3 Volumes
Surmounting Health Costs to Retire: Health (and Retirement) Savings Accounts
Health Savings Accounts: Steps To Lifetime Health Insurance
From 1981 to the Present.
Consolidated Health Reform Volume
To unjumble topics
Health (and Retirement) Savings Accounts: Steps To Lifelong Health Insurance
If you are a fast reader, we will begin with a ten-minute summary of Health Savings Accounts. At first, it covers future revenue, then spending projections follow. No matter how medical care changes, cost and revenue must remain in balance.
President Trump has been elected. This book is written during the "lame duck" interval between election and inauguration. The Democrats have been defeated, but still have a vote; in another couple of months, real changes of office take place. News media have nothing much to talk about, except Presidential appointments and conjectures about the future. We are in much the same position, except we offer a serious alternative to the Affordable Care Act.Dozens of times, the Republican House of Representatives has already voted to repeal the Affordable Care Act, only to have either a Senate filibuster or a Presidential veto turn back repeal. Republicans are now reminding the public that not a single Republican Congressman has ever voted for the Affordable Care Act. Obamacare might be one thing or another, but it surely isn't bipartisan.
With changing control of the White House, and a majority of the Senate re-emerging Republican in the recent election (to say nothing about dozens of state legislatures), a successful repeal effort for ACA seems inevitable if only as a victory announcement; serious crippling amendments likely to follow. In that uproar, only five Democratic Senators need to acknowledge a public mandate from the election, and ACA will be gone. Republicans temporarily conceal serious weakness in changes they prefer; lacking details to attack, Democrats taunt the Republicans as having no replacement at all. It's a weak moment in our system of government, raising concern our international enemies might take advantage of its predictability.
Transition. Even if Republicans display a perfect plan, they must then navigate a vulnerable transition to implement, possibly even to pass it. Transition in a plan matches transition in political control, so authors of books must adjust as they can. Our intention originally was to spend the briefest time introducing a plan, and then go on to the subject of its transition. The book now is reversed: transition first, then return to a fuller description of how Health Savings Accounts would provide a cheaper and better framework for financing healthcare. And then -- how to keep revenue and spending in continuous balance, when they are separated by at least one generation. To some degree, the plan and its transition are much the same, and it isn't accidental. In fact, the pair would extend over such a long period, the two of them become more a process of continuous change than a static blueprint. This time, reform must absolutely have a bipartisan flavor.The unprepared reader must consequently forgive this brief introduction to a very complicated system.
First of all, is there enough money in our economy to do it? We are lucky to have actuaries like Dale H. Yamamoto figure out a rough way to predict how much it will cost in the future. It probably isn't precise to say it will average $350,000 per lifetime in year 2000 dollars, but at least the assumptions for such approximation can be stated, to be revised as we revise the assumptions. The demographic prediction -- how many people there will be -- is equally rough, but similarly based on definable assumptions. They lead to a prediction of xxx millions in 2117. Multiplying one by the other, we would arrive at a figure for how much for the whole nation will need -- in inflated dollars -- for healthcare by that time.
That really is less useful than how much it will cost per person, adjusted for inflation, no matter what our population. It will be $350,000 in year 2000 dollars, less or greater, largely depending on scientific discoveries in the meantime. For methodologic reasons, I suspect it is 17% more than that, adjusted for insurance costs, and therefore will be 17% more in the future, as one example of adjusted assumptions. That's surely inaccurate, but it gives us a ballpark number.
Or it might expose a counter-proposal which the voters simply don't like. We might even go back to where we were in the past, but doing so would raise an unpleasant question about why we ever went through all the fuss. Two quite different questions are posed. This book is a brief analysis of both (Is there enough money to cover a better system? How do we get from here to there?) There might be enough money, if we rearrange payment flows, as we shall shortly see.
Finding big money might be accomplished the way whole-life life insurance does it, by collecting many small premiums years in advance, magnified by compound interest in the meantime. But how can we then find revenue for actual healthcare every single day during a century of growth and change-over? How do we transform "pay-as-you-go", into total pre-payment? Since we are considering total lifetimes, in our existing system it comes in pieces which we cross-subsidize in an expensive way, for almost a century. Transition from Medicare for a portion of it is somewhat easier; it purports to be funded by taxation, so it needs less transition, and no one has the courage to change it much, anyway. So we heedlessly begin with Medicare, which some people hope will never be disturbed, while others feel, everything should imitate. Serious health costs are constantly migrating toward Medicare, no serious analysis can avoid discussing it.
