have not examined the minutes of our Board to see if it really was discussed and voted upon by a majority of the members, but when I joined in 1968, I was told that Dr. White's bequest had been used for this annual dinner in his memory as long as there was money to pay for it, then only to buy the champagne for the toast to his memory, and then in my time even the champagne money was drunk up.
We still talk about him. He was in every sense a "character", a special Philadelphia character. A lot of this information comes from a biography his friend Agnes Repplier published in 1991. J. William White's father James William White Senior was a doctor, the founder of Womens' Maternity Hospital, and President of the S.S. White Dental Supply Company, an extremely successful business which operated until recently from a big building just down there on 12th Street. The Money that flowed from this business enabled our Dr. J. William White to do pretty much what he wanted all of his life.

|
| Professor Louis Agassiz |
He was a very smart boy, strong, and with a bad temper. He got into fights at school, but he also managed to earn both an MD and Ph.D. from the University of Pennsylvania in 1871, at the age of 21. He maintained a passionate loyalty to Penn all of his life. Directly after graduation, he obtained a job on a U.S. Coastal Survey ship, theHassler on a survey of marine life and ocean bottoms conducted by Professor Louis Aggassiz of Harvard. He was hired as a "Hydrographic Draughtsman" but it turned out he was to be the expedition photographer and film developer because nobody else knew how to do that. Before they sailed, he also wangled a job as correspondent for The New York Herald. They sailed from Boston in December 1871, explored their way around South America and arrived in San Francisco in August of 1872. On his way home by train, young Dr. White stopped in Salt Lake City to hear Bringham Young preach. Bringham Young preached against doctors and lawyers, and told the women in his audience that they should not employ obstetricians, that they and their babies would be better off without them.
When Dr. White returned to Philadelphia, he went to work, first as a resident at

|
| PGH |
Philadelphia General Hospital, then a doctor for Eastern State Penitentiary, where he apparently lived for a while, where he took boxing lessons from a giant prisoner. By 1876 he was an Assistant Demonstrator of Practical Surgery at Penn, and a couple of years later he was working under the most prominent Philadelphia surgeon Dr. D. Hayes Agnew. In Thomas Eakins' famous painting "Dr. Agnew in his Clinic" we can see Dr. White doing the actual cutting, while Dr. Agnew is giving the lecture.
This picture is also interesting because

|
| Agnew Clinic |
right there in the middle of the action is a stalwart female, the surgical nurse. By the time of this picture, both Drs White and Agnew were having trouble with the Board of Governors: female students were complaining that they were not allowed into these clinics.
Drs Agnew and White replied that "the nature of the diseases and the conditions of the patients made the presence of females undesirable."
The doctors offered to quit and the Governors apparently backed down. But what about that nurse?
Another famous story: In 1877 Dr. White was elected to the First City Troop

|
| First City Troops |
. For some reason, this didn't look right for a young doctor, because in these long years between wars, the Troop was known more for parties, banquets, and balls than for national defense. However, he joined, enjoyed the parties and the riding. Previous Troop surgeons had worn regular street clothes; Dr. White put on the fancy Troop uniform. Probably at a party, a Trooper named Adams objected, became loud. Dr. White floored him. Mr. Adams sent a formal challenge to a duel.
Sensation! Nobody could remember a duel in Philadelphia, where it was against the law. The newspapers were in an uproar, the New York Herald,
for which Dr. White once wrote letters from his voyage around South America, invented a story about a lady who was supposed to be the real cause of the fight. Mr. Adams and Dr. White, accompanied by seconds and a surgeon, crossed the Mason-Dixon Line, took single shots at each, shook hands and went home. Dr. White shot into the air. Years later, Adams confessed that he had aimed at Dr. White, but missed. Eventually, the storm blew over, but it is remembered as the last duel around here -- as far as I Know.
As to the City Troop, Dr. White's Will left $5,000 in Trust for a "J. William White Fund, the income to keep remembrance of the facts that I served as Surgeon and was the first incumbent of that position to be directed by the Troop to wear the time-honored full dress uniform."
I don't know if the Troop bought champagne to keep remembrance.

|
| Franklin Field |
Although Dr. White became one of the best surgeons here, and wrote several successful textbooks, he is mainly remembered for his passion for athletics. He was made the first Director of Athletics at Penn.

|
| Army-Navy Games |
He built the first Gymnasium, he built Franklin Field, he arranged for Army-Navy Games to be played here, he got his friend Theodore Roosevelt to attend, he spent every summer either climbing the Rockies or climbing the Alps together with his very sporting and strong wife, Letitia.
Letitia was also a better shot than her husband.
Perhaps Dr. White's most famous sport was called "Angling for Men". He learned this sport on vacation in
|
| Narragansett Bay |
Narragansett Bay. The players are in a rowboat, and the contestant jumps into the water, with a strong rope tied around his waist. The Men in the boat try to haul the Swimmer back into the boat, while he resists. When Dr. White was 46 years old it took three of his friends 38 minutes to get him back within 100 feet of the boat, but they never got him in!
Dr. White moved in very exalted circles. Among his close friends were Henry James,
whom he visited in Rye and who lived with the White's on his visits to Philadelphia: John Singer Sargent, whom Dr. White persuaded to paint his portrait although Sargent had given up portraits; and the famous English doctors Sir Frederick Treves and Sir Joseph Lister, and as I said, President Theodore Roosevelt.
In later years, after retiring from regular surgery, Dr. and Mrs. White traveled all over the world, although some patients including John G. Johnson insisted that only Dr, White could do any procedures upon their own bodies!
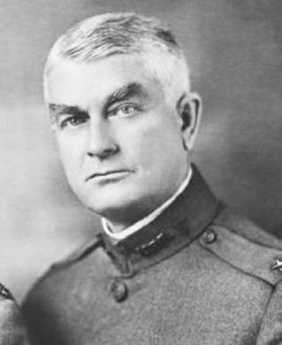
|
| William Mayo |
Well, of course, Dr. White had his own problems, and like all men, became a patient himself. In 1906, he developed a hard nodular mass in his left iliac fossa which, I gather, is not good. Probably cancer. He knew what to do. He took a train Rochester, Minn. To his friends the Mayo Brothers. When they decided to operate, three top surgeons from Penn went out to watch. Dr. William J. Mayo operated and successfully removed congenital diverticulitis which had caused a perforation of the bowel.
Later: Dr. Mayo: "Well, you're all right."
Dr. White "Well, you're a good liar. I've been there myself, and I know."
Dr. Mayo: You don't know everything. It's like a bag full of black beans, and one white bean. You pull out the white one. Now get well!"
|
| Thomas Hardy |
By next summer he was well and traveling again. He received a degree from University of Aberdeen, he met Thomas Hardy, he went to Egypt, next year to China, when the First World War began he was passionately pro-Allies, visited friends in London, visited wounded soldiers at the American Ambulance Hospital in Paris, spent much time there but did not operate, flew over the battlefields in a French military plane, and visited Reims during a German bombardment. He visited the British front, returned to London, involved himself in the issue of Henry James becoming a British citizen because of America's Neutrality, then sailed home across an ocean full of U-Boats.
Back in Philadelphia - actually on his estate in Delaware County he raised money for the American Hospital in Paris, and again involved himself in several disputes, about the War, about a Penn faculty member...but now he was dying, we're not clear from what, but it sounds like cancer, after all. He was in great pain and had to be hospitalized. He died in his beloved University Hospital, surrounded by colleagues and friends, on April 24, 1916.
I close with a few more words about his Will. As I said, it is 26 legal-size pages, really the story of a life, packed with bequests to every person who was close to him, every organization he belonged to-- and most of them, like the one to us here at the Inn, ask that something be done to remember J. William White, which seems --to me -- little sad. Why were this popular, successful men so afraid of being forgotten? Was it because he and his wife had no children?
I don't know, but here, tonight, we remember: I raise my glass-- champagne or not--to the memory of Dr. J. William White, a character if there ever was one!
------given at the Franklin Inn Club on January 14, 2005, by Arthur R. G. Solmssen
Albert C. Barnes, M.D.
A private investor has the general goal of accumulating enough wealth so, come what may, there will be a little left when he dies. If he has dependents or heirs, he needs somewhat more. Either way, he is not planning for perpetuity or thinking in astronomical time periods. Albert C. Barnes (1872-1951) had to switch his investment goals, in the 1920s, from investing for a comfortable retirement to investing for a perpetual art foundation. Perpetual.
|
| A bottle of Argyrol |
Having graduated from medical school (University of Pennsylvania) in 1902, and then writing a doctoral thesis in chemistry and pharmacology at the Universities of Berlin and Heidelberg, Barnes invented a patent medicine that quickly made him rich. Argyrol was a mildly effective silver-containing antiseptic with the unfortunate tendency to turn its users permanently slate-gray. The advent of antibiotics has since made Argyrol almost sound like quackery, but it was effective enough at the time to require factories in America, Europe, and Australia, and Barnes became immensely rich with it. The American Medical Association strongly disapproves of physicians who patent remedies, so Barnes was never held in high regard by his colleagues; but it could well be argued that he had as much training as a chemist as a physician, and spent his entire professional life as a chemist, manufacturer, and investor.

|
| The Barnes Gallery |
Barnes was eccentric, all right, but on Wall Street, the saying goes, "What everyone knows, isn't worth knowing." Guided by that principle, in 1929 he sold his company at the very peak of market euphoria, getting out of common stocks at the top of the market. It is small wonder that he soon instructed his Foundation to invest its endowment entirely in bonds. During the 1930s, commodities were extremely cheap because no one had any money. Barnes, of course, had a potful of money and bought hundreds, even thousands, of artworks very cheaply. He also bought 137 acres of Chester County, PA, real estate, and a 12-acre arboretum in Merion Township on the Main Line. Although he is famous for acquiring hundreds of French Impressionist paintings with the advice of Gertrude Stein and her brother Leo, he also bought great quantities of Greek and Roman classical art, African art, and the art of the Pennsylvania German community. He picked up a notable collection of metallic art objects. Most of these "losers" are down in the basement because he had so many Renoirs, Matisse, and Picasso (some of them may be worth $200 million apiece) that the upstairs galleries were pretty well stuffed with them. Viewed from the perspective of an investor with a goal of perpetuity, of course, the things in the basement just happen to be temporarily out of fashion, just like those bonds in the portfolio.
|
| A view inside the Barnes gallery |
Since the Foundation is currently strapped for ready cash, Judge Stanley Ott of the Montgomery County Orphans Court is now being urged to allow the Foundation to break Barnes' will in some way or other. Move the museum to downtown Philadelphia where it can attract more paying visitors. Sell some of that land. Sell some of those paintings in the cellar. Fire some of those employees. But all of these suggestions are short-term solutions, which may injure the long term. Everybody has an idea of what Barnes the rich eccentric would have done if he were alive to do it, but I suspect he would have rejected the whole lot. Barnes the shrewd investor would have taken the most expensive painting off the wall, and sold it to the highest bidder. Buy low, sell high, and the niceties of non-profit professionals are damned. Barnes wasn't in love with one single painting, or one particular school of painterly interpretation, he was in love with Art.
Investment theory has improved in the past fifty years; there have even been some Nobel prizes awarded for new insights. But it still isn't possible to put an investment portfolio on autopilot for perpetuity. Every museum, university, and the foundation has the same problem, with the result that the landscape is littered with the bones of perpetual organizations destroyed by following a fixed formula. With the singular success that Barnes displayed, it isn't surprising that he went a little too far with instructing his successor trustees in what to invest in. Never sell the paintings or the real estate, avoid the common stock, were ideas that worked brilliantly, and may even work most of the time. But sooner or later, the institution will be endangered by following them too literally. Somebody has to have some flexibility. But there is something else that is inevitable, too. Sooner or later, whether it takes fifty years or five hundred years, sooner or later someone will be given the responsibility and the necessary flexibility -- but will try to run off with the boodle, for himself. The balance between necessary prudence and necessary flexibility is impossible to maintain forever, and the Judge will surely have a hard time deciding what Barnes would have decided.
Victor Rambo, Indian Eye Surgeon
|
| Apostle of Sight |
There have been at least twelve documented generations of the Rambo family in Philadelphia. Historical justification can be found for the idea that this was the first family to settle within what are now the city limits. Victor Clough Rambo MD was an unpaid intern at the Pennsylvania Hospital in 1927; you will find his nameplate on the wall.
Victor early made up his mind that he was going to go where he could do the most good. Considerable thought led him to learn how to extract cataracts, and go to India to extract as many as he could. from time to time, he would return to America to visit family, and to give some speeches to raise money for his project.
The builders of our enormously costly hospital castles might give some thought to the fact that Victor did most of his surgery in tents. His system was to send out teams to the next two villages, whenever he was, with the news, "Bring in your blind people, the eye doctor is coming." When he then arrived, he set about operating on cataracts from dawn to dusk, in a country where the supply of cataracts was essentially unlimited. There was no time to operate on the comparatively minor visual disturbances so commonly treated in America today; he had to concentrate on people who were really blind, and in both eyes.
He wrote a book about his experiences, and perhaps there you could find data to calculate the number of people who were restored to a useful existence by his efforts. Surely, it was thousands. He just kept going at it, and when he died he was a very old man.
Illicit Drugs are Eliminated in Philadelphia
It seems fair to say that America is nearly desperate to find a successful way to eliminate the illegal narcotic trade. We've had a war on drugs, which seems to have three components, all failures. We have an occupying army in Afghanistan where most heroin comes from. We've sprayed weed killers on Bolivia, Colombia, Mexico, and found various other ways to assist local narcotic agents in their efforts to break up the planting of cocaine in Latin America. We've got high-speed patrol boats and helicopter patrols around southern Florida. Spies of all sorts have been hired to infiltrate the distribution channels. We've spent other tons of money educating school children that experiments with chemical recreation are risky, immoral, dumb, whatever. Sly, naughty allusions to drugs with cute code names have been pretty well driven off the television, night club acts, and even glitzy cocktail parties in the advertising business. Ronald Reagan had a simple solution --"Lock 'em up" which led to the passage of national law, leap-frogging the trials of drug offenses ahead of all other criminal offenses. The consequence was that prisons filled up and overcrowded conditions became a scandal. It may cost more to send someone to jail than to send them to Harvard, but the situation seemed to require us to ignore the cost, get them off the street, bring this problem to an end. If any of this work, or if all of it collectively worked, it didn't work very well. This is a very big problem that seems to defy solution.
So, one of the desperate ideas put forward has been to decriminalize drugs. That is, stop making their sale and use illegal. Abundant drugs would become cheap, cheap prices would eliminate the drug dealers' profit, and lack of supply of pushers would cause the supply to dry up. That is, no one would bring the heroin from Afghanistan, or the cocaine from Bolivia -- because there was so much of it around that the profit disappeared. Wait a minute. Did you just say that no one would import expensive narcotic because we would already have so much cheap narcotic? Somehow, it isn't persuasive that decriminalizing drugs would eliminate addiction. So, what other methods can claim proven success?

