0 Volumes
No volumes are associated with this topic
Old Age
New topic 2019-04-09 16:04:33 description
Observations About Old Age--From a Participant
As I write this, I am 94 years old. That doesn't set any records, but it currently gets me help with theater seats and silverware dropped on the floor. My mother lived to be 103 (102 might have been better) and many people expect to be 90, someday. It is the latter who don't know what is ahead of them, and may be curious.
Let's start with pot-bellies, which are usually caused by osteoporosis of the spine, but not exclusively so, which leads to excessive curvature of the back, in turn causing protrusion of the belly. Until pot belly becomes advanced, it is usually not noticed, except by tailors and dressmakers. But osteoporosis is more common among women, who ordinarily are more conscious of their appearance. Therefore, the exceptions are more striking: some women have unusually straight backs in spite of advanced osteoporosis. It's rather attractive, the condition seems to be inherited, and is by no means painless. My mother-i-law had this variant, as do a few of my more attractive acquaintances. Mother lived to be 96 but had numerous broken bones for slight cause. This all probably means something, but as yet we mostly don't understand it.
Naturally, my attention has been more focused on the male variant, which seems to affect the gastroenterological tract (GI for short). My wife, who was a radiologist, informed me that the descending colon is mostly empty, most of the time. Therefore, it tends to fill with gas (methane) when you lie in bed for hours at a time. And when you roll over, especially toward the morning, you squash the belly, forcing the gas to travel, and announces it is morning by releasing flatus (farts, in Anglo-Saxon expression.) You can also imagine why most bowel movements take place after breakfast. You, males, can also understand why appearance-conscious young women tend to favor wasp-waists, while older women who have had pregnancies have relaxed abdominal muscles and tend to favor waste-concealing jackets and ballooning skirts. They have pot bellies, too, but they know how to hide them.
Redesigning Old Age
A friend of mine, treated as my contemporary but probably only sixty years old, was recently speaking of a club picnic he, unfortunately, wouldn't be able to attend. His mother was now living with him, and since she was 84, obviously neither of them could go to a picnic on a sailing vessel. The club committee, listening to this regret, chuckled that of course, we shouldn't expect him. My thoughts were somewhat different. Since I'm 94 myself, I was wondering if she was available for a date. And of course I am going to that picnic, why shouldn't I?
| You can't scare me very much about the future scientific costs of medical care. But Insurance and administrative costs are something else of course. If the problem of foolish borrowing puts Medicare out of business, it's hard to see how that could be the fault of my profession, unless perhaps something or other undermines our traditional system of ethics.
Where the ethics thing comes in is in the obvious conclusion that we are spending a lot of money treating diseases we crusty old docs once wouldn't have thought were worth our time. We are fast approaching the point when substantially all the medical catastrophic costs are concentrated in the first year of life and the last year of life. Increased life expectancy is a matter of widening the interval between those two signposts. Medical care between those years consists of treating the disease successfully, preventing disease and managing complaints we once would have dismissed as 'that's nothing'. Even the cost of doing this kind of medical care should decline: patents should expire equipment should simplify treatment should become standardized or even routine. But we notice people won't leave us alone: our government has just spent $27 billion forcing office computers on doctors who don't see the need to be bothered with them. People persist in using our time to inject botulism toxin into wrinkles and to listen to complaints about how lonesome they are. That is to say, the public is beginning to insist on substituting their own view of what they want, for what doctors have traditionally thought was worth treating. This is an expensive way to enjoy the freedom of choice and it is only a matter of time before bureaucrats figure out the least obtrusive way to curtail it. Only when forces come to equilibrium will it be feasible to extrapolate future health costs. What should appall us is the cost of paying for a progressively protracted retirement of so many unemployed people and the absolute impossibility of paying for it by continuing on our present funding path. Maybe that's what all this obesity means. Maybe people are trying to store up enough fat when they are forty, so they can go without eating from age sixty to ninety. A Doctor's Toast to His Patients
A Toast to Them All One the "Four Horsemen" of Johns Hopkins, it may have been Halstead, once remarked on the great debt Gynecology owed to the Baltimore negro woman. In a similar vein, Weir Mitchell might have noted the debt owed by Neurology to the wounded Civil War soldier. But I would go beyond that, to give expression to the gratitude of the whole medical profession to its sick patients. They willingly pull back the curtain on their darkest secret, in the hope their Doctor may find some use for it. A toast to them all. Itch
If the reader has had itchy, dry skin, or a diagnosis of eczema before the age of say 65, stop reading right now and go see a dermatologist. Most elderly people have skin problems, but here we talk about elderly people who have developed skin problems for the first time. We particularly talk about brisk busy people who proudly boast they never had skin problems, but boy they sure have them now. Such people have never been to a dermatologist, wouldn't know where to find one, and therefore don't even know the basics of the subject. Furthermore, what they likely have right now is related to old age, because you mostly can't have diseases of old age until you achieve the status of the elderly. So, if you had something like this before, it becomes complicated to distinguish it from the disorders of old age and you better go see a dermatologist. If that sounds too simple to accept, just think about the following. Dermatitis means skin disease, and eczema is synonymous with dermatitis with the proviso that it oozes, and unfortunately most dermatitis oozes at least to some degree. Take a quick look at eczema in a computer search engine; the first thing it will tell you is the cause is not understood. The second thing it will say is that eczema is mostly found in children. Perhaps now you get the idea; if you have had this in the past, go away and see a skin doctor. On the other hand, any group of old folks sitting around the table in a retirement home will immediately brighten up at the mention of skin problems, since most old folks have skin problems. These people itch and itch badly. Everyone at any age has been bitten by mosquitoes and had an occasional run-in with poison ivy, but these produce bearable itches; the itch of senile eczema is unbearable, gets your full attention. It keeps you awake at night, and thus makes you drop off asleep during the day. The things everybody learns will give heavenly quick relief are generally agreed to make you worse, don't do them. Scratching makes things worse, leading to a mysterious thickening of the skin known as lichenification (that's thickening of the skin, in Latin) which is sort of a scarlet letter among dermatologists, you bad person. And the second thing is a habit of deep scratching so bad you cover your shoulders and back with little red ulcers without fully realizing you are doing this yourself, excoriating your skin with your fingernails. Since people do this without realizing it, of course, they deny it, and doctors for a long time regarded them as nut cases. However, the current more balanced view is that somehow this kind of excoriation suppresses, depresses or otherwise mysteriously inhibits the unbearable itch. So all of this adds up to saying that elderly eczema drives an old codger to the point of dominating his whole thought process; good manners are damned, he wants to talk about it. Better still, do something about it, right now.
That being the case, helpful friends of a certain age know what to advise: hydrocortisone ointment, or the even more potent fluorinated steroid ointments. This stuff really works, particularly if there is some sort of visible skin eruption to direct your effort, but it's dangerous to use too much. It makes the skin lesion and the itch vanish in a couple of days, although of course, it is likely to return in a week; keep that up and you will get skin atrophy, and in large quantities will suppress the activity of your adrenal glands. So, if the area of the itch is so small there is no danger from the ointment you probably can get along without it, whereas if the affected area is large, you are unwise to paint yourself with a lot of this poison. You could take the same stuff in pills, but that gets you to a dermatologist, so you are already in the pay grade above where you should self-medicate. The other home remedy which offers instant relief is hot water. Usually administered as a hot shower lasting a good long time, or luxuriating in a warm tub, or best of all a hot whirlpool bath. Unfortunately, this is really bad news for eczema, almost surely making it much worse. Swimming pools and whirlpool baths are used communally, so they are chlorinated; don't do this to yourself. Instead, do the opposite; go for a week or ten days without a bath. You heard me right, go right ahead and stink. You'll find that deodorants take care of the armpits, so a limited amount of perfume-free soap to the groin and perianal area is the limit. For the rest of your carcass, go back to Biblical times and apply oil, preferably one of the many skin-healing cosmetic lotions that are somewhat overpriced but generally quite soothing. So that's it; no bath for a couple of weeks, use oils for reasonable cleanliness. There's a long-handled lotion dispenser available for a few dollars, that applies the lotion through plastic balls that act like ball bearings. Since being greasy soon becomes part of the problem, this dispenser cleans and soothes with a minimum of oil. If this suggestion fails to work, you are getting closer to the dermatologist's office every minute, because you have not only stopped scalding your skin in the shower, you have eliminated the perfumes and antiseptics in soaps and detergents. By the way, while going without a bath, go without shampoo as well; most shampoos are detergents. Drying of the skin by excessive bathing, allergy to soaps and detergents, are the main causes of this condition, so if going without a bath doesn't work, you may well not have the common form of the condition. There are a couple more things to try, however. You can moisturize your skin with alpha Keri, take Benadryl to help you sleep, aspirin to relieve the itch. You can consider laundering your sheets with soap, or plain water, or just about anything except sodium laurate, the main detergent which has more familiar trade names. If the itch is localized to identifiable areas, the underwear covering that area should be laundered in plain water, or the mildest form of unperfumed soap. Recently, a fairly new idea has surfaced in the form of little bottles of hand lotion, touted to prevent the transmission of the common cold. Whatever its value or lack of it in the cold transmission arena, this stuff seems to kill surface germs for quite a number of hours; applying it to an itchy area is worth a try, because many itches are really allergies to skin bacteria and/or fungus. It's particularly effective for athlete's feet, and if you have that, you may have the fungus elsewhere. But don't keep repeating it very long; chronic application of any chemical is usually hard on the skin. Before the pharmaceutical industry became so advanced and overpriced, this approach was effectively addressed by weak topical (it's a poison if you swallow it) solutions of KMnO4 ("Potassium permanganate"); a dollar's worth of which could cure three-quarters of a regiment of its itches. The other quarter better see a dermatologist. It should take several weeks to exhaust the potential of all of these ideas, so if things are no better, off to the doctor. Every medical student is trained to look for the most serious possible cause of your complaint, no matter how rare. So if we haven't helped your problem, in a few weeks we probably haven't made it much worse, either. When you are filling out your questionnaire at the doctor's office, mention Hodgkins Disease, mycosis fungoides, uremia, and biliary cirrhosis, just in case he thinks you were taking advice from a beginner. Barber of Saville: Male Pattern BaldnessWe don's have any clearer idea of why men lose their hair in the shape of "male-pattern baldness" than why most of us have a bushy head of hair when we are young. It's just the way we are. Most men don't care much, but politicians see a full head of hair as a sign of youth, so politicians tend to wear partial wigs. Vice-President Biden went even further and had expensive hair transplants, but it doesn't fool as many people as he thinks. All barbers must learn what to do about this, and it's called a "comb-over". Male pattern baldness is usually more pronounced at the top of the head, so the parting of the hair is moved gradually to one side and covering to top, gets shoved to the other side. Otherwise, the man would have a flat-headed appearance, with the side hair growing longer and combed over the balding spot in the middle. This leads to a more complex problem: the bald spot eventually gets bigger than the surrounding hair. The barber will counter this tendency as it gradually happens, but unless he is careful, the client will be left with the appearance of two bald spots with a thinning comb-over in the middle. So he resorts to combing the side-hair even further forward and concealing it with stickum. It lasts a day or two and then looks worse, but by that time the barber has his tip and an early-returning client. The wig looks somewhat better, but wigs are hot. Women who are afflicted usually resort to wigs earlier, and put up with the heat.
Buying-Out MedicareOn his 66th birthday, a Health Savings Account owner has only one choice at present: to turn any surplus from healthcare into an IRA (Individual Retirement Account), for taxable retirement living. However, that's a step better than Medicare or employer-based insurance alone, which return unused surplus to the donor of the gift, either the government or the employer, in the guise of the reduced premium cost. However, economists agree the salary soon adjusts downward to treat the confidently expected gift, as part of wage costs. Therefore, health insurance is more expensive than it would be if the surplus were returned to the beneficiary directly. These forms of health insurance have been dominant so long, everyone feels they describe necessary features of health insurance, rather than terms of a contract negotiated by parties other than the beneficiary. The presumption is made the individual has Medicare, so any accumulated surplus in his HSA needs to be spent after age 66, but not on health, since he assumes he will then be completely covered. This presumption is strengthened when the employees of a group plan are merged into a group, but quickly emerge when transfers are made. So any surplus is an average of the group, not specific to the individual. Data is not available to determine whether the size of this issue is enough to worry about. But a pathway probably was not created for overfunding Medicare to create retirement savings through employer-based insurance. In the first place, the surplus does not exist. In the second place, any surplus was probably expected to flow back into Medicare to reduce its cost. In 1965, it was probably expected that Social Security would fill this need, but increasing longevity has created resistance to enhancing all entitlement programs. It scarcely matters, today.
However, if changes in laws and regulations would make it possible, there might be other choices, one of which would be to overfund Medicare coverage, continue the HSA, and spend the generated surplus on retirement. But notice this: as things stand, if you don't need Medicare anymore, you don't get anything back and the government can spend the surplus on battleships. Just as, in plain fact, a commercial insurance company can spend a surplus on executive salaries. It's not fair to say Medicare will "never" have a surplus. By design, any surplus will always be used for healthcare, because that's thought to be part of "share the risk". It's a design feature common in sharing the risk programs, although not a devastating one. The long-range reasoning, however, is this: in 2015 the great need is for flexibility. Some of us will need to spend every dime we have on staying alive. And some of us will need to save every dime we can, in order not to outlive our retirement funds. But that probably won't be the same dilemma, fifty years from now. Almost every one of us could be threatened with poverty during extended retirement into undefinable longevity. It strains the imagination to think of ways to pay for both the present elaborate Medicare and an extended retirement in addition. So, by that time, I fully expect people to have come to the realization that Medicare must be liquidated piece by piece. Not to fund Obamacare, but to pay for their own retirement. When you go to a funeral every week, the idea doesn't usually occur that dying too early might ever become a thing of the past.
Proposal 1:At present, Health Savings Accounts are limited to age 21-66. There should be no age limits at either end, and some provision should be made for inheritance of surplus to newborn children, sufficient to cover their healthcare up to age 21. (3320) Proposal 2: At present, contributions to Health Savings accounts are limited to $3500 per year, age 21 to 66. This should be changed to an aggregate lifetime amount, at least until latecomers have had an adequate transition to the program. (3320)Health Savings Accounts provide the flexibility to do this, but at present many Medicare program details are awkwardly designed to anticipate the need. Right now, the program is not sufficiently modular to permit dropping one feature but retaining others and letting the funds follow the needs. And designing partial proposals is inhibited by a political terror that the public will misinterpret motives. So the first step is for people like me, who have nothing to lose, to step forward and start talking about it. The need for retirement money is looming ahead; we need to prepare Medicare for gradual liquidizing, to pay for it. The first step is probably to design a way to buy out of Medicare, save some money by substituting an HSA for their healthcare, and buy something more appealing with the surplus. The first version will probably be crude and awkward, but it provides a platform to build on. Most politicians, whatever they may think of Medicare and its financing, regard talk of privatizing Medicare as political suicide, so we should be thinking of pilot studies, think tanks, and experimental projects. The old folks who have, or will soon have, Medicare coverage regards it as such a treasure, they tell their elected representatives that privatizing Medicare is the third rail of politics: touch it and you are dead. But a Washington sage once remarked that if things can't go on, they will stop. So, what would it require, induce potential Medicare beneficiaries to select something else, before circumstances abruptly force it on them? That's probably not the best way to go about it. The early initiatives should be generated by scientific advances. The likelihood is great that science will cure one or two of the big five (cancer, diabetes, Parkinsonism, Alzheimer's Disease, schizophrenia) and bit by bit, Medicare will get cheaper in spite of the rent-seeking. As it does, it will seem attractive to increasing numbers of people, to consider cheaper health insurance, shifting Medicare funding to retirement income. The rules should be relaxed to let early-adopters test the changing environment. We already have a flexible funding vehicle in Health Savings Accounts, and fifteen million existing subscribers who will endorse it. The Problem With Medicare. Medicare is 50% self-funded by payroll deductions and premiums and is 50% subsidized by the federal government. The old folks get a dollar for fifty cents and are not about to give it up. They obviously should get their own fifty cents back. It's the fifty cents of government subsidy which is at issue, and the published budget should reflect that fact. Just notice how retirees display almost no interest in the Obamacare controversy, except for one thing. Old folks are uneasy that funding for Medicare might get squeezed in order to finance Obamacare, particularly if the two were in the same budget compartment. When the conversation gets around to that point, retirees suddenly wake up and start talking loudly. If the discussion centered on the subsidy, things might subside, somewhat. But hold on. A retiree approaching his 66th birthday has already pre-paid approximately a quarter of the costs of Medicare, and when he joins, his premiums will later amount to another quarter of the cost. That 50% is the retiree's share of the present costs of Medicare, and naturally, he doesn't expect to see it disappear. The 50% subsidy provided by the government, on the other hand, is what concerns everyone. Even the people who advocate "single payer" systems are talking about extending Medicare to the whole population, gradually perhaps, but probably including the 50% subsidy to everyone. Since healthcare now consumes 18% of Gross Domestic Product, are we willing to see 9% of GDP go from the private sector to the public sector in extra taxes? Or in increased borrowing from foreign nations? We will have to let the politicians wrestle with issues like that, but it will be hard to persuade the public to go along with it. Meanwhile, let's see what persuasion can do if we offer a good enough deal. For a start, let's presume someone in his late fifties had invested in his HSA while he was young, and is approaching the age where he could augment his retirement income from a substantial balance in his IRA (recently converted from HSA). Then, let us say he also wakes up to the realization he gets a second tax deduction from an HSA if he spends extra retirement money on medical care, either on Medicare payroll deductions or Medicare premiums. And if he stops spending some other obligation, he effectively gets a further tax deduction from spending the money on something else which is tax-free. Potentially, that could add a few thousand dollars a year to his income from age 21 to the day he dies. It's a very attractive goal, and while it really would be legitimately spent on healthcare, Congress might well decide they can't afford to lose that much tax revenue. So, the rumination goes, the proposal must somehow save some money for the Government, too. If the subscriber were allowed to make a deal to buy out his Medicare, he might make a payment out of his HSA of about $86,000 untaxed, which with 6.5% declining income, would repay the costs of Medicare throughout his remaining life expectancy, all from the invested lump sum. That might seem like enough on paper, but the government has been going in debt for some time to foreigners and would like to stop doing that. If possible, it would like to pay back the earlier loans. If you include this debt, the Medicare cost is revealed as greater than it seems. Furthermore, the GAO will quickly tell you, if you save tax money, you, unfortunately, make it harder to balance the federal budget. The details of all this may be hard to explain, but the general sense of it all is pretty clear. Let's qualify the simplifications. Different people will have different payroll deductions, at different ages. To some extent, these balance out, because if you have a larger balance in your HSA, you are likely to be older, and likely to have paid more into your Medicare payroll deductions. And to some extent, averages will cancel out and vary with the economy from time to time. A change in the tax code would scramble all of these numbers, but it's preliminary. Medicare is best privatized in pieces, and for that you need prices, so preliminary pricing should be devised for those people who for religious or other reasons, would be interested. Furthermore, accumulating money of this order will require normal interest rates, not abnormally low ones as at present. Since that time is hard to predict, it is necessary to supply minimum interest guarantees, best approximated by index funds of 10-year treasury bonds. Buying out Medicare is a very delicate matter, and should be approached very slowly. The first step is to talk about it without starting a panic. The initial appeal will be found among those who perceive a greater risk from outliving their income than their risk of a major illness cost. They are rare at present, but times will change, Podiatrists Strike it Sort of RichBetween the Civil and First World Wars, we had a flirtation with specialty hospitals. Usually small, they were often owned by physicians with a large specialty practice. As a preamble to the Flexner Report and development of medical centers, they often clustered around a larger general hospital. Thus, the Pennsylvania Hospital was surrounded by several small special hospitals, in an era generally ending with their absorption into some larger general hospital with a wider range of services. So I taught podiatrists for a while and went crosstown to teach future veterinarians. I wasn't paid, I received no title; I just taught because some staff member asked me to, as a small extension of the "rotating" internship concept. That veterinary hospital is still the only private veterinary school in the nation, all others are state schools. To complete the background, the School of Podiatry was in the building of the Skin and Cancer Hospital, a block away from the Babies Hospital. Of these, only podiatry expanded and was moved a few blocks away, under the supervision of Temple University. Others just withered away. The University of Pennsylvania absorbed the veterinary school, found a few wealthy families to pay for it, and moved closer to the farms which survived the shrinkage of agricultural workers to 2% of the workforce. I have to suppose podiatry flourished while the others withered because podiatry patients have since grown abundant, insurable and smelly--you could make a living without as much competition. Like funeral parlors, I see them scattered around the city, often taking up abandoned mansions in formerly prosperous suburbs. The tools of this trade are the heavy clippers for fungus-thickened toenails, and the occupation was once satirized by Tom Stoppard in the preamble to"Rosenkrantz and Guildenstern are Dead". Stoppard himself missed the point of Rosenkrantz's monologue, which was that older people mostly went to a podiatrist because their backs were so stiff they couldn't reach their toenails themselves. , Limits on What Can be Promised: Healthcare Plus a Modest Retirement.This study of Health Savings (and Retirement) Accounts was begun thirty years ago, and with increased intensity in the past five years. During most of that time, paying for health costs was the central concern. Paying a big chunk of health costs would be an achievement, paying for it all would be an impossible dream. Therefore, paying for the whole healthcare system became a goal of my proposals -- to extend the duration of the compound interest generated. If it fell short, well, it paid for a big part of it. Either way, we could afford to leave Medicare alone. But once Medicare came into focus as the main impediment to solving an even bigger problem for exactly the same age group, "saving" it becomes a relatively smaller issue. There had to be some money left over for retirement living, which meant all of Medicare must first be covered, and then, new revenue must be found. The quality of care must not be injured, and -- most of all -- public opinion must be re-directed. This is a specialist's game, but the public is now the supervising coach. Whether they realize it or not, a dependable agent is what they are going to need. And the agency has a long history of imperfection.
Imperfect Agents Theoretically, the best result anyone could provide would be to give a newborn baby a couple of hundred dollars at birth, let a big corporation do the investing, and pay a million dollars worth of bills over the next ninety years on his behalf, at no charge. The long investing period would provide some astonishing returns, and it would be entirely carefree for the customer. But that really overstates things quite a lot.