But in just what condition president-elect Trump will find the rest of medical care, is far less clear and it too must be studied. The rest of healthcare may contain the poor people; it also contains all the revenue creation. The non-Medicare portion was designed piecemeal, with resulting gaps and overlaps. In fact, the uproar about health insurance might be described as actually a confused rebellion of healthy young people, reluctant to continue subsidizing sick old ones. That's especially true in a recession which hits younger people harder than older ones. In the case of employer-based insurance, it would be new hires rebelling against existing ones, because new hires often move to new jobs before they get much benefit from their insurance reserves, which then become cheaper for the old hires. There's really no alternative to discussing every major component.
Tons of money for future use do not pay current bills, but lengthy transition pushes huge Medicare expenses to the head of the line. There are people in hospital beds today, expecting their bills to be paid. The "J-shaped curve" of lifetime medical expenses does make revenue accumulation possible, but pre-payment transforms this J-shape into a big problem for transition. This "transition problem" requires a clever navigator, who has sensible plans to choose between. The Health Savings Account offers both long term solutions and a fall-back for current emergencies. Quite obviously, a bond issue might be needed to cover early funding gaps, but beyond that, there must be re-designs to cover criss-crossing needs, with an effective salesman leading public support for a proposal which is hard to understand.
There are many pieces to this transition problem. President Obama discovered thirty million people with such wildly different requirements (prison inmates, illegal immigrants, soldiers in uniform, mentally retarded, etc.) they didn't fit any one-size fits- all solution, no matter what had been promised to average folks. President Trump is about to discover different solutions are needed for different age groups. Early problems requiring bond issues will discover existing bonds; we have already issued too much debt from wars and other entitlements. Medium term solutions for a decade of change, and long-term issues may not be suitable for bonds at all. Meanwhile, the system is so huge, mistakes in judgment had best be corrected before they get worse.
We begin this discussion with Medicare, because serious healthcare problems are migrating into the elderly. Medicare covers 50% of healthcare costs, and the proportion steadily increases. With 9 million disabled persons added to 44 million old folks, Medicare will increase still faster and more expensively. Meanwhile, President Obama chose to structure the ACA to include a large portion of the wage-earning age group of non-sick, only to discover they also didn't conform to community distributions of disease. The employer-based group, in the same age group but selectively healthier, found their premiums could then do nothing but go up. It didn't prove to be a useful beginning, so let's look first at the sick half he excluded, which you might suppose is receiving a subsidy from younger people.
Here are some blueprints, Donald. Good luck, Mr. President. Whether some citizens hate you, or some citizens love you, doesn't much matter . What matters is, we all need you to succeed.
Paying for Medicare Transition with Trust Funds.
Since its finance isn't much affected by the Affordable Care Act, there's a temptation to skip over Medicare. But ACA deficits and design flaws frequently grew out of Medicare's initial design decisions. Furthermore, the scientific tendency has been to cure acute diseases of younger people first, so the trend predicts still more high expense (chronic disease) patients will migrate toward Medicare. The ultimate prediction is for little to be left uncured at some distant time, except in the first year of life and the last year of life.
Changed Circumstances. There have been three main changes since some wag called Medicare the third rail of politics -- "just touch it and you're dead". The first change since 1965 is much-increased longevity as a consequence of much-better healthcare. Someone must have seen this coming, but apparently, no one spoke up. Although prolonged retirement is expensive, notice also how it prolongs the period of time available for compound interest to work, so the income curve starts to bend upward after thirty or forty years, regardless of the economy.
Secondly, passive, or index, investing has greatly simplified and strengthened amateur investing. Finally, the Health Savings Accounts appeared, often producing savings of 20-30%. It's time to re-examine the assumptions of 1965, with these three lights shining on them: longevity, passive investing, and payment design. We are not recommending that HSA be entirely funded by index funds, but merely recoiling from too much debt backed by government guarantees. (see below)
Proposed. In "Ye Olde" Medicare, the average beneficiary pays $56,000 per lifetime (in payroll withholding tax and premiums), but it actually costs the government at least $112,000 per person -- the remaining $50,000 or so per person is secondarily borrowed, so there are no left-overs for retirement. But prolonged longevity and longer retirement, hence more borrowing, are inevitable consequences of better healthcare with the present design. Viewed in that light, Medicare is broke. But viewed as a transition problem, it paradoxically addresses half of it; since half, the Medicare transition is already covered by bond issues. Put that together with the halving provided by Last Year of Life re-insurance, and you have made big progress toward transition. We also offer several other proposals for transition.