|
| Conan Doyle |
Let's try Philadelphia's system, by which I mean Philadelphia from 1940 to 1960. I graduated from medical school in 1948, filled with instruction about how to recognize the signs of drug addiction, how to detoxify, what precautions you ought to take to keep the student nurses from stealing the ward morphine supply, how carefully you had to monitor the pharmacy and anesthesia departments. Our older instructors were full of anecdotes about how clever the addicts were in fooling the doctor, how they themselves had been tricked or almost tricked, medical friends they knew who got hooked. Bad business, and it's important that every new innocent doctor is warned about how prevalent and how deceptive it was. Just read detective novels by Conan Doyle, who was a physician, addict, or De Quincey confessing to being an opium eater, or Coleridge writing Kubla Khan while in a drug stupor.
|
| Angelo Bruno |
So, my teaching and mentoring prepared me to believe that narcotic addiction was rampant before 1940. But when I came to Philadelphia I absolutely never encountered any of it, or at least until about 1970 when the Beatles and the Flower Children of California made it a deliciously tempting adventure. And I spent most mornings during that period doing teaching and charity work at Philadelphia General Hospital for thousands of indigents. If drug addiction had been anywhere in the city, it seems to me it would have been at PGH. We had thousands of cases of alcoholism, of tuberculosis, of syphilis in all its forms, suicides, homicides, bullet wounds, a prison ward full of manacled prisoners. But no drugs, nossir. It was a nice situation, and after a little while, you stop wondering about dogs that don't bark, and drug addicts that don't come in the accident room door. But a couple of decades later, when we had lines of heroin addicts waiting for their treatment, it all came back to us that we had experienced a remarkable absence of what was now quite common again. It had apparently been prevalent, it disappeared for twenty years, and then it came back. It now seems quite evident that we were enjoying a two-decade drug holiday, but what isn't so clear is what caused it. Whatever could have caused this remarkable temporary disappearance of illicit drugs?
Well, I don't know; and when you say that, you invite everybody to make some wild conjecture. So let me make my own well-ruminated guess, first. It seems worth investigating whether Angelo Bruno, the head of the mob, did it. It is a widely-held belief that Bruno hated the narcotics trade, and issued orders that there was to be none of it in his territory. It's quite possible that this was a purely business decision since there was plenty of money to be made from bootlegging and loan-sharking, whereas the narcotics business got you a lot of unwelcome heat from the police that would interfere with your profitability. By that reasoning, perhaps the war on drugs did have a beneficial effect, but it operated indirectly on the mob boss. Who was in a position to know what was going on in his territory, who was responsible, and what methods might be effective in discouraging the trade. But that explanation assumes the worst possible motives on Bruno's part.
Let's at least consider the possibility that Bruno had a large streak of decency in him, and really didn't like the narcotics racket even if it cost his organization money to get rid of it. And got his head blown off when greedier folk decided to eliminate this obstacle to their prosperity.
So, by that analysis, you have the Philadelphia System for a drug-free city. A system of proven effectiveness, when every other proposal has failed. Just pass the word that nobody will bother you in your loan-sharking and bootlegging, just so the distribution of illegal drugs stops completely. How you accomplish this is up to you.
Computerizing Medical Care
Note: This article was written in 1999, long before Computerized Medical Insurance Exchanges were such a disaster:
|
| First Computer |
My first encounter with a computer was in 1958, and I have loved them ever since. As president of what called itself the Delaware Valley Hospital Computing Society, I remember giving a dinner speech concluding as follows: "If you want to be happy for a day, get drunk. If you want to be happy for a week, get married. But if you want to be happy for a lifetime, get a computer!" After fifty years, my affection continues. But to be candid, billions of dollars about to be spent on computers in medical care will mostly be wasted. Even worse, like malpractice suits computers will induce behavioral changes in the system costing far more than the directly visible costs.
That's unpopular news at present since the National Business Coalition for Health has launched a major lobbying campaign to persuade Congress to spend an initial billion dollars inducing physicians to maintain an electronic medical record. Various health insurance companies already provide financial incentives to doctors to file electronic claims forms, eventually threatening to reject any claim submitted on paper. The American College of Physicians has established a rather large department to develop programs for physicians to use in their practices; twenty years ago the University of Indiana started much the same thing. The College of Physicians of Philadelphia has spent close to a million dollars on such a project. It is reported that Microsoft Corp. has a massive project underway to supply electronic medical records. It sounds fairly easy to obtain large research grants from the government to devise something, anything, useful in this area. In my own case, training funds really weren't necessary, since I eagerly got into the field when everybody was a beginner. I was just as good a beginner as any other beginner. But let me repeat: the electronic medical record has been in the past and will be for decades, an expensive digression. In health care, creating more administrative work isn't the solution, it is the problem.
For fifty years the problem with an electronic medical record was that it took too much of the doctor's time to complete his part of the input, and then cost him too much to pay employees to do the rest. Presumably, automatic voice recognition and dictation will soon make it possible to record doctor's notes without handwriting or typing. Since, however, the elimination of current paper forms and check-off boxes will create a major problem in organizing the dictation verbiage, it could add five or ten additional years before programmers manage to rearrange dictation material and effectively integrate it into organized form, complete with laboratory results, dictated x-ray and EKG reports, even small images of the original material. Temperature, blood pressure, weight, photographs and the like can all be readily integrated into the stored electronic record, but to do so usefully is an expensive programming project. Doctors are quite right to be anxious they will lose control of the usefulness of their records in order to ease the task of programmers, speed up the sluggish pace of development, and reduce what will surely be an unexpected cost overrun. Storage and retrieval of such records is known to be an achievable but expensive task, which however also risks sacrificing the speed and ease requirements of the medical task it is supposed to serve -- in the name of cost-effectiveness.
Computers are no longer an unfamiliar tool; physicians have altogether too much experience with "vaporware", unrealized promises of convenience, and the damaging effect on the medical quality of the philosophy of Quick and Dirty. To respond to their resistance to design blunders with an accusation of undue conservatism is to provoke an icy stare and gritted teeth. Inevitably, the effective use of automation will require a redesign of workflow with major disintermediation of "gopher" staff; after all, that is how cost savings are to be achieved. That will provoke outcry that physician time is the most expensive component in the process, but unfortunately, physicians will discover Information Specialists with a business background will brush that argument aside. The most overpaid people on the face of the earth are investment bankers, but information consultants have persuaded business executives that inefficiency of the investment process is more expensive than even an investment banker's time. Having been through this themselves, insurance executives are unlikely to pay the slightest attention to physicians dancing to a familiar old tune.
For all that, data input is not the real problem; it's just the first problem. It's in a class with data storage and retrieval, which is expensive and cumbersome when you add a need for instant access and total privacy. But costs will come down steadily, and eventually, we can expect automated fingerprints or other biological identification, and cheap instant retrieval. Doctors will be able to make rounds in the hospital with a computer in their pocket, record telephone calls in their entirety, dial automatically and whatnot. There are problems with wireless transmission inside buildings with steel girders, and legal requirements for signatures on narcotic orders, but if we are determined, these problems can be overcome as easily as they were with electronic check writing and stock brokerage. Cost may top twenty billion dollars in twenty years, but it all can be done if we insist.
But then you encounter the real problem. Information will accumulate in these records in staggering amounts. Even if you resolutely resist demands to have the nurses record every groan, and the orderlies file every laundry slip, the legitimately important medical information will be exposed as the massive heap of transients that they really are. Plaintiff lawyers will insist no scrap of data may be deleted, hospital administrators will insist on compliance, when in fact most of a doctor's concentrated effort is devoted to brushing aside momentarily distracting data in order to see what's going on and react to it instantly. When a quick look doesn't solve the problem, the doctor goes back for additional data. If you disrupt these skills and traditions of coping with information overload, evolved over centuries, you will at best impose frustrating delays on a complex system under pressure, and ultimately inspire elaborate systems of short-cuts. The Armed Forces are famous for paperwork, but even they know better than to ask a pilot for his Social Security number as he starts a bombing run. The hospital nursing profession has already just about collapsed under paperwork pressure. If you see five nurses in a hospital, three of them will be sitting down writing something. The terrible truth is that no one reads it, no one checks it, and ultimately it sits in the record room waiting for a plaintiff lawyer with unlimited time to sieve out some misrecorded misconception or uninformed conclusion. My faith in the computer is such that I feel sure that methods can be devised to produce periodic summaries, automatic alarm signals, and mostly effective prioritization of data elements. Unfortunately, medical care is changing at such a rapid rate that ad hoc automation of physician thought processes cannot keep up with the current pace of change in medical progress. You would think some things would be unthinkable, but since I can remember the organized campaign to suppress the CAT scan as an unnecessary expense, I confidently predict that programmer inability to keep up with some advance in medical care will at times lead to organized outcry that we should slow down the pace of improving medical care, so that computer clerks can keep up with it. But that is only a small part of the issue, which at its center is that physician time will be dissipated and his attention distracted by presenting him with unwieldy amounts of neatly printed, spell-checked, encrypted and de-encrypted, biometrically secure, hierarchically prioritized -- avalanches of data which are irrelevant to the issues of the moment. The goal is not, after all, an electronic record. The local goal is to decrease the cost of medical care by increasing the productivity of the physician, and the overarching goal is high-quality patient care at a reasonable price. Behind all that, since the impetus comes from NBCOH -- the ones paying the insurance premiums -- suggests that the local goal is not so much the improvement of care as oversight reassurance that cares provided has been as good and as cheap as possible. The goal is legitimate, but this cybernation approach looks to be self-defeating by being overly specific.
If the reader has the patience for it, let me now cite a historical example of the third-party tail wagging the medical dog. In this case, third-party health insurance similarly overextended its reach by imposing internal health system changes, trying to facilitate the role of monitoring it externally. Specifically, the system of diagnostic code numbers was changed from one devised by the medical profession for its purposes, into a different coding system devised outside medial profession sponsorship, which seemed to suit the needs of payment agencies better even though it suited medical purposes less. After twenty-five years, it is now clear that third-party payers have shot themselves in the foot on this matter, and everyone is worse off. The topic, please pardon the obscurity, is the diagnostic coding system.
To go back to beginnings, the American Medical Association perceived a need for a diagnostic coding system in the 1920s. Organizing or even merely indexing vast amounts of information about a disease required more specificity than freestyle verbal nomenclature could provide. Quite a distinguished panel of specialists and consultants then produced the Standard Nomenclature of Diseases (SNODO) which in time became the Standard Nomenclature of Diseases and Operations. In order to reduce ambiguity, this system developed a branching-tree code design for anatomy, linked to a branching-tree for causes of disease, ultimately linkable to a branching tree of procedures. These three sets of three-digit codes linked the components together with hyphens (000-000-000). The first digit of each was the most general, as in Digestive, Musculo-skeletal, etc. and subsequent digits were progressively more specific and detailed, as in "Digestive, large intestine, sigmoid colon". The causes of disease would resemble "Infections, bacterial, streptococcal". An example of Procedures would be "Incision, incision, and drainage, drainage and insertion of the drain". In nine digits, it was thus possible to represent " incision, drainage, and insertion of a drain into a streptococcal infection of the sigmoid colon". After a while, the codes grew from three to five and six digits, again repeated three times, so an immensely detailed, unambiguous description might be coded in fifteen digits by a physician who knew the rules but didn't own a codebook. This code was ultimately taken over by the Academy of Pathology, expanded and is called SNAP. The pathologists absolutely refused to give it up.
The rest of the profession gradually yielded to the pressure of hospital administration, who was pressured by the Association of Medical Record Librarians, responding to the views of outside statistical interests, particularly insurance. A simpler, shorter coding system was needed, they felt, concentrating on the thousand most common diseases. The International Classification of Diseases was produced, reducing the millions of SNODO diagnoses to 999 by heavy use of several varieties of "Miscellaneous" or "Not Otherwise Classifiable (NOC)". Since the goal was to count the incidence of common diseases, the coding system was stripped of any logical tree-branching and became a short list of what was most common, starting with 1 and going to 999. In time, of course, the common-ness of conditions changed, and various complaints from various directions forced the ICD to go to 4 digits, then five. Unanticipated conditions or complications eventually required the patchwork of some alpha "modifiers", and the original short hodge-podge became a long and bewildering hodge-podge. Coding accuracy declined markedly, but ho-hum. The health insurance companies paid the bill, no matter what the code said. At another place, we will discuss the entertaining way that Ross Perot became a billionaire out of the computer chaos of Blue Cross and Medicare at this time, but right now the central theme to follow is DRG, Diagnosis Related Groups. Try to follow, please.
By 1980, Medicare was fifteen years old. It was clear that certain things just had to be changed because the excuse that the system was new and untried was beginning to wear thin. The early designers of the system based their payments on auditing a hospital's yearly costs, auditing the proportion of patients who were Medicare beneficiaries, and paying a proportionate share. That was easy and reasonably accurate, but it had a rather significant flaw that it took no account of whether the patients needed to be in the hospital in the first place. Or whether they needed to stay so long. The response they adopted (in the Budget Reconciliation Act of 1983) is a measure of just how desperate they must have felt. Knowing full well how inaccurate the ICD coding system was in practice, it was all there was. Consultants, particularly at Yale, ran computer simulations of various subsets of ICD codes to find a formula that would produce approximately the same hospital payments as the system of cost reimbursement. If memory serves, the original formula was to divide the thousand ICD codes into 27 diagnosis-related groups (DRG). Eventually, the process was tweaked to seventy or eighty groups. Walter McNerny, then Past President of the American Hospital Association told Congress hospitals could live with this system, and promptly we had a system for paying out hundreds of millions of dollars. It was touted as a highly sophisticated advance in the arcane science of hospital reimbursement, so it must have included a lot of deliberate overpayment. I can remember trying to remonstrate with McNerny, who felt he didn't have time for the discussion. Physicians had very little to do with the DRG portion of the 1983 Medicare Amendments because the AMA had long insisted that physicians and hospitals go their separate ways on reimbursement. Russell Roth, who was president of the AMA at the time, recounted many times the episode in the Oval Office, when it was announced to Lyndon Johnson that Dwight D. Eisenhower"was in the next room waiting for him. LBJ excused himself to leave, and on the way out said to Wilbur Cohen, "Give him anything he wants." Things were destined to change, but at least for a very long time, physician and hospital reimbursements were strictly independent.
Cost of Medical Care
|
| Milton S. Hershey |
On several occasions, Richard A. Kern M.D. (1891-1982) told the story of his part in the founding of the Hershey School of Medicine. Dick Kern was a distinguished professor of Medicine at Temple University, well known for his contributions in the field of asthma and allergy, a past president of the College of Physicians of Philadelphia, and a former Grand Master of Pennsylvania Freemasonry. The Milton S. Hershey School was considering the creation of a medical school and needed advice.
Milton Hershey had been a strict Mennonite, which is closely related to Quakerism, and had accumulated a huge fortune making chocolate candy. He left generous trusts to endow a theater and various other public services in the town of Hershey, but his ownership shares in the chocolate company had been left to the Hershey School for orphans. The value of the shares had far outgrown the ability of the school to employ them usefully, and they were considering a medical school. In 1963, as at present, everybody else was wondering how to get out from under the crushing cost of running a medical school. The sudden inquiry from a donor both willing and able to start a whole new medical school from scratch was an opportunity not likely to appear again soon. Kern carefully considered the options, including the danger of scaring off the naive potential donors with too high a price. Finally, he screwed up his courage and suggested a price to the trustees, of fifty million. The prompt answer was, done, you've got your medical school.
In due course, Kern found himself on the platform at the inaugural ceremonies of the school, sitting next to the guest of honor, that man who had made such an instant decision. Chatting amiably, Kern mentioned that he had always wondered how high the Hershey Foundation would have been willing to go. The answer was just as prompt as the original one. "Hundred-twenty."
Working Girls Get the Faints
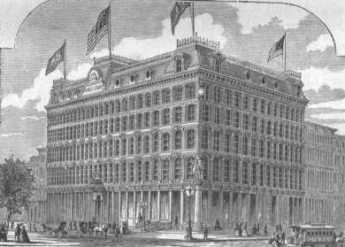
|
| Curtis Building |
Curtis Publishing Company once covered a full city block of Philadelphia, from Sixth to Seventh Streets, Walnut to Chestnut. The northern half of this complex was the Public Ledger Building, once housing a failed diversification move into newspaper publishing and later rented out as commercial office space after the newspaper died. On the top floor of the Ledger Building was the Down Town Club, quite a palatial meeting place for the whole publishing industry which stretched for blocks around. Both Curtis-owned buildings have the same architectural design and together make a massive looming presence next to Independence Hall on one street and Washington Square on the other. To build from Walnut to Chestnut means shutting off Sansom Street in the middle, and that permits the jewelry trade to nestle in a cul de sac on the West side of the publishing complex.
So Curtis was once a little city within a city, and most of the rest of the town only saw its facade and the crowds of people coming and going through the entrances. To a neighborhood doctor on an emergency call, however, it was almost exclusively inhabited by young women. Kitty Foyles, you might say. I certainly formed that impression after having a medical office two blocks away, getting occasional calls.