Last Will of Benjamin Franklin
The Last Will and Testament of Benjamin Franklin I, Benjamin Franklin, of Philadelphia, printer, late Minister Plenipotentiary from the United States of America to the Court of France, now President of the State of Pennsylvania, do make and declare my last will and testament as follows:
To my son, William Franklin, late Governor of the Jerseys, I give and devise all the lands I hold or have a right to, in the province of Nova Scotia, to hold to him, his heirs, and assigns forever. I also give to him all my books and papers, which he has in his possession, and all debts standing against him on my account books, willing that no payment for, nor restitution of, the same be required of him, by my executors. The part he acted against me in the late war, which is of public notoriety, will account for my leaving him no more of an estate he endeavored to deprive me of. Having since my return from France demolished the three houses in Market Street, between Third and Fourth Streets, fronting my dwelling-house, and erected two new and larger ones on the ground, and having also erected another house on the lot which formerly was the passage to my dwelling, and also a printing-office between my dwelling and the front houses; now I do give and devise my said dwelling-house, wherein I now live, my said three new houses, my printing- office and the lots of ground thereto belonging; also my small lot and house in Sixth Street, which I bought off the widow Henmarsh; also my pasture-ground which I have in Hickory Lane, with the buildings thereon; also my house and lot on the North side of Market Street, now occupied by Mary Jacobs, together with two houses and lots behind the same, and fronting on Pewter-Platter Alley; also my lot of ground in Arch Street, opposite the church-burying ground, with the buildings thereon erected; also all my silver plate, pictures, and household goods, of every kind, now in my said dwelling-place, to my daughter, Sarah Bache, and to her husband, Richard Bache, to hold to them for and during their natural lives, and the life of the longest liver of them, and from and after the decease of the survivor of them, I do give, devise, and bequeath to all children already born, or to be born of my said daughter, and to their heirs and assigns forever, as tenants in common, and not as joint tenants. And, if any or either of them shall happen to die under age, and without issue, the part and share of him, her, or them, so dying, shall go to and be equally divided among the survivors or survivor of them. But my intention is, that, if any or either of them should happen to die under age, leaving issue, such issue shall inherit the part and share that would have passed to his, her, or their parent, had he, she, or they were living. And, as some of my said devisees may, at the death of the survivor of their father or mother, be of age, and others of them underage, so as that all of them may not be of capacity to make division, I in that case request and authorize the judges of the Supreme Court of Judicature of Pennsylvania for the time being, or any three of them, not personally interested, to appoint by writing, under their hands and seals, three honest, intelligent, impartial men to make the said division, and to assign and allot to each of my devisees their respective share, which division, so made and committed to writing under the hands and seals of the said three men, or any two of them, and confirmed by the said judges, I do hereby declare shall be binding on, and conclusive between the said devisees. All the lands near the Ohio, and the lots near the centre of Philadelphia, which I lately purchased of the State, I give to my son-in-law, Richard Bache, his heirs and assigns forever; I also give him the bond I have against him, of two thousand and one hundred and seventy-two pounds, five shillings, together with the interest that shall or may accrue thereon, and direct the same to be delivered up to him by my executors, canceled, requesting that, in consideration thereof, he would immediately after my decease manumit and set free his Negro man Bob. I leave to him, also, the money due to me from the State of Virginia for types. I also give to him the bond of William Goddard and his sister, and the counter bond of the late Robert Grace, and the bond and judgment of Francis Childs, if not recovered before my decease, or any other bonds, except the bond due from ----- Killian, of Delaware State, which I give to my grandson, Benjamin Franklin Bache. I also discharge him, my said son-in-law, from all claim and rent of money due to me, on book account or otherwise. I also give him all my musical instruments.
The king of France's picture, set with four hundred and eight diamonds, I give to my daughter, Sarah Bache, requesting , however, that she would not form any of those diamonds into ornaments either for herself or daughters, and thereby introduce or countenance the expensive, vain, and useless fashion of wearing jewels in this country; and those immediately connected with the picture may be preserved with the same. I give and devise to my dear sister, Jane Mecom, a house and lot I have in Unity Street, Boston, nor or late under the care of Mr. Jonathan Williams, to her and to her heirs and assigns forever. I also give her the yearly sum of fifty pounds sterling, during life, to commence at my death, and to be paid to her annually out of the interests or dividends arising on twelve shares which I have since my arrival at Philadelphia purchased in the Bank of North America, and, at her decease, I give the said twelve shares in the bank to my daughter, Sarah Bache, and her husband, Richard Bache. But it is my express will and desire that, after the payment of the above fifty pounds sterling annually to my said sister, my said daughter be allowed to apply the residue of the interest or dividends on those shares to her sole and separate use, during the life of my said sister, and afterwards the whole of the interest or dividends thereof as her private pocket money. I give the right I have to take up to three thousand acres of land in the State of Georgia, granted to me by the government of that State, to my grandson, William Temple Franklin, his heirs and assigns forever. I also give to my grandson, William Temple Franklin, the bond and judgment I have against him of four thousand pounds sterling, my right to the same to cease upon the day of his marriage; and if he dies unmarried, my will is, that the same be recovered and divided among my other grandchildren, the children of my daughter, Sarah Bache, in such manner and form as I have herein before given to them the other parts of my estate. The philosophical instruments I have in Philadelphia I give to my ingenious friend, Francis Hopkinson. To the children, grandchildren, and great-grandchildren of my brother, Samuel Franklin, that may be living at the time of my decease, I give fifty pounds sterling, to be equally divided among them. To the children, grandchildren, and great-grandchildren of my sister, Anne Harris, that may be living at the time of my decease, I give fifty pounds sterling to be equally divided among them. To the children, grandchildren, and great-grandchildren of my brother James Franklin, that may be living at the time of my decease, I give fifty pounds sterling to be equally divided among them. To the children, grandchildren, and great-grandchildren of my sister, Sarah Davenport, that may be living at the time of my decease, I give fifty pounds sterling to be equally divided among them. To the children, grandchildren, and great-grandchildren of my sister, Lydia Scott, that may be living at the time of my decease, I give fifty pounds sterling to be equally divided among them. To the children, grandchildren, and great-grandchildren of my sister, Jane Mecom, that may be living at the time of my decease, I give fifty pounds sterling to be equally divided among them. I give to my grandson, Benjamin Franklin Bache, all the types and printing materials, which I now have in Philadelphia, with the complete letter foundry, which, in the whole, I suppose to be worth near one thousand pounds; but if he should die under age, then I do order the same to be sold by my executors, the survivors or survivor of them, and the money be equally divided among all the rest of my said daughter's children, or their representatives, each one on coming of age to take his or her share, and the children of such of them as may die under age to represent and to take the share and proportion of, the parent so dying, each one to receive his or her part of such share as they come of age. With regard to my books, those I had in France and those I left in Philadelphia, is now assembled together here, and a catalog made of them, it is my intention to dispose of them as follows: My "History of the Academy of Sciences," in sixty or seventy volumes quarto, I give to the Philosophical Society of Philadelphia, of which I have the honor to be President. My collection in a folio of "Les Arts et les Metiers," I give to the American Philosophical Society, established in New England, of which I am a member. My quarto edition of the same, "Arts et Metiers," I give to the Library Company of Philadelphia. Such and so many of my books as I shall mark on my said catalog with the name of my grandson, Benjamin Franklin Bache, I do hereby give to him; and such and so many of my books as I shall mark on the said catalog with the name of my grandson, William Bache, I do hereby give to him; and such as shall be marked with the name of Jonathan Williams, I hereby give to my cousin of that name. The residue and remainder of all my books, manuscripts, and papers, I do give to my grandson, William Temple Franklin. My share in the Library Company of Philadelphia, I give to my grandson, Benjamin Franklin Bache, confiding that he will permit his brothers and sisters to share in the use of it. I was born in Boston, New England, and owe my first instructions in literature to the free grammar schools established there. I, therefore, give one hundred pounds sterling to my executors, to be by them, the survivors or survivor of them, paid over to the managers or directors of the free schools in my native town of Boston, to be by them, or by those person or persons, who shall have the superintendence and management of the said schools, put out to interest, and so continued at interest forever, which interest annually shall be laid out in silver medals, and given as honorary rewards annually by the directors of the said free schools belonging to the said town, in such manner as to the discretion of the selectmen of the said town shall seem meet. Out of the salary that may remain due to me as President of the State, I do give the sum of two thousand pounds sterling to my executors, to be by them, the survivors or survivor of them, paid over to such person or persons as the legislature of this State by an act of Assembly shall appoint to receive the same in trust, to be employed for making the river Schuylkill navigable. And what money of mine shall, at the time of my decease, remain in the hands of my bankers, Messrs. Ferdinand Grand and Son, at Paris, or Messrs. Smith, Wright, and Gray, of London, I will that, after my debts are paid and deducted, with the money legacies of this my will, the same be divided into four equal parts, two of which I give to my dear daughter, Sarah Bache, one to her son Benjamin, and one to my grandson, William Temple Franklin. During the number of years I was in business as a stationer, printer, and postmaster, a great many small sums became due for books, advertisements, postage of letters, and other matters, which were not collected when, in 1757, I was sent by the Assembly to England as their agent, and by subsequent appointments continued there till 1775, when on my return, I was immediately engaged in the affairs of Congress and sent to France in 1776, where I remained nine years, not returning till 1785, and the said debts, not being demanded in such a length of time, are become in a manner obsolete, yet are nevertheless justly due. These, as they are stated in my great folio ledger E, I bequeath to the contributors to the Pennsylvania Hospital, hoping that those debtors, and the descendants of such as are deceased, who now, as I find, make some difficulty of satisfying such antiquated demands as just debts, may, however, be induced to pay or give them as charity to that excellent institution. I am sensible that much must inevitably be lost, but I hope something considerable may be recovered. It is possible, too, that some of the parties charged may have existing old, unsettled accounts against me; in which case the managers of the said hospital will allow and deduct the amount, or pay the balance if they find it against me. My debts and legacies being all satisfied and paid, the rest and residue of all my estate, real and personal, not herein expressly disposed of, I do give and bequeath to my son and daughter, Richard and Sarah Bache. I request my friends, Henry Hill, Esquire, John Jay, Esquire, Francis Hopkinson, Esquire, and Mr. Edward Duffield, of Benfield, in Philadelphia County, to be the executors of this my last will and testament; and I hereby nominate and appoint them for that purpose. I would have my body buried with as little expense or ceremony as may be. I revoke all former wills by me made, declaring this only to be my last. In witness whereof, I have hereunto set my hand and seal, this seventeenth day of July, in the year of our Lord, one thousand seven hundred and eighty-eight. B. Franklin Signed, sealed, published, and declared by the above named Benjamin Franklin, for and as his last will and testament, in the presence of us. Abraham Shoemaker, John Jones, George Moore. CODICIL I, Benjamin Franklin, in the foregoing or annexed last will and testament named, having further considered the same, do think proper to make and publish the following codicil or addition thereto. It has long been a fixed political opinion of mine, that in a democratical state there ought to be no offices of profit, for the reasons I had given in an article of my drawing in our constitution, it was my intention when I accepted the office of President, to devote the appointed salary to some public uses. Accordingly, I had already, before I made my will in July last, given large sums of it to colleges, schools, the building of churches, etc.; and in that will I bequeathed two thousand pounds more to the State for the purpose of making the Schuylkill navigable. But understanding since that such a work, and that the project is not likely to be undertaken for many years to come, and having entertained another idea, that I hope may be more extensively useful, I do hereby revoke and annul that bequest, and direct that the certificates I have for what remains due to me of that salary be sold, towards raising the sum of two thousand pounds sterling, to be disposed of as I am now about to order. It has been an opinion, that he who receives an estate from his ancestors is under some kind of obligation to transmit the same to their posterity. This obligation does not lie on me, who never inherited a shilling from an ancestor or relation. I shall, however, if it is not diminished by some accident before my death, leave a considerable estate among my descendants and relations. The above observation is made as merely as some apology to my family for making bequests that do not appear to have any immediate relation to their advantage. I was born in Boston, New England, and owe my first instructions in literature to the free grammar schools established there. I have, therefore, already considered these schools in my will. But I am also under obligations to the State of Massachusetts for having, unasked, appointed me formerly their agent in England, with a handsome salary, which continued some years; and although I accidentally lost in their service, by transmitting Governor Hutchinson's letters, much more than the amount of what they gave me, I do not think that ought in the least to diminish my gratitude. I have considered that, among artisans, good apprentices are most likely to make good citizens, and, having myself been bred to a manual art, printing, in my native town, and afterward assisted to set up my business in Philadelphia by kind loans of money from two friends there, which was the foundation of my fortune, and all the utility in life that may be ascribed to me, I wish to be useful even after my death, if possible, in forming and advancing other young men, that may be serviceable to their country in both these towns. To this end, I devote two thousand pounds sterling, of which I give one thousand thereof to the inhabitants of the town of Boston, in Massachusetts, and the other thousand to the inhabitants of the city of Philadelphia, in trust, to and for the uses, intents, and purposes hereinafter mentioned and declared. The said sum of one thousand pounds sterling, if accepted by the inhabitants of the town of Boston, shall be managed under the direction of the selectmen, united with the ministers of the oldest Episcopalians, Congregational, and Presbyterian churches in that town, who are to let out the sum upon interest, at five per cent, per annum, to such young married artificers, under the age of twenty-five years, as have served an apprenticeship in the said town, and faithfully fulfilled the duties required in their indentures, so as to obtain a good moral character from at least two respectable citizens, who are willing to become their sureties, in a bond with the applicants, for the repayment of the moneys so lent, with interest, according to the terms hereinafter prescribed; all which bonds are to be taken for Spanish milled dollars, or the value thereof in current gold coin; and the managers shall keep a bound book or books, wherein shall be entered the names of those who shall apply for and receive the benefits of this institution, and of their sureties, together with the sums lent, the dates, and other necessary and proper records respecting the business and concerns of this institution. And as these loans are intended to assist young married artificers in setting up their business, they are to be proportioned by the discretion of the managers, so as not to exceed sixty pounds sterling to one person, nor to be less than fifteen pounds; and if the number of appliers so entitled should be so large as that the sum will not suffice to afford to each as much as might otherwise not be improper, the proportion to each shall be diminished so as to afford to everyone some assistance. These aids may, therefore, be small at first, but, as the capital increases by the accumulated interest, they will be ampler. And in order to serve as many as possible in their turn, as well as to make the repayment of the principal borrowed easier, each borrower shall be obliged to pay, with the yearly interest, one-tenth part of the principal and interest, so paid in, shall be again let out to fresh borrowers. And, as it is presumed that there will always be found in Boston virtuous and benevolent citizens, willing to bestow a part of their time in doing good to the rising generation, by superintending and managing this institution gratis, it is hoped that no part of the money will at any time be dead, or be diverted to other purposes, but be continually augmenting by the interest; in which case there may, in time, be more than the occasions in Boston shall require, and then some may be spared to the neighboring or other towns in the said State of Massachusetts, who may desire to have it; such towns engaging to pay punctually the interest and the portions of the principal, annually, to the inhabitants of the town of Boston. If this plan is executed, and succeeds as projected without interruption for one hundred years, the sum will then be one hundred and thirty-one thousand pounds; of which I would have the managers of the donation to the town of Boston then layout, at their discretion, one hundred thousand pounds in public works, which may be judged of most general utility to the inhabitants, such as fortifications, bridges, aqueducts, public buildings, baths, pavements, or whatever may make living in the town more convenient to its people, and render it more agreeable to strangers resorting thither for health or a temporary residence. The remaining thirty-one thousand pounds I would have continued to be let out on interest, in the manner above directed, for another hundred years, as I hope it will have been found that the institution has had a good effect on the conduct of youth, and been of service to many worthy characters and useful citizens. At the end of this second term, if no unfortunate accident has prevented the operation, the sum will be four million and sixty-one thousand pounds sterling, of which I leave one million sixty-one thousand pounds to the disposition of the inhabitants of the town of Boston, and three million to the disposition of the government of the state, not presuming to carry my views farther. All the directions herein given, respecting the disposition and management of the donation to the inhabitants of Boston, I would have observed respecting that to the inhabitants of Philadelphia, only, as Philadelphia is incorporated, I request the corporation of that city to undertake the management agreeably to the said directions; and I do hereby vest them with full and ample powers for that purpose. And, having considered that the covering a ground plot with buildings and pavements, which carry off most of the rain and prevent its soaking into the Earth and renewing and purifying the Springs, whence the water of wells must gradually grow worse, and in time be unfit for use, as I find has happened in all old cities, I recommend that at the end of the first hundred years, if not done before, the corporation of the city Employ a part of the hundred thousand pounds in bringing, by pipes, the water of Wissahickon Creek into the town, so as to supply the inhabitants, which I apprehend may be done without great difficulty, the level of the creek is much above that of the city, and may be made higher by a dam. I also recommend making the Schuylkill completely navigable. At the end of the second hundred years, I would have the disposition of the four million and sixty-one thousand pounds divided between the inhabitants of the city of Philadelphia and the government of Pennsylvania, in the same manner as herein directed with respect to that of the inhabitants of Boston and the government of Massachusetts. It is my desire that this institution should take place and begin to operate within one year after my decease, for which purpose due notice should be publicly given previous to the expiration of that year, that those for whose benefit this establishment is intended may make their respective applications. And I hereby direct my executors, the survivors or survivor of them, within six months after my decease, to pay over the sum of two thousand pounds sterling to such persons as shall be duly appointed by the Selectmen of Boston and the corporation of Philadelphia, to receive and take charge of their respective sums, of one thousand pounds each, for the purposes aforesaid. Considering the accidents to which all human affairs and projects are subject in such a length of time, I have, perhaps, too much flattered myself with a vain fancy that these dispositions, if carried into execution, will be continued without interruption and have the effects proposed. I hope, however, that is the inhabitants of the two cities should not think fit to undertake the execution, they will, at least, accept the offer of these donations as a mark of my good will, a token of my gratitude, and a testimony of my earnest desire to be useful to them after my departure. I wish, indeed, that they may both undertake to endeavor the execution of the project, because I think that, though unforeseen difficulties may arise, expedients will be found to remove them, and the scheme be found practicable. If one of them accepts the money, with the conditions, and the other refuses, my will then is, that both Sums be given to the inhabitants of the city accepting the whole, to be applied to the same purposes, and under the same regulations directed for the separate parts; and, if both refuse, the money, of course, remains in the mass of my Estate, and is to be disposed of therewith according to my will made the Seventeenth day of July, 1788. I wish to be buried by the side of my wife, if it may be, and that a marble stone, to be made by Chambers, six feet long, four feet wide, plain, with only a small molding around the upper edge, and this inscription: Benjamin And Deborah Franklin 178- to be placed over us both. My fine crab-tree walking stick, with a gold head, curiously wrought in the form of the cap of liberty, I give to my friend, and the friend of mankind, General Washington. If it were a Sceptre, he has merited it and would become it. It was a present to me from that excellent woman, Madame de Forbach, the Dowager Duchess of Deux-Ponts, connected with some verses which should go with it. I give my gold watch to my son-in-law Richard Bache, and also the gold watch chain of the Thirteen United States, which I have not yet worn. My timepiece, that stands in my library, I give to my grandson, William Temple Franklin. I give him also my Chinese gong. To my dear old friend, Mrs. Mary Hewson, I give one of my silver tankards marked for her use during her life, and after her decease, I give it to her daughter Eliza. I give to her son, William Hewson, who is my godson, my new quarto Bible, and also the botanic description of the plants in the Emperor's garden at Vienna, in folio, with colored cuts. And to her son, Thomas Hewson, I give a set of "Spectators, Tattlers, and Guardians" handsomely bound. There is an error in my will, where the bond of William Temple Franklin is mentioned as being four thousand pounds sterling, whereas it is but for three thousand five hundred pounds. I give to my executors, to be divided equally among those that act, the sum of sixty pounds sterling, as some compensation for their trouble in the execution of my will; and I request my friend, Mr. Duffield, to accept moreover my French waywiser, a piece of clockwork in Brass, to be fixed to the wheel of any carriage; and that my friend, Mr. Hill, may also accept my silver cream pot, formerly given to me by the good Doctor Fothergill, with the motto, Keep bright the Chain. My reflecting telescope, made by Short, which was formerly Mr. Canton's, I give to my friend, Mr. David Rittenhouse, for the use of his observatory. My picture, drawn by Martin, in 1767, I give to the Supreme Executive Council of Pennsylvania, if they shall be pleased to do me the honor of accepting it and placing it in their chamber. Since my will was made I have bought some more city lots, near the center part of the estate of Joseph Dean. I would have them go with the other lots, disposed of in my will, and I do give the same to my Son-in-law, Richard Bache, to his heirs and assigns forever. In addition to the annuity left to my sister in my will, of fifty pounds sterling during her life, I now add thereto ten pounds sterling more, in order to make the Sum sixty pounds. I give twenty guineas to my good friend and physician, Dr. John Jones. With regard to the separate bequests made to my daughter Sarah in my will, my intention is, that the same shall be for her sole and separate use, notwithstanding her coverture, or whether she be covert or sole; and I do give my executors so much right and power therein as may be necessary to render my intention effectual in that respect only. This provision for my daughter is not made out of any disrespect I have for her husband. And lastly, it is my desire that this, my present codicil, be annexed to, and considered as part of, my last will and testament to all intents and purposes. In witness whereof, I have hereunto set my hand and Seal this twenty-third day of June, Anno Domini one thousand Seven hundred and eighty-nine. B. Franklin. Signed, sealed, published, and declared by the above named Benjamin Franklin to be a codicil to his last will and testament, in the presence of us. Francis Bailey, Thomas Lang, Abraham Shoemaker. Franklin's Codicil to His Will: Strange Afterthoughts
"I would have my body buried with as little expense or ceremony as may be. I revoke all former wills by me made, declaring this only to be my last. I wish to be buried by the side of my wife, if it may be, and that a marble stone, to be made by Chambers, six feet long, four feet wide, plain, with only a small molding around the upper edge, and this inscription: Benjamin And Deborah Franklin 178- to be placed over us both. The king of France's picture, set with four hundred and eight diamonds, I give to my daughter, Sarah Bache, requesting , however, that she would not form any of those diamonds into ornaments either for herself or daughters, and thereby introduce or countenance the expensive, vain, and useless fashion of wearing jewels in this country; and those immediately connected with the picture may be preserved with the same. My fine crab-tree walking stick, with a gold head curiously wrought in the form of the cap of liberty, I give to my friend, and the friend of mankind, General Washington. If it were a Sceptre, he has merited it and would become it. It was a present to me from that excellent woman, Madame de Forbach, the Dowager Duchess of Deux-Ponts, connected with some verses which should go with it. I give my gold watch to my son-in-law Richard Bache, and also the gold watch chain of the Thirteen United States, which I have not yet worn. My timepiece, that stands in my library, I give to my grandson, William Temple Franklin. I give him also my Chinese gong. To my dear old friend, Mrs. Mary Hewson, I give one of my silver tankards marked for her use during her life, and after her decease, I give it to her daughter Eliza. I give to her son, William Hewson, who is my godson, my new quarto Bible, and also the botanic description of the plants in the Emperor's garden at Vienna, in folio, with colored cuts. My picture, drawn by Martin, in 1767, I give to the Supreme Executive Council of Pennsylvania if they shall be pleased to do me the honor of accepting it and placing it in their chamber." TV and Politics
If we must have a national debate about political campaign finances, with laws being proposed by candidates for office, perhaps it is time to say a few things that politicians are forced to skirt. About 75% of the campaign finance money is spent on television advertising. The effect on television itself has not been mentioned. While the net revenues of television are simply astronomical, television news coverage is getting skimpier and skimpier. That's clearly not because they need to save money. It's because television is now in a position where it cannot afford to offend any politician by expressing opinions about current affairs. Both political parties in any local, state or national election have plenty of money to spend onTV advertising, and there is a significant risk to television revenue if they take any sides on any issue.
