1 Volumes
Medicine
New volume 2012-07-04 13:34:26 description
Hospitals and their Future
New topic 2019-03-21 19:29:46 description
Philadelpia Hospitals, Past and Future
It was sixty years before Philadelphia had a second hospital, so the way things were done at the Pennsylvania Hospital tended to set patterns. The central pattern was: charity for poor folks, during a period when prosperous people were treated in their homes. Since Franklin was the secretary of the Board of Managers, it is in his own handwriting that we see "Founded for the sick poor and, if there is room, for those who can pay." In 1900, two-thirds of all hospital beds in Philadelphia were still ward beds for the poor. In 1948 when I was a two-year unpaid intern there, a posted sign said the accident room charge was fifty cents, but in fact, it was only collected if the patient happened to have insurance. The student nurses ran the place unpaid, and the main exceptions were the two paid administrators, the Steward, and his secretary. Philadelphia was settled for religious freedom, enjoyed many new religions, and consequently had a long era of Methodist, Episcopal, Presbyterian, two Jewish hospitals and the hospitals belonging to three Catholic Orders.
With the advent of the Civil War, PGH (Philadelphia General) grew to seven thousand beds, all of them free, when it was discovered more soldiers were dying from diseases than from wounds. Surgeons and obstetricians built specialty hospitals for their patients, mostly small ones, like Babies Hospital, Preston Retreat, Contagious Disease (mostly polio), Casualty, and a host of tuberculosis and psychiatry hospitals, Eye Hospitals, HEENT Hospitals, Children's Hosptial, and a number of small paying hospitals. The Civil War and the invention of anesthesia created a need for small hospitals for people who could pay, like Skin and Cancer.often in the shadow of larger charity hospitals for those who couldn't' pay. The first question any audience asks with bewilderment is about the cause of so many current hospital mergers. Part of the answer is we once had too many hospitals, and the rest of the answer was that the Flexner Report created a surplus of government money, intended to support research, and similarly stimulated by the creation of Blue Cross in the 1920s. Flexner favored research money, and the Universities grabbed it. The insurance mechanism was the best available means to save money when you were well, in order to spend it later when you were sick, but insurance muffed the chance. They chose one-year term insurance, mostly because short-term business was paying the bill. When money was no object, money was wasted.
The quickest example of honey attracting flies was observed shortly after 1965, when Philadelphia teaching hospitals (there were 104 of them at the time) went to Mayor Rizzo, suggesting PGH should be closed, ostensibly in order to facilitate the flow of federal funds to private hospitals. Thus they would help teaching hospitals absorb the abundant flow of government charity while eliminating the $11 annual cost of PGH to the City. That transformation from mostly charitable to largely private hospital care took from 1977 to 2010, to the private amusement of those who had been present at the meeting. At the end of this transformation, their positions had reversed; the teaching hospitals now bemoaned the shocking disappearance of the city's medical charity through PGH, casting such people back onto the teaching hospitals. Vannevar Bush probably had a hand in this, as the pretext was that only teaching hospitals did research. Meanwhile, they lobbied strenuously to retain monopoly control of federal research money, at the expense of charity beds within the teaching hospitals. In other words, we had a reasonably satisfactory system of charity care until charity patients demanded equal facilities from public money. Lyndon Johnson gloried in his achievements, but the fact is they opened the door to the unsupportable expense. The nursing profession was utterly flummoxed to be given degrees in return for the disappearance of their profession. If the combatants had stopped long enough to ask, there simply was not enough money to do what politics was demanding. The nursing school was always the heart of the hospital; the doctors were too busy tending to patients. And charts which they mostly falsified to save wasted time. Adding to the confusion was the effect of shifting nurse training costs, from the hospitals (diploma) to university responsibility (bachelorette degrees) and the adverse effect on nurse quality was noticeable. Doctors no longer married nurses, for example, they married lawyers and similar pre-professionals. The greatest effect, aside from higher cost, was to remove the loudest objectors from the scene, at just about the wrong time. The universities were clamoring to transform the nursing profession into administrators, in order to satisfy a seemingly insatiable demand stirred up by muddling the medical record-keeping system with the task of creating huge records which no one has time to read. The public regards medical matters as too obscure to understand and so does not appreciate how much cost has been created by switching everything non-essential around. It seemed obvious to them that non-essentials were poorly done. But not being medically trained, they weren't able to tell what was non-essential. Improving legibility and interphysician communication was nice, but it wasn't the main business of a hospital. Physicians learned to practice good medicine in tents and scarcely saw any difference.
Lawyers have learned something, too. They learned that antitrust violation is not signaled by per se violations or even vertical integration. It is signaled by mergers. Senator Specter may have kept Robert Bork from the Supreme Court. But the Law is slowly catching up with mergers, and Bork's books are still in print.
The future of hospitals does not lie in buildings. Doctors' practices are easily moved to retirement villages where the old folks are. Patients are there a long time, and equipment is easily moved there to be with them. It would save a lot of money because diseases are disappearing. Something like five diseases now represents something like 80% of the cost, but all that money spent on hospital buildings has already been spent, so it will take too long to get there peacefully. For all I know, five new diseases will replace five old ones, but the trend is downward. Costs keep going up. Doesn't that tell you something? What's going to happen to all that real estate after we cure cancer?
Specialized Surgeons

|
| Regina E. Herzlinger |
Local attitudes always somewhat persist among migrants from home. What's distinctive about the Philadelphia diaspora is how unconscious most of them are about still carrying the hometown mark. Philadelphia leaves a prominent birthmark, but it's sort of back between your shoulder blades and you forget it's there. What occasions this observation is a Christmas call from a prominent California surgeon who was once my roommate, back in the days when residents were actually resident in the hospital. More than fifty years ago Bill Doane also served as best man at my wedding. Our conversation turned to clots in the lung, and he related a story. He had once fixed a hernia for a 22-year old girl in the days when it was customary to keep hernia cases in bed for a while. Getting out of bed for the first time, she coughed and turned blue, suddenly on the edge of death. Taken back to the operating room, her chest was opened, and Bill removed a clot which was essentially a cast of the blood vessels of one entire lung. As surgeons like to say, she then did very well.
One doctor can tell such a story to another doctor in four sentences, while lay people who overhear it miss the whole point. The fact is, not one surgeon in ten thousand today could carry this off. Nowadays we train thoracic surgeons to open the lungs; they never repair hernias. Conversely, we train hernia surgeons to fix a dozen hernias daily through a little telescope; they never open a patient's chest. So it is hard to imagine many contemporary surgeons who could recognize this disastrous complication of hernia repair, then fix it themselves in time to rescue the patient. Although this disheartening decline into repetitive super specialties has been forty years in the making, it has been recently popularized with the general public by Regina E. Herzlinger, a Harvard business professor. Writing books and speaking to businessmen groups, she has popularized the proposal to outsource the general hospital into what she calls "focused factories." She rightly characterizes the medical profession as reluctant. She's a nice person, and undoubtedly sincerely believes focused factories will save money, improve quality. But we must not let this idea take hold.

|
| Pennsylvania Hospital |
Specialty hospitals have actually been given more than a fair trial. About a hundred years ago, the landscape was peppered with casualty hospitals, receiving hospitals, stomach hospitals, skin and cancer hospitals, lying-in hospitals, contagious disease hospitals, and a dozen other medical specialty boutiques. With a few notable exceptions, they all failed for the same reason. Sooner or later they found they could not adequately service their specialty without the backup of a full hospital service. Children's hospitals do thrive, but they have patients who are generally of the wrong physical size to fit adult hospital facilities and equipment. There are plenty of things to regret about general hospitals' design, but the inescapable fact is they all must have a very wide range of services to perform any mission, no matter how discrete. It would be still better if the doctors had an equally wide range of skills in their own heads, but the avalanche of innovation and lawsuits has forced sub-specialization, compartmentalizing, and narrowness of viewpoint. Circumstances have forced the profession to hunker down, but that trend must be resisted, not celebrated.
The instant and successful repair of pulmonary embolism make a dramatic illustration, but the reasons for broad medical training are more extensive than that. In the first place, it is much cheaper to use the generalist office than to bounce people to a gastroenterologist for heartburn, a psychiatrist for anxiety, and a dermatologist for pimples. The American employer community is desperate for a way to reduce its burden of employee health costs, and flocks back to their nurturing business schools for advice. They would do better to seek repeal of the tax dodges which tempted them into their present muddle, of course. But in any event, they must be persuaded to recall the disaster of managed care and at least, avoid meddling in hospital design.
That's the cost issue, where specialization surely raises costs. Constant repetition of the same procedure seems superior to first-time fumbling, although it is questionable how long it takes a well-trained surgeon to pick up a new procedure and do it well. But for this system to work, the referring physicians need to be more skillful, not less, in choosing a good one to refer to. There's just nothing like the experience of working for a few weeks in the specialty as a rotating intern, to tell you what to look for and what to avoid. If every doctor in a hospital is making a dozen internal referrals a day, the cumulative effect on the quality of the whole institution is dramatic -- when they have had sufficient past involvement in the specialties to which they now only refer patients. Some specialists will become popular and rich; others will sulk around unnoticed for a while, then go elsewhere. This process, of course, occurs everywhere; what's institutionally distinct is the culture underlying the standards for preferences.
We'll talk later about the Doane brothers of Bucks County, who were judged to be too handsome to hang. Right now, the point of this story can be summarized by the old Pennsylvania Hospital adage, that you must first be a good doctor before you can be a good specialist. Not only was the Pennsylvania Hospital the first in the nation. For sixty years it was the only hospital in the nation, and for decades after that, it was the only hospital in Pennsylvania. In medical history circles, it is said that the history of American medicine, is the history of the Pennsylvania Hospital.
Don't You Touch My Medicare!
We have heard Medicare described by Senators as the "third rail of politics" -- just touch it, and you're dead. Unfortunately for clever phrases, the costs of the last decade of employment are shifting to a point we may foresee major health costs for working people getting heedlessly dumped onto Medicare as a desperation measure. Meanwhile, Medicare grows more expensive and national indebtedness grows worse. That's what single-payer enthusiasts demand, but even politicians on the campaign trail acknowledge that something must be sacrificed in the name of affordability. A growing gap in coverage for divorced women and early retirees already exists between the end of employer coverage and the beginning of Medicare, because no one has figured out either how to cover the increasing longevity, or how to assign the gap cost to multiple former employers. So, we might well pass through a phase where Medicare costs are rising, employer costs are declining, while the political parties merely blame each other for failing to cover the growing gap of uninsured which lies between dual coverages for elderly healthcare and simple retirement. Life insurance companies may suggest themselves merging Medicare with retirement insurance, but former employers reply "catch us if you can." Politicians describe "affordability," but that's what it amounts to.
If we could shift the cost of employee medical cost elsewhere, we might have an unbeatable wall against foreign goods, but there are perplexing limits, even to success. As we found at the Bretton Woods Conference, if we have all the money, foreigners can't buy anything. To be useful, a solution to the American hospital payment problem must be gradual, and it must be adjustable. Plenty of desperate foreigners stand ready to cut your throat if it isn't. So medical costs and retirement costs simply must be reduced as a painful but inevitable price to pay.
After we solve that issue -- wonder of wonders -- scientists will start to pick off the diseases of old age. We are already given to understand that the NIH has ordered a priority to grants for curing the most expensive ten diseases. That somewhat conflicts with the goals of scientists, who tend to concentrate their attention on the easiest diseases to cure. But money is money, and so we find that eighty percent of health care costs are caused by eight or ten diseases. With over thirty billion dollars flowing into research annually, relatively soon one or two of those dread diseases will disappear from concern, longevity will increase somewhat, and we hope some less expensive disease will finish off the temporarily lucky survivors. No doubt, we could use a few billion to pay off debts to the Chinese for our previous deficits. But the time will surely come when buccaneers will wish to spend the surplus generated in this manner, on something else more trendy than elderly health care.
Unless we have the foresight to anticipate this collision of interests, an unfortunate precedent might have been set. Leaders of the elderly and their concerns should anticipate this battle, and be better prepared to meet it. The best way to meet it is with a completed plan in operation to shift Medicare gains from research to retirement funding as they appear. The problem of funding Medicare (which is 50% subsidized by foreign bond sales to an insupportable degree) would then take the form of changing the name of Medicare to Retirement Care, because most of the money then goes to that purpose, a fairly meaningless and thus easier political problem to manage, because it will take a generation or two to happen.
By the way, Medicare represents the largest expense in the healthcare budget, so liquidating it gracefully will generate the largest source of new funding for the lifelong scheme. We now turn to the problem of funding the early years of life, which seems destined to be the hardest problem to address. In fact, it is so difficult there are essentially no competitive plans of any substance so a workable proposal might have surprisingly clear sailing.
Academia Gets Its Share of Blame
In 1910, Abraham Flexner produced a book-long report on reforming medical education, under the sponsorship of the American Medical Association and the funding of the Carnegie Institution. The report was a product of the progressive era of reform which ended the Gilded Age, and can fairly be described as the handbook of a revolution in American medicine. The book had an impact on closing 106 of the 160 medical schools in the United States and Canada. To Flexner that was a disappointment; he thought only 31 were worth saving. To be a good doctor, in his opinion, required between six and eight years of scientific training. The quality of student, as well as the quality of schools, was important, justifying a vast shrinkage of the student body. He liked research and unleashed an avalanche of medical research which subsequently transformed medical care in a hundred ways.
Having said all that, it must be acknowledged, Abe Flexner had been educated in Germany, and his efforts mainly crystallized the transfer of German academic medicine to America, and from here onward to the world. What's being acknowledged is that for a time, German Medicine was far ahead of us, in an environment where we aspired to be the leaders.
