1 Volumes
Insurance in Philadelphia
Early Philadelphia took a lead in insurance innovation. Some ideas, like life insurance, flourished. Others have faded.
A Fair Plan for Fire Insurance (and Health Insurance, too?)

|
| Penn Mutual |
The Fair Plan (sixth and Chestnut, Philadelphia) is a fire insurance company with unusual features. Some day, it is to be hoped some scholar will write a book about the highly mixed motives of the people who created it, compared with the unexpected ways it did or did not fulfill original expectations, of both its creators and its enemies. The Fair Plan only issues fire insurance on houses, if other insurance companies have turned that house down as a bad risk. Such risky houses would normally draw higher premiums for fire insurance, but the Fair Plan insures these risky houses at normal rates. Therefore, it loses money, which is made up by the other regular fire insurance companies in the state in proportion to the business they do, obviously thus raising the price of fire insurance for everybody. But in this way, Pennsylvania guarantees that everybody can get fire insurance. Is this a good idea? Might this be a way to give health insurance to all those people who can't get health insurance? Let's talk about the Fair Plan.
We'll set aside discussion of whether the Fair Plan was a product of cynical politicians pandering for votes, or whether it was a noble gesture for fairness and equality for our poorer citizens. It very likely had elements of both motives in it, but that doesn't matter any more. It's a form of hidden taxation, of course, and it has the result of making Fire Insurance seem more expensive in Pennsylvania than in other places that do their social work with real taxes. Go too far with that, and people will end up buying their insurance in Bermuda instead of boarded-up former fire insurance companies in Pennsylvania.
As the story is now told, the regular insurance companies had a choice of taking the "substandard" applicants in turn ("Assigned Risk") or creating a new company (Joint Underwriting Association). They decided they preferred the JUA. So a company was formed which specializes in nothing but bad risks, including a few arsonists and other unmentionables, but mostly poor people in bad neighborhoods. If we are ever thinking about following the Fair Plan model in health insurance, it would run the risk of being accused of creating a two-class healthcare system. But no one seems to bring up that rhetoric about fire insurance, primarily because there is comparatively little intrusion of politics in the matter, This system is given orders to spread the extra cost of universal fire insurance out to the policy holders of all fire insurance, and it does it very efficiently, without extending its mandate into setting firefighter wages, running fire departments or repainting scorched woodwork. The fundamental decision was whether to spend Society's money this way. Once that decision is taken, the task is to do it efficiently. Notice, this is not compulsory fire insurance; it is compulsory availability of fire insurance.
After the Fair Plan had been running for ten or so years, a funny thing emerged. There were years when the Fair Plan made a profit! The fire insurance industry had absorbed the Fair Plan into their scheme of things, and felt free to increase the number of applicants they rejected, during years when money was tight or business was bad. If you had compulsory availability of fire insurance, the provision of a company which could not refuse an application made it possible for every other company to refuse when it pleased. When the economy encouraged rejection, a better class of applicant came to the Fair Plan, which made the plan more profitable. When economic conditions reversed, this reversed, and the Fair Plan again lost money. For this reason, the insurance industry is very anxious to prevent the Fair Plan from becoming political, or getting tangled up in worthy but extraneous ventures. And that's probably a good model, too, if we are considering adopting a similar system for the health insurance world: stick to your mission.
Since this simple, tested idea never seems to get into the discussion phase of present agonizing over health insurance for the uninsured, it's one clear sign that such discussions at present are not terribly serious.
"New" Health Care Reform, 1965

|
| Lyndon Johnson |
In 1965, Lyndon Johnson caused the enactment of two amendments to the Social Security Act, Titles 18 and 19. Title 18 is now called Medicare (for the elderly), and Title 19 is called Medicaid (for poor people). These two laws were cobbled together as negotiated compromises; the history of this contraption no longer concerns us. The outcome is that Congress created a Federal program for the elderly, and a state-administered program for the poor, partly financed by the states but mostly financed by federal taxes. The states howl that Medicaid is an unfunded mandate, and the Federal bureaucracy snarls that the states are mismanaging someone else's money. The welfare patients are bitter about second-class treatment, and doctors have as little to do with this system as possible. The focus of this article, however, is on the harmful effect of Medicaid on hospitals. Of all the stakeholders affected by Medicaid, the hospitals have historically been the best treated. Nevertheless, it has brought them to the brink of ruin, most of them acknowledge it, and matters are so hopelessly snarled that it is time to call for a transfer of the medical components of Medicaid to Medicare. In plain language, that means replacing state administration with federal Medicare management.
It may seem peculiar to call for extracting the medical components from a medical program. Forty years of creeping modifications in fifty different state directions have resulted in many state Medicaid programs spending more on nursing homes, home care, and various educational programs -- than on the activities of doctors and hospitals as originally intended. After forty years, this creeping mandate shows no sign of abating. It may never abate, but certain parts of it could rather easily be transferred to federal Medicare program, leaving the innovative fringes to fight their own battles with state legislatures, arguing those merits independently of this issue.
From the hospital point of view, Medicaid pays substantially (20-40%) less than the costs it claims to cover. The chiseling is worse in some states than others, but it is hard to find a single state Medicaid program which clearly pays its costs in full. Medicare is pretty tight-fisted, too, but at least a majority of knowledgeable insiders would admit it comes pretty close to paying its audited costs. Everybody else pays more than costs, but for this discussion that is irrelevant. Government as a whole is not paying its fair share, the state-administered portion is responsible, and there was never any non-political justification for having two programs. So, combine them. Other components of Medicaid, however worthy in intent or effect, are the responsibility of the various states which created them. When the states have got non-hospital, non-doctor issues carved out and audited, the merits of federal funding can be examined.
Two other features of the Medicaid mess can be mentioned, so long as they are not allowed to befuddle the main message of program consolidation. In general, the proportion of elderly or poor clients in rural hospitals does not materially differ from the proportion of such clients in urban hospitals. There is institutional variation, of course, but the principal distinguishing feature is that small rural hospital is necessarily semi-monopolies within fifty-mile districts, whereas urban hospitals face competition more directly. State governments, therefore, are unable to impose discounts on rural hospitals with the same leverage and severity. Seeing this, urban hospitals have often applied political pressure on the legislature to extend comparable relief to them. Since local labor and living costs are lower in rural areas, an excuse is created to word regulations and state laws in a way which recognizes parity in the ratio of audited costs to charges rather than the charges or costs themselves. Quite often, hospital accountants can outwit legislatures in these obscurities, leading to rather obscenely high list prices for hospital services, to shift the ratio. Although it has the temporary advantage of further obscuring public market prices for such services, it constitutes a serious injury to uninsured patients. Other persons, who might perceive no personal need for insurance, are driven to buy it in order to protect themselves from gouging.
Medicare itself is certainly not perfect. The largest remaining issue confounding hospital charges can be traced back to weaknesses of a 1983 Medicare law, the Budget Reconciliation Act. Reimbursement legislation traditionally overpays initially, with every intention of paring prices down later. The providers, hardened to this maneuver, try to stonewall all subsequent amendments as long as they can. In this case, the overpayments have persisted so long they have become basic assumptions, triggering internal re-adjustments which make resolution still more difficult. A number of hospitals have been severely fined for violating the spirit of this law, however close they may come to obey the letter of it. On the other hand, other courts have held that a situation which has been allowed to persist so long can be deemed to be settled law. The result is a predicament which is quite unnecessary, and might be rather readily corrected.
But let's not wander too far from the basic proposal. The corresponding (doctor and hospital) portions of Medicaid should be consolidated into Medicare, with remaining issues settled independently. Consolidating two government programs may not quite be the "single payer" concept that others had in mind, but it resolves most of the legitimate problems which provoked that mysterious slogan.
Insuring the Uninsured is Not Entirely a Health Issue

|
| James Madison |
shrewdly observed that people could and would restrain state taxation by moving to a neighboring state. The founding fathers never contemplated health insurance or Medicaid, of course, but the same principle applies there in reverse. If one state gets too generous with health and welfare benefits, people in neighboring states will nowadays hear of it and get on a bus to relocate advantageously. A flood of new low-income citizens may or may not be what a particular state wants, depending on local economic conditions.
For example during the great depression of the 1930s,

|
| The Great Depression |
Unemployment was so widespread that no state dared attract still more of it with generous welfare benefits. On the other hand, during the recovery period that followed World War II, the industrial northern states definitely did attract cheap labor from the southern states, using better health care, freely available, along with better unemployment benefits. In each case, employers alternate between wanting cheap labor or low taxes, while labor representatives relax or toughen their resistance to the cheap competition. Politicians are always looking for the argument that carries the most votes. If you want to understand the persistence of employer-based health insurance alongside unobtainable health insurance for others, look into this trio of motivations.
While it's true state legislatures must tend to the infrastructure, crime conditions and education, they can in the main be regarded as debating societies between employers and labor. There is some, but not much, the difference between Republicans and Democrats on the Medicaid issue. A Democratic Governor will welcome an influx of low-income voters who will normally vote for his party, but labor unions will soon remind him that enough is enough. A Republican Governor will gladly supply cheap labor for the state's employers until rising taxes bring an end to his support. Since the financial stability of the local hospital can be badly jarred by the instability of Medicaid payments, doctors soon get annoyed with the misalignment between state motives and the welfare of their patients. It is not much of an exaggeration, that state coffers might be overflowing with the surplus, but the budget of Medicaid will not rise a penny if it would attract poverty migrants from neighboring states during a period of high unemployment.
The obvious solution is a federal one, imposing uniform standards. But think that over a little before you jump at it. If the federal government pays all of Medicaid costs, it is going to want to administer the program. All states resist that idea, more so if local and federal political domination is in conflict. Small states will universally be fearful of being overwhelmed by large neighbors, particularly when they have achieved advantageous niches. The disastrous condition of the auto industry might persuade Michigan to agree, but Tennessee and other states with Japanese car plants might disagree. As you get close to the border of large states, hospitals near the border can often attract many patients from the other state; strange political bedfellows can link arms in Congress when you might not expect it.
None of this, absolutely none of it, has to do directly with medical care. But the quality of health care is strongly affected, and doctors are sick of hearing about poor sick folks when the real issue is labor availability. The voice is Jacob's voice, but the hand -- is the hand of Esau.
What Good Did Medicare Do?

|
| Amy Finklestein |
An article in the Wall Street Journal Amy Finkelstein of MIT describes evidence that Medicare seemingly produced no provable increase in longevity during the period she studied, which was 1965 to 1975. Thinking back to that time in the practice of Medicine, the conclusion while surprising seems entirely plausible after a little reflection. Our system of charity care was good enough so I really doubt if very many people were allowed to die prematurely because of poverty in 1965, at least in Philadelphia. Charity took care of them. Elective repairs were an entirely different matter, however. Working in charity clinics at the time, I well remember that almost every patient seemed to have bad teeth, an unrepaired hernia, untreated varicose veins, or a positive Wasserman and similar threatening but non-fatal conditions. There existed a vast backlog of untreated non-fatal conditions, almost to the point where it seemed we would never catch up, but of course, we did eventually catch up. Whatever the costs of the government health programs during that decade, they mainly reflect that huge backlog project of correcting health impairments which were nevertheless not an immediate threat to life, in addition to lifting the former financial burden from our charity institutions of treating conditions which were undeniably life-threatening.
From this historical experience it can be deduced that any new proposals for modifying or reforming the medical system should start with the medical situation as we happen to find it. If a great many people are dying of treatable conditions as they are in Asia and Africa today, then it is likely that extra finance will promptly reflect itself as improved population longevity. If that's not the case and other institutions are providing emergency care, you must then look among the backlogs of untreated conditions -- in that locality -- for a justification of new costs and disruption. Since even the non-urgent backlog in America has now been almost totally eliminated, something else must be proposed as a goal for legitimate improvement. Otherwise, you would have to be so far-sighted that you make a decision to spend an extra 10% or so of the Gross Domestic Product for benefits, every year for ten years until some unpredictable long-term benefits appear. It's difficult to imagine our political process launching forth on such an adventure.
|
| NIH Map |
However, let's continue to look at what did happen, to see what arguments we might have been imaginative enough to adopt. First of all, we can see that the quality of life of the elderly generation, the one I now belong to, has been enormously enhanced by joint replacement and cataract repair --significantly reducing wheelchair crippling and blindness. Neither of these benefactions can be said to result from a brilliant insight by a genius, but rather a slow, incremental process of adding small enhancements until the desirable result becomes standard practice. This sort of development, as in research and development, is very likely a response to a general increase in the funding of the provider community, as contrasted with targetted extra appropriations to the NIH for example. A plausible case can be made for asserting that the undesignated increased funding of the early Medicare program gave tens of thousands of elderly people -- in the next generation -- a comfortable life rather than a miserable one, several decades sooner than a more frugal medical system would have done.
Secondly, life expectancy did finally increase substantially, perhaps extending an average of ten or more years of life in the period subsequent to the enactment of the Medicare Act. But it did so only after a fifteen or twenty-year lag. It's uncertain how much we may credit Medicare with this benefit, however; the increased basic research funding of the National Institutes of Health seems plausibly responsible. However, at least half of the longevity benefit must be credited to research efforts in the private pharmaceutical industry, which was funded in large measure by Medicare dollars, recirculated through drug purchases. But there's restrained exuberance about even these miracles, which were surely the greatest medical advances in human history.
We have greatly extended the comfortable, useful life of our population, but now must grudgingly admit we directed these benefits to a group of people who are no longer engaged in economic activity. Unemployable people have been transformed into employable ones, but sadly we have mainly given a twenty-year vacation to people who are capable of doing productive work, but don't. Instead, we import millions of foreigners to do the work or outsource it, which accomplishes much the same result without the demographic disruptions. Worse still, we may find these people will often outlive their savings, so the extra longevity could result in years of economic misery and despair, not necessarily an improvement on the physical and medical varieties. In other words, if we had possessed the foresight to see that ultimately improved longevity and life quality was a worthwhile goal, we should then have simultaneously taken the steps to improve economic circumstances which make that medical miracle seem worthwhile.
As we now consider further steps to over fund medical care, or reform it, or make it universal or whatever, perhaps there will be time to consider whether other improvements in American life are needed before there is a net beneficial effect. Either undertaken simultaneously with the health care financing initiatives or even possibly, instead of them.
Community Volunteers in Medicine

|
| Comm Volu In Medicine |
Mary Wirshup has a very different medical background from mine, but she's my kind of doctor. I couldn't help wishing, as she addressed our urban luncheon club, there could be thousands more like her, even while understanding more fully than she seems to, the reasons why doctors are driven from her behavior model. As we parted, it felt like saying a last goodbye to the Spartans marching to Thermopylae.
As 46,000 medically uninsured persons in Chester County get sickness and injuries, they know that a Federal Law prohibits a hospital accident room from refusing to see them, so ways are found to shunt patients to the CVIM free clinic, run by volunteers. This law is, in turn, a response to a government-created situation where a hospital which "accepts" patients must keep them. Any economics teacher can tell you that supply/demand issues are best addressed by price adjustment, so price controls in whatever guise lead to shortages. I must say I have little sympathy with the devious strategies which hospitals often employ to disguise their rejection of uninsured patients. At the same time, I know a lifeboat will sink if too many climbs aboard. Nevertheless, the semantic switch from lack of insurance to lack of care implies that only more insurance can surmount the barriers to care, which is absurd. For one thing, I know too many hospital administrators who are paid a million dollars a year, and one who is paid two million. And at least two health insurance executives are in the newspapers with a net worth over a billion -- yes, that's billion with a b. We have reached a point where reducing all physician income to zero would only reduce "healthcare" costs by 10%. As I look at Dr. Wirshup's modest clothing I can only surmise she plans to continue her modest living until she is 80 years old, after which her savings might see her out. Squeezing physician reimbursement is not intended to save significant money, nor intended to restore physician incomes to more equitable levels. It is intended to address the oversupply of physicians without confronting either the universities or the foreign trained lobby.
The elite tranche of medical schools do their part to relieve physician oversupply without reducing class size, through the encouragement of their students to go into research. I was well along at the National Institutes of Health before I finally decided I had not gone into medical school with that goal, and returned to teaching and patient care in a more satisfying model not too different from CVIM's obviously Pennsylvania Dutch spirit. The Amish at the far western end of Chester County reject the whole idea of insurance; their most characteristic statement is "Don't send me no bills." That attitude is rather a contrast with the shiny housing and automobiles in the Silicon Valley developments of Southern Chester County, or even with some rather bewildered Quaker farm families scattered over the rest of the county next to the horsey set. Chester County is America.
On Second Street in Society Hill, next to the park where William Penn's house stood and a few feet from Bookbinders, is the house of Dr. Thomas Bond. Bond conceived the idea of building the first hospital in America and with Franklin's publicity machine succeeded in getting it built, to care for the "sick poor". Dr. Bond started a second enduring tradition as well. When the Legislature expressed doubt that the institution was sustainable, he pledged to convince the local medical profession to serve the poor without charge. Some of the legislators who voted for the measure did so in the belief that charity care would never appear so the gesture would be without cost. The physicians did indeed come forward, in sufficient numbers to run many institutions for two hundred years. In 1965 health insurance made its national appearance and has regarded the benchmark low costs of charity care as a threat, ever since.
Picking Up the Usual Suspects
The federal government directly controls about half of health care spending and makes rules affecting most of the rest.