|
| Christopher Morely |
So far as I can remember, Curtis had only one medical problem, repeated over and over. An anguished call would come that someone at Curtis was unconscious, come immediately, take the elevator to the third or fourth or fifth floor. At the elevator, the doctor would be met by a somewhat older woman, obviously the den mother of the working girls. Into the ladies room, we would go, where a young woman was usually sitting on a couch looking sheepish, although occasionally she was still passed out. The key finding was a very slow pulse. She had fainted, she was better, and now what. It was Curtis policy to send the fainters home after the faint, and I never could see any particular objection to that.
For me, there were never any men to be seen, at Curtis. Surely there must have been dozens of writers and editors and advertising people, but somehow they would vanish when one of these fainting things happened. Curtis was nothing but women when I was there, mostly watching me like a beach full of seagulls, watching a fisherman.
Kenneth Gordon, MD, Hero of Valley Forge
There's no statue of Ken Gordon at Valley Forge National Park, although it would be appropriate. No building is named after him; it's probable he isn't even eligible to be buried there. But there would be no park to visit at Valley Forge without his strenuous exertions. One day, Ken's seventh-grade daughter came home from school with the news that the father of one of her classmates said that Valley Forge Park was going to be turned into a high-rise development. That's known as hearsay, and lots of things you hear in seventh grade are best ignored. But this happened to be substantially true. At that time, the Park was owned by the Commonwealth of Pennsylvania, and Governor Shapp was finding the upkeep on the Park was an expense he needed to reduce. The historic area had two components, the headquarters area, and the encampment area. One part would become high-rise development and the other would become a Veteran's Administration cemetery. Although any form of rezoning has the familiar sound of politics to it, Dr. Gordon (a child psychiatrist) had the impression that Sharp was mostly interested in reducing state expenses, and had no particular objection to some better use of the historic area. At any rate, when Gordon went to see him, he said that he would agree to a historic park if Gordon could raise the money somehow. The Federal Government seemed a likely place to start. Well, the sympathetic civil servants at the National Park Service told him how it was going to be. You get the consent of the local Congressman (Dick Schulze) and it will happen. If you don't get his consent, it won't happen. It seemed a simple thing to visit that Congressman, persuade him of the value of the idea, and it would be all done; who could refuse? After the manner of politicians, Schulze never did refuse, but somehow never got around to agreeing, either. It takes a little time to learn the political game, but after a reasonable time, the National Park employees told Gordon he was licked. Too bad, give up. He didn't give up, he went to see his Senators, at that time Scott and Clark. They instantly thought it was a splendid idea, and instead of going pleasantly limp, they sent Citizen Gordon over to see Senator Johnson of Louisiana, the chairman of a relevant committee. Johnson also thought it was a great idea, and called out, "Get me a bill writer!" A bill writer is usually a government lawyer, tasked with listening to some citizen's idea and translating it into that strange language of laws -- section 8(34), sub-chapter X is hereby changed to, et cetera. Bill writers have to be pretty good at it, or otherwise, they will misunderstand the intent of the original idea, modified by the personal spin of the committee chairman, the comments of the authorizing committee, and later bargains struck in the House-Senate conference committee. Having negotiated all those hurdles, a bill has to be written in such a prescribed manner that it won't be found to have multiple loopholes when it later reaches the courts in a dispute. A good deal of the time of our courts is taken up with making sense of some careless wording by bill writers. That's what is known as the "Intent of Congress", an ingredient that may or may not survive the whole process.
Ken Gordon had to go through this process, including testimony at hearings, for three separate congressional committees. To get everybody's attention, he organized several hundred supporters to write letters and get petitions signed by several thousand voters. These supporters, in turn, influenced the media and started a lot of what is known as buzz. All of this is an awful lot of work, but there is one thing about this case that can make us all proud. Not once did a politician suggest a campaign contribution was essential in this matter. In time, ownership of the Park did in fact migrate from the Commonwealth to the U.S. Department of the Interior, hence to the National Parks Service. Everyone agrees it has been well managed, and increasing droves of visitors come here every year. It is now clearly a national treasure. Unfortunately, the encampment area got away and has been commercially developed, although not nearly as high-rise as originally contemplated. Along the way, many discouraging words were spoken about the futility of fighting against such odds. The outcome, however, is the embodiment of two slogans, the first by Ronald Reagan. "It's amazing what can be accomplished, if you don't care who gets the credit for it." The other slogan is older, and Quaker. All you need, to accomplish anything, is leadership. And leadership -- is one person. One day Ken Gordon, the very busy doctor, was asked how much of his time was taken by this effort. His answer was, ten hours a week, every week for five years. Money BagsThis little morality tale was told to me by two unrelated sources, one of whom was a staff aide to Wilbur Cohen, the author of the Medicare law. And the other was a high official of Pennsylvania Blue Shield, the appointed administrative agent for Medicare in Pennsylvania. Its relevance to the more recent SNAFU with Insurance Exchanges introducing the world to Obamacare should be fairly obvious. After Lyndon Johnson rammed the Medicare amendment to the Social Security Act through Congress in 1965, he wasn't shy about drawing attention to it. The press was present in great numbers, with staff officials who had a role in crafting the document, members of Congress, and anyone else who was standing around. The legislation was laid before him and signed with twenty different pens to be presented as mementos to the in-group. Each pen was only used to inscribe about half of one letter of his name, so it was a slow but joyful process. As intended, it got lots and lots of publicity.
So, thousands of thankful old folks saw the ceremony on television, though they heard that the law was in effect immediately, and proceeded to dump their medical bills into a shoe box, sending them to Medicare to be paid. Unfortunately, Medicare didn't have an office, a staff, or even a telephone number. These things take time. As fast as they could, the Medicare staff constructed a system of carriers and intermediaries, carriers for part A, and intermediaries for part B. And almost without exception, appointed the local Blue Cross and Blue Shield organizations to be the carriers and intermediaries. Consequently, the organization of Medicare was patterned closely after the organization of the two administrative corporations. Meanwhile, the bills from old folks just kept pouring in through the postal service. It was about all the staff in Washington could do, just to direct the mail out to the local intermediaries and at least get it out of their hair. Less than a year later, that's how the claims manage to Camp Hill, PA, a little suburban town near Harrisburg. In desperation, Blue Shield had rented a local vacant supermarket and piled the mailbags ten feet high. There were quite a few telephone calls of inquiry, and the old folks were politely told the matter was being looked into. It was beginning to look as though one supermarket wasn't big enough. Computers were, of course, rented from IBM, who had a policy of renting, not selling, its valuable equipment. Keypunch operators, computer operators were hired, air conditioning was installed, and one team after another of computer programmers was hired -- and fired. Consultants were called, scratched their heads, sent big consultation bills, and turned sadly away. Sorry, but somehow it just doesn't work. So that's how it happened that one Friday afternoon, a vice-president of Texas Blue Cross named H. Ross Perot came in, accompanied by a fellow with glasses so thick they looked like the bottom of Coca Cola bottles. So far as anyone can remember, the guy with coke-bottle glasses never said one word. The desperate, hopeless mess was explained to Perot, whose salary at that time was rumored to be twenty-five thousand dollars a year, about right for a Blue Cross executive. His background as a kindred Blue Cross person inspired confidence, and the conversation rambled on for an hour or so. Meanwhile, the guy with coke bottles went over to the Penn-Harris Hotel across the street and got to work. By the end of the weekend, he had come back a couple of times, but eventually, would you believe, it really, well it really worked. Contracts were quickly signed, the wheels began to turn, the mailbags in the supermarket began to march through the processing cycle. Blue Shield, the Medicare program, the finances of the nation's elderly, and Lyndon Johnson's reputation -- were all rescued. As everyone now knows, the Medicare processing contracts made Ross Perot into a billionaire, living on Bermuda in the lap of luxury, eventually upsetting the re-election hopes of George Bush, senior by running for President himself on a third party ticket that had something or other to do with giant sucking sounds. A Congressional investigating committee looked into the outrageous profits Perot had extracted from his homeland's elderly, volleyed and thundered. Whether Perot actually thumbed his nose at them is doubtful, but he certainly was in a position to do so. Meanwhile, whatever happened to that guy with the coke bottle glasses, no one seems to know. Nobel Prize: Michael Brown, MD
The College of Physicians of Philadelphia annually sponsors a lecture by a winner of the Nobel Prize in Medicine or Physiology. There is never any doubt of the high quality of any such lecture, but it does add an element of local pride whenever the Nobel Laureate comes from Philadelphia, as he did this year. Michael S. Brown, MD graduated from Cheltenham high school in 1958, received a B.A. from the University of Pennsylvania in 1962, and his M.D. degree in 1966. Nineteen years later, he was awarded the Nobel Prize in Medicine for his work in describing the cholesterol pathways, and the human defects in it which lead to heart attacks, strokes and other consequences of atherosclerosis. Almost immediately, Japanese investigators found the so-called stain drugs being produced by relatives of the penicillin mold for no, particularly obvious purpose. The patents have not yet expired on most of these drugs, but many millions of people have already been spared death or disability from hardening of the arteries, the commonest killer in modern life. The speaker, now a gastroenterologist practicing in Texas, chose to organize his talk around the manner in which biochemical discoveries are currently being made. Physicians in medical research endure news media presentations, usually in silence, of scientific research performed by basic scientists with Ph.D. degrees, with MDs then merely dispensing the drugs. It sometimes happens that way, but in general, the basic scientist is too highly focused on the techniques of the scientific cutting edge to be well positioned to see the direction that should be taken next. The physician-scientist, on the other hand, is aching to find a solution to current problems, but often lacks the necessary technical skills to perform the experiment. James Shannon, one of the early directors of the National Institutes of Health, recognized this mutual deficiency was impairing progress and set about establishing training programs for cross-fertilization between the scientific approaches. Dr. Brown was one of the early trainees of that program, and now describes its glories, going from the patient bedside to the scientific laboratory bench, and then back to the bedside to test the results. Competition has morphed into collaboration. Some day, someone will conduct a study of Nobel Laureates, seeking out the traits which characterize them. The next step after that would probably be cloning them, although public opinion will first have to catch up with that thought. From an observers point of view, Nobel prize winners all seem gifted with the ability to give a logical, entertaining and succinct description of a complicated matter. Almost all of them are located in very large research environments, where news of small scientific discoveries in obscure scientific journals is quickly picked up by a hundred eyeballs, filtered for the benefit of the local enthusiast of the topic, and often fitted together with something which that enthusiast has discovered but not published, or published too recently to be well known. Research is not just expert marksmanship, it is marksmanship within a boiling cauldron of undigested facts. One other thing about Nobel Laureates: as a group, they tend to drive over the speed limit, even when going to the local supermarket. Anyway, it's really nice to take the statin drug and watch your cholesterol go down, secure in the knowledge that invisibly your longevity is improved. There's just nothing more attractive than having more longevity. At least, it's hard to imagine what would ever replace it in attractiveness. House that Love Built: Ronald McDonald of PhiladelphiaKim Hill had the misfortune to develop leukemia, but the great luck to have Fred Hill of the Philadelphia Eagles football team for a father. Driven by gratitude for the treatment at St. Christopher's Hospital for Children
Fred demanded to be told what he could do and was referred to Dr. Audrey Evans. This world-famous pediatric oncologist was well known for her philanthropic activities and had frequently expressed the need for a temporary residence for families of children needing protracted medical treatments. Young children have young parents, whose savings are soon exhausted by travel, hotel and other non-insured costs related to a seriously sick child. The Hills had just been through such an experience and grasped the problem immediately, adding to it the discomfort and loneliness of families in such a situation. Fred Hill quickly enlisted the enthusiastic support of the whole professional football organization, and Jim Murray the Eagles' general manager recruited Don Tuckerman from their advertising agency, who got to Ed Rensi, the regional manager of McDonald's. Together, they got the project financed and started with a seven-bed facility near Children's Hospital of Philadelphia.
In 25 years, the Philadelphia Ronald McDonald House has grown to a capacity of 44 families, in a century-old mansion at 39th and Chestnut Streets filled with Mercer tiles and the like. The operation uses eighteen volunteers at all times, runs two jitney buses, and is one huge teeming family home for people confronting a common issue, supporting each other through a wrenching emotional experience. Although it actually costs about $65 a day per family, the charge is $15 and over half of the clients cannot afford even that. Although an effort is made to have family cooking, the McDonald's restaurant chain supplies 20% of the budget along with generous help with exigencies and in-kind assistance with such things as clowns for the entertainment program, birthdays and the like. Although McDonalds's is probably the world's premier franchising corporation, every one of the 300 worldwide Ronald McDonald Houses is an independent local organization, run without a central headquarters or any sort of standards-setting and the like. Every one of the other 299 Houses got the idea from Philadelphia but proceeds in its own way. Philadelphia created it, but Philadelphia does not own the idea. In this connection, it is probably worth reflecting on the history of this topic. When Benjamin Franklin and Dr. Thomas Bond started the Pennsylvania Hospital in 1751 at Eighth and Spruce Streets, it was the custom to be diagnosed, treated, be born and to die in your own house. The unique perception behind the nation's first hospital was that poor people generally did not have home facilities that were adequate to support home care. In Franklin's own handwriting the purpose of the Pennsylvania Hospital was stated to be "for the sick poor, and if there is room, for those who can pay." It was understood that poor sick people needed a place to take care of them, not merely for their surgery and overwhelming illness, <but for convalescence and rehabilitation as well. Two centuries later, in the first thrill of founding the Medicare and Medicaid programs, it was imagined that things would remain exactly the same, only paid for by the Government. But after four or five years, it became abundantly clear that it was far too expensive to use hospitals in that way. The very act of federally paying for the program undermined its volunteer spirit, raised its mandated standards, and made it financially unsustainable. And so, although the 1965 Amendments to the Social Security Act insisted, and still pretend, that no change was to be made to the delivery of care, the delivery of care simply had to be changed. Not only was domiciliary and custodial care to be excluded, but heroic efforts were to be made to reduce the length of stay in the hospital to what would once have been regarded as special intensive care. In effect, if a type of service could normally be handled at home by non-indigent people, it was to be prohibited for everybody. Since the cost of care in hospital has continued to escalate far in excess of the cost of living, it seems unlikely we will ever go back to the days of rest and in-hospital recuperation. So, just as Dr. Bond recognized the problem and went to Ben Franklin to handle the philanthropy, Dr. Evans had the idea and Fred Hill made it work. Around the Ronald McDonald house, the idea is frequently heard expressed that every hospital needs such a place nearby, for people of all ages. Perhaps that is workable, but it offhand seems more likely that Retirement Villages, so-called CCRC, will be called on to supply this badly needed service, at least for senior citizens. And that what we now call hospitals will evolve into the scientific "focused factories" so popular in the minds at the Harvard Business School. Getaway
Occasionally prisoners must be taken to the hospital, and that's a problem for the authorities. Philadelphia General Hospital had a special prison unit on its grounds, so the problem for the guards was merely to transport the prisoner to the locked hospital ward and bring him "home" after his medical problems were fixed. The State of Delaware doesn't have a prison unit in any hospital, so the security risk must be addressed by sending at least two guards, night and day, to some hospital, and securely manacle the prisoner to the bedstead. Nobody likes this situation, particularly the head nurses, but no one has a better solution to offer. When prisoners have to make an outpatient trip for an x-ray or similar, there is usually an iron rule: no one is to know about it in advance. In one particular case, however, a convicted Delaware murderer had to have an x-ray of his gallbladder, which in those days required swallowing some large pills the night before. That was the tip-off. On the specified morning, he was bundled into a patrol car with manacles and guards, and whisked off to the Delaware Hospital, now the Delaware Division of the Wilmington Medical Center. The x-ray department was at the end of a long corridor, with the diabetic clinic on the right and the bathrooms on the left side of that corridor. The entrance was on the side of this corridor, right next to the office for visiting consultants. Things were busy but peaceful that morning when a commotion arose. Three prison guards came marching through the door, surrounding their manacled prisoner. They turned left, and down the long hall to the x-ray department. As they passed the men's room, the prisoner begged his guards to let him relieve himself, so they took him into the bathroom, removing the handcuffs. He washed his hands, dried them with a paper towel, pushed it into the waste container. Then quick as a flash he thrust his hand deeper into the crumpled waste paper, got the loaded revolver his accomplices had put there, and emerged from the wastebasket -- shooting. The guards got down on the floor, a bullet went into the Diabetic Clinic were a very prominent society lady was working in a pink volunteer's uniform, and another bullet went into the consultants' office, which on other days I might have been using. The escapee was running hard, fired one final bullet into the ceiling at the door, and was out in a second to the waiting getaway car where his buddies were ready. He got away clean, as they say. There's nothing like an episode of that sort to bring people together. We were survivors of an exhilarating experience, having something in common that no one could take away. For a couple of years afterward, the bullet hole remained unobtrusively in the ceiling by the entrance. The nurses told me that workmen had arrived several times to patch it up, and the society lady, who was a trustee of the hospital, wouldn't let them fix it. That was our bullet hole. Radioactive River Bend
A mile or two south of Pottstown, the Schuylkill River encounters a rocky ridge several hundred feet high and makes a bend around it. The first Treasurer of the United States, Michael Hillegas, built a colonial mansion on the point of the bend, and it has been lovingly restored and preserved by a noted Philadelphia surgeon and his wife. Alexander Hamilton, the first Secretary of the Treasury under the Constitution, has his picture on the modern version of a ten-dollar bill. So it is appropriate that Hillegas, the first Treasurer under the Articles of Confederation, had his picture on many versions of a ten-dollar gold note, back in the days when the American dollar was as good as gold. River Bend Farm is not only colonial, charming and maintained in mint condition, but it is also tucked away between the bend in the river and the high ridge to one side, giving it seclusion and privacy. A high ridge near a river is unfortunately also an ideal place to build a nuclear power plant, and that's where the Limerick plant now looms up, glowing at night, occasionally making faint humming noises. There's a limited-access highway from Philadelphia to Reading which swoops up the valley, and the two high cooling towers of Limerick dominate the landscape for twenty miles. Because of the river bend, you aim straight for those towers for a long time before you swerve off, and the view is much like that from the bomber cockpit of the final scene in the movie "Dr. Strangelove". It gets your attention harmlessly, but it's hard to ignore. In spite of all sorts of official reassurance, everybody knows about Three-Mile Island, and Chernobyl, but few people emphasize there has never been a single injury from an American nuclear plant. So, in 1981, everybody was ready to go into orbit when a worker named Watrus showed up for work at the nuclear plant and set off all manner of clanging alarms from radioactivity detectors. Panic and pandemonium for weeks, until a remarkable phenomenon was discovered. Watrus wasn't radioactive from the nuclear plant at all, but from having his work clothes laundered in his own basement. It slowly developed that radon gas seeps through the ground in many places in the United States, particularly over rocky ground. The gas then rises into the basement of houses and gets trapped. The more tightly the storm windows are applied and the more carefully sealed the seams of the house, the harder it is for the radon to escape. The Pennsylvania Dutchmen who live around Limerick are a little skeptical of this story and are not inclined to live any closer to the power plant that they have to. They are just as much in favor of oil self-sufficiency as anyone else, but still, no one likes being close to it. The big winners from all this confusion are the people with radiation detectors, who go around the country testing people's basements for radon, for a fee. But unless you are willing to go live on the Sahara Desert, it isn't easy to see where you are going to go to avoid radon. Inscrutable ChineseDinner With Hoffa
Although she lived for twenty more years, in 1975 my mother was eighty years old. Nevertheless, she did not display the slightest surprise, or hesitation in answering, "Sure", when asked if she would like to have dinner with Jimmy Hoffa. One of her constant pleasures was to be doing things that other women couldn't match. The Philadelphia County Medical Society's Center City branch was having dinner, and the program chairman had the main goal in life of attracting speakers who would bring an overflow audience. Jimmy Hoffa, the former president of the Teamsters Union, recently released from prison, certainly filled that description; one of the members of the branch had a patient who was a teamster official who happened to know that Jimmy would love to speak to the doctors about medical care in prisons. Not only was he willing, but he also paid his own expenses to fly up from Florida to give the speech. As by far the oldest lady present, my mother was not to be denied when she demanded to be seated at the head table. Hoffa was indeed a charming person and an able proponent of his cause. He had experienced medical care in a prison, he felt mistreated, and the doctors in the audience were sympathetic to what they suspected was quite true. They generally began that evening with conflicting opinions, because it is generally known that doctors in the prison environment are often threatened, and occasionally harmed. We know quite well how reluctant the Legislature is to spend one cent on a group of people they dislike, and how they all wish the problem would just go away. By the end of the evening, Hoffa held his audience in his hand. No wonder he rose to the top of his organization. Well, the impact of the evening was certainly heightened, even in my mother's view, by the fact that two weeks later Hoffa just disappeared, and there have been hundreds of books and articles written about his probable grisly murder by the Mafia. The latest is called I Heard You Paint Houses, in which one Frank Sheeran is quoted as claiming, or even boasting, that he had been the hit man. I wouldn't know. The title, however, is reliably known to refer to all the blood which is found splattered about, following a mob rub-out. Calling them wise guys is quite apt. The reawakening of this topic by the book does raise some other old questions of the highest rank. Reviewing the evidence, it is possible to believe Hoffa was not guilty of precisely what Bobby Kennedy was accusing him of. At least, the prosecution failed to convince one jury of it. The FBI records do seem to indicate that J. Edgar Hoover offered him evidence of the questionable Kennedy private lives, which Hoffa refused to use in his defense in the trial. And there seems to be little doubt that he worked hard to elect Richard Nixon, or that Nixon later commuted his sentence. Generally speaking, he was on the side of the angels concerning Mafia influence in the Teamsters Union. But his strange relationship to Nixon and the Kennedy family is quite another matter, although equally obscure. Philadelphia in 1976: Legionaire's Disease
No other city in America is remembered for an epidemic; Philadelphia is remembered for two of them. The Yellow Fever epidemic, for one, that finished any Philadelphia's hopes for a re-run as the nation's capital. And Legionnaire's Disease, that ruined the 1976 bicentennial celebration. One is a virus disease spread by mosquitoes, the other a bacterial disease spread by water-cooled air conditioners. Neither epidemic was the worst in the world of its kind, neither disease is particularly characteristic of Philadelphia. Both of them particularly affected groups of people who were guests of the city at the time; French refugees from Haiti and attendees at an American Legion convention. In 1976, dozens of conventions and national celebrations were scheduled to take place in Philadelphia as part of a hoped-for repeat of the hugely successful centennial of a century earlier. Suddenly, an epidemic of respiratory disease of unknown cause struck 231 people within a short time, and 34 of them died. Every known antibiotic was tried, mostly unsuccessfully, although erythromycin seemed to help somewhat. The victims were predominantly male, members of the American Legion of a certain age, somewhat inclined to drink excessively, and staying in the Bellevue Stratford Hotel, one of the last of the grand hotels. Within weeks, it was identified that a new bacterium was evidently the source of the disease, and it was named Legionella pneumophila. Pneumophila means "love of the lungs" just as Philadelphia means "city of brotherly love", but still that foreign name seemed to imply that someone was trying to hang it on us. Eventually, the epidemic went away, but so did all of those out-of-town visitors. The bicentennial was an entertainment flop and a financial disaster. Since that time, we have learned a little. A blood test was devised, which detected signs of previous Legionella infection. One-third of the residents of Australia who were systematically tested were found to have evidence of previous Legionella infection. A far worse epidemic apparently occurred in the Netherlands, at the flower exhibition. Lots of smaller outbreaks in other cities were eventually recognized and reported. It becomes clear that Legionnaire's disease has been around for a very long time, but because the bacteria are "fastidious", growing poorly on the usual culture media, had been unrecognized. And, although the bacteria were fastidious, they were found in great abundance in the water-cooled air conditioning pipes of the Bellevue Stratford Hotel. Even though the air conditioning was promptly replaced, everybody avoided the hotel and it went bankrupt. When it reopened, 560 rooms had shrunk to 170, and it still struggled. Although there is little question that lots of other water-cooled air conditioning systems were quietly ripped out and replaced, all over the world, the image remains that it was the Bellevue, not its type of plumbing, that was a haunted house. There is even a website devoted to its hauntedness. Contemporary GermantownThe Strittmatter Award is the most prestigious honor given by the Philadelphia County Medical Society and is named after a famous and revered physician who was President of the society in the 1920s. There is usually a dinner given before the award ceremony, where all of the prior recipients of the award show up to welcome to this year's new honoree.
This is the reason that Henry Bockus and Jonathan Rhoads were sitting at the same table, some time around 1975. Bockus had written a famous multi-volume textbook of gastroenterology which had an unusually long run because it was published before World War II and had no competition during the War or for several years afterward; to a generation of physicians, his name was almost synonymous with gastroenterology. In addition, he was a gifted speaker, quite capable of keeping an audience on the edge of their chairs, even though after the speech it might be difficult to recall just what he had said. On this particular evening, the silver-haired oracle might have been just a wee bit tipsy. Jonathan Rhoads had likewise written a textbook, about Surgery, and had similarly been president of dozens of national and international surgical societies. He devised a technique of feeding patients intravenously which has been the standard for many decades, and in his spare time had been a member of the Philadelphia School Board, a dominant trustee of Bryn Mawr and Haverford Colleges, and the provost of the University of Pennsylvania. Not the medical school, the whole university, and is said to have been one of the best provosts of the University of Pennsylvania ever had. When he was President of the American Philosophical Society, he engineered its endowment from three million to ten times that amount. For all these accomplishments, he was a man of few words, unusual courtesy -- and a huge appetite in keeping with his rather huge farmboy physical stature. On the evening in question, he was busy shoveling food. "Hey, Rhoads, wherrseriland?". Jonathan's eyes rose to the questioner, but he kept his head bowed over his plate. "HeyRhoads, Westland?" The surgeon put down his fork and asked, "What are you talking about?" "Well," said Bockus, "Every famous surgeon I know, has a house on an island, somewhere. Where's your island? "Germantown," replied Rhoads, and returned attention to his dinner. National Business Coalition on Health