Flexner was a charismatic figure, supported by American Medical Association reports from its Council of Medical Education, the wealth of the Carnegie Institution, and the enormous resources of the Rockefeller Foundation. American academic medicine pointed to the example of the Johns Hopkins Medical School, formed before the ferment of pre-World War I, and now being given prominence by Teddy Roosevelt, Woodrow Wilson and the rest of the muckraking era who aspired to replace the Gilded Age with something better. America was aching to take charge of something, had great gobs of philanthropic money at its disposal, and the wind in its sails. Abraham Flexner was a towering figure, all right, but he was not a physician, an academic, or a scientist. He was more the agent of revolution than its originator, ending up as the patron saint of several political factions, individually fighting academic wars with each other. He was, in short, a rain-maker.
 Abe Flexner, the Rainmaker 
|
| German Model for Medical Schools |
Abe Flexner and his book aimed to reduce the number of medical schools from 160 to 31, demanding the survivors look like German schools. This was not so strange; like Japan and China today competing with America, Flexner wanted to compete with Germany more than he wanted to worship it. The students of his dreams were required to be college graduates, the curriculum was to be four years along with two years of science followed by two years of hands-on learning. If the school could afford it, the professors would be on a full-time salary, free of any need to practice in order to make a living. On this last point, many begs to differ, arguing you have to get on a boat to learn how to sail one. There were many echoes of the ferment to come, in the upheavals of the 1960s, and the Humboldt's University of Berlin was the source of quite a few, in both cases.
Immediately there arose a town-and-gown competition. The gown group had the point they could afford the time to do some research. The town group had the point you couldn't teach doctors if you weren't one, yourself. The distinction is probably best understood by comparing medical students with law students. Both were originally taught by practitioners; schools were late arrivals. Many lawyers have remarked that a law school graduate now knows almost nothing about the practice of law until he joins a firm which teaches it to him. A medical student (post-Flexner) can do a pretty good job with most medical problems, the day he graduates. The practicing physicians have retreated into specialty training; a doctor has trouble becoming a specialist if he didn't have the right residency. The rest of the awe-inspiring march of medical progress in the Twentieth century, is the consequence of pouring unbelievable amounts of money into the system, thereby attracting a glittering array of talented medical students. Some of the talents are unbelievable. My own medical school, as an example, has a symphony orchestra made up of students in their spare time, performing on a truly professional level for their own amusement. In a sense, all of this was due to Flexner. In another sense, Flexner himself had little to do with originating it.
Now, forget the yellow journalism, or muckraking, quality of what I am about to relate. A book was recently published relating that a particular medical school was able to support its operations without touching a penny of medical student tuition for ten consecutive years. Instead, the tuition money was transferred to the University's undergraduate schools, and the medical school subsisted on research and other funds. The undergraduates continue to protest about rich doctors, while the medical students complain about going a hundred thousand into debt -- to pay their tuition. But forget that part. The most undesirable situation it reflects is that for ten years, the school was totally able to exclude any parent and student influence in an area that unfortunately has a growing power over events, the school's finances. If the students, families, and alumni of a university have no power to influence its decisions, who do have such power?
Two Central Mistakes In The Design of Health Insurance.
Concentrate on two flaws in healthcare. If uncorrected, no scoring -- dynamic or otherwise -- will conceal collective failure to address health costs seriously. Other problems should stand aside while these two are considered.
The first is pay-as-you-go. Its name misleads, because the younger generation, enjoying good health, pays its parent's high health costs toward the end of life, passing their own to their children. Medicare's first generation thus was given a free ride, so my mother who died at the age of 103, represents a whole generation who paid essentially nothing for thirty years of expenses. This example of debt being passed along for fifty years, got bigger with time throughout 18% of Gross Domestic Product, even with low-interest rates. We must liquidate that debt, invest the idle savings until needed for healthcare, and eliminate the annual 50% Medicare deficit to creditors. Quite a task.
An important result would be the incentive to save, replacing the incentive to spend. HSAs demonstrate net savings in health- the cost of at least 20% because, in a Health Savings Account, young people of each generation earn interest while they save for their own subsequent health costs, instead of spending immediately for anonymous demographic groups of strangers. At this point, another unexpected bonus appeared:
Some people have the luck not to get very sick, thus able to accumulate tax-exempt money in the account until they turn 66. Since everyone gets Medicare eventually, current law turns HSA accumulations into largely unnoticed tax-exempt retirement funds. (It's mandatory, whereas I would prefer an option.)
A second blunder reached the surface. Medicare provided better medical care, but made longevity increase, laying bare it had added thirty years of retirement cost. Sickness cost is episodic, but retirements are continuous. Consequently, additional retirement costs can become several times as costly as the sickness costs they replace. Talk about sweeping something under a rug.
It will not be easy to produce packages of proposals to cover the transition to a less costly funding system. But no health funding scheme other than Health Savings Accounts provides even the flimsiest scaffold for addressing this issue. Social Security has such a mission but is hopelessly underfunded. So the second of two big problems facing us, is: we failed to anticipate success.There is a third big elephant in this room to be wiped out with a paragraph of legislation. Scratch any regulation and you find a lobbyist underneath it. Half the population enjoys a tax deduction denied the other half, and that other half is restless. Unless big corporations yield to the demand for equality, there will be continued agitation. No doubt lobbyists promise to address this issue under tax reform and perhaps plan to reserve their concessions for later trade-offs. But one half of the public owes such a large debt to that other half, little quid pro quo is justified. Permitting HSA to pay the premiums for required high-deductible insurance could accomplish it in a handful of sentences.--------------------------------------------------------------------------------------------
The fourth big issue offers hope, instead of despair. Medicare coverage for young unemployable persons ("disabled") was effectively broadened to over 90 %, by unemployed effectively changed to unemployable. Higher costs were thus added to basic costs for 9 million of the 46 million regular Medicare recipients, rather than remaining lumped with the 30 million uninsured unemployables (requiring specialized programs.) These higher costs of average Medicare per employable person, have been overlooked by most commentators, making ordinary Medicare seem costlier than it really is. It's bad, all right, but not quite as bad as it seems. Documenting that fact, as well as shifting the medical income tax inequity to the tax bill, leaves only two new issues to address: pay-as-you-go, and retirement funding. That's quite enough for a first round.
Hospital Cost-Shifting Between Payer Classes
Diagnosis Based Payment: A Warning
I was sitting in the Congressional hearing room when it happened. A proposal from the hospital association was made to Congress in 1983 that instead of paying hospitals for each step of treatment, they should be paid by the diagnosis, and Congress soon agreed to the idea for Medicare. This system was to be limited to helpless inpatients. The idea had some good features: if a patient had to be fed with a spoon, he had little interest in the cost of his treatments. Under these circumstances, market mechanisms would never restrain the cost of hospitalized patients. If they were anesthetized, it was even truer.
|
DRG: An Object Lesson for Control Freaks With Little Interest in What They Are Controlling.
|
So in this way, by arranging the assignment of costs to codes, Medicare and the hospital coding clerks took over the job of pricing. No doctor understood what in the world they were doing. And by steps familiar to accountants, the DRG was enlarged back to a thousand codes and internally arranged to come out paying the hospital a 2% profit margin for inpatients. Since we were running a 3% inflation at the time, the effective push was on-- to move in-patients to the out-patient area. No matter how many tests, no matter how long the patient stayed, the DRG came out to produce a 2% profit margin. The cost the insurance had to pay was lessened, the costs the hospital actually incurred, became the hospital's problem. Meanwhile, interest rates were low, so new outpatient buildings seemed cheap. Pretty soon, hospitals were paying doctors above-market prices to fill the outpatient area. There's more to say, but the idea is clear. Once you find a rationing tool, the accountants are in charge, the doctors are out, and eventually would be really out. And the beauty part of it was, no one understood what was happening, or who did it. Except you will find a lot of empty out-patient buildings when the music stops.
Health Savings Accounts: Synopsis
Ben Franklin felt medical care would pay for itself by putting sick people back to work. Not quite.
1. It works for some people, sometimes. That's the old system, which now needs a few tweaks.
2. To work for a whole nation, it needs more money -- a magnification system, which implies fewer options to choose between.
1. For individuals, it can be lifetime, which would be shunned by unsuitable clients.. There should be no age or other limits, so everyone can have one, at all times if he is able. If it has been unused (for medical payment) for a full year, it should still continue to generate income, but the premium for catastrophic insurance should be waived for the following year as an incentive to save it. It may accept additional deposits, however. This seems to be the administratively simplest way to keep it functioning as an investment while temporarily managing duplicate insurances (from employers or marriage difficulties, etc.)
HSA is the only health insurance where fund surplus becomes retirement income at age 65. That should remain an option until death, changing into a 21-year post-mortem trust fund which is permitted to use fund balances for medical debts and purposes, untaxed, with final surplus taxable in an estate as if an IRA). It probably should not accept additional deposits, however. (This option replaces the present mandatory exchange for an IRA upon acquiring Medicare coverage, and the mandatory Catastrophic feature should be dropped when Medicare coverage begins.)
The catastrophic system needs statements and limits about its regulation, fees, state coordination, what to do about abnormally low returns (using domestic total market indexes as a benchmark). It ought to address state vs. federal issues in a general way.
2. To serve the whole nation, rather than just the individually suitable subscriber, it needs a uniformly longer time horizon , more augmentation of income by compounding, more attention to security and long-term income, and more benefits to compensate for fewer options. In fact, it may need a consultation about passive investing of index funds. To preserve funds for long periods of time, audited escrows are absolutely required for protection against the imperfect agency. Starting small, this system could grow to enormous size. Because of longer time frames, the fund may need to allow flexibility for other investment strategies which at the moment are discouraged. I suggest the total stock market index as an audit benchmark with adequate penalties for failure to match it. The smaller investor needs rules, the bigger ones may not. If it has a good income return, it may require less attention to its format. Events will determine whether this is mostly a campaign document or a long-term strategy and whether it must be implemented in steps. Both Medicare and ACA took on too much all at once and stumbled. I suggest reforming Medicare first, children later, working people piecemeal.
The post-mortem trust fund needs to be checked out with estate lawyers. the last years of life reinsurance as an alternative. My sense is the trust fund is politically easier for the elderly to understand, but the elderly may want to plan ahead and so would prefer an insurance approach. Those who are fearful of outliving their income may have a preference. Lawyers have mixed incentives about closing estates early.
I don't see why due diligence hasn't appeared for every change of party, for all programs. Insurance salesmen may prefer to lock you into one program or another, and flexibility is not always in their interest.
Changing the legal responsibility for children's costs will be generally resisted, but the parents are young and fearful.
The elderly have most of the health costs, while working people have most of the revenue. The trick is to transfer the funds without so much resistance. There must be some sort of trade-off for employers to let go of their loophole. It took the Civil War to weaken states rights in the Constitution, and World War II to give employers their tax loophole. Making the public understand compound interest may require another 2007 crash. But as long as we have 3% inflation, it's about our only hope. Under no circumstances allow the government to own common stock. or socialists to control corporations.
I know the weaknesses of subsidized research. Somehow, subsides never get called or counted, as costs.
The Effect of Tax Law on Health Costs: The IRA for Health
The Effect of Tax Law on Health Costs
The IRA for Health
Section I
Chapter Three
Introduction
If the preceding chapters have done nothing else, I hope they have at least acquainted the reader with the fact that the current federal deficit is currently made worse by seventy billion dollars through the tax exemption of health insurance premiums, the largest American tax loophole ever recorded. Further, this tax exemption is inequitably distributed and is a source of societal friction which could express itself in unpredictable ways. And therefore the politics of dealing with it must be very carefully handled. This chapter is a serious description of a proposal for dealing with the issue. I believe it contains nothing which would injure a component of society, and it would not increase the federal defeat. It would slowly remove health costs from employer budgets, and it would ultimately nudge them considerably.
The idea of a Health IRA had its beginning at a dinner for the White House policy staff which I was invited to address in 1980, and the Provocateur was John Mc Claughry, then Senior Policy advisor in the Reagan administration. It must be remembered that the IRA (Individual Retirement Account) law had not yet been passed, but John must have heard about it, and suggested an extension to health costs. Since Mc Claughry’s main intent was in agriculture, he never did much with the health idea. But I was electrified by the idea and took it back to the American Medical Association. Curiously a relatively similar idea was independently brought to the AMA by Dr. Michael Smith of Thibodaux, Louisiana (he called it The CHIP program) the AMA took quite a while to digest the idea but it was eventually adopted by the AMA House of Delegates as an official AMA policy proposal. Somewhat later, but entirely independently Peter Ferrara of the Cato Institute and John Goodman of the Institute of Policy and Research came on the idea and pushed it forward as a replacement for the Medical program. My own views are more expansive. I believe that all health insurance should be eligible for the IRA approach. with a voluntary conversion provision any time after age 65..
Funded Insurance.
Having rattled the cage about tax deductibility in the previous two chapters, it is necessary to make another digression before discussing the Health IRA. It relates to the second flaw in the tax laws affecting health insurance. Employer- paid health insurance premiums are tax deductible, but it is forbidden to carry the benefit forward beyond the year in which it is earned. There were probably good uses for this limitation which are obscure to me, but the essential fact is this limitation made it impossible to build up cash value within a health insurance policy the way you normally build up a cash value within a whole life insurance policy, except by HSAs. Using the reasoning of life insurance, all health insurance is term insurance. Using the reasoning of social legislation, health insurance is a pay as you go scheme. Any way you look at it, health insurance is by law hampered in using the massive power of compound infected to reduce its ultimate cost. Here is the appeal of IRA for Health in the eyes of Peter Ferrara and John Goodman: forty years of compounding where it could greatly reduce the cost of Medicare when the individual reaches age 65, and the existence of the funded reserve would make the insurance promise a lot more secure. Alternatively, just allow everyone to have two policies, one for the current expense, and one for saving for the future.
Portability.