Meanwhile, television is one of the main factors in the decline of newspapers, who characteristically do take partisan sides. There can be lots of reasons why newspapers are more opinionated, but they have relatively little revenue to lose from political advertising, hence little to fear in the way of retaliation. But television has been stealing the advertising revenue of other sorts, forcing the newspapers to cut expenses. Between the two news sources, the effect has been to reduce the flow of news, one because it can't afford news, the other because it doesn't dare injure its golden goose. There once were forty newsmen assigned to cover Philadelphia City Hall. Now, there are five. What do you suppose that will do to the volume of corruption? Curiously, the effects extend in other strange directions. Television has jacked up its prices for advertising in the month of October to the point where a lot of advertisers are forced out of the market. October is just before Christmas, the main retail selling period. That can't be very good for Christmas sales volume. These things are beginning to attract attention from groups like the Committee of Seventy, who are starting a website of their own to fill the vacuum. There's been a lot of talk about internet blogs creating competition for the news. Maybe, the bloggers are just filling an unmet need. Retire LaterUnions teach their supporters: never retreat. Yell, shout, threaten, roll on the floor in simulated agony, denounce and declaim -- but never give back a single concession you have previously won. The hallmark of ratcheted positions about givebacks, is they are not negotiable.
By having some personal contact with union officials, who are generally decent enough fellows when not in their negotiating stance, I have learned that, to them, advancing the retirement age is absolutely not negotiable. Some of this intransigence is fake, having to do with negotiating traditions, and some of it has to do with the equally traditional stance that work is some dreadful thing which has been inflicted on the working man by unfeeling employers, or management, or the rich aristocracy or somebody. Reflex belligerence is therefore triggered immediately by suggesting that people are going to have to work more than they expected to. Much as I hate to offend people in their deeply held religious beliefs, I bring the news that retiring later would immediately solve the problem of affording to retire and that no other proposal under the sun has greater chance of solving that problem. But it's like the Law of Gravity. When dealing with demographics, to declare that something is off the table, or unacceptable, or a giveback -- is just bombast. With the present data, we are going to have to re-set the retirement age to 70. If medical and demographic trends are unexpectedly extreme, we may have to go to 75. If you think someone has promised you can retire at 55, you had better be in an iron lung or drinking your meals through a straw.
It's easy to see that later retirement cuts lifetime costs in two ways: it increases the duration of earning and saving. And it shortens the years of retirement payout. The later you retire, the better it is. So the less you save, and the more lavish your lifestyle, the older you will be when you can afford to retire. A lot of things can be debated, and a lot of clever ideas can be worked with. But it is going to take an atomic attack or something similar to modify this particular prediction about the future. And even doomsday predictions just make the future look worse, not better. Because as the insurance salesman tells you, you can have it one way or the other. You can die too soon or you can live too long. Since you can't know in advance which it will be, you would be wise to work a little longer, just in case. Starving the Beast of Early Retirement
Inflation-targeting, unless someone is keeping a big secret from us, is the only arrow in the quiver of a nation's central bank, in our case the Federal Reserve. A strong case that the Federal Reserve should acquire no other duties, rests on the fear that any new duty might conflict with holding inflation on target (at present, 2% per year). The recent adventure of the present Chairman, Ben Bernanke, into "Quantitative Easing" illustrates that diluting and confusing the role of the Federal Reserve will tempt the Executive Branch to poach on its independence. In this particular case, the adventure was the purchase of vast amounts of bad loans in order to remove them from the economy, never mind the future problem it will create of re-selling those loans to someone. Mr. Bernanke is lending credibility to the outcry of Representative Ron Paul (R, Tx) that the Federal Reserve should be abolished entirely.
Maintaining price stability (Inflation targeting) rests on Alan Greenspan's simplification of Milton Friedman's "monetary" theory that you can combat inflation or deflation by appropriate adjustments of interest rates and the money supply. Greenspan's further insight was that you needn't measure "monetary aggregates", you just have to measure inflation itself and react like a helmsman with a compass. Until 2008 it looked as though Greenspan had won the argument, by avoiding a deep recession for seventeen years, in the so-called "Great Quieting". Inherent in this helmsman theory is a deeper theory that all episodes of deflation (depression, recession, whatever) are merely over-reactions to inflation; avoid inflation and then forget about deflation. Still further behind this analysis is the observation that all governments at all times are pushing toward inflation, count that as an immutable law. The blunder of holding interest rates too low in 2001-3, for example, has been blamed as deliberately inflating in order to combat the Dot-Com crash of 2001 for political reasons; by this reasoning, the rescue of the DotCom dip led straight to the 2008 Subprime plunge. There is thus evidence that monetary effort by the Federal Reserve is powerful enough to control inflation, provided other branches of government abstain from political interference. In the long run, however, the Fed can only smooth out wobbles in the main trajectory. As Rogoff has shown, all crises whether of currency, banking, commodities or securities, are pretty much the same and caused by unwise borrowing. Avoiding inflation is enough to prevent a recession since government pressure to inflate can be counted on. Paul Volcker may have proved the issue in another way in 197_. During the Carter Administration, the country experienced "stagflation", we had inflation and unemployment at the same time. Improving one might seemingly make the other worse. But, dismissing the whole mess as inflation in disguise, Volcker promptly jacked up interest rates a great deal -- and both inflation and unemployment then went away. What seems proven is that stagflation is just a variant of inflation and should be treated by sharply raising interest rates. If inflation targeting is as powerful as that and as simple as that, what could go wrong? One present worry is that so much American money has fallen into foreign hands that the Federal Reserve could lose control. There is a second source of danger. Broadly speaking, this concern is that public opinion might demand inflation -- or policies which would surely cause it -- and in a democracy, the time might come when the Federal Reserve would have to give people what they demand. James Madison warned us about that. In a democracy, it's their country to ruin if they please.
New Jersey increased the number of state employees and their fringe benefits. As is so often the case, these state employees and their union became the core voting bloc for the party in power, usually Democrats. Not only are there a remarkable number of employees in each of the local offices for the Bureau of Motor Vehicles for example, but New Jersey included the local municipal and school employees (mainly police and school teachers) in the state health and pension system, a decidedly unusual step. These were not trivial costs. Longer life expectancy makes pensions and health care more expensive. Just how a ten-mile ambulance ride gets to cost $1700 is a related story, passed over here. And then, a few years ago it seemed like clever bookkeeping to float a bond issue to bring the state pension system up to full funding. Long term full funding tends to mean a stock portfolio, buying stocks with a bond issue is like buying stock on margin. By a stroke of timing, the booming dot-com stock market promptly crashed, taking New Jersey's margined stocks down even faster. In a sense, not only has the state raised the reimbursement of its workers, it has guaranteed them for life. New Jersey has always had high real estate taxes, now painfully high. But Jersey residents once could console themselves they had no sales tax and no income tax. Now, NJ sales and income taxes are nearly the highest in the country, and just about every other form of state taxation is at unsustainable levels. Doesn't matter, the state is running a $5 billion deficit and will run a greater deficit for as long as anyone can predict. Forbidden by the courts to borrow money, it's not easy to see what the Governor can do except raising taxes some more. Well, perhaps there is one thing if the unions will let him. He can extend the retirement age of state employees from the present age 55 to age 75. Having retired at age 81 I have little sympathy and have even written a long essay praising the joys of late retirement. But let's see him try to do that without anyone noticing. Cost-shifting Overview
Cost shifting has come to describe something evil, something to be eliminated. Perhaps it is not illegal, but the common view is that at least it represents "rent-seeking", an economist term for reaping unearned or undeserved profits, and getting away with it. This attitude must be revised; a modern healthcare system cannot function without a certain amount of cost-shifting. The funds to
Go to Delaware, Elephants?
No one is supposed to know where elephants go to die, but if they are smart as people say they are, my suggestion is to search for dead elephants in the state of Delaware. Most taxes, and estate taxes, in particular, are considerably lower, there. At least this was the message Christopher J. Topolewski, Esq. conveyed to the Right Angle Club recently. His firm, West Capital Management, has prepared a table comparing the taxes in the three states that come together at the southeast corner of Pennsylvania, which for residents of the Philadelphia area are within easy commuting distance of each other. Although Delaware has a marriage penalty (one couple is taxed more than the sum of two singles), it has no estate tax at all, no sales tax, and a property tax rate only half that of Pennsylvania, only a quarter of that in New Jersey. For residents of New Jersey, there is almost no tax which is not lower in Delaware, because but ex-Pennsylvanians would then have to be careful to die or cohabit since ordinary income tax and capital gains taxes are higher in Delaware than Pennsylvania. If you must die (and who doesn't?), go die in Delaware. This was a situation specifically contemplated as a way to discipline greedy state governments, by James Madison when he was formulating the U. S. Constitution. And there is evidence it is working. By happenstance, I once encountered an official of New Jersey taxation, who told me that 43% of New Jersey taxes are paid by 1% of the population. And that 1% was moving out of the state as fast as it could. If it does, the other 99% of New Jersey residents will find their taxes rising by 43%. West Capital reports that taxation as a percent of income is 1.23% in Delaware, 3.46% in Pennsylvania, and 5.82% in New Jersey, suggesting that a selective flight of the 1% would raise the state taxes of everyone else by 43%, and thus make state taxation as a percent of lowered average income rise to roughly 20%. Relating total income to total tax revenues would be an even better way to detect hidden indirect taxes, such as overtaxing utilities in the knowledge it will be passed on to the consumer. I recently discovered that a few years ago, the Legislature got tired of hearing complaints about local taxes, so they transferred half of the local taxes to the state tax. That's pretty much like taking it from one pocket and putting it into another because now all the hubbub is about state taxes. Armed with even partial information, it becomes easier to understand why New Jersey would evict a governor who had been Co-chairman of Goldman Sachs, during a financial crisis. If a financial whiz can't change this, maybe it requires a meat ax. This is a time of growing restlessness about public spending, and Tea Party revolts are likely to accelerate during the remaining nine months before the next election. The conjecture is growing about a coming deadlock between a Republican Congress and a Democratic President, lasting at least two more years. What might emerge from a strong third party congressional delegation is too arcane to discuss. But at least the Republicans who leave can console themselves they are selectively raising the taxes of Democrats. It seems almost inconceivable that professional politicians would demonstrate such a forest of tin ears as to let this happen, but the rest of Mr. Topolewski's talk just heated up the fire. His long-scheduled talk was designed to give guidance about the new estate tax laws, but he found himself confounding his audience with the news that there are no new estate tax laws; in fact, there will be no estate tax laws at all after this year unless they emerge from the congressional gridlock we already have. Which apparently will be followed by a gridlock we can scarcely imagine. Imagine asking your lawyer to write a will which straddles the contingencies that there will be no law, that there might be a continuation of the present one, or there might be some new law of quite uncertain wording. One of the suggestions offered is to allow your executor the discretion to accept or disclaim certain hypothetical provisions. And that brings up an old story. William Penn was the largest private landowner in the history of America, possibly the whole world. He had a trusted agent, who gave him an enormous pile of papers to sign. A busy rich man like Penn is regularly confronted with a discouragingly large number of routine legal documents to sign. So, Penn signed them all, not noticing that one of the various papers in the pile gave the entire state of Pennsylvania -- to his agent. The outcome of the ensuing uproar was that Penn spent six years in debtors prison. Widower's Friend
It was a large funeral service with probably a couple hundred attendees, held in the formal hall of his life's honored profession, its walls draped with portraits of officers in academic gowns, and men wearing beards. The hall had been built to impress visitors and it did, but those who served for decades as fellows and officers found it very homelike and intimate. He was eighty-sixing. Yes, eighty-six and a revered friend of every doctor now in the room. Death had been sudden and unexpected if that is possible for anyone eighty-sixes. A dozen or more attendees had greeted him heartily at the opera a week earlier, others had gone to dinners and meetings of volunteers for favorite nonprofit activities where he was a lively presence. He was comfortably fixed, could have gone on that way for decades, at least it once seemed so. He was a widower, well known to be keeping company with a widow who was also familiar to the crowd, as was her former husband who had been very well liked and respected. The two, widow and widower, had not remarried for whatever reason their circumstances demanded, possibly just reluctance to break formal ties with the past. The funeral arrangements, the caterer and all that fuss, had been taken over by his several adult children. The first sign, a small one, of the younger generation's inexperience and uncertainty entering into a new role as heads of a large family, was to be noticed in the obituary. Surely written by the undertaker and re-written by the newspaper editor, the facts were supplied by his children. Somewhere in this information chain, all mention was omitted that he had the affectionate companionship for several years of our other good friend the widow, who quite possibly had expressed a desire to remain in the background. These are all nice people; they want to do right, and certainly had no wish to hurt anyone's feelings. The attendees at funerals learn their role with practice. When there is nothing to say, they have mostly learned ways of saying something gracious. But little about that role teaches much about being in the other role, of conducting the services, being the host, setting the tone. Particularly in a secular service with no pastor trained in the ceremonial details, one can be thoroughly adult without knowing the rules. Not even knowing if there are any rules. Each of a half dozen particular friends and notables came to the front of the room to give eulogies they had time to prepare. The music was perfect. The reception was exquisite. The attendees were often old friends from the same social circle; if they created any missteps it was to express delight in seeing each other, then remembering why they were there, and dropping back in momentary confusion. Of course, our friend who had died would have sincerely wanted everyone to have a good time at his party. Perhaps that wasn't entirely a perfect answer, but we were all friends of many decades, and it didn't matter, did it. The caterer, sort of understanding the situations emerging in his trade, had addressed another issue by placing an empty serving stand, about four feet high where the widow/companion could stand by the door, greeting both her special friends and his. It was nice to have a place to put her pocketbook and her largely untouched drink and food. At first, this worked, but inevitably her group of friends entering the room ran out before he did, and his lifetime friends turned to chat with each other. In time, the large formal room was a cluster of his old friends, but with his formerly closest companion now standing uneasily alone at her position by the door, her pocketbook looking rather forlorn as the waiters quickly cleared other dishes away, with replacements declined. A glance across the room told what was on her mind; should she be the first to leave or the last? Momentarily she stayed on when a couple of young ladies stopped by to speak with her, and then the outcome suddenly became clear. If she stayed much longer she would be the only one there. She slipped out the door unnoticed and walked unsteadily down the long marble stairs. Alone, again. The Coming Baby Boomer Retirement Problem
In 2004, the Nobel Prize in economics was shared by Edward C. Prescott and Finn E. Kydland, for advancing the concept that business cycles are caused as much by what people expect to happen as by what actually does happen. By this reasoning, myriads of individual decisions are constantly made in the direction suggested by simple undeniable truths. What truths face us? Demographic facts related to how many people have already been born, and how fast they are dying, force everyone to acknowledge that both Social Security and Medicare are seriously underfunded. Consequently, it seems inescapable that the boomers must work longer and retire later. To whatever degree they don't, the country must go deeper into debt. Prescott, writing in the December, 2006 Wall Street Journal, stated this truism slightly differently to reach the next step: the national debt must increase. Increasing the national debt raises interest rates, which is good for savers. At the moment, the main savers are American retirees and foreign governments. However, the bond market is and always has been a zero-sum game. What's good for American retirees is bad for American business. And mortgage-holders. And everyone else who is in debt. Higher interest rates, which are seemingly inevitable, encourage saving and discourage borrowing. Prescott seemingly welcomes those features, because he is remarkably cheerful about the inevitable coming demographic crunch. There are at least two things about it which should be bothersome. The first is that the boomers will not be borrowing money from their own generation but from their children. Getting the chance to live longer than their parents, they seemingly want to retire at the same age or earlier, asking their children to pay for the unearned twenty-year vacation. Boomers simply must be shamed into later retirements. The American Gross Domestic Product has a long term growth rate of about 3% per year; 2% of that total comes from increased productivity, about 1% from population growth. Extending domestic working years has the same economic effect as, say, illegal immigration; it's good for the whole country to make this nativist substitution. The other disturbing consequence of borrowing our way out of debt is the effect on banks. That's harder to explain, but the interest rates we have been describing are long-term rates, established by the world marketplace. Short-term rates are independently set by the Federal Reserve to control (or "target") inflation, and currently they are higher than market-set long term rates. Any sensible saver will therefore use moneymarket funds rather than buy bonds. That's mostly bad for banks because their profit largely derives from "borrowing short and lending long". The so-called inverted yield curve, then, is good for old folks and bad for banks. If the Treasury fails to issue enough long term bond debt, or the Federal Reserve fails to issue enough short-term debt, banks are in danger of going broke. To summarize the whole puzzle, the government clearly will become more deeply indebted, but it must preserve a proper balance between short-term and long-term borrowing. Otherwise, either a bank crisis or inflation will sink us. As a guess, I would say that banks are the likeliest to fail. They are in precarious condition anyway because of wrenching changes in technology. And they are in the process of discrediting themselves by failing to pass along the currently soaring short-term rate bonanza to the public. Just compare your own money-market interest rate with the 5.25% which the Federal Reserve has dumped on the banking system, and see if your blood doesn't boil a little. If this pick-pocketing continues much longer, banks will be in a bad public relations position when they must come to the public with hat in hand. So, there's only one defensible response to this demographic retirement problem. The baby boomers, having been handed several years of unexpected longevity, must spend a portion of it working longer. Migrating to Retirement Villages
Institutions choose their locations for their own reasons, chief among which is cheap land, but the location near public transportation is another factor. They want to be near a source of employees but they also want to have cheap construction costs. Quite obviously, they are responding to cost pressures. Whatever the thought process underlying it, nursing homes and retirement villages usually get built in the far suburbs, often near the end of a public transportation route. A resulting problem is a vexing difficulty for a center-city hospital to find a nearby nursing home for convalescents. In time, suburbs grow up around these new institutions. A frequent consequence is a community of elderly people who need bus service to the doctor, surrounded by a community of young parents who must chauffeur their children to the doctor downtown. In typical American fashion, it eventually straightens itself out, but only after a lot of unnecessary inconvenience. What is proposed here is that ways be found to encourage doctors to establish their offices on the campus of retirement villages. Doctors certainly like the idea of being near a cluster of people who see doctors a lot, while old folks like the idea of putting on a bathrobe and walking to the doctor's office. It would be hard to entice surgeons to locate anywhere except close to the hospital where they operate, so the natural first movers would be internists, geriatricians, pediatricians. If enough of them locate somewhere, a laboratory, pharmacy, and an x-ray department are sure to follow quickly. That initial medical cluster would be enough to attract the local townspeople since there is almost always a surplus of parking space. The rehabilitation and physiotherapy units which are often already in place would get more activity, and the doctors would make rounds among their patients in a somewhat expanded infirmary. A regular jitney bus service would take people to one or more hospitals for surgery and major illnesses. In time, the center of medical care would move away from hospital office buildings, out into the suburban community. Acute care hospitals might not welcome the concept, but they would enjoy higher income from filling their beds with greater intensity of care, and the reduced costs of somewhat constraining their scope of service. Medical care would be more diffusely distributed within a metropolitan region, which is generally a good thing, and educational interaction with other doctors would grow, but in different locations. Almost all of these changes should tend to reduce costs and improve productivity. The simplest definition of the center of care is not the medical center but the location of primary physician offices and the most important step would be to discourage contractual links between referring physicians and a specific acute care hospital. Doctors left to themselves will locate offices where the patients are, and increasingly it is possible to see a shift of patients requiring chronic disease management and terminal care, into the retirement village. The tendency of doctors and laboratories to cluster around hospitals impedes this more natural shifting together. If doctors shift their offices and are allowed a choice, laboratories and x-rays will soon follow them. Before Medicare, the center of care was found near the high-rent districts of cities. In London it was Harley Street, in Philadelphia it was Spruce Street. As reimbursement changed, it shifted toward the hospital campus, where the parking problem is also solved. Nowadays, early discharge and reimbursement shifts have made it unattractive for a primary care physician to visit his patients in the hospital, so hospitalist and emergency room specialties are flourishing, with computerization feebly bridging interruptions to the continuity of care. The primary care physician would find the retirement village also solves the parking problem; pharmacies and laboratory pick-up are often already in place, and non-surgical specialists would soon follow primary care physicians. Patient transportation, at present crippled by expensive municipal monopolies, would be greatly eased by such shifts of medical interaction. Moreover, expanded infirmaries of retirement villages offer convenience and comfort near home. As for the effect on the retirement community itself, the most effective force elevating standards for nursing care, have no doubt of it, is the ease with which friends within the community drop in for visits. They have time for it, especially to and from the dining room, and all of them keep a watchful eye on how they would likely be treated there themselves when their turn comes. In retirement communities, client consensus is a powerful force. What is lacking is a willing sharing of reimbursement with acute care hospitals. Therefore, the idea of brief hospitalization followed by longer recovery near home is now only realistically available to the affluent. But the choices of those who can afford them show the way, as they always did before third-party insurance dominated the scene. For a while, little children may think it is funny to get their shots at the old folks home, but they will soon get over it. It's harder to say what the effect on teaching hospitals would be. No doubt an unfortunate amount of isolation already exists between town and gown, which the profession at large tends to blame on the Ivory Tower pulling up its skirts. But anyone who attends conferences at teaching hospitals would have to admit that attendance is already very sparse, sometimes no more than five graduate physicians in attendance out of a faculty member of several hundred. It is likely the main factor at work is an excessive workload, forcing doctors to sacrifice new knowledge for the sake of using somewhat older knowledge in every spare moment. Generally, continuing medical education has moved to several-day national conferences, out of town. The teaching may be better, but it is uncertain whether the learning is as good as it was when teaching was local and informal. The teachers at teaching hospitals may despair at losing what little audience they have, but they must look elsewhere for a cure. In any event, while Society has a legitimate interest in preserving the quality of care, it does not fulfill that duty by transferring it to reimbursement agencies. During wars, surgery is satisfactorily performed in tents, for an extreme example of how expendable much oversight can be. Another principle would be to ease impediments to overlaps of functions between institutions, particularly including the backward sharing of component services and records toward the lower-level institution. Since such sharing is often observed to occur without objection within vertically integrated institutions, there is every indication it is both desirable and feasible between competitors. And finally, if this shift of locale seems so desirable, why hasn't it happened already? Some of the answers to that are the prestige of associating with teaching hospitals, which is well deserved. Some of it is inertia and given enough time much of it will happen by itself. But to whatever extent it lies in archaic regulations, protected by those who see themselves as injured by competition, it needs some leadership to change it. And the likeliest bastions of power to resist such change without being noticed, reside in the habits and rules of third-party reimbursement. A Few Rooms of Your Own