|
| Claude Rain |
Every group or business which receives some of this money is alert not to lose it. Many other groups are alert for openings to get more of it. All employ sentries in Washington. False alarms are frequent, stealth attacks are a constant threat, constituents paying the bills demand immediate reassurances. Members of Congress seldom initiate a disturbance unless someone from inside an industry brings it to them. Consequently, when proposals do surface and seem to be serious, the question to be immediately answered is -- who's behind this? If you know who starts something, you can readily imagine the motive, assess the political strength, decide how to respond. With what little was generally known about the Clinton Health Care Plan of 1993, it was easy to imagine a host of people with some motive, but very hard to say who was actually pushing one. Must be a Democrat, obviously, but not immediately obvious which of several possibilities was the real agitator.
Health insurance companies would always seem likely to have proposals about national health insurance. Blue Cross dominates the market in large geographical markets, mainly East Coast, and would seem fearful to lose that dominance in a major upheaval. But other market areas of the country are dominated by commercial insurance companies who might seek to upend the Blue Cross monopoly, but whose form of business would be even more seriously threatened by health insurance innovations. Most commercial health insurance was written by large life insurance companies who regard health insurance as a small sideline for the convenience of their industrial customers. Blue Cross was somewhat more comfortable with government work, particularly since the 1965 Medicare and Medicaid programs were patterned after them. However, Blue Cross was non-profit, thus lacking in incentives, and historically controlled by health care providers. That is, Blue Cross was formed by and dominated by the hospital associations, and Blue Shield was formed by and dominated by medical societies. Since doctors and hospitals were very prompt in announcing their deep concerns and uncertainties about the Clinton Plan, Blue Organizations seemed unlikely to make daring proposals so likely to provoke trouble at home.
Not that some doctors and some hospitals didn't try to see what might be made of this opportunity. At the American Medical Association, certain leaders known to have Blue Shield involvement offered conciliatory remarks about waiting for further details before taking a stance but were abruptly halted by a general opinion that things had apparently already gone too far for substantive negotiation. Much the same thing occurred at the Hospital Association; the winners had too much to lose, the losers had too little influence to matter, and nobody stepped up to claim an inside track. Hospital trustees didn't know what was going on, strongly suspected something was going on and didn't like either situation. If the doctors got mad enough at a hospital, they could ruin it, and if hospitals got mad enough at Blue Cross, it too was ruined. The main strength behind the Blue Cross monopoly position was the secret discount provided to them by hospitals, which was refused to competitor insurance companies but could easily be extended in the interest of fairness. If need be. The commercial competitors wanted that discount much more than they wanted new insurance models.
There is one subset of doctors and hospitals that might be suspected of generating a sweeping revision of the medical system -- academia. Medical schools think of themselves as the appropriate source of vision about the profession they are training, and they run large prestigious hospitals. Their heavy dependence on government research grants, teaching subsidies, and tuition support programs puts them in constant contact with Washington bureaucracy and politics; propinquity is a great match-maker. Their style of salaried faculty creates estrangement from making a living by being paid fees for specified services, and they are reasonably comfortable with the flaws and techniques of professional promotion within a large organization. So, a slogan which has been attributed to Wilbur Cohen himself does not greatly jar on their ears. The author of the Medicare Act is said to have announced that the entire medical system of America could be accommodated by thirty or forty Mayo Clinics. Twist that just a little, and you are imagining he said forty or fifty medical school teaching hospitals. The briefest contemplation and rebuttal will knock down that proposal, such as pointing out that we have several times that many teaching hospitals at present without achieving anything like the nation-wide coverage envisioned. After absorbing the administrative chaos of readjusting to that model, you would confront the old repeated history of grossly overestimating, and then grossly underestimating, the future manpower needs of a medical system in the process of constant scientific turmoil. Suppose you built the fifty Mayo Clinics and found you needed two hundred? Suppose you built two hundred and found you needed seventy? And then, finally, remember that each big city could expect to contain one of these organizations, but the fewer of them there are, the longer the distance everyone else would have to travel to get to them. No one has even ventured to speculate how you could go about doing such a thing, let alone doing it three or four times to get it right. But, but. The infeasibility of academia at the center of medical care delivery does not eliminate the possibility that the idea underlying the Clinton Health Plan may have originated in academia, or that academia might support some similar proposal with something else at its center.
Since it was soon clear that the traditional "players" in the health policy arena were unlikely to be sponsoring some self-serving policy that might masquerade as the Clinton Health Plan, the search went on. There were a number of professional groups within the medical community who had traditionally chafed at the domination of the hierarchy by physician leadership. Nurses, hospital administrators, pharmaceutical companies, druggists, corporate human resources officers, public health officials, social workers, biology teachers all represented groups who derived status with the public by displaying inside knowledge of medicine. But all of them fell silent when a physician entered the room, and tended to shift their emphasis to faults of the "system" or the "industry". Their Washington representatives placed their emphasis on changes in the existing system which might elevate the prestige and income of the members and were particularly vigilant for system modifications intended for other purposes which might nevertheless create advantageous loopholes for the members. All of this is normal striving in the good ole' American way, a polite variant of the mixture of bellicosity and restraint usually seen in the Union movement. These people wanted to improve their income and working conditions but were ultimately quite hesitant about radical proposals that might sink the ship. A quick survey showed they were not supporting any particular reform project, even though they could be counted on to support any reform project. Furthermore, they consistently injured their political strength by extending beyond economic goals to issues like radical feminism in the case of nurses, or direct advertising to the public as in the case of the drug companies, or practicing medicine without a license in the case of limited-license practitioners. These people had votes, influence, and lobbyists, but they did not have a national project for health care reform of their own devising, and they surely were not the people behind the Clinton Plan.
During the six months before The Plan was presented to Congress and the Public, a White House task force said to consist of five hundred secret members was meeting under the direction of President Clinton's wife Hillary. No doubt part of their purpose was to give Hillary a public platform on which to show her stuff, with the idea of someday succeeding her husband as President sort of in the back of her mind. But most of it was also quite practical; somebody had to figure out what this proposal was going to be, and newly elected Bill had to spend most of his time learning how to run the rest of the country. Buried in here was an efficiency principle too; the staff members of every important congressman and senator were involved in the process, making the deals and surfacing the political angles before things had to come down to votes and filibusters. Meanwhile, the rest of the country had to wait outside closed doors, fed by rumors and spin.
How well I remember one public seminar on the subject during this period of suspense. The audience was filled with people thought to be influential with the public, the usual suspects in that sense, too. Representatives of various interest groups were seated up front at a table, and for some reason, I had been picked to represent doctors. Next to me was a druggist who had made a billion dollars starting an HMO; it was intriguing to watch how many well-dressed women with no interest in health care paraded up to the table to show their stuff to the billionaire, while we waited for the meeting to begin. All of the usual suspects of Philadelphia medical care were at the table, each of us wondering what the other was going to say. When some last Very Important Person had wandered in and taken a seat, it was time to begin. The moderator told a funny story or two, and then asked each one of us what we thought of the Clinton Health Plan. One by one, to the utter amazement of us all, we each explained how we were opposed to it.
So obviously this proposal was not coming from the usual agitators. But, remember, somebody was surely behind it. Before we take a stab at that mystery, let's humanize the usual suspects by describing a few of them.
Equal Pay for Equal Work

|
| American Medical Association |
The House of Delegates of the American Medical Association holds a five day convention twice a year. The meetings last from 7 in the morning until midnight, although the main sessions in the auditorium only last eight hours a day for three days. The rest of the time is consumed with meals, committee meetings, geographical caucuses, and even cocktail parties. Newcomers often object to the numerous parties until they come to see that these are merely committee meetings in a different form, with different subsets of the organization picking up the necessary costs. This group of workaholics has to vote on several hundred issues each session, and most Delegates have little advance opinion when they enter the headquarters hotel on the first day. But after meeting with their specialty in one committee, and members of their geographical region in another, and members of their medical school alumni association in yet another, and with issue-oriented groups, political allies, and other layers of an overlapping matrix day after day -- by the time the vote is actually called for, most Delegates could safely predict the correct outcome with very few exceptions. The AMA works at its similar job with far greater intensity than Congress does because Congress has all year to do it, while the doctors have to go home to make a living. Don't worry about the parties, they are really working sessions for everyone except rank newcomers, outsiders, visitors, and wives. What is perhaps more worrisome is the rare occasion when just about every delegate arrives with one opinion and is persuaded by the leadership to adopt the reverse. That can only happen if new information is suddenly revealed, with little time to check its accuracy.
There are usually fifteen or so parties every night, hosted by large state delegations, large specialty assemblies, and coalitions of smaller groups. Fifteen drinks a night would be quite a bit for most folks, and some newcomers are duped into trying to be polite about it. The rest of us take the proffered drink, walk over to a nearby plant stand and dump it. I hate to think of how many potted palms I have fried that way. Each delegation has its own system of organizing these minutes, and I'll try to describe the Pennsylvania system.
Nobody will come to your party if you don't go to theirs, so we make a list and divide the group into those who "travel" to the parties of other states, and those who remain to host our own party, "at the door". Everyone is expected to wear a name tag, containing your name in large type underneath which is your caucus designation, in my case "Pennsylvania". The older members instruct the newer ones to put the name tag just under their right shoulder. That way, you can seem to be looking at the hand you are shaking while freshening your recollection of who in the world you are meeting. You can, of course, do anything you please, but time is short for the transaction of a lot of business, and it's just easier to do routine things the regulation way, and get on with it.
On the evening in question, I was "at the door". The formula, repeated many times, was to extend a hand of greeting and recite, "Welcome to Pennsylvania. Are you looking for some friend in particular? Let me see that you have a drink. Come on in and meet my fellow delegate, Scotty Donaldson." You can shepherd a lot of people more or less gracefully if you reduce the formalities to a routine. After several people had been brought in under the tent, a man with highly polished shoes came up, wearing a name tag that said, "Blue Cross of America". He was greeted, his hand pumped, a drink procured, and was introduced to Scotty, our most famous extrovert. I quickly turned to the next person at the door.
Well, this lady was six inches taller than I am, and fifty pounds lighter. She wore a name tag, identifying her as President of some Nurses Association, "Welcome to Pennsylvania! Is there someone from Pennsylvania you know or would like to meet? Can I......" The apparition didn't even look at me as she brushed past through the door. Heading straight for the gentleman from Blue Cross, she poked her index finger into his chest, stopped him in mid-sentence as he talked to Scotty.
"What I want to know, " she announced to this startled man, "Is when are you people in Blue Cross going to pay nurses as much as you pay doctors?" And here I must admit I have to give this guy credit for unperturbability.
"Well, madam," he said cheerfully, "I think that's going to be quite some time."
A New Gorilla in the Cage

|
| William Clinton |
News reports began to surface that big business was talking to Democrats in the White House about major revisions in the national health delivery system. That in itself was news, because big business normally forbids its employees to talk with regulators, and does not commonly welcome any new regulations. But the Clinton Administration was looking for political allies, while the business community was willing to examine proposals to lighten the burden of employer-based health insurance. The discussions soon probed whether a common system might reduce government costs of Medicare and Medicaid, and simultaneously reduce the costs of employer-paid health insurance. For years, big business had been suspicious that the health community had somehow forced employers to pay an unfairly large share of other people's health costs, through some arcane manipulation of hospital cost accounting. Their term was cost shifting.
The administrators of government programs believed the same thing was happening to them. Since the only group left to benefit were uninsured, the arithmetic was somehow wrong. A 7% population group, most of whom are young and healthy, could not account for annual premium jumps far in excess of the cost of living, occasionally as much as 30% in one year. In both governmental and business minds, the main beneficiaries of cost-shifting must be the hospitals themselves, and the doctors who control them. Somehow, it seems not to have occurred to them that this news was brought to them by their fiscal agents, the health insurance companies, and was therefore likely slanted to avoid attention to middle-man costs. Whenever major negotiations are to be held, CEOs and top politicians take over to make the deals, necessarily basing their judgments on filtered information. Since this is a familiar situation, they employ high-priced consultants.

|
| Clark Havighurst |
The five hundred secret members of Mrs. Clinton's task force were willing to listen to the ideas of anyone who had political clout, especially staff members of Congressional committee chairmen. But these people had been struggling with the problem for fifty years to no avail, so the emphasis had to be on change, on big new ideas. Universities and think tanks were especially welcome to comment, and
Clark Havighurst was particularly influential. But there had to be some kind of track record, some practical experience on which to base such an enormous national initiative. The best available model was the Health Maintenance Organization (HMO), whose most famous proponent was Paul Ellwood, a former midwestern pediatric neurologist who had gravitated into health insurance consulting. Ellwood had a vacation home in Jackson Hole, Wyoming, where he then gathered the non-government component of this movement into his front parlor. Insurance companies, human resources officials, academics, and in later stages the news media, were given the Word, an opportunity to criticize, and an opportunity to have their views coordinated with the government group in Washington. There was a rough division of labor, establishing general regions of dominance; but ultimately, the two components intended to fit together in a unified health system for the whole country, bar none. The business community began to see that inevitably, in that case, the final overarching decisions would be made in Congress.
Health Maintenance Organizations (HMO)

|
| HMO |
It's an ancient wrangle whether a manufacturer should actually own its suppliers or the reverse; or instead whether it's healthier for industry components to stand at arm's length from each other. At issue is not only what is best, but what is fair. If industry mergers seem sufficiently unfair, it will be proposed they should be illegal. That's the main substance of a lot of antitrust argument. Unfortunately, what is valid in good times may be reversed in a downturn. A prosperous supplier of materials often acts as a "cash cow", saving a merged enterprise from bankruptcy. Unfortunately, within a different economic climate one badly failing supplier can bring down the whole merged enterprise. There's also organizational friction; a temporarily prosperous unit may get to thinking it should boss the less prosperous units around. At the very least, the cash cow resists the use of its cash reserves to help "losers". Several centuries of experience have thus left a minefield of old laws, traditions, and ingrained prejudice to undermine any broad standards for what is best. In no field is this truer than the Medical Industry.
Eighty years ago in Houston, the first Blue Cross health insurance company was started for a single group of school teachers to pay for service in a single hospital. That expanded to other subscribers and other hospitals, soon making it more workable for insurance, subscribers, and hospitals to stand at arm's length, allowing for a variety of local combinations. During World War II, combat in the Pacific led shipyards to be built on the West Coast, but westward migration of steelworkers was hampered by lack of local medical facilities for them and their families. Taking advantage of the loophole provided in the wartime wage and price controls, Kaiser Industries attracted medical personnel by building hospitals, paying salaries, and offering physicians ready-made medical practices. Because of various licensing laws, Kaiser's medical enterprise was divided into two corporations, Kaiser and Permanente, so a specialized corporation within the Kaiser-Permanente Foundation could accommodate the licensed practitioners. The salaried nature of the physician organization immediately caused trouble with local fee-for-service practitioners, who were thus excluded from a large population in their neighborhood when they could not readily adjust to varying mixtures of the two payment methods. Their reaction, led by an obstetrician in Stockton, California, was also to organize dual-corporation structures which were exclusively fee-for-service. Because Kaiser had a Foundation, they also called their organizations Foundations for Medical Care. Then, as now, it proved difficult to run a practice with two different reimbursement philosophies in the same waiting room; in time, friction between the two styles tended to increase as doctors who were more comfortable with each style tended to segregate themselves. Since offers of salaries are more immediately attractive to newly-trained physicians, they flocked to California to serve the steelworkers who were in need of doctors. Fee for service, on the other hand, allowed the gradual assembly of a more durable practice composed of patients who could test what they liked before making a permanent allegiance. Essentially, the transients went to Kaiser, more permanent settlers used fee-for-service.
Thus, it came about that several models for health care reform were tested in a few smallish towns of central California. These demonstration experiments may perhaps not meet everyone's standard for scientific purity, but at least they were public examples with the dumber features knocked away. They certainly provided a laboratory where ideas could develop about topics that otherwise were merely opinions and unsupported conjecture. The Foundations demonstrated that physician-dominated organizations could contain costs and maintain quality in a satisfactory way; there had previously been doubted about their ability to contain cost. The Kaiser organization showed that salaried practice performed acceptably as well, both to most staff physicians and to a majority of the patients; there had been doubt about the willingness of the public to limit choices to a panel of assigned physicians, mostly young and usually from elsewhere. Finally, the two systems seemed to be able to live together more or less peacefully; indeed, the California public seemed reassured that two systems apparently kept each other in check.
The first main difference rested on the system of quality control. The local Foundations developed review systems based on peer review and peer pressure; these worked remarkably well, particularly in constraining non-physician costs like pharmacy, tests, and hospitalizations. Cost and quality control in the Kaiser system was more rule-bound and quicker to apply discipline, kept within bounds however by the ability of both patients and staff to jump ship for the other system. Aside from professional peer review, the Kaiser system experimented with owning hospitals, laboratories, pharmacies. Here, the experience directly paralleled the experience of manufacturing industry with its suppliers; when reimbursement was generous suppliers generated welcome revenue. When reimbursement was constrained and substandard, ancillary service losses were unwelcome. Taken overall, the Houston experience was repeated, that ownership of such facilities was mostly a headache. Indeed, subsequent experience has shown the two systems usually co-exist nicely within independent ancillary facilities.
The Stockton, or Foundation for Medical Care, approach grew popular in the West. The variant which grew up in Utah was locally popular and attracted the attention of Senator Wallace Bennett. The Bennett Amendment to the Medicare Act then picked out the peer review system as the secret of success and set up a nationwide system of Professional Standards Review Organizations (PSRO) to conduct peer review of Medicare and Medicaid patients. The drawing of boundaries around these organizations was the most difficult part, and sometimes the boundaries were inept. Rural districts were adamant that the standards of big-city medical schools were not to be applied to their scattered resources, and urban areas saw themselves as ancient Rome surrounded by hostile tribes. Although these difficulties were foreseen, it is not always possible to draw a line that will separate the cultures, particularly where the outward migration of suburban housing was more rapid than the construction of suburban medical facilities, leaving the medical culture unstable. The PSRO system was quite successful in many areas but caused trouble in others that were not adequately addressed. The central concept of the review system was that the doctors who worked together could quite readily identify the outliers, and better than anyone else could judge whether the local situation was justified. True, some practitioner might try to abuse the system to the disadvantage of his competitor, so no adverse decision was final until there had been an opportunity for outside appeal. There might even be a few circumstances requiring a still higher appeal. The system was new and untried, but it produced eminently satisfactory results from the point of view of the Federal Government paying the bills. As former President of one of the largest PSROs in the country, I will assert that there was remarkably little friction or resistance in the medical community. My very good friend, the President of the New York City PSRO says much the same, and most people would say that if you can carry off a new system in New York without a lot of argument, it must work pretty smoothly. The Government wanted to eliminate unnecessary Medicare costs, particularly in hospitals, and it wanted to maintain peace with the medical profession. Hospital costs are obscured by the wide gap between posted charges and true underlying costs, compounded by disagreement about the proper assignment of overhead charges. Charges were not the assignment of the PSRO, utilization was. Days of hospitalization per thousand enrollees fell from roughly 1000 days per thousand to roughly 200 days per thousand, and that satisfies me at least that we were doing our job; physician peer review was doable.
It is likely, however, that peer review was much more apt to produce friction in rural districts. Philadelphia has had more than a hundred hospitals for more than a century. Birds of a feather tend to flock, so the sorting-out process was already far advanced by the application of constrained referrals to practitioners who failed local standards. Mixing members of different hospital staffs on appeals committees was easy in the big cities, and the naturally censorious tendencies of many physicians could be safely counted on to produce adversary balance. Most committees seemed visibly pleased, even relieved, to discover generally good quality in their competitors' practices. However, in the much smaller and more scattered institutions in the nation's regions with low population density, these informal arrangements cannot stretch as well. When there is only one specialist in a field, for example, it is sometimes hard to know whether he is a good one or not, but always easy to say whether you like him or not. Where the population thins out, much greater wisdom is required to make judgments, the number of close cases is greater, and the limited supply of judicious reviewers is similarly stretched. At least that is my surmise, based on knowing the background of most of the AMA delegates who eventually voted 105-96 to condemn the program in a standing vote. The result was the Dornenberger Amendment, which much weakened the system when instead it should have triggered a more profound analysis and reconsideration.
Perhaps we spend too much time here describing a technical process. It is, however, at the heart of what makes the Foundation approach (sometimes called IPA or Independent Practice Association) superior to the HMO. It is now perfectly clear that both doctors and patients vastly prefer the IPA approach to the HMO, and any reasonable politician would jump at it. But there is one fear, summarized by the slogan that the Fox is guarding the Henhouse. In both systems, an attempt is made to combine insurance with the delivery of health care. In the IPA, the physicians are taking the financial risk that aggregate income will exceed aggregate costs; it's a risk contract. In the case of an HMO, the employer or the government is taking the financial risk and therefore wants to control it. If revenue is good, the doctors will prosper in an IPA; the insurance company intermediary will prosper in an HMO. Doctors will care about that little difference, but why should the rest of the country care?
Because the prospect is overwhelmingly likely that future revenues will be constricted until something hurts, and when you starve with a tiger, the tiger starves last. In the case of an HMO, the insurance middlemen will starve last, and the quality of health care will starve fairly early. That's an unwise design. When we get to the point where Congress cuts the budget and watches to see what happens, Congress will cut it some more if nothing bad happens; it will back off only if something bad happens, so something bad is certain to happen. In designing the system, you need to design the internal review authority so it will cut the waste, inefficiency, and luxury first. The reviewer, no matter who it is, will cut himself last, so you need to arrange the incentives for waste to be cut before the reviewer suffers, and quality of care only after the reviewer has suffered. If you wonder why a whole lot of special interests hate physician-dominated review systems, a short answer will be found in this synopsis. A special exception must be devised for rural health systems, which do have a unique problem.
To return to the well-worn slogan about foxes and henhouses, we have overlooked the central question. Who's the fox, and who is the hen?
National Business Coalition on Health