I like that thought, too but for me, an equally important need is to build up a reserve within the policy so the individual could experience periods of unemployment without losing his health insurance. To lose your insurance when you lose your job crippled the Clinton Health Plan, and preventing a pre-existing condition limitation crippled the finances of the insurance companies because the average time between job turnovers was 3.5 years Obama plan, almost all chronic disorders were excluded unless the Obama administration was willing to raise premiums. Some hidden hand was unable to concede the point, and Obamacare costs spiraled out of control. Either the insurance must transform from term insurance to permanent insurance, or else cost would be insupportable. Apparently, those speaking on behalf of employers were unable to concede either point, so the situation just drifted and got more expensive. I have repeatedly seen patients who became sick while they were unemployed. And then became they had developed a “preexisting illness†they became uninsurable even if they got a job. Or they couldn’t get a job because employers recognized they were expensive to hire. To me, the linking of health insurance to employment was a concept which needed re-thinking if individual tragedies were to be avoided. Somehow, it was easier to characterize such opinions as insensitive, than to do anything to repair the underlying problem.
Furthermore, part of my job is to listen to people’s troubles. Many times I have heard patients complain they hated their jobs but were afraid to quit for fear they would become unemployable during the change-over. For practical purposes, health insurance under the employer-based system is not portable between jobs. It has not already collapsed because so many diseases of younger people have been cured, adding thirty years to life expectancy. If the new employer provides group health insurance, it is on his own terms and those terms may be unfavorable to the individual. I have just once in sixty years of practice, encountered an employer who changed the benefits of his group policy and was thus able to terminate the ongoing payments to the dependent of one employee. Employer casual group health insurance is a reasonably good system. But as the health of the nation improved it developed lots of flaws which might have been corrected. They weren't, because the health part was never the main concern of enough employers, so they permitted the health companies to resort to short term patching.
To me, it is a flaw that the employer sets the terms of the policy. It seems much better if a way can be found for the employee to own his own policy, raise, lower or change the benefits as he is willing to pay for them and carry his policy with him as he chooses his own employment circumstances. The employer is mainly interested in the cost of the employee benefit, so let him restrict his interest to how much he is willing and able -- to pay.
Reducing Unnecessary Care with Health Savings Accounts
B
Other Voices: Rethink Lifetime Health Finance
(Revised)
Medical finance is an inter-generational funds transfer. Sickness costs migrate later, workers age 18-64, get less sick. Retirement seemingly replaces sickness, but -- so far -- merely displaces it later, without added revenue. One-eighth of lifetime medical cost now transfers between generations by payroll taxes, another quarter must be borrowed. Nine million disabled-under-65 are paid revenue originally intended for the elderly. The rest is roughly balanced, or was before the Affordable Care Act raised alarm about government's indifference.
Since 1965, Medicare collects 2.9% payroll deductions, immediately spent for their parents as "pay-as-you-go ", gathering no income. Lifelong debt concentrates into Medicare debt, as healthcare migrates toward the elderly. Politicians, terrified to touch "the third rail" of Medicare, respond at the wrong end of life. Thirty years are added to longevity, while healthcare debt evolves into retirement costs. And then, the money runs out. Statistics are rough, but retirement deficits equal Medicare's laundered debts getting worse as healthcare improves. Talk about conflicted incentives.
A solution: view one eighth of revenue as accumulated over 42 years, whereas a quarter of costs could be more than recovered by compounding the same idle money over 104 years. Try it free on the Internet. This achievable result comes from 1) extending age limits of Health Savings accounts down to birth and up to a trust Fund's perpetuity, defined in common law as a lifetime plus 21 years, while using an unfunded HSA to unify unspent compounded income for his own retirement, not for demographic groups of strangers. 2) Investing the payroll tax at no less than total market index funds, assuming a 3-7% lifetime return. 3) applying grandpa's surplus $4000 to grandchild's underfunded $4000 shortfall. (Please read that twice).
The compounding period is extended upward by post-mortem Trust Funds escrowed for Medicare-related costs only, extinguished when transition debt ends. It is extended downward 21 years by grandparents transferring approximately $4000 to one grandchild or equivalent, as HSA to HSA. Trust funds finance the transition deficits. This has the advantage of terminating Health Savings Accounts around age 18 when medical costs are lowest. Add the additional possibility of transferring the mother's obstetrical costs to the child, thus reducing premium costs for the 18-45 year age group as well. Much of this magic lies in the superiority of compounded rates over inflation rates. Long-term solvency appears likely, and borrowing is ended.
George Ross Fisher MD 3 Haddon Avenue South Haddonfield, NJ, 08033
Cell 215-280-6625 office 856-427-6135 Email: grfisheriii@gmail.com
The Two New Revenue Sources for HRSAs: Investments and Compound Interest
Two "new" revenue sources, which we need to discuss, are really quite old. But widespread use of third parties to pay medical bills diminished consumers' attention to their value. Patients become like Queen Victoria, indifferent to what it costs to run a household, even forgetting how to do it. We fit some details into the discussion of Health and Retirement Savings Accounts, but they are capsulized here for descriptive convenience, in an era when personal management has largely moved from junior high schools to the curriculum of graduate business schools. In the process, we have forgotten a timeless message: never let an agent manage your checkbook for you.
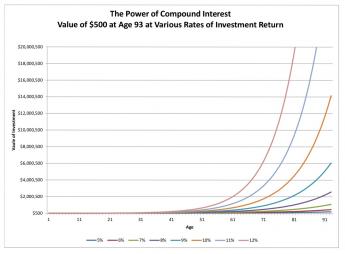
1. Compound Interest. Aristotle complained it gets more expensive to repay debts, the longer you take to pay them off. That's the debtor's viewpoint, of course. The creditor's view of it is, the longer the better. But restated as a neutral mathematical comment, an essential feature of compound interest is that both principal and effective interest, rise over time. To repeat: income rates (and/or borrowing costs) from a debt, increase with duration. About half the capital of every major corporation consists of debt, so even owning common stock has some of the quality of being a debtor. Furthermore, this effect is seen sooner, with quite small rises in nominal interest rates. A graph of sample interest rates demonstrates this simple truth with greater clarity:
|
As a result of centuries of haggling and experimentation, most modern loans charge interest rates of 5-15%. That's an enormous swing, but only for long-term investing. It makes little difference whether this range of rates reflects the supply of money in the economy, or the vigor of the economy, or something else macroeconomic. So long as rates remain steady, or even if they are changing at a slow steady rate, borrowers and lenders can reach an agreement and negotiate a long-term loan. If there is uncertainty about rates in general, they may rise precipitously, so all borrowers know to keep loans as short as possible, and creditors quickly raise rates when they must cover longer time periods.
The moral is, as you become older you tend to become a creditor, so adjust your mentality from borrowing short to lending long. For centuries, nobody thought much about this invisible equilibrium, because life expectancy was stable at the Biblical threescore and ten -- and in fact only twoscore. But suddenly around 1900, life expectancy at birth began to rise, and starting in 1950 it entered a steep climb from forty-seven to eighty-four years. Thirty-year loans remained the extreme, however, because the proportion of those who would chisel you doesn't seem to change much. Stagecoach robberies went away, but inflation took their place. Underneath it all, governments prefer to expand the currency supply rather than raise interest rates, printing repayments rather than repaying them. Interest rates are, as they say, volatile. Within limits, they are also malleable.
Nevertheless, the expansion of longevity created a new opportunity. The long-term investment was more profitable for everybody. The upturn in interest rates was relatively negligible for the first forty years of compound interest, but progressively quite handsome after that. In practical terms, buy-and-hold became a better strategy. The difference of a tenth of a percent means little in a ten-year loan, but it can create a stupendous profit in a ninety-year loan. One suspects the interest rate on a bank loan has more to do with the debtor's working life (the period available for confident repayment) than his life on earth. In this book, we concentrate on the creditor, whose lifespan should not affect interest rates as much as it affects his opportunity to enjoy money, so long as he has some of it. But a long life without money at the end of it is a fearsome prospect, indeed.
2. Equity Index Investing. The stock of only one company (General Electric) was a member of the Dow-Jones Industrial Average a century ago. By definition, the DJII always contains thirty leading stocks; others have been replaced many times. It takes a long time to become a household name, and by the time an investor has heard the name, it is often ready to decline. Active investing, meaning sell one to buy another, was once quite necessary for success. Unless fading leaders are replaced by new leaders, however, the average would fall behind, But it is easy to see the average has moved steadily upward, so it must be actively managed by someone.
If you are careful to avoid the spongers and the fly-by-nights, the investment world is rapidly changing, mostly for the better. To some extent, this reflects a flight from the bond market which governments deal with, but most investors now think total market index funds are safer. When the Federal Reserve forces banks to buy its bonds through "Quantitative Easing", the supply of bonds goes up and so the price goes down. "Passive" investing is certainly easier for the small investor to deal with, and investors are responding.
Later we will try to take advantage of one obvious flaw in such investing. If a single investment represents thousands of companies, investor control is diluted to meaninglessness. The only effective control over management then resides in the shares which are not held by funds; and even there, more and more corporate control rests with insiders and managers. The effect of such a trend is not merely that manager salaries are inflated, but the corporation becomes less responsive to the consumer public. Its legitimate business plan is to make a profit, but to make a short-term profit at the expense of long-term profits is not so defensible. Because of the corporate shield, many corporations borrow too much, risk too much, and collapse too often, but their managers often walk away with riches. If Health and Retirement Savings Accounts really get popular (at last count, they only had thirty billion dollars invested), its counterweight of stock ownership should help restrain consumer prices. Nevertheless, experience seems to show that competition between companies has been a more effective guardian of public interest, than stockholder control of individual competitors.
HSAs collect money when it is not needed, spend it decades later when it is badly needed, and invest the money during the interval, tax-free. The longer the interval, the more it earns. And with careful application of the principles of compound interest and index investing, the earnings are considerably magnified. If your Christmas Savings Fund earns more money, it reduces the effective cost of what you buy. But if you are careless, investment fees and inflation will ruin everything. So that, in sum, is another message.
Stretching Out Your Retirement Savings
|
| Benjamin Franklin |
Benjamin Franklin was able to retire from the printing business at the age of 42. His partners bought him out in eighteen yearly installments. In the Eighteenth century, it was unusual to live past the age of 60, so Ben felt pretty well fixed. Unfortunately for this planning, he lived to be 82, so when he did reach the age of 60 he was forced to look around for postmasterships and other ways to survive, for what proved to be 22 more years.
This is the other side of a coin; on one side is written, "Protect your family in case you die young". On the opposite side is written, "Be careful not to outlive your savings", relying on the old Quaker maxim that the best way to have enough--is to have a little too much. For centuries, life insurance was sold to people who mainly feared the first, commonest, possibility, but never completely addressed the opposite contingency, which was growing steadily commoner. Annuity insurance ordinarily is sold for a fixed number of years, so insurance commissioners ordinarily require what is most probable. Unfortunately, this response shifts the risk of guessing wrong onto the subscribers' shoulders. Since science has unexpectedly lengthened average life expectancy (by thirty years since 1900, or by five years in the last ten), experience rather like Ben Franklin's has become a commonplace, but rather poor business judgment. The business remains solvent only as long as the decision to drop the policy is later than the life expectancy.
|
| Retirement Saving Debt |
There may exist insurance policies to address this issue, but few companies offer it. We will briefly describe this sort of policy, in case it becomes more widely available, but it is primarily described here to illustrate the issues to consider. If you can get it for a reasonable price, or if you can get it at all, the outline of the policy would be to set a premium and promise to pay 6% for the rest of your life. Underneath the promise is the reality of paying 6% for eighteen years as a non-taxable return of principal. Following that, you don't need to get a postmastership, you are paid a taxable 6% until you die. Presumably, the insurance company has actuaries to help with the math, so the company makes money if you live less than your life expectancy, and loses money if you live longer. If life expectancy suddenly extends much longer (let's imagine a cure for cancer appears), the insurance company is going to go broke. That's why insurance commissioners are uncomfortable with the concept, even though it is obvious how desirable it might be. So that's why annuity insurance typically states a fixed number of guaranteed years and expects the subscriber to shoulder outlier risk.
Any insurance has an administrative cost, so everyone must consider some non-insurance solution to the whole problem. Therefore, we propose you re-examine the old saw about "never dip into principal". If you don't have enough money, you can't do very much except depending on the government, your family, or your fairy godmother to help you out, although it must be obvious that all Americans would be wise to consider retiring five or ten years later than they hoped. Very likely, the government is going to have a difficult time sustaining even the present tax exemption of retirement funds, medical insurance, and social security. Those are called entitlements, but if the government eventually can't afford them, it won't matter what you call them. If entitlements keep getting extended, we can expect our nation to resemble the ancient Chinese and Indian nations -- able to build palaces in their golden era, but eventually crumbling into a gigantic slum in centuries afterward. So please, if you are able to do it, try to keep gainfully employed for a few extra years. If you do it (and some people can't) you may be able to realize the American Dream.

|
| Inheritance Tax |
The traditional American dream was to accumulate enough money to live off the income from it indefinitely, never touching principal, and then exposing the principal to destructive estate taxes after you finally die. Unless you are unusually wealthy, there isn't much left for the next generation after estate and inheritance taxes and expenses. It's a little inefficient to accumulate more than you actually need, but the government gravitates toward the least painful methods of collecting taxes. By confiscating this safety surplus, however, it declares that "Every ship (generation) must sail on its own bottom." And therefore it must acknowledge responsibility for what inheritances ordinarily pay for, like charity and good works. But there remains a quirk to this.
If Ben Franklin's partners had arranged to invest the money until he needed it, they could at least have afforded to finance two or three extra years. After inflation and expenses have eaten away at your retirement income, your principal may not generate enough income to last forever, but it is still big enough to pay for several years of retirement, which may in fact be longer than you are destined to live. Remember two things: 1) a principal sum, big enough to support you indefinitely, must be roughly eighteen times your yearly expenses. If it is only big enough to support you for fifteen years, it will seem too small until you realize you are probably actually going to live, say, five years. And 2) as far as leaving an inheritance to your children is concerned, there is a realistic probability that the government will consume most of the estate before it ever gets to the kids. These fundamental truths are presently obscured by the Federal Reserve artificially forcing interest rates to less than 1%. But if you can just hold out for a few years, it seems entirely likely that interest rates will return to 6% (meaning your principal will once again produce eighteen equal installments). But such a return of interest rates to normal levels will force the government to pay a comparable amount as interest on its bond debts (meaning it will get hungrier to escalate your estate taxes.) This isn't nearly as satisfactory a solution to the life expectancy quandary as retiring five years later than you once expected to, but you can't say we didn't warn you.