If William Penn could revisit Philadelphia today, he would surely feel disappointed that the Greene Country Towne still hasn't materialized. Even a century after Penn's real visits, Philadelphia at the time of the Revolutionary War still nestled East of Fifth Street. There have been many conjectures about this, perhaps fear of Indian attack, perhaps lack of firewood, desire to be near the port, perhaps a number of things. Let's examine whether it's just the nature of a successful city to organize itself the way it does. Ancient Athens, for example, was a nice warm place without much rain, which possibly accounts for the miserable little hovels where people lived, contrasting with the magnificent Acropolis, Parthenon, Stoa and other public buildings. It has been speculated that the architecture created the social system, not the other way around; the same contrast between big stone temples and little wooden huts is also seen in the Mayan cities of Yucatan. Hong Kong certainly isn't poor, but it's built like that. Japan cannot claim that lack of land forces the citizens to live in tiny apartments. It's hard to say whether the lowly social state of Japanese women accounts for the contrast between where they live and where their husbands spend most of their time because it's just as easy to believe the proposed cause is really an effect. The more you look around the world, the more you wonder if it isn't the American suburb that's out of step with the world. When they can afford it, hardly any of the world seems to want to live in the suburbs; their homes are seldom their castles. There's New York City, of course. New Yorkers seem to like living in high-rises. An architect friend makes short work of construction economics as a driving feature. According to him, it is unduly expensive to live in a high-rise. Just a pointless ego trip. The cost per square foot of usable floor space just keeps going up as the building gets taller, requiring more elevator shafts, more elaborate HVAC. That's heating, ventilating and air conditioning. Everything has to be built with a derrick, the traffic congestion at the base is horrific, high winds can break the window glass. The list rapidly grows convincing. Why does anyone pay all that extra money to live high in the sky? Not my idea of something to do, says Cole Porter. Notice there is a major difference between sleeping in the suburbs as they do in Japan, and sleeping in apartments right near the center of town, as they do in Budapest, Berlin, Prague, and Vienna. The Orientals are staying close to work for longer hours, while the Central Europeans are staying close to the cafes and theaters to which they flock the moment work is over. Just what to think of the Spanish siesta system isn't clear, but it seems to have the main effect of bringing people back into the center of the town at night. You can't live very far away from work if you have to commute twice a day. The Lord only knows where everybody in New York is going every Friday night, with return traffic jams in the other direction on Sunday night. The weekly exodus suggests they don't really luxuriate in their penthouses or flock to their entertainment district on weekends; apparently, a cabin in the woods is beckoning. As, by contrast, the empty nesters in the suburbs eventually look around for retirement villages to live, repeating the endless complaint about the nuisance of maintaining a big house and garden. Pennsbury looks like a comfortable place to live, but even William Penn seems to have tired of it. One really does have to wonder whether a heart's desire in architecture all too frequently leads to heart's discontent in lifestyle. Philadelphia appears to be trying a new approach; the suburbs are moving back downtown. We'll eventually see if it changes our character and lifestyle so somebody can write sociology books about it. Front Stuff: Pearls on a String: Further Extending Health (and Retirement) Savings Accounts...Also by the same author: The Hospital That Ate Chicago, Saunders Press, 1980 Health Savings Accounts: Planning for Prosperity, Ross & Perry, Inc. 2015 Surmounting Health Costs to Retire: Health (and Retirement) Savings Account. 2016 Pearls on a String: Further Extending Health (and Retirement) Savings Accounts (This Volume), 2016 --------------------------------- Ross & Perry Book Publishers 3 South Haddon Avenue Haddonfield, New Jersey 08033 856-427-6135 ---------------------------------- Pearls on a String: Further Extending Health (and Retirement) Savings Accounts Copyright: ISBN #: (978-1-932080-56-8) -----------------------------------
Acknowledgements
For advice and support about the thrust of this much-revised book, I owe new debts to the many people who read the first versions and commented. The first book was written as ideas developed in my mind, and rather in a hurry. The second revision was written so later thoughts could be introduced earlier in the argument. This one was written and rewritten to rise above the twin possibilities that either, the Affordable Care Act would be completely repealed, or it would essentially survive forever. I still don't know its future, whether it is too big to fail, or too big to survive. Either way, I think it failed to reform some things which should be reformed. The best way to defend that position is to propose an alternative which is much simpler, but more radical. ----------------------------------------------------------------------
Foldback, Front CoverThis book outlines the hidden advantages of Health Savings Accounts, which the author had a hand in creating in 1981, along with John McClaughry of Vermont when John was Senior Policy Advisor in the Reagan White House. HSAs had more advantages than we realized. By turning them into retirement funds at the end, not a word was changed but they created a new incentive to save, by adding a new reason to save. By simplifying reimbursement, they exposed the ineffectiveness of third-party policing and saved money to be multiplied by investment. They were a vehicle for subsidies to the poor, a Christmas savings fund for the frugal, and interstate mobility for the rich. Finally, the idea dawned that such simplicity provided an avenue for a gradual transition to new programs, as well as an escape hatch if they failed. Beads on a string, as it were, with a common retirement fund at the end, as a universal incentive for savings in each program added. It might take fifty years to implement every step proposed. But then, it took fifty years to get into this situation. --------------------------------------------------------
Foldback, Back Cover
George Ross Fisher, MD, the author of this book, graduated from the Lawrenceville School in 1942, from Yale University in 1945, and from Columbia University, College of Physicians and Surgeons in 1948. After postgraduate training at Pennsylvania Hospital, Thomas Jefferson University, and the National Institutes of Health, he spent 60 years practicing medicine in Philadelphia and consulting in New Jersey and Delaware. During that time, he spent 25 years as a delegate to the American Medical Association, and as a trustee of a number of medical organizations. Following retirement, he formed a publishing company, Ross and Perry, Inc, which has published several hundred books, mostly reprints. He is personally the author of eleven books about Philadelphia history, from William Penn to Grace Kelly. He is the author of the following three books about medical economics: The Hospital That Ate Chicago; Health Savings Accounts: Planning for Prosperity; Surmounting Health Costs to Retire: Health (and Retirement) Savings Accounts and (the current volume.) ------------------------------------------------------------------------
Dedication PageTo Senator Bill Roth of Delaware, who demonstrated the road between private and public sectors, need not be a one-way street. ------------------------------------------------------------------------- Book cover back page, possibly in conjunction with above box and introduction, please discuss:
Health savings accountFrom Wikipedia, the free encyclopedia This article is about medical savings accounts in the United States. For international uses, see medical savings account. Health care in the United States ______________________________________________________ A health savings account (HSA) is tax-advantaged medical savings account available to taxpayers in the United States who are enrolled in a high-deductible health plan (HDHP).[1][2] The funds contributed to an account are not subject to federal income tax at the time of deposit. Unlike a flexible spending account (FSA), HSA funds roll over and accumulate year to year if they are not spent. HSAs are owned by the individual, which differentiates them from company-owned Health Reimbursement Arrangements (HRA) that are an alternate tax-deductible source of funds paired with either HDHPs or standard health plans. HSA funds may currently be used to pay for qualified medical expenses at any time without federal tax liability or penalty. Beginning in early 2011 over-the-counter medications cannot be paid with an HSA without a doctor's prescription.[3] Withdrawals for non-medical expenses are treated very similarly to those in an individual retirement account (IRA) in that they may provide tax advantages if taken after retirement age, and they incur penalties if taken earlier. The accounts are a component of consumer-driven health care. -------------------------------------------------------------------
All Right, Hippocrates. So What's the Basic Problem?
It took me a chapter to describe what went wrong with the Affordable Care Act. Five chapters to describe what should be done about it, in whole or in part. But the best final goal of it all, one which has the best chance of making medical care affordable, can be described in a few words. Until we decide where we want to go, we are unlikely to go there. and I simply can't believe that modification of health insurance is worthy of all this uproar. Health insurance executives may be forgiven for thinking so, but it is hard to imagine the rest of the nation has such priorities. Without stopping to argue that unprovable point, I offer what I believe is a self-evident, and better, goal. One paragraph more of history is needed.
Medical turmoil in its present form seems to have begun in the Progressive Era, sometimes called the Gilded Age, which briefly preceded and probably had something to do with, the First World War. It certainly involved President Teddy Roosevelt, who first proposed National Health Insurance, generating considerable appeal within the American Medical Association. After a brief flirtation, the Association then changed its position and has been more or less opposed ever since. At that time, the AMA turned its attention to the so-called Flexner Report of 1914, which advocated the physical and managerial relocation of medical education into the existing Universities. Out of this grew an unexpectedly vigorous medical research environment, responsible in time for the amazing transformation of medical care which characterized the 20th Century. This transformation which in turn probably generated the idea that Medical Schools were the natural center of the profession, a suggestion which greatly annoyed the AMA, triggering an unfortunate power struggle between medical school faculty and their practicing alumni. Since this battle divided those who were paid salaries from those whose income came from patient fees, parochial teaching issues were allowed to migrate into conflicts about how all doctors should be paid. From that the two groups soon split over the payment arrangements of health insurance, which also seeped out into questions of how all "health" care employees were to be paid, especially nurses, and thus who should manage them. In short, the subject material for a restructuring of medical payment wandered around for a century, getting further and further from resolution as new voices were heard, times changed, and the new arguments had little to do with the old ones. To summarize this century of argument in a few sentences leaves everyone confused about the topic, but certainly leaves no participant in a position to criticize the others. It is even possible to claim this bickering was good for the profession, because, for all the scolding, medical care has undeniably flourished in the meantime. I only picked up the trail, joining the profession during the Second World War. I was a practicing physician for fifteen years before Medicare made its appearance. My viewpoint may be narrow, but I have been at work in Medicine before, during, and after most of the major changes in the medical care of the last seventy years. To come to the present concluding point, I believe the American medical system actually does have its own unique plan already for the future of health care. Never mind what the rest of the world does; they never had the resources to do what comes naturally to Americans. It goes like this: We resolved without saying so, to pour tons of money, in amounts the Europeans cannot even imagine, into a medical system populated by the best students we could identify. This somewhat pampered priesthood has one main mission: eliminate the disease, and thereby eliminate the cost of disease for everyone, rich or poor, the world over. Some physicians are more idealistic than others, and there is some grumbling. But scarcely anyone dares to challenge the results, summarized by thirty years of increased life expectancy achieved in a single century. Arithmetic alone makes it impossible to repeat that performance. Sounds pretty grandiose, doesn't it? As to costs, how much do we spend, today, on polio, tuberculosis, rheumatic heart disease, and thirty other diseases I once spent my time with? And how little will we soon be spending on Hepatitis C and HIV? A lot, at first, but in ten years, probably very little. The great killers of my medical student days, like syphilis, subacute endocarditis, heart attacks, and strokes, are declining fast, so probably no more than a quarter of what they used to be. People have their gall bladders and appendices removed, but they don't even go to the operating room to do it. Improved longevity is taken for granted. Doesn't anyone want to live an extra thirty years? Doesn't everyone want his cataracts and knees replaced? The list goes on so long it is ineffective to recite it. We got our orders, and we delivered. No other nation on earth could even dream of such a project, and yet someone still occasionally challenges me with statistics about infant mortality in Luxembourg. Our inpatient psychiatry is a disgrace, yes I will give you that. But wipe out disease, that's the way to reduce health care costs for everyone. We're going to do it, and nobody else has a prayer of a chance. It is remarkable that costs keep rising while disease keeps disappearing, but even that trend must come to an end. Inevitably, there will be a reckoning of details.
It's probably fair to ask who told us to do such a thing. Everybody did, and nobody did. As much as anybody, my contemporary at the NIH, Jim Shannon exemplified this dream of the conquest of disease, and was in a position to do something about it. Maybe it was Vannevar Bush, who was the same sort of scientific evangelist. But somehow that search doesn't feel like the right one. What feels right is that the generation of Americans who conquered the armies of the world just pushed us onward to conquer a little thing like a disease. American exceptionalism did it, and right or wrong is going to get it done. It's true that I worry we will keep people on thirty-year vacations, which our grandchildren will take at the beginning of life instead of the end of it. It begins to sound as though Reverend Malthus may have been right about feeding all these people, and maybe there will be problems with employment. But that isn't our mission. We feel the nation wanted very badly for us to do what we did, and they are just going to have to whip up a generation of environmentalists, or sociologists, or banjo players -- if there are to be new directives. Passerby, go tell the Spartans: We lie here, forever obedient to their laws.
Since I am about to launch, in closing, a proposal for revising the goals of American health care, it seems appropriate to begin it by recalling a remark of one of my medical school teachers, delivered at the close of the Second World War. "The goals for medical research,' said this pathologist, "are relatively small. When we've found a cure for cancer and arteriosclerosis, we're about done." Since the current generation of students would regard anything known before 1945 as not worth knowing, and the treatment of cancer has not advanced much since the time of this prophecy, we had best be modest about what we already know. It is widely stated that fifty percent of drugs currently in use, was totally unknown only seven years ago. That may well be true and may continue to be true for centuries to come. The limits of knowledge for medical students were once defined in a study by Howard Becker called Boys in White and go as follows: First-year medical students are determined to learn it all. By sophomore year they have decided you can't possibly learn it all, so you only try to learn what is important. By Junior year even that seems impossible to learn, so you only try to learn what is going to be on the tests. Essentially what this says is that the faculty finally gets control of things by Junior year, and their selectivity defines the horizons of what students pay any attention to. This is a strangely limited selection of topics, which is finally set straight by the training directors of postgraduate Residency programs. Having played each of these roles in my time, I feel the residency directors have it about right, but only for inpatient care. Outpatient care is now the source of nearly half of hospital revenue, and the proportion is rapidly growing. The inpatient faculty reasserts control by writing the Board Examinations, and the final mixture is defined as the present state of medical knowledge, but it remains strangely neglectful of the outpatient half of medical care (notice, I did not say health care, which has become a rapidly growing world as non physicians assert control over funding sources). But even an assessment based on all these biases may still not be a good measure of where Society stands in its search for scientific progress. For one thing, we haven't been serious about science for very long. The first course in science, of any sort in any American university, was only offered at the time of the Civil War. Although I had already decided to enter the Medical Profession by the Second World War (eighty years later), I nevertheless chose a college major more suitable for a gentleman. English literature, now that was the thing. In a few elite colleges, it still is. A bachelor in engineering is a degree for people who invent things; a bachelor in science was for those who would discover things. But a bachelor in the Arts was a degree for someone who planned to run things. Until that witticism loses its bite, we haven't really become serious about how much we can depend on the average patient knowing what he needs to know, to assume cost-effective control of his health. Young women and mothers chatter about pediatric topics quite a lot, but for the rest of the population, the state of medical information remains what the physician priesthood understands and has the time to communicate. In 1945, the limits of medical knowledge were thus only two: how to cure cancer, and what to do about atherosclerosis. Today, we finally discover that sleep has a lot to do with the circulation of spinal fluid through the brain, which sounds about as advanced as Harvey's discovery of the circulation of blood in 1642. This year it became possible to see that protein synthesis is like a zipper in thousands of ribosome molecules inside zillions of cells inside you, me, Eucalyptus leaves, and dinosaur bones. Since cellular chemistry is pretty much protein chemistry, the potential for drug synthesis, to say nothing of understanding cell activities, is immense. I have had a reasonable acquaintance with a couple of dozen Nobel Prize winners, and mostly I don't know what they are talking about. The point is this: right now, it is practically impossible to know how much more there is to know, and therefore what discoveries are possible in the next twenty-five to fifty years. My pathology professor was obviously pitifully ignorant in 1945 about what lay ahead, and we haven't even cured cancer yet. How long it will take for a lot of billionaires to be created after they discovered a cure for something, isn't known and isn't knowable. But God bless them all, because the money they will save us in the cost of medical care, simply staggers the mind. Who will care about the cost of health insurance, when every disease the present generation of medical students will learn about, has disappeared? On the other hand, perhaps the scientific opportunities which are uncovered will trivialize the new pharmaceuticals of only seven years ago, which are half of the drugs presently in use. As long as the music keeps playing, we will have to keep dancing and hope for the best.
The Economic Consequences of the Health and Retirement Savings AccountJohn Maynard Keynes invented the science of macroeconomics after the First World War, and since then everybody seems to hate the subject. But after proposing a radical change in medical finance which involves eighteen percent of the gross domestic product, it is time to reflect on where it might go. Politically, a spread of Health Savings Accounts would make everybody an investor, and therefore more sympathetic toward investing. But the same idea was applied to affordable housing, and it caused a major economic crash in 2007, with real estate getting the worst of it. It taught us if there is a crash, it's hard to sell your house, so it's hard to move to a place where jobs are plentiful. So it follows if everyone is an investor, people will love you when the market is up, hate you when the market is down, but the worst part of it will probably be quite unexpected. For example, executives are clearly overpaid because the stockholders are too remote to have their vote matter. A spread to stock index investing might reawaken legislation to give the stockholders more power, or it might stimulate the German system of placing union members on the board of what is often a family-owned business. It's hard to know what to think about that outcome. My own prediction is increasing ownership by patients will act as a counterweight to drug and medical device prices, but will also restrain government regulation of those industries. The public wants low prices, but it will in time want higher profits in those companies. Perhaps some way can be devised to put those motives into balance for the benefit of all. The same conflict exists with health insurance companies and other corporate medical enterprises. And yet, with the quick passage of the McCarran Ferguson Act, the insurance companies emphatically endorsed state regulation over federal for insurance. Would the public be the pawn of big corporations, or would the reverse happen? Hard to say, so we might as well just watch to see.
Overfunding for RetirementIndependence Blue Cross (of Philadelphia) has imaginatively designed a Health Savings Account product for retirement purposes, by allowing the employer or the employee to overfund an HSA with $750 annual contributions, looking ahead to the employee's retirement. The HSA part is presented as an add-on to conventional Blue Cross, although it is unclear whether that is required. Independence Blue Cross should be given credit for a good idea. Whether it supplements health insurance before retirement, is apparently left up to the employee, but of course, it does supplement any other after-retirement arrangements the employee may have because the HSA continues on after Blue Cross itself terminates at age 66. Since employers may soon face an un-suspended requirement to provide health insurance meeting ACA requirements, the high deductible from the government plan might simultaneously supply the high-deductible requirement for the HSA. This seems an efficient way to address present uncertainties and could provide the basis for compromise discussions between the two political parties on the whole subject of fringe benefits. High-deductible is good; adding subsidies confuses the intent. Keep them separate.
Over-investment in Health Savings Accounts -- The Retirement Alternative. Because it's a new program, with financing uncertainties, we advise everyone with an HSA to consider overfunding it as a precaution. Just about everyone could readily use surpluses for some of his retirement. Although the employer only donates $750 per year, the law allows a total of $3350 as a maximum, and so a $2600 personal supplement is required in the following three hypothetical but typical situations. At this level, the employer contribution is a small factor; what really matters are inflation and interest return. And starting at an early age.Example One. Let's say an employee starts the program at age 21 and remains with the company until retiring at age 66, contributing $3350 per year to the HSA (in the Blue Cross plan, $750 comes from the employer, and the employee must supplement $2600 from personal funds). (It makes no difference whether the employee rises through promotions or remains at an entry level; the maximum is the same.) Result: the employee receives a taxable retirement income at age 66 from the HSA to IRA transfer of $81,616 per year until age 83, dropping to 66,642 with 3% inflation. If the life expectancy of 93 is anticipated, the yearly annuity drops to $65,621, dropping to 48,595 with inflation.. Example Two. Another employee enrolls at age 21 but retires to get married at age 26. At age 66, until death, there is a yearly $23,423 retirement income assuming a life expectancy of 83, and dropping to 19,125 with 3% inflation. Assuming 93, the annuity is $ 18,832 with and $ 13,946 without 3% inflation. Example Three. An employee joins the firm at age 61 and remains until age 66. His retirement income is $1,886 per year, dropping to $ 1,540 with inflation, Assuming expectancy of 93, he gets $1,516 yearly, or $1,123 after 3% inflation.
In the examples, many things jump out. The first is the large disparity between what five years of work will get you, starting at age 21, compared with the almost pitiful amount a person age 61 will get for the same absolute, and maximum allowable, contribution. The difference between examples is the difference between whole social classes. That difference, of course, is made up out of the income compounded internally for 40 years. And the moral is clear, a small steady investment at an early age is worth far more than the same investment at the end of working life. It happens to cost the employer the same, either way, and he may not realize it. His viewpoint will depend on what value he places on maturity and experience in an older employee, as compared with vigor and strength in a younger one; the pension costs would be the same. However, this is a major change in pension design, and people should familiarize themselves with it. The employer can make far more difference in an employee's life with the selection of savings plan, than with salary. Perhaps another way of looking at it is the employee gets to keep the interest compounding in an HSA, whereas in other plans the employer gets to keep it. Or, depending on how the contract is written, some middle-man gets to keep it. The old defined benefit plans placed much more emphasis on training and experience and much less on the age and duration of enrollment. It's a new ball game. For example, there is no reason why an employer couldn't have two plans, with an optional choice, one for young people, the other for latecomers. The second point revolves around the interest rate being paid. The investment manager, whether in-house or by way of a vendor, is able to earn and should be able to earn, 12% on an index fund of the common stock of the whole American market. Inflation at a steady rate of 3% for a century, reduces that return to 9%, net of inflation. How much is the employee entitled to? Much depends on whether inflation is pre-deducted in advance, or calculated at some later time. If an employee is paid less than 3% per year for his HSA, he actually loses money on the exchange. If he is paid 7.5% gross, he only receives 4% net of inflation, in spite of surrendering half of the net gain (4.5% of 9%) to the broker or manager. In this example we have arbitrarily assigned him 6.5%, which is 3.5% net of inflation, yielding well over half of the margin to the broker. I have to wonder whether the services provided are really worth more than 1% (for example, one nearby trillion dollar firm only charges a tenth as much), so it seems as though a fair return to the investor/subscriber should be 5%, net of inflation, net of fees, or 8% gross. So, be careful to identify whether inflation is anticipated, or only calculated after it happens. Sometimes, both approaches are adopted, and someone is seriously affected by not noticing it. That means the price debate ranges between 3% (no profit to the investor at all) and 8% (essentially the wholesale price). Throughout this book, I have generally adopted 6.5% as an average, mainly to be safely conservative and avoid arguments. The marketplace will eventually settle on the "right" price, but if it's less than 3.5% net of inflation, it's less than a quarter of the wholesale price. Eventually, I expect the price to be knocked up to 8%, net of inflation, or 11% gross. The ultimate effect of this price pressure on the cost of health care would be considerable, indeed. Sustainable retirement would come into sight, and as we have mentioned, the price of healthcare is linked to it. Now, I don't want to be accused of starting a revolution, but my calculator tells me if the passive investment could achieve 6.5% income return, the first of the three examples cited above would receive a retirement income of $81,616 per year. And the old fellow who decided to work for a few years to build up his retirement would receive $1,866. The youngster who worked for five years and then quit could look forward to a pension of $23,423 per year. Something tells me this is too destabilizing, so I'm not going to get impaled on the barricades discussing it. Ultimately, it probably reflects a reduction of transactional costs by electronics, which has not yet worked its way through to retail consumers. So, one way or another, something is going to happen, and it's up to all of us to make sure it is benevolent. Overfunding health insurance by one means or another is a very good idea if you can afford it -- and you keep your wits about you.