|
| NCOH |
In 1992 the National Business Coalition for Health was just forming at a convention in Chicago. Before I really understood what it was all about, I agreed to their flattering invitation to be the keynote speaker at the kick-off luncheon. Who suggested my name was and is a mystery to me, and I arrived in Chicago with very little idea what they wanted to hear. However, it followed the familiar pattern of inviting the speakers to stay overnight at the hotel on the evening before the meeting began and to meet for drinks at the bar with the organizing leaders. I had enough experience with public speaking to know I could learn the general slant of the thing at such an informal party and adjust the speech to the audience to whatever degree seemed needed. Among the people scattered around at tables was Harry Schwartz, who was also there to give them a speech. Harry had been on the editorial board of the New York Times for many years and was known to be generally quite favorable to physicians. We had both written books about medical care, The Hospital That Ate Chicago in my case, and The Case for American Medicine, in his. We liked each other immediately and fell into an animated cocktail conversation that would eventually be renewed every six months at the American Medical Association House of Delegates meetings, where I was a delegate and he covered the topic for various news media. As we chuckled together about one anecdote or another of medical politics, the bar gradually emptied out. It soon became clear that all the other cronies had wandered off to dinner together, so we ordered dinner on the house, neither one of us have learned just what we were there to talk about. It really didn't bother either one of us very much, since from long experience we could tell some jokes and make it up as we went along. I knew what I wanted to tell businessmen, so it was just a matter of finding a way to lead into it.
The speech seemed to go well. There were several hundred, perhaps even a thousand in attendance, quite convivial and prosperous. As executives usually do, they looked younger than you might expect from the titles on their name tags; they laughed at the appropriate points and applauded at the end. In other words, I went home from Chicago with no more idea what this organization was up to than I had before I came. At the very least, it is clear they were forming a national organization of businesses, with constituent representatives largely drawn from Departments of Human Resources. They wanted to speak for American Business with a more or less unified voice, and the topic seemed to be health care. Although fate had put me into the debate at the very earliest moment at Wills Eye Hospital, this convocation of extroverted Republicans seemed to know a lot more than I did about what was secretly afoot among the Democrats in Washington.
This Chicago tea party did one other thing for me. Many months later, when the editors of USAToday were in search of an editorial page writer who was both a physician and opposed to the Clinton Health Proposal, they called Harry Schwartz. And he suggested to me. They ultimately ended up with a Medical Editorial Advisory Board of five members, at least three of whom were far to the left of me. At the New York Times, of course, Harry Schwartz was considerably more outnumbered than I was. After it was over, Harry and I used to joke that both sides were fairly evenly matched.
Nowheres-ville

|
| Jacob S. Hacker |
In more recent writings, Jacob S. Hacker seems obsessed with social inequality, but while he was a graduate student he wrote an excellent and objective book, The Road to Nowhere containing unique insights into the politics of the Clinton Health Plan of 1993. After that hubby was over, he interviewed most of the important actors in that drama, at least those active in the liberal politics of it, and they talked freely. Like the rest of us, he was unable to identify let alone talk with the leaders of big business, who are of course still pursuing their original goals. What emerges does sound roughly accurate; Hillary Clinton and Ira Magaziner designated to find out what this health business was all about; solicit every proposal on the mind of political, particularly congressional, allies; gather and examine all the useful ideas in circulation in academia and the insurance community; and negotiate possible solutions with a surprising new ally, the big corporate employers. A huge semi-secret task force was then assembled to exchange ideas, discard really bad ideas, and work the proposal into legislative form. There would be internal inconsistencies and conflicts but no matter.

|
| William Clinton |
Congress would work it out, differing versions would appear in House and Senate bills, and President Clinton himself would eventually be able to intervene when things got to the House-Senate Conference committee. Since the Clintons really had no pre-conceived ideas on this complicated topic, the will of the people would emerge from a huge debate, and the will of the people would prevail.
That's one version. The other way to picture this circus would be that a highly skilled politician would offer everybody a chance to propose pet projects, and those who failed adversary process would be obligated to support the ones who did prevail. Trade-offs would be made, as needed, and the political ringmaster in the White House would have the final say.
But the final version was the one that came through to the public and the leaders of big business. You weren't going to know what the plan was all about until it was too late to do anything but accept it after a big sales talk full of snake oil. Big business, which had a serious interest in a particular outcome, also had an army of experienced Washington lobbyists. These people were aware of the unpredictable quirks of the house-senate conference system, were completely confident that the membership of that committee would be stacked in favor of a particular outcome, and knew that a congressional staff with agendas different from those of business would, in the end, be perfectly capable of stealing the show. For major employers, that settled it.
Big business had been wavering about whether to go ahead with their own plans, anyway. They had listened politely and carefully to what the government wished for its own insurance plans, Medicare and Medicaid, and were probably willing to agree. But as matters approached a unified approach, too many things surfaced they didn't like, and too much chance the decisions would go against their wishes. There was too much to lose, too little to gain, and well, we're sorry, we can't go along. This or something rather like it seems to have been the final outcome. The press had been furious about exclusion from major news items, coupled with annoyance at the favoritism toward Mr. Weinstein of the New York Times. The whole medical industry was jittery about exclusion from consultation or even notice; the insurance industry was pretty comfortable with the status quo; the public was in a state of utter confusion After the main partner dropped out, the proposal never even came up for a vote in Congress.
Hold the Presses

|
| Stop the Presses |
At USAToday, techniques are astounding. After getting an 800-word piece, an editor by phone will suggest cuts to 300 words; the piece is always improved. Last-minute speed, trying to watch television, is unbelievable. On one occasion, after a medical meeting in Kansas City, watching a baseball game go into extra innings I fell asleep with the game undecided. The next morning a newspaper was pushed under my door. It was USAToday, not only carrying the final score but a full story, under a color photo of the winning play. Just consider the precision Chicago reporting, Washington DC editing, Kansas City printing and local delivery that took place in seven hours. By contrast in book publishing, a full year often intervenes between manuscript submission and actual bookstore sales.
So on a certain Monday night, the editor called. The Senate Majority Leader, George Mitchell, finally was to unveil the Clinton Health Proposal tomorrow morning. Would I please submit an editorial to run in the morning paper; he would supply the title. It was to be called, What Should Congress Do Now? and the deadline was 7 PM tonight. My watch read 5:30 PM.
Well, what fun. After a few minutes of stumbling around, I resolved to build the editorial around the theme, Don't Make Things Worse. It then seemed natural to allude to similar proposals gone famously wrong, define some predictable traps, and end up with Hippocrates. Over and over it is thundered at medical students: Primum non nocere. First do no harm. It all came together in my head, and I sat at the typewriter to bang it out. But when I came to that last sentence, pleading at least do no harm, I was hit by terrible doubt.
That phrase comes to us in Latin, and Hippocrates was a Greek, living at least five hundred years before the Roman Empire. Famous though the saying is, it wasn't (then) in Bartlett's Quotations, or Roget's Thesaurus, or anything else I could lay my hands on in what was, after all, a medical office. It was 6:50 PM. I called a learned friend from his dinner-table, and he agreed it was a strange business, looked at a couple of books, couldn't help, sorry. So, I drew a deep breath, said the Hell with it, typed in, "As Hippocrates said, At Least Do No Harm," and shoved it into the fax machine. The next morning it appeared, next to two million copies of my photo; so at least the editor seemed to like it. Some friends soon called to say that Senators Dole and Moynihan had adopted the line on the noon and six o'clock news, each attributing it to Hippocrates. No matter what happened to the Clinton Health Plan, it looked to me as though I would be forever guilty of supplying the world with a highly quotable misquotation.
Since then, with more time to do a proper search, I'm unfortunately still uncertain. William Safire at the New York Times, was intrigued but could only refer me to a nice lady at the Library of Congress who was a crony. She tried to help but was stumped. Some Hippocrates scholars at the Library of the Philadelphia College of Physicians were able to find a reference in The Epidemics which seems to say what we are looking for, and that reference has tardily crept into Bartlett's latest edition. Some people think Galen really wrote it, which might account for the Latin; but even that is unsatisfying to scholars. Somebody or other took that phrase, whether written by Hippocrates or not and pounded it over and over until it became a medical student incantation. Even if Hippocrates actually did express that sentiment in passing, it doesn't come through as a really important statement, and there isn't much evidence that his students were repeating it over and over as the words of the master.
My present suspicion is that vague rumors about Samuel Hahnemann, the father of Homeopathy having a hand in promoting the slogan during the Nineteenth century, may have some underlying substance. Homeopathy was a belief system which emphasized the prescribing of infinitely minute doses of medicines. It had a flurry in the 19th Century when conventional Medicine was reeling from excesses of bleeding and purging, which surely did a lot of harm to victims of, say, Yellow Fever. The acrimony even spilled over into the emotionalism of the abortion debate, because laws prohibiting abortion had been sponsored by the allopathic American Medical Association. The verbal warfare between doctors of Homeopathy and "Allopathy" was bitter beyond describing. Although conventional medical care finally got its feet on the ground, and homeopathy is now pretty much a historical relic, the homeopaths did have that big strong point. Doing nothing is clearly better than doing something harmful. Nobody takes Latin, much, anymore. So the modern medical way of saying the same thing has come to be, "The hardest thing to do, is to do nothing". This way of stating the same idea is widely believed to have been offered by William Osler, but after all the controversy about Primam non-nocere , I am now reluctant to be too sure about anything in this area.
Be Careful What You Wish For