And as for what happened to Ben Franklin, you can read his will. He died a very rich man as a result of shrewd investments, later in his life. Ben left eight or nine houses, several thousand acres in several states, a gold-handled cane, and a portrait of the King of France surrounded by hundreds of diamonds. But it would not seem wise for the rest of us to count on accumulating that much new wealth, after attaining the age of sixty. The way things are going, once you attain your life expectancy, everyone should have some non-insurance plan for supporting himself for two or three extra years.
Paying for the Healthcare of Children
It has been said by others that eventually healthcare will shrink down to paying for the first year of life, and the last one. Right up to that final moment, medical payments must somehow evolve in two opposite directions. We might just as well imagine two complimentary payment systems immediately because the two persisting methodologies could eventually conflict unless planned for. Paying in advance is fundamentally cheaper than paying after the service is rendered because there is no potential for default in payment.
The two methods even result in different aggregate prices; in one case you pay to borrow, while in the other you get paid to loan the money. Dual systems are a fair amount of trouble; remember how long it took gasoline filling stations to adjust to credit cards versus cash. When gas prices eventually got high enough, they just charged everybody a single price, again. This isn't just lower middle-class stubbornness. Dual payment systems slow you down, and profit is generated from repeated rapid transactions. The buyer wants the goods and the seller wants the money. The profit comes from doing exchanges as fast and often as you can manage them.
In a well designed lifetime scheme, with balances successively transferred from one pidgeon-hole to another, it becomes possible to maintain a positive balance for years at a time (thereby reducing final prices, because the income from compound interest keeps rising toward its far end). That was a discovery of the ancient Greeks, but sometimes Benjamin Franklin seems like the only person to have noticed.
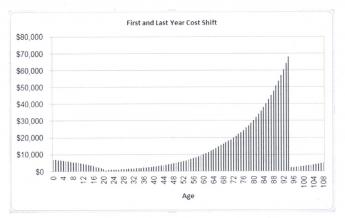
|
The last year of life is more expensive, But the first year of life may cause more financial pain.
|
However, In real-life health costs, there is one intractable exception. Because obstetrics can be costly, particularly the high costs of prematurity and congenital abnormalities, the first year of life averages $10,500, or 3% of present total health costs. It, therefore, results in pricing which many young parents cannot afford, in spite of insurance overcharges to catch up later. And thereby a multi-year stretch of interest income is jumbled up, often lost entirely. It gets worse: childhood costs from birth to age 21 average 8% of lifetime healthcare. Please notice: Single-year term insurance premiums always rise to a much higher level than a lifetime, or whole-life, premium costs, because of internal float compounds in whole-life. Modern medicine has also resulted in rising lifetime costs, with only this obstetrical exception. Someone surely would have figured this out, except excessive taxation of corporations created a motive not to notice the effect on tax exempted expenditures.
This problem obviously could be approached by borrowing or subsidizing. Someone might even envision a complicated process of transferring obstetrical costs to the grandparents for thirty-five years, then transferring the costs back to the parent generation. Since we are describing a cradle-to-grave scheme, it seems much better to imagine a single person's costs eventually becoming unified. Grandparents do in fact share continuous protoplasm with grandchildren, but before that was recognized, the courts had decided a new life begins when a baby's ears reach the sunlight. Stare decisis beats biology, almost every time. A society which already has a high divorce rate and plenty of other family upheavals probably feel better suited to the principle of "Every ship on its own bottom." -- except for this financing issue. For childless couples and parentless children, some kind of pooling is possibly more appealing, and the complexities of modern life may eventually lead that way.
|
In the meantime, lawyers, who see a great deal of human weakness, are probably better suited to suggest a methodology for transferring average birth costs between generations, and back, although a voluntary process seems more flexible. It would seem grandparents are often most likely to be in a position to leave a few thousand dollars to grandchildren in their wills, and age thirty-five to forty seems the time when competing costs are at a lifetime low, making that the best time to pay it back.
Some grandparents are destitute, however, and some parents are basketball stars. There are surely generalizations with many exceptions. The process is happily simplified by a birth rate of 2.1 children per couple, which is also 1:1 at the grandparent/grandchild level and our Society has an unspoken wish to increase the birth rate if it could afford it. For legal default purposes, matrilineal rather than patrilineal descent may be more workable. But -- if every grandparent willed an appropriate amount to some grandchild's account, it would work out (with a small balancing pool), creating a small incentive for the intermediate generation to have more children.
The answer to this dilemma probably lies in revising the estate-resolution process, making HSA-to-HSA transfers largely automatic within families, devising a common law of special exceptions and adjustments, and creating a pooling system for special cases which defy simple-minded equity. A large proportion of grandparents have an indisputable defined obligation, and a large proportion of grandchildren have an indisputable entitlement. The difficult problems reside in the exceptions and require a Court of Equity to decide them. We leave it to others to fill in the details because there could be many ways to accomplish this, and some people have strong preferences. The basics of this situation are the grandparents with surplus funds are likely to die later, but they are still likely to die, close to the age when newborns are appearing on the scene.
When you get down to it, the problem isn't hard if you want to solve it. By arranging lifetime deposits in advance, a large number of grandparents could die with an HSA surplus of appropriate size. A large number of children will be born without a standard-issue family and need the money. After the standard-issue cases have been automatically settled, these outliers can be referred to a Court of Equity charged with doing their best. After a few years of this, the results can be referred back to a Committee of Congress to revise the rules.
A basic fact stands out: most newborn children create a healthcare deficit averaging 8% of $350,000, or $29,000, by the time they reach age 21. Most young parents have difficulty funding so much, and so all lifetime schemes face failure unless something unconventional is done to help it. A dozen more or less legitimate objections can be imagined, but seem worth sacrificing to make lifetime healthcare supportable. The main alternative is to pour enormous sums into the government pool, and then redistribute them. I am uneasy about letting the government get deeply mixed into something so personal. So, speaking as a great-grandfather myself, about all that leaves as a potential source of funds, is grandpa, and even grandpas sometimes have an aversion to long hair and rock music.
Last Four Years of Life Reinsurance
Half of lifetime medical expenses are reimbursed by Medicare. And half of Medicare represents the cost of the last four years of someone's life.
Having got middle-men off our chest, we return to a search for other ways to introduce greater efficiency into the medical financing system. That might be accomplished by reducing medical prices or eliminating medical problems with the research. Rationing, however, never seems to work without distorting resource allocation, and medical research is best left in the hands of the scientists. Here, we offer a third method, which is to increase the revenue by modifying its structure, while minimizing changes to the medical system it pays for. The National Institutes of Health (NIH) research budget is already $33 billion a year, and somehow that seems like enough. Right now, our mission is seeing what might be done with the payment system to fit its purpose.
Up until recently, paying for medical care has been treated as just part of paying for anything else, but it has some special features. For example, because of a welter of scientific advances, it is possible to imagine a future when nothing except the first and last years of life will contain any substantial medical costs unless they are self-inflicted to some degree. The American public seems consistently adverse to subsidizing self-inflicted conditions, which it views as a disguised form of suicide. Since homeless, addicted males seldom have children because females avoid them, non-cohabitation of the Lizistrata sort is a hidden way of punishing them for failing to support their families. With exceptions of this sort, medical care is an expensive need which will gradually become less essential. Except the system should be arranged to accommodate unexpected changes because change itself is confidently expected to occur.
What's Reinsurance for the Last Years of Life All About? Ends of life concepts were designed to take advantage of the permanently J-shaped curve of medical costs to increase with age. They divide revenue into two investment classes maturing at different rates. The longer the period of compounding, the more we should want to save it for heavier expenses. (And the less we should be interested in spending a valuable resource on age groups with little to fear.)
Start by cutting escrowed Medicare costs into two subaccounts, differing in content and thus in timing. Overall, while all curves of lifetime health expenses are J-shaped, skewing progressively toward old age, containing roughly half of the expenses in Medicare, and half of that (one-fourth of total costs) concentrates in the last four years of life. (Later on, we will apply the principle to cover the increased cost of being born, addressing that initial upswing of the J.) There are six or eight variations, but our version has Subaccount A starting at age 25, the least expensive health year for the typical person, but also the time when Medicare withholding tax begins its forty-year climb. Our Subaccount B, by contrast, begins at birth with a major obstetrical expense, but currently must abandon this opportunity to achieve maximum compounded interest because of a newborn's lack of income. (The age group from 25 to 65 is temporarily abandoned to the Affordable Care Act until the nation decides whether to continue ACA, change its scope, or abandon it.) What follows is a description of financing everything except the Affordable Care Act, while temporarily accepting the implausible assumption ACA will seem revenue-neutral, until after the public gains full access to its books. The big data approach should speed up this examination.
Therefore leaving out ACA, and examining only what is left, Subaccount A buys out Medicare voluntarily, paying for retirement (which usually begins at the same time) with what is left over, in return for the hope of retirement income. Subaccount B pays for the last four years of life, thus removing half of Medicare cost from part A, as well as funding one grandchild equivalent until he or she reaches age 25. In effect, Account B pays for childhood, later materially helps buy out Medicare by re-insuring the last four years of life and eventually becomes the basis for First and Last Years Insurance as a pre-paid substitute for pay-as-you-go Medicare. It may take a long time to get there, but that's the goal. Meanwhile, it effectively cuts the cost of Medicare into two equal parts and thus makes it more digestible for a buy-out. (By applying different revenue sources, its timing is different in the two pieces.) During the long transition period, the payments for Medicare are divided between the two funds to satisfy obligations, one of them is extinguished, the other continuing to fund retirement costs until the death of the subscriber. It amounts to shifting the costs and revenue around, taking advantage of longer compounding for heavier costs. Ultimately, it raises questions of how far the public is willing to go with all that, including donations to another generation, and being educated it's a sensible thing to do. By accomplishing many things at once, it acquires what mathematicians call elegance, but the public may regard it as too complicated unless it is accomplished in steps.
If, during the transition phase, there still remains a deficit, consideration might be given to establishing postmortem trust funds as a fall-back to continue the interest compounding until its debts are paid, and/or conceivably pre-birth trust funds anticipating childhood costs (see below). At the moment, mandatory conversion into an IRA would be subject to tax. However, we hope Congress can be persuaded to defer the taxes until the date of death. In this way, unpaid taxes could be utilized to extend retirement benefits until they are needed, and taxes can be discontinued if they aren't needed. Meanwhile, savings continue to gather investment income. During the transition, there might be several revenue/cost mismatches which require expediency and/or bond issues, and there is no reason to see it as shameful.The substance of the following table is that the investment of $250 at birth would result in $21,714 cash for retirement at 65, plus the present value of $28,000 in Medicare premiums, plus an uncertain value for the improved structure. But this improved structure assumes no interest is gained on the premiums, and in fact, they would probably be discounted to present value. So, it seems better to sacrifice the structure for improvement in cash flow. That would be summarized as follows:
The last four years of life are not the same as the last four years of Medicare. It is only possible to establish which four years are someone's last ones after the date of death is known. The proposal here is to set one half aside as a special fund for the last four years of life because old-age health and retirement funds will generally not be needed for decades, but costs will eventually be heavy. When costs can finally be known, the Last Years fund reimburses Medicare. Some funds must be constantly consumed for medical care, and they should utilize funds which are soon to expire, and not be escrowed. Escrowed funds are usually set aside for distant medical costs, and like Odysseus bound to the mast, keep him from yielding to the temptation to use them prematurely. Meanwhile, a third, non-escrowed, subaccount is free to manage current expenses, and need not be dealt with further in this section. Medicare doesn't know when you are going to die any better than you do, so it reimburses every cost at the time it is incurred, spending revenue about as fast as it is received. Account A was designed for future healthcare costs in all but the last four years, a burden considerably lightened by removing those last four years and letting the revenue grow. The switch isn't exactly insurance, it is re-insurance. The beneficiary is then dead, and even his relatives would scarcely notice this transfer has taken place, except by auditing receipts.
When costs can finally be known, the Last Years fund reimburses Medicare.As a matter of fact, Medicare needn't reimburse the particular costs for specific last-four-years clients, since there are only two parties directly involved, both of the insurance companies. By maintaining aggregate books, Medicare merely needs to determine the average cost for all its dying patients, to emerge with equal aggregate reimbursements for everyone who dies. Whether this bookkeeping short-cut can actually be utilized, however, depends on whether variations in regional cost are too substantial for local politics to tolerate. Even then, statewide averages might serve. This detail is an accounting efficiency which the two parties could sort out with Congress.

|
|
Everybody is born, everybody dies, and nobody does either thing twice.
|
Eventually, the taxpayer under present law might pay long term capital gains tax of 25% on withdrawals from tax-free accounts; revising such tax laws is under discussion. The present value of such revenue is difficult to estimate, but it would likely be offset by the reduction of interest rates paid on the indebtedness, which is also hard to predict. And all of this would be offset by a long term rise in the stock market, also subject to capital gains tax. Since a rise in bond, rates seems almost certain at present, and thus a long-term rise in stock market averages is likely, it seems reasonable to suppose the government would make a huge profit on an expanded Health Savings Account. Only a major prolonged recession or a war would reverse this judgment, and even that would see bond revenue mitigating the stock market loss. The private purchase of huge amounts of stock would certainly raise stock prices and might put any qualms of the IRS to rest. It is true, stock market exuberance can lead to a bubble which collapses, but this observation never seems to restrain a bull market.
To review the matter, splitting Medicare payment into two escrowed subaccounts and one non-escrowed one, has simple purposes related to transitioning between systems, and really isn't that hard to understand.
1) Technically, it allows longer-term funding to avail itself of compound interest for longer periods, largely by devoting more attention to the matter and ignoring the original assignment of the funds.