In 1992 the National Business Coalition for Health was just forming at a convention in Chicago. Before I really understood what it was all about, I agreed to their flattering invitation to be the keynote speaker at the kick-off luncheon. Who suggested my name was and is a mystery to me, and I arrived in Chicago with very little idea what they wanted to hear. However, it followed the familiar pattern of inviting the speakers to stay overnight at the hotel on the evening before the meeting began and to meet for drinks at the bar with the organizing leaders. I had enough experience with public speaking to know I could learn the general slant of the thing at such an informal party and adjust the speech to the audience to whatever degree seemed needed. Among the people scattered around at tables was Harry Schwartz, who was also there to give them a speech. Harry had been on the editorial board of the New York Times for many years and was known to be generally quite favorable to physicians. We had both written books about medical care, The Hospital That Ate Chicago in my case, and The Case for American Medicine, in his. We liked each other immediately and fell into an animated cocktail conversation that would eventually be renewed every six months at the American Medical Association House of Delegates meetings, where I was a delegate and he covered the topic for various news media. As we chuckled together about one anecdote or another of medical politics, the bar gradually emptied out. It soon became clear that all the other cronies had wandered off to dinner together, so we ordered dinner on the house, neither one of us have learned just what we were there to talk about. It really didn't bother either one of us very much, since from long experience we could tell some jokes and make it up as we went along. I knew what I wanted to tell businessmen, so it was just a matter of finding a way to lead into it. The speech seemed to go well. There were several hundred, perhaps even a thousand in attendance, quite convivial and prosperous. As executives usually do, they looked younger than you might expect from the titles on their name tags; they laughed at the appropriate points and applauded at the end. In other words, I went home from Chicago with no more idea what this organization was up to than I had before I came. At the very least, it is clear they were forming a national organization of businesses, with constituent representatives largely drawn from Departments of Human Resources. They wanted to speak for American Business with a more or less unified voice, and the topic seemed to be health care. Although fate had put me into the debate at the very earliest moment at Wills Eye Hospital, this convocation of extroverted Republicans seemed to know a lot more than I did about what was secretly afoot among the Democrats in Washington. This Chicago tea party did one other thing for me. Many months later, when the editors of USAToday were in search of an editorial page writer who was both a physician and opposed to the Clinton Health Proposal, they called Harry Schwartz. And he suggested to me. They ultimately ended up with a Medical Editorial Advisory Board of five members, at least three of whom were far to the left of me. At the New York Times, of course, Harry Schwartz was considerably more outnumbered than I was. After it was over, Harry and I used to joke that both sides were fairly evenly matched. Equal Pay for Equal Work
The House of Delegates of the American Medical Association holds a five day convention twice a year. The meetings last from 7 in the morning until midnight, although the main sessions in the auditorium only last eight hours a day for three days. The rest of the time is consumed with meals, committee meetings, geographical caucuses, and even cocktail parties. Newcomers often object to the numerous parties until they come to see that these are merely committee meetings in a different form, with different subsets of the organization picking up the necessary costs. This group of workaholics has to vote on several hundred issues each session, and most Delegates have little advance opinion when they enter the headquarters hotel on the first day. But after meeting with their specialty in one committee, and members of their geographical region in another, and members of their medical school alumni association in yet another, and with issue-oriented groups, political allies, and other layers of an overlapping matrix day after day -- by the time the vote is actually called for, most Delegates could safely predict the correct outcome with very few exceptions. The AMA works at its similar job with far greater intensity than Congress does because Congress has all year to do it, while the doctors have to go home to make a living. Don't worry about the parties, they are really working sessions for everyone except rank newcomers, outsiders, visitors, and wives. What is perhaps more worrisome is the rare occasion when just about every delegate arrives with one opinion and is persuaded by the leadership to adopt the reverse. That can only happen if new information is suddenly revealed, with little time to check its accuracy. There are usually fifteen or so parties every night, hosted by large state delegations, large specialty assemblies, and coalitions of smaller groups. Fifteen drinks a night would be quite a bit for most folks, and some newcomers are duped into trying to be polite about it. The rest of us take the proffered drink, walk over to a nearby plant stand and dump it. I hate to think of how many potted palms I have fried that way. Each delegation has its own system of organizing these minutes, and I'll try to describe the Pennsylvania system. Nobody will come to your party if you don't go to theirs, so we make a list and divide the group into those who "travel" to the parties of other states, and those who remain to host our own party, "at the door". Everyone is expected to wear a name tag, containing your name in large type underneath which is your caucus designation, in my case "Pennsylvania". The older members instruct the newer ones to put the name tag just under their right shoulder. That way, you can seem to be looking at the hand you are shaking while freshening your recollection of who in the world you are meeting. You can, of course, do anything you please, but time is short for the transaction of a lot of business, and it's just easier to do routine things the regulation way, and get on with it. On the evening in question, I was "at the door". The formula, repeated many times, was to extend a hand of greeting and recite, "Welcome to Pennsylvania. Are you looking for some friend in particular? Let me see that you have a drink. Come on in and meet my fellow delegate, Scotty Donaldson." You can shepherd a lot of people more or less gracefully if you reduce the formalities to a routine. After several people had been brought in under the tent, a man with highly polished shoes came up, wearing a name tag that said, "Blue Cross of America". He was greeted, his hand pumped, a drink procured, and was introduced to Scotty, our most famous extrovert. I quickly turned to the next person at the door. Well, this lady was six inches taller than I am, and fifty pounds lighter. She wore a name tag, identifying her as President of some Nurses Association, "Welcome to Pennsylvania! Is there someone from Pennsylvania you know or would like to meet? Can I......" The apparition didn't even look at me as she brushed past through the door. Heading straight for the gentleman from Blue Cross, she poked her index finger into his chest, stopped him in mid-sentence as he talked to Scotty. "What I want to know, " she announced to this startled man, "Is when are you people in Blue Cross going to pay nurses as much as you pay doctors?" And here I must admit I have to give this guy credit for unperturbability. "Well, madam," he said cheerfully, "I think that's going to be quite some time." A New Gorilla in the Cage
News reports began to surface that big business was talking to Democrats in the White House about major revisions in the national health delivery system. That in itself was news, because big business normally forbids its employees to talk with regulators, and does not commonly welcome any new regulations. But the Clinton Administration was looking for political allies, while the business community was willing to examine proposals to lighten the burden of employer-based health insurance. The discussions soon probed whether a common system might reduce government costs of Medicare and Medicaid, and simultaneously reduce the costs of employer-paid health insurance. For years, big business had been suspicious that the health community had somehow forced employers to pay an unfairly large share of other people's health costs, through some arcane manipulation of hospital cost accounting. Their term was cost shifting. The administrators of government programs believed the same thing was happening to them. Since the only group left to benefit were uninsured, the arithmetic was somehow wrong. A 7% population group, most of whom are young and healthy, could not account for annual premium jumps far in excess of the cost of living, occasionally as much as 30% in one year. In both governmental and business minds, the main beneficiaries of cost-shifting must be the hospitals themselves, and the doctors who control them. Somehow, it seems not to have occurred to them that this news was brought to them by their fiscal agents, the health insurance companies, and was therefore likely slanted to avoid attention to middle-man costs. Whenever major negotiations are to be held, CEOs and top politicians take over to make the deals, necessarily basing their judgments on filtered information. Since this is a familiar situation, they employ high-priced consultants.
The five hundred secret members of Mrs. Clinton's task force were willing to listen to the ideas of anyone who had political clout, especially staff members of Congressional committee chairmen. But these people had been struggling with the problem for fifty years to no avail, so the emphasis had to be on change, on big new ideas. Universities and think tanks were especially welcome to comment, and Clark Havighurst was particularly influential. But there had to be some kind of track record, some practical experience on which to base such an enormous national initiative. The best available model was the Health Maintenance Organization (HMO), whose most famous proponent was Paul Ellwood, a former midwestern pediatric neurologist who had gravitated into health insurance consulting. Ellwood had a vacation home in Jackson Hole, Wyoming, where he then gathered the non-government component of this movement into his front parlor. Insurance companies, human resources officials, academics, and in later stages the news media, were given the Word, an opportunity to criticize, and an opportunity to have their views coordinated with the government group in Washington. There was a rough division of labor, establishing general regions of dominance; but ultimately, the two components intended to fit together in a unified health system for the whole country, bar none. The business community began to see that inevitably, in that case, the final overarching decisions would be made in Congress. Be Careful What You Wish For
Events at the time of the introduction of the Clinton Health Plan to Congress were a confused jumble, but one vignette stands out in my memory. The five hundred or so members of the secret work group were all invited to the White House for a big party, with saxophones and all. On a television interview at home in Minnesota, Paul Ellwood said he wasn't going to the party. Indeed, he looked rather morose and had little to say. It is clear he had advance notice, before the plan even reached Congress, that things were not going the way he wanted. Since the public, even Congressional leaders, were still unclear just what was to be proposed, Ellwood's dejection, or rejection did not come from them. No one has said so, but it must be presumed the rejection came from his sponsors, the business leaders. Business, in short, had pulled out; responsibility probably lies with no more than half a dozen CEOs who continue to be anonymous fifteen years later. At that confusing time, the reasoning of the masterminds was obscure. Perhaps they decided HMOs were no good; perhaps an outrageous political demand had been linked to the proposal; or there was to be too much political control, too little business control; or perhaps government costs had been shifted onto the backs of employers; perhaps the whole idea sounded too leftist to be comfortable. And perhaps a lot of other things, who knows. Even today, no one has written a book or even listed a few plain sentences of reminiscence. What is known is that major business employers immediately launched a nationwide initiative to go ahead with a strong push to convert employer-based plans from fee-for-service to managed care HMOs. This was to be the way employers handled health care they were paying for; the government could do as it liked. It must be admitted it was a bold stroke, quite effectively handled. When you consider the rather uncertain legal right they had to impose a system of health care on their employees, it took more audacity to go ahead than you would suppose they could summon. It was a gamble that the Clinton White House would lack the courage to challenge a private initiative to go ahead with what they had so publicly endorsed, and that providers would be so surprised by the concerted coup that they would hold back legal challenge until evidence of antitrust or conspiracy emerged. It was a sort of Battle of the Bulge in reverse, and it might well have been hugely successful except for one thing they did not anticipate. Their employees almost universally hated HMOs when they tried them out. No one likes to be hustled into something he doesn't understand, no one likes to change doctors, no one like to be told he can't have what he expects to have. Employers expected resistance of this sort, but it simply had to be done to save the fiscal health of the business. Unfortunately, what emerged was that it didn't save much more money than its own extra cost to administer. The hard reality of business life is you regularly have to bully people in order to make any money. But bullying people without making any money is a quick route to dismissal. No wonder there have been no memoirs written. A quick re-appraisal of the Clinton Health Plan was that the two systems, Medicare for people over sixty-five and employer-based for people under sixty-five, were to be merged into a single system for efficiency and better control. There were to be local, regional, and national governing bodies; evidently, the purpose of the National Business Coalitions for Health was to supply a unified business hierarchy to match it up and down the line. Hated politicians, hated bureaucrats and hated unions could be counted on to apply strong pressures; business would have to remain well informed, sternly disciplined, and speak with a single voice for any hope of surviving in such an environment. It is my surmise that such a prospect seemed to guarantee failure for a business. No, we're sorry, Business would draw a bright line at age sixty-five, and run its own show where it ruled the roost. Nowheres-ville
In more recent writings, Jacob S. Hacker seems obsessed with social inequality, but while he was a graduate student he wrote an excellent and objective book, The Road to Nowhere containing unique insights into the politics of the Clinton Health Plan of 1993. After that hubby was over, he interviewed most of the important actors in that drama, at least those active in the liberal politics of it, and they talked freely. Like the rest of us, he was unable to identify let alone talk with the leaders of big business, who are of course still pursuing their original goals. What emerges does sound roughly accurate; Hillary Clinton and Ira Magaziner designated to find out what this health business was all about; solicit every proposal on the mind of political, particularly congressional, allies; gather and examine all the useful ideas in circulation in academia and the insurance community; and negotiate possible solutions with a surprising new ally, the big corporate employers. A huge semi-secret task force was then assembled to exchange ideas, discard really bad ideas, and work the proposal into legislative form. There would be internal inconsistencies and conflicts but no matter.
Congress would work it out, differing versions would appear in House and Senate bills, and President Clinton himself would eventually be able to intervene when things got to the House-Senate Conference committee. Since the Clintons really had no pre-conceived ideas on this complicated topic, the will of the people would emerge from a huge debate, and the will of the people would prevail. That's one version. The other way to picture this circus would be that a highly skilled politician would offer everybody a chance to propose pet projects, and those who failed adversary process would be obligated to support the ones who did prevail. Trade-offs would be made, as needed, and the political ringmaster in the White House would have the final say. But the final version was the one that came through to the public and the leaders of big business. You weren't going to know what the plan was all about until it was too late to do anything but accept it after a big sales talk full of snake oil. Big business, which had a serious interest in a particular outcome, also had an army of experienced Washington lobbyists. These people were aware of the unpredictable quirks of the house-senate conference system, were completely confident that the membership of that committee would be stacked in favor of a particular outcome, and knew that a congressional staff with agendas different from those of business would, in the end, be perfectly capable of stealing the show. For major employers, that settled it. Big business had been wavering about whether to go ahead with their own plans, anyway. They had listened politely and carefully to what the government wished for its own insurance plans, Medicare and Medicaid, and were probably willing to agree. But as matters approached a unified approach, too many things surfaced they didn't like, and too much chance the decisions would go against their wishes. There was too much to lose, too little to gain, and well, we're sorry, we can't go along. This or something rather like it seems to have been the final outcome. The press had been furious about exclusion from major news items, coupled with annoyance at the favoritism toward Mr. Weinstein of the New York Times. The whole medical industry was jittery about exclusion from consultation or even notice; the insurance industry was pretty comfortable with the status quo; the public was in a state of utter confusion After the main partner dropped out, the proposal never even came up for a vote in Congress. Healthcare Reform: Looking Ahead (1)
By this point, a patient reader of these reminiscences has probably learned quite enough about the Clinton Health Plan and its immediate aftermath. There is, of course, more to say, but except for political junkies, the topic doesn't warrant protracted dissection. It might be worth knowing the motivations of the insurance industry when they launched that bombardment of "Harry and Louise" television advertisements. Opinion within the insurance industry must certainly have been divided, however, and the main decision makers are probably all now retired. The Harry/Louise ad campaign is often given credit for the political assassination of the Clinton Plan, but that seems unlikely. The decisions about medical care were made without heeding the opinions of providers of medical care, so it would not be surprising to learn that decisions about insurance were made without completely candid discussion with insurance professionals. In fact, grieving too much for the past may have led to looking too little at the future, which clearly contains a whole new set of facts. When the largest generation in history, the baby boomers, start to retire in 2012, those boomers own children will then be at peak earning power but will be a very small generation, too small to support their more numerous parents. Consequently, the 12.5% tax the current teenagers pay for retirement benefits will be too small to pay for their parents' health costs. It will be uncomfortable to increase that 12.5% by much. Thus, the Ponzi scheme we have run for eighty years will then be unable to conceal its facts with talk of trust funds and lock boxes. For nearly a century, Congress has spent the Social Security and Medicare tax surplus for non-medical purposes. They will have to stop doing that in less than ten years. Consequently, we can confidently expect the boomers to protest loudly: they contributed 12.5% of income during their whole working lives to support medical care, and now learn that nothing was saved for their own health care. Even more exasperating is that the second Bush administration did attempt to introduce legislation in 2006 to set aside some current surplus to reduce the impact of the coming crunch -- and Bush was howled down. It would thus appear to be the nature of current politics that this boomer health cost shortfall will not be seriously addressed until the crisis is actually upon us. Democrats will apparently stonewall the matter to avoid blame for designing and ballyhooing a welfare expedient of the 1930s that was swept under the rug during decades of affluence. Republicans will be determined not to be paymasters for a welfare scheme they had opposed from the beginning. So what will happen? Government only has two options in funding programs where the money has already been spent; they can raise taxes or they can borrow money. By raising taxes, they risk precipitating an economic depression. By borrowing, they flirt with hyper-inflation of the sort that destroyed Germany and Austria in the 1920s. By adopting a little of both remedies, we wander into "stagflation", a term invented in the 1970s to describe a very unpleasant episode. Whatever the description, there seems a very strong likelihood of economic pain and political uproar. It sounds pretty unlikely the public will be in a mood for expensive additions to health insurance coverage. All this is a preamble to impending cuts in the health budget. We must anticipate the only approach government ever uses for program reduction, the only arrow in the government quiver. It goes like this: first you cut a program budget by, say, ten percent and watch to see if anything bad happens. If nothing bad happens, cut it again. If something bad does happen during a series of cuts, deny that it did happen, and scramble around to patch up the damage. If possible governments restore some of the cuts when they go too far, but in Medicare whose unfunded deficit is in the trillions of dollars, that may not be possible. Try to get re-elected after you pull off one of these capers, and you begin to sense how dictators get into office. It really isn't comfortable to talk apocalypse this way, and one would certainly hope there is some flaw in the prediction. There could be other unexpected events in the meantime, deus ex machina, but a stock market crash, a thermonuclear war, or violent changes in the environmental temperature are all going to weaken the world economy, not make things better. This doomsday scenario seems almost certain to include some serious cost-cutting in the health financing system. Therefore, it is only common sense to examine what advance changes might be made in the health delivery system to minimize the damage to it. My proposal amounts to suggesting that we put the doctors in charge of the cost-cutting. In accident rooms, battlefield medical stations, and even television war serials, the person in charge of sorting out the influx of unexpected casualties is said to be in triage. In triage there is one basic rule: put your best man in triage. If the security guard, the admissions clerk, or the night watchman directs the emergency down the wrong corridor, the ensuing blunders will cascade as the system struggles to get things back on track. We can expect objections to what I have to propose which will take the form of warnings about letting foxes watch the henhouse, but in general, the public already supposes the non-physicians will step aside for the doctors in an emergency. So the more open the discussion about command and control, the better, with ultimate faith that the public will support the common-sense approach of putting your best-trained person in charge. For present purposes, the general proposal is that when drastic cuts in budget get imposed, it should be the physicians of the local community, not the administrators or the insurance executives or the local business leaders -- who should make the painful choices between what is essential and what can be sacrificed. This is most readily achieved by setting aside the Maricopa decision and clarifying the HMO enabling acts to the effect that it is not an antitrust violation for physicians professionally practicing in nominal competition to participate in the shared governance of health maintenance organizations. In other words, that HMOs such as the Maricopa Foundation need not fear antitrust action, using the experience of a dozen other Foundations for Medical Care as proof of the harmlessness of the approach. It should not be necessary for these organizations to prove positive value, only to demonstrate lack of harmfulness. If they can be established and allowed to compete with insurance-dominated or employer-dominated HMOs, their worth can be established by success in the marketplace. Ultimately, the choice of governance form will thus be made by the patients, and the proposal should be a popular one. It should also be popular with hospital administrators. They chafed at physician control thirty years ago, but that was before they encountered the far more brutal price negotiations of HMOs dominated by business and insurance. The consequent costly and disruptive wave of hospital mergers is defended by very few, although it would be interesting to examine dispassionate analysis. Probably no one adequately appreciated the threat that employer domination of these practice groups represented to hospital administrations. When hospitals confronted employer groups in serious hard price negotiations, hospitals came to the shocking realization that these people actually had the power to move large groups of people to a competitive hospital, and they certainly talked as though they were capable of doing it. The resulting panic of hospital mergers, consolidation into chains, and the emergence of for-profit competition by hospitals that had no thought of a charitable mission, has created a degree of cost and disorder that was not in the original plan. Hospitals in rural California who told their colleagues of the burdensome power of their staff doctors under doctor-run Foundations would now have to admit that a return to that environment would be a distinct relief. And there might even be a reconsideration by business leaders. What physicians would bring to the table, what is now new and different, is the undeniable experience that dominating captive HMOs has not proved as useful to employers as they hoped it would be. The cost savings have been disappointing, the exploitation by insurance intermediaries, and the undeniable employee restlessness was not exactly anticipated. Running employee health projects is a large distracting time waster for C.E.O.s who have other goals and mandates to pursue. If employers keep a focus on their reason for involvement in employee health, hardly any of them could defend a posture of resisting the emergence of new choices which make a reasonable claim to reducing employee contentiousness, at a competitively lower cost. And the government? Among the various unpleasant alternatives that Congress must consider, is the possibility to be discussed next that employers may want to pull out of employee health care entirely. Allowing competitive forms of ownership of existing arrangements might not seem too risky a step, compared with that prospect. Healthcare Reform: Looking Ahead (2)
The Industrial Revolution crowded people together into smoky, draughty unhealthy places to live and work, and thus created ideal conditions for the spread of smallpox, tuberculosis, plague, poliomyelitis and many other infectious diseases. With better sanitation and hygiene, those diseases declined steadily for two centuries. Meanwhile, medical science developed a steady stream of expensive enhancements to health like removing an inflamed appendix, inserting pins into broken bones, utilizing CAT scans and artificial kidneys. These things each made life more comfortable and extended it a little longer, but steadily increased the cost of care. Here and there major leaps forward occurred, like the discovery of antibiotics and the prevention of arteriosclerosis, but it seldom seemed that medical care was stamping out disease, it was just making it more complicated and expensive. But if you stopping plodding forward for a moment and looked backward, the aggregate progress was astounding. Dozens of diseases either disappeared entirely or are well on the way to disappearing, like polio, smallpox, tuberculosis, syphilis, rheumatic fever, and what have you. Life expectancy for Americans at birth, which had been 47 years in 1900, was approaching 80 years in 2000. When I started as an attending physician in 1955, I was in charge of a 40-bed ward continuously full of diabetic amputees; during the last fifteen years of my practice, however, I did not attend a single diabetic amputation. At some point in this amazing medical pilgrimage I can remember realizing that for really important purposes, there were only two diseases left. Arteriosclerosis and cancer; and now arteriosclerosis mortality has declined fifty percent in ten years. So now it is possible to have the luxury of asking: what will happen when we finally cure cancer? Oh sure, there is Alzheimers Disease, HIV/AIDS, schizophrenia and childbirth, plus an apparently endless variety of ways to produce self-inflicted conditions. Everyone will eventually die of something, so doctors will keep busy. It is not necessary to predict the end of medical care to see that some important social transformations are likely. For example, if we cure cancer around the time of financial chaos caused by the retirement of baby boomers, it is going to be hard to resist the demand that we reduce spending on medical research. Every tedious word of the impending debate on the topic could be written right now to save time because it is a very strong probability that spending on medical research will decline, once an effective cure for cancer is behind us. Let's, however, continue our march into the future of healthcare reform. When employers became self-insured for employee health costs, they came into possession of data about what they were buying. It didn't look adequate to them to explain the sums of money they were spending, so they concluded they were being hoodwinked by hospital cost shifting, with consequences summed up as the Clinton Health Plan. Now put yourself in their shoes when the Wall Street Journal tells you cancer has been conquered. Michael De Bakey once pressured Lyndon Johnson to start a crusade against Heart Disease, Stroke, and Cancer, and now even cancer is gone. A significant number of C.E.O.s are likely at that point to decide that since Far Eastern competitors don't have this cost to contend with, perhaps it is time to declare that you have been fleeced long enough. Give the employees some money, and tell them to buy their own health insurance. There are even some more legitimate arguments for doing so. Individually owned and selected health insurance would be portable, putting an end to "job lock", the fear of changing jobs for fear of losing health coverage in the process. Employee divorces create a different twist to job lock, and inequities jump out at you from the tangle of arguments about dual coverage for working couples. Add same-sex marriages to this issue and employers are driven to despair. Individual policies would simplify all of these issues, and open the door to life-long coverages, which we will discuss in a later section. If medical progress makes just the right progress in the impending time interval before doomsday, it is even possible to start talking about eliminating health insurance in a practical way. If there is no threat of medical expense, why buy insurance against it? Since everybody will die of something, it is hard to envision a time without insurance. But maybe Medicare is enough. Senator Edward Kennedy (D, Massachusetts) will finally have his universal single-payer system -- by default. What we have here are the daydreams of a corporate C.E.O., struggling to make his numbers for the next quarter, and they are pretty strong stuff. But who can doubt the power of these concepts to move the system away from an employer-based formulation? Healthcare Reform: Looking Ahead (3)