Overfunding for Retirement (2)We have begun the exploration of Health Savings Accounts, out to the edges of the potentials for the idea. Somewhat to our surprise, the idea has the potential for generating surpluses if carried out long enough, at a high enough interest rate. The immediate reaction is how to control this feature so that even if it all works out as anticipated, it does not wreck our rather fragile system of controlling the currency. The suggested technical solution lies in forcing the account to come nearer to a zero balance more frequently, a result rather easily accomplished by constraining the permissible balance transferred between existing programs, possibly even forcing it to zero. After a certain amount of experimentation, it should be possible to retain the compound interest feature for desired intervals, but imposing more zero balance constraints if it starts to get out of control. But there are other approaches. There is always the rather simple-minded approach of forbidding what you fear, imposing fines or the threat of imprisonment for violations. Any physician would recognize that approach as merely treating symptoms, rather than getting to the root of the matter. It would seem, if the desired outcome of a surplus is achieved, it would be better to suggest a different use than health care, rather than permit potential hustlers from diverting the surplus to their own purposes. The obvious need is to fund retirements with it. There is going to be a great need for assisting retirements if improvements in health care continue to lengthen life expectancy. Still, further down the road, there is even a limit to this need, but it seems better to let signs of it appear in future generations before we actually take steps toward constraining it in some foolish way In the meantime, the need to guard against the consequences of too little disease, death, and disability is just starting to appear, and it is huge. In the language of Congress, it makes its appearance as a deficit in the Social Security program which needs to be repaired in some way. When that need appears more imminent, it might be well to demand improvements in Social Security, or even its total replacement with a new program, rather than adopt the expedient of dipping into some other program with a? temporary? surplus. The South American approach of privatized Social Security investments was apparently bungled, but it might be re-examined for repair and revival. Much will depend on relative size; if living too long ever becomes a bigger problem than dying too soon, it would be a pity to allow the smaller program to dominate the larger one, because of tradition. It is probably not too soon to be thinking about these potential problems, but it may well be too soon to act on our plans.
New York Times: Splendid Idea for Old AgeThe New York Times devoted an entire issue of its Sunday News of the Week in Review on April 7, 2019, to variations of the theme that "Elderly People Have Surplus Spare Time." Although I have several personal connections with the editors of the Times by marriage, and other connections to the newspaper through Columbia's College of Physicians and Surgeons, I seldom agree with its New Yorkerish hunt for evil from greedy enemies. But this particular attack struck me as right on the mark. Sympathy with downtrodden unions has led to commercial forces preferring fragile cheap products needing to be replaced when broken, discouraging home repairing and the ultimately of the population's ability to repair. At the same time, a lot of old folks have time on their hands and limited opportunities to supplement their retirement income, even ultimately leading to the disappearance of the needed skills to make simple repairs. The Times doesn't suggest the two unfortunate curable ends of the Industrial Revolution could cancel each other out, but it seems to me they might fit if coaxed. Apple seems to be the biggest offender, substituting unnecessary cheap electrical connectors for successive versions of expensive machinery. When you need to replace a thousand-dollar computer for its broken ten-cent plastic connector, the commercial motive is obvious to the consumer, and pretty annoying, too. A broken plastic connector isn't worth its twenty-dollar markup, but the expensive computer would justify its connector markup, which ultimately becomes a one-dollar markup for a Chinese imitator. The situation in the computer industry was explained to me in person by Michael Dell. When he had his nineteenth birthday, his mother gave him an expensive IBM portable computer. He took it to his bedroom with a screwdriver and found that not a single component was actually manufactured by IBM. He wrote each individual manufacturer for prices and discovered he could make an imitation (but identical) computer, selling it profitably and ultimately driving IBM out of the portable computer business. Substituting Chinese names for Michael Dell you get quite a different story, which paints quite a different description, about excessive markups by greedy Americans. Nevertheless, the moral I draw is the ultimately self-defeating nature of excessive markups, for commercial unfair motives. Smaaart when you reveal them to friends, but unwise, in the long run. But buried in all this petty maneuvering is a solid truth. We once had a population which took woodshop in the seventh grade and metal shop in the eighth. for boys. And the girls were learning how to cook and sew in separate rooms. This system needs a little updating, but the point is that these abbreviated courses were adequate to teach the essentials of home repairing to whole generations of the population. You wouldn't need to buck the unions, who proved able to destroy the whole vocational school system of fresh competitors, in order to restore simple home repair to the whole population. The old retired folk could repair the broken plastic widgets in their simple lives. The ladies could cook a little instead of continuing plastic-wrapped dinners they now have more than enough time to play around with. Hardware stores would reappear to satisfy the need for widgets. And the retirees wouldn/t need to sit around for lack of simple things to do. It's a brilliant idea, even if it did come from the New York Times.
Another Proposal for Residents of Retirement Villages to ConsiderThere's a law against throwing old folks out of a nursing home or retirement community, just because they exhausted their assets and can't pay for further care. Responding to this demand, it is now customary to demand an up-front deposit. The deposit has many possible uses, but among them is re-align the interests of clients with those of the organization. The indigent resident will always have this asset available at death, to meet unpaid bills. Depending on prevailing interest rates, the front-end deposit will pay for six to twelve years of residence. That's not absolutely guaranteed to solve the problem, because everybody involved has also acquired an incentive to encumber this asset for other purposes. When the building of CCRC's finally meets or exceeds the demand for them, ways will probably have appeared to use the asset to promote marketing. For the present, however, everybody has this assured estate. When that is exhausted, almost all residents will still have an incentive to squirrel away some savings for a rainy day. By this, they probably have inflation in mind, and no one will deny the wisdom of inflation protection of some sort.
Meanwhile, consider a CCRC named Kearsley. Dr. Kearsley was a Tory in Philadelphia during the Revolutionary War; the rebels didn't treat him very well. However, in time he was pivotal in the creation of a home for indigents, associated with Christ Church and originally located on nearby Third Street. In time, the town grew and Kearsley was forced to look for more space, which turned out to be the farm of the Roberts family, located on City Line Avenue. To shorten the story, Kearsley eventually became a CCRC surrounded by the Bala Country Club golf course, mostly filled with indigent Episcopalian gentlewomen fallen on hard times. Its management was brisk and active, seeking charitable and government funds to make it possible to live there without personal assets. The chairman of the board set a challenge for Kearsley: I want this place to be every bit as good as the CCRC I am planning to enter, myself. Well, times change and sometimes it becomes quite a hustle to find the money to keep that promise. The center of Philadelphia has moved away from Christ Church, so the pool of charitable parishioners has dwindled. Nevertheless, here is a retirement village with an almost certain perpetual need for assistance, and a track record of management expertise in the fine points of government assistance programs. Without meaning to give offense to the development officers of every other retirement village in the nation, it seems likely that a think-tank which concentrated on this issue, located on the campus of a working model with a two-hundred-year track record, would enhance the efforts of every other CCRC trying to achieve the same objectives. For them to an affiliate in some manner with other CCRC's with many residents who have the same interests but more surplus funds, would seem to be fairly natural. The Whole Town as a Retirement CenterTHE automobile changed American living habits. A few suburbs had once organized around railroad commuting, and even earlier a few had organized around steamboat commuting. But universal auto ownership was what triggered wholesale flight to the suburbs, completely reorganizing metropolitan living patterns. As suburbs tumbled into neighboring farmland, they seemed to obey a rule that 30-minute commuting was normal. Extremes of regular two-hour commuting do exist, but they conflict with a second hidden rule of suburbs, that some adult must be available when the kids get out of school. A third rule is that most young families move from town to distant suburbs when the first child reaches fourth grade. The unspoken reason this is true is pretty obvious, and I had hoped the election of Barack Obama would focus the Presidential leadership on fixing the inner-city schools, as only a black President would be uniquely qualified to do. Instead, his focus was on reforming the medical system, where he was probably uniquely unqualified. Suburban parents eventually seek a different lifestyle when their last child graduates from high school. For American families attracted by the schools, automobile commuting makes suburbs attractive, while empty nests largely end that interest. And social unrest at school makes parents flee to the exits no matter where they live.
Although it takes one extra logical step to get there, this insight suggests suburban retirement patterns surprisingly might be changed by improving the inner-city school system. Upgrade the quality and safety of inner-city schools, the rush to the suburbs will slow down, and suburbs become less expensive places for elderly folks to live. That's because school taxes are now the most expensive component of suburban living. Two-earner families are also more likely to be three-car families when they have high school children, so driving would become easier for retirees without so much overconfident competition for the roads if we could find ways to reduce the concentration of high schools in suburbs. If suburbs become a more natural place for retirees to live, they become more natural places for retirement villages to locate, which is the main point of this article. The concentration of high schools in suburbs is a somewhat artificial response to urban disorders. My local suburban school system acquired a reputation for outstanding quality in a couple of decades. It did so by pouring money into the system, bragging about the schools somewhat unrealistically, usually stopping considerably short of demanding the academic rigor found in private boarding schools. The process was abetted by the local real estate industry, who shrewdly recognized that a popular product was high school glamor, not necessarily discipline and homework. This maneuver uncomfortably transformed a town which, fifty years earlier, found two thirds of the houses owned by families without children in public school. By contrast, just about every house in town today houses nearly two school children, and the school taxes have been driven uncomfortably high. Meanwhile, four or five neighboring suburbs actually developed shortages of children, two school districts even have closed. It seemed clear that families were moving into the "good school" suburb, willingly paying higher taxes while there were children to educate, but eventually moving back to low-tax neighboring suburbs when school quality no longer mattered to them. This recirculation was economically rational, although not necessarily the most efficient use of community resources. Retirees now have difficulty living in my town, because school taxes are prohibitively high for residents without children in school. Long-time residents regularly sell half-empty houses to newcomers with lots of kids, and then those old-timers move a mile or so away to a low-tax suburb, often into a house as large as the one they just left. Others respond to the situation by moving to a CCRC. Is this a rational way to make rather basic life decisions? Is a suburb dominated suburb by teen-agers really the best place to locate a retirement village? Is a locality created by universal automobile ownership a good place to put an age group with cataracts and slow muscle reflexes? So retirement villages are located in or nearby to suburbs because potential clents want to live there. The answer they usually give when asked is they want to retain the local medical system they had grown accustomed to. Since every one of them is covered by Medicare, that seems a strange answer, which more specifically means they want to keep the same cluster of doctors, pharmacies and hospitals they got accustomed to when their kids were in high school. They formed those habits at a stage in life when health care was a less dominant feature of their lives, so the connection is not strong. But they were young enough to experiment, and now they are old enough to quit experimenting. The politicians who continue to monkey with the payment system seem strangely unaware of this affiliation. Or the irritation these people will feel if they are coerced into changing. Among the various reasons given to move to a retirement community, a chief one advanced by many people is that it is cheaper. Alternatively moving back into the center of a neighboring city might be more suitable, substituting a richer cultural and educational environment for a monastic one. In either case, retirement moves imply making a new set of friends, not particularly easy for old people to do. Commuting is no longer a price retirees are willing to pay; hardly anyone without children is willing to commute. Safety from crime, and nearness to medical care beat cultural richness most of the time; sadly, even golf and bridge games usually beat culture, which is more a European ideal than an American one. Although most retirees have forgotten how to enjoy what a city has to offer, center-city life really seems like a more natural attraction for retirees. Although the soccer moms seem to be having a fairly good time at the PTA, teenage cultural dominance of suburbs warps the livability for almost everyone else. Even for teenagers, commuting seems a rather high price to pay for six or seven years of high school excitement, particularly if note is made of the disconsolate loneliness of most adolescents. Inner city schools should improve, dissuading many from moving to the suburbs in the first place; inner city crime and taxes should be controlled to entice a return of the empty-nesters. At the very least, the suburban merchants and real estate agents should be squelched for their constant bad mouthing of neighboring cities. The present sociology of suburbs is a rather fragile thing. If it becomes financially and socially possible for retirees to continue living in their lifetime homes, is it wise for them to do so? There is, first, the potential need for making financial provision for nursing, convalescent, or hospice care. Long-term care insurance aims at covering this need, but because these costs are high, the premiums for coverage are also high. It is difficult to know whether these prices are reasonable, because they must contain a margin of error against inflation, risk selection, and moral hazard. The technical insurance terms refer to the fact that the client almost certainly knows more about his impending health risks than the insurance company does, and secondly the mere existence of the insurance presents a temptation to use it. Someone living in the residential area of a retirement village surely has less temptation to move to its nursing facility than some other person still living in a house but potentially able to sell it and cash in his long term care insurance. There is also the danger lurking in the insurance that a client may get tired of paying premiums and drop the insurance shortly before needing it. Some types of insurance, notably term life insurance, actually pay claims to less than ten percent of clients; the rest drop the policies prematurely and receive no benefit. The tentative conclusion has to be reached that entering a CCRC is probably a better concept than buying long term care insurance, at least when both members of a marriage couple are comparatively healthy. Once the first one gets impaired or dies, the plight of the survivor definitely gets more precarious, without a volunteer caregiver or at least an in-house alert system. One thing is pretty clear. At the present time, almost everyone is strongly advised to get on the waiting list of some CCRC, without hesitating to consider whether that is a final best decision. The deposit is ordinarily rather small, typically around a thousand dollars (returnable if unused). It at least eliminates that dreadful situation of urgently requiring admission, only to find the waiting list is years long. Even paying a deposit on several of these facilities at once can be justified if children move around enough to make a specific choice hard to make. An estate lawyer who was my patient was on the waiting list of five CCRCs for many years before he made a final choice; in his profession, he had many opportunities to see the wisdom of this approach. A less advisable choice made by many people is to enter the community before they need to. Comparatively few of these CCRCs permit you to sell out and move elsewhere without a penalty. Nevertheless, why should you go, why should you disrupt your life this way? The answer seems to lie in the organization and its administration. When life choices are complex, unforeseeable and largely undesirable, and when your abilities may be slipping away, you may want some help without knowing it, or knowing where it get it. Maybe all you need is a new lawyer or tax accountant, or a different type of doctor, but have a little trouble telling a good one from a bad one. A tightly-knit little town can sometimes supply this service, but somehow it must be supplied. For that purpose, a Quaker organization in Philadelphia called Friends Lifecare at Home will manage an annual reassessment and call in the help necessary to remaining in your own home. It is a noble experiment, steadily growing in success. In a way, it supplies the function of the absent spouse, part caregiver, part watchman, and with a large Rolodex. Its main difficulties have come from Medicare, when seemingly capricious program changes change the assumptions in the yearly premium. Lifecare supplies service when Medicare doesn't; what happens when Medicare stops providing something? Lifecare helps you get a new doctor; what if the old doctor doesn't like that very much? The network of specialists and institutions may be just as important as the doctor, but the network changes when you change doctors. Many nursing care agencies refuse to allow their employees to have a key to the house, on advice of a lawyer who senses liability. Sometimes there is an emergency, no one can get in the door, and the fire department must be summoned to break in. There are problems with any arrangement, and there are problems with any alternative arrangement. This one works best when it is selected, not because it is cheaper, but because living at home is strongly preferred. There's an architectural problem. Most suburban houses are built for families with children. If you plan to live in that house as a frail old pensioner, you had better fix the stair problem. One-story houses are certainly best, and even one-story houses often have stairs at the front door. Installing a home elevator is often prohibitively expensive, but would not be at the time the house is built. Most of the cost of an elevator lies in the construction of a shaft which has not been anticipated. If an elevator is added to a new house, the shaft is little more than two matching closets on two floors. The cab and motor are surprisingly inexpensive, and need not be added when the house is built. It's the design of closet over closet that makes it inexpensively feasible; what house could not use two extra closets? There are a lot of less defensible requirements in most building codes. While you are at it, be sure the doorways are wide enough to admit a wheelchair, the toilet seats low enough to permit wheelchair use, at least one walk-in shower is available, and handlebars provided near the bathtubs. These are things to think about, before you break your hip. If you don't it may add many thousands of dollars of unwelcome expenses at a rehab center, nursing home, or whatever. And not only expense; your roommate in a semi-private room may enjoy raunchy television channels. There's also a local government problem, I'm afraid. The local volunteer ambulance service, often but not always run by the police or fire department, has its rules. If you are counting on this service to take you to a hospital or other medical service, you'd do well to check with them to see if they will take you to the place of your choice, if that ever becomes necessary. That's particularly true if you have enrolled in some "medical home" or home care service. If the local ambulance service won't take you there, you better know that in advance. If that's the case, don't argue with them. Either take effective political steps to get them to change their rules, or make other plans to get where you might want to go, at that unknown time in the future when you want to go there. If you live in a little town, drop in and visit with the Mayor or Commissioner, who might be unaware of your problem and easily able to fix it. If you live in a larger town, you may not be able to puzzle out where you could appeal. One easy way to work this particular system is to join the ambulance service as a volunteer, and make inquiries when you are on the inside. As a final last resort, if you live in a big city, go see the local ward leader who can fix things. Some of them will want money, but more likely they will only want your vote at the next election. If you are a member of a very large family, you will get more attention, because there are potentially lots of votes in your family. It's all rather sad, but the fact is that local politics usually control local ambulances, and their allowed destinations. A solution to the problem more directly available, is to talk with some of your neighbors who have cars. All that's needed except for unusual circumstances is transportation. You need not, and in fact usually should not, speed. Whenever I have put someone in an ambulance, my parting words to the driver are, "Don't go through any red lights!" Most of the cumbersome rules hampering ambulance use are imposed by insurance companies because of the high rate of accidents from those sirens and flashing red lights on the roof. If not insurance rules, it's lawyers, watchful for, or against, all the lawsuits which have been induced by Section 1983, a Reconstruction-era statute more recently reinterpreted to encourage citizens to sue local officials for just about anything at all, not just Jim Crow abuse. And finally, there's a neighbor problem. It was first illustrated to me by my own 90-year old mother, who found everybody in her address book had died, so she threw the book away. One day when she needed a plumber, she just dialed zero and asked for "central", which in this case amazingly called the local police, who took care of it. But don't count on being that lucky. Portable cell phones help a lot with the problem of summoning assistance, providing you know someone to call. In a suburb, a lot of people move away for various reasons, and eventually an elderly pensioner living there is marooned in a neighborhood of strangers, never mind living in the same house for seventy years. The television and the Internet can be a great comfort to a hermit, but when help is needed, some familiar name should be pasted to the refrigerator door. Meals on wheels are nice, but they don't come when your sink is plugged up. A friendly local plumber is nice, but he won't help if the roof leaks. Everybody builds up a local network of friends and vendors, but older people need to watch out that it doesn't get out of date. They badly need what many of them don't think they need, a circle of friends. The Segments of Lifetime Healthcare:
|






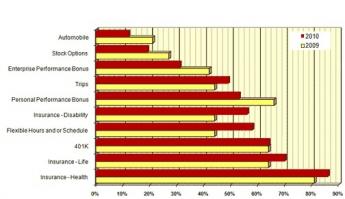









 We must assign a reasonable definition to a "decent" retirement, provide for a marginal one, and leave the rest to our own sources of wealth. 
|
Medicare As a Financial Issue. Medicare is about half paid-for, half borrowed, but it's really totally under water. According to Mrs. Sibelius, about half of Medicare expenditures are supported by the general fund or general taxation. The general fund is in deficit, however, providing some fairness to the description of Medicare as a fund borrowed from the Chinese, although China and Japan combined only purchase 13% of ten-year Treasury bonds. In the event of Medicare default, the main creditor victims will be U.S. citizens. The purchasers may change, but the deficit looks to be permanent. Until deficits are paid off, it will remain true that Medicare provides a dollar of care for fifty cents. That sounds wonderful until it suddenly sounds terrible. Medicare is bleeding money. If you want to know how brutal our government can get, read the section later on, about the Diagnosis Related Groups.First and Last Years of Life Re-Insurance By far the best proposal for refinancing Medicare, however, is to anticipate the way science is going to re-design costs. In the long, long, run, there should be very little medical cost left, except for the first and last years of life. We have no idea how long it will take, but that's the direction things are almost sure to be going.An accountant might say, Medicare's cash revenue is roughly divided between premiums paid by the beneficiaries, and pre-paid as a payroll tax of 3% on workers not yet old enough for benefits. (About half of this wage tax comes directly from the employee, another half from the employer. We skip over the technicalities that some parts of the program are tied to one fund, other parts to another, and also some are subject to higher income tax). About a quarter of Medicare is paid in advance on a "pay-as-you-go" basis, which is to say some people pay current costs of other people -- they are definitely not saved in anticipation of the contributors becoming beneficiaries, as the term "Trust Fund" implies.
About half of the Medicare deficit is paid as you go, about another half is borrowed; only a quarter of the budget is current revenue from the beneficiary age group.A second quarter is indeed paid and spent by current beneficiaries as Medicare premiums. That is, about half of the deficit is paying as you go, another half is borrowed from foreigners; only half of the deficit is matched by current revenue from the beneficiary age group. Nevertheless, the payers of pay-as-you-go are about thirty years younger than the spenders of it. If we put the youngsters' cash to work for thirty years, what interest rate would it take to grow one dollar into three? The answer is about five to seven percent. For quicker understanding, a few unfamiliar tools are needed:
So, phase in a restructuring of funding for both children and elderly first, and then add in the rest of a lifespan, step by step. That way, you first fund an obligation you are always sure to have. Be sure to do it in such a way that maximizes the investment income at compound interest. This might be a project under construction for decades, but its first step would be to begin funding for the Last Four Years of Life, which happens to be an early proposal in refinancing Medicare. Since the reader may be unprepared for the topic, it is considered in a free-standing way, in the next section.
Pay at the time, or pre-pay in advance?> At first, it might seem frugal to have people pay for what they spend; let them pay for what it costs, when you know who ran up the cost. But in the case of birth and death, it's going to be 100%, and the amount of it is a lottery. By far the more important issue is the compound interest you earn by paying in advance. Using the rule of thumb that money at 7% will double in ten years, a life expectancy of 90 should double 9 times from birth to death. That is, a dollar at birth is worth $512 at death.
What's more, 50% of Medicare is reported to be spent in the last four years of someone's life. That's likely to represent terminal care, but it doesn't matter. If you prepay those four years, the rest of Medicare has its cost cut in half. In those two simple statements is found the nut of paying for half of Medicare for $100 -- ninety years from now. It's up to actuaries and accountants to find the "sweet spot", of the most revenue enhancement for the shortest time of investment.
Plans for Healthcare Financing Retirement, Too
The preceding chapter seems like enough to say about the existing Health Savings Account. It should suffice for anyone who is stranded without health coverage, since it is already existing law, tested many times, and ready to go in a pinch. The handful of technical amendments are only about what you would expect from any fairly new program, and with any luck, they will slide through and suffice. The public, however, would be entitled to be disappointed with such thin gruel after so much hubbub, although repealing Obamacare outright would certainly make things more exciting. There has been an insufficient time in a lame duck session to render it effectively booby-trapped, but the pre-existing Obamacare law and its regulations are voluminous. After passing legislative actions to repeal it dozens of times, I have to assume the low-hanging fruit has already been picked by Congress. I would hate to see a relaxation of forwarding progress at the present stage; the resulting chaos would be considerable.