2) Secondly, a transfer of $18,000 out of a million-dollar retirement fund would not meet with nearly the same resistance as it would from a fund scraping the barrel to survive. We take this intergenerational transfer up in a later section, but here it should suffice to summarize, this transfer would solve a number of problems which hitherto have been treated as issues one simply has to endure.
2) Part of a spectacular revenue enhancement comes from adding twenty years of compounding a rather large sum ($1650 annually for 20 more years) onto the end of a long period (40 years) of compounding a smaller contribution, of $825 a year. Reversing the sequence (Medicare premiums first, payroll withholding subsequently) would generate even more revenue, and advancing Medicare premiums to childbirth-to age 25, would generate the most. Furthermore, any one of these sequences follows the design of original Health Savings accounts by ultimately depositing left-over funds into the individual's retirement account, as a sort of reward for being frugal. Acquiring revenue for other insurance components, what had previously been a unique feature of HSAs for retirement, it discourages early diversion of these funds to unrelated government activities (aircraft carriers, etc.), recurring anxiety of beneficiaries. Perhaps more to the point, it gives the client a tangible reason to be frugal, at an age when such ideas are not entirely natural.
3) The proportions of the public who have already consumed, or paid for, parts of Medicare will vary with their demographics, largely related to the year they happen to have been born. But a rising proportion of cost in one compartment means a decline in the other half. Because revenue often has unexpected connections to cost, this will always be a rough proportion, but it ought to help placate the sense of helpless public disenfranchisement which attends all major transitions.
4) And finally, this new configuration approximates the way things are probably going to go anyway, with ever-increasing concentrations of medical cost pushed toward the end of life. Not everybody dies at Medicare expense right now, but the universal trend is for people to die later, eventually making it approach 100%. Further, as we describe later, it provides a framework for first year-of-life coverage as well. That is to say, the trend is for health insurance to narrow down to the beginning and end of life, as science gradually eliminates the disease. One day in the far future it might be said, nothing else is left of major health costs. Everybody is born, everybody dies, and nobody does either thing twice. Insurance as we currently think of it will slowly become a thing of the past, replaced by what is more frankly a pre-payment methodology on a much grander scale. And eventually, the public will see it happening, which eases political resistance considerably
(1) Medicine at the Two Ends of Life: First year of Life, and Last Years of Life.
Benjamin Franklin founded the Ivy League's University of Pennsylvania, but he was surely no academic. He was a practical man, looking for practical results, and some of the fiercest battles he fought concerned the direction and purposes of his University, especially the nature of its mission. At a time when most Ivy League Universities were mostly divinity schools, he would not Pennsylvania tolerate it that way for his own, and to this day the University of Pennsylvania has no divinity school, although it does have something very close. If there had been such a thing in his day as a Nobel Prize, he would have won it for his achievements in electricity. In the centuries-long journey from divinity school to occupational credentials, Franklin's position and the general academic position have drawn marginally closer together. The first academic course in science was only taught around the time of the Civil War. The term "philosophy" would now be used as a word for "science", and a Doctorate of Nuclear Physics would puzzle most physics majors, even though they aspire to achieve that Ph.D. degree. The American Philosophical Society is quite definitely a scientific society, and most definitely was founded by Benjamin Franklin. These were not idle arguments in the Age of Reason.
To speak more practically, a great bulk of scientific achievement consists of experiments to reduce complexity, and ultimately to reduce costs. No doubt there are scientific discoveries of new fields, and probably the greatest prestige attaches to those who uncover some totally original feature. But the surprising bulk of the effort is devoted to simplifying and reducing costs. If a scientist employed by a big company should discover some cheaper way to do something more simple, he will be rewarded, and it may well make his career. If he discovers how to solve a mathematical equation in significantly fewer steps, his accomplishment is described as "elegant". That's the nature of science, to accomplish a goal, no matter how complicated. To make it profitable, you cut out a lot of the fumbling and get right down to the nub of a solution, with fewer steps, and cheaper materials. If you are unsatisfied with this generalization, just compare some random salaries of chemical engineers, with theoretical chemists.
There's even a story they tell in England about Franklin and King George. It seems lightning struck the steeple of St. Paul's Cathedral, and quite naturally the King consulted with Franklin about a lightning rod since Franklin lived a few blocks away. The King wanted a brass ball on the top of his church. Franklin made the rare miscalculation of openly disagreeing with the King. "No, your Majesty, it should be an iron spike. " The English implies the story depicts a foreign printer telling the King what to do and was, therefore, himself a fool. The American version of the same story would have it the King was a fool to tell the greatest living expert on lightning rods what was what about lightning rods. The founder of the American diplomatic corps probably would never have chosen such words, but "Who the hell do you think you are, telling me what is best in lightning rods", would probably summarize it. Well, America and Great Britain fought an eight-year revolution over this difference in attitudes, and so it seems likely Franklin and the Trustees of the University he founded, used stronger words that are now reported in alumni magazines.
The moral of all this is, no matter how silly the argument seems to strangers, the protagonists sometimes feel strongly enough to make trouble for those who do not accord their views proper deference. The fact Franklin acted in such an out-of-character way, is probably proof of how strongly he really felt about it.
So, to sum it all up, it is an American trait to acknowledge start-up costs but to surmise that in the long run, it's cheaper to eliminate a disease than to count the cost of curing it. No one knows whether research will lead to eliminating the cost of disease, but most Americans will presume it will, and most Americans will somewhat minimize the time it will take to accomplish it. We imitate the attitudes we suppose our mentor must have had, and indeed he may well have had them. The logic of the matter will only take you so far. At the rate we are going, I feel we might eliminate most diseases within the span of the next century. I feel medical costs a century from now will be -- not just could be --eliminated except for the cost of childbirth and death. You may disagree; no one knows. That's why participation in a long-term program to deal with the matter, should remain voluntary until the outcome is clear. In matters like this, everyone tends to overstate his case. Therefore, no one is entitled to force others to swallow their doubts.
The Future of Index-fund Investing, Itself

|
| Bank Collapse |
An abundance of threatening international situations might unexpectedly lead to a banking collapse, but since every bull market "climbs a wall of worry", it isn't a threat unless it happens. The introduction of a new international currency is either never going to happen, or it is going to be needed without much warning. It's needed in the developing world, but there's a long way to go before it topples banking systems in the developed world. At the moment, nation-wide index funds might make a perfectly satisfactory currency substitute, like the Spanish pieces of eight. Index funds are tested and available in huge amounts and trusted by everyone who talks about them. They are growing fast and may eventually dominate choices unless something even better comes along. If something better comes along, it is hard to see why we couldn't let the market replace them as fast as people want to buy them. In any event, we have tons of gold as an inert reserve. The question is, will they hang around in their present form long enough to be a useful tool? At the moment, bitcoins are the popular rage to make people rich, but most people feel a secret currency is a good way to make people poor.
|
| Stock Certificates |
Of course, no one can answer such a vague question about a vague future for a vague development. But index funds are essentially nothing but bundles of stock certificates which are easy to buy and sell, easy to lock in a vault, and easy to carry. They have real intrinsic value which can change with the economy and whose value can be checked in an instant. If something better comes along, it's hard to see why you couldn't buy it with index funds. It's hard to see why two or more currencies couldn't co-exist, particularly if the co-existence was temporary and brief. It's hard to see why it couldn't be limited to central banks, who support local secondary currencies with instantaneous appraisals of the mark-up premium. On the other hand, it's hard to see why it couldn't be divided into subunits and carried around in everyone's pocket, if that's what is chosen to do. Since we got along with Spanish doubloons for centuries, it can be assumed it will serve the purpose. Since ownership is registered, it's even got one certain improvement: you can lose it or have it stolen, and still have a way of getting a replacement. In a sense, that was Robert Morris' contribution to currency theory: if a wooden boatload of gold sank, it was gone. But if a boatload of gold certificates sank, the underlying gold was still safe at home.
|
| Charles de Gaulle |
Resistance from those it would put out of work can safely be assumed. Just scratch any regulation, and you will find a lobbyist, usually very well funded. But the hardcore opposition would be from those who see that the currency has real value if you own it legitimately. Its value as a currency is that it is a real value, a piece of the economy, which you can carry with you anywhere. It, therefore, upsets the principle of national boundaries established long ago by the Treaty of Westphalia. If you want to defend this fact, you will say you could buy the country that way, by imagining a horde of "tourists" who open their knapsacks and demand what they bought, which is your economy. Some elderly people may remember the French battleship which Charles de Gaulle sent to New York harbor to demand his gold. It wouldn't take very long for that to be disruptive, as the more recent Irish experiment with lowered tariffs also graphically demonstrated with migrant corporations. Eventually, even the United States had to make itself competitive with the 12.5% tariffs of the Irish Republic. You will find, even though it is denied, that nations with weak economies don't want to be rescued by richer countries, so they will cook their books. Portable ownership of the means of production is not merely portable socialism, it is portable ownership of a corporation which may be indefensible legally, therefore leads to war if you try to exercise the right. So unless simple prevention can be devised, sovereignty is the one thing this money won't buy, even with Brexit. It might someday seem useful to prevent economic sovereignty as well, and for that, we must look to what the European Union devises for its individual component nations since they don't want to adopt the American one. With the exception of the Civil War, we managed to buy our way out of trouble by having rich states support poor ones, since we are all Americans, right? Until we reach the point of industrial states getting along with slave states, it would be better to have national currencies, based on national economies, type unspecified.

|
| Treaty of Westphalia |
Until someone figures out a solution to that issue, a confederation of national currencies based on index funds is about the best we can offer as a short-term solution. You can gamble on long-term stability, but it's your risk to do so, just as it is today. Short-term is worth something substantial, however. Reducing the cost of trade would almost surely inject several percents of GDP into everybody's economy, net of the cost of doing it. It should be the basis of a bull market, for quite a while.
Tax Legislation--Just A Condominium Squabble

|
| Constitution |
Congress meets every year and, almost every year, most Americans are more interested in athletic games. People who make politics their profession may be more involved more of the time, but eventually, it is taxes which supply the force to involve the public. Occasionally it is the Constitution, but the Constitution mainly establishes structure, and people are generally satisfied with the present structure. There is limited time for debate, and to tell the truth, limited patience for it so the party leadership is left with the power to manipulate timing around holidays And the leaders organize the limited "floor" time carefully to preserve their control of it. Right now is one of those corners of our time, when an important issue gets crowded next to a holiday recess, the issue gets explained to the public, and public opinion is closely divided at first. It all sounds familiar, but there are important particularities.
Everybody is affected, everybody thinks he knows what George Washington thought. We had once just finished the Revolutionary War, almost losing that war because we had so much trouble agreeing to tax ourselves, to defend and govern ourselves thereby. When the Continental Congress abandoned Philadelphia to the British in 1779, only Robert Morris stayed behind as acting President, and never forgot the dreadful experience of governing without a government. In fact, about five future Constitutional delegates were trapped by an angry mob in the upper floors of James Wilson's house at the so-called Battle of "Fort Wilson". There was no need for these patriots to debate later about the need for taxes, law or order. This experience settled the tax issue for them, permanently.

|
| Revolutionary War |
A whole host of tax issues are vitally important to someone somewhere, but the tax issue dominates almost all three hundred million citizens of every age and occupation. lowering by how much is desirable for corporate taxes, and lowering by how much is ideal for federal taxes shared with state and local governments. Corporations were then a new and unanticipated way to run a business, and generally, a more efficient way, although not a perfect one. About half the country half-believes it is urgent to go in opposite directions on details and divide in opposite directions on a subject, but the other half is suspicious of some hidden agenda. There probably isn't enough slack in the systems to do split the difference. If we try to change, we dispute how much to change. In this case, we have the example of southern Ireland, which went too far in lowering corporate taxes to 12.5% in a single step. It seems simple enough, but we dispute who gets the credit, and most of the leadership is fearful of getting too far ahead of the public. The Civil War is the only time in our history when compromise wasn't sufficient, and in retrospect, it probably might have been handled without a war.

|
| The Civil War |
The result needs improvement because of repeated patching, so simplification is desirable but not paramount. It would be nice to stop gerrymandering, but no one proposes a feasible way, as is true of the narrow balance between the two parties. It is clear that the Congressional power of the purse is weakened by overspending the budget and then demanding that we avoid a default by funding an unauthorized deficit. Since it is unclear how to accomplish these three structural approaches peacefully, we probably can't do them. So we will probably resort to half-measures, with fuller measures after we can see what happens. The risk is that the North Koreans, or the Saudi princes, or the defeated Russians, or some other foreign power will solve the problem for us in the meantime. This approach amounts to buying some time by surrendering some control, and we may be sorry we did it. But we keep on building more condominiums, so it must have some utility.
Broad Brush
Other Voices: Rethink Lifetime Health Finance
Barron's recently invited 1000-word summaries of radical change proposals. tg.donlan@barrons.com
Health insurance financing is a gigantic wealth transfer system. Politically, it is described as a transfer from rich to poor. But it really is a transfer from one age bracket (working people) to two non-working ones, children and retirees. Add thirty years of longevity by curing the diseases of one age group faster than another, and the balance between age and wealth distributions gets bent out of shape. Socially, it's dangerous. It gets even worse to base one-year casualty insurance on employment, tempting employers to dump a system which ends when employment does patch together by tax incentives. Average employment duration is around three years, so almost every condition soon becomes a pre-existing one, whenever employees lose their insurance. Insurance companies see what's coming, and cannot be blamed for getting out before it collapses.