|
| Pulse |
Events at the time of the introduction of the Clinton Health Plan to Congress were a confused jumble, but one vignette stands out in my memory. The five hundred or so members of the secret work group were all invited to the White House for a big party, with saxophones and all. On a television interview at home in Minnesota, Paul Ellwood said he wasn't going to the party. Indeed, he looked rather morose and had little to say. It is clear he had advance notice, before the plan even reached Congress, that things were not going the way he wanted. Since the public, even Congressional leaders, were still unclear just what was to be proposed, Ellwood's dejection, or rejection did not come from them. No one has said so, but it must be presumed the rejection came from his sponsors, the business leaders. Business, in short, had pulled out; responsibility probably lies with no more than half a dozen CEOs who continue to be anonymous fifteen years later.
At that confusing time, the reasoning of the masterminds was obscure. Perhaps they decided HMOs were no good; perhaps an outrageous political demand had been linked to the proposal; or there was to be too much political control, too little business control; or perhaps government costs had been shifted onto the backs of employers; perhaps the whole idea sounded too leftist to be comfortable. And perhaps a lot of other things, who knows. Even today, no one has written a book or even listed a few plain sentences of reminiscence.
What is known is that major business employers immediately launched a nationwide initiative to go ahead with a strong push to convert employer-based plans from fee-for-service to managed care HMOs. This was to be the way employers handled health care they were paying for; the government could do as it liked. It must be admitted it was a bold stroke, quite effectively handled. When you consider the rather uncertain legal right they had to impose a system of health care on their employees, it took more audacity to go ahead than you would suppose they could summon. It was a gamble that the Clinton White House would lack the courage to challenge a private initiative to go ahead with what they had so publicly endorsed, and that providers would be so surprised by the concerted coup that they would hold back legal challenge until evidence of antitrust or conspiracy emerged. It was a sort of Battle of the Bulge in reverse, and it might well have been hugely successful except for one thing they did not anticipate. Their employees almost universally hated HMOs when they tried them out. No one likes to be hustled into something he doesn't understand, no one likes to change doctors, no one like to be told he can't have what he expects to have. Employers expected resistance of this sort, but it simply had to be done to save the fiscal health of the business. Unfortunately, what emerged was that it didn't save much more money than its own extra cost to administer. The hard reality of business life is you regularly have to bully people in order to make any money. But bullying people without making any money is a quick route to dismissal. No wonder there have been no memoirs written.
A quick re-appraisal of the Clinton Health Plan was that the two systems, Medicare for people over sixty-five and employer-based for people under sixty-five, were to be merged into a single system for efficiency and better control. There were to be local, regional, and national governing bodies; evidently, the purpose of the National Business Coalitions for Health was to supply a unified business hierarchy to match it up and down the line. Hated politicians, hated bureaucrats and hated unions could be counted on to apply strong pressures; business would have to remain well informed, sternly disciplined, and speak with a single voice for any hope of surviving in such an environment. It is my surmise that such a prospect seemed to guarantee failure for a business. No, we're sorry, Business would draw a bright line at age sixty-five, and run its own show where it ruled the roost.
Computerizing Medical Care
Note: This article was written in 1999, long before Computerized Medical Insurance Exchanges were such a disaster:
|
| First Computer |
My first encounter with a computer was in 1958, and I have loved them ever since. As president of what called itself the Delaware Valley Hospital Computing Society, I remember giving a dinner speech concluding as follows: "If you want to be happy for a day, get drunk. If you want to be happy for a week, get married. But if you want to be happy for a lifetime, get a computer!" After fifty years, my affection continues. But to be candid, billions of dollars about to be spent on computers in medical care will mostly be wasted. Even worse, like malpractice suits computers will induce behavioral changes in the system costing far more than the directly visible costs.
That's unpopular news at present since the National Business Coalition for Health has launched a major lobbying campaign to persuade Congress to spend an initial billion dollars inducing physicians to maintain an electronic medical record. Various health insurance companies already provide financial incentives to doctors to file electronic claims forms, eventually threatening to reject any claim submitted on paper. The American College of Physicians has established a rather large department to develop programs for physicians to use in their practices; twenty years ago the University of Indiana started much the same thing. The College of Physicians of Philadelphia has spent close to a million dollars on such a project. It is reported that Microsoft Corp. has a massive project underway to supply electronic medical records. It sounds fairly easy to obtain large research grants from the government to devise something, anything, useful in this area. In my own case, training funds really weren't necessary, since I eagerly got into the field when everybody was a beginner. I was just as good a beginner as any other beginner. But let me repeat: the electronic medical record has been in the past and will be for decades, an expensive digression. In health care, creating more administrative work isn't the solution, it is the problem.
For fifty years the problem with an electronic medical record was that it took too much of the doctor's time to complete his part of the input, and then cost him too much to pay employees to do the rest. Presumably, automatic voice recognition and dictation will soon make it possible to record doctor's notes without handwriting or typing. Since, however, the elimination of current paper forms and check-off boxes will create a major problem in organizing the dictation verbiage, it could add five or ten additional years before programmers manage to rearrange dictation material and effectively integrate it into organized form, complete with laboratory results, dictated x-ray and EKG reports, even small images of the original material. Temperature, blood pressure, weight, photographs and the like can all be readily integrated into the stored electronic record, but to do so usefully is an expensive programming project. Doctors are quite right to be anxious they will lose control of the usefulness of their records in order to ease the task of programmers, speed up the sluggish pace of development, and reduce what will surely be an unexpected cost overrun. Storage and retrieval of such records is known to be an achievable but expensive task, which however also risks sacrificing the speed and ease requirements of the medical task it is supposed to serve -- in the name of cost-effectiveness.
Computers are no longer an unfamiliar tool; physicians have altogether too much experience with "vaporware", unrealized promises of convenience, and the damaging effect on the medical quality of the philosophy of Quick and Dirty. To respond to their resistance to design blunders with an accusation of undue conservatism is to provoke an icy stare and gritted teeth. Inevitably, the effective use of automation will require a redesign of workflow with major disintermediation of "gopher" staff; after all, that is how cost savings are to be achieved. That will provoke outcry that physician time is the most expensive component in the process, but unfortunately, physicians will discover Information Specialists with a business background will brush that argument aside. The most overpaid people on the face of the earth are investment bankers, but information consultants have persuaded business executives that inefficiency of the investment process is more expensive than even an investment banker's time. Having been through this themselves, insurance executives are unlikely to pay the slightest attention to physicians dancing to a familiar old tune.
For all that, data input is not the real problem; it's just the first problem. It's in a class with data storage and retrieval, which is expensive and cumbersome when you add a need for instant access and total privacy. But costs will come down steadily, and eventually, we can expect automated fingerprints or other biological identification, and cheap instant retrieval. Doctors will be able to make rounds in the hospital with a computer in their pocket, record telephone calls in their entirety, dial automatically and whatnot. There are problems with wireless transmission inside buildings with steel girders, and legal requirements for signatures on narcotic orders, but if we are determined, these problems can be overcome as easily as they were with electronic check writing and stock brokerage. Cost may top twenty billion dollars in twenty years, but it all can be done if we insist.
But then you encounter the real problem. Information will accumulate in these records in staggering amounts. Even if you resolutely resist demands to have the nurses record every groan, and the orderlies file every laundry slip, the legitimately important medical information will be exposed as the massive heap of transients that they really are. Plaintiff lawyers will insist no scrap of data may be deleted, hospital administrators will insist on compliance, when in fact most of a doctor's concentrated effort is devoted to brushing aside momentarily distracting data in order to see what's going on and react to it instantly. When a quick look doesn't solve the problem, the doctor goes back for additional data. If you disrupt these skills and traditions of coping with information overload, evolved over centuries, you will at best impose frustrating delays on a complex system under pressure, and ultimately inspire elaborate systems of short-cuts. The Armed Forces are famous for paperwork, but even they know better than to ask a pilot for his Social Security number as he starts a bombing run. The hospital nursing profession has already just about collapsed under paperwork pressure. If you see five nurses in a hospital, three of them will be sitting down writing something. The terrible truth is that no one reads it, no one checks it, and ultimately it sits in the record room waiting for a plaintiff lawyer with unlimited time to sieve out some misrecorded misconception or uninformed conclusion. My faith in the computer is such that I feel sure that methods can be devised to produce periodic summaries, automatic alarm signals, and mostly effective prioritization of data elements. Unfortunately, medical care is changing at such a rapid rate that ad hoc automation of physician thought processes cannot keep up with the current pace of change in medical progress. You would think some things would be unthinkable, but since I can remember the organized campaign to suppress the CAT scan as an unnecessary expense, I confidently predict that programmer inability to keep up with some advance in medical care will at times lead to organized outcry that we should slow down the pace of improving medical care, so that computer clerks can keep up with it. But that is only a small part of the issue, which at its center is that physician time will be dissipated and his attention distracted by presenting him with unwieldy amounts of neatly printed, spell-checked, encrypted and de-encrypted, biometrically secure, hierarchically prioritized -- avalanches of data which are irrelevant to the issues of the moment. The goal is not, after all, an electronic record. The local goal is to decrease the cost of medical care by increasing the productivity of the physician, and the overarching goal is high-quality patient care at a reasonable price. Behind all that, since the impetus comes from NBCOH -- the ones paying the insurance premiums -- suggests that the local goal is not so much the improvement of care as oversight reassurance that cares provided has been as good and as cheap as possible. The goal is legitimate, but this cybernation approach looks to be self-defeating by being overly specific.
If the reader has the patience for it, let me now cite a historical example of the third-party tail wagging the medical dog. In this case, third-party health insurance similarly overextended its reach by imposing internal health system changes, trying to facilitate the role of monitoring it externally. Specifically, the system of diagnostic code numbers was changed from one devised by the medical profession for its purposes, into a different coding system devised outside medial profession sponsorship, which seemed to suit the needs of payment agencies better even though it suited medical purposes less. After twenty-five years, it is now clear that third-party payers have shot themselves in the foot on this matter, and everyone is worse off. The topic, please pardon the obscurity, is the diagnostic coding system.
To go back to beginnings, the American Medical Association perceived a need for a diagnostic coding system in the 1920s. Organizing or even merely indexing vast amounts of information about a disease required more specificity than freestyle verbal nomenclature could provide. Quite a distinguished panel of specialists and consultants then produced the Standard Nomenclature of Diseases (SNODO) which in time became the Standard Nomenclature of Diseases and Operations. In order to reduce ambiguity, this system developed a branching-tree code design for anatomy, linked to a branching-tree for causes of disease, ultimately linkable to a branching tree of procedures. These three sets of three-digit codes linked the components together with hyphens (000-000-000). The first digit of each was the most general, as in Digestive, Musculo-skeletal, etc. and subsequent digits were progressively more specific and detailed, as in "Digestive, large intestine, sigmoid colon". The causes of disease would resemble "Infections, bacterial, streptococcal". An example of Procedures would be "Incision, incision, and drainage, drainage and insertion of the drain". In nine digits, it was thus possible to represent " incision, drainage, and insertion of a drain into a streptococcal infection of the sigmoid colon". After a while, the codes grew from three to five and six digits, again repeated three times, so an immensely detailed, unambiguous description might be coded in fifteen digits by a physician who knew the rules but didn't own a codebook. This code was ultimately taken over by the Academy of Pathology, expanded and is called SNAP. The pathologists absolutely refused to give it up.
The rest of the profession gradually yielded to the pressure of hospital administration, who was pressured by the Association of Medical Record Librarians, responding to the views of outside statistical interests, particularly insurance. A simpler, shorter coding system was needed, they felt, concentrating on the thousand most common diseases. The International Classification of Diseases was produced, reducing the millions of SNODO diagnoses to 999 by heavy use of several varieties of "Miscellaneous" or "Not Otherwise Classifiable (NOC)". Since the goal was to count the incidence of common diseases, the coding system was stripped of any logical tree-branching and became a short list of what was most common, starting with 1 and going to 999. In time, of course, the common-ness of conditions changed, and various complaints from various directions forced the ICD to go to 4 digits, then five. Unanticipated conditions or complications eventually required the patchwork of some alpha "modifiers", and the original short hodge-podge became a long and bewildering hodge-podge. Coding accuracy declined markedly, but ho-hum. The health insurance companies paid the bill, no matter what the code said. At another place, we will discuss the entertaining way that Ross Perot became a billionaire out of the computer chaos of Blue Cross and Medicare at this time, but right now the central theme to follow is DRG, Diagnosis Related Groups. Try to follow, please.
By 1980, Medicare was fifteen years old. It was clear that certain things just had to be changed because the excuse that the system was new and untried was beginning to wear thin. The early designers of the system based their payments on auditing a hospital's yearly costs, auditing the proportion of patients who were Medicare beneficiaries, and paying a proportionate share. That was easy and reasonably accurate, but it had a rather significant flaw that it took no account of whether the patients needed to be in the hospital in the first place. Or whether they needed to stay so long. The response they adopted (in the Budget Reconciliation Act of 1983) is a measure of just how desperate they must have felt. Knowing full well how inaccurate the ICD coding system was in practice, it was all there was. Consultants, particularly at Yale, ran computer simulations of various subsets of ICD codes to find a formula that would produce approximately the same hospital payments as the system of cost reimbursement. If memory serves, the original formula was to divide the thousand ICD codes into 27 diagnosis-related groups (DRG). Eventually, the process was tweaked to seventy or eighty groups. Walter McNerny, then Past President of the American Hospital Association told Congress hospitals could live with this system, and promptly we had a system for paying out hundreds of millions of dollars. It was touted as a highly sophisticated advance in the arcane science of hospital reimbursement, so it must have included a lot of deliberate overpayment. I can remember trying to remonstrate with McNerny, who felt he didn't have time for the discussion. Physicians had very little to do with the DRG portion of the 1983 Medicare Amendments because the AMA had long insisted that physicians and hospitals go their separate ways on reimbursement. Russell Roth, who was president of the AMA at the time, recounted many times the episode in the Oval Office, when it was announced to Lyndon Johnson that Dwight D. Eisenhower"was in the next room waiting for him. LBJ excused himself to leave, and on the way out said to Wilbur Cohen, "Give him anything he wants." Things were destined to change, but at least for a very long time, physician and hospital reimbursements were strictly independent.
Healthcare Reform: Looking Ahead (1)
|
| baby boomers |
By this point, a patient reader of these reminiscences has probably learned quite enough about the Clinton Health Plan and its immediate aftermath. There is, of course, more to say, but except for political junkies, the topic doesn't warrant protracted dissection. It might be worth knowing the motivations of the insurance industry when they launched that bombardment of "Harry and Louise" television advertisements. Opinion within the insurance industry must certainly have been divided, however, and the main decision makers are probably all now retired. The Harry/Louise ad campaign is often given credit for the political assassination of the Clinton Plan, but that seems unlikely. The decisions about medical care were made without heeding the opinions of providers of medical care, so it would not be surprising to learn that decisions about insurance were made without completely candid discussion with insurance professionals.
In fact, grieving too much for the past may have led to looking too little at the future, which clearly contains a whole new set of facts. When the largest generation in history, the baby boomers, start to retire in 2012, those boomers own children will then be at peak earning power but will be a very small generation, too small to support their more numerous parents. Consequently, the 12.5% tax the current teenagers pay for retirement benefits will be too small to pay for their parents' health costs. It will be uncomfortable to increase that 12.5% by much. Thus, the Ponzi scheme we have run for eighty years will then be unable to conceal its facts with talk of trust funds and lock boxes. For nearly a century, Congress has spent the Social Security and Medicare tax surplus for non-medical purposes. They will have to stop doing that in less than ten years. Consequently, we can confidently expect the boomers to protest loudly: they contributed 12.5% of income during their whole working lives to support medical care, and now learn that nothing was saved for their own health care. Even more exasperating is that the second Bush administration did attempt to introduce legislation in 2006 to set aside some current surplus to reduce the impact of the coming crunch -- and Bush was howled down. It would thus appear to be the nature of current politics that this boomer health cost shortfall will not be seriously addressed until the crisis is actually upon us. Democrats will apparently stonewall the matter to avoid blame for designing and ballyhooing a welfare expedient of the 1930s that was swept under the rug during decades of affluence. Republicans will be determined not to be paymasters for a welfare scheme they had opposed from the beginning. So what will happen?
Government only has two options in funding programs where the money has already been spent; they can raise taxes or they can borrow money. By raising taxes, they risk precipitating an economic depression. By borrowing, they flirt with hyper-inflation of the sort that destroyed Germany and Austria in the 1920s. By adopting a little of both remedies, we wander into "stagflation", a term invented in the 1970s to describe a very unpleasant episode. Whatever the description, there seems a very strong likelihood of economic pain and political uproar. It sounds pretty unlikely the public will be in a mood for expensive additions to health insurance coverage.
All this is a preamble to impending cuts in the health budget. We must anticipate the only approach government ever uses for program reduction, the only arrow in the government quiver. It goes like this: first you cut a program budget by, say, ten percent and watch to see if anything bad happens. If nothing bad happens, cut it again. If something bad does happen during a series of cuts, deny that it did happen, and scramble around to patch up the damage. If possible governments restore some of the cuts when they go too far, but in Medicare whose unfunded deficit is in the trillions of dollars, that may not be possible. Try to get re-elected after you pull off one of these capers, and you begin to sense how dictators get into office. It really isn't comfortable to talk apocalypse this way, and one would certainly hope there is some flaw in the prediction. There could be other unexpected events in the meantime, deus ex machina, but a stock market crash, a thermonuclear war, or violent changes in the environmental temperature are all going to weaken the world economy, not make things better. This doomsday scenario seems almost certain to include some serious cost-cutting in the health financing system. Therefore, it is only common sense to examine what advance changes might be made in the health delivery system to minimize the damage to it.
My proposal amounts to suggesting that we put the doctors in charge of the cost-cutting. In accident rooms, battlefield medical stations, and even television war serials, the person in charge of sorting out the influx of unexpected casualties is said to be in triage. In triage there is one basic rule: put your best man in triage. If the security guard, the admissions clerk, or the night watchman directs the emergency down the wrong corridor, the ensuing blunders will cascade as the system struggles to get things back on track. We can expect objections to what I have to propose which will take the form of warnings about letting foxes watch the henhouse, but in general, the public already supposes the non-physicians will step aside for the doctors in an emergency. So the more open the discussion about command and control, the better, with ultimate faith that the public will support the common-sense approach of putting your best-trained person in charge.
For present purposes, the general proposal is that when drastic cuts in budget get imposed, it should be the physicians of the local community, not the administrators or the insurance executives or the local business leaders -- who should make the painful choices between what is essential and what can be sacrificed. This is most readily achieved by setting aside the Maricopa decision and clarifying the HMO enabling acts to the effect that it is not an antitrust violation for physicians professionally practicing in nominal competition to participate in the shared governance of health maintenance organizations. In other words, that HMOs such as the Maricopa Foundation need not fear antitrust action, using the experience of a dozen other Foundations for Medical Care as proof of the harmlessness of the approach. It should not be necessary for these organizations to prove positive value, only to demonstrate lack of harmfulness. If they can be established and allowed to compete with insurance-dominated or employer-dominated HMOs, their worth can be established by success in the marketplace. Ultimately, the choice of governance form will thus be made by the patients, and the proposal should be a popular one.
It should also be popular with hospital administrators. They chafed at physician control thirty years ago, but that was before they encountered the far more brutal price negotiations of HMOs dominated by business and insurance. The consequent costly and disruptive wave of hospital mergers is defended by very few, although it would be interesting to examine dispassionate analysis. Probably no one adequately appreciated the threat that employer domination of these practice groups represented to hospital administrations. When hospitals confronted employer groups in serious hard price negotiations, hospitals came to the shocking realization that these people actually had the power to move large groups of people to a competitive hospital, and they certainly talked as though they were capable of doing it. The resulting panic of hospital mergers, consolidation into chains, and the emergence of for-profit competition by hospitals that had no thought of a charitable mission, has created a degree of cost and disorder that was not in the original plan. Hospitals in rural California who told their colleagues of the burdensome power of their staff doctors under doctor-run Foundations would now have to admit that a return to that environment would be a distinct relief.
And there might even be a reconsideration by business leaders. What physicians would bring to the table, what is now new and different, is the undeniable experience that dominating captive HMOs has not proved as useful to employers as they hoped it would be. The cost savings have been disappointing, the exploitation by insurance intermediaries, and the undeniable employee restlessness was not exactly anticipated. Running employee health projects is a large distracting time waster for C.E.O.s who have other goals and mandates to pursue. If employers keep a focus on their reason for involvement in employee health, hardly any of them could defend a posture of resisting the emergence of new choices which make a reasonable claim to reducing employee contentiousness, at a competitively lower cost.
And the government? Among the various unpleasant alternatives that Congress must consider, is the possibility to be discussed next that employers may want to pull out of employee health care entirely. Allowing competitive forms of ownership of existing arrangements might not seem too risky a step, compared with that prospect.
Healthcare Reform: Looking Ahead (2)

|
| health care |
The Industrial Revolution crowded people together into smoky, draughty unhealthy places to live and work, and thus created ideal conditions for the spread of smallpox, tuberculosis, plague, poliomyelitis and many other infectious diseases. With better sanitation and hygiene, those diseases declined steadily for two centuries. Meanwhile, medical science developed a steady stream of expensive enhancements to health like removing an inflamed appendix, inserting pins into broken bones, utilizing CAT scans and artificial kidneys. These things each made life more comfortable and extended it a little longer, but steadily increased the cost of care. Here and there major leaps forward occurred, like the discovery of antibiotics and the prevention of arteriosclerosis, but it seldom seemed that medical care was stamping out disease, it was just making it more complicated and expensive. But if you stopping plodding forward for a moment and looked backward, the aggregate progress was astounding. Dozens of diseases either disappeared entirely or are well on the way to disappearing, like polio, smallpox, tuberculosis, syphilis, rheumatic fever, and what have you. Life expectancy for Americans at birth, which had been 47 years in 1900, was approaching 80 years in 2000. When I started as an attending physician in 1955, I was in charge of a 40-bed ward continuously full of diabetic amputees; during the last fifteen years of my practice, however, I did not attend a single diabetic amputation. At some point in this amazing medical pilgrimage I can remember realizing that for really important purposes, there were only two diseases left. Arteriosclerosis and cancer; and now arteriosclerosis mortality has declined fifty percent in ten years.
So now it is possible to have the luxury of asking: what will happen when we finally cure cancer? Oh sure, there is Alzheimers Disease, HIV/AIDS, schizophrenia and childbirth, plus an apparently endless variety of ways to produce self-inflicted conditions. Everyone will eventually die of something, so doctors will keep busy. It is not necessary to predict the end of medical care to see that some important social transformations are likely. For example, if we cure cancer around the time of financial chaos caused by the retirement of baby boomers, it is going to be hard to resist the demand that we reduce spending on medical research. Every tedious word of the impending debate on the topic could be written right now to save time because it is a very strong probability that spending on medical research will decline, once an effective cure for cancer is behind us.
Let's, however, continue our march into the future of healthcare reform. When employers became self-insured for employee health costs, they came into possession of data about what they were buying. It didn't look adequate to them to explain the sums of money they were spending, so they concluded they were being hoodwinked by hospital cost shifting, with consequences summed up as the Clinton Health Plan. Now put yourself in their shoes when the Wall Street Journal tells you cancer has been conquered. Michael De Bakey once pressured Lyndon Johnson to start a crusade against Heart Disease, Stroke, and Cancer, and now even cancer is gone. A significant number of C.E.O.s are likely at that point to decide that since Far Eastern competitors don't have this cost to contend with, perhaps it is time to declare that you have been fleeced long enough. Give the employees some money, and tell them to buy their own health insurance.
There are even some more legitimate arguments for doing so. Individually owned and selected health insurance would be portable, putting an end to "job lock", the fear of changing jobs for fear of losing health coverage in the process. Employee divorces create a different twist to job lock, and inequities jump out at you from the tangle of arguments about dual coverage for working couples. Add same-sex marriages to this issue and employers are driven to despair. Individual policies would simplify all of these issues, and open the door to life-long coverages, which we will discuss in a later section.
If medical progress makes just the right progress in the impending time interval before doomsday, it is even possible to start talking about eliminating health insurance in a practical way. If there is no threat of medical expense, why buy insurance against it? Since everybody will die of something, it is hard to envision a time without insurance. But maybe Medicare is enough. Senator Edward Kennedy (D, Massachusetts) will finally have his universal single-payer system -- by default.
What we have here are the daydreams of a corporate C.E.O., struggling to make his numbers for the next quarter, and they are pretty strong stuff. But who can doubt the power of these concepts to move the system away from an employer-based formulation?
Healthcare Reform: Looking Ahead (3)
|
For fifty years, turmoil in the health insurance industry has originated in the steel and auto industries. It seems strange that no heroes have come to general public attention, although there may be heroes who are known to insiders; somebody may yet write a book about it. This may be of only passing importance, but the present distress in the American Big Three automakers suggests that unexpected legislative proposals concerning health financing could emerge from that direction. The turmoil in Detroit once centered on the auto industry enjoying windfall profits which labor wanted to share. More recent discord comes from the opposite direction: the automakers now cannot afford to honor those contracts they signed with labor having to do with health benefits.
The contract for the United Auto Workers was certainly generous. Printed up in a little red book for wide distribution, the contract states emphatically that an employee for six months or more will be completely covered for medical expenses for the rest of his life. If Medicare pays some of the cost, that is fine, but if Medicare reduces its benefits, the employer is liable. Some features of this contract may have been changed since it was printed, but it is difficult to imagine what incentives the UAW would have to agree to modifications. Except, of course, the self-interest which emerges when it looks as though the employer might go out of business unless there is some form of relief from wage costs.
To judge what is going to come of this is to judge the likelihood of the various arguments, predictions, and recriminations that are so common in heated disputes. Two things are pretty clear to auto industry outsiders: the UAW contract provides more generous health benefits than almost any other employee group enjoys, while the auto industry has worse earnings than many or most other industries. Consequently, both the employees and the stockholders have an incentive to make adjustments in the auto industry, a situation shared by the steel industry and other major auto suppliers. The form this has seemed to take is to favor some form of national health insurance, in which the taxpayers would take over the obligations of the auto manufacturers. So, look out for proposals from Senators and Congressmen from Michigan, and watch which nominees for U.S. President are favored by the rust-belt political delegations.
Workers in other industries are not certain to go along with such proposals. After all, most people resent it when someone else makes out better than everyone else for decades, and then comes asking for a hand-out.
Segmented Health Insurance
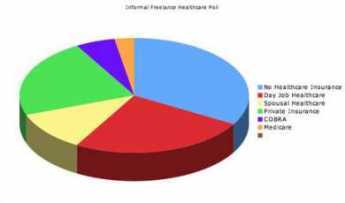
|
| Pie Graph |
Everybody knows the old insurance saw, that the big print gives but the small print takes away. If health insurance pays for one sort of thing but not another, there is anxiety that a bewildered patient can be deprived of coverage he thinks he paid for. A patient knows he was sick, that he saw a doctor, or that he went to a hospital; beyond that, it's better not to leave room for arguments. To a certain degree, this is what has made HMOs seem so threatening; complicated assurances can lead to disappointing loopholes. So, for a century it has almost been an article of religious faith that health insurance should cover everything that costs money when you are sick. However, that headlong faith is exactly why the matter needs to be subject to critical review. Not only does monolithic insurance conceal a vast system of cross-subsidies. It has existed for too long when everything else in Medicine has changed for the original premise to be immune to change.
There are health insurance considerations which go beyond mere convenience of administration. Transparency and flexibility, for instance, suffer when everything is under a single blanket. Women pay a share of prostate surgeries they will never have themselves, people who hate abortions have to pay a share of them anyway. The ability to buy what you think you need is taken away, so some people who could afford what they need are unable to afford the whole package because it includes what they feel they would never need. And then there is moral hazard. Some people reach for what they don't need just because it costs nothing extra. Well, this isn't 1930; we don't need to debate the whole issue top to bottom. But there may nevertheless be a few features of global health insurance which could be advantageously teased out separately.
For a first example, look at terminal care. Everybody is going to die, and mostly the cost is picked up by Medicare because most people who die are elderly. Some insight into the issue and a reasonably workable definition of terminal care is provided by the statistic that a third of the expenditures of Medicare is paid for someone in the last year of life. Statistics on the average age at death are known with great precision, so it would be easy to calculate the yearly premium cost at any age or the size of a single-premium policy needed at any age to cover the average cost of the last-year-of-life. If we are ever to fund the unfunded Medicare program, this is the place to start. And if you are wondering how you know in advance when you are going to die, you don't need to know. Just establish an independent "endowment" fund, which reimburses the current Medicare program for any expense incurred during what proves in retrospect to have been the last year. Presumably, the cost of running the unfunded portion of Medicare would then drop by a third, while the cost of the funded third would be diminished by the investment strategy of its manager. The relatively few people who die without Medicare eligibility might be treated in the same way, reimbursing whoever paid the costs, but the risk calculation would be more difficult, and a life insurance policy might be preferable. Once the younger individual with such a designated life insurance policy attained Medicare eligibility, some sort of coordination would be desirable.
Everyone dies once, and no one escapes death. But terminal care benefits are not so terribly different from some other health issues. Nowadays, just about everybody can expect to have two cataract operations, and most people can expect a hernia repair, a gallbladder removal, and if male a prostate removal. Everybody ought to have a pneumonia immunization, and a colonoscopy, by age 66. It would be easy to compile lifetime risks and update them yearly, for the typical male with 1 death, 1 pneumonia vaccination, one colonoscopy, 0.76 prostatectomies, 0.59 cholecystectomies, 0.37 hernia repairs and so on. The cost of this sort of routine care is not really insurance, it is pre-payment. It is not subject to abuse, and need not be challenged or reviewed unless statistical monitoring shows that the incidence of some component was rising in a particular zip code area. In that case, what would be called for would not claim review, it would be provider review.
Perhaps the reader can see where this is going. Having stripped out routine pre-payment as much as is practical, you are left with the unknowable "all other". Insurance which covers this sort of risk becomes true insurance, in an umbrella form. As medical care continues to advance, more things can be moved from "all other" to "routine". Ultimately, and probably sooner than most people would guess, you can achieve a true insurance system, defined as having a trivial insurance premium for a remote risk. From that point forward, you can direct your cost-cutting attention to reducing the cost of routine care. That would include the devising of strategies to pay for luxury versions of routine care, as desired.
Making Money (8): Virtual Money
 When money was tangible you had to guard it, now that it's mostly virtual you have to verify it. Hardly anybody can, and that's a problem. 
|
When money and wealth were wampums, precious metals, and paper currency, these physical objects required physical protection. It was all a big nuisance, with six-guns on the belt, bank vaults, and appraisers of one sort or another. But now that wealth is merely a bookkeeping entry on someone's computer, things may be even more nuisance because verification is almost beyond us. Counterfeiting of the computer variety must be left to institutions to detect or deflect, causing them to introduce firewalls of various sorts that also block legitimate inspection by customers. "Trust but verify" doesn't work so well in this environment. Let's use a personal example, slightly fictionalized to protect the innocent.
Several software products now exist to download transaction information automatically from various institutional sources to a customer's home computer; they are either free or cost a nominal amount, and are quite "user-friendly". In my case, however, the reports they generated were quite significantly at variance from the monthly reports which were issued directly by my counterparties. Dear Sirs, Please explain.
What I soon discovered was that everyone blamed someone else, and everyone blamed me for bothering them. Quite obviously, I had little understanding of these specialized accounting niceties, and quite obviously I had too much spare time on my hands. Telephone help desks, often located in India, will not give out telephone numbers for incoming calls and are programmed to check the size of your account before placing you in a call-back queue. The first call is usually taken by a trainee whose job it is to screen out the silliest sort of help request, and then to refer to a supervisor if things rise in complexity. Supervisors have supervisors. That's if you are lucky. More commonly, the tedious software business has been farmed out to a vendor, and the contracting agency has neither the necessary understanding of the issue nor any ability to fix it. From the sound of it, the vendor often gives the contracting agency the same sort of isolation treatment that they would give a customer if he could find their telephone number. And guess what. At the end of the day, one of those high-handed defensive linemen -- turns out to have been at fault.
Let's explain one problem. On the surface, we were talking about a $40,000 difference in account balances; one may have been correct, but a second one must have been wrong. That rises to lawsuit level, so the matter got intensive study. It turns out the stockbroker had misinterpreted instructions for a "sweep-account" system. When a stock in your portfolio pays a dividend, the amount of the dividend is subtracted from that stock's line item and added to the line item of your money-market fund. That's fine, but there is one exception. When the money market fund itself pays a dividend, subtracting that dividend cancels out the addition, and the dividend essentially disappears from your net worth. Was this intentional? Certainly not; no one could stay in business doing that. It's not even a highly stupid error, since you can easily see yourself making the same oversight of the one implicit exception to the rule of sweep accounting. Because of this "bug" in the program involved one institution making a mistake and transmitting it to a second institution, the systematic error did not unbalance any books, until it reached mine. But since I did not detect the error for five months, there must be dozens, hundreds, maybe thousands of customers who did not detect it. Ouch. Do the math yourself to judge whether this was a serious error.
This illustration, only one of several on my personal report, leads to at least two larger principles. The first is that the transformation of money from tangible to virtual has occurred so rapidly that bullet-proof safeguards have not had time to emerge. After a century of use, most people cannot balance their checkbooks, but enough people can balance them so that systematic errors are not likely to slip past. When enough people with home computers repeatedly test the internal complexities of their virtual money accounts, confidence will develop that the system is probably working. Confidence is an important matter; it is possible to imagine quite a bank panic if the public suddenly got the idea that virtual money is maybe a mere vapor. In fact, the securitized credit panic of 2007 is a little like that. With a few new regulations and a lot of computer programming it surely will be possible to know who owns how many bum mortgages. That innovative mortgage system got ahead of its tracking verification, and we now just have to hope nothing serious happens before that gets fixed.
The second important lesson is that our health insurance system has a similar problem of far greater size and complexity. We are here talking about at least ten percent of Gross Domestic Product, in which one daily unit of measurement is in truckloads of insurance claims forms. Stocks and bonds are admittedly complicated but compared with thousands of different diagnoses, drugs, procedures, and hospitals -- verifying financial transactions is trivial compared with measuring medical ones. With a twenty billion dollar budget and ten years of lead time, we might have a shot at it. Except for the fact that during the ten-year interval, medical care will have changed so much, you will have to start over on the project.
Exit, Pursued by a Bear
|
| John Kastor |
Everybody ends up getting fired in a recent book by John Kastor about recent events at the University of Pennsylvania just like everybody ending up dead in an Elizabethan play. The vital difference, of course, is that the dramatis personae at Penn can still relate to a bewildered audience their own versions of those grand events. To protect himself, the author peppers his book with more footnotes than a Ph.D. thesis. And thousands of stakeholders at the University can now realize that during those eventful times they were as clueless as Rosencranz and Guildenstern.
One basic fact about that institution is that the medical school spends three-quarters of the entire university budget. That leads to grudges in the little law school, the little engineering school, and the little president's office, as they knuckle under to the Golden Rule. The department chairman with the gold makes the rules. Since most of that gold comes from research grants, hence ultimately from the federal government, the medical students and the teaching faculty don't have the same power they had during the Vietnam War era, either. Although medical school tuition imposes a crushing burden on the students and their families, leading to debts close to a quarter of a million dollars apiece, the tuition money doesn't amount to much in the university scheme of things, either. In some schools, tuition amounts to two percent of the medical school budget. You could eliminate the students entirely and not see much difference in the "school".
Unfortunately, when you become dependent on government grants, you find they can suddenly be terminated, or awarded without funding, or held up for several months by Congressional bickering. Meanwhile, there are salaries to pay, contracts to fulfill. Even if you can furlough some of the staff, it's not easy to see what you do about a thirty-year mortgage on a research building when there is a lull in its research funding. If you try to save money, the granting agency will try to get it back; they aren't authorized to make grants to be squirreled away. If you shift money to unauthorized uses, you risk going to jail. And yet, if you don't do something along those lines, the whole enterprise can collapse.
Having said that much to be fair, it is still uncomfortable to see the financial transparency of our most valued nonprofit institutions vanish behind a Byzantine fog of secrecy, out of which arise the magnificent towers of new buildings, and in front of which an occasional limousine is to be observed. No wonder the research scientists feel the constant pressure to produce. A Nobel Prize every ten years, or so, would go a long way toward quieting envious remarks from the liberal arts faculty.
Housed in those ivy towers are three institutions, the teaching hospital, the medical school, and the university, with three boards of trustees, and at least three ruling potentates. At irregular intervals, congressional committees do things to the Budget Reconciliation Act which enrich one of the three components of the institution or suddenly impoverish another, or both. Integration of the three under one governance sounds plausible until you notice how radically different is the mission of each one. You can take a big building away from one component and rent it back to them, and things like that, but you can't do it without starting whispers about Enron. You can gather up surplus funds from one of them during the decade of the eighties, but you have trouble giving it back twenty years later. Officials at Blue Cross come snooping to see if health insurance premiums are passing through this shell game, ultimately paying salaries in the department of English Literature. Everybody distrusts everybody else, somebody sasses somebody, and everybody gets fired.
Nothing unusual about that. It happens at every medical school.
South Amboy Explodes