The J-Shaped Cost Curve. From a high altitude viewpoint, the healthcare of an average lifetime costs about $350,000 in the year 2000 dollars. It divides easily into roughly three thirty-year compartments: childhood up to age 25, employment from 25 to 65, and retirement from age 65 to death at age 84. Childhood is necessarily a gift from someone else, retirement costs are a gift of at least 50% from the government, and the lifetime operation is almost entirely funded by the working age group from 25 to 65 if you consider the government as being funded by the employed segment's taxes. Last year's NIH research budget was $33 billion, the Medicare budget was $55 billion.
This is quite a natural consequence of the way money is earned and spent in our society, but I consider it hazardous. Remember, the working segment (age 25-65) is not terribly sick. For a non-sick third to be supporting the sick two-thirds, is asking for a grievance to be expressed, and for somebody to be tossed out during economic upheaval. Let's put it another way: the people earning money aren't sick. The people who are sick may seem to have some money, but if they lose it, look out. The curve of health spending is said to be J-shaped: a childbirth expense and neonatal costs, then gradually increasing expenses clustered toward the end of life. Later on, we will discuss the proposal for First and Last Years of Life Reinsurance, which seems to me to match the future much better than what we now have.
Self-Funding, Rather Than Bulk Funding of Subsets. Furthermore, a long period of saving precedes a reasonably short period of spending. So a person's early saving would pay for later healthcare claims cost if we judiciously match savings with insurance. That's the Health Savings Account function, to which is added using surplus funds for retirement, by overfunding the premiums and keeping the invested surplus for later use. Somebody in 1965 made the serious blunder of overlooking the extended longevity provided by better healthcare. The awkward fact is retirement and Medicare begin at the same age, and retirement by some reckonings can cost five times as much. Retirement costs are continuous, while sickness comes in episodes. Further, saving for your own future needs will create an incentive to save; paying for whole classes of strangers creates an incentive to spend other people's money. Because when you create such a system, the money belongs to someone else. The newspapers report that health insurance averages 17% to pay its own costs, and the other 83% still goes to someone else. It isn't too hard to see where 30% of savings might come from.
To synthesize an example of a $5000 annual premium, 30% savings, for 40 years at 7% compound interest, would generate $13,600. At 6%, it would only generate $6800.
Competitive Institutions: Paying for Assisted Living
Around the turn of the 20th Century, it was the fashion to build specialty hospitals, devoted to a single disease like tuberculosis or polio, or one specialty like obstetrics or bones and joints. Eventually, it was realized that almost any disease is handled better if a full range of services is readily available to it. Around 1925, some inspired philanthropists made it possible to combine specialties within a medical center, and it is now generally agreed this is a better way when population density permits it. On the other hand, it is likely a source of price escalation. Time marches on, and the problems of excessive bigness are also beginning to predominate. The idea immediately occurs, to winnow out the routine cases which do not need so much technology, so that we can concentrate and devote high technology (and costs) to patients who will really benefit. And, immediately the perplexing outcry is heard that such rationalization is "cherry picking", which will soon bankrupt the finest institutions we can devise. The validity of such assertions needs to be examined impartially.At the same time, the horse and buggy era has been left behind, causing new separations along class lines, the flight to the suburbs, and the migration of philanthropy toward the exurban sprawl, as well as into urban centers. In all this commotion it was overlooked for a long time that medical care was not merely following the patients to new locations, it was becoming more of an outpatient occupation. Inpatient care was shrinking, and somehow expensive hospitals were swallowing their smaller (and less expensive) competitors. It wasn't a necessary development; Switzerland still favors small luxury "clinics" of ten or twenty beds, usually containing wealthy patients of a celebrity doctor. Local customs like this will change slowly. What America appears to need is more hospital competition and more ambulance competition; the two may actually be somewhat connected issues. For amusement, I once studied the patients in the Pennsylvania Hospital on July 4, 1776, when historical notables were congregating three blocks away. The diseases were remarkably similar to what is seen in hospitals today; problems with the legs, mental incapacity, major injuries, and terminal care. People are treated in hospitals because they can't care for themselves at home.
A BLUE-RIBBON COMMITTEE NEEDS TO STUDY INSTITUTIONAL COMPETITION IN HEALTHCARE.
This is a complicated issue and may take several years, or even several studies to sort out. What is useful for urban settings may be inappropriate in exurban ones; local preferences must be separated from special pleading, and that is not always easy. However, the continuing care center seems to be a permanent direction which is growing in popularity, as is also true of rehabilitation centers and retirement communities. Many of these institutions might incorporate doctors offices for their surrounding community, using the same parking facilities and many of the same medical specialties for both the neighborhood and the core facility. There seems no reason to oppose either rentals or private condominium-style ownership nor any reason to resist group clinics. Exclusive arrangements, however, are more questionable. All of these arrangements should be studied, and unexpected problems flushed out. No doubt the preliminary studies would lead to pilot and demonstration programs. And some practices which initially seem harmless, should in fact be prohibited. We have a lot to learn before we start overturning the existing order. But nevertheless, some arrangements will prove to be superior to others, almost all of them are regulated in some fashion, and the regulations should be examined, too. It should accelerate needed changes to know in advance which ones are ready to be tested, and tested before they are demanded.
*******
.jpg)
|
| CCRCs |
Everyone knows Americans are living thirty years longer because of improvements in health care, and some grumpy people are waiting with glee to see if Obamacare will put a stop to that sort of thing. It must be left to actuaries to tell us whether the nation saves money or not by delaying the inevitable costs of a terminal illness. But one consequence has already made its appearance: people are entering retirement villages in their eighties rather than their seventies. Presumably, people in their seventies are feeling too well to consider a CCRC, although other explanations are possible.
Accordingly, a great many CCRCs are seen to be building new wings dedicated to "assisted living". A cynic might surmise there must be some hidden insurance reimbursement advantages to doing so, but the CCRCs are surely responding to some kind of increased demand when they make multi-million dollar capital expenditures. Assisted living is a polite term for people with strokes or Alzheimers Disease, or some other condition making it hard to walk, or, as the grisly saying goes, perform the activities of daily living. One really elegant place in Delaware has suites with servants quarters, but for most people, the only affordable option is to be in a room designed around the idea of assisting an invalid. It's generally smaller and more austere but fitted out with railings and bars and special knobs. Meals generally have to be supplied by room service.
Not everyone is destined to have a protracted period of decline, but it's fairly frequent and universally feared, so it's a comfort to know your present residence is attached to a wing which provides for it. The question is how to pay for it. There are two main approaches currently in use, adapted to the limited financial resources of the aged and the particularities of CCRC arrangements.
In the first arrangement, there is no increased charge for moving to assisted living, which helps overcome resistance to going there. However, the monthly maintenance charge for others who remain behind in "ambulatory living" is increased, usually about 20%, to provide funding for those who eventually need special assistance. That's a financial pooling arrangement, sort of an insurance plan, and like all insurance, it has a tendency to increase usage unnecessarily. It also increases the cost to those who enter the CCRC at an earlier age, because they make more monthly payments before they use them. Although the monthly premium probably goes up as the costs rise with inflation, there may be some savings hidden in applying an earlier payment stream at a lower rate. That's called "present value" accounting, but like just about all accounting, its unspoken advantages and disadvantages contain a gamble on unknown future inflation.
In the other common financial arrangement, you pay as you go, when and only if you actually use the assisted living quarters. Because of the likely limit to resources, there is usually an attached agreement to garnishee the initial entrance deposit if available funds prove insufficient. The one thing which won't happen is being thrown out in the snow for non-payment; there's a law prohibiting that. Bigger apartments with large initial returnable deposits are of course better off paying list prices. Those with smaller apartments may have smaller deposits, and favor payment by a percent withdrawal. Some places haven't thought this through and offer no choice. In that case, more attention should be paid to those list prices and the percentage markup from audited cost. Better still is to have a free choice of both options, with cost transparency.
The remaining choice is between two CCRCs with differing options, made at the time you enter. The Obamacare fuss has made a lot of people acquainted with "adverse risk selection", which is largely based on the idea that an individual has a better idea of his health future than an institution does since that includes family history as well as earlier health experiences. But in general, a young healthy person is going to live longer without needing assisted living than an old geezer who going to need it pretty soon. A hidden adverse incentive is created for younger healthier people to set the choice aside, and come back in ten years, providing they remain alert to the underlying reason the monthly fee is then somewhat higher than in some competitive CCRC. At the far end of the age spectrum, an incentive is created to go into assisted living quarters a little earlier in life, generally regarded as an undesirable choice.
All this financial balancing act can seem pretty overwhelming to an elderly person who isn't entirely comfortable with the CCRC idea in the first place. Rest assured that everything has to be paid for somehow, and after you die you won't care what choice has been made. If you trust the institution to have your best interests in mind, the only consideration of real importance is whether your money will last you out. The institution cares about that even more than you do, so while they aren't likely to offer unrealistically bargain choices, they may offer a few which are too costly.
America has had a ninety-year romance with insurance because it is so comforting to be secure and oblivious to finances. This is just another example of the struggle between the search for a security, and the struggle to devise ways to pay for it. While no one can be positive about it, we're all in this together.
Playing The Cards As You Are Dealt Them

|
| Hand your Dealt |
A century ago it began to be usual to expect to earn a living for most of your life, certainly for most of your life after you finish school. But at the turn of the Twenty-first century, it is becoming more accurate to say that life is divided into thirds, one for school, one for work, and one for retirement. It seems hard to believe this trend can continue much further, with two-thirds of the population either in school or just loafing. Sooner or later there is surely going to be a revolution in the education industry, and a second one in the retirement entitlements of fairly healthy people who could be working but are not. At the moment, planning consists of devising strategies for coping with uncertainties about just where the boundaries will fall for individuals or couples; that's the topic on the table. But it is impossible to avoid mentioning that the largest unemployed labor pool is soon going to be the group from age 65 to age 85, and it is this group which is going to have to supply the unaffordable manpower required to care for a huge future population aged 85 to 105. At the other end of the working-years border, the education industry seems already starting to force the issue. College tuitions have been raised to approximately double their actual underlying cost, with the surplus internally redistributed as scholarships to more than half the students. That increases the pool of students able to afford college, but it only conceals for a few more years the recognition that we are graduating more students than the workforce can absorb, and must eventually stop doing it. After all, very few of our Founding Fathers went to college, while Benjamin Franklin the greatest overachiever of them all, only finished the second grade.
At the moment, however, the greatest opportunity for individuals to re-align their assets with their life expectancies, is to retire later or to go to college less, thus stretching out individual earning years by as much as ten percent. Our society could pour more money into medical research, but once we have achieved a cheap effective cure for cancer and Alzheimer's disease, the demand for research will soon experience a cooling of public enthusiasm. And individuals have the ability to make appreciable reductions in their living costs by re-defining what is a luxury and what is a necessity. This essay confines itself to planning the finances to match revenue to need, as currently defined by public opinion.
Let us assume a young person begins to work at an average age, accumulates as many after-tax assets and as much tax-sheltered retirement income as possible, retires at an average age, and lives for an average life expectancy. Since these times and amounts cannot be precisely predicted, they should be conservative. Thirty years of retirement is more than most people currently get, but may even be an underestimate of what the average person can expect. Thirty years of no earned income will require a nest-egg of two million dollars at retirement time if annual expenditures of $100,000 are expected. That's pretty generous, but half that amount is not certain to provide luxury living at $50,000 a year, and still requires a million-dollar nest egg. Cutting that in half a second time confronts people with $25,000 income based on half a million in savings. Most people cannot expect so many assets to accumulate, and most people would have a marginal existence on $25,000.
It simplifies planning somewhat to narrow the time-spans. If a person is within ten years of his life expectancy, he can probably safely spend every penny of his savings if there is some sort of insurance or cost averaging annuity for his age group. Above a certain asset level, this would take the form of an average terminal-years fund, plus a contingency fund. However, there would assuredly be hardship cases who cannot manage such a minimum and would require a subsidy. Estimating in advance just what proportion would require subsidy is difficult, but the magnitude essentially will determine whether this approach is feasible or not. If not, we would essentially be in the position of a third-world country, taxing the working population to pay for this subsidy, and thus crippling the economy. Long before this was tolerated, the education industry would have experienced some harsh treatment designed to force a larger proportion of students back into the workforce.
An Under-used Veterans Benefit
The U.S. Department of Veterans Affairs has has 56 regional offices in the United States and is one of the largest providers of medical care and insurance in the country. Robert Costantini from the Philadelphia office told the Right Angle members about one of the VA's programs which seems to be way under-used but which is readily available and has been for many years. It's called Aid and Attendance and can help a vet or his spouse meet assisted living or nursing home expenses. With rates for such care easily hitting $4500 to $6000 per month it doesn't take too much imagination to see that even well-off retirees could soon run through their savings. Luckily, a Pennsylvania law prevents nursing homes from removing a patient for lack of funds once they have been accepted.
Possibly one reason that the program is not tapped more frequently is that to be eligible a veteran's yearly income must be less than a certain threshold, currently just under $20,000 for a veteran alone and a bit more than $23,000 with one dependent. Although this is a relatively low amount many people who are unable to care for themselves could easily meet the criteria since non-reimbursed expenses for assisted living (both in a commercial facility and in-home help) and nursing home care can normally be deducted from the total income of a family. This, more often than not, will drop them way under the threshold and allow them to begin receiving the payments which can be as high as $2600 a month for a totally disabled person. The rates actually awarded are based on the percentage of the disability.
It's not unknown for government rules and regulations to be confusing and overwhelming for even the stoutest individual, but there is even help available to reduce the hassle burden on people in poor health. Keith Fishlinger of Estate Management Services of Schwenksville, PA, spoke along with Robert about the help his company can provide in this area. They know the rules and know who to contact and can provide all the bureaucratic navigation expertise to get the money flowing when it is due. Our own John White also provided some insight into a recent Pennsylvania law that required children to be held responsible for their parent's care expenses in certain cases so the Aid and Attendance benefits from the VA could conceivably benefit even them.
It would behoove most of us Right Anglers to become familiar with the VA programs since so many of us are veterans. It certainly won't hurt to get the word out to others, either, since the lawmaker in Harrisburg and elsewhere never seem to run out of ways to get as much of everyone's funds as they can.
Computerizing Medical Care
Note: This article was written in 1999, long before Computerized Medical Insurance Exchanges were such a disaster:
|
| First Computer |
My first encounter with a computer was in 1958, and I have loved them ever since. As president of what called itself the Delaware Valley Hospital Computing Society, I remember giving a dinner speech concluding as follows: "If you want to be happy for a day, get drunk. If you want to be happy for a week, get married. But if you want to be happy for a lifetime, get a computer!" After fifty years, my affection continues. But to be candid, billions of dollars about to be spent on computers in medical care will mostly be wasted. Even worse, like malpractice suits computers will induce behavioral changes in the system costing far more than the directly visible costs.
That's unpopular news at present since the National Business Coalition for Health has launched a major lobbying campaign to persuade Congress to spend an initial billion dollars inducing physicians to maintain an electronic medical record. Various health insurance companies already provide financial incentives to doctors to file electronic claims forms, eventually threatening to reject any claim submitted on paper. The American College of Physicians has established a rather large department to develop programs for physicians to use in their practices; twenty years ago the University of Indiana started much the same thing. The College of Physicians of Philadelphia has spent close to a million dollars on such a project. It is reported that Microsoft Corp. has a massive project underway to supply electronic medical records. It sounds fairly easy to obtain large research grants from the government to devise something, anything, useful in this area. In my own case, training funds really weren't necessary, since I eagerly got into the field when everybody was a beginner. I was just as good a beginner as any other beginner. But let me repeat: the electronic medical record has been in the past and will be for decades, an expensive digression. In health care, creating more administrative work isn't the solution, it is the problem.
For fifty years the problem with an electronic medical record was that it took too much of the doctor's time to complete his part of the input, and then cost him too much to pay employees to do the rest. Presumably, automatic voice recognition and dictation will soon make it possible to record doctor's notes without handwriting or typing. Since, however, the elimination of current paper forms and check-off boxes will create a major problem in organizing the dictation verbiage, it could add five or ten additional years before programmers manage to rearrange dictation material and effectively integrate it into organized form, complete with laboratory results, dictated x-ray and EKG reports, even small images of the original material. Temperature, blood pressure, weight, photographs and the like can all be readily integrated into the stored electronic record, but to do so usefully is an expensive programming project. Doctors are quite right to be anxious they will lose control of the usefulness of their records in order to ease the task of programmers, speed up the sluggish pace of development, and reduce what will surely be an unexpected cost overrun. Storage and retrieval of such records is known to be an achievable but expensive task, which however also risks sacrificing the speed and ease requirements of the medical task it is supposed to serve -- in the name of cost-effectiveness.
Computers are no longer an unfamiliar tool; physicians have altogether too much experience with "vaporware", unrealized promises of convenience, and the damaging effect on the medical quality of the philosophy of Quick and Dirty. To respond to their resistance to design blunders with an accusation of undue conservatism is to provoke an icy stare and gritted teeth. Inevitably, the effective use of automation will require a redesign of workflow with major disintermediation of "gopher" staff; after all, that is how cost savings are to be achieved. That will provoke outcry that physician time is the most expensive component in the process, but unfortunately, physicians will discover Information Specialists with a business background will brush that argument aside. The most overpaid people on the face of the earth are investment bankers, but information consultants have persuaded business executives that inefficiency of the investment process is more expensive than even an investment banker's time. Having been through this themselves, insurance executives are unlikely to pay the slightest attention to physicians dancing to a familiar old tune.
For all that, data input is not the real problem; it's just the first problem. It's in a class with data storage and retrieval, which is expensive and cumbersome when you add a need for instant access and total privacy. But costs will come down steadily, and eventually, we can expect automated fingerprints or other biological identification, and cheap instant retrieval. Doctors will be able to make rounds in the hospital with a computer in their pocket, record telephone calls in their entirety, dial automatically and whatnot. There are problems with wireless transmission inside buildings with steel girders, and legal requirements for signatures on narcotic orders, but if we are determined, these problems can be overcome as easily as they were with electronic check writing and stock brokerage. Cost may top twenty billion dollars in twenty years, but it all can be done if we insist.
But then you encounter the real problem. Information will accumulate in these records in staggering amounts. Even if you resolutely resist demands to have the nurses record every groan, and the orderlies file every laundry slip, the legitimately important medical information will be exposed as the massive heap of transients that they really are. Plaintiff lawyers will insist no scrap of data may be deleted, hospital administrators will insist on compliance, when in fact most of a doctor's concentrated effort is devoted to brushing aside momentarily distracting data in order to see what's going on and react to it instantly. When a quick look doesn't solve the problem, the doctor goes back for additional data. If you disrupt these skills and traditions of coping with information overload, evolved over centuries, you will at best impose frustrating delays on a complex system under pressure, and ultimately inspire elaborate systems of short-cuts. The Armed Forces are famous for paperwork, but even they know better than to ask a pilot for his Social Security number as he starts a bombing run. The hospital nursing profession has already just about collapsed under paperwork pressure. If you see five nurses in a hospital, three of them will be sitting down writing something. The terrible truth is that no one reads it, no one checks it, and ultimately it sits in the record room waiting for a plaintiff lawyer with unlimited time to sieve out some misrecorded misconception or uninformed conclusion. My faith in the computer is such that I feel sure that methods can be devised to produce periodic summaries, automatic alarm signals, and mostly effective prioritization of data elements. Unfortunately, medical care is changing at such a rapid rate that ad hoc automation of physician thought processes cannot keep up with the current pace of change in medical progress. You would think some things would be unthinkable, but since I can remember the organized campaign to suppress the CAT scan as an unnecessary expense, I confidently predict that programmer inability to keep up with some advance in medical care will at times lead to organized outcry that we should slow down the pace of improving medical care, so that computer clerks can keep up with it. But that is only a small part of the issue, which at its center is that physician time will be dissipated and his attention distracted by presenting him with unwieldy amounts of neatly printed, spell-checked, encrypted and de-encrypted, biometrically secure, hierarchically prioritized -- avalanches of data which are irrelevant to the issues of the moment. The goal is not, after all, an electronic record. The local goal is to decrease the cost of medical care by increasing the productivity of the physician, and the overarching goal is high-quality patient care at a reasonable price. Behind all that, since the impetus comes from NBCOH -- the ones paying the insurance premiums -- suggests that the local goal is not so much the improvement of care as oversight reassurance that cares provided has been as good and as cheap as possible. The goal is legitimate, but this cybernation approach looks to be self-defeating by being overly specific.
If the reader has the patience for it, let me now cite a historical example of the third-party tail wagging the medical dog. In this case, third-party health insurance similarly overextended its reach by imposing internal health system changes, trying to facilitate the role of monitoring it externally. Specifically, the system of diagnostic code numbers was changed from one devised by the medical profession for its purposes, into a different coding system devised outside medial profession sponsorship, which seemed to suit the needs of payment agencies better even though it suited medical purposes less. After twenty-five years, it is now clear that third-party payers have shot themselves in the foot on this matter, and everyone is worse off. The topic, please pardon the obscurity, is the diagnostic coding system.
To go back to beginnings, the American Medical Association perceived a need for a diagnostic coding system in the 1920s. Organizing or even merely indexing vast amounts of information about a disease required more specificity than freestyle verbal nomenclature could provide. Quite a distinguished panel of specialists and consultants then produced the Standard Nomenclature of Diseases (SNODO) which in time became the Standard Nomenclature of Diseases and Operations. In order to reduce ambiguity, this system developed a branching-tree code design for anatomy, linked to a branching-tree for causes of disease, ultimately linkable to a branching tree of procedures. These three sets of three-digit codes linked the components together with hyphens (000-000-000). The first digit of each was the most general, as in Digestive, Musculo-skeletal, etc. and subsequent digits were progressively more specific and detailed, as in "Digestive, large intestine, sigmoid colon". The causes of disease would resemble "Infections, bacterial, streptococcal". An example of Procedures would be "Incision, incision, and drainage, drainage and insertion of the drain". In nine digits, it was thus possible to represent " incision, drainage, and insertion of a drain into a streptococcal infection of the sigmoid colon". After a while, the codes grew from three to five and six digits, again repeated three times, so an immensely detailed, unambiguous description might be coded in fifteen digits by a physician who knew the rules but didn't own a codebook. This code was ultimately taken over by the Academy of Pathology, expanded and is called SNAP. The pathologists absolutely refused to give it up.