More revenue would help, but existing sources are almost exhausted at 18% of GDP, while a rapid change in health delivery would flirt with disaster. But one thing remains: using the idle money in pay/as/you/go to fund a transition matching a change in spending incentives, or even scientific research eventually eliminating the disease. It would work with income returns of between 3-7%. Compound interest on money already collected would pay the deficit. Extension of the age limits on Health Savings Accounts would stop the borrowing, and trust funds would extend the compounding for 21 years past the average age of death upward, to the point it would far exceed the need for retirement funding through taxation or borrowing. Transfer of $4000 of each grandparent's HSA surplus (at death plus 21) to the HSA of one grandchild would add another 21 years to compounding downward, leaving several millions of dollars per person for retirement, curing a number of social turmoils in the process. That probably wouldn't happen completely, but a Medicare surplus rather than a deficit would allow any transition to be much speedier. The present 2.9% employment tax presently collected from working people would equal or exceed what is needed if compounded. Since the new fiscal limits would be enforced by the laws of mathematics, there would be far less temptation to spend it on battleships. Further extensions of longevity would increase revenue faster than inflation could undermine it. Essentially, it would be asked to match 104 years of compounding--with what took 42 years to accumulate. There's plenty of slack if you try those simple numbers on a free compound interest calculator, found on everybody's Internet. A second chance to do what we should have done in the first place.
True, the necessary change in incentives would come from unifying three systems into one lifetime one, incentivized by noticing the remarkable savings already created by millions of Mid-Western subscribers to HSA. A few sentences of amendments to existing law should be all that Congress needs to struggle with since these are existing programs. Whereas the R's need to see a single-payer system has become a single-saver system, the D's can save face by asserting they are the same thing.
George Ross Fisher MD 3 Haddon Avenue South Haddonfield, NJ, 08033 Cell 215-280-6625 office 856-427-6135 Email: grfisheriii@gmail.com
Retirement Communities
Prior to the Second World War, old-age homes were almshouses, slightly modernized. Since few people lived very long after they retired, the old-age home took care of a few stranded old folks unable to care for themselves. The places were depressing and sparse, with a characteristic odor of urine and poorly-ventilated kitchens. But when time spent in retirement lengthened to twenty or more years, a new dynamic had to be considered. The dingy old single rooms changed into multi-room apartments, the dining room went upscale, and the infirmary changed into a skilled nursing facility. The idea was, you could graduate to more specialized medical care when you needed it, and be visited by your friends in the community who would someday be in the nursing facility themselves. They were paying to keep it up, and they would raise a ruckus if the infirmary service began to look uninviting. Whether the community was paying for it collectively or the younger generation was supporting it, the Retirement Village provided a more civilized way to grow old and die.
|
THe CCRC falls somewhere between a college dormitory and a resort hotel.
|
People chose these places for a variety of reasons, depending in large part on what they could afford. Widows are often overwhelmed by maintaining a house, widowers are often overwhelmed by cooking. And retired couples are often simply tired of both chores, or sufficiently crippled or befuddled enough to look for a way to give those tasks to younger people. One system grew up, of acquiring a second home in a vacation area and then replacing the main house with an apartment in a retirement community. If you stay in the vacation home for six months and one day each year, certain combinations can lead to appreciable tax savings. Sometimes a married couple is in perfect health and uses a retirement community as a comfortable suburban apartment complex, "just going on living the way we always did". The idea in their mind is the folk wisdom that you need to get used to a place and develop a circle of friends there; to do that, you ought to be less than eighty years old. When that's a general idea, it can be self-defeating to join a group of friends with pooled meal tickets. Thirty friends, or fifteen couples, can each host a party for thirty, once or twice a month. Unfortunately, they are quickly sequestered and disliked by everyone else as they make the regular rounds of nightly parties; but this sort of thing happens in upscale places, the kind of retirement community where some apartments have servants' quarters, and nobody much cares what anything costs. For people in this circle, the most detestable thing about a retirement community is the pressure to have dinner at 5 PM. Early dinner is ordinarily the surest sign the place is managed primarily for the convenience of the employees, but it can also mean there is nothing else to do except watch prime-time television.
|
| Retirement Funds |
For most people, however, even having ample funds for retirement is constrained by the uncertainty of how long the retirement will have to be, how much must be held in reserve, even at age 100. The gallows humor continues to repeat some version of trying to plan a way to spend your last dollar on the last day of your life. It isn't just how long you will live, it is how. If you or your spouse become blind, or bedfast, or in chronic pain, your level of living is going to change and your daily expenses may rise dramatically. Even if you never gave such gloomy things a moment's thought, the experience of eating in the same dining room with several hundred elderly acquaintances soon teaches all the lessons of unexpected illnesses and weekly funerals. Some people cannot bear the idea of living in such a community, for precisely the reason that it becomes impossible to kid yourself. And one thing no one can kid himself about is the reality that you have to have one awful lot of money before you can ignore the need to watch your pennies. And it isn't just your spending money; it's also the lack of a basement, attic, and garage in which to expand or from which to draw reserves, or just to enjoy old books and mementos buried in dust.
Retirement communities seem to have developed independently in the Quaker suburbs of Philadelphia, and along the California coast. Except for the climate, there isn't much difference. More tennis in California, more trips to the theater on the East Coast. The early communities had a strong focus on finances, which assumed a lifetime retirement fund derived from selling the family home. The fancier the house, the more elaborate the apartment it would finance. As the duration of retirement grows progressively longer, roughly three years every decade, it is certain that the sale value of the average American family home will get progressively stretched to extend to the average age at death -- especially if you focus on the average age of the second of a couple to die, or become blind, or become bedfast.

|
| CCRC, Continuing Care Retirement Community) |
So, the patterns of financing are changing, at least experimentally. Some retirement communities (the term is are purely rental, partly room and board, extra charge for the nursing facility, or a la carte for all services. People who enter any sort of community are often planning to move to a different one after a period of time, either to adjust to their reduced physical capacities or changes of location of their families. Some of them actually say they plan to live luxuriously and then move into their children's houses when the money runs out, although it is usually hard to know how seriously to take such comments.
Obviously, what is needed is some sort of insurance mechanism to pool everybody's risks, but there is a fundamental problem. Insurance companies make a big profit on life insurance in two ways: either from clients who drop the policy before they cash it in or from premiums which underestimate the actual age of death compared with the average experience at the time the policy was taken out. But in the retirement case, essentially all policies mature at death and the duration for compounded investment is brief. So such insurance is either overpriced or unobtainable. The same underlying phenomenon affects Medicare and explains its impending insolvency. Those early retirement communities which based their charges on the assumption that Medicare would continue unchanged are repeatedly stranded when Congress cuts back on Medicare benefits. Someday, demographic trends will level off and insurance can be restored to practicality, but that time is certainly two or more decades away. Many states, including Pennsylvania, have passed laws that residents of retirement communities may not be evicted if they become impoverished, so the communities are forced to be strict about advance funding. Ultimately, the danger is that the community will be forced out of business, stranding the occupants. With so much time available to discuss such matters in a common dining hall, occupants of these facilities can become obsessed with the need to save for the future, and no one can be certain they are wrong about it.
What Long Term Thinking Looks Like.
Let's apply a Due Diligence approach to the technical steps of this proposal. That is, skip past the overwhelming detail of existing data, to focus on conclusions to test. First, divide the population into three groups: dependent children, the working age group, and retirees, and start with Medicare. That's ignoring the advice that Medicare is the "third rail of politics--touch it and you're dead". The easiest place to begin is with the elderly, because they have the greatest medical cost, and anyway if we continue to "kick the can down the road", we are admitting defeat before we even start. Medicare is not only where most of the costs are, but predictably where they will migrate further. It's only half paid for by the recipients, while a major goal is to break even. Indeed, as science cures diseases, surplus should be consumed into a retirement fund, so realistic projection errors could overstate the revenue. As the old Quaker observed, the best way to have enough is to have too much.
The Composition of Medicare. With the single important exception of disabled persons, Medicare eligibility is age-related not income-related. Everyone between the ages of 65 and death (averaging now 84 years) is eligible, regardless of finances. We also contemplate funding children out of this source by transferring 5% for them. It's not much, but it is central, and it dramatizes the cost distribution. The raw data is blindingly comprehensive, sometimes to the point of obscuring important conclusions, so rather than starting with it, we should come back to data after we see what we need.
A fair working assumption is that Medicare borrows about half its costs, while Medicare totals constitute about half of total medical costs. So at least a quarter of all medical costs are already indebted. Medicare's actual sources of hard revenue are about evenly divided between payroll deductions from future beneficiaries, and premiums from existing ones, or about an eighth of total costs, each. So about twice as much is borrowed, as pre-paid in wage tax (one-quarter of total cost borrowed, versus one eighth pre-paid). Since lifetime costs are estimated by actuaries to be $350,000 in year 2000 dollars, the problem is to take $42,500 and turn it into $85,000 in 21 years in a post-mortem trust fund--seemingly at only half the rate of a reasonable rate goal of 7%. Average costs are even somewhat overstated because the 9 million disabled come from younger age groups who also contribute less than average. Furthermore, leftover revenue would probably be available for covering gaps in healthcare coverage in other age groups, as yet to be decided by Congress. You might cover these gaps by doubling the wage withholding tax, but it would be uncomfortable. Our proposal is to substitute compound interest principles, which are harder to explain, but easier to accept.At present, the Health Savings Account is the only medical payment system which could adjust to the predicted migration from healthcare to retirement care, and it is the only component which could then fund all children with about a 4% carry-over from each grandparent to an average of 2.1 children per mother. HSA currently provides for money still left in the account at the time of achieving Medicare coverage, to flow into an IRA which can be spent on anything. If you are lucky with health problems, you can even seem to use the same money twice. That's something to brag about, but it could be made even better. Right now, for a system hoping for millions of subscribers, it is too rigid and uniform. The idea of post-mortem Trust Funds (see 1b) somewhat smooths this out as well as generating a four-fold increase in revenue. Money is left over from Medicare for retirement, and then if there is no debt left over from retirement, you do not need a Trust Fund. But flexibility would be particularly useful during the transitions; some will need it, some won't. The fact that you don't know in advance, enhances the ("Old Quaker") incentive to overfund the balances.
I see no reason for HSA/IRA migrations to be so uniform, so one-size fits all. Surely there will be subscribers who would prefer to accumulate funds for later life, rather than as soon as possible. There is no reason to demand that everyone be within a certain age group or to stop depositing at a certain age. If there is some such reason, it ought to provide for a court or agency to approve exceptions. The same court could handle the vagaries of marriage affecting grandchildren (see 2.0, below).
For example, there is even no reason to terminate accounts at the time of death. The transition will uncover numerous exceptional situations, and some people would even want to create an HSA at age 64. If they want to do it, why spend hours figuring out how someone might somehow game the system with his own money? If their parents can fund an HSA at birth, why not get started twenty years sooner and add four times as much accumulation by age 21? If there must be disincentives to accumulate money, apply them after the termination of the Trust Fund, when family responsibilities are mainly (but not invariably) coming to an end.
Growth. Money at 7% doubles in ten years, so one specific proposal is to re-direct the money already being collected during 60 years, doubling it during a gradually declining 104 years. The money must earn 7% within a Health Savings Account if it is to pay for Medicare plus a million dollars per person left over for retirement. (Bear inflation in mind, however: money at 3% gross might not grow at all.) Compounding should start early in life, remaining in one continuous storage location for as long as possible, with escrowed compartments for specific goals, like buying out or consolidating shorter-term vehicles and anticipating some marital ones. Tweaks to current Health Savings Accounts will suffice but must be at least mentioned in the legislative language, to guide the long-term regulatory one.Only a few present limitations on HSA prevent this lifetime compounding from beginning immediately, and 7% annual returns are expected back from financial intermediaries over the longer term. Even though raw stock market returns have averaged 12% annually over the last century the financial community will probably object to 7% return for the customer from total market index funds because of its 3% inflation assumption within the middleman portion, and the intermediaries have already shown they resent the security measures. (Fear of the trial bar probably plays a role in fiduciary disputes.) But the reward for winning the lobbyist war is funding half of the shortfall deficit by placing risk on the proper shoulders. Two principles guide revenue enhancement : begin to save early, and relentlessly escrow inescapable life goals. Benefits from careful adjustment of terms with legal permission might range all the way from doubled returns, to cutting them in half.
Running through this dispute with your financial advisor is the need to use the "annual total returns" on major domestic total stock market indexes as a benchmark to be exceeded to escape penalties for ethical misbehavior. The principle in Law is well established that if there is no injury, there is no case.
1. Creating Revenue Instead of Floating Bond Issues.
The underlying problem is to fund retirements after you have funded Medicare when both of them begin at the same time. Suggested technical steps now follow, trying to co-ordinate designated approaches as beginning with as little amendment as possible, until the fate of the Affordable Care Act is decided. Beyond that, it is a possibility that, if the tax exemption of employer-based insurance is equalized, funding might become easier for the other half of the employable population . At the time of closing down the trust, there are only two eligible recipients, the Medicare Trust fund, and the IRS, so it usually makes no difference how the Government got the money during the long transition phase, and the extra administrative cost would be considerable.
1b. Post-Mortem Trust Funds. Some parts of this proposal are not obvious, and should at least be mentioned in the statute to guide the subsequent regulatory phase. For example, I see no good purpose in limiting Health Savings Accounts by age or occupation. Expenditures from these Trust Funds should only pay off Medicare-related debts. This trust fund concept alone would quadruple available revenue (and beneficiaries during a transition.) The Health Savings Account already devotes any surplus after 65 to a retirement IRA; why not make the timing optional, and hence more flexible? Underneath any regulation you will usually find a lobbyist.
The transition from our present system to a better one will be the biggest problem; why make it harder to manage? If someone is aged 64 when the program starts, why not give his estate twenty more years to invest and retire when it judges he can afford it? With a trust fund, if he is dead and has money left in the account, why write off his retirement debts immediately after he dies? The money in a trust fund will continue to grow until it becomes perpetuity -- one lifetime plus 21 years. That means his estate will have four times as much money to pay his debts--what's the matter with that? The central point is to expand the number of people able to pay back what they owe -- to the government; who cares if they are alive or not when the money is paid. Effectively, an index-fund certificate is funding an escrow account. Why not "take delivery" of the certificate by the creditor, whether or not the debtor is alive? The result would be many more funded accounts, not more bad debts.