For fifty years, turmoil in the health insurance industry has originated in the steel and auto industries. It seems strange that no heroes have come to general public attention, although there may be heroes who are known to insiders; somebody may yet write a book about it. This may be of only passing importance, but the present distress in the American Big Three automakers suggests that unexpected legislative proposals concerning health financing could emerge from that direction. The turmoil in Detroit once centered on the auto industry enjoying windfall profits which labor wanted to share. More recent discord comes from the opposite direction: the automakers now cannot afford to honor those contracts they signed with labor having to do with health benefits. The contract for the United Auto Workers was certainly generous. Printed up in a little red book for wide distribution, the contract states emphatically that an employee for six months or more will be completely covered for medical expenses for the rest of his life. If Medicare pays some of the cost, that is fine, but if Medicare reduces its benefits, the employer is liable. Some features of this contract may have been changed since it was printed, but it is difficult to imagine what incentives the UAW would have to agree to modifications. Except, of course, the self-interest which emerges when it looks as though the employer might go out of business unless there is some form of relief from wage costs. To judge what is going to come of this is to judge the likelihood of the various arguments, predictions, and recriminations that are so common in heated disputes. Two things are pretty clear to auto industry outsiders: the UAW contract provides more generous health benefits than almost any other employee group enjoys, while the auto industry has worse earnings than many or most other industries. Consequently, both the employees and the stockholders have an incentive to make adjustments in the auto industry, a situation shared by the steel industry and other major auto suppliers. The form this has seemed to take is to favor some form of national health insurance, in which the taxpayers would take over the obligations of the auto manufacturers. So, look out for proposals from Senators and Congressmen from Michigan, and watch which nominees for U.S. President are favored by the rust-belt political delegations. Workers in other industries are not certain to go along with such proposals. After all, most people resent it when someone else makes out better than everyone else for decades, and then comes asking for a hand-out. Health Maintenance Organizations (HMO)
It's an ancient wrangle whether a manufacturer should actually own its suppliers or the reverse; or instead whether it's healthier for industry components to stand at arm's length from each other. At issue is not only what is best, but what is fair. If industry mergers seem sufficiently unfair, it will be proposed they should be illegal. That's the main substance of a lot of antitrust argument. Unfortunately, what is valid in good times may be reversed in a downturn. A prosperous supplier of materials often acts as a "cash cow", saving a merged enterprise from bankruptcy. Unfortunately, within a different economic climate one badly failing supplier can bring down the whole merged enterprise. There's also organizational friction; a temporarily prosperous unit may get to thinking it should boss the less prosperous units around. At the very least, the cash cow resists the use of its cash reserves to help "losers". Several centuries of experience have thus left a minefield of old laws, traditions, and ingrained prejudice to undermine any broad standards for what is best. In no field is this truer than the Medical Industry. Eighty years ago in Houston, the first Blue Cross health insurance company was started for a single group of school teachers to pay for service in a single hospital. That expanded to other subscribers and other hospitals, soon making it more workable for insurance, subscribers, and hospitals to stand at arm's length, allowing for a variety of local combinations. During World War II, combat in the Pacific led shipyards to be built on the West Coast, but westward migration of steelworkers was hampered by lack of local medical facilities for them and their families. Taking advantage of the loophole provided in the wartime wage and price controls, Kaiser Industries attracted medical personnel by building hospitals, paying salaries, and offering physicians ready-made medical practices. Because of various licensing laws, Kaiser's medical enterprise was divided into two corporations, Kaiser and Permanente, so a specialized corporation within the Kaiser-Permanente Foundation could accommodate the licensed practitioners. The salaried nature of the physician organization immediately caused trouble with local fee-for-service practitioners, who were thus excluded from a large population in their neighborhood when they could not readily adjust to varying mixtures of the two payment methods. Their reaction, led by an obstetrician in Stockton, California, was also to organize dual-corporation structures which were exclusively fee-for-service. Because Kaiser had a Foundation, they also called their organizations Foundations for Medical Care. Then, as now, it proved difficult to run a practice with two different reimbursement philosophies in the same waiting room; in time, friction between the two styles tended to increase as doctors who were more comfortable with each style tended to segregate themselves. Since offers of salaries are more immediately attractive to newly-trained physicians, they flocked to California to serve the steelworkers who were in need of doctors. Fee for service, on the other hand, allowed the gradual assembly of a more durable practice composed of patients who could test what they liked before making a permanent allegiance. Essentially, the transients went to Kaiser, more permanent settlers used fee-for-service. Thus, it came about that several models for health care reform were tested in a few smallish towns of central California. These demonstration experiments may perhaps not meet everyone's standard for scientific purity, but at least they were public examples with the dumber features knocked away. They certainly provided a laboratory where ideas could develop about topics that otherwise were merely opinions and unsupported conjecture. The Foundations demonstrated that physician-dominated organizations could contain costs and maintain quality in a satisfactory way; there had previously been doubted about their ability to contain cost. The Kaiser organization showed that salaried practice performed acceptably as well, both to most staff physicians and to a majority of the patients; there had been doubt about the willingness of the public to limit choices to a panel of assigned physicians, mostly young and usually from elsewhere. Finally, the two systems seemed to be able to live together more or less peacefully; indeed, the California public seemed reassured that two systems apparently kept each other in check. The first main difference rested on the system of quality control. The local Foundations developed review systems based on peer review and peer pressure; these worked remarkably well, particularly in constraining non-physician costs like pharmacy, tests, and hospitalizations. Cost and quality control in the Kaiser system was more rule-bound and quicker to apply discipline, kept within bounds however by the ability of both patients and staff to jump ship for the other system. Aside from professional peer review, the Kaiser system experimented with owning hospitals, laboratories, pharmacies. Here, the experience directly paralleled the experience of manufacturing industry with its suppliers; when reimbursement was generous suppliers generated welcome revenue. When reimbursement was constrained and substandard, ancillary service losses were unwelcome. Taken overall, the Houston experience was repeated, that ownership of such facilities was mostly a headache. Indeed, subsequent experience has shown the two systems usually co-exist nicely within independent ancillary facilities. The Stockton, or Foundation for Medical Care, approach grew popular in the West. The variant which grew up in Utah was locally popular and attracted the attention of Senator Wallace Bennett. The Bennett Amendment to the Medicare Act then picked out the peer review system as the secret of success and set up a nationwide system of Professional Standards Review Organizations (PSRO) to conduct peer review of Medicare and Medicaid patients. The drawing of boundaries around these organizations was the most difficult part, and sometimes the boundaries were inept. Rural districts were adamant that the standards of big-city medical schools were not to be applied to their scattered resources, and urban areas saw themselves as ancient Rome surrounded by hostile tribes. Although these difficulties were foreseen, it is not always possible to draw a line that will separate the cultures, particularly where the outward migration of suburban housing was more rapid than the construction of suburban medical facilities, leaving the medical culture unstable. The PSRO system was quite successful in many areas but caused trouble in others that were not adequately addressed. The central concept of the review system was that the doctors who worked together could quite readily identify the outliers, and better than anyone else could judge whether the local situation was justified. True, some practitioner might try to abuse the system to the disadvantage of his competitor, so no adverse decision was final until there had been an opportunity for outside appeal. There might even be a few circumstances requiring a still higher appeal. The system was new and untried, but it produced eminently satisfactory results from the point of view of the Federal Government paying the bills. As former President of one of the largest PSROs in the country, I will assert that there was remarkably little friction or resistance in the medical community. My very good friend, the President of the New York City PSRO says much the same, and most people would say that if you can carry off a new system in New York without a lot of argument, it must work pretty smoothly. The Government wanted to eliminate unnecessary Medicare costs, particularly in hospitals, and it wanted to maintain peace with the medical profession. Hospital costs are obscured by the wide gap between posted charges and true underlying costs, compounded by disagreement about the proper assignment of overhead charges. Charges were not the assignment of the PSRO, utilization was. Days of hospitalization per thousand enrollees fell from roughly 1000 days per thousand to roughly 200 days per thousand, and that satisfies me at least that we were doing our job; physician peer review was doable. It is likely, however, that peer review was much more apt to produce friction in rural districts. Philadelphia has had more than a hundred hospitals for more than a century. Birds of a feather tend to flock, so the sorting-out process was already far advanced by the application of constrained referrals to practitioners who failed local standards. Mixing members of different hospital staffs on appeals committees was easy in the big cities, and the naturally censorious tendencies of many physicians could be safely counted on to produce adversary balance. Most committees seemed visibly pleased, even relieved, to discover generally good quality in their competitors' practices. However, in the much smaller and more scattered institutions in the nation's regions with low population density, these informal arrangements cannot stretch as well. When there is only one specialist in a field, for example, it is sometimes hard to know whether he is a good one or not, but always easy to say whether you like him or not. Where the population thins out, much greater wisdom is required to make judgments, the number of close cases is greater, and the limited supply of judicious reviewers is similarly stretched. At least that is my surmise, based on knowing the background of most of the AMA delegates who eventually voted 105-96 to condemn the program in a standing vote. The result was the Dornenberger Amendment, which much weakened the system when instead it should have triggered a more profound analysis and reconsideration. Perhaps we spend too much time here describing a technical process. It is, however, at the heart of what makes the Foundation approach (sometimes called IPA or Independent Practice Association) superior to the HMO. It is now perfectly clear that both doctors and patients vastly prefer the IPA approach to the HMO, and any reasonable politician would jump at it. But there is one fear, summarized by the slogan that the Fox is guarding the Henhouse. In both systems, an attempt is made to combine insurance with the delivery of health care. In the IPA, the physicians are taking the financial risk that aggregate income will exceed aggregate costs; it's a risk contract. In the case of an HMO, the employer or the government is taking the financial risk and therefore wants to control it. If revenue is good, the doctors will prosper in an IPA; the insurance company intermediary will prosper in an HMO. Doctors will care about that little difference, but why should the rest of the country care? Because the prospect is overwhelmingly likely that future revenues will be constricted until something hurts, and when you starve with a tiger, the tiger starves last. In the case of an HMO, the insurance middlemen will starve last, and the quality of health care will starve fairly early. That's an unwise design. When we get to the point where Congress cuts the budget and watches to see what happens, Congress will cut it some more if nothing bad happens; it will back off only if something bad happens, so something bad is certain to happen. In designing the system, you need to design the internal review authority so it will cut the waste, inefficiency, and luxury first. The reviewer, no matter who it is, will cut himself last, so you need to arrange the incentives for waste to be cut before the reviewer suffers, and quality of care only after the reviewer has suffered. If you wonder why a whole lot of special interests hate physician-dominated review systems, a short answer will be found in this synopsis. A special exception must be devised for rural health systems, which do have a unique problem. To return to the well-worn slogan about foxes and henhouses, we have overlooked the central question. Who's the fox, and who is the hen? Hold the Presses
At USAToday, techniques are astounding. After getting an 800-word piece, an editor by phone will suggest cuts to 300 words; the piece is always improved. Last-minute speed, trying to watch television, is unbelievable. On one occasion, after a medical meeting in Kansas City, watching a baseball game go into extra innings I fell asleep with the game undecided. The next morning a newspaper was pushed under my door. It was USAToday, not only carrying the final score but a full story, under a color photo of the winning play. Just consider the precision Chicago reporting, Washington DC editing, Kansas City printing and local delivery that took place in seven hours. By contrast in book publishing, a full year often intervenes between manuscript submission and actual bookstore sales. So on a certain Monday night, the editor called. The Senate Majority Leader, George Mitchell, finally was to unveil the Clinton Health Proposal tomorrow morning. Would I please submit an editorial to run in the morning paper; he would supply the title. It was to be called, What Should Congress Do Now? and the deadline was 7 PM tonight. My watch read 5:30 PM. Well, what fun. After a few minutes of stumbling around, I resolved to build the editorial around the theme, Don't Make Things Worse. It then seemed natural to allude to similar proposals gone famously wrong, define some predictable traps, and end up with Hippocrates. Over and over it is thundered at medical students: Primum non nocere. First do no harm. It all came together in my head, and I sat at the typewriter to bang it out. But when I came to that last sentence, pleading at least do no harm, I was hit by terrible doubt. That phrase comes to us in Latin, and Hippocrates was a Greek, living at least five hundred years before the Roman Empire. Famous though the saying is, it wasn't (then) in Bartlett's Quotations, or Roget's Thesaurus, or anything else I could lay my hands on in what was, after all, a medical office. It was 6:50 PM. I called a learned friend from his dinner-table, and he agreed it was a strange business, looked at a couple of books, couldn't help, sorry. So, I drew a deep breath, said the Hell with it, typed in, "As Hippocrates said, At Least Do No Harm," and shoved it into the fax machine. The next morning it appeared, next to two million copies of my photo; so at least the editor seemed to like it. Some friends soon called to say that Senators Dole and Moynihan had adopted the line on the noon and six o'clock news, each attributing it to Hippocrates. No matter what happened to the Clinton Health Plan, it looked to me as though I would be forever guilty of supplying the world with a highly quotable misquotation. Since then, with more time to do a proper search, I'm unfortunately still uncertain. William Safire at the New York Times, was intrigued but could only refer me to a nice lady at the Library of Congress who was a crony. She tried to help but was stumped. Some Hippocrates scholars at the Library of the Philadelphia College of Physicians were able to find a reference in The Epidemics which seems to say what we are looking for, and that reference has tardily crept into Bartlett's latest edition. Some people think Galen really wrote it, which might account for the Latin; but even that is unsatisfying to scholars. Somebody or other took that phrase, whether written by Hippocrates or not and pounded it over and over until it became a medical student incantation. Even if Hippocrates actually did express that sentiment in passing, it doesn't come through as a really important statement, and there isn't much evidence that his students were repeating it over and over as the words of the master. My present suspicion is that vague rumors about Samuel Hahnemann, the father of Homeopathy having a hand in promoting the slogan during the Nineteenth century, may have some underlying substance. Homeopathy was a belief system which emphasized the prescribing of infinitely minute doses of medicines. It had a flurry in the 19th Century when conventional Medicine was reeling from excesses of bleeding and purging, which surely did a lot of harm to victims of, say, Yellow Fever. The acrimony even spilled over into the emotionalism of the abortion debate, because laws prohibiting abortion had been sponsored by the allopathic American Medical Association. The verbal warfare between doctors of Homeopathy and "Allopathy" was bitter beyond describing. Although conventional medical care finally got its feet on the ground, and homeopathy is now pretty much a historical relic, the homeopaths did have that big strong point. Doing nothing is clearly better than doing something harmful. Nobody takes Latin, much, anymore. So the modern medical way of saying the same thing has come to be, "The hardest thing to do, is to do nothing". This way of stating the same idea is widely believed to have been offered by William Osler, but after all the controversy about Primam non-nocere , I am now reluctant to be too sure about anything in this area. Intelligensia, Philly Style
On a hot summer evening, attendance at computer user-group meetings is light, so after a recent one got through discussing spammers and new software, we adjourned to the sidewalk tables of a nearby pizza joint, just off Broad Street. United only by a common interest in computer hardware, software, and techniques, this one comes from many corners of the Philadelphia social scene and goes back to those corners after the meeting. Whatever their background, computer geeks are uniformly good at math. But on this particular evening, the conversation turned to medical experiences. A middle-aged man with a ponytail related he had recently experienced Bell's Palsy, a paralysis of the muscles of one side of the face. The group was fascinated to hear how saliva dripped from a corner of his mouth, and his unclosable eye dried out and got sore. His doctor told him there was not much to do except wait, an opinion confirmed by a specialist. Immediately, this man who makes his living programming computers set out to find the best acupuncture person he could find. It was a familiar story, and I remained as quiet as I could while he essentially related that when the regular medical profession confesses failure, the patient feels released to take matters into his own hands. His instincts were to do something, anything, even if that something was plainly futile. He could not bear the idea of doing anything, and sure enough, in time he got better.
I said nothing because it was a familiar reaction to conditions that either would or would not get better by themselves. The more serious studious members of our little club were quiet, too, because their instincts were to do what they were told, and in his place wouldn't have acted the same way, didn't completely approve. In a moment, a large muscular man took up the medical subject by telling that he had spent two years in a hospital after falling down an 18-story elevator shaft. Man, oh man, it seemed like it took two weeks as I was going down, and when I hit I wasn't knocked out. He had landed on one buttock and his leg was nearly wrenched off, but he remained awake, not bleeding much. Within minutes, he was headed for an operating room and reached out to grab the clipboard from the nurse. On it was written "amputation", which he circled, wrote "No amputation!!", dated and signed it. No way were they going to cut off his leg. His leg was in fact saved; he now scarcely walks with a limp. Then another computer nerd chimed in.
This man's story was that he spent fifteen months in a hospital after a motorcycle accident. He somersaulted seven times through the air before he landed on his chest, and twenty years later he could still remember every single twist of all seven turns. He, too, related many hospital disputes about morphine injections and contemplated surgeries. Both men related dubious experiences with young interns and medical students, and numerous proposed remedies that had been rejected. All three of these medical veterans expressed violent hatred of HMOs, for reasons unspecified. I was quiet; no argument from me. This motorcyclist eventually had his vehicle repaired and proceeded to ride it for six more months until he sold the machine. So there. We all had different thoughts about this, I suppose. I was lost in thought about why they had survived and imagined that not being knocked unconscious meant that they had not hit their heads. Heavily muscled men like this were probably cushioned by their muscles; a skinny little bony nerd would have been much more smashed up. The negative side of that protection came out in hearing them both describe their heart problems, with by-pass surgery and whatnot later on in life. That's probably the negative side of their muscularity. Neither man smoked, but I bet they both did at one time. As we strolled home from the pizza joint, it occurred to someone that the national political conventions were on television that evening. The women were fighting with the blacks. The studious nerds were silent; the wild men merely grunted. That didn't seem like something to fight about, or even to comment on. As I walked into the darkness, I wondered if such a conversation would seem normal in any other city in the world. Friends Lifecare at HomeOver thirty Quaker retirement villages scatter through America, more than twenty in the suburbs of Philadelphia -- "under the care of the Yearly Meeting", as their expression has it. But for some people, community living seems unattractive. It does not speak to their condition. For one thing, it may not be affordable.
Or the style of may seem too fancy, or too plain, for some tastes regardless of cost. The increasing emotional rigidity of growing older is a factor; by the time people get to be seventy-five, they had better make this decision or forget it. Plenty of people are hale and hearty at ninety, but they establish pretty firm ideas about the sort of person they want for neighbors while they are still in the workforce. Quite often it's just a habit, people have lived in their home for several generations and cannot imagine another neighborhood, lifestyle, or environment. This is home, and they intend to die there. So, to address this need, or market, a group of Quakers conceived of a retirement village without walls. Live in your own home and someone will come to oversee things, will know what to do if there is an emergency, and may eventually make the decision for you that you absolutely must go somewhere else. All of this is wrapped within an insurance vehicle, to recognize the fixed incomes of retired people, the inevitability of terminal illnesses, and the occasional risk of monumental medical expenses. At present, about 1600 people in Philadelphia are enrolled in the unique plan of Friends Lifecare at Home, making it one of the largest retirement communities in the country. The organization receives universal praise for its imaginative responses, as well as the dependability and high quality of the people it sends out to the homes of subscribers. Friends Lifecare is a pioneer, and it is gradually weeding out the ideas that didn't work and adding new features that were not originally contemplated. One of its greatest challenges is the need to adapt to unexpected and uncontrollable changes in the Medicare program. Slashes in the Medicare program could bankrupt Friends Lifecare, and even sudden windfalls like the Medicare Drug Benefit create management problems. There can be no doubt that one element of trust exists for which there is no substitute; Philadelphians know that the invisible support of the community and its Quaker core is behind them. If anyone can possibly preserve a moral commitment to the elderly, it will be the Quakers. Ultimately, the commitment is not so much to 1600 subscribers as to the notion of finding out what works. Life expectancy has extended by three additional years, during the past ten; that's a joy, but it's a problem to finance. The optimum size of the organization is also an unsettled question. Although this program is relatively large by comparison with individual retirement villages, it may not be large enough to have spare capacity to cope with influenza epidemics or record-breaking spells of bad weather. Since it's the only one of its kind, it is vexed by the popularity in ever-widening geographic areas. It must grow to some reasonable size in one area before it can spread its resources to another. By the same reasoning, it must have a reasonable number of prosperous subscribers if it is to accept even a limited number of poor ones. The idea of creating a seamless partnership with the residential-type retirement villages is certainly attractive, but Friends Lifecare must be careful to avoid becoming too much of a life raft for other people's problems. When the resale price of residential housing rises in a housing bubble, people wish to cling to a rising investment. During the same economic period, the entry and rental price of residential villages also rise. With a great many uncertainties that are specific to this pioneering effort, it is hard to know what policies to develop to insulate the lifecare environment from speculation in the mortgage and housing markets. Or, right now, high-rise apartment development. All of this creates a need for clear minds in the governance, determined to see and acknowledge difficult reality. If anyone can do it, Quakers can. Please Don't Lose Any Sleep Over This
The Institute for Experimental Psychiatry Research Foundation meets alternatively in Boston and Philadelphia, in recognition of its rather complicated historical relationship with Harvard and Penn. The Spring 2005 trustees meeting was held in Boston, with Dr. Charles Czeisler of the Brigham and Women's Hospital making a presentation of his work with sleepy resident physicians. Sleep is now a central focus of the work of the Institute, particularly the effect of lack of sleep on performance. Resident physicians are a group with lots of experience with sleep loss, so much that such experiences as residents are central imprinting in the lifelong brotherhood of the profession. The public tends to regard the torment of protracted craving for sleep as some kind of dangerous hazing inflicted on professional newcomers by sophomoric seniors. Every once in a while, someone gets hurt by these games. That seems to be a general public reaction. For the most part, by contrast, members of the profession who have themselves undergone the experience turn away silently from such unfeeling remarks. As the old contraceptive joke about the Pope has it, if you don't play the game, don't make the rules. In the first place, it is wrong to suggest that resident physicians are somehow helpless victims of authority, abused slaves of somebody's profit motive, or warped masochists enduring the process in order to inflict it on someone else. Perhaps the example of my classmate Seibert is useful. As a freshman medical student, Seibert was so overwhelmed by the volume of facts he was expected to learn, that he decided to give up sleep entirely. Seibert, by the way, was no moron; he was an honors graduate of a very selective Ivy League university. And he actually did stop sleeping for more than two weeks until he collapsed and had to be stopped. This was his own choice, gamely adopted in spite of general ridicule. And to show that overachieving is not limited to physicians, there was my oriental patient, the daughter of the President of her country. She related that as a graduate student she did not go to bed for three years; during all that time, she sat at her desk, slapping her face to keep awake. What we are talking about here is a self-selected group of committed and dedicated people, perhaps overly shamed by the specter of failure. The work of our Institute has helped document and understand the injurious effect of sleep loss on performance; no one can go very long without sleep before responses and vigilance begin to deteriorate. A great many vehicle accidents are caused by drowsy drivers; it is a concern that pilots of airplanes on long-distance flights are to some provable degree less competent to land the plane. Therefore, it is not completely surprising to find that interns on protracted duty do make 20% more errors in medication orders, and nearly 50% more diagnostic errors. It is jarring to discover a measurable increase in the number of intern auto accidents, particularly when driving home from work. Maybe we ought to pass a law about it. Commiseration is one thing; proposals to interfere are quite another. For one thing, the time-honored protection against the harm of this problem is redundancy. The complex, fast-paced and dangerous environment of a hospital, like that of an airline cockpit, has very little tolerance for lack of vigilance. Our solution has been to do everything three times, with overlapping responsibilities and repeated opportunity for catching errors before they get through to the patient. Although the malpractice lawyer seeks to pin the whole blame on some person, particularly one who is covered by insurance, the reaction of doctors to adverse events is to presume that at least three people must have cooperated in letting it slip through. At night and on weekends, the reduced staff tends to weaken the defensive network. But by every assessment, the greatest threat to our protective screen of redundancy is cost control. Any manager of managed care can find duplication and overlap in ten minutes of searching for it in a hospital; redundancy is a big factor in the high cost of running a hospital. The law of decreasing returns will dictate that it becomes very expensive to eliminate the last one percent of errors. To state it in reverse: it is very tempting to save a bundle of money in a competitive world, by accepting only a small increase in the errors. Since it is a matter of opinion, physicians are grimly determined that it shall be physicians who strike that balance. Those who press for more punitive treatment of physicians in the matter of errors should reflect that it surely will convince physicians to flee the risk of responsibility for the decision of where to strike the balance. If you bend metal repeatedly it will crack; if you stretch a rope too hard it will snap. These unfortunate events are not called errors, and it is improper to search for blame in them. The medical profession is aghast that the public does not seem to appreciate that average life expectancy has increased by thirty years in the past century. That's not ancient history; life expectancy has increased by three years in the past ten. A system that produces a result like that is entitled to a certain amount of tolerance for its errors if we must call them errors. In other environments, that's known as pushing the envelope. Anyone who thinks it's fun to stand on your feet for thirty-six consecutive hours -- hasn't tried it. Surgeons are perhaps somewhat more conscious of the need to train young professionals to drive themselves beyond ordinary endurance. After all, if an operation is unexpectedly prolonged, the surgeon can't just quit, he must finish. Neurosurgeons, with their fourteen-hour procedures, are particularly vehement on the topic. But it is true of every physician, too. When the telephone rings in the middle of the night, will this young fellow haul himself out of bed, or will he tell the patient to take an aspirin and call again in the morning? Increasingly, we hear complaints from patients that other doctors didn't even take the trouble to examine them; the implication that we are somehow not like that is very flattering. Part of the training is forbearance, too. At three in the morning, it is very easy to feel sorry for yourself and to reflect that an administrator with four times your income is home in his nice warm bed. The fact is, that if the person who is up and on his feet doesn't do the job, no one will.