The rest of the profession gradually yielded to the pressure of hospital administration, who was pressured by the Association of Medical Record Librarians, responding to the views of outside statistical interests, particularly insurance. A simpler, shorter coding system was needed, they felt, concentrating on the thousand most common diseases. The International Classification of Diseases was produced, reducing the millions of SNODO diagnoses to 999 by heavy use of several varieties of "Miscellaneous" or "Not Otherwise Classifiable (NOC)". Since the goal was to count the incidence of common diseases, the coding system was stripped of any logical tree-branching and became a short list of what was most common, starting with 1 and going to 999. In time, of course, the common-ness of conditions changed, and various complaints from various directions forced the ICD to go to 4 digits, then five. Unanticipated conditions or complications eventually required the patchwork of some alpha "modifiers", and the original short hodge-podge became a long and bewildering hodge-podge. Coding accuracy declined markedly, but ho-hum. The health insurance companies paid the bill, no matter what the code said. At another place, we will discuss the entertaining way that Ross Perot became a billionaire out of the computer chaos of Blue Cross and Medicare at this time, but right now the central theme to follow is DRG, Diagnosis Related Groups. Try to follow, please.
By 1980, Medicare was fifteen years old. It was clear that certain things just had to be changed because the excuse that the system was new and untried was beginning to wear thin. The early designers of the system based their payments on auditing a hospital's yearly costs, auditing the proportion of patients who were Medicare beneficiaries, and paying a proportionate share. That was easy and reasonably accurate, but it had a rather significant flaw that it took no account of whether the patients needed to be in the hospital in the first place. Or whether they needed to stay so long. The response they adopted (in the Budget Reconciliation Act of 1983) is a measure of just how desperate they must have felt. Knowing full well how inaccurate the ICD coding system was in practice, it was all there was. Consultants, particularly at Yale, ran computer simulations of various subsets of ICD codes to find a formula that would produce approximately the same hospital payments as the system of cost reimbursement. If memory serves, the original formula was to divide the thousand ICD codes into 27 diagnosis-related groups (DRG). Eventually, the process was tweaked to seventy or eighty groups. Walter McNerny, then Past President of the American Hospital Association told Congress hospitals could live with this system, and promptly we had a system for paying out hundreds of millions of dollars. It was touted as a highly sophisticated advance in the arcane science of hospital reimbursement, so it must have included a lot of deliberate overpayment. I can remember trying to remonstrate with McNerny, who felt he didn't have time for the discussion. Physicians had very little to do with the DRG portion of the 1983 Medicare Amendments because the AMA had long insisted that physicians and hospitals go their separate ways on reimbursement. Russell Roth, who was president of the AMA at the time, recounted many times the episode in the Oval Office, when it was announced to Lyndon Johnson that Dwight D. Eisenhower"was in the next room waiting for him. LBJ excused himself to leave, and on the way out said to Wilbur Cohen, "Give him anything he wants." Things were destined to change, but at least for a very long time, physician and hospital reimbursements were strictly independent.
Rejecting Preventive Health Care for Good Reason
WHILE we debated in 2010 whether to disregard what could be afforded, and provide sickness care to all, the idea subtly changed to providing "health care" for all. That is, the proposal was not merely to expand sickness care to everyone, it included an indefinite expansion of what everyone would get, and who would provide it. Medical care is provided by physicians, sickness care is provided by doctors, nurses, and hospitals, and healthcare is provided by a much larger undefined group of "providers". No wonder it costs more, and therefore a surprising number of people are unsure they do want all of it. It's almost a certainty that most people do not want to lose control of this definition, at least if it is to apply to them, personally. The issue centers on "healthcare" versus sickness care". How's that, again?
|
Preventive Health Care poses unique issues for seniors.
|
| Dr. Fisher |
For example, the notion that preventing disease is superior to treating disease, goes back at least to Benjamin Franklin. Arguing that the Pennsylvania Legislature ought to help build the nation's first hospital, Franklin offered the truism that it saves money in the long run to treat people early and get them back to work. Franklin could hardly have foreseen that it isn't always true. Preventive medicine implies it is cheaper to spend small amounts, possibly every year, for many people, than to spend large amounts for a few. It's a matter of arithmetic, of course, and doesn't always have the same answer. When the math works against a preventive approach, it's usually argued the gain in health is worth it; but that's not invariably the case, either. Once a person ceases to be an infant, the equation rebalances. And as an individual approaches end of life, his renunciation of what it takes to prolong life gathers more respect. It's a conflicted opinion, of course. Older people are outraged by any suggestion their lives do not deserve to be prolonged, but still, outspokenly prefer to die rather than wear a colostomy bag, or a respirator, or be fed with a spoon. If they are Jehovah's Witnesses and refuse transfusions, that too, commands more respect when they are elderly. This is a familiar problem, not a new one. What's new is more subtle and pervasive.
The public probably does not fully appreciate the disappearance of what might be called capricious diseases, caused by the operation of chance, or God's will. These are fatal illnesses like heart attacks, strokes, epidemics, and other things not anyone's fault. Except for cancer and Alzheimer's Disease, most really common serious illnesses which remain, are to some extent self-inflicted. Smoking causes lung cancer, alcoholism causes accidents and homicides as well as cirrhosis of the liver, taking recreational drugs damages lives, unprotected sex causes HIV. Obesity causes hypertension and diabetes, neglecting your medicine undermines treatment. If this keeps up, we are going to see the day when every obituary will seem too shameful to print. Poor Jud is dead; it's his own fault.
It's maybe even worse than that.The 2000-page Obama care plan was too complicated for even the Congressional committees to understand. But the public was not hostile for technical reasons, the public was irked at the idea. All the President's celebration of saving money through mandatory preventive care provoked the public to tell him, Get off my back. Almost every smoker has tried at least once to quit, absolutely every obese person has repeatedly tried to lose weight unsuccessfully. It's hard, let's see you try it. And now it goes beyond nagging, we are going to take the position that every person with a self-inflicted disease is costing the nation money we can't afford. The country has a right to punish people who drive us to bankruptcy. Let's have some Wellness police, and fair but firm punishments. Is that really what Obama has in mind? Well, sir, you just get off my back.
Even so compliant and dutiful a person as my late wife declared that when she got to be seventy, she was going to try marijuana. The fact that she actually lived thirteen years longer without doing it, did not change her basic attitude. When you get to a certain age, many of the old rules don't apply to you, doggone it.
Stretching Out Dwindling Assets (1)

|
| Dwindling Assets |
Only a few insurance companies have adopted the idea, but after some searching for it, a company may be found offering an option to transform life insurance into a guaranteed annuity, paying approximately 6% guaranteed for life. The rest of the companies are uncomfortable with offering guarantees which extend more than a fixed number of years, leaving the subscriber with the risk of guessing how well that matches his life expectancy. Since elderly folks near the end of life have no prospect of ever acquiring new funds after their savings run out, the idea may be widely admired, but it has not had much implementation.
Retirement Communities
Prior to the Second World War, old-age homes were almshouses, slightly modernized. Since few people lived very long after they retired, the old-age home took care of a few stranded old folks unable to care for themselves. The places were depressing and sparse, with a characteristic odor of urine and poorly-ventilated kitchens. But when time spent in retirement lengthened to twenty or more years, a new dynamic had to be considered. The dingy old single rooms changed into multi-room apartments, the dining room went upscale, and the infirmary changed into a skilled nursing facility. The idea was, you could graduate to more specialized medical care when you needed it, and be visited by your friends in the community who would someday be in the nursing facility themselves. They were paying to keep it up, and they would raise a ruckus if the infirmary service began to look uninviting. Whether the community was paying for it collectively or the younger generation was supporting it, the Retirement Village provided a more civilized way to grow old and die.
|
THe CCRC falls somewhere between a college dormitory and a resort hotel.
|
People chose these places for a variety of reasons, depending in large part on what they could afford. Widows are often overwhelmed by maintaining a house, widowers are often overwhelmed by cooking. And retired couples are often simply tired of both chores, or sufficiently crippled or befuddled enough to look for a way to give those tasks to younger people. One system grew up, of acquiring a second home in a vacation area and then replacing the main house with an apartment in a retirement community. If you stay in the vacation home for six months and one day each year, certain combinations can lead to appreciable tax savings. Sometimes a married couple is in perfect health and uses a retirement community as a comfortable suburban apartment complex, "just going on living the way we always did". The idea in their mind is the folk wisdom that you need to get used to a place and develop a circle of friends there; to do that, you ought to be less than eighty years old. When that's a general idea, it can be self-defeating to join a group of friends with pooled meal tickets. Thirty friends, or fifteen couples, can each host a party for thirty, once or twice a month. Unfortunately, they are quickly sequestered and disliked by everyone else as they make the regular rounds of nightly parties; but this sort of thing happens in upscale places, the kind of retirement community where some apartments have servants' quarters, and nobody much cares what anything costs. For people in this circle, the most detestable thing about a retirement community is the pressure to have dinner at 5 PM. Early dinner is ordinarily the surest sign the place is managed primarily for the convenience of the employees, but it can also mean there is nothing else to do except watch prime-time television.
|
| Retirement Funds |
For most people, however, even having ample funds for retirement is constrained by the uncertainty of how long the retirement will have to be, how much must be held in reserve, even at age 100. The gallows humor continues to repeat some version of trying to plan a way to spend your last dollar on the last day of your life. It isn't just how long you will live, it is how. If you or your spouse become blind, or bedfast, or in chronic pain, your level of living is going to change and your daily expenses may rise dramatically. Even if you never gave such gloomy things a moment's thought, the experience of eating in the same dining room with several hundred elderly acquaintances soon teaches all the lessons of unexpected illnesses and weekly funerals. Some people cannot bear the idea of living in such a community, for precisely the reason that it becomes impossible to kid yourself. And one thing no one can kid himself about is the reality that you have to have one awful lot of money before you can ignore the need to watch your pennies. And it isn't just your spending money; it's also the lack of a basement, attic, and garage in which to expand or from which to draw reserves, or just to enjoy old books and mementos buried in dust.
Retirement communities seem to have developed independently in the Quaker suburbs of Philadelphia, and along the California coast. Except for the climate, there isn't much difference. More tennis in California, more trips to the theater on the East Coast. The early communities had a strong focus on finances, which assumed a lifetime retirement fund derived from selling the family home. The fancier the house, the more elaborate the apartment it would finance. As the duration of retirement grows progressively longer, roughly three years every decade, it is certain that the sale value of the average American family home will get progressively stretched to extend to the average age at death -- especially if you focus on the average age of the second of a couple to die, or become blind, or become bedfast.

|
| CCRC, Continuing Care Retirement Community) |
So, the patterns of financing are changing, at least experimentally. Some retirement communities (the term is are purely rental, partly room and board, extra charge for the nursing facility, or a la carte for all services. People who enter any sort of community are often planning to move to a different one after a period of time, either to adjust to their reduced physical capacities or changes of location of their families. Some of them actually say they plan to live luxuriously and then move into their children's houses when the money runs out, although it is usually hard to know how seriously to take such comments.
Obviously, what is needed is some sort of insurance mechanism to pool everybody's risks, but there is a fundamental problem. Insurance companies make a big profit on life insurance in two ways: either from clients who drop the policy before they cash it in or from premiums which underestimate the actual age of death compared with the average experience at the time the policy was taken out. But in the retirement case, essentially all policies mature at death and the duration for compounded investment is brief. So such insurance is either overpriced or unobtainable. The same underlying phenomenon affects Medicare and explains its impending insolvency. Those early retirement communities which based their charges on the assumption that Medicare would continue unchanged are repeatedly stranded when Congress cuts back on Medicare benefits. Someday, demographic trends will level off and insurance can be restored to practicality, but that time is certainly two or more decades away. Many states, including Pennsylvania, have passed laws that residents of retirement communities may not be evicted if they become impoverished, so the communities are forced to be strict about advance funding. Ultimately, the danger is that the community will be forced out of business, stranding the occupants. With so much time available to discuss such matters in a common dining hall, occupants of these facilities can become obsessed with the need to save for the future, and no one can be certain they are wrong about it.
Retirement Communities (CCRC)
Let's confess my meager authority to generalize about trends in retiree convalescence. When I graduated from medical school in 1948, average American longevity was twelve or fifteen years shorter than today, and most assumptions rested on it's remaining the same forever. Someone who reached eighty was really old, obviously facing a prompt decline. Today, essentially everybody lives to be eighty. We only half-expect such long life, which is modest of us, and only halfway plan for it, which is foolish.
|
Picking the right CCRC is as hard as picking the right spouse.
|
In 1950 a general practitioner in Haddonfield, NJ called for help from the son of one of his patients. The son was a doctor on the staff of the Pennsylvania Hospital, where I was finishing my internship. The GP hadn't had a vacation for twenty years and wondered if one of the graduating internets might take his practice for a month. I volunteered and then learned about retirement in a prosperous suburb. My employer had many tasks, among them a schedule of ten or twenty monthly house calls. There may have been some male patients on those rounds, but all I remember were old ladies living on the third floors of big old houses. I wasn't expected to do very much when I visited, at least by Emergency Room standards in the hospital. The families with whom the grandmothers were living wanted to be reassured that nothing was neglected. They also wanted to form their own assessment whether the doctor really knew them, and would come immediately if needed.

|
| Doctor House Call |
My next insight came a few months later when another doctor on the staff of the hospital had a heart attack; the Chief of Medicine gave me the time off to take care of this practice while the doctor recovered. When I first arrived at the door of the brick Philadelphia row-house where the doctor had his office, I was met by his nurse already wearing a raincoat, handing me an umbrella. We visited ten or fifteen other row houses along the neighboring streets, where to my amazement I found patients with oxygen tents and intravenous infusions. If the patients needed blood tests or electrocardiograms, the nurse arranged for them to be performed at home. Drugs by injection were administered, hospital-like bedside charts were maintained. This was a working-class neighborhood substitute for hospital care, but I was astonished to see how adequate it was. By this time, we had many resident physicians at the hospital who had seen service in the war and returned for specialty training; they regaled us at the lunch table about treating major illnesses -- in a tent. This wasn't the Civil War we were talking about, it was 1950.
Fifteen or twenty years later, my personal situation had improved; Medicare had arrived in 1965, but I was in practice as a center-city specialist and hardly noticed the new insurance system. But I did have three patients who insisted on being treated at home, which even by then had become an unusual arrangement. All three lived in condominium apartments in buildings with dining rooms on the main floor which would send up take-out dinners. All three patients had live-in nurses and hospital beds rented from an agency. One spinster lady absolutely refused to be treated in a hospital, because the Queen of England set up a little hospital in her palace when she needed it, and this lady said for practical purposes she had as much money as the Queen. Because she was dying of cancer, I resisted this idea, but if you had seen Katherine Hepburn in The Philadelphia Story you got the helpless feeling this dame was going to have her way. We called in laboratory and x-ray services as needed, administered injections, maintained a hospital chart. In this case, when I made a house call, her chauffeur would pick me up and deliver me, helping to ensure my promptness. Her lawyer and I kept careful financial records of the experience, which was new to him, too. After she died, we totaled it up and discovered with astonishment that the whole thing had been cheaper, a lot cheaper, than going to the hospital. Since she left a sum to the hospital in her will, even the hospital was pleased.
Well, nowadays there are more than fifty retirement communities scattered around the periphery of Philadelphia, many or most of them sponsored by Quakers. It's a national movement, and there are people in California who feel they had the idea first. There are now enough of these organizations to permit some classification of them into types, which mostly follows the sort of community model they resemble. There are some that look and are run like college dormitories, some that resemble convalescent homes, some are very like big-city apartment condos, and some behave like resort hotels. One of them, the Kearsley, sits in the middle of the Bala golf course, attempting to provide the first-class service to indigents by using existing government assistance programs, but has lately had to fall back on the Episcopal Church for financial help.

|
| CCRC |
Since a financial shadow hangs over all of them, it should be mentioned first. Every person in a retirement village is eligible for Medicare and Social Security, and with the help of a social worker can fall back on less-known assistance programs. It's impossible to ignore the existence of these funds, but most unwise to depend on them. As the age and number of retirees constantly grow, state and federal governments are starting to draw back from initial generosity. Laws have passed that a CCRC resident may not be evicted for non-payment of debts, so the institutions have had to impose conditions which guarantee them payment from new entrants in the case of later inability to pay. The risk remains that clients who entered before the rules were imposed, can only be extricated by going before Congress and raising a piteous cry on bended knee. Such laws and embarrassments vary from state to state, and from year to year, but unstable finances destabilize any business. When the customers all depend on their savings, and average investment experience is a drop of 30-50% in the past couple of years, no one escapes anxiety.
Although there must be college courses in how to administer a CCRC by now, current administrators are drawn from the environment the place mostly resembles, so the resemblance gets stronger. The former manager of a country club tends to neglect the infirmary; the former directress of a convalescent home doesn't notice institutional food. If the administrator treats customers as complaining nuisances, you get one kind of war; if the board of directors is accustomed to ruling corporations by dictate, you get another. Mainly, these institutions differ from models of other institutions by the degree to which they have active volunteers in charge. The inmates may run the asylum, but only if they become useful volunteers. A curious distinction evolves between those CCRCs which emerge from college alumni associations and those which are sponsored by churches. University faculties are not accustomed to, nor generally sympathetic with, teamwork. Every faculty member is on his own career path, which he hopes leads straight upward; teamwork to them is a code term used by business executives to imply blind obedience, Charge of the Light Brigade, or worse. Church groups, on the other hand, prize volunteerism. In a church environment, the proposal that Let's Have a Picnic is supposed to be met with a chorus of Great, I'll be Glad to Bake a Cake. Church-sponsored CCRCs, therefore, are generally more adaptive to innovation in a formless society. University groups have camaraderie and complaining, but little follow-through. By contrast, business people know what you are supposed to do, you are supposed to make something happen. Church volunteers want to know how they can help. Paradoxically for that reason, the more evidence of golf clubs around the place, the more likely it is to be innovative.
Let's return to the point, succinctly. Life-threatening and potentially convalescence-requiring medical conditions are destined to segment increasingly into Medicare, to the point where what remains outside of Medicare is elective, preventive or outpatient. Obstetrics is an exception, remaining more naturally part of the hospital than the CCRC. The rest of medical care thus seems inclined to migrate toward the suburban ring of retirement communities. The more natural transportation flow is for younger people to travel to either a hospital-centered medical cluster or a CCRC-centered cluster, not for frail old folks to leave the convalescent environment except for major surgeries from which they soon return to their infirmary. It doesn't have to be that way, it just seems like the natural arrangement.
Probably the main reason it doesn't work that way today resides in the Medicare law. The 1983 amendments restrained inpatient reimbursement much more than outpatient care or home nursing care, and consequently, inpatient costs have risen 18% in five years, compared with 47% for outpatient. Outpatient care is not migrating toward retirement communities because hospitals need revenue. Somehow, it seems easier to modify these reimbursement rules than to upend suburban CCRCs and relocate them next door to an urban hospital. If the payment rules become reasonable, the system will readjust its geography in a reasonable way, without coaxing.
Surely, non-residents of the CCRCs are destined to wish to convalesce in the spare beds of CCRC infirmaries which should then treat younger people as a much-needed revenue source; any licensing requirements which block this seem unreasonable. Medical hardware,-- x-rays, MRIs and the like,-- is most naturally concentrated in the periphery of CCRCs, as are pharmacies, outpatient labs, doctors' offices. That's going to require a lot of parking space. It's a good thing this will take a couple of decades to happen; many mid-course adjustments will be imperative. But the basic fact is that the whole community's medical need is getting concentrated in CCRCs via Medicare, and so the community's facilities should move closer to that need. The younger community is well able to travel anywhere for elective medical services, especially when they move away. Makes a good chance to visit the grandparents while they are there, too.
All of these proposals depend on getting the attention and cooperation of other self-centered institutions: Medicare, hospitals, medical societies, municipal governments. The CCRC community has scant experience with asserting itself; its future will depend on how skillfully it begins to do so.
Nearly every retirement village has four or five retired physicians living in the place, as well as a dozen retired nurses, lab technicians, and others with medical experience. Every CCRC infirmary has four or five patients whose spouse is a resident of the community, visiting the infirmary regularly, and with sharpened insight. Some other people are natural leaders. If these people could be assembled into a permanent committee of medical oversight, charged with visiting other CCRCs in the region for ideas and perfecting the interface between the CCRC and nearby hospitals, medical facilities, transportation vendors, and politicians -- things would start to move. Spending twenty percent of our gross domestic product on health is, quite enough. Let's either stop spending so much or else make something good of it.
Health Savings Accounts
The legislation removes the hampering restrictions of the 1995 Law. What follows is a brief outline of the main features of the HSA/MSA clause in the 2003 law,

|
| U.S. Capital |
as published by the main authorizing committee, the House of Representatives, Committee on Ways and Means. From this point forward, more specifics of the program will probably be written by the Executive Branch and published in the Federal Register. The Ways and Means Committee will continue to exercise oversight authority, however, in conjunction with the Senate Finance Committee. As a consequence, statutory modifications of the program are likely to appear in future annual budget reconciliation acts, or else in any new Medicare amendments. The legislative route map becomes more understandable when it is recalled that Medicare itself is considered to be an amendment (Title XVIII) of the Social Security Act.
Committee on Ways and Means
Medicare Prescription Drugs, Improvement And Modernization Act of 2003
Health Savings Accounts (HSA's)
Lifetime savings for Health Care
Working under the age of 65 can accumulate tax-free savings for lifetime health can needs if they have qualified health plans.
A qualified health plan has a minimum deductible of $1,000 with $5,000 cap on out-of-pocket expenses for self-only policies. These amounts are doubled for family policies.
Preventive care services are not subject to the deductible.
Individuals can make pre-tax contributions of up to 100% of the health plan deductibles. The maximum annual contributions are $2,600 for individuals with self-only policies and $5,150 for families (indexed annually for inflation).
Pre-tax contributions can be made by individuals, their employers, and family members.
Individuals age 55-65 can make additional pre-tax "catch up" contributions of up to $1,000 annually (phased in).
Tax-free distributions are allowed for health care needs covered by the insurance policy. Tax-free distributions can also be made for the continuation coverage required by Federal law (i.e., COBRA), health insurance for the unemployed, and long-term care insurance.
The individual owns the account. The savings follow the individual from job to job and into retirement.
HSA savings can be drawn down to pay for retiree health care once an individuals reach Medicare eligibility age.
Catch-up contributions during peak savings years allow individuals to build a nest egg to pay for retiree health needs. Catch-up contributions allow a married couple to save an additional $2,000 annually (once fully phased in if both spouses are at least 55.
Tax-free distributions can be used to pay for retiree health insurance (with no minimum deductible requirements), Medicare expenses, prescriptions drugs, and long-term care services, among other retiree health care expenses.
Upon death, HSA ownership may be transferred to the spouse on a tax-free basis.
Contain rising medical costs- HSA's will encourage individuals to buy health plans that better suit their needs so that insurance kicks in only when it is truly needed. Moreover, individuals will make cost-conscious decisions if they are spending their own money rather than someone else's.
Tax-free asset accumulation- Contributions are pre-tax, earnings are tax-free, and distributions are tax-free if used to pay for qualified, medical expenses.