Our "New" Medicare, by contrast, seemingly could pay for all its present medical care, plus appreciable retirement cost, with the same revenue. Minimal extra government debt, no rationing or curtailment of service. It does it without changing major program elements; this is a financial change, not a medical one. It really does let you keep your own doctor, and doesn't tell him how to treat you, because it doesn't concern such things. Half of all medical expense is covered by Medicare. And we propose to fund half of that, plus all of the obstetrical/pediatric care, with First and Last Years of Life Re-Insurance. Transition begins to look feasible if we can convince old folks with a fixed income to take a chance on it.
Tools Seemingly Available for Transition to the New System, But Presently Not Provided For in Law: (See below) 1) Scientific break-through cures which significantly reduce the cost of Medicare. 2) Gradual buy-ins for latecomers, which significantly reduce the buy-in cost for people well past 65 at the start. 3) Special Trust Fund Extension eligibilities after death or before childbirth. Compound interest doesn't need the owner to be alive. 4) Delaying the Start of a Childhood Roll-Over. 5) Graduated Retirement as funding develops. All of these will be explained later, and the news is not all bad.Transition costs dominate the replacement of almost any health insurance, so let's restate the theory. A J-shaped cost curve forces a J-shaped revenue stream. When you switch systems, you must reverse the order, paying expensive existing ones first; and funding proves inadequate unless you can double it. If you could just manage, it would be possible to make partial cost savings you could boast of, but except for the Postmortem Trust Fund way you must pay double for all of it, or give up the attempt. By contrast, if you have at your disposal a large new source of credit like a postmortem Trust Fund, with an elastic retirement fund absorbing embarrassing surpluses, you can survive early misjudgments. Medicare could pay for its entire cost with compound interest on what subscribers now contribute, save for the fact it will have inadequate cash flow from people on their deathbeds. But if the death of the subscriber is ignored, the inflow of funds from surviving depositors could continue into postmortem trust funds of the decedents. At 7% return, extending the payments to the length of perpetuity (21 years) would multiply its amount four times, reducing the problem to a quarter of where it started. The transition time is thereby considerable shortened. For transition purposes, it might be wise to create a contingency fund, of up to $250 at birth. But remember, the size of the gap in a life plan can only be finally addressed after we see what is to become of the ACA (Obamacare). For the purposes of this book, we simply treat the ACA as if it were revenue-neutral, a somewhat unlikely forecast, but a completely understandable assumption.Extra Tools, Needed From Congress: "Change the destination" of Medicare's Withholding Tax, and Premiums, so the same money, plus interest, end up in the individual's Health Savings Account, instead of Medicare. That's in return for the subscriber agreeing to buy out Medicare at its mandatory onset, plus any other imposed conditions. There is one technicality: the tax exemption is currently distributed through the income tax system, while it should be added to the HSA, instead. Furthermore, if a considerable surplus (more than $100, say) from compound interest persists after withdrawals, the choice of buying out Medicare can be offered at its beginning age up to the perpetuity limit (on average, age 104), disregarding whether the depositor is still alive or covered by a special successor trust fund. Re-depositing in an HSA should make such contributions tax-exempt and earn compound interest (we hope, at 7%) in an escrowed sub-account which bypasses current medical costs until it is time to use them for Medicare. At least, escrowed in a way which cannot be diverted from Medicare use. Therefore, average payroll-withholding transforms from $28,000 ($700 yearly for forty years, taxable) into health care worth on average 18% more than that, or $825, because it's before-tax, and at 7% grows to $138,000 at age 65 (Try that out on your Internet compound interest calculator). That's what folks are paying right now, but including the tax exemption isn't as smooth as it could be. Don't forget the escrow feature, which keeps people from being their own worst enemies when other purchases compete for the single-purpose savings escrow.