Some incomprehension from bystanders must simply be endured with patience. Beyond that, it could be futile to seek a complete understanding. Quite recently, I was explaining to a young lady in a tailored suit who Thomas Cadwalader was. His portrait, beneath which we were standing, hangs in the great hall of the Pennsylvania Hospital. Although he died in 1789, Dr. Cadwalader is still famous for his remarkable, unfailing courtesy. A sailor in a tavern on Eighth Street once waved a gun and announced to the crowd he was going out the swinging doors to shoot the first man he met. The first man happened to be Dr. Cadwalader, who tipped his hat and said, "Good morning, sir." So, the sailor shot the second man he met. The young lady in the tailored suit brightened up. "The moral of that story, " she said, "Is always wear a hat." A New Food and Drug Category
An editorial in the April 7, 2006 Wall Street Journal rouses a proposal germinating in my mind for twenty years, a new compassionate status of pharmaceutical regulation for dangerous but effective new therapeutic agents, not presently provided for in law. The editorial concerned a new drug treatment for multiple sclerosis, a crippling and usually ultimately fatal condition which destroys the nervous system. In a hearing of the tests of this new drug, we hear numbers like 85% total remission. Unfortunately, we also hear of four patients who died, quite possibly from the treatment. From that point on, you could write the reports from memory. Patients come forward, declaring their willingness to run any risk to get the drug; politicians are sympathetic. The Food and Drug Administration feels forced to withhold the drug from the market until the situation is clarified; other politicians are sympathetic. We are reminded of thalidomide, which was luckily withheld from the American market until the German experience showed that pregnant women who took thalidomide could have babies without arms or legs. This lucky illustration of the value of bureaucratic procrastination gave Senator Kefauver the strength to push through an amendment bearing his name, demanding proof of efficacy, something quite irrelevant to the safety of thalidomide. Seldom mentioned is the fact that thalidomide has since proved to be quite useful for the bone cancer called Multiple Myeloma; this value took a very long time to surface, under the circumstances. The efficacy rule accomplished the purpose, however, by delaying all drug approvals, unfortunately also shortening the time left for patent coverage, and vastly increasing the cost of drugs by shortening the time on a patent to recover development costs. After thirty years of hearing the same arias re-echoing about one drug introduction after another, it begins to look unlikely that Congress will ever be able to stand the political heat which would be generated by a serious attempt to fix this problem. But surely that can't be allowed to continue forever. Taking the multiple sclerosis treatment as an example, the patients want the drug, and their doctors want to use the drug but they don't want to be sued or prosecuted. It's almost certain that most of these patients would sign anything, accept any risk, even agree to a shortened life expectancy in return for an 85% chance of stopping the disease in its tracks. All the doctors want is to be held harmless by the courts for exercising reasonable care under the circumstances. The same is probably true in a political sense, for the FDA and Congress, who surely would be satisfied to have the doctors take the blame for any problems encountered. The drug companies want to preserve their patent protection, surely that can be accommodated. Perhaps they should be asked to contribute to a fund for the victims of unforeseen accidents; they would probably agree. What would satisfy the trial bar is less certain; they should be asked to stipulate something. As a matter of fact, anyone at all who has qualms about such a system of special defined exemptions should be asked to come forward with serious suggestions. There would then ensue a lengthy and ultimately tedious debate about details. This would all take some time; at the end of it, someone would have to make some arbitrary decisions. But at least we could expect more progress than we have seen in the last thirty years of indecision. Membership and Fellowship in the College
The College, I fear, has allowed itself to resemble the Board certification process, where a great deal of effort is put into attaining the honor, but once attained, there is not a great deal to do. I believe this is the main reason we see so many Fellows stop paying dues after a few years. Last year, I believe it was said there were 90 drop-outs from all causes. My suggestion is that we contemplate a more formal subdivision by specialty, linked to local specialty societies, and ultimately to the national specialty societies -- especially when they hold their annual conventions in Philadelphia. We already have a small number of specialty societies who use our facilities, and it would be important to learn their feelings about what I propose before doing anything that might upset them. I am proposing more than just renting the hall. My proposal is that we explore offering College membership (not fellowship) to every physician active in a specialty society which joins with us, for the duration of his activity in the specialty section. I think we should require their officers to be fellows of the College, and suggest that their national President be offered the honor of yet another new class of affiliation, that of Master. For this to be seemly, our own officers might be made Masters as well. When national meetings are held in town, I would hope that officer dinner here at the College might be welcomed. There are things to be explored. Many of the local specialty societies have the expenses of their monthly meeting dinners paid for by drug firms, and I am familiar with the discomfort the College has felt with pharmaceutical relationships. Perhaps if the pharmaceutical companies themselves had a membership class, there might be sufficiently generous dues to substitute for the present system. I am not proposing this idea as a revenue center, but rather as a way to get the physician community within the building, hoping that a substantial number would go on to full fellowship, but recognizing that many residents and junior staff may have only transient interest in Philadelphia. The relationship I would seek is not between their staff and our staff, but between their leaders and ours. I would hope they could be given space to display their trophies, and possibly specialty libraries, and accorded space among College meeting notices, and website space. As a footnote, I considered the idea of linkages to local hospital staffs, but discarded it. It might be fine if every hospital linked up, but for a long time, there would be affiliates and non-affiliates, which has led to a caste system in the past and would do so again. Curiously, having some specialties affiliate and others not seems to avoid this issue. Perhaps you remember that Philip Synge Physick was called the Father of American Surgery, but he was never a fellow of the College because he was only a surgeon. Those days are behind us, but it is always good to be sensitive. Unequal Health in an Unequal World
In 2007, the Sonia Isard Lecture was delivered at the College of Physicians of Philadelphia by Professor Sir Michael Marmot on the topic of Health in an Unequal World . Sir Michael is the Director of the International Institute for Science and Health, and MRC Research Professor of Epidemiology and Public Health, at University College, London. His starting point is the commonly accepted view that the richer you are, the better your health. The life expectancy of the poorest level of society is almost everywhere seen to be shorter than the local average. In less developed countries and in children, the excess mortality is concentrated in infectious diseases. However, in more affluent nations, it is obesity, diabetes, hypertension which seems to account for it. Regardless of the cause, the common denominator everywhere is poverty, which leads to a general opinion that the alleviation of poverty contains the solution to the health gradient. There is even another logical presumption, that improved health care will directly remedy the problem, without necessarily addressing a more daunting obstacle, the elimination of poverty. Although the provision of equal access to quality health care may be almost more than we can accomplish, in this analysis of causes, it is a short-cut. Sir Michael is not so sure. Great Britain has had a national health service for fifty years, but it is still clear to British physicians that the class distinction persists in health if not in health care. Mortality statistics confirm the professional opinion. The conclusion is general that the British health system must be flawed, or underfunded, or poorly run. Not necessarily correct, not necessarily correct. Buried in a mountain of data from the Whitehall Studies of British civil servants, Dr. Marmot teased out the fact that a striking inverse gradient of mortality and morbidity existed in a highly educated group that had essentially equal health care and, while not rich were certainly not poor. The gradient persisted at all levels; the higher you rose in the bureaucracy, the longer you were destined to live after retirement. Evidently a huge amount of statistical work followed this insight, confirming its thesis in a wide variety of situations. The caste system in India provided a confirming example that was unrelated to education or occupational strivings. Marmot's observation is a gradual gradient, not a two-part, either/or. Not rich versus poor, but richer versus less-rich, less-rich versus even-less rich. Every occupational, social or financial step up makes you live a little longer. I wish he had stopped there. But the pressure to explain has generated the hypothesis that what we are looking at maybe progressive degrees of empowerment. Others who have contemplated Professor Marmot's observations suggest it is due to progressive degrees of happiness. Sorry, but that's a little too touchy-feely for me. I don't know what empowerment is, or how to measure happiness. The monk in his cell may have achieved serenity, not necessarily happiness, certainly not empowerment. The prisoner in his cell has no serenity, happiness or empowerment. I prefer to believe it is premature to speculate publicly about the mechanisms which produce these observations. Meanwhile, it seems to be true that if you aspire to be rich you may not become happy, but you will probably live longer. If you want to rise in the hierarchy and still live longer, you need not be afraid to strive. For at least a little while longer, that's going to have to suffice as a definition of wisdom. Community Volunteers in Medicine
Mary Wirshup has a very different medical background from mine, but she's my kind of doctor. I couldn't help wishing, as she addressed our urban luncheon club, there could be thousands more like her, even while understanding more fully than she seems to, the reasons why doctors are driven from her behavior model. As we parted, it felt like saying a last goodbye to the Spartans marching to Thermopylae. As 46,000 medically uninsured persons in Chester County get sickness and injuries, they know that a Federal Law prohibits a hospital accident room from refusing to see them, so ways are found to shunt patients to the CVIM free clinic, run by volunteers. This law is, in turn, a response to a government-created situation where a hospital which "accepts" patients must keep them. Any economics teacher can tell you that supply/demand issues are best addressed by price adjustment, so price controls in whatever guise lead to shortages. I must say I have little sympathy with the devious strategies which hospitals often employ to disguise their rejection of uninsured patients. At the same time, I know a lifeboat will sink if too many climbs aboard. Nevertheless, the semantic switch from lack of insurance to lack of care implies that only more insurance can surmount the barriers to care, which is absurd. For one thing, I know too many hospital administrators who are paid a million dollars a year, and one who is paid two million. And at least two health insurance executives are in the newspapers with a net worth over a billion -- yes, that's billion with a b. We have reached a point where reducing all physician income to zero would only reduce "healthcare" costs by 10%. As I look at Dr. Wirshup's modest clothing I can only surmise she plans to continue her modest living until she is 80 years old, after which her savings might see her out. Squeezing physician reimbursement is not intended to save significant money, nor intended to restore physician incomes to more equitable levels. It is intended to address the oversupply of physicians without confronting either the universities or the foreign trained lobby. The elite tranche of medical schools do their part to relieve physician oversupply without reducing class size, through the encouragement of their students to go into research. I was well along at the National Institutes of Health before I finally decided I had not gone into medical school with that goal, and returned to teaching and patient care in a more satisfying model not too different from CVIM's obviously Pennsylvania Dutch spirit. The Amish at the far western end of Chester County reject the whole idea of insurance; their most characteristic statement is "Don't send me no bills." That attitude is rather a contrast with the shiny housing and automobiles in the Silicon Valley developments of Southern Chester County, or even with some rather bewildered Quaker farm families scattered over the rest of the county next to the horsey set. Chester County is America. On Second Street in Society Hill, next to the park where William Penn's house stood and a few feet from Bookbinders, is the house of Dr. Thomas Bond. Bond conceived the idea of building the first hospital in America and with Franklin's publicity machine succeeded in getting it built, to care for the "sick poor". Dr. Bond started a second enduring tradition as well. When the Legislature expressed doubt that the institution was sustainable, he pledged to convince the local medical profession to serve the poor without charge. Some of the legislators who voted for the measure did so in the belief that charity care would never appear so the gesture would be without cost. The physicians did indeed come forward, in sufficient numbers to run many institutions for two hundred years. In 1965 health insurance made its national appearance and has regarded the benchmark low costs of charity care as a threat, ever since. Exit, Pursued by a Bear
Everybody ends up getting fired in a recent book by John Kastor about recent events at the University of Pennsylvania just like everybody ending up dead in an Elizabethan play. The vital difference, of course, is that the dramatis personae at Penn can still relate to a bewildered audience their own versions of those grand events. To protect himself, the author peppers his book with more footnotes than a Ph.D. thesis. And thousands of stakeholders at the University can now realize that during those eventful times they were as clueless as Rosencranz and Guildenstern. One basic fact about that institution is that the medical school spends three-quarters of the entire university budget. That leads to grudges in the little law school, the little engineering school, and the little president's office, as they knuckle under to the Golden Rule. The department chairman with the gold makes the rules. Since most of that gold comes from research grants, hence ultimately from the federal government, the medical students and the teaching faculty don't have the same power they had during the Vietnam War era, either. Although medical school tuition imposes a crushing burden on the students and their families, leading to debts close to a quarter of a million dollars apiece, the tuition money doesn't amount to much in the university scheme of things, either. In some schools, tuition amounts to two percent of the medical school budget. You could eliminate the students entirely and not see much difference in the "school". Unfortunately, when you become dependent on government grants, you find they can suddenly be terminated, or awarded without funding, or held up for several months by Congressional bickering. Meanwhile, there are salaries to pay, contracts to fulfill. Even if you can furlough some of the staff, it's not easy to see what you do about a thirty-year mortgage on a research building when there is a lull in its research funding. If you try to save money, the granting agency will try to get it back; they aren't authorized to make grants to be squirreled away. If you shift money to unauthorized uses, you risk going to jail. And yet, if you don't do something along those lines, the whole enterprise can collapse. Having said that much to be fair, it is still uncomfortable to see the financial transparency of our most valued nonprofit institutions vanish behind a Byzantine fog of secrecy, out of which arise the magnificent towers of new buildings, and in front of which an occasional limousine is to be observed. No wonder the research scientists feel the constant pressure to produce. A Nobel Prize every ten years, or so, would go a long way toward quieting envious remarks from the liberal arts faculty. Housed in those ivy towers are three institutions, the teaching hospital, the medical school, and the university, with three boards of trustees, and at least three ruling potentates. At irregular intervals, congressional committees do things to the Budget Reconciliation Act which enrich one of the three components of the institution or suddenly impoverish another, or both. Integration of the three under one governance sounds plausible until you notice how radically different is the mission of each one. You can take a big building away from one component and rent it back to them, and things like that, but you can't do it without starting whispers about Enron. You can gather up surplus funds from one of them during the decade of the eighties, but you have trouble giving it back twenty years later. Officials at Blue Cross come snooping to see if health insurance premiums are passing through this shell game, ultimately paying salaries in the department of English Literature. Everybody distrusts everybody else, somebody sasses somebody, and everybody gets fired. Nothing unusual about that. It happens at every medical school. Durance Vile
Visitors to the royal castle of Ferdinand and Isabella are routinely shown the iron grating beneath the throne, below which is a small dark hole for a couple of prisoners. By contrast, most American cities have prisons containing thousands of prisoners. At the time of the discovery of America, dungeons were places to hold a few important prisoners waiting for execution or ransom. What happened to other criminals is left to the imagination, and ranged from public flogging to public execution, often preceded by torture. Torture was not primarily a method for extracting espionage from a spy, it was a form of punishment, quite explicitly designed to horrify and intimidate others who needed the warning to prevent crime. Imprisonment was too expensive to be justified in the case of ordinary crime; in the Eighteenth Century, it was common to hang people for stealing a loaf of bread. Hanging alone might not be sufficiently awesome; the hanged criminal was often torn apart and the pieces of meat dragged through the streets by horses. In extreme cases, hanging was dispensed with and it was sufficient to draw and quarter the miscreant.
Without further unnecessary detail, the point must be made that imprisonment was originally devised as a humane improvement, an enlighted advance. It is nevertheless entirely true that prison conditions in every jurisdiction in every country -- are unspeakably bad. While it is probably true that public officials commonly take the view that if we must have these prisons, it is of some deterrent value to spread rumors that they are worse than they actually are. The central truth is that prisons are more expensive than most people want to spend on deterrence and punishment; so they are characteristically underfunded, and most evils grow out of the pinch-penny management which the taxpayers force on the wardens. Bleak, dank and dirty, usually a century or more old, with disgusting food, cramped quarters, and a pervasive atmosphere of suppressed violence, sometimes inadequately suppressed, these forgotten warehouses confine prisoners and jailers alike in a cloud of well-justified terror of each other. Add to this mess of the Victorian era, the more modern features of HIV, male rape and smuggled drugs, and everyone involved are ready for a new approach. If only someone could devise one.
At the Franklin Inn recently, Allen Hornblum appalled the literary lights of the city with a description of one of the lesser but nevertheless unnecessary sins of the system, the recruitment of volunteer prisoners for medical experimentation. Forget that the prisoners are all convicted of serious crimes, often as a result of a psychopathic mindset; many of them are illiterate, bored to tears, and desperate for a little spare cash to spend on the prison luxuries of sex, cigarettes, drugs, protection from other prisoners, candy and prestige. The prisons themselves set the monetary exchange rate at $.25 a day for working in the laundry; pharmaceutical firms may be unnecessarily generous in paying a dollar a day for medical volunteers. As described in his two books, Acres of Skin and Sentenced to Science, this Temple professor felt skin experiments were particularly gruesome to behold. When the prisoners were often covered with many Band-aids over their patch tests and biopsies, it gave newcomers an immediate impression that they represented widespread fighting and violence, when of course they were mostly harmless. The language of the streets is magnified in prison, and it infects the speech of the clinical investigators no matter how hard they try to blend in while they do their work.
Meanwhile, medical personnel in a prison are neither jailers nor prisoners, and commonly inject a worrisome outside observer status into the submerged civil war. Both prisoners and jailers court the nurses and doctors but occupy a dangerous ground. They can give out medical excuses, drugs, escape opportunities, and more or less impartial testimony if there is an outbreak of violence. Violence by the guards is observed without comment or intervention because the guards are the only hope of protection if the prisoner's riot. Guilty secrets are more or less kept inviolate, but both sides of the war distrust this ethical principle. Everybody, but especially a doctor or nurse, endures constant silent appraisal. Unattractive rumors abound. Consequently, medical care in prison everywhere is unavoidably substandard. Although the jailhouse lawyers would love to sue somebody for something, it's hard to see what could be accomplished for more than a brief time. There seem to be a number of billionaires who would like to do something to help this situation, but what this problem needs is not more money, but a better idea. Should we really go back to flogging, branding irons and gouging out eyes? It would be cheaper, but if the reformers really want reform, they have to suggest something that would work. So we could all agree to do it. Link to:Medical Club of PhiladelphiaThis concludes the general topic Medicine in Philadelphia. The more specific topic area of the Medical Club of Philadelphia (founded 1892 and still operating) can be reached by clicking on the title below. It's large, so wait a moment for it to come up: » Click here for THE MEDICAL CLUB OF PHILADELPHIA « The American Health Non-system
Dr. Jock Murray has recently been Chairman of the American College of Physicians. He is also a Canadian. Recently, he was invited to address the College of Physicians of Philadelphia on an evaluation of the lessons to be learned from comparing the health systems of the two neighboring nations. It was an excellent, fair, and well-balanced address. The man who introduced him referred jokingly to the American non-system and Dr. Murray emphasized two epigrams about national systems in general. No nation on earth can afford to fill all of the health demands of all its people. So, all nations confront the three main demands, to deliver everything, to deliver it to everyone, and to do so immediately (ie without waiting lists). Fulfilling any two of these three demands is possible, but to deliver all three is impossible. Comparison of health systems in various countries amounts to identifying which two of the three they have chosen to have, which one they choose to surrender. I hope and believe Dr. Murray would mostly agree to this caricature of his remarks. As a member of his audience, it does seem to be fair to acknowledge we have a non-system, and probably even fair to go further and observe we fundamentally resist those irksome constraints implicit in having a planned system. No organized system, and proud of it. But we do have something else. Let's call it a vision. Without formally stating it, or even widely acknowledging it, Americans seem to have embraced a dream that we can indeed have everything for everybody right away. Yes, we can. The method available is to gamble that research can eliminate the disease. We hope, although we know it is not certain, that cancer, schizophrenia and Alzheimer's disease will reduce the cost of care. Our model exists in Rheumatic Fever and poliomyelitis, for which there are essentially no remaining treatment costs. We know that everyone ultimately dies of something; we assume we are already paying everybody's terminal costs. Eliminating diseases postpones terminal costs, but surely does not add to them. We have knowingly and recklessly embarked on a program of pouring huge amounts of money into medical research. I believe the public mostly suspects that much of our present high cost of health insurance eventually finds its way into supporting research, and the public mostly acquiesces in whatever cost-shifting is involved. The people who devote their lives to research in turn vaguely recognize that we might reach a point where the country cannot afford this gamble any longer, and they could have half-wasted a career. We all vaguely understand it's a gamble; major elimination of disease might not be just over the horizon and might lead us on to indefinite postponement of a foolish dream. But those are the chances you take; we seem resolved to take them. We are going to give it a go. If we can, we are going to spend whatever it takes to give everything to everybody, right away. We are going to eliminate diseases, on the unproven but plausible assumption that doing so will eventually bring costs down. Corrupt and ContentedIn 1904, first in McClure's Magazine and then in the book Shame of the Cities, Lincoln Steffens described the root cause of Philadelphia's bad local politics as failure of the people to turn out to vote. The Philadelphia machine isn't the best. It isn't sound, and I doubt if it would stand in New York or Chicago. The enduring strength of the typical American political machines is that it is a natural growth -- a sucker, but deep-rooted in the people. The New Yorkers vote for Tammany Hall. The Philadelphians do not vote; they are disfranchised, and their disfranchisement is one anchor of the foundation of the Philadelphia organization." Just exactly a century later, a Republican member of the Legislature coined a phrase: "You show me a hundred thousand dollars, and I'll show you a Pennsylvania judge." Asked to comment, two Democratic politicians on the inside (although one is dead and the other is in Federal prison for embezzlement) replied: "That isn't precisely so. The precise way of stating it is that, to be elected a judge has two basic requirements. The first is the approval of a local ward leader. The second is the expenditure of between seventy and hundred-thirty-thousand dollars. With these two requirements fulfilled, just about anyone can be elected judge, regardless of legal qualification." Is it a mystery why we have a malpractice crisis? Other explanations are offered, but this one, the system of "elected" judges, should be examined first. It's a slightly worse system than appointing them. Someday, someone will discover why state courts are much more corrupt than federal ones. Is the court system getting worse from the bottom up? Or getting better from the top down?
Picking Up the Usual SuspectsThe federal government directly controls about half of health care spending and makes rules affecting most of the rest.