Portability- Assets belong to the individual; they can be carried from job to job and into retirement.
Benefits for Medicare beneficiaries- HSA's can be used during retirement to pay for retiree health care, Medicare expenses, and prescription drugs. HSA's will provide the most benefits to seniors who are unlikely to have employer-provided health care during retirement. During their peak saving years, individuals can make pre-tax catch-up contributions.
Chairman Bill Thomas Committee on Ways and Means 11/19/2003 12:56 PM
Amending HSAs To Include Tax Sheltering

|
| Bill Archer |
There is nothing the matter with Bill Archer's law to enable Health Savings Accounts, except one thing: it forbids payment of health insurance premiums via the Accounts. Probably, that provision was a necessary compromise, to get the bill passed. But just imagine what would happen if it were amended to permit such payments: money legitimately passing through the accounts gets an income tax deduction.

|
| Henry J Kaiser |
Anybody can start an HSA, so with a small amendment, anyone could get an income tax deduction for health insurance, by writing a check from the Account to pay the premium on his present health insurance, or even just notifying his bank's Bill-Pay to do it automatically. By this simple maneuver, everyone would be eligible for the Henry Kaiser tax exemption now limited to employer-paid insurance. This simple change would eliminate a festering sore of unequal treatment under the law which has been allowed to persist for eighty years. Except possibly for those who don't want a tax exemption or don't want to take the trouble to use the HSA. It's hard to imagine anyone taking that attitude, so a powerful incentive to create HSAs would leap into place. As we have said in many places, if the tax cost of the universal exemption to the government is an objection, it could easily be paid for by lowering the exemption for employer-based insurance. The number with the exemption at present so greatly outnumbers the population excluded from it, that the reduction in tax exemption making it equal is surely less than 25%. It will nevertheless be resisted, not because of the small tax cost, but because the present inequality drives people toward employer basing. Even employers would not lose much because all the business competitors would be treated equally. The main resistance would come from insurance companies which specialize in the weird forms of health insurance specially designed to adjust to existing law. Perhaps they should be compensated for their loss, although that sort of thing is seldom done in our system of government. Rather, they would be expected to accommodate the new rules of business or go out of the business. That's traditional, and it is traditional for their stockholders to insist that they resist it, leading to the eternal struggles of "creative destruction," which is universally praised as an ornament of our culture, except when it applies to yourself.
Conversely, insurance companies which provide Health Savings Accounts will flourish with new customers, so existing health insurance companies are urged to add a new form of business and prosper. Any change of the rules requires time to re-adjust, so there will be room for both kinds of health insurance, for a long transition period, perhaps permanently. Let a hundred flowers bloom. In fact, all of the current plans being offered under Obamacare contain deductibles of at least $6000, so the designers of that Act have grasped the right idea, which includes tacit phasing out co-payments. A copayment of 20% is well demonstrated not to be enough to influence patient behavior, and a copayment of 50% is seen by the public as no insurance at all. Copayment has always been a way of making the premium cost appear smaller than it really is, and it's very simple to calculate in a bargaining negotiation. A twenty percent copayment reduces the premium by twenty percent, and that's about all there is to it. Total costs are largely unaffected, except they trigger the invention of another layer of insurance to cover them.

|
| Obamacare |
It presently is difficult to know how many people will have health insurance after Obamacare settles down, and how much it will cost. But the Wall Street Journal reports that all of the plans being offered by the Insurance Exchanges have at least $6000 deductibles, and the various approved insurance plans cost between $187 and $590 a month. The Obama administration seems to have grasped the idea that paying small claims with three layers of insurance is a pretty expensive way to pay your bills. Therefore, it is possible to imagine an agreement between the Democratic Senate and the Republican House of Representatives, for reasons of cost, alone. Later in this book, we propose that all small claims by everyone be paid out of Health Savings Accounts, and all hospital claims are paid by diagnosis since the bedfast patient has no opportunity to bargain in the marketplace. Getting the hospitals to charge everyone the same, is an entirely different issue. The concern about such a rule is that it may contain an incentive to perform elective surgery as an inpatient when a vast number of small surgeries are adequately managed as less expensive outpatient procedures. Special accommodating adjustments such as patient discounts will probably prove necessary to prevent such an unwise migration of the locus of care. Indeed, the small but irritating local monopolies of ambulances may need to be addressed, as well, since a patient may be well enough to recover at home, but not well enough to drive himself home.
For the moment, let's not get down into the weeds of this thing. Let's just pass it, and immediately.
Increased Potential for Retirement Villages

|
| Pennsylvania Hospital, Nation's First Hospital, 1751 |
Healthcare institutions may well have mission statements, but the main force visibly shaping hospital mission is third-party reimbursement. One must be sympathetic with institutions which really prefer their own mission to the pressures from third parties, particularly when the "second party" -- the patient -- also likes the original mission better. Teaching hospitals surely would prefer to concentrate on streamlining tertiary care, retirement villages on enriching the lives of elderly residents, etc. And they could probably make a better case for what they prefer than third-parties can. When one-size-fits-all health insurance is imposed on institutions which must survive by internal cost shifting therefore, insurance mandates invisibly prevail. It is not always strictly a matter of "Who pays the piper calls the tune", as it is "Who pays the most can run the place."
Considering these invisible forces of control at work, it seems highly desirable to search for situations in which the incentives of the third-party do not run parallel to the incentives of the provider community. In the case of government third-parties, the goals of the agency may not even be parallel to the will of Congress. The public clearly prefers to pay for private rooms and private duty nurses if it can afford to, but those are mainly relics of the past. Doctors used to work out of offices in their homes, but you seldom see that, now. There once were twenty hospitals in Philadelphia which were owned, paid for and operated by churches, but now at most, the church name is a relic on the front door surviving from a former era. If these changes were a response to public preference it would be another thing, but they are usually not even traceable to a written mandate which might be appealed. So it becomes all the harder to defy a mandate which grew out of the hospital's surmise as to what the third party would probably prefer. Perhaps some examples of social pressures at work would be useful.
It happens my own first office experience was in the home of an older doctor on vacation. The location of that family residence was a careful triangulation of convenience, expense, distance to the hospital, and the preferences of the patients. It was a grand experience to put aside the breakfast coffee, walk into the next room, and see the first patient of the day. Or to interrupt office hours for an emergency in the neighborhood for less than an hour and to have your excuses readily accepted by the waiting patients upon return. My colleagues had explained the financial advantages of sharing a roof and heating system with a tax-deductible business. But my accountant explained that the Internal Revenue Service didn't like offices in the house, and would surely audit any doctor silly if he persisted. So I spent fifty years in an office across the street from the hospital, commuting and seeing patients who had to commute to see me; the extra expenses of parking and the rest of that arrangement are easy to imagine. True, it was easier to visit the hospital patients, and nice to eat lunch with other doctors in the hospital cafeteria. But all of these decisions were not my own first choice. I never got a letter from the IRS or heard a murmur from them, but I always believed I was responding to their mandate. When an IRS agent finally wandered into my office as a patient, he admitted the IRS prejudice but said he believed it grew out of fear the business expenses reported would really be the expenses of a hobby, not a business.
A second relevant experience occurred when I was a resident physician. A staff physician at the hospital had a heart attack, and the Chief of Medicine asked me to take a few days off to tend to the problems in the stricken doctor's practice. His home and office were in the midst of a row-house district of town. When I arrived, the office was empty of patients, but the nurse was waiting with an umbrella. "Before we see the office patients, we must make rounds to see the bedridden patients at home." To my amazement, within a three-block radius of his office, there were nearly twenty patients in hospital beds at home. Some of them had oxygen tents, several of them had intravenous fluids dripping into their arms. The nurse told me that she drew blood for pickup by a laboratory and that with a little argument a portable x-ray machine could be brought to the home. At the foot of each bed was a hospital chart, all up-to-date with notes and reports. It might not be possible to run such a show in many other neighborhoods, but the city row house neighborhood was ideal. Or, not ideal perhaps, because there must have been many problems. But it was clear why Blue Cross had slow progress making sales to the people accustomed to this arrangement. And it even made clear why patients were content with open twenty-bed wards in a hospital, for at least ten years after Medicare would have gladly paid for a semi-private room. No private duty nurses, however, it might set an unwise example.
Two things are at work, here. Things happen to medical care which is undesirable, so someone needs to complain about them, and complainers must be provided with a place to appeal. The reverse is also true; good things which ought to happen, don't happen. So in addition to providing an appeals system, we somehow have to provide a wise and unbiased ombudsman to suggest what new initiatives ought to be undertaken. And the two functions, negative and positive, need to commune with each other. Parenthetically, since everybody gets involved in health care to some degree, adversary roles must be filled in this process, containing representatives of patients and also providers (both institutional and individual), as well as guardians of the purse. Since the process quickly becomes unwieldy, it needs to be associated with a special committee of Congress and needs to be able to summon both witnesses and experts. An annual convention in some pleasant spot might enhance the concept.
Institutions are another matter since quite often the personal opinions of the spokesman are constrained by the incentives of the institution. It must be made clear to them which opinion is desired.
Institutions choose their location for other considerations, chief among which is cheap land, but the location near public transportation is another factor. Whatever the thought process underlying it, nursing homes and retirement villages are almost always in the far suburbs. A related problem is a vexing difficulty for a center-city hospital to find a nearby nursing home for convalescents. These annoyances are protracted by the licensing rules in a round-about way. When a corporation is formed, typically a lawyer with a yellow pad asks two questions: "What are you going to name this organization?", and then, "What is its purpose?". Presumably, he then completes some forms and files the necessary applications. The stated purpose may well have other uses, but it defines the sort of license needed, and eventually either match or does not match the rules some third-party reimbursement agency has laid down for what sort of institution is eligible for reimbursement. After that, the system becomes much more rigid than it needs to be. As long as the institution remains defined as a hospital it will be paid by the third-party, and without that designation, it won't. Effectively, the state licensing board acquires the power to shut off the revenue of some institution which displeases it. But what displeases it (let's say, mice in the kitchen) usually bears a scant relationship to whether or not the institution is capable of performing additional tasks. It does not take long for these issues to get blurred and forgotten; the retirement village can't receive hospital reimbursement because it doesn't have a hospital license. A hospital license would permit it to do a lot of things it doesn't want to do. While the general idea is sound enough, the rigidity it imposes is excessive, particularly when you consider the penumbra of reluctance it provokes from employees. Obviously, the interpretations vary greatly between jurisdictions. It leads to hospitals which may perform heart transplantations but may not run a day-care center for the children of their employees.There are many simple solutions to this simple problem, but because so much of it is buried in-laws, it would probably require a special court to be appointed to oversee it. How busy that court would be would depend on how vigorously competitors would resist it, which would probably vary with the region.
In any event, Society has a legitimate interest in preserving the quality of care, but it does not fulfill that duty by transferring it to reimbursement agencies. During wars, surgery is satisfactorily performed in tents, for an extreme example of how expendable much oversight can be. Another principle would be to ease impediments to overlaps of functions between institutions, particularly including the backward sharing of component services and records toward the lower-level institution. Since such sharing is often observed to occur without objection within vertically integrated institutions, there is every indication it is both desirable and feasible between competitors.
Going much farther back to the town meeting form of oversight, the most radical departure from present custom would be to encourage a shift of the center of care from inpatient hospitals toward retirement villages. The simplest definition of the center of care would be the location of primary physician offices, and the most important step would be to discourage mandatory links between referring physicians and particular acute care hospitals. Doctors left to themselves will locate where the patients are, and increasingly it is possible to see a shift of patients requiring chronic disease management and terminal care into the retirement village. The tendency of doctors and laboratories to cluster around hospitals impedes this natural shifting together. If doctors shift their offices and are allowed a choice, laboratories and x-rays will soon follow them. Before Medicare, the center of care was found near the high-rent districts of cities. In London it was Harley Street, in Philadelphia it was Spruce Street. As reimbursement changed, it shifted toward the hospital campus, where the parking problem is also solved. Nowadays, early discharge and reimbursement shifts have made it unattractive for a primary care physician to visit his patients in the hospital, so hospitalist and emergency room specialties are flourishing, with computerization feebly bridging interruptions to the continuity of care. The primary care physician would find the retirement village solves the parking problem; pharmacies and laboratory pick-up are often already in place, and non-surgical specialists would soon follow primary care physicians. Patient transportation, at present crippled by expensive municipal monopolies, would be greatly eased by such shifts of medical interaction. The ultimate shift of the center of care would be for the more mobile younger population of suburbs to shift allegiances toward the retirement village location, a change mostly affecting pediatricians. It would take some time, and it would always be a partial migration. However, the infirmaries of retirement villages offer convenience and comfort near home.
The most effective force maintaining standards for this level of care, have no doubt of it, is the ease with which friends within the community drop in for visits. They have time for it, especially to and from the dining room, and all of them keep a watchful eye on how they would likely be treated there themselves when their turn comes. In retirement communities, client consensus is a powerful force. What is lacking is a willing sharing of reimbursement with acute care hospitals. Therefore, the idea of brief hospitalization followed by longer recovery near home is now only realistically available to the affluent. But their choices show the way, as they always did before third-party insurance dominated the scene. For a while, little children may think it is funny to get their shots at the old folks home, but they will soon get over it.
The Staggering Full Cost of Healthcare plus Retirement: $40 Trillion Plus Retirement
Study of Health Savings (and Retirement) Accounts was begun thirty years ago, increasing rapidly in the past five years. During that time, paying for unknowable health costs emerged as the central concern. At a recent Congressional hearing, the actuary testified his estimate of the first ten years of costs for "Medicare for everybody" to be 40 trillion dollars in addition to present costs, which will themselves require additional revenue in 5 or so years to avoid bankruptcy. Retirement costs would require even more additional revenue. Furthermore, it would take at least five years to make such a massive transition, possibly ten years.
This emergency testimony before the "Speaker's Rules Committee" seemed to be Nancy Pelosi's signaling we should lower our sights on such impossible spending proposals, no matter how many Democrat candidates for President endorse them. Paying a big chunk of health costs would be a significant achievement, paying for two issues simultaneously might just be an impossible dream. Nevertheless, paying for the whole healthcare system was something the public expected to happen quite soon, and would punish the ruling political party if it didn't sacrifice everything else to achieve it. We might afford to leave Medicare alone. But when eventually Medicare came into focus as the main impediment to solving a double problem for exactly the same age group; "saving" it becomes a relatively minor issue. New revenue must be found, the quality of care must not be injured, and -- most of all -- public opinion must be satisfied. This is a specialist's game, but avoidance of a disappointing outcome is becoming a decisive player. As Congress dithers, it only becomes clearer that deficit financing from foreign enemies cannot continue much longer.
Resource Assessment. Adding up all the economies of Health (and Retirement) Savings Accounts, but now also including the retirement costs, the conclusion is left that HSAs might somehow pay for health costs, plus some but not all retirement costs. Much of the shortfall comes from difficulty stating a "decent" retirement payment which would satisfy most people. What is enough for a Trappist monk is not enough for a movie star, and what will be called decent in 60 years is pretty hard to say. So at most, we should aspire is healthcare plus some retirement; supplementing retirement as we can. Even promising that much is a stretch, but is certainly superior to government healthcare plans without the discipline of individual ownership. Unfortunately, that forces the individual to some choices he must make for himself, versus allowing some big anonymous corporation to do it all for him at a hefty administrative markup. Let's specify the two big dangers the individual must navigate:
Imperfect Agents Theoretically, even the best anyone could provide from HSAs (we jump ahead, here) would be to give a newborn baby a couple of hundred dollars at birth, let a big corporation do the saving and investing, and pay out a million dollars for medical bills (that's what total health costs over the next ninety years might cost} on his behalf, at no charge. The long investing period could provide some astonishing returns, but it would not be entirely carefree for the customer. For example, it might actually cost that much, not just be borrowed with every intention of defaulting on the loan.After Assessing Obstacles Comes Strategy. Most HSAs make payments with a debit card suitable for passive investing (utilizing total market index funds) for inexperienced investors and for otherwise undesignated accounts. However, there's a technical problem: the earning period is not the first stage of life; it's the second, following nearly a third of life in childhood and educational dependency or debt. Health expenses in the childhood third of lifespan may be comparatively small, but the earning capacity is essentially zero. This unconquerable fact leads to splitting investment considerations into three stages, the first and last thirds subsidized by the middle one. The result is, two systems feeding off the middle third in opposite ways, requiring opposite approaches, and jumping between generations. Somehow, it must all come out in balance at the end. And remember, it starts with a deficit in the obstetrical delivery room unless we re-arrange something else. There is no choice but to take things one at a time.Unfortunately, experience over thousands of years has demonstrated agents -- especially governments--will eventually extract much of the resulting profit for themselves. Countless kings have been known to shave the edges of gold coins, some of them have been found to have employed inflation of the currency to pay their own bills. Investment managers are almost invariably well compensated, usually for mediocre returns, so this cost must be automated with index funds. William Penn, the largest private landholder in history, was put into debtors prison by his wayward agent, as was Robert Morris, the financier of the American Revolution. Whole-life insurance companies are the closest approximation of an agent for a Health Savings Account who might propose to get paid a level premium for decades before paying out a benefit for a dead client. They seem to survive by promising a single defined fixed-dollar benefit and counting on inflation to work for them as it sometimes does for dictators, overseen by an honest insurance commissioner. Unfortunately, they have the moral hazard of falling back on other surviving firms to bail out bankruptcies, and the political hazard of trying to force premiums downward for the taxpayer without reliable benchmarks or overgenerous recompense. Just how much they have been rescued by lengthened longevity is something only an actuary knows. Long ago, the imperfect agency situation was summarized by the question, "And where are the customers' yachts?"
Inexperienced Solo Management. If Warren Buffett had an HSA, he would have no problem managing it, and neither would a great many other savvy folks. The problem is to make the management so simple and standard that expenses can be kept low without injuring investment returns -- for the average citizen. This consideration almost drives the conclusion that lifetime health costs might be best divided into at least three component parts, with benchmarks and averages published regularly, since the medical and beneficiary problems divide into the same three (childhood, working age, and retirement) components. It begins to look as though a new profession of fee-for-service advisors needs to become educated and distributed widely, perhaps in local bank branches. As will be described in later sections, the need is for the income stream to be kept in balance with the probable expenditures, adjusted for inflation or deflation. It is not, to achieve the maximum possible revenue return, regardless of risk. That is to say, the purpose of the HRSA is not to make as much money as possible, but to be sure as much medical need as possible can be satisfied by the revenue available. Let's put it all in a nutshell: There's a big difference between designing a system to cover a public need inexpensively -- and designing a business model to make a profit. But even that's not nearly as big a problem, as trying to do both at the same time.
|
If you spend too much too early, you won't have anything left for later.
|
|
41 Blogs
Observations About Old Age--From a Participant
Redesigning Old Age
A Doctor's Toast to His Patients
Itch
Barber of Saville: Male Pattern Baldness
Podiatrists Strike it Sort of Rich
Limits on What Can be Promised: Healthcare Plus a Modest Retirement.
Last Will of Benjamin Franklin
Franklin's Codicil to His Will: Strange Afterthoughts
TV and Politics
Retire Later
Starving the Beast of Early Retirement
Go to Delaware, Elephants?
Widower's Friend
The Coming Baby Boomer Retirement Problem
Migrating to Retirement Villages
A Few Rooms of Your Own
Front Stuff: Pearls on a String: Further Extending Health (and Retirement) Savings Accounts
All Right, Hippocrates. So What's the Basic Problem?
The Economic Consequences of the Health and Retirement Savings Account
Overfunding for Retirement (2)
New York Times: Splendid Idea for Old Age
Another Proposal for Residents of Retirement Villages to Consider
The Whole Town as a Retirement Center
The Segments of Lifetime Healthcare: Medicare Including Retirement Pearl #1
Plans for Healthcare Financing Retirement, Too
Competitive Institutions: Paying for Assisted Living
Playing The Cards As You Are Dealt Them
An Under-used Veterans Benefit
Computerizing Medical Care
Rejecting Preventive Health Care for Good Reason
Stretching Out Dwindling Assets (1)
Retirement Communities
Retirement Communities (CCRC)
Health Savings Accounts
Amending HSAs To Include Tax Sheltering
Increased Potential for Retirement Villages
The Staggering Full Cost of Healthcare plus Retirement: $40 Trillion Plus Retirement
|
 The authors of the Bible believed human life was designed to end at age 70. The revised scientific guess is 100.
The authors of the Bible believed human life was designed to end at age 70. The revised scientific guess is 100.
 New Jersey may be about to demonstrate that taxpayers should be on the lookout for too many government employees, not too much government spending.
New Jersey may be about to demonstrate that taxpayers should be on the lookout for too many government employees, not too much government spending.
 In a few years, the baby boomers will retire and two things will happen. They will have to retire later in life, and the country will have to borrow money to pay for the rest.
In a few years, the baby boomers will retire and two things will happen. They will have to retire later in life, and the country will have to borrow money to pay for the rest.
 A benefit which most any veteran can take advantage of seems to be little-known and consequently not many vets are taking advantage of it. It's called Aid and Attendance and can help defray the expenses of assisted living.
A benefit which most any veteran can take advantage of seems to be little-known and consequently not many vets are taking advantage of it. It's called Aid and Attendance and can help defray the expenses of assisted living.
 Healthcare is mainly information processing, but utilizing computers has been a disappointment. Be prepared for high costs and continuing disappointment for decades to come.
Healthcare is mainly information processing, but utilizing computers has been a disappointment. Be prepared for high costs and continuing disappointment for decades to come.
 No one seems to be considering the opinion of older citizens about preventive health care.
No one seems to be considering the opinion of older citizens about preventive health care.
 Retirement communities are fairly new ideas, still experimenting with the ideal model, so it is hard to generalize about them. But they look to be a possibility for everybody's future.
Retirement communities are fairly new ideas, still experimenting with the ideal model, so it is hard to generalize about them. But they look to be a possibility for everybody's future.
 Retirement communities of the continuing-care variety, are a comparatively new and apparently splendid development. The present economic crisis is their first major test.
Retirement communities of the continuing-care variety, are a comparatively new and apparently splendid development. The present economic crisis is their first major test.
 In late 2003, Congress passed and the President signed, legislation enabling tax exemptions for contributions to Medical Savings Accounts. This monumental reform was included in a law which created a number of Medicare prescription drugs benefits which received more attention in the press. Such accounts were renamed Health Savings Accounts, which was the original terminology in 1980 when John McClaughry of Vermont and George Ross Fisher of Pennsylvania, shortly joined by Michael Smith of Louisiana, first introduced the concept.
In late 2003, Congress passed and the President signed, legislation enabling tax exemptions for contributions to Medical Savings Accounts. This monumental reform was included in a law which created a number of Medicare prescription drugs benefits which received more attention in the press. Such accounts were renamed Health Savings Accounts, which was the original terminology in 1980 when John McClaughry of Vermont and George Ross Fisher of Pennsylvania, shortly joined by Michael Smith of Louisiana, first introduced the concept.