1c. Last Four Years of Life Reinsurance. Alternately, a more complicated 50% partial buy-out of Medicare could continue present systems at half price. Eventually, the cost can be adjusted from actual payment histories, both individual and collective. The outcome might be having the transition time by pre-payment and repayment to Medicare at death, as well as replacing a liability with an asset. This is hard to explain, and post-mortem trust funds are probably politically preferable.
1d. Revenue Estimation By Exclusion. This discussion envisions lifetime coordination, but since future revenue is uncertain, adopts the temporary hypothetical that ACA is revenue-neutral. Like Frank Sinatra's song about "making it" in New York, if the idea is feasible without ACA and/or tax exemption revenue, it surely would be even more feasible with those two Laws adding revenue. Without such revenue, this proposal still addresses the majority of present medical cost but would need to be endlessly integrated with whatever emerges from ACA. One tweak is apparent: catastrophic insurance is mandatory in an HSA, but there may be long periods of employment or marital situations when a lifetime depositor has two health payment systems at once. Therefore, if a Health Savings Account has not made a health payment for a year, the premium for catastrophic coverage should be waived for the following year, substantially reducing its overall cost. The underlying assumption is that when you have two health insurances, you especially don't need two reinsurance. To pay the premium by the HSA itself would greatly ease this problem.
1e. Steadily Improved Longevity v. Steadily Greater Retirement Cost. For the first time in history, longevity has increased by 30 years in a century, followed by 3 more years in the past decade. That's a good thing, of course. But someone neglected to plan for increased retirement costs, in some ways a "bad" thing, directly caused by living longer. That is, while the present working third of the population is paying for its parents, the cost of transition will double in size, but costs of the retired third who benefit may increase tenfold. By that time, the contributors will evolve into becoming retired beneficiaries without employment, so revenue will not increase tenfold, and the situation becomes impossible to correct. The imperfect precision of these projections is irrelevant to their gloomy conclusions. Furthermore, the interests of the citizen and his government will often get into conflict, an inherently disruptive situation which interferes with solutions.
2. Grandpa Pays For Grandchild With Newly Created Funds.
A vexing parallel situation is the location of children in the scientific cost curve. Medical costs for children may sometimes seem impossibly high, particularly if obstetrical costs are lumped with them. But they are really quite small when compared with the late-in-life compounded revenues of retirees. In our plan, the money is newly created, belonging to no person, so it can be shifted with less resistance. Costs of children are disproportionately troublesome because of their timing within the context of their entire family. Politically, they insure a lot of people at not much insurance cost, so expect a lot of new children's hospitals to be built if they are insured.
2a. Shifting the Cost of Obstetrics and Pediatrics From Mother to Child, and Having Deceased Grandpa pay the Bill. The lifetime medical cost curve is J-shaped, with the lowest point at about age 17, rising steadily until death averaging age 84. The shape of the J-curve is emphasized by half of Medicare cost being experienced during the last four years of life. (This conclusion is blurred somewhat by adding 9 million younger disabled to the Medicare rolls. That adds to lifetime average Medicare cost, appearing to portray lifetime cost as even more J-shaped.) Even accounting for the distortion, financially struggling young parents have a hard time managing medical costs, made even worse for unmarried mothers. Middle-aged women often have gynecologic costs which lack a satisfactory resolution if they also have marital financial problems. Most of these distortions are artificial. Stripping them away by assigning them to the child would expose a steeper incline to the J-shaped cost curve of both sexes. From a politician's standpoint, equalizing medical costs of the two sexes would soften some political noise, by reducing employer costs, reducing female wage inequality, even affecting immigration by raising the citizen birthrate.
2b. How Is Money Transferred from Grandpa to Grandchild? The answer is simple: it is transferred from HSA to HSA at Grandpa's death, or Grandchild's birth, as a 5% transfer. The math means one transfer suffices for 2 grandchildren, at a 2.1 birth ratio.
3. The Working Age Group From 18 to 64.
Our basic position is simple: we ignore the working age group until business and government reach an agreement. Meanwhile, we treat both Obamacare and Employer-based insurance as unchanged and revenue-neutral, while fervently hoping for some surplus revenue to reduce the cost of the dependent two-thirds of the population. Employer groups have resisted being taxed for indigents since long before the Affordable Care Act, arguing that hospital cross-subsidies were already more than their fair share of charity. We hope things will evolve as two new systems, one of which is an HSA with temporary waivers of catastrophic premiums, but both employer groups and ACA have regarded their negotiations as nobody else's business. Blue Cross seems to be taking a cautious look at HSAs. We wish they would read one of John Bogle's books.
3a. Employer Donated Employee Groups and Tax Implications. Two other vexing laws stand in the road of peaceful resolution. The first is the Henry J. Kaiser tax loophole, apparently the largest tax loophole for individuals of all time. So much profit is at stake, one scarcely blames big business for trying to extend it, but it seems nevertheless un-Constitutional to permit a tax loophole of this size to persist for 70 years for half the population, while stone-walling extension of it to the other half. It is as though no one could read the "equal protection" clause. There is little doubt the fairest solution would be to abolish the health-insurance double tax exemption for everyone, but the resultant confounding of world trade prices would be daunting. The simplest solution is to have Health Savings Accounts pay the catastrophic insurance premium, thereby extending a full tax exemption to everyone. That maneuver would reduce federal revenue, which would then have to be adjusted in the coming Tax Reform legislation.
3b. Big business seemingly has no pre-existing condition problem, but in fact they avoid hiring impaired people to avoid this issue if they can, leaving it to their smaller competitors to wrestle with last hired, first fired. So a small issue became a big one; in a sense they created it.
3c. Medicaid: A Special Age Class Trying To Become An Age-Independent Income Class.
Finally, there is the Affordable Care Act, with missteps addressed. Medicaid was originally a state-sponsored program for mothers and dependent children. The Affordable Care Act tried to expand it to all poor people and met with mixed success in different states, so Medicaid expansion potentially invades the working age groups. It is uncertain whether the nation can afford expansion, and its fate probably depends on the decision, possibly on constitutional grounds. If healthcare is ever to pay for itself, extra funds must ultimately derive from the working third of the population. (Children have no means to pay for future care, while retirees are largely without working income until the very end.) In this analysis, we treat the net cost of the age group 18-64 as revenue-neutral. That means this one-third of all inhabitants must generate its own costs, plus enough surplus to cover the deficits of the other two thirds who are dependents. Reduce the dependent cost, and you will reduce the strain on the employee group. Furthermore, the J-shaped medical cost curve means most new costs will increasingly arise among retirees. Already, Medicare is 50% subsidized, and then re-borrowed with bonds. That means it is already 50% laundered and can scarcely stand more burden. It is very difficult to make long-term plans when the finances of ACA are so obscure, and its margin for error so narrow. In one form or another, we repeat this performance every time political control reverses. The private sector could not survive without a better form of "due diligence" than this. I suggest the President immediately assemble a due diligence team for his own information, mostly consisting of accountants, to give him the news, however bad, of where we stand. And then, ways must be found to extend the "surplus" from employed people to the unemployed two thirds, stretching a tiny surplus to meet a big shortfall. Without that tiny surplus, medical finance is close to a cost spiral.11. The final point to be made concerns Subsidies. The foregoing discussion focuses on Payment Structure. Whoever considers costs must add the cross-subsidies which shift real costs from poor patients to insured ones. At first, reimbursed systems appear cheaper than straight-forward ones, simply with prices re-named reimbursements. But be sure to include subsidy cost before deciding which structure is really cheaper. If you want to subsidize this system, go right ahead.4. Constitutional Issues.
For the most part, the rest of the uproar about the cost of medical care is mostly man-made, thus seemingly should be negotiable. The problem with this attitude is the man-made problems are so numerous and of such long standing, they appear more intractable than one would suppose is realistic. In the first place, the Tenth Amendment of the Constitution clearly makes the licensing and regulation of medical care reside exclusively in several states, even in spite of greatly increased nation-wide transportation. Both specifying state regulation (for instance, the McCarran-Ferguson Act) and national regulation (ERISA) are so clear and carefully worded it is hard to guess why both have not been challenged, or indeed which side would win an appeal. The Maricopa 4-3 Supreme Court decision clouds judicial resolution along anti-trust lines. Reams of legislation by State Legislatures suggesting one organizational pattern, and voluminous Congressional legislation suggesting the opposite, allow the citation of precedent to be almost anything. Certainly, no one wants another Civil War.
5. Pay As You Go. A major mistake was made in 1965 when Medicare adopted the "pay as you go" system. The program might never have started without it, so Lyndon Johnson cannot be exclusively blamed. But the first year recipients were enrolled free to the beneficiaries, and since then, revenues have been spent as fast as they are generated. No interest was generated on this enormous foregone revenue, and the recipients are now dead. Continuing revenue consists of payroll withholding of 2.9% of income during working years. It also consists of premiums amounting to a similar total. Before the books were scrambled with ACA subsidies and $30 billion for "meaningful use" of electronic medical records from the stimulus package, this revenue source would almost have paid for Medicare if it earned 7% income. At present, it will have to be amortized. I suggest we change the recipient address on the envelope of this revenue, from Washington DC to individual Health Savings Accounts, who would then employ John Bogle's system of passive investment of index funds, hoping to achieve 7%. In time, the numbers could be adjusted to be revenue precise. When the due diligence team reports the equilibrium state of affairs, further adjustments will have to be made. They won't be revenue neutral, but we are starting 70 years late.
6. Substituting Passive Investment for Pay/Go. So far, we have only explored one approach to paying for lifetime healthcare for everyone -- take the money already being spent on Medicare, deposit it into escrowed individual Health Savings Accounts instead of milking it for pay-as-you-go, when index investing could on average double it at 7% tax-free returns in ten years (sixteen-fold increase in forty years, thirty-two in fifty years, etc). Doubling its revenue should make it self-sufficient, easily surpassing almost any expected inflation after a ten-year transition. Because Medicare costs are age-stratified, not income-stratified, this heaviest of Medical costs now subsidizes no other age groups except disabled persons, so paradoxically, voluntary participation is facilitated.
7.The hardest thing to explain to non-mathematicians is the power of compound interest to increase virtual interest rates, a concept that baffled even Aristotle. Essentially, compounding explains why increasing longevity steadily increases effective interest rates, a saving grace for this whole idea for beating inflation. In fact, this saving grace increases effective interest rates after age 60 by so much, that paying for a grandchild's health cost is fairly trivial, compared with the struggle their young parents might endure. A five percent dollar transfer would hardly be noticed by grandpa's heirs at age 84, whereas it might seem an insurmountable amount to his young children, acting on behalf of his grandchildren. Simultaneously protecting grandchildren and grandparents with a single rearrangement may strike some as fraud, but it isn't. What's really strained are two things: convincing 300 million people to do the simple math quietly, and to keep the custodians from spending the boodle, whether on stockbroker income or on aircraft carriers. In fact, I have omitted much mention of "last year of life re-insurance" as unneeded, but to be held in reserve in case a chaotic transition requires shortening.
9. There are other approaches to paying for medical care, and we may need them all. In addition to earning income on idle cash balances, we could thus display the cost of care by moving most patients from the hospital to the home or retirement community, and exposing the internal cost subsidies (usually transferred through indirect overhead charges). The wrong people are doing the medical commuting; shifting the center of care to the retirement community, along with doctors' offices, laboratories and parking lots, would reduce costs by reversing the commuting. Its biggest cost savings would come from disrupting the internalized accounting, getting control of malpractice awards, rationalizing wage and executive costs, and removing middle-man costs from supplies, especially drugs. But I predict these streamlining efforts will prove to be disappointing. The public is proud of its hospitals, and will defend them.8.Why use Health Savings Accounts, when we could just use single payer? Well, that translates to, Who do you trust not to misappropriate it? Robert Morris of Philadelphia took great pains to arrange the Constitution and the First Congress to prevent the federal government from ever owning shares of a business, because of fear of "imperfect agency". That is to say, Morris foresaw the greater danger in diverting medical money to battleships, than to Credit Default Swaps. No doubt your victorious government would share some of your money with you if it won a war, but what if it lost a war? You can make your own translation of what Morris meant, but it was essentially what is very wrong with medical cost control in general: Nobody spends someone else's money, as carefully as he spends his own.
10. The best way to reduce costs is by research. Much of the research is wasted money, and there are hundreds, perhaps thousands of diseases. But scientists are not fools, they concentrate on the expensive and devastating diseases. It is estimated that a majority, perhaps 80%, of medical cost is spent on four to ten diseases. I'm afraid that eradicating diseases like cancer and diabetes might lengthen longevity somewhat, while other diseases like Parkinsonism and Alzheimer's could take their place. After a while, of course, the disease burden will diminish, and within a century perhaps the cost effect will be to reduce health costs to the first and last years of life. In the meantime, however, the cost of research, new drug development, etc, may even raise medical costs. In the meantime, the immediate effect of research on costs could be uncertain. When a tough-minded drug czar is finally appointed and faces down public clamor, we may well discover how to identify and direct the efforts of good researchers. Generally speaking, research is a young man's game; they burn out. Because they are young, they make poor administrators. Somehow, the system needs shaking up, so unproductive researchers can be identified sooner and shifted to teaching, administration, and clinical practice, without fear of stigma or shame. That's mostly identifying research failures. Identifying scientific brilliance is an entirely different thing, because brilliance is in great demand, financially and otherwise. I'm afraid the American system is expensive but effective: we throw money at a goal until it succeeds. No other nation can afford to match that. Some time within the next century, I expect we will be down to the expensive first and last years of life, plus a horrendous retirement expense. We should arrange our systems to direct unspent medical money into more comfortable retirements, without exactly knowing when the two requirements will mesh. That's why a self-adjusting overflow surplus has great advantages.
At present, the Health Savings Account is the only medical payment system which can currently adjust to this predictable change from healthcare to retirement care. HSA currently provides for money still left in the account at the time of achieving Medicare coverage, to flow into an IRA which can be spent on anything. That's something to brag about, but it could be made better. For a system hoping for millions of subscribers, it is too rigid and uniform.
George Ross Fisher M.D.