Every group or business which receives some of this money is alert not to lose it. Many other groups are alert for openings to get more of it. All employ sentries in Washington. False alarms are frequent, stealth attacks are a constant threat, constituents paying the bills demand immediate reassurances. Members of Congress seldom initiate a disturbance unless someone from inside an industry brings it to them. Consequently, when proposals do surface and seem to be serious, the question to be immediately answered is -- who's behind this? If you know who starts something, you can readily imagine the motive, assess the political strength, decide how to respond. With what little was generally known about the Clinton Health Care Plan of 1993, it was easy to imagine a host of people with some motive, but very hard to say who was actually pushing one. Must be a Democrat, obviously, but not immediately obvious which of several possibilities was the real agitator. Health insurance companies would always seem likely to have proposals about national health insurance. Blue Cross dominates the market in large geographical markets, mainly East Coast, and would seem fearful to lose that dominance in a major upheaval. But other market areas of the country are dominated by commercial insurance companies who might seek to upend the Blue Cross monopoly, but whose form of business would be even more seriously threatened by health insurance innovations. Most commercial health insurance was written by large life insurance companies who regard health insurance as a small sideline for the convenience of their industrial customers. Blue Cross was somewhat more comfortable with government work, particularly since the 1965 Medicare and Medicaid programs were patterned after them. However, Blue Cross was non-profit, thus lacking in incentives, and historically controlled by health care providers. That is, Blue Cross was formed by and dominated by the hospital associations, and Blue Shield was formed by and dominated by medical societies. Since doctors and hospitals were very prompt in announcing their deep concerns and uncertainties about the Clinton Plan, Blue Organizations seemed unlikely to make daring proposals so likely to provoke trouble at home. Not that some doctors and some hospitals didn't try to see what might be made of this opportunity. At the American Medical Association, certain leaders known to have Blue Shield involvement offered conciliatory remarks about waiting for further details before taking a stance but were abruptly halted by a general opinion that things had apparently already gone too far for substantive negotiation. Much the same thing occurred at the Hospital Association; the winners had too much to lose, the losers had too little influence to matter, and nobody stepped up to claim an inside track. Hospital trustees didn't know what was going on, strongly suspected something was going on and didn't like either situation. If the doctors got mad enough at a hospital, they could ruin it, and if hospitals got mad enough at Blue Cross, it too was ruined. The main strength behind the Blue Cross monopoly position was the secret discount provided to them by hospitals, which was refused to competitor insurance companies but could easily be extended in the interest of fairness. If need be. The commercial competitors wanted that discount much more than they wanted new insurance models. There is one subset of doctors and hospitals that might be suspected of generating a sweeping revision of the medical system -- academia. Medical schools think of themselves as the appropriate source of vision about the profession they are training, and they run large prestigious hospitals. Their heavy dependence on government research grants, teaching subsidies, and tuition support programs puts them in constant contact with Washington bureaucracy and politics; propinquity is a great match-maker. Their style of salaried faculty creates estrangement from making a living by being paid fees for specified services, and they are reasonably comfortable with the flaws and techniques of professional promotion within a large organization. So, a slogan which has been attributed to Wilbur Cohen himself does not greatly jar on their ears. The author of the Medicare Act is said to have announced that the entire medical system of America could be accommodated by thirty or forty Mayo Clinics. Twist that just a little, and you are imagining he said forty or fifty medical school teaching hospitals. The briefest contemplation and rebuttal will knock down that proposal, such as pointing out that we have several times that many teaching hospitals at present without achieving anything like the nation-wide coverage envisioned. After absorbing the administrative chaos of readjusting to that model, you would confront the old repeated history of grossly overestimating, and then grossly underestimating, the future manpower needs of a medical system in the process of constant scientific turmoil. Suppose you built the fifty Mayo Clinics and found you needed two hundred? Suppose you built two hundred and found you needed seventy? And then, finally, remember that each big city could expect to contain one of these organizations, but the fewer of them there are, the longer the distance everyone else would have to travel to get to them. No one has even ventured to speculate how you could go about doing such a thing, let alone doing it three or four times to get it right. But, but. The infeasibility of academia at the center of medical care delivery does not eliminate the possibility that the idea underlying the Clinton Health Plan may have originated in academia, or that academia might support some similar proposal with something else at its center. Since it was soon clear that the traditional "players" in the health policy arena were unlikely to be sponsoring some self-serving policy that might masquerade as the Clinton Health Plan, the search went on. There were a number of professional groups within the medical community who had traditionally chafed at the domination of the hierarchy by physician leadership. Nurses, hospital administrators, pharmaceutical companies, druggists, corporate human resources officers, public health officials, social workers, biology teachers all represented groups who derived status with the public by displaying inside knowledge of medicine. But all of them fell silent when a physician entered the room, and tended to shift their emphasis to faults of the "system" or the "industry". Their Washington representatives placed their emphasis on changes in the existing system which might elevate the prestige and income of the members and were particularly vigilant for system modifications intended for other purposes which might nevertheless create advantageous loopholes for the members. All of this is normal striving in the good ole' American way, a polite variant of the mixture of bellicosity and restraint usually seen in the Union movement. These people wanted to improve their income and working conditions but were ultimately quite hesitant about radical proposals that might sink the ship. A quick survey showed they were not supporting any particular reform project, even though they could be counted on to support any reform project. Furthermore, they consistently injured their political strength by extending beyond economic goals to issues like radical feminism in the case of nurses, or direct advertising to the public as in the case of the drug companies, or practicing medicine without a license in the case of limited-license practitioners. These people had votes, influence, and lobbyists, but they did not have a national project for health care reform of their own devising, and they surely were not the people behind the Clinton Plan. During the six months before The Plan was presented to Congress and the Public, a White House task force said to consist of five hundred secret members was meeting under the direction of President Clinton's wife Hillary. No doubt part of their purpose was to give Hillary a public platform on which to show her stuff, with the idea of someday succeeding her husband as President sort of in the back of her mind. But most of it was also quite practical; somebody had to figure out what this proposal was going to be, and newly elected Bill had to spend most of his time learning how to run the rest of the country. Buried in here was an efficiency principle too; the staff members of every important congressman and senator were involved in the process, making the deals and surfacing the political angles before things had to come down to votes and filibusters. Meanwhile, the rest of the country had to wait outside closed doors, fed by rumors and spin. How well I remember one public seminar on the subject during this period of suspense. The audience was filled with people thought to be influential with the public, the usual suspects in that sense, too. Representatives of various interest groups were seated up front at a table, and for some reason, I had been picked to represent doctors. Next to me was a druggist who had made a billion dollars starting an HMO; it was intriguing to watch how many well-dressed women with no interest in health care paraded up to the table to show their stuff to the billionaire, while we waited for the meeting to begin. All of the usual suspects of Philadelphia medical care were at the table, each of us wondering what the other was going to say. When some last Very Important Person had wandered in and taken a seat, it was time to begin. The moderator told a funny story or two, and then asked each one of us what we thought of the Clinton Health Plan. One by one, to the utter amazement of us all, we each explained how we were opposed to it. So obviously this proposal was not coming from the usual agitators. But, remember, somebody was surely behind it. Before we take a stab at that mystery, let's humanize the usual suspects by describing a few of them. Segmented Health Insurance
Everybody knows the old insurance saw, that the big print gives but the small print takes away. If health insurance pays for one sort of thing but not another, there is anxiety that a bewildered patient can be deprived of coverage he thinks he paid for. A patient knows he was sick, that he saw a doctor, or that he went to a hospital; beyond that, it's better not to leave room for arguments. To a certain degree, this is what has made HMOs seem so threatening; complicated assurances can lead to disappointing loopholes. So, for a century it has almost been an article of religious faith that health insurance should cover everything that costs money when you are sick. However, that headlong faith is exactly why the matter needs to be subject to critical review. Not only does monolithic insurance conceal a vast system of cross-subsidies. It has existed for too long when everything else in Medicine has changed for the original premise to be immune to change. There are health insurance considerations which go beyond mere convenience of administration. Transparency and flexibility, for instance, suffer when everything is under a single blanket. Women pay a share of prostate surgeries they will never have themselves, people who hate abortions have to pay a share of them anyway. The ability to buy what you think you need is taken away, so some people who could afford what they need are unable to afford the whole package because it includes what they feel they would never need. And then there is moral hazard. Some people reach for what they don't need just because it costs nothing extra. Well, this isn't 1930; we don't need to debate the whole issue top to bottom. But there may nevertheless be a few features of global health insurance which could be advantageously teased out separately. For a first example, look at terminal care. Everybody is going to die, and mostly the cost is picked up by Medicare because most people who die are elderly. Some insight into the issue and a reasonably workable definition of terminal care is provided by the statistic that a third of the expenditures of Medicare is paid for someone in the last year of life. Statistics on the average age at death are known with great precision, so it would be easy to calculate the yearly premium cost at any age or the size of a single-premium policy needed at any age to cover the average cost of the last-year-of-life. If we are ever to fund the unfunded Medicare program, this is the place to start. And if you are wondering how you know in advance when you are going to die, you don't need to know. Just establish an independent "endowment" fund, which reimburses the current Medicare program for any expense incurred during what proves in retrospect to have been the last year. Presumably, the cost of running the unfunded portion of Medicare would then drop by a third, while the cost of the funded third would be diminished by the investment strategy of its manager. The relatively few people who die without Medicare eligibility might be treated in the same way, reimbursing whoever paid the costs, but the risk calculation would be more difficult, and a life insurance policy might be preferable. Once the younger individual with such a designated life insurance policy attained Medicare eligibility, some sort of coordination would be desirable. Everyone dies once, and no one escapes death. But terminal care benefits are not so terribly different from some other health issues. Nowadays, just about everybody can expect to have two cataract operations, and most people can expect a hernia repair, a gallbladder removal, and if male a prostate removal. Everybody ought to have a pneumonia immunization, and a colonoscopy, by age 66. It would be easy to compile lifetime risks and update them yearly, for the typical male with 1 death, 1 pneumonia vaccination, one colonoscopy, 0.76 prostatectomies, 0.59 cholecystectomies, 0.37 hernia repairs and so on. The cost of this sort of routine care is not really insurance, it is pre-payment. It is not subject to abuse, and need not be challenged or reviewed unless statistical monitoring shows that the incidence of some component was rising in a particular zip code area. In that case, what would be called for would not claim review, it would be provider review. Perhaps the reader can see where this is going. Having stripped out routine pre-payment as much as is practical, you are left with the unknowable "all other". Insurance which covers this sort of risk becomes true insurance, in an umbrella form. As medical care continues to advance, more things can be moved from "all other" to "routine". Ultimately, and probably sooner than most people would guess, you can achieve a true insurance system, defined as having a trivial insurance premium for a remote risk. From that point forward, you can direct your cost-cutting attention to reducing the cost of routine care. That would include the devising of strategies to pay for luxury versions of routine care, as desired. Health Maintenance Organizations, Reconsidered
Paul Ellwood once enjoyed the title of Father of the HMO, while the captains of industry who came so close to pushing HMOs down the nation's unwilling throat remain invisible, quite willing to let Bill and Hillary twist in the wind for the near-miss. In the fifteen years since the Plan was dropped by Congress, 10,000 major employers coerced their employees into HMOs; endured much greater employee resistance than anticipated; and watched in dismay as administrative costs ate up the savings. The National Business Coalition for Health has been transformed from its intended role into an information system for encouraging, testing and swapping experience about minor enhancements and tweakings. Much ado about, well, less than was hoped for. But in spite of all that, let me state right here that it would only take one fundamental change to make the HMO model into a popular and desirable system.
There's an underlying truism about all effective cost-saving measures in a service industry: regardless of whether you eliminate waste or cut into essentials, you have got to fire a whole lot of people. If you fire the loafers, the quality of your product is improved; if you fire the productive workers, the product is injured. The third choice is to streamline your production methods; you may maintain high quality in spite of firing some good people. But no matter how you go about it, if you are successful, it will be the result of putting good managers in charge. The American Academy of Actuaries once calculated waste in the American healthcare system to be 30%, but in spite of opportunities of that magnitude, the present design of HMOs cannot seem to do more than barely break even. And that is in spite of wide-spread dissatisfaction with denials of care, inconvenient service, and increased paperwork. There's a tragedy here. The alternative model has already been tested, shown to reduce costs, and produced the general satisfaction of both patients and physicians.
That model was the original one, called the Foundation for Medical Care, devised in Stockton and Sacramento California in the 1950s. The Foundations were expressly created to compete with Kaiser-Permanente, both for patient satisfaction and cost-effectiveness, so judging their success is simply a matter of getting out the records and submitting them to impartial evaluation. The Foundation movement was brought to a dead stop by the legislation which enabled the present employer-based version of HMO, as well as an unfortunate Supreme Court Decision (Maricopa) whose evidence was never put on trial, but based on a motion for summary judgment. The central underlying difference between an HMO and a Foundation is that an HMO is run by an insurance company, while the Foundations were formed and controlled by the physicians who worked for them. While it might be argued that circumstances have changed in the last thirty years, it still seems reasonable to suppose that physician-run HMOs remain superior to the present insurance company-run variety. The reason for this confidence is the benchmark of Kaiser-Permanente, whose only difference is that Kaiser physicians are paid salaries, and a few of the affiliates own hospitals. Kaiser systems are at present having a serious struggle in competition with an insurance company owned HMOs. Some years, some branches of Kaiser are profitable, sometimes they lose money. The triumphant flag that Foundations waved in their heyday was, "We beat Kaiser." So where is the problem? Actually, there are two. The Foundations were usually although not invariably set up as non-profit corporations because of squeamishness of the doctors about the appearance of self-dealing. That eliminated both insurance profit and incentive to interfere with payments, although it naturally displeased commercial insurance companies. Since I can name at least two HMO operators who rewarded their CEOs with more than a billion dollars each, you can understand the displeasure with the non-profit competition. The other resistance came from hospitals. The Foundation system of utilization review put a weapon in the hands of the attending physicians in their eternal tension with hospital administrators, giving the administrators little choice but to do what the physicians wanted. Essentially, what the physicians wanted was for hospital quality to be maintained while any cost cuts affected hospital revenue before they affected physician revenue. The predictably unfortunate consequences for the hospital were held in check by opening staff privileges to physicians who were not participants in the Foundation. Their vigilance and competitive power were on the side of the administrator, for the benefit of their own patients in the common hospital. Kaiser, by contrast, usually found that owning closed-staff hospitals was itself a major headache. A hidden advantage to shifting control of healthcare to physicians is that the system acquires the management talents of the staff physicians, essentially without charge. The plain fact is that most physicians hate administrative work, and it comes closer to the facts to say that physicians abandoned management chores than to say they were deprived of them. And just in case it needs restating, it is easier to teach management to a physician than to teach medicine to administrators. While there may be some initial fumbling, physicians are the logical group to be in charge of the management of a medical system, and indeed most lay people suppose they are already in charge. Unlike the situation just after World War II, physicians would now have much more enthusiasm for administration. Not only are their own incomes suffering, but they see their product beginning to disintegrate. And it has not escaped their attention that most large-hospital administrators are paid more than a million dollars a year. No doubt physician income would be enhanced by shifting from HMO to Foundation, but less than you might suppose. Physicians are a censorious lot. Technical footnote: Two technical obstacles must be overcome before Foundations for Medical Care -- HMOs run by physicians -- can be restored to viability. For sixty years, insurance has been regulated by state governments as a result of the McCarran Ferguson Law. Large corporations doing interstate business have found it quite unworkable to comply with fifty different regulators and were given relief by a Federal law called ERISA. ERISA is so large and complex as a consequence of a large number of trade-off compromises, that for many years it was deemed impossible to amend it in any way. That gridlock was broken in 2006. The Supreme Court decision in State of Arizona v. Maricopa has always seemed dubious as a result of a 4-3 decision which lacked a majority at the time it was handed down, and in any event, never had a hearing on the evidence. The decision was based on a technicality related to a motion for summary judgment. With the passage of time and changing the membership of the Supreme Court, it is easily possible to imagine a reversal of this decision. On a political level, the climate of opinion has also changed. Insurance companies, and quite possibly hospitals, might well resist. However, it is the business community which supplied the main political force for the present version of insurance company-controlled HMO. Since that model has proven to be a disappointment from the employer perspective, but the cost problem has become much worse, it may now be possible to persuade business to allow a competitive model to emerge. Immigration and Universal Health InsuranceAmong the many articles about the economic wonder of Dubai,
along the Persian Gulf, is the comment that only 20% of Dubai's residents are citizens of that country. The other 80% seem to be immigrant workers, flocking there to make $2 an hour because at home they can only make $1. America only has 12 million illegal immigrants at the moment, but comparing our problems with such extreme cases sharpens the discussion. No matter what position you take on the question of universal American health care or universal anything else for that matter, you eventually have to re-examine your beliefs about our national borders. It is plainly absurd to propose that America should provide health care for the whole world, but if we allow essentially unlimited immigration it comes close to the same thing if you provide health care for everyone who is here. The reason Dubai is a useful example is that we, too, are working our way into the fix of basing our prosperity on immigration we cannot handle. In recently seeking bids for a new roof, the choices I received were from Costa Ricans, Poles, and Puerto Ricans. True, one American citizen did inquire, but he was merely a contractor for some others, who were almost surely illegal migrant workers. Following the advice of a friend, I chose the Costa Ricans because they were rather small in size; my friend said they were less likely to get hurt falling off the roof. Although the situation in Dubai is more advanced, we seem to share the same difficulty that our economy would become pretty unworkable without immigrant labor. That problem for us does introduce an element of fairness into providing health care for people we really do depend on, or you could adopt the line that issues of practicality urge us to find a solution. Either way, you confront a dilemma, a problem offering two solutions or possibilities, of which neither is acceptable. Perhaps at least we could invent a new term, a multi lemma, defined as a problem with lots of solutions, none of which would work. Making Money (8): Virtual Money
When money and wealth were wampums, precious metals, and paper currency, these physical objects required physical protection. It was all a big nuisance, with six-guns on the belt, bank vaults, and appraisers of one sort or another. But now that wealth is merely a bookkeeping entry on someone's computer, things may be even more nuisance because verification is almost beyond us. Counterfeiting of the computer variety must be left to institutions to detect or deflect, causing them to introduce firewalls of various sorts that also block legitimate inspection by customers. "Trust but verify" doesn't work so well in this environment. Let's use a personal example, slightly fictionalized to protect the innocent. Several software products now exist to download transaction information automatically from various institutional sources to a customer's home computer; they are either free or cost a nominal amount, and are quite "user-friendly". In my case, however, the reports they generated were quite significantly at variance from the monthly reports which were issued directly by my counterparties. Dear Sirs, Please explain. What I soon discovered was that everyone blamed someone else, and everyone blamed me for bothering them. Quite obviously, I had little understanding of these specialized accounting niceties, and quite obviously I had too much spare time on my hands. Telephone help desks, often located in India, will not give out telephone numbers for incoming calls and are programmed to check the size of your account before placing you in a call-back queue. The first call is usually taken by a trainee whose job it is to screen out the silliest sort of help request, and then to refer to a supervisor if things rise in complexity. Supervisors have supervisors. That's if you are lucky. More commonly, the tedious software business has been farmed out to a vendor, and the contracting agency has neither the necessary understanding of the issue nor any ability to fix it. From the sound of it, the vendor often gives the contracting agency the same sort of isolation treatment that they would give a customer if he could find their telephone number. And guess what. At the end of the day, one of those high-handed defensive linemen -- turns out to have been at fault. Let's explain one problem. On the surface, we were talking about a $40,000 difference in account balances; one may have been correct, but a second one must have been wrong. That rises to lawsuit level, so the matter got intensive study. It turns out the stockbroker had misinterpreted instructions for a "sweep-account" system. When a stock in your portfolio pays a dividend, the amount of the dividend is subtracted from that stock's line item and added to the line item of your money-market fund. That's fine, but there is one exception. When the money market fund itself pays a dividend, subtracting that dividend cancels out the addition, and the dividend essentially disappears from your net worth. Was this intentional? Certainly not; no one could stay in business doing that. It's not even a highly stupid error, since you can easily see yourself making the same oversight of the one implicit exception to the rule of sweep accounting. Because of this "bug" in the program involved one institution making a mistake and transmitting it to a second institution, the systematic error did not unbalance any books, until it reached mine. But since I did not detect the error for five months, there must be dozens, hundreds, maybe thousands of customers who did not detect it. Ouch. Do the math yourself to judge whether this was a serious error. This illustration, only one of several on my personal report, leads to at least two larger principles. The first is that the transformation of money from tangible to virtual has occurred so rapidly that bullet-proof safeguards have not had time to emerge. After a century of use, most people cannot balance their checkbooks, but enough people can balance them so that systematic errors are not likely to slip past. When enough people with home computers repeatedly test the internal complexities of their virtual money accounts, confidence will develop that the system is probably working. Confidence is an important matter; it is possible to imagine quite a bank panic if the public suddenly got the idea that virtual money is maybe a mere vapor. In fact, the securitized credit panic of 2007 is a little like that. With a few new regulations and a lot of computer programming it surely will be possible to know who owns how many bum mortgages. That innovative mortgage system got ahead of its tracking verification, and we now just have to hope nothing serious happens before that gets fixed. The second important lesson is that our health insurance system has a similar problem of far greater size and complexity. We are here talking about at least ten percent of Gross Domestic Product, in which one daily unit of measurement is in truckloads of insurance claims forms. Stocks and bonds are admittedly complicated but compared with thousands of different diagnoses, drugs, procedures, and hospitals -- verifying financial transactions is trivial compared with measuring medical ones. With a twenty billion dollar budget and ten years of lead time, we might have a shot at it. Except for the fact that during the ten-year interval, medical care will have changed so much, you will have to start over on the project. Specialized Surgeons
Local attitudes always somewhat persist among migrants from home. What's distinctive about the Philadelphia diaspora is how unconscious most of them are about still carrying the hometown mark. Philadelphia leaves a prominent birthmark, but it's sort of back between your shoulder blades and you forget it's there. What occasions this observation is a Christmas call from a prominent California surgeon who was once my roommate, back in the days when residents were actually resident in the hospital. More than fifty years ago Bill Doane also served as best man at my wedding. Our conversation turned to clots in the lung, and he related a story. He had once fixed a hernia for a 22-year old girl in the days when it was customary to keep hernia cases in bed for a while. Getting out of bed for the first time, she coughed and turned blue, suddenly on the edge of death. Taken back to the operating room, her chest was opened, and Bill removed a clot which was essentially a cast of the blood vessels of one entire lung. As surgeons like to say, she then did very well. One doctor can tell such a story to another doctor in four sentences, while lay people who overhear it miss the whole point. The fact is, not one surgeon in ten thousand today could carry this off. Nowadays we train thoracic surgeons to open the lungs; they never repair hernias. Conversely, we train hernia surgeons to fix a dozen hernias daily through a little telescope; they never open a patient's chest. So it is hard to imagine many contemporary surgeons who could recognize this disastrous complication of hernia repair, then fix it themselves in time to rescue the patient. Although this disheartening decline into repetitive super specialties has been forty years in the making, it has been recently popularized with the general public by Regina E. Herzlinger, a Harvard business professor. Writing books and speaking to businessmen groups, she has popularized the proposal to outsource the general hospital into what she calls "focused factories." She rightly characterizes the medical profession as reluctant. She's a nice person, and undoubtedly sincerely believes focused factories will save money, improve quality. But we must not let this idea take hold.
Specialty hospitals have actually been given more than a fair trial. About a hundred years ago, the landscape was peppered with casualty hospitals, receiving hospitals, stomach hospitals, skin and cancer hospitals, lying-in hospitals, contagious disease hospitals, and a dozen other medical specialty boutiques. With a few notable exceptions, they all failed for the same reason. Sooner or later they found they could not adequately service their specialty without the backup of a full hospital service. Children's hospitals do thrive, but they have patients who are generally of the wrong physical size to fit adult hospital facilities and equipment. There are plenty of things to regret about general hospitals' design, but the inescapable fact is they all must have a very wide range of services to perform any mission, no matter how discrete. It would be still better if the doctors had an equally wide range of skills in their own heads, but the avalanche of innovation and lawsuits has forced sub-specialization, compartmentalizing, and narrowness of viewpoint. Circumstances have forced the profession to hunker down, but that trend must be resisted, not celebrated. The instant and successful repair of pulmonary embolism make a dramatic illustration, but the reasons for broad medical training are more extensive than that. In the first place, it is much cheaper to use the generalist office than to bounce people to a gastroenterologist for heartburn, a psychiatrist for anxiety, and a dermatologist for pimples. The American employer community is desperate for a way to reduce its burden of employee health costs, and flocks back to their nurturing business schools for advice. They would do better to seek repeal of the tax dodges which tempted them into their present muddle, of course. But in any event, they must be persuaded to recall the disaster of managed care and at least, avoid meddling in hospital design. That's the cost issue, where specialization surely raises costs. Constant repetition of the same procedure seems superior to first-time fumbling, although it is questionable how long it takes a well-trained surgeon to pick up a new procedure and do it well. But for this system to work, the referring physicians need to be more skillful, not less, in choosing a good one to refer to. There's just nothing like the experience of working for a few weeks in the specialty as a rotating intern, to tell you what to look for and what to avoid. If every doctor in a hospital is making a dozen internal referrals a day, the cumulative effect on the quality of the whole institution is dramatic -- when they have had sufficient past involvement in the specialties to which they now only refer patients. Some specialists will become popular and rich; others will sulk around unnoticed for a while, then go elsewhere. This process, of course, occurs everywhere; what's institutionally distinct is the culture underlying the standards for preferences. We'll talk later about the Doane brothers of Bucks County, who were judged to be too handsome to hang. Right now, the point of this story can be summarized by the old Pennsylvania Hospital adage, that you must first be a good doctor before you can be a good specialist. Not only was the Pennsylvania Hospital the first in the nation. For sixty years it was the only hospital in the nation, and for decades after that, it was the only hospital in Pennsylvania. In medical history circles, it is said that the history of American medicine, is the history of the Pennsylvania Hospital.
Wow, fantastic blog layout! How long have you been blogging for? you made blogging look easy. The overall look of your web site is wonderful, let alone the content! kcbdegfedfde
Thank you so much for a gret site(I have NO idea how I found it). I'm in Florida, but I love Philly!!!! Great medicine, great vets,umm..great posions.
Happy New Year
67 Blogs
Nation's First Hospital, 1751-2016
Franklin Crown Soap
Pembertons
A Toast to Doctor Franklin
July 4, 1776: Patients in the Pennsylvania Hospital on Independence Day
The First and Oldest Hospital in America
Pennsylvania Prison Society
Germantown Nurses the Yellow Fever, 1793
Dr. Cadwalader's Hat
College of Physicians of Philadelphia
Joseph Priestley, Shaker and Mover
Abortion
Old Blockley (P.G.H.)
A Toast To Silas Weir Mitchell, MD
Eakins and Doctors
Emperor's Doctor
Discipline for the Disciple
Goat Head Merchant
Lin
Mind Your Manners
Funny Toes: A Physician Viewpoint
A Toast To J. William White, MD
Yet Another Toast to Dr. J. William White
Albert C. Barnes, M.D.
Victor Rambo, Indian Eye Surgeon
Illicit Drugs are Eliminated in Philadelphia
Computerizing Medical Care
Cost of Medical Care
Working Girls Get the Faints
Kenneth Gordon, MD, Hero of Valley Forge
Money Bags
Nobel Prize: Michael Brown, MD
House that Love Built: Ronald McDonald of Philadelphia
Getaway
Radioactive River Bend
Inscrutable Chinese
Dinner With Hoffa
Philadelphia in 1976: Legionaire's Disease
Contemporary Germantown
National Business Coalition on Health
Equal Pay for Equal Work
A New Gorilla in the Cage
Be Careful What You Wish For
Nowheres-ville
Healthcare Reform: Looking Ahead (1)
Healthcare Reform: Looking Ahead (2)
Healthcare Reform: Looking Ahead (3)
Health Maintenance Organizations (HMO)
Hold the Presses
Intelligensia, Philly Style
Friends Lifecare at Home
Please Don't Lose Any Sleep Over This
A New Food and Drug Category
Membership and Fellowship in the College
Unequal Health in an Unequal World
Community Volunteers in Medicine
Exit, Pursued by a Bear
Durance Vile
Link to:Medical Club of Philadelphia
The American Health Non-system
Corrupt and Contented
Picking Up the Usual Suspects
Segmented Health Insurance
Health Maintenance Organizations, Reconsidered
Immigration and Universal Health Insurance
Making Money (8): Virtual Money
Specialized Surgeons
|