Starting at any age before 66, it could then transform $1400 yearly Medicare premiums, before tax, and thus really $1650 into 18% more for twenty more years, and also pays tax-exempt interest. (Most people will find they have to read this several times because Health Savings Accounts are the only plan enjoying these particular features.) The net effect of augmented income tax augmentation, compounded, is to transform $56,000 before tax, into $534,000 before-tax at age 84, the present life expectancy, not counting $112,000 borrowed by the government, which we hope they can eventually stop borrowing. That doesn't sound like good arithmetic, but If you don't believe it is possible, just try it on one of the Internet's free compound interest calculators. (Furthermore, if an afterdeath trust fund is created to the limit of a legal perpetuity [one lifetime plus 21 years], the present expenditure would be subsequently transformed by compound interest into whatever $2,066,000 is worth at the time, we should hope amply providing for all of Medicare, plus some generous retirement without government borrowing. You won't be surprised to find others think this is more than you will need. We will later suggest better ways to rearrange the same facts, but this summary contains the general idea in highly condensed form.
Although an accumulation of over $2 million per subscriber seems adequate for any normal purpose, it should be recognized that this figure only applies to someone who started saving from birth and waited 104 years to collect. Therefore it would only be a theoretical issue for a long time. A far more generous sum is possible earlier if the original purposes of payments are ignored, and the principle adopted that the largest contribution should begin earliest. That maneuver results in payments age 104 of $30,165,195.00 which would make most people giggle. The obstacle to overcome is the resistance stirred up by matching Medicare premiums to newborn children's HSAs. However, if the system needs more money, this is the place to get it. By adopting this principle, a $2 million fund is achieved at age 60 instead of 104, which eliminates the need to consider several other strategies, expenses and objections thereto, subsequent to a Medicare buyout. It would make an $18,000 grandchild gift seem trivial, and last year of life strategy unnecessary, for example.
Two Central Mistakes In The Design of Medicare.
There are surely dozens of misjudgments in our health system but concentrate on two of them. If correct, they could transform the system, while if uncorrected, no scoring -- dynamic or otherwise -- will conceal our collective failure to address health costs seriously. Other problems can stand aside while these two are considered.
The first is pay-as-you-go. Its name is misleading, because the younger generation, mostly enjoying good health, pays for the previous generation's dauntingly high health costs toward the end of life. Medicare started in 1965 and grew for fifty years. The first generation thus was given a free ride, so my mother who died at the age of 103, represents a whole generation who paid essentially nothing for thirty years of expenses. This hot potato of debt was passed along for fifty years, getting bigger with time and baby booms. The burden of 18% of Gross Domestic Product became unsupportable, even with abnormally low-interest rates. We must now liquidate the debt burden, invest the idle savings until needed for healthcare, and thus eliminate the annual 50% Medicare deficit to foreign nations. Quite a task.
An important result of replacing pay-go with pre-payment is the incentive to save, replacing the historical incentive to spend. Actual experience with HSAs demonstrates net savings in health cost to be at least 20%. Using a Health Savings Account, young people of each generation save for their own subsequent health costs, instead of spending immediately for anonymous demographic groups of strangers. At this point, another unexpected bonus appeared:
Some young people have good luck not to get sick very much, thus accumulating tax-exempt money in the account when they turn 66. In fact, most people do escape serious illness until about age 55. Since everyone gets Medicare eventually, current law turns HSA accumulations into a tax-exempt retirement fund, a provision which went largely unnoticed. (It's mandatory, while I would prefer an option.)
At this point, a second blunder by the designers of Medicare reached the surface. Medicare provided better medical care, made longevity increase, but laid bare it had added thirty years to be financed as retirement cost. Sickness cost is episodic, but retirement costs are continuous. Consequently, these additional retirement costs may eventually become several times as costly as the sickness costs they replaced.
I cannot claim it will be easy to scrape together a package of proposals to cover the transition to a considerably less costly funding system. But I have tried, and suggestions follow in this book. No health funding scheme other than Health Savings Accounts provides even a flimsy scaffold for addressing this new issue. Social Security does have such a mission, but it is hopelessly underfunded. I'm afraid we have to say this impending disaster is largely a consequence of Medicare's success. So this is the second of two big problems facing us: we failed to anticipate success.But there is a third big elephant in this room which might be wiped out with a paragraph of legislation. Scratch any regulation and you usually find a lobbyist underneath it. Somewhat over half of the population enjoys a tax deduction which is denied to the other half, and that other population is restless about it. Unless big corporations soon yield to the demand for equality of treatment, there will be continuing agitation. No doubt it is contemplated to address this issue in the looming tax reform, and perhaps the defenders of this inexcusable situation plan to reserve their concessions for later trade-offs. But after seventy years of this inequity, one half of the public owes such a large debt to that other half, little quid pro quo is justified. Permitting HSA to pay the premiums for its required high-deductible insurance could accomplish this in a handful of sentences, eliminating the grievance.