203 Chews Landing Rd
Haddonfield, NJ 08033
grfisheriii@gmail.com
(Cell) 215-280-6625
(Office) 856-427-6135
(Fax) 856-427-6136
Competition for the Hospital, Rehab Center, and Nursing Home
Milton Friedman Price Restraint by Competitors. Milton Friedman once devoted his Nobel Laureate speech to creating new price competition for doctors by removing their licensing requirement; naturally, many physicians were outraged. It seemed to them we saw plenty of competition between individual practitioners. Competition between Homeopaths and Allopathic physicians had a history of unspeakable viciousness in the Nineteenth century; it could not have been of benefit to the public. Competition between Optometrists and Ophthalmologists has created unanswerable quandaries about specialization without a preceding general medical background, about the limitations inherent in a superspecialized lifetime, and the conflict of interest between giving advice and profiting from products which implement the advice. On the whole, it takes one to know one, and the Hippocratic tradition of peer pressure may have been as far as surveillance can usefully go. Lately, however, the herding of solo practitioners into group practices (by insurance) may require some reconsideration of heightened issues of organized fee splitting, cross-subsidy, and the loss of personal responsibility. Universal government involvement in reimbursement will surely unbalance these old issues, and it would probably be wise for the government to hold back until we can see if its heightened interest in cost control improves matters, or worsens them.
Turning matters over to the trial bar, however, commercializes the motives of the investigator and provokes defensive medical behavior which is just as expensive as any negligence left in a practitioner after a decade of education. Healthcare institutions with business departments moreover have the uncomfortable incentive to use the price of hospital malpractice insurance as a major metric, thus exaggerating the role of plaintiff lawyers in escalating unwarranted defensive behavior within the institution. For a century we have observed more expensive institutions destroying less expensive ones, always using other descriptions of the process. Horizontal integration could be forgiven when more expensive hospitals shouldered heavy burdens of indigent care, but the 20th Century transfer of indigent care to the government also transferred much of the credit for it. Research is also mainly a governmental transfer of funds rather than a payment, with administrative costs a local bonus to be enjoyed rather than deplored. These disloyal viewpoints justify the proposal that more competition for healthcare institutions would be beneficial, at the fortuitous time that escalated construction costs discourage government funding of it, while private borrowing costs are essentially zero.
Teaching hospitals are unchallengeable the best place for delivering tertiary care, and must not be injured by mere reformist ideas. However, this function is probably underfunded at present, subsidized by inflated costs for so-called bread and butter medical care, transferred by cost shifting. Considerable cost savings are possible if this system is brought more in line with its true costs, but it must be done carefully. Having said that, it is surely true that much of the care delivered in tertiary institutions could be capably performed in less expensive institutions.
The Central Locus of Healthcare. When I started medicine, which was fifteen years before there was a Medicare, the doctors of Philadelphia tended to have their offices on Spruce Street. It was like, and it looked like, Harley Street in London. In time, doctors moved their offices to the campus of a nearby hospital, where they now can be found, using the parking lot and the laboratories, and seeing each other at lunch in the hospital cafeteria. I now propose that this hospital locus no longer serves, and should be moved.
Thirty major diseases have disappeared since this was entirely appropriate, and patients are a great deal older. The hospitals charge inordinately for sharing a bed in a room with a stranger; the last time I was a patient, no one gave me a bath or a back rub. All the nurses wore signs because you couldn't tell them from dieticians. The hospital is now threatened with fines if a patient is judged to have stayed in bed too long. On the other hand, if he goes home too soon and has to return, the hospital is also fined. The doctors tend to make rounds at 6 AM, because later than that the commuting traffic is horrendous. A profession of hospitalists has grown up because it isn't worth a doctor's time to come to town to see one or two patients. The whole medical complex is in the wrong place, driven there by third-party reimbursement.
I can't say what things are like in other cities, but in Philadelphia, there are at least fifty retirement villages scattered in the suburbs, filled with old folks. They all have infirmaries, most of them have drug stores and collection stations for blood tests. For the most part, what they don't have our doctors, x-ray machines and operating rooms. What they have in great abundance are sick old folks who need a lot of attention. I see no reason why the young folks with SUVs can't visit the doctors if doctors had their offices there, and x-ray machines will appear if there is a call for them by doctors practicing nearby. This complex probably needs a full-time ambulance or jitney to take people to the hospital for a one-day surgery, but after that, they can stay in the retirement village infirmary as long as they like. Imagine that; no one will find you for staying a month too long, in the judgment of a utilization clerk. Furthermore, it's all voluntary. Other places don't need to do it if they don't want to.
The Cost of Meeting Unmet Medical Needs
For fifteen years before Medicare, I practiced medicine in Philadelphia. At that time, the backlog of unmet medical care seemed infinite, impossible to satisfy. For one thing, we didn't have enough hospitals to fix all the hernias, gallstone, rotten teeth, festering bad leg veins, positive blood tests for syphilis, and a dozen other matters. But we set about it, doubling the number of medical students in each school's class, and doubling the number of schools. We built or renovated and re-equipped 124 hospitals in Philadelphia alone, as I remember.
Well, we were successful. It is no longer true that everybody's teeth are rotten, or that one Wasserman test in six is positive. Instead of throwing up our hands at infinity of unmet elective surgical cases, we now hear suspicions that perhaps cataracts are being "harvested", cardiac pacemakers becoming universal apparel, tummies being tucked. But professional jealousies to one side, an undeniable statistic emerges. We only have thirty hospitals.
Backlogs are like waterfalls. The level seems limitless until it suddenly disappears from sight. We spent far too much money on new hospital capital construction, and that spending spree has to account for a major portion of the cost of medical care that now doesn't seem to be producing anything worthwhile. These are the training costs of what can now be seen as temporary construction.
These thoughts came to me when a visitor to the Federal Reserve from Kazakhstan talked recently about medical care in that vast wasteland. At a time when petroleum supplies are short, Kazakhstan has discovered it has possession of the largest new oil field in the world. The social scene is like Texas in the Twenties, or perhaps the Yukon fifty years earlier. Whereas today it is questionable whether to spend the money to perform a Wasserman in America, positive tests are widely abundant in Kazakhstan. I daresay the hernias, varicose veins, bad teeth, and whatnot are just as bad there as they were in America in 1960. And they are gunning up their engines to build lots of the biggest most expensive hospitals anywhere because they can afford them.
Prediction: in 2050 nobody will be able to explain why medical costs are so high in Kazakhstan. After all, at that time there will be no positive Wasserman, no hernias, no gallstones.
A New Definition of Poverty
Ann Carrns has recently written a short column in the New York Times to help banks afford to lend to marginal cases, but I would propose it actually contains a new and better way to define poverty. As some wag suggests, we have currently worked ourselves into the corner where almost no one is eligible for a loan unless he doesn't need a loan.
That slander isn't exactly the case, and it trivializes the problem. The interest a bank must charge to break-even includes the cost of those who default. If the bank underestimates the default rate, it will go broke, or at least must raise interest rates for those who do not default. Therefore, all interest rates are a little higher than they need to be, to protect the bank against mis-predicting the default rate. Furthermore, the bank must assign someone to make that judgment, case by case ( "underwrite the risk"), and that raises the overall cost still greater. It could be more profitable for banks just to skip questionable cases, so this "opportunity cost" must be guessed at and added. It's actually quite a considerable cost.
To guess wrong by underestimating the risk is equally and visibly expensive in reverse. To some extent, errors on the high side cancel out errors on the low side, so combining and pooling the two helps the problem, and enlarging the pool by combining banks is a good thing. So continuous computerized pooling is a big cost saver. The bigger the pool, the narrower the spread. Finally, an optional insurance layer of risk, if large enough, should soon result in a national market with a narrow spread which is considerably lower than present underwriting methods -- steadier, and permitting the acceptance of riskier poor clients within a more clearly defined range. This approach should improve the reputational risk of banks in general, whether they participate or not, consequently lowering interest rates by isolating a narrower layer of uncertainty.
And finally, it should establish a nation-wide definition of poverty. The government can assume that anyone who cannot afford the cost of this system defines himself as below the poverty level. It does this by stating that no amount of internal rebalancing of the private sector is apparently sustainable without raising somebody's rates. That is, someone may or may not be poor by other definitions, but has reached the limit of imagination within the private sector. It is thus a definition of the poverty level, constantly changing with the money supply, the value of the dollar, and the locality. Loans to a suboptimal client are permissible but are dangerous to the bank who issues them. This definition of poverty is the lower border of a band. The upper limit of that band is the level at which private-sector banks ignore the warning and make the decision to lend, in spite of it. The system may uncover non-market manipulation by this approach but, if so it could be useful for the voters to detect it, early.
Basic Lifetime Health Care?
Lifetimes are divided into sequential episodes for various practical reasons, and in the past fifty years, a brand-new episode known as retirement has even been added to the end of the sequence. We started with two thirty-year periods, childhood, and adulthood. For its own purposes, the medical payment system stretched to three segments within a 90-year lifetime, and then for practical purposes, a five-segment one: childbirth, childhood, education, employment, and retirement. The employer community pioneered this American hybrid, but almost all other national systems are government-dominated, so the American system segmented slightly to accommodate the reality that two employers (the parents and the child) must be recognized. The new retirement era tends to unite retirement with the government as becoming the organization which pays the bills tending to dominate the choice of payment. It probably does not overstate matters to say that recent immigrants favor a unified lifetime government system, while employers are reluctant to give up control for fear government control will spread out through the opening. The fact that medical revenue at any age originates in the employment interval lends plausibility to this attitude. Comparison of the quality of the two existing approaches does not seem to disqualify either employer-based or single-payer (lifetime national governmental), although the Constitution seems to favor individual 50-state hybrids.
What is gradually shifting during the past century is the inclusiveness of the sponsor groups, retirees enlarging at the expense of the employed. These groups see themselves becoming potential beneficiaries but changing at different rates and with different costs. Shifting costs are befuddlement, but it seems safe to predict that costs will ultimately fall to slightly more than the first year of life and the last year of life. Before that point is reached, we will probably experience a rising period of development costs in the middle. Actuaries calculate an average present lifetime cost of $300,000, net of inflation, around which actual costs will fluctuate. Taking a wild guess that first and last year will eventually settle down to $100,000 per average lifetime, or perhaps $150,000 including terminal care, the elements of the first-and-last year of life insurance should be calculable, and the premium approximated and re-adjusted annually on a current-cost basis. In the meantime, healthcare costs can be monitored by big-data methods. No one would expect such data to be precise at first, but a ten-year probationary period should suffice to arrive at commercially workable net costs for all citizens for the two universal costs for everyone -- birth and death. There will be universal outcries that other costs will be neglected, underestimated or misjudged, but a workable and basic universal system can nevertheless be established, and the intervening other medical costs managed in the conventional political way.
.
25 Blogs
Philadelpia Hospitals, Past and Future
The first hospital in the Western Hemisphere was the Pennsylvania Hospital, founded by Benj. Franklin and Dr. Thomas Bond in 1751, still going strong at 8th and Spruce Streets. Philadelphia General and New York's Bellvue challenge this primacy, but they were originally almshouses.
Specialized Surgeons
Specialty hospitals have actually been given more than a fair try. About a hundred years ago, the landscape was peppered with casualty hospitals, receiving hospitals, stomach hospitals, skin and cancer hospitals, lying-in hospitals, contagious disease hospitals, and a dozen other medical specialty boutiques.
Don't You Touch My Medicare!
New blog 2016-03-31 19:53:23 description
Academia Gets Its Share of Blame
Academia acts as though it wants to control the whole medical empire, and shares in the corruption as long as it remains profitable. It's sort of like the newsmedia -- we badly need them, but they are pretty unattractive, up close.
Two Central Mistakes In The Design of Health Insurance.
Hospital Cost-Shifting Between Payer Classes
New blog 2015-04-13 01:54:48 description
Diagnosis Based Payment: A Warning
New blog 2016-08-10 22:28:37 description
Health Savings Accounts: Synopsis
The Effect of Tax Law on Health Costs: The IRA for Health
IRA
Reducing Unnecessary Care with Health Savings Accounts
New blog 2015-06-07 23:56:28 description
Other Voices: Rethink Lifetime Health Finance
Barron's recently invited 1000-word summaries of radical change proposals.
tg.donlan@barrons.com
The Two New Revenue Sources for HRSAs: Investments and Compound Interest
New blog 2016-07-14 16:02:12 description
Stretching Out Your Retirement Savings
"Don't spend principal" is pretty good advice, except as retirement income starts to run low.
Paying for the Healthcare of Children
New blog 2015-02-18 20:16:10 description
Last Four Years of Life Reinsurance
Half of lifetime medical expenses are reimbursed by Medicare. And half of Medicare represents the cost of the last four years of someone's life.
(1) Medicine at the Two Ends of Life: First year of Life, and Last Years of Life.
Every person is born and will die. For other health care, a cure might be possible.
The Future of Index-fund Investing, Itself
Tax Legislation--Just A Condominium Squabble
New blog 2017-11-11 02:52:56 description
Broad Brush
A one-page summary of lifetime Health Savings Accounts.
Retirement Communities
 Retirement communities are fairly new ideas, still experimenting with the ideal model, so it is hard to generalize about them. But they look to be a possibility for everybody's future.
Retirement communities are fairly new ideas, still experimenting with the ideal model, so it is hard to generalize about them. But they look to be a possibility for everybody's future.
What Long Term Thinking Looks Like.
Each of three age-related switches creates a transition issue. The need is to store surpluses in one escrowed vehicle, allowing transfers to enhance compound interest faster than inflation can slow it.
Competition for the Hospital, Rehab Center, and Nursing Home
New blog 2013-04-19 14:37:47 description
The Cost of Meeting Unmet Medical Needs
If you are careless, the cost of meeting unmet medical needs will continue long after the needs have been met.
A New Definition of Poverty
If we propose to subsidize poverty, we must devise a flexible way to define it.
Basic Lifetime Health Care?
One of the main reasons healthcare payments are so fragmented, is that it is so difficult to imagine how to unify them.