 >
>
















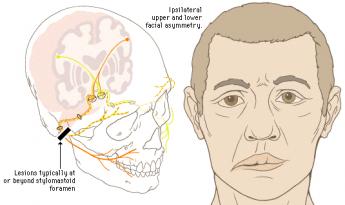




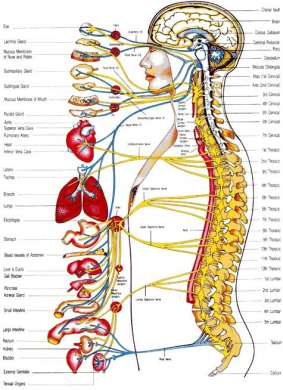




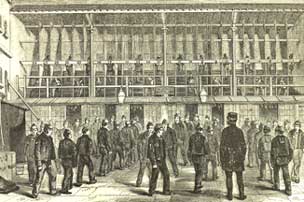



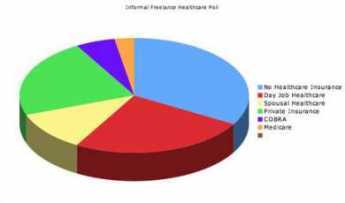








 Refugees from Haiti slave revolts brought Yellow Fever to south Philadelphia.
Refugees from Haiti slave revolts brought Yellow Fever to south Philadelphia.
 Every proposal for eliminating illicit drugs has failed except the one Philadelphia used after World War II.
Every proposal for eliminating illicit drugs has failed except the one Philadelphia used after World War II.
 Healthcare is mainly information processing, but utilizing computers has been a disappointment. Be prepared for high costs and continuing disappointment for decades to come.
Healthcare is mainly information processing, but utilizing computers has been a disappointment. Be prepared for high costs and continuing disappointment for decades to come.
 When Medicare started it was chaos, worse confounded.
When Medicare started it was chaos, worse confounded.
 The river geography around Pottstown created a lot of history.
The river geography around Pottstown created a lot of history.
 American tourists in Tian a men Square never even knew they were present at one of the great revolutionary riots of the century.
American tourists in Tian a men Square never even knew they were present at one of the great revolutionary riots of the century.
 Large employers, distressed by costs of employer-based health insurance, had formed a coalition to do something radical about their problem when the Clinton Health Plan burst into the news. Both groups decided to have a joint look at Health Maintenance Organizations (HMO).
Large employers, distressed by costs of employer-based health insurance, had formed a coalition to do something radical about their problem when the Clinton Health Plan burst into the news. Both groups decided to have a joint look at Health Maintenance Organizations (HMO).
 After the Clinton Health Plan faded, but before new ones emerged, participants thought it safe to talk to graduate students studying the event. What emerges is a picture of big business pulling the plug.
After the Clinton Health Plan faded, but before new ones emerged, participants thought it safe to talk to graduate students studying the event. What emerges is a picture of big business pulling the plug.
 When money was tangible you had to guard it, now that it's mostly virtual you have to verify it. Hardly anybody can, and that's a problem.
When money was tangible you had to guard it, now that it's mostly virtual you have to verify it. Hardly anybody can, and that's a problem.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}