And what might be called the fourth big issue actually offers hope, instead of despair. Medicare coverage for young unemployable persons ("disabled") was effectively broadened to over 90% in 1984. Narrowly higher costs were thus added to basic Medicare costs for 9 million of the 46 million regular Medicare recipients, rather than remaining lumped with the 30 million uninsured unemployables (requiring specialized programs.) These higher costs of average Medicare per employable person, have been overlooked by most commentators, making ordinary Medicare seem costlier than it really is. It's bad, all right, but not quite as bad as it seems. Documenting that fact, as well as shifting the medical income tax inequity to the tax bill, thus leaves onlytwo new issues to address: pay-as-you-go, and retirement funding. That's quite enough for the first round.
Modifying Medicare Early, Using It Later
Pay/Go Becomes Prepaid
In 1965, the originators of Medicare made two mistakes, both of which seemed perfectly understandable at the time. To get the program rolling, they enrolled my parents' generation to enjoy the benefits without charge, if they were already over age 65 (my mother lived to be 103). And for the same reason, they used current revenues to pay for such older people, who had never contributed to their own costs. The system was called "pay as you go" to justify taking current revenues to pay for benefits unsupported by previous contributions. Money flowed out as fast as it was received, but Medicare never made a serious effort to catch up.
Consequently, there was no interest paid for the use of the money, but the program did get started, years before it would otherwise seem feasible. The program is now over fifty years old however, and it still isn't gathering interest on cash which doesn't get spent for decades. Furthermore, the health of the population invisibly improved so rapidly that decades were added to the lifespan of Americans, and the interest income being lost steadily increased, as well. Since everyone likes to live thirty years longer, pay as you go was considered a reasonable price to pay for it.
However, the possibility has apparently been overlooked that a transition to pre-paid insurance might only be mildly painful. And even if the transition proved to be very painful, eventually the cost savings of Medicare passed on to the subscriber, might be reduced by millions and millions. It is now time to examine whether biting this bullet could really be relatively painless any longer and whether it would save much money. The answer appears to be Yes to both questions. To begin, the arithmetic will be skipped, and the reasoning explained. Following that, the arithmetic is concentrated for those who wish to reassure themselves; it may be skipped by those who don't. If you get the reasoning straight, the math is easily checked by compound interest calculators on the Internet. If you do that, you may find the Internet calculators sometimes create some errors themselves, however, so check your fact-checking.
Medicare is partially prepaid by withholding roughly 3% of a subscriber's wages in advance, as can be seen on any pay stub. From age 25 to age 65, the money aggregates to equal about a quarter of Medicare's actual cost. Another quarter is repaid by premiums, from people actually receiving Medicare. Although the data is overwhelmingly voluminous, it can be found among the Internet reports of CMS, the Center for Medicare and Medicaid. Since patient payment revenues thus aggregate to only half of the total Medicare expenditures, the residual half is paid out of the general fund of taxes, and later borrowed to restore the fund. (Partisans might say it is laundered through the general fund before it is borrowed.) About 13% of our bonds are held by oriental foreigners, and most of the rest is loaned to American citizens. This is how Mrs. Sibelius explained things in her report on the Internet when she was in charge of it. The accumulating debt is now becoming serious, even accounting for the slang phrases used in Congress, suggesting this debt can never be repaid. Stick it to the Chinese, except 87% of it is ultimately owed to U.S. citizens. And U.S. citizens would take most of the haircut, as another saying goes if the debt were dishonored.
Now, focus on an important feature of the average Medicare cost. As a total departmental cost, it includes every person who becomes eligible for Medicare by attaining age 65. It is not exactly what the average person pays, rather, it includes the whole program including those who pay nothing. Therefore, privatizing Medicare with the same funds would not deprive the indigent of anything at all; present funding already includes them. That's one of the main attractivenesses of "single payer", defined as Medicare for everyone at any age-- it's essentially all-inclusive. Unfortunately, its deficit is all-inclusive, too. For present analysis it's a rhetorical advantage to say, any new system using the old money would be all-inclusive as well. Except for half of the increased cost causes a correspondingly increased deficit. At present, the annual deficit is about $200 billion.