|
| Explosion |
South Amboy, New Jersey, is a waterfront industrial town on a remote promontory behind Staten Island, jutting into lower New York Bay. It's across the Raritan River from historically important Perth Amboy, but it's fair to say that few people ever heard of South Amboy until sunset on May 18, 1950, when they suddenly heard a lot. An entire freight train, five lighters, and a railroad pier suddenly exploded and disappeared. About twenty-five people were never seen again; the largest piece of metal from the explosion was only about a foot in length. A significant part of the town was leveled, steeples were knocked off churches, and windows were broken in five surrounding counties. Considering what caused it, it seems remarkable that so few people were killed. The explanation usually given is that the explosion blew straight up and straight down; the distant windows were smashed by pressure implosion.
When Pakistan split off from the rest of India, there were bloody migrations in which millions of people died. So Pakistan bought the rights to the design of certain land mines to protect its new borders and contracted with a firm in Newark, Ohio to manufacture the mines. Two trainloads of these explosives were shipped from Ohio to a railroad pier owned by the Pennsylvania Railroad in South Amboy, to be lightered out to a waiting cargo ship and sent to Pakistan. The first of these two shiploads sailed off uneventfully, and on May 1, 1950, the second shipment had already left Ohio and was underway, when the Coast Guard suddenly declared the South Amboy pier to be closed and forbidden. As the train chugged slowly eastward, frenzied negotiations took place with Admirals in Washington. There was plenty of time, because the train moved very, very slowly and it was detoured over six different railroads to Wilmington Delaware, where the Hercules Powder Company had packed two freight cars with dynamite, which were to be hooked onto the end of the train as it inched its convoluted way to South Amboy.

|
| South Amboy Explodes |
The method of packing the land mines was of some importance during the huge litigation which inevitably followed. Land mines were packed in cardboard boxes about six feet long, divided into six compartments. Our own Army regulations about such things state that never, never should fuse be packed in the same carton with the mines. However, this particular shipment had five mines to a carton, with the fuses in the sixth. It was later argued that this particular arrangement proved harmless in the first of the two Pakistan shipments, but there was the testimony that defective fuses were removed from those boxes and passed back up the line, where those deemed satisfactory were re-packed in the cartons which were in this, the second shipment. A fuse, by the way, does not quite describe these objects, which were screwed into a hole provided on the bomb part. They contained a spring and a steel ball in a tube; when the gadget was cocked it was held by a hare-trigger. The idea was that the pressure of stepping on the mine shot the steel ball into the ball of explosives, and boom.
The railroad ammunition pier, for some reason called The Artificial Island, consisted of two rail lines extending a quarter mile from land, but no structures. Stevedores transferred the boxes from the train to the lighters, and then five lighters took the partial shipments out to the anchorage where the ocean freighter was waiting. The deck of the lighters was lower than the train tracks, so a wooden ramp was laid from the freight car to the lighter, resting on several mattresses on deck. It all worked on the first shipment, didn't it?
Well, it didn't work this time, and we have no way of knowing who stumbled or dropped something; we only know it all went sky-high. For this, the ship-owners were delighted because it is a well-established principle of Admiralty law that unless the ship was in contact with the owners, their liability is limited to the value of the damaged vessel. Under conditions of total disintegration, that means the lighters had a liability of zero. But there were six railroads, the Pakistani government, the Coast Guard and the two manufacturers of the explosives available to sue. Everybody had insurance, so a dozen insurance companies were involved. All of the victims and hundreds of people with property damage, all had lawyers; everyone agrees that many lasting friendships were established among lawyers who were milling around. Finally, the judge declared this case just had to be settled, or else it would continue for the rest of everybody's lifetime. The total amount of the claims submitted came to $55 million. Obviously, the settlement would be for less than that, but settlements are kept secret and you are not supposed to know how it turned out.
So, the question that remained was this. If everybody was insured, why not let the insurance companies haggle about who owed what to whom. Why did all of those railroads have lawyers hanging around? Well, the answer is a lesson for all of us. You need a lawyer to watch your insurance company's lawyer, because once a claim action begins, you and your insurance company develop a conflict of interest.
www.Philadelphia-Reflections.com/blog/1482.htm
Veterans Hospital

|
| Philadelphia VA Medical Center Home |
At a recent meeting of the Right Angle Club, Stephen C. Bennett an administrator, and Alix Esposito a social worker, kindly addressed the club about the Veterans Hospital where they work. The federal government pushes its mass produced products into every city, but gradually a local flavor starts to creep in; how this process works is illustrated by the fact that Steve's grandfather Claude was once the manager of the Bellevue Stratford Hotel. The VA hospital may be a piece of Washington D.C. planted on Philadelphia soil, but Philadelphia will surely absorb it with the passage of enough time. The VA was once a part of the Veterans Administration, but now it is a part of Department of Veterans Affairs, run by a Cabinet Secretary, no less. It's the second largest department of the federal government, and since the only bigger department is the Department of Defense, the combination of the two shows you how far we have come from the nation's original opposition to "standing armies". The fact that these two components of our war machine are separate, on the other hand, surely symbolizes some hidden tensions between our regular armed forces and the American Legion, or the hidden frictions between two congressional committees, or else some other mystery of bureaucratic politics.
The Veterans Administration was founded in 1930, the Philadelphia VA Hospital was built in 1950. Originally, it was designated as a Deans Hospital, signifying the intention to confer prestige and lessen friction with the medical schools. Originally, Philadelphia's VA was affiliated with several medical schools, but in time its proximity to the University of Pennsylvania led to the elimination of ties with other schools. Although the bed capacity is growing in reaction to America's successive wars, its open wards converted after 1960 to more semi-private style, and its focus of medical activity shifting with changes in medical science, the VA remains isolated from the rest of the city and the rest of Philadelphia medicine. Part of this is physical; the hospital is confined by the University of Pennsylvania, the parking complex next to the Amtrak line, and the Woodland Cemetery, so there is little room to grow. And comparatively little commonality with the neighbors. There are 2000 employees and a $30 million budget, marooned in a sea of automobile traffic going elsewhere in a big hurry, too big to ignore but too small to influence the local culture.

|
| Vietnam War |
The patients are distinctly different from those you find in other hospitals. There is a great deal of chronic mental disorder a heavy influence of alcohol and substance abuse and rehabilitation, and even some residential apartments for patients. On a national level, between a third and a half of homeless people are veterans, but for some reason in Philadelphia, only a tenth of the homeless are veterans. During the Vietnam War, the system of draft avoidance through educational exemptions resulted in that generation of veterans coming from an unusual concentration of low income and low educational subgroups. The system of government pensions and promotions tend to retain employees in the system for a lifetime. It's true that informal transfer arrangements allow a certain amount of migration to Florida (in the winter), or Maine (in the summer), or California (to see what LaLa land is all about), but those who do this stay within the VA system. Consequently, the interchange of ideas and techniques that professionals carry with them between hospitals is curtailed, confined somewhat to variations within the VA system, conforming to its social norms. An archipelago, although not exactly a gulag archipelago.

|
| Veteran |
But by far the greatest source of distinctiveness in the VA hospitals comes from the byzantine eligibility standards for the patients. The reimbursement systems of Medicare, private insurance -- which more or less copy each other -- changed around 1988 in a way that more or less eliminated psychiatric inpatient care in the community, especially if it lasts more than a month. The VA, on the other hand, was forced by circumstances to increase its attention to this area. Consequently, all social workers everywhere inquire immediately whether an addict or a schizophrenic might be a veteran. A differential sorting process quickly gets underway, with the VA as the preferred place to send such patients if at all possible. Non-veteran victims of the same conditions tend to have a worsened time of it, because the pressure on state and local governments to make some provision, has been relieved.

|
| Walter Reed Hospital |
At the other extreme, the social elite of the armed forces are not admitted, either. President Eisenhower was unquestionably a veteran, but he had his famous hospitalizations at >Walter Reed Hospital. There's an income limit for VA admission, which automatically cuts off 20-year veterans above a certain rank, possibly major. And there are overlapping disability classifications for military hospitals and veterans facilities, with considerable latitude available to uniformed boards of three serving officers, only one of whom is a physician. The result is a general perception that if you have any influence at all, you can generally avoid the VA and be treated in a military hospital, probably in a VIP unit. Good for them; I'd take advantage of it if I had a chance, too. But by siphoning off the top brass, a lot of pressure to improve quality is removed as well. If a VA hospital had eight or ten Admirals and Generals as patients, with academy classmates coming to visit, it's safe to assume that courtesy, orderliness, and cleanliness would instantly improve. And take it from me, the quality of care would improve, as well.
Madeira Party 2009

|
| Madeira Wine class= |
The hundred years war, the thirty years war, the seven years war, and other European disagreements made it difficult to import wine to England, turning the wine import trade to Portugal. Port wine was, of course, prominent, but the best wine of all came from the Portuguese colony of Madeira. The island of Madeira is closer to Africa than to Portugal, so the triangular slave trade made it easy to import Madeira wine to the British colonies in America. The eastern seaboard of America had no grape culture of any note, so the beverage trade centered on rum, whiskey, beer, and Madeira. George Washington is widely reported to have had half a bottle of Madeira every day for lunch, for example.
|
| S. Weir Mitchell. Mitchell |
The other evening at the Franklin Inn Club, a traditional Philadelphia Madeira party filled the hall, and the membership was brought up to date on some of the traditions and finer points of the occasion. In the first place, the Franklin Inn was founded by S. Weir Mitchell. Mitchell, in his spare time as Father of Neurology, had written a short story called The Madeira Party which worked in a large number of details about what was what about Madeira, ending with ribald tipsiness. Nathan Steven, a well-known wine authority, instructed the group in the various types of grape and vintage, and other members who have summered in Madeira related current conditions. Because the volcanic island is a favorite place for visitors, particularly Englishmen, real estate is at such a premium that most vineyards have only one or two acres of grapes. The wineries whose names are on the bottles pick up the crop from these local growers and take it on from there. This seems as good as any other explanation for the current high prices of the wine. However, a century ago a disease wiped out the French and Portuguese vineyards, who were forced to beg back some exported grapevines from California to get back in business. So, one wonders about the scarcity claim.

|
| Madeira in a barrels |
It is related that a number of cargoes of Madeira, particularly those of John Hancock of Boston were caught being smuggled to the colonies, and got returned. It was discovered that the taste of the wine was greatly improved by the tumult so that each vintner experimented with various methods of agitating and heating the wine to produce a particular brand. Madeira, like sherry, is a fortified wine, with various proportions of grain alcohol and brandy added in secret formulas. On one point there is general agreement, that if fortified wines are aged for long enough periods, eventually they all taste alike. There thus has emerged a tricky business of aging the wine long enough for the vintage of the wine to match the age or anniversary of the person being honored by the gift. Fifty years is the tricky goal; it's the most popular gift, but perilously close to the point where you can't tell if it is sherry or Madeira. There are four main varieties of Madeira (brand names are something else), getting progressively sweeter, darker colored and more expensive as they age. Malmsey, in a barrel of which Shakspere portrayed the royal princes being drowned, is claimed to be the very best. Some people regard it as too sweet, however. At proper Madeira party, each variety is served with a different course of terrapin or whatever. The President of the Franklin Inn read off the instructions for cooking the traditional first course of jellied boiled boar's head, and the guests agreed that modern tastes called for a substitute. After the reading of Mitchell's short story, the group added a new tradition of singing Flanders and Swann's ribald song, "Have Some Madeira, m'dear".
Chuck Barber, the current President of the Green Tree Insurance Company, added an entirely new historical slant. The Insurance Company is well known for having the best dinner in town at its meetings since directors of insurance companies don't do much. At the dinner in 1799, the news was brought in that George Washington had just died. A member rose to propose what has become an annual toast in Madeira, "To President Washington!" In time, S. Weir Mitchell became a member of the board, and the famous short story was the outcome which firmly fixed the rules of the Philadelphia Madeira Party. Bill Madeira was called on to verify this history, but he protested that his family name was derived from the wine, not the other way around.
It seems appropriate to add another historical note. Benjamin Franklin, after whom the club is named, suffered severely from gout. Although some sort of association with liquor had been mentioned as far back as Hippocrates, Franklin's powers of observation and his fame as a scientist placed him in a position to make it an irrefutable doctrine that gout was a medical penalty for drinking liquor. It was, of course, Madeira that old Ben was drinking, and it was the rule that Madeira was transported in lead-lined kegs. The Green Tree has some of the old kegs if you doubt it. Franklin's observation was acute, but what he was reporting was the effect of the lead poisoning, not of the wine.
Reforming Health Reform, New Jersey Style
 |
| Congressman Robert Andrews |
A single e-mail to constituents, and no other communication visible to the general public, announced a town hall meeting with our Congressman, Bob Andrews, on the campus of Rowan University, from 6 to 8 PM, August 24, 2009. The subject was to be Health Care Reform Legislation. On arrival, it was hard to find the auditorium in the square mile of new college campus, and only a small sign entitled "Event" indicated the place to park. Lots of cars.
By counting seats in a row and multiplying by the number of rows, the University Auditorium held 3000 people, but at 6 PM it was difficult to find a vacant seat. The doors were almost blocked by two lines of people standing to speak at microphones in the center of the hall, snaking all the way out past the television cameras and then out the door. These people were strangely silent, preoccupied but not rude, apparently rehearsing their speeches. In the lobby outside the doors, several workers were distributing posters showing "Thank You!", checking people off on lists of some sort. Many of those who got posters were wearing red T-shirts emblazoned with something or other.
 |
| Rowan University |
When I finally got a seat inside, it was behind a whole row of such T-shirted poster-holders, mostly but not entirely of the black race. The Congressman was giving a little speech to the effect that he was one of the committee members who wrote the bill, so of course, he had to support it. Strange, that as a member of Commerce and Labor he was working on a bill which traditionally is the province of the Subcommittee on Health, of the Ways and Means Committee. In any event, that gave him the ability to explain some of the languages which were a little too hard to understand. Several in the audience shouted out something unintelligible at that point, but mostly the audience sat in silence, waiting for the questions. He soon opened it up for questions, because he wanted to know what his constituents were thinking.
Although a few inevitably wandered off the point, questioners were confident, moderately deferential, remarkably effective. No matter how it was stated, and no matter how it began ("I have always voted for you, Congressman"), they were at the microphone to run a sword into him. To some extent, posting the entire bill on the Internet had changed politics. One old man, reading from his papers, said that page 343 says, etc; to which the harassed Congressmen blurted out, "That isn't true!" But the old man held his ground, "Oh, yes, and what else isn't true, that's written in the bill?"
Our congressman represents a working-class district, as clearly illustrated by his previously running for Congress without opposition. In searching for the reason this solidly Democrat audience was so antagonized, one gathers they generally have Unionized health benefits and feel threatened that ensuring the "illegals" will be paid for by impairing their own insurance. Somehow they feel that anyone who denies it is lying to them. ("It isn't what's in the bill, it's what will be in the bill ten years from now.") Except for college professors, Union members have the most luxurious health insurance coverage in America and are accustomed to boasting of it. Somehow, this privileged position drowns out their envy of rich people. When told that only the top x% of the country would have its taxes raised, one man bore right in on the Congressman. "You never heard anyone asking a poor man to give him a job". (Yeah, right, right on, Yeah.)
Although the people in red shirts holding posters put up a fight for fifteen minutes or so, they soon subsided out of recognition of who "owned" the room, and the remaining three hours of "questions" were almost uniformly negative. After an hour, the television cameras left the room, and at that signal, the people in front of me wearing red shirts also left. After a succession of speakers praised physicians somewhat excessively, a couple of physicians got up and made a poor showing at the microphone. One of them, a fat woman, had the poor judgment to tell these folks that many diseases like diabetes were self-inflicted, but was to hear back that it would help if our President would himself stop smoking and leave the rest of us to mind our own business. Two women who proclaimed themselves single mothers were no better treated..
At 9:30, a meeting scheduled to end at 8 PM still had a thousand people in the audience, and fifty at the microphones. But I had enough. They made their point. All that remains is to see how fairly the television editors extract significant clips and to find out how the rest of the nation feels.
LATER FOOTNOTE: As matters turned out a few months later, this national legislation had more of a local New Jersey effect than the audience could have guessed. Mandating health insurance for 30 million uninsureds, Obamacare accomplished it for 15 million of them by forcing them into the state Medicaid program, which is widely acknowledged to be the worst program in American medicine, because it usually is the most under-funded. New Jersey residents are firmly opposed to anything which raised their already high local taxes and will focus intently on the attempt in the coming lame-duck session of Congress (November 2010) which intends to transfer federal money to states to pay for Medicaid, and which is given only the narrowest chance of success. Republican Governor Christie deftly split the industrial unions from the public sector unions with the remark, "Every time they get a raise, you get a tax increase." It was hard to answer.
Time To Care
|
| Dr. Norman Makous |
It sometimes seems as though Medicare has been a standard part of the scene for so long it now needs major reform, but when a doctor has practiced Medicine for sixty years he has seen a lot of contrasts between the old way and the new way, not all of them favorable to the new -- which we are now tired of, and trying to repair. That's particularly true if the doctor practiced at America's first and oldest hospital, because it sustained many traditions from two centuries before, and was among the last to yield to the imperatives of newcomers for the last forty years, their hands grasping for the purse strings. Dr. Norman Makous must either have a remarkable memory or a thick, detailed diary. He tells three hundred pages of fast-reading anecdotes about sixty years of his own medical practice, before summing up in fifty pages of reflection. One by one, he describes the innovations in his field of cardiology and how they affected him and his patients. Thiomerin, one of the first of many easy ways to pump out excess body fluid accumulation, transformed the treatment of congestive heart failure. Synthetic digitalis claimed to but probably did not much improve things over dried digitalis leaves; it certainly raised the cost. Cardiac catheterization, electro-shock resuscitation, ultra sound diagnostics, MRI and CAT scans, cardiac surgery using the heart-lung machine, and finally cardiac transplants -- all started out as headline-news spectaculars, evolved into cutting-edge advances, and then settled down into the Standard of Care that you obtained a plaintiff lawyer to sue about. All in one medical lifetime, supposedly prepared for by one Medical School course, followed by one residency apprenticeship, the specialty of Cardiology was completely transformed at least six times.
Meanwhile, the leadership of the medical profession was tenaciously resisted by those who supposedly followed its direction. Hospital administration.
Competitive Institutions: Paying for Assisted Living
Around the turn of the 20th Century, it was the fashion to build specialty hospitals, devoted to a single disease like tuberculosis or polio, or one specialty like obstetrics or bones and joints. Eventually, it was realized that almost any disease is handled better if a full range of services is readily available to it. Around 1925, some inspired philanthropists made it possible to combine specialties within a medical center, and it is now generally agreed this is a better way when population density permits it. On the other hand, it is likely a source of price escalation. Time marches on, and the problems of excessive bigness are also beginning to predominate. The idea immediately occurs, to winnow out the routine cases which do not need so much technology, so that we can concentrate and devote high technology (and costs) to patients who will really benefit. And, immediately the perplexing outcry is heard that such rationalization is "cherry picking", which will soon bankrupt the finest institutions we can devise. The validity of such assertions needs to be examined impartially.At the same time, the horse and buggy era has been left behind, causing new separations along class lines, the flight to the suburbs, and the migration of philanthropy toward the exurban sprawl, as well as into urban centers. In all this commotion it was overlooked for a long time that medical care was not merely following the patients to new locations, it was becoming more of an outpatient occupation. Inpatient care was shrinking, and somehow expensive hospitals were swallowing their smaller (and less expensive) competitors. It wasn't a necessary development; Switzerland still favors small luxury "clinics" of ten or twenty beds, usually containing wealthy patients of a celebrity doctor. Local customs like this will change slowly. What America appears to need is more hospital competition and more ambulance competition; the two may actually be somewhat connected issues. For amusement, I once studied the patients in the Pennsylvania Hospital on July 4, 1776, when historical notables were congregating three blocks away. The diseases were remarkably similar to what is seen in hospitals today; problems with the legs, mental incapacity, major injuries, and terminal care. People are treated in hospitals because they can't care for themselves at home.
A BLUE-RIBBON COMMITTEE NEEDS TO STUDY INSTITUTIONAL COMPETITION IN HEALTHCARE.
This is a complicated issue and may take several years, or even several studies to sort out. What is useful for urban settings may be inappropriate in exurban ones; local preferences must be separated from special pleading, and that is not always easy. However, the continuing care center seems to be a permanent direction which is growing in popularity, as is also true of rehabilitation centers and retirement communities. Many of these institutions might incorporate doctors offices for their surrounding community, using the same parking facilities and many of the same medical specialties for both the neighborhood and the core facility. There seems no reason to oppose either rentals or private condominium-style ownership nor any reason to resist group clinics. Exclusive arrangements, however, are more questionable. All of these arrangements should be studied, and unexpected problems flushed out. No doubt the preliminary studies would lead to pilot and demonstration programs. And some practices which initially seem harmless, should in fact be prohibited. We have a lot to learn before we start overturning the existing order. But nevertheless, some arrangements will prove to be superior to others, almost all of them are regulated in some fashion, and the regulations should be examined, too. It should accelerate needed changes to know in advance which ones are ready to be tested, and tested before they are demanded.
*******
.jpg)
|
| CCRCs |
Everyone knows Americans are living thirty years longer because of improvements in health care, and some grumpy people are waiting with glee to see if Obamacare will put a stop to that sort of thing. It must be left to actuaries to tell us whether the nation saves money or not by delaying the inevitable costs of a terminal illness. But one consequence has already made its appearance: people are entering retirement villages in their eighties rather than their seventies. Presumably, people in their seventies are feeling too well to consider a CCRC, although other explanations are possible.
Accordingly, a great many CCRCs are seen to be building new wings dedicated to "assisted living". A cynic might surmise there must be some hidden insurance reimbursement advantages to doing so, but the CCRCs are surely responding to some kind of increased demand when they make multi-million dollar capital expenditures. Assisted living is a polite term for people with strokes or Alzheimers Disease, or some other condition making it hard to walk, or, as the grisly saying goes, perform the activities of daily living. One really elegant place in Delaware has suites with servants quarters, but for most people, the only affordable option is to be in a room designed around the idea of assisting an invalid. It's generally smaller and more austere but fitted out with railings and bars and special knobs. Meals generally have to be supplied by room service.
Not everyone is destined to have a protracted period of decline, but it's fairly frequent and universally feared, so it's a comfort to know your present residence is attached to a wing which provides for it. The question is how to pay for it. There are two main approaches currently in use, adapted to the limited financial resources of the aged and the particularities of CCRC arrangements.
In the first arrangement, there is no increased charge for moving to assisted living, which helps overcome resistance to going there. However, the monthly maintenance charge for others who remain behind in "ambulatory living" is increased, usually about 20%, to provide funding for those who eventually need special assistance. That's a financial pooling arrangement, sort of an insurance plan, and like all insurance, it has a tendency to increase usage unnecessarily. It also increases the cost to those who enter the CCRC at an earlier age, because they make more monthly payments before they use them. Although the monthly premium probably goes up as the costs rise with inflation, there may be some savings hidden in applying an earlier payment stream at a lower rate. That's called "present value" accounting, but like just about all accounting, its unspoken advantages and disadvantages contain a gamble on unknown future inflation.
In the other common financial arrangement, you pay as you go, when and only if you actually use the assisted living quarters. Because of the likely limit to resources, there is usually an attached agreement to garnishee the initial entrance deposit if available funds prove insufficient. The one thing which won't happen is being thrown out in the snow for non-payment; there's a law prohibiting that. Bigger apartments with large initial returnable deposits are of course better off paying list prices. Those with smaller apartments may have smaller deposits, and favor payment by a percent withdrawal. Some places haven't thought this through and offer no choice. In that case, more attention should be paid to those list prices and the percentage markup from audited cost. Better still is to have a free choice of both options, with cost transparency.
The remaining choice is between two CCRCs with differing options, made at the time you enter. The Obamacare fuss has made a lot of people acquainted with "adverse risk selection", which is largely based on the idea that an individual has a better idea of his health future than an institution does since that includes family history as well as earlier health experiences. But in general, a young healthy person is going to live longer without needing assisted living than an old geezer who going to need it pretty soon. A hidden adverse incentive is created for younger healthier people to set the choice aside, and come back in ten years, providing they remain alert to the underlying reason the monthly fee is then somewhat higher than in some competitive CCRC. At the far end of the age spectrum, an incentive is created to go into assisted living quarters a little earlier in life, generally regarded as an undesirable choice.
All this financial balancing act can seem pretty overwhelming to an elderly person who isn't entirely comfortable with the CCRC idea in the first place. Rest assured that everything has to be paid for somehow, and after you die you won't care what choice has been made. If you trust the institution to have your best interests in mind, the only consideration of real importance is whether your money will last you out. The institution cares about that even more than you do, so while they aren't likely to offer unrealistically bargain choices, they may offer a few which are too costly.
America has had a ninety-year romance with insurance because it is so comforting to be secure and oblivious to finances. This is just another example of the struggle between the search for a security, and the struggle to devise ways to pay for it. While no one can be positive about it, we're all in this together.
Foreground: Parliament Irks the Colonial Merchants

|
| Charles Townshend |
Charles Townshend, Chancellor of the Exchequer under King George III in 1766-67, had a reputation for abrasively witty behavior, in addition to which he did carry a grudge against American colonial legislatures for circumventing his directives when earlier he had been in charge of Colonial Affairs. His most despised action against the Colonies, the Stamp Act, seems to have been only a small part of a political maneuver to frustrate an opposition vote of no confidence. The vote had taken the form of lowering the homeland land tax from four to three shillings (an action understood to be a vote of no confidence because it unbalanced the budget, which he then re-balanced by raising the money in the colonies.) The novelist Tobias Smollett subsequently produced a scathing depiction of Townshend's heedless arrogance in Humphry Clinker, but at least in the case of the Stamp Act, its sting was more in its heedlessness of the colonies than vengeance against them. One can easily imagine the loathing this rich dandy would inspire in sobersides like George Washington and John Adams. After Townshend was elevated in the British cabinet, almost anything became a possibility, but it was a fair guess he might continue to satisfy old scores with the colonies. When King George's mother began urging the young monarch to act like a real king, Townshend was available to help. On the other hand, the Whig party in Parliament had significant sympathy with the colonial position, as a spill-over from their main uproar about John Wilkes which need not concern us here. Vengefulness against the colonies was not widespread in the British government at the time, but colonists could easily believe any Ministry which appointed the likes of Townshend might well abuse power in other ways before such time as the King or a more civilized Ministry could arrive on the scene to set things right. It was vexing that a man so heedless as Townshend could also carry so many grudges. Things did ease when Townshend suddenly died of an "untended fever", in 1767.
Whatever the intent of those Townshend Acts, one clear message did stand out: paper money was forbidden in the colonies. Virginia Cavaliers might be more upset by the 1763 restraints on moving into the Ohio territories, and New England shippers might be most irritated by limits on manufactures in the colonies. But prohibiting paper money seriously damaged all colonial trade. Some merchants protested vigorously, some resorted to smuggling, and others, chiefly Robert Morris, devised clever workarounds for the problems which had been created. Paper currency might be vexingly easy to counterfeit, but it was safer to ship than gold coins. In dangerous ocean voyages, the underlying gold (which the paper money represents) remains in the vaults of the issuer even if the paper representing it is lost at sea. Theft becomes more complicated when money is transported by remittances or promissory notes, so a merchant like Morris would quickly recognize debt paper (essentially, remittance contracts acknowledging the existence of debt) as a way to circumvent such inconveniences. In a few months, we would be at war with England, where adversaries blocking each other's currency would be routine. By that time, Morris had perfected other systems of coping with the money problem. In simplified form, a shipload of flour would be sent abroad and sold, the proceeds of which were then used to buy gunpowder for a return voyage; as long as the two transactions were combined, actual paper money was not needed. Another feature is more sophisticated; by keeping this trade going, short-term loans for one leg of the trip could be transformed into long-term loans for many voyages. Long-term loans pay higher rates of interest than short-term loans; it would nowadays be referred to as "riding the yield curve." This system is currently in wide use for globalized trade, and Lehman Brothers were the main banker for it in 2008. And as a final strategy, having half the round-trip voyage transport innocent cargoes, the merchant could increase personal profits legitimately, while cloaking the existence of the underlying gun running on the opposite leg of the voyage. If the ship is sunk, it can then be difficult to say whether the loss of such a ship was military or commercial, insurable or uninsurable. In the case of a tobacco cargo, the value at the time of departure might well be different from the value later. Robert Morris became known as a genius in this sort of trade manipulation, and later his enemies were never able to prove it was illegal. Ultimately, a ship captain always has the option of moving his cargo to a different port.
Other colonists surely responded to a shortage of currency in similar resourceful ways, including barter and the Quaker system of maintaining individual account books on both sides of the transaction, and "squaring up" the balances later but eliminating many transaction steps. Wooden chairs were also a common substitute as a medium of exchange. But "Old Square-toes," Thomas Willing, experienced in currency difficulties, and his bold, reckless younger partner Morris displayed the greatest readiness to respond to opportunity. Credit and short-term paper were fundamental promises to repay at a certain time, commonly with a front-end discount taking the place of interest payment. The amount of discount varied with the risk, both of disruption by the authorities, and the risk of default by the debtor. This discount system was rough and approximate, but it served. Quite accustomed to borrowing through an intermediary, who would then be directed to repay some foreign creditor, Morris, and Willing added the innovation of issuing promissory notes and selling the contract itself to the public at a profit. Thus, written contracts would effectively serve as money. A cargo of flour or tobacco represented value, but that value need only be transformed into cash when it was safe and convenient to do so.
The Morris-Willing team had already displayed its inventiveness by starting a maritime insurance company, thereby adding to their reputation for meeting extensive obligations; they established an outstanding credit rating. Although primarily in the shipping trade, the firm was also involved in trade with the Indians. There, they invented the entirely novel idea of selling their notes to the public, essentially becoming underwriters for the risk of the notes, quite like the way insurance underwriters assumed the risk of a ship sinking. Their reputation for ingenuity in working around obstacles was growing, as well as their credibility for prompt and reliable repayment. In modern parlance, they established an enviable "track record." A creditor is only interested in whether he will be repaid; satisfied with that, he doesn't care how rich or how poor you are. The profits from complex trading were regularly plowed back into the business; one observer estimated Robert Morris's cash assets at the start of the Revolution were no greater than those of a prosperous blacksmith. It didn't matter; he had credit.
In the event, this prohibition of colonial paper money did not last very long, so profits from it were not immense. But ideas had been tested which seemed to work. Today, transactions devised at Willing and Morris are variously known as commercial credit, financial underwriting, and casualty insurance. In 1776, Robert Morris would be 42 years old.
Black Swans (Financial Variety)
|
| Nicolas Baudin |
The mouth of the Delaware River once teemed with white swans, but black swans were unknown until the French explorer Nicolas Baudin brought home a few from Australia, where they are now celebrated as the state animal of Western Australia. Empress Josephine Bonaparte was delighted with them, made them known as her birds, and thus made the term "Black Swan" more or less synonymous with rare chance occurrences. The implied inference that every white swan contains a remote potential for breeding a black one is doubtful biology, however. More likely, black swans are a distinct species -- Cygnus atratus-- confined to Australia and New Zealand, and just about extinct in New Zealand. In that view of things, the rarity of black swans is equivalent to the prevalence of black ones, mixed within the population of generally white ones. Nevertheless, for this article, it is convenient to continue the unlikely conjecture that most, or perhaps every, white swan contain a small potential to hatch a black one.
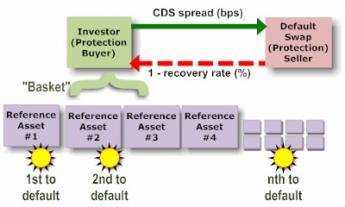
|
| Credit Default Swaps |
Many theories exist for the discovery that financial crises are commoner than chance alone would seem to predict; if they follow a Gaussian normal distribution curve, it must be somehow different from the distribution curve of smaller fluctuations. Observing this discordance is more or less how the phenomenon was discovered. The normal volatility of economic activity is calculated from the fluctuations observed in, say, twenty years. When that derived curve is extrapolated to include cataclysmic events which by a theory of the unmeasured "long tail" occur every hundred years, speculators have later discovered by actual measurement that, alas, such disasters actually occur much more frequently. Calculated risks derived from such extrapolations have upended many insurance companies and insurance-like vehicles like Credit Default Swaps, who set their premium charges to match the mathematics. Since CDS approached a hundred trillion dollars in the last crisis, it is important to understand the mechanics of this kind of Black Swan if we possibly can.

|
| Black Swan |
One way to do that is to question the conventional equivalence of risk and volatility ; that is, that the more markets bounce around, the riskier they become. Why should that be true, we might ask. And if it is somewhat true, why does that make it is converse true, those calm seas are safe ones? Those of us who sit and watch the ocean shore soon adopt the habit of speech that high waves at the shore mean a storm is approaching, not that it will ever arrive. After all, the center of the storm may be traveling parallel to the coastline, not directly toward it. And calm seas are particularly undependable predictors; no matter how calm it may be, the next storm might arrive in a few hours, or it may not come for months. Many other analogies spring up, once one puts aside the basic assumption that world economies can be depicted as a linear electrocardiogram. At the very least, they are two-dimensional, possibly three. Possibly four, if you regard time as a dimension.
|
| Dow Jones |
It must be noticed that market volatility is universally viewed as linked to bad things, and many efforts have been made by central banks to reduce risk by constraining volatility. Alan Greenspan is famous for having controlled the economy for seventeen years without major depression. Is that necessarily a good thing? Is it equally possible that kinetic energy was constrained within the inflating balloon until the bursting of it was a far more damaging explosion than small planned deflations would have been?
Experimental testing of these ideas has itself been constrained by an inability to predict the explosion point of expanding financial balloons. Planned deflations have been particularly feared, because of lack of assured ways to get them to stop deflating. But practical warnings such as these are not the same as claiming that lack of volatility is always the ideal state.
Bonds--Do They Have A Future?
|
| Relic of the Past? |
EVER since we finally went off the gold standard completely during the Nixon Administration, the Federal Reserve has adjusted our money supply to create a fairly steady 2% inflation. If inflation is ever less than 2%, the Fed puts more money into circulation. Since many bonds are paying less than a 2% dividend, everybody who buys and holds them at par will lose money in "real" terms. That is, everyone who buys bonds when they are issued and sells them when they mature will lose spending power. Since they fluctuate in the meantime, it is possible for a trader to buy them when they are undervalued by the market. That trader will possibly make money, but only because someone else lost money. Something like that occurred during the recent financial crash bailout, when interest rates declined from 3% to less than 2% but were repurchased by the Fed as "Quantitative Easing", effectively giving speculators a 33% profit at government expense. But that doesn't happen often, and just guess who ultimately lost the money the speculators made. There is also that daunting question: when the time comes for the Federal Reserve to disgorge them, just who is going to buy all these cheapened bonds? In Japan, bonds paid a dividend of less than the rate of inflation for more than a decade; it's hard to think of a reason why the same thing could not happen in America. So it's also hard to imagine a reason why buy-and-hold investors should not abandon bonds, perhaps suddenly all at once, at some unknown time in the future. At that point, many of them will resolve never to try that, again. The whole idea is troubling.
It's particularly troubling in view of the lack of success, so far, of TIPS. These vehicles are new; perhaps the algorithm is set to ignore minor inflation and will over-respond to more major inflation, ultimately rewarding those who buy them. But at least so far, they are a disappointment. Furthermore, TIPS are quite cleverly designed to be inflation-protected, while unfortunately inflation usually does not follow a straight line but is volatile, or saw-toothed; the jury is still out. The jury better hurry up, because all investors look for net income after expenses, which include brokerage costs, taxes, and inflation. A long-term bond might have to pay a dividend approaching 4%, just to emerge with the same net value it started with; after five years of 4%, you could be 20% behind. And yet, the bond market with or without inflation protection is far larger than the stock market and compares in size with all other kinds of market. Who buys them, especially in these huge quantities?
Somebody must maintain statistics which answer this question, but as a guess, the main buyers are insurance companies, endowments, annuities, hedge funds, banks. And foreigners, of course, to whom our follies seem trivial compared with their own. The great argument for bonds is the safety of principal, and although safety is in question anywhere there is inflation when the topic is cash flow, safety is definitely an issue. Cash shortages are what cause bankruptcies, which are mainly useful in providing time to liquidate underlying wealth to pay restless creditors. The management of a non-profit organization must meet its payroll out of cash flow, so non-profits protect themselves from dissolution by having a regular flow of nominally secure bond dividends. Income from donations and contributions can be particularly weak during times of economic stress. Since most for-profit organizations also experience variable periods of time without profits, their situation does not differ greatly from nonprofits. That's particularly true when a for-profit organization has a vocal, activist stockholder group, who will protest fiercely if the management retains abundant cash. For such a predicament, holding bonds creates safety by some definition. The price of that safety is the long-term average loss on the bond portfolio; the company's alternative losses are whatever it takes to maintain a stable work force during unstable times. The business school assessment of this tradeoff is that bond losses can usually be passed through to the customers as a business cost, while layoffs and strikes may not be.
To restate the characteristics of willing bond purchasers, they are governments and corporations who have no common stock issuance alternatives, but regularly face a need to have money available for payroll. They also include borrowers and lenders at nominal interest rates like banks and insurance companies, who can afford to ignore inflation because their own liabilities are in nominal dollars, or come due at a date certain. And then, there are a host of beneficiaries of special-interest bond provisions, like "Flower bonds", state and municipal governments, foreign aid, student aid, etc. As an overall statement, natural bond buyers are those who either do not possess steady equity (common stock) alternative to offer investors or else are shielded in some way from the inflation and tax costs of buying bonds. Speculators and traders are excluded from the discussion because fixed-income trading is a zero-sum game, something you should teach your children to avoid. Other than these special niche opportunities, bonds should be regarded by the ordinary investor as trading opportunities when interest rates get too high, which is roughly every fifteen years or so.
Things in the bond market were not always so bad; Robert Morris, Jr. was a genius for devising this market in 1784. But the equity market was then not so well developed, life expectancies were shorter, and a minimum 2% inflation was not guaranteed by the Federal Reserve. The income tax had not been invented. It was possible to enjoy the promised benefits of lending in those days, for decades or even lifetimes. It was much harder to find investments of superior performance, without getting involved in business management. Meanwhile, the bond market just got huger and huger. Modifying or dismantling it in logical ways would have enormous disruptive effects. So enormous, the Congress has just adopted the stance called "kicking the can down the road", which is a debt you never seriously intend to repay.
Are we waiting for the bond market, the bond vigilantes, or speculators to find some vital vulnerable flaw, and topple it all into the ashcan of history? Or is there some better plan that no one has mentioned?
Weather Man
|
| Paul Walsh |
PAUL Walsh, our local weatherman, recently addressed the GIC (Global Interdependence Center) at the Federal Reserve, and presumably because everyone talks about the weather, the meeting was well attended. While he is too experienced to get drawn into a global warming controversy, we get the general outline of his views. What we call the weather is largely a result of various clouds and wind currents blowing around the planet in response to the rotation of the planetary mixture of oceans and land masses. The familiar landscape visible to astronauts makes it easy to accept this view of things.
The global warming issue, however you explain it and where ever it may be going, is a weather cycle to be measured in centuries. Shorter cycles of about eight years in duration tend to result in American weather patterns sometimes blowing Canadian cold air toward the East Coast, and sometimes blowing California winter weather Eastward. In 2011-12 we seem to be experiencing a California winter, while the preceding two winters were unusually cold, reflecting Canadian conditions. What may or may not be happening with the hundred-year global warming cycle is not easily slipped into our daily conversations. It is probably quite irrelevant to global trends whether or not last year was a cold one, or whether our sidewalks are unusually slippery this morning.
Inquiries about the weather are the number one topic to be clicked on the Internet, reaching 17% of queries. That's nearly double the second largest category and four times the number of inquiries about the stock market. Ordinary variations of the weather have been calculated to have an economic value of $384 billion, or 3.4% of the Gross Domestic Product (GDP). Insurance claims for more severe weather abnormalities run between ten and fifty billion dollars a year. The number of hurricanes and similar disasters is highly variable, sometimes running as high as fifty in a bad year.
Predictions are improving, but ridicule of weatherman errors is still highly embarrassing to the professionals in the business. A generation ago, it was almost impossible to get a one-minute warning of an approaching tornado, but nowadays we average fourteen minutes warning for them. That's almost long enough to be useful. Hurricanes seem to be increasing in frequency, but decreasing in average intensity. But insurance claims are getting steadily higher, largely because more people are building more structures in harm's way.
Small wonder that weathermen are a cautious lot about predictions. The present party line, in case you wanted to ask, is that predictions more than ten years in advance -- are just about impossible.
Obamacare's Constitutionality

|
| President Barack Obama |
Any idea of a smoothly orchestrated introduction of the new law was jarringly interrupted by the U. S. Supreme Court, which granted a hearing to a complaint by 26 State Attorney Generals, that the ACA Act was unconstitutional. It was big news that the whole Affordable Care Act might be set aside without selling a single policy of insurance. The timing (before the Act had actually been implemented) served to guarantee that the constitutional issue, and only that issue, would be discussed at this Supreme Court hearing. By implication, there might be more than one episode to these hearings.
While many could have declaimed for an hour without notes, about difficult issues perceived in the Obama health plan, questioning its constitutionality had scarcely entered most minds. Then of a sudden, near the end of March 2012, a case testing the constitutionality of mandatory health insurance was granted certiorari and very promptly argued for three full days before the U.S. Supreme Court. Twenty-six state attorneys general brought that case, so it was not trivial. In jest, one Justice quipped he would rather throw out the whole case than being forced to spend a year just reading 2500 pages of it. But Justices are practiced in the art of quickly getting to the heart of a matter; it soon boiled down to one issue: was it constitutional for Congress to force the whole nation to purchase health insurance? Is there no limit in the Constitution about what the federal government can force all citizens to do, even though the federal government itself is severely limited in scope? Even though the Tenth Amendment states that anything not specifically granted to the federal becomes the province of the states? Would a people who fought an armed revolution for eight years over a 2-cent tax on tea, now consent to a much larger requirement which it was not constitutionally authorized to impose? Most people finally wrapped their heads around some formulation of this non-medical concept to a point where they vaguely understood what the Judges were arguing about. This was beginning to look like a topic where We The People made a covenant with our elected leaders, and reserve the sole right to change it.
|
The powers not delegated to the United States by the Constitution, nor prohibited by it to the States, are reserved to the States respectively, or to the people.
|
| Tenth Amendment |
The Constitution describes a Federal system in which, a few enumerated powers are granted to the national government but every other power is reserved to the state legislatures. The Constitution had to be ratified by the states to go into effect, and the states had such strong reservations about the surrender of more than a handful of powers that they would not ratify the document unless the concept of enumeration was restated by the Tenth Amendment. If states could not be persuaded of the need for a particular power to be national, they might refuse to ratify a document which enabled permanent quarrels about the issue. That wariness explains why The Bill of Rights goes to the extra trouble of declaring certain powers are forbidden to any level of government.
Separation of powers further explains why Mr. Romney's mandatory health insurance plan might be legal for the Massachusetts legislature but prohibited to Congress. After Chief Justice Roberts got through with it, whether that truly remains the case will now depend on whether it is described as a tax, a penalty, a cost, or whatever, and only if the U.S. Supreme Court later agrees that was a proper definition. Because -- to be considered a tax it must be too small to be considered coercion. The law itself apparently does not underline this distinction in a way the Justices felt they could approve. Indeed, while Mr. Obama in his speeches firmly declared it was not a tax, later White House "officials" declared it might be. There was agreement the Federal government could tax, but no acknowledgment that taxes might have any purpose other than revenue.
Under circumstances widely visible on television, however, it was clear that the House of Representatives had been offered no opportunity to comment on this and many other points in this legislation. To a layman, that fact itself seems as clear a violation of constitutional intent as almost any other issue, since the Constitution indicates no idea was ever contemplated that any President might construct laws, nor like the courts, interpret their meaning. The first three Presidents repeatedly raised the question of whether they had the authority to do certain things we now take for granted. And Thomas Jefferson was similarly boxed in by a clever Chief Justice, who said, in effect, Agree to This Decision, or be Prepared to Get a Worse One. The Constitution says it is the function of the Executive branch to enforce the law, "faithfully". Presumably, all of the thousands of regulations issued by the Executive Branch under this law must meet the same test.
Given that the Justices now hold it constitutional for the federal Congress to mandate universal health insurance, based on some authority within taxation, the immediate next issue is paying for it. Millions of citizens, usually young and healthy but sometimes for religious reasons, do not want to buy health insurance and would be forced to do so by this law because the only available alternative is to pay a revenue tax. The purpose of including them is to overcharge people who will predictably under-use community-rated insurance, and thus enable the surplus to reduce costs for those who do want to buy health insurance. (Here, the Court had the pleasure of reducing an unusually opaque law to an unusually succinct summary.) To avoid the charge of a "taking", the Administration must either surrender on the universal mandatory point or else surrender the level premiums of community rating. The lawyers for the complaining attorneys general laid great stress on this particular issue in their arguments, and it occasioned much of the discussion from the bench. However, until the law is in action there is as yet no cause for damages.
Here it will depend on whether you call it a permissible activity for Massachusetts or for the Federal government. The Constitutional point seems to be that it is a legitimate Federal power to tax for the "general welfare", so it now becomes essential to know if the taxes for noncompliance in Obamacare are really a penalty. The Justices seemed to be questioning whether the whole scheme would collapse with the forced subsidy eliminated, and because of that be deemed to have been a "general welfare purpose" adequate to meet the constitutional requirement of a permissible enumerated purpose. Lawyers can generally find such a defined purpose in the words of the Constitution, even if they have to dip into the penumbras and emanations of the words. So the question might just devolve into whether a majority of the Justices wish to declare the penumbra to be within the enumerated powers of Congress. To all of this, the lawyers for the attorneys' general reply that such an enumerated power is impossible because there is no limit to what could be done by this method. Congress would then be allowed to mandate that everyone eat broccoli for dinner, or buy a General Motors car in order to pay for the deficits of rescuing that company from bankruptcy. Almost anything could be mandated by establishing a penalty called a tax; including a mandate that everyone buys a product in order to pay for the deficits of mandating it, illustrates there exists at least one circularity of enumerating something like a power of Congress. According to this reasoning, mandated health insurance cannot, therefore, be an enumerated power of Congress, either now or at any time in the future. The sort of speculative law outlined in this paragraph is exactly the sort of thing the Supreme Court dislikes and shows the utility of denying access to the courts to anyone who cannot claim "standing", defined as a claim of actual injury from a law.
The Justices undoubtedly had to weigh the fact that the American public has a strong distaste for this sort of convoluted reasoning, which sounds like a convention of Jesuit priests having fun. On many other occasions, however, the public has accepted the judgment of people it hired to understand this sort of thing; that's called respect for the law. Eighty years ago in the Roosevelt court-packing case, there was the same sort of collision between the Court and the President, and the Court knuckled under even though the public supported the Court. In both cases, the Court seemed to be yielding to the President, with the unspoken compromise that the President would not pursue his earlier course with quite so much vigor. Since the really central 1937 question of overturning the Interstate Commerce clause ("Commerce among the several states") was left unaddressed, the velvet glove might yet contain an iron fist.
"They Don't Make That, Anymore"
They Don't Make That, Anymore These words from the nice young lady in the drug store, left me astonished, baffled, bewildered, and angry.
Although I am retired from the practice of medicine, my limited license permits me to prescribe ethical drugs for myself. I had not realized, until that very moment, that to some extent it also isolated me from the experiences of my fellow patients. Let me explain.
The drug involved was tetracycline, which I had surely prescribed a thousand times, and to which I had a sort of loyalty growing out of the fact that I took it myself. In the days when I was a college student, I came down with a form of pneumonia that involved a lot of coughing, like whooping cough. It was then called virus pneumonia because it was somewhat different from ordinary pneumonia, even though it was called Primary Atypical Pneumonia in polite academic circles. Eventually, we learned that its cause was neither a virus nor a bacterium, but rather something in between in size, called Mycoplasma. All of this is important to know, because it tends to appear as a question on a certification examination, but the fact of the matter is, it was a disease for which there was no effective treatment. We could cheer up a little to know that of four hundred recruits at an Alabama training center who came down with it, only one died. On the other hand, Legionnaire's Disease is also caused by a Clamydia and lots of them died, probably because most of them were older. But no matter, in 1944 there was no treatment, and I can tell you it is very unpleasant for a very long time, no matter how young you are.

|
| CAT Scan |
In 1950 I got it again, but this time I was a doctor and knew there was a good treatment. It sounds strange to say so, but I was sort of happy to be able to try out the new medicine, which was then called Aureomycin because the powder was golden yellow. Aureomycin was a trading name, with a patent, and when the patent expired the generic form was called Tetracycline. It worked just fine, and in three or four days I was out of the hospital, perhaps a little weak and shaken, but cured. Incidentally, I discovered an interesting feature of the disease which I believe has not been previously reported. It had long been observed that the chest x-ray showed pneumonia while the stethoscope perceived very little abnormality, a feature which disconcerted those of us who were concerned with the cost of medical care, particularly members of a generation who felt sniffy about the dependence younger physicians displayed for x-rays, and nowadays for CAT scans and MRIs. Unfortunately, in this particular instance, x-rays are clearly superior to stethoscopes.
My third time around for "viral" pneumonia was a few years later; I was sitting on a park bench near the hospital when I recognized the old symptoms were coming back again, so I went straight to the x-ray department and had a chest x-ray less than an hour after the symptoms appeared. I planned to have an x-ray to prove it, go get some tetracycline and be all better over the weekend, with a rollicking anecdote to tell doctor friends about. Unfortunately, the x-ray was normal, so I was admitted into the hospital to see what was wrong. The next morning the x-ray showed a densely consolidated lung, so it had been viral pneumonia all along. And so my old prejudices were vindicated; it was possible to be too quick to order x-rays after all. Unfortunately, the extra twelve hours without treatment allowed me to get a lot sicker than I had to be. I think I know this because, doggone it, I developed the same disease several decades later, took no shortcuts to the drug store, and was fine in a couple of days after I immediately started taking tetracycline. You could say this strange recurrence of Mycoplasma pneumonia over one-lifetime sort of illustrates how medical care of the disease has become progressively cheaper. Instead of a month in the hospital with no treatment, it was now a matter of skipping the stethoscope, skipping the x-ray, skipping the hospital, and just swallowing some cheap tetracycline capsules. You have to have the nerve to do it, of course, and ethically you probably only have a right to do it to yourself, knowing the risks and being willing to accept them. There is, however, one flaw in this story.
When Aureomycin first emerged from the clutches of the FDA (and well before that accursed Kefauver Amendment), it seemed astonishingly expensive. Because I knew what it weighed (250 milligrams per capsule), and I knew what gold cost ($35 an ounce), it was easy for an idle mind to calculate that Aureomycin cost more than gold. Gold now sells for $1700 per troy ounce, so you could take this story in the direction of inflation. I rather prefer to take it in the direction of nominal dollar amounts, because Aureomycin retailed for $5 a capsule the third time I had the disease, and $1 per capsule when it lost its patent and became tetracycline. The fourth time I had the disease, I bought a container of fifty capsules for 76 cents. But as you have already heard, by the fifth time I couldn't buy it for any price, because everybody had stopped making it. Since my view of the economics of useful commodities is that low prices will only cause shortages if there is artificial market interference, the usual cause of shortages is rationing. Somebody who understands the 2500 pages of Obamacare better than I do will have to tease out the way rationing has caused shortages of tetracycline. And when they are done confusing the public, let them explain why you also can't buy KMnO4 crystals (potassium permanganate), which has cured more cases of athlete's foot for twenty cents, than all those cans of stuff in spray canisters.
Looming Early Issues in Obamacare

|
| Obama Care |
The Attitude of Big Business. In order to preserve maximum flexibility as long as possible, many important features of the Affordable Care Act (Obamacare) remain unrevealed, and some are perhaps still unsettled. Furthermore, attitudes change with experience. At the formation of the Obamacare idea, the leaders of big business (at the time) were more concerned about foreign competitors than about employee attitudes. The traditional goal of a "level playing field" led them to favor an employer mandate to provide employee healthcare. It probably was presented to them that they could only have their desires by agreeing to a universal individual mandate for everybody. Although it was uncertain whether the employees would agree, universal was the price to be paid, and they paid it. Whether new leadership supports this compromise or not, it is generally assumed that big business feels obliged to support Pete Stark's universal mandate until it is tested. Only time will tell whether businesses will withdraw their support in the face of events, but fragile beginnings certainly do not assure permanent support. Since it was the withdrawal of this group's support which destroyed the Clinton plan in 1994, a significant issue hangs in the balance. Therefore, when conflicts were discovered with the ERISA laws under which big business works, the inclusion of big businesses in the framework of the Affordable Care Act was postponed for a year. How it will emerge next year or whether the ACA can survive for a year without major business inclusion, both remain to be seen.
The Rising Voice of the Uninsured. A financial recession usually increases the number of health uninsured, but at present unemployment is slowly falling. However, decades of scientific medical advances are not only extending longevity but reducing non-fatal illness among the young and uninsured. Although it is unclear whether youthful perceptions match the actual changes in their morbidity, young healthy people who rebel at paying health insurance premiums may actually increase in number substantially during the coming decade. Although overall inflation has been moderate, discomfort from competing costs of college debts and items such as gasoline have escalated. When the Affordable Care Act is fully implemented, youthful perception may make the first serious test of its usefulness. Those among them who actually get sick may get an opportunity to sample Medicaid and report their experiences to their friends. To some extent, this will be a race between efforts to improve Medicaid in order to forestall complaints, and the tendency of young people to try to get their way by pounding the table with their shoe. If successfully managed, it could promote some badly needed improvements in Medicaid. Handled poorly, however, it could bring the program down.
Cost of the Program. The fact must be squarely faced that insurance almost always increases costs. That is true of all casualty insurance, whether auto, homeowners, or maritime. Correctly applied, it can indeed redistribute costs, but insurance imposes extra administrative expenses, and it produces "moral hazard", so total costs are increased by insurance. Moral hazard is a term of art, signifying that nobody spends someone else's money as carefully as his own. Actuaries calculate the extra cost imposed by present American forms of health insurance to be at least 30% of the total service, and arguments can be made it will be so much more, that level historical costs cannot conceal the appreciably higher premium level. Longevity is improved by reducing the number of brushes with life-threatening illnesses in a lifetime; costs go up because prices go up.
Universal coverage now introduces its own uniquely unwelcome issue, that eliminating non-insurance market benchmarks for medical prices also eliminates the cost guidance they formerly provided. Crippled though it may have been, the partial cash market did set benchmarks, if not prices, which insurers then had to match -- and those benchmarks will possibly soon be seriously diminished. That development will be welcome to those who wish to receive higher prices, but cause dismay among those who have to pay for them. The result is predicted to lead to price controls, which will, in turn, provoke shortages, possibly demonstrations or worse. Matters may not follow that path, but it is hard to see why not. As to any reduced overhead like marketing costs, employer-basing has already reduced them to a small opportunity for streamlining. In the past, a resort to price controls has almost invariably led to shortages. Even in 2013, there have been shortages of cancer drugs, an almost unheard-of event in the past century.
To put it mildly, rationed healthcare is politically disadvantageous for those who attempt to enforce it. The most conservative projections now suggest that Obamacare will increase healthcare costs by 22%. Since the following proposals would by contrast almost surely reduce costs by a conservative 30%, it is not impertinent to suggest that no matter remains closed while a 50% overall cost swing remains credible. That would be particularly true when it concerns 17% of gross domestic product (GDP) during a recession. In fact, no one has even contemplated what it would mean to inject 5% of American GDP back into the world economy, especially by the mechanism of releasing a paralyzed medical system.
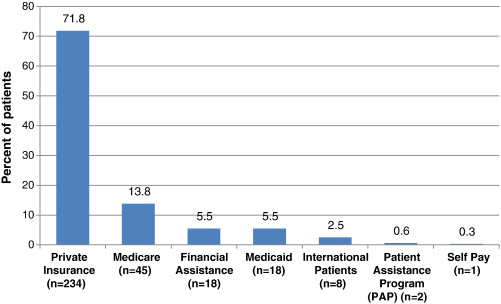
|
| Patient Participation |
Patient Participation in Claims Costs, Generally Speaking. For the insurance industry, this is an old story. Industry survival has depended on success in answering it effectively. In health insurance, the traditional approaches have mainly been 20% co-pay and about $500 annual deductible. The first means 20% of all benefits cost, the second means the first $500 of benefit costs in a year. These figures evolved out of countless negotiations between labor and management, or within legislatures, are now accepted as traditional, and are accepted by the public. These figures also represent how much each side thinks it can afford since they see themselves as ultimately paying the bill. Until recently, however, patient participation at such small levels has not reached a point where it significantly influences patient behavior, which is set by entirely different forces and is now the main long-term cause of healthcare cost inflation. As mentioned above, business negotiators seldom pay much heed to imposed costs, just so long as their major competitors must pay the same costs; in fact, that is one of the flaws in our corporate system. However, governments as third-party payers enjoy no such luxury, and most of the complaining about healthcare cost inflation has originated with governments. Consequently, businesses not infrequently drag governments to higher cost levels, and this must be recognized as a reality of entitlement programs. Furthermore, attempts at raising patient cash contributions have always had political rather than economic origins, usually loudly characterizing any cost constraints at all as crippling the intent of insurance, making false promises, and depriving the poor of humane treatment. If patient contribution ever reaches 50% of costs, the program will likely be called a failure (Insurance exchanges please take note.).
However, it would appear incentives cannot affect overall patient behavior very much until patient payments to reach a much higher point, and we may well see some experiments to test what that level may be. (As it is argued here, this dilemma need not be completely dispositive.) More recently, steadily rising healthcare costs have actually led to employer increases in co-pays and deductibles, and the Obama administration has been giving signs of yielding to the behavior modification argument. However, these approaches cannot be called a success until they seriously reduce long-term healthcare cost inflation, and that remains a doubtful outcome.
In fact, no desperately sick patient should ever be expected to pay much attention to costs. The restraint of partial cash payment should be reserved for lesser conditions, and even provider discipline should be reserved for what are provably individual provider decisions, whether at the institutional level or the professional one. There are certainly broad areas where no patient cost restraint whatever can be justified, and program design should recognize that premise. Nevertheless, much more could be done with patient participation in costs than is done at present.
|
| Cost Restraint |
Targets for Cost Restraint Requiring Two Distinctive Approaches. There are two factors in overall medical costs: the item price, and item volume. Above a certain level of sickness severity, only item prices can be legitimately constrained, not the volume of service. Before any of that happens, of course, all published prices should be audited and forced to conform to standard cost-to-price ratios, because cost-shifted indirect costs are so prevalent. For minor conditions and illnesses, volume control on the patient remains legitimate, particularly for conditions where patients are usually responsible for inciting them. Patient cost-sharing is, therefore, a legitimate out-patient approach. Officials given the right to set such boundaries will almost surely be assailed as having a conflict of interest, or untrained for the decisions; it is an unpleasant role, attractive only to unpleasant people.
The healthcare market segments itself into two quite different approaches and successful administration consists of accurately distinguishing the two. As soon as the patient enters a hospital, his control of cost creation is taken away along with his clothes. Therefore, payment by diagnosis is a sensible approach for inpatients and could be even more effective if the diagnosis codes were revised to include greater stratification by the additional use of laboratory and other billing sources as confirmatory evidence. An argument can be made that fee for service to a helpless patient operates without cost resistance. But having removed incentives for abuse, the laboratory data becomes even stronger evidence of underlying diagnostic distinctions. Since Obamacare has apparently not fully examined such distinctions, there remains hope it can be persuaded to see the codes need expansion. At present, DRG codes are very crude and rely heavily on errors on the high side canceling out errors on the low side. Furthermore, they are derived from (ICD), the International Classification of Disease, which identifies individual diseases only if they are common, responding to the needs of medical records librarians who complained that usage did not justify the effort of coding every case. This combination of short cuts and errors is too crude for the advanced use now planned for them and would benefit from substituting the coding system called SNOMED3. A case can be made for both lumping and splitting; perhaps two codes are required, a crude one derived by computer-lumping precise ones of the same average cost -- rather than by similar etiology. As matters now stand, teaching hospitals have no way to assert a need for greater reimbursement for greater case complexity, specialty hospitals are able to select inexpensive cases within expensive categories, and rural hospitals are left without satellite cash cows.
However, this is tinkering around the edges of volume measurement. Much greater savings are immediately possible from attention to prices, through billing for direct and indirect costs separately, recognizing indirect costs as the present main locus of cost-shifting. Some serious thought should be given to the growing shift of profitability to the outpatient area, with inpatient care transformed into a loss-leader. As that is increasingly true, it becomes wiser to shift attention to the prices of outpatient and emergency room services. Going all the way to Health Savings Accounts would be ideal because it enlists patient incentives to the side of prices restraint. HSA also comes inherently segmented, between outpatient and inpatient hospital. Beyond segmenting price and utilization controls, however, consideration should also be given to segmenting health insurance itself, to match natural cost segmentations. Prison inmates, persons mentally impaired, and illegal immigrants account for nearly 30 million persons, and require specific ministrations, not patchwork exceptions to what the rest of the population requires.
Higher-cost Health Insurance is What's Mandatory

|
| Obamacare |
Millions of people were unexpectedly canceled by health insurers at the onset of the Obama Insurance Exchanges. The President repeatedly told the public under Obamacare they could keep their old plans if they wished, even after notices to the contrary were mailed out. Insurance spokesmen firmly responded that the terms of the law required they could not keep the old plans for a single day. This promise was reinforced by the original section 1251 but later amended in confusing ways. The public had been told nothing like that during a three-year opportunity to be open about it; in their view, it was sprung on them. Maybe they had even been lied to; more likely, someone objected, causing revision that could be interpreted in several ways. In any event, postponement of the large-employer plans made it moot for the customer but not for the voters. To quell the uproar, the President quickly delayed the cancellations for a year, then extended the suspension, and soon provoking alarmed announcements from the insurance industry that such insurance would lose money. It suddenly became a question whether he could make the insurance companies take them back, and some said they wouldn't, even for just one year. It all sounds like an uproar on the other side of the curtain. The irresistible conclusion emerges there is more to this arrangement than is revealed, with further surprises to be feared. After all, the old rates had been set by the insurers, so something extra must have been added by someone else, but possibly it triggered some clause in the risk corridor provisions. Long accustomed to caveat emptor from salesmen, the public will have trouble getting over the assumption that insurers had been promised more expensive products to sell, in return for doing something of value for the Obama administration we haven't yet learned about.
In a world long accustomed to government anti-trust constraints, that higher prices with less competition could be mandated by law was almost too good for insurance companies to imagine. But now, after the deal is suddenly "postponed", any other industry groups who may have negotiated secret accords, are warned of the price: they must expect to absorb some costs whenever this President is forced to abandon his side of a bargain. The National Journal recently quoted an interview with an insurance lobbyist that large amounts of insurance money helped finance Tea Party meetings, suggesting internal dissension within the industry.
In any event, the canceled policies were almost entirely individual policies in the end, and the ultimate goal is speculative. A different way of expressing the thought is, a large collection of individual policies can more easily resist pressures to cross-subsidize other favored clients. One thing is almost uniformly true of persons who hold individual (as opposed to group) policies: they pay for health coverage with after-tax dollars and therefore are out of pocket by 20-30% extra for equivalent insurance. Many of them may well resist higher-priced products for that reason. Eliminating individual policies would cost the government considerable tax money and indirectly raise premiums. There must be some other motive for animosity toward individual policies, but we will have to wait to find out what it is. It may be just as simple as reducing the visible cost gap between the old system and a new one.
| Posted by: how to get facebook fans free | Feb 13, 2012 10:00 AM |
| Posted by: cheapoair discount | Feb 13, 2012 9:37 AM |
| Posted by: esalerugs promo code | Feb 13, 2012 9:16 AM |
| Posted by: JLLocumTenens | Jan 18, 2011 2:49 PM |
34 Blogs
A Fair Plan for Fire Insurance (and Health Insurance, too?)
Pennsylvania subsidizes risky neighborhoods through a fire insurance company that intentionally loses money. Safe neighborhoods pay higher rates to subsidize the process.
"New" Health Care Reform, 1965
Medicaid, or Title XIX of the Social Security Law, has existed for forty years. That's ample time to demonstrate its hopeless failure. It needs to be repealed, transferring the strictly medical parts to Medicare.
Insuring the Uninsured is Not Entirely a Health Issue
The health industry resents its unwelcome role as a political tool in the tensions between labor shortages on the one hand, and unemployment on the other.
What Good Did Medicare Do?
Statistics seem to show that Medicare did not increase the life expectancy of elderly people during the first ten years of the program.
Community Volunteers in Medicine
A little group of medical volunteers in Pennsylvania's Chester County may not understand the underlying issues very well, but they just pitch in and do what they can about the medically underserved.
Picking Up the Usual Suspects
When the U.S. President plans to change health care, everyone involved in healthcare gets excited. Some want to resist change, some want to exploit it, but everyone wants to have influence.
Equal Pay for Equal Work
Sometimes the representatives of political interest groups try, just a little too hard.
A New Gorilla in the Cage
 Large employers, distressed by costs of employer-based health insurance, had formed a coalition to do something radical about their problem when the Clinton Health Plan burst into the news. Both groups decided to have a joint look at Health Maintenance Organizations (HMO).
Large employers, distressed by costs of employer-based health insurance, had formed a coalition to do something radical about their problem when the Clinton Health Plan burst into the news. Both groups decided to have a joint look at Health Maintenance Organizations (HMO).
Health Maintenance Organizations (HMO)
Paul Ellwood gets credit for inventing the term HMO, and for selling a version of it to large employers, as well as the Clinton Administration. It's been a bumpy ride.
National Business Coalition on Health
The NCOH was founded in 1992, at the time of the Clinton Health Plan. The national body is headquartered in Washington, coordinating seventy or so state and local coalitions of businesses that are paying for employee health care.
Nowheres-ville
 After the Clinton Health Plan faded, but before new ones emerged, participants thought it safe to talk to graduate students studying the event. What emerges is a picture of big business pulling the plug.
After the Clinton Health Plan faded, but before new ones emerged, participants thought it safe to talk to graduate students studying the event. What emerges is a picture of big business pulling the plug.
Hold the Presses
The Clinton Health Plan was dead on arrival, but the media didn't know that.
Be Careful What You Wish For
After the Clinton Health Plan of 1993 fizzled, major employers, pushed their employees into managed care. The negative reaction to HMOs was as unambiguous as it was unexpected -- we hate it.
Computerizing Medical Care
 Healthcare is mainly information processing, but utilizing computers has been a disappointment. Be prepared for high costs and continuing disappointment for decades to come.
Healthcare is mainly information processing, but utilizing computers has been a disappointment. Be prepared for high costs and continuing disappointment for decades to come.
Healthcare Reform: Looking Ahead (1)
It's safe to predict two upheavals in the cost of health care which will overwhelm all the old assumptions. The first upheaval comes in 2012 when the boomers retire.
Healthcare Reform: Looking Ahead (2)
Spending for health care will just grow and grow forever. Oh, yeah?
Healthcare Reform: Looking Ahead (3)
If radical new proposals for health care reform appear in the next few years, they are likely to originate in Detroit.
Segmented Health Insurance
For a century, insurance has treated all medical care as one big lump. It's time to have a second look at this.
Making Money (8): Virtual Money
 When money was tangible you had to guard it, now that it's mostly virtual you have to verify it. Hardly anybody can, and that's a problem.
When money was tangible you had to guard it, now that it's mostly virtual you have to verify it. Hardly anybody can, and that's a problem.
Exit, Pursued by a Bear
Its medical school consumes 75% of Penn's budget, causing a lot of difficulty for the rest of the University.
South Amboy Explodes
 On May 18, 1950, South Amboy, New Jersey blew up, breaking windows of five counties in its neighborhood.
On May 18, 1950, South Amboy, New Jersey blew up, breaking windows of five counties in its neighborhood.
Veterans Hospital
In spite of much effort and expense, Veterans hospitals are not typical of American healthcare.
Madeira Party 2009
In Colonial America, Madeira was what the upper crust drank.
Reforming Health Reform, New Jersey Style
U.S. Representative Robert Andrews (D, NJ) had a night he won't soon forget on August 24, 2009. Facing 3000 constituents angry about Health Reform, he practically had a public stoning.
Time To Care
A physician who practiced for sixty years, before and after Medicare, has a lot of stories to tell about how Medicine has changed and been changed.
Competitive Institutions: Paying for Assisted Living
Everyone knows that Americans are living longer, but it creates some new problems.
Foreground: Parliament Irks the Colonial Merchants
The Townshend Acts, upsetting trade and hated by Americans, bordered on economic warfare. The British tested tea, stamps and manufactures, but the most effective economic pressure points proved to be paper money and gunpowder. The Americans reacted to all this as second-class citizenship.
Black Swans (Financial Variety)
How many financial crises can be understood as "Black Swans" if we regard a financial Black Swan as a case of constrained energy kinetics?
Bonds--Do They Have A Future?
It's increasingly hard to imagine why investors buy bonds because it's increasingly difficult to imagine an end to inflation.
Weather Man
The weather is a big business.
Obamacare's Constitutionality
Obamacare's constitutionality was argued before the U.S. Supreme Court in late March, 2012.
"They Don't Make That, Anymore"
 Pharmaceutical drugs seem to follow a trajectory of fifty years, from new and expensive, to cheap, old and eliminated.
Pharmaceutical drugs seem to follow a trajectory of fifty years, from new and expensive, to cheap, old and eliminated.
Looming Early Issues in Obamacare
Obamacare is constructed from the regulations issued by the Secretary of Health and Human Services. They respond to the laws passed by Congress which were two thousand pages long. After two years, only the outlines of this program are known. What are the looming issues?
Higher-cost Health Insurance is What's Mandatory
 Cancellations of millions of health insurance policies show the Affordable Care Act aimed to mandate a few specific types of policies, and not merely to the uninsured. Without a government subsidy, most plans would cost more. The promise that you can keep your old plan, and keep your doctor, was an empty one.
Cancellations of millions of health insurance policies show the Affordable Care Act aimed to mandate a few specific types of policies, and not merely to the uninsured. Without a government subsidy, most plans would cost more. The promise that you can keep your old plan, and keep your doctor, was an empty one.