It's also important to acknowledge that extended retirement benefits are an innate obligation of Medicare, and right now retirement costs aren't provided at all, except for the (older) Social Security program. Good care leads to a longer life, and we should be grateful. But longer life is expensive, and most people will find they have not saved nearly enough to make it comfortable. For this, there should be more sympathetic. Nothing like this had ever happened before, so some skeptical people cannot be entirely blamed for wanting to see some hardship before they believe the government cannot borrow its way out of it. The financial crunch of some sort is surely coming in the near future because we are recovering from a recession, a political party deadlock, and the threat of both domestic uproar and international discord, both at once. But the health care arithmetic remains pretty clear, as we will see in the next section.
At present, about half the cost of Medicare is recovered by the U.S. Treasury. Without paying any interest, the revenue immediately gets spent, and an equal amount is borrowed -- that's what we just said. So to speak, we only propose to change the mailing address of the checks, that's what we also said. Just deposit that same money (in the same amount) into your Health Savings Account, get a tax deduction for doing so, and earn compound interest on the combined amount. With a tax deduction adding 18% in value and transferring the money at age 65, it will in fact be more money than you appear to need, and it would certainly be less debt.
For the first time, it provides some retirement money "to compensate" for the extra longevity Medicare has provided. If you earn enough investment income (say, 7%), it will be enough to pay for the whole program, including indigents and disabled, so long as they are over 65 or entitled to a special Medicare disabled program, as 9 million already are. Remember, that promise includes a retirement fund. If you don't earn enough investment income, it won't cover it all but it will surely cover more than it would have, without any compound interest and tax shelter. And the investment return would probably be increased at the expense of the financial community, who will resist. Fee-only advice, rather than commissions, would add about one percent to investor returns, according to the Wall Street Journal, although lobbyists for Wall Street vigorously deny it. The proposal here is to insist both systems operate side-by-side until the difference is clear.
Although the arithmetic seems to be pretty evident, we do advise creating a contingency fund in addition, just to be safe. The contingency fund would have to be at least a hundred dollars at birth and might be as much as two hundred-fifty. That's the only extra expense for a lifetime of healthcare and retirement which actuaries estimate to cost an average of $350,000 per average lifetime, plus an equal amount for retirement, to say nothing about the hidden elimination of the government's deficit for Medicare. That's a pretty good bargain, so we suggest consideration of paying some of the resulting surpluses to a children's fund, rather than just letting it appear in estates. You can tell yourself you've helped little children while protecting yourself against contingencies. The Medicare crisis goes away, the Retirement crisis is abated, the national debt stops expanding, and a start is made on the childhood problem -- all with money you're already spending, plus a hundred or so dollars, just for safety and dignity. Read on, just in case you are good at math, and you don't believe in miracles.
By the way, it has been implied this release of money is due to inflation, and it is true the inflation assumption (for income and general expenses alike) remains about 3%. But the real success secret beyond any person's control is inherent in the mathematics of compound interest. When an investment goes much beyond thirty years in duration, the effective interest rate rises spectacularly; you can thank Medicare for that, if you wish, or perhaps Aristotle. Inflation raises your retirement cost, that is true. But it also raises your income, so at present, it's a short-term wash except for scientific advances, which are surely a long-term net improvement.
Steps in the Staircase, Extending for Decades.
There are traps on every step of the staircase to an improved healthcare financing system. They are teased out in four preceding books, step by painful step. A brief summary is therefore important for orientation, especially for newcomers.
A Health Savings Account misleads a newcomer into thinking it is a single process, when in fact it starts with two processes, welded together. It begins with a high-deductible health insurance policy and adds a Christmas Savings Fund to help beginners overcome the initial deductible. That is, it began as a bare-bones indemnity policy for poor people because it's the cheapest form of insurance. It has the characteristic that the higher the deductible, the lower the premium. It's true it leaves the subscriber without coverage for a few years when he is young, but the Affordable Care Act has made high deductibles essentially mandatory, so we start out even. Once there are enough deposits in the account to cover the deductible, the subscriber is completely covered from the first dollar of health care. But since he has the alternative of paying cash for small claims, it carries an incentive to leave it untouched as a tax-exempt fund for larger later claims. Since the true deductible is what is left unpaid, it is quite true the premium does not rise when the depositor crosses that invisible line. When he does, he can rightly claim to have first-dollar coverage at high-deductible (low) premiums. It's a bargain, and he is allowed to deposit $3400 yearly into the account, getting a tax deduction for it, and no taxes when he spends it for healthcare. Health Savings Accounts are the only health plan with this feature. It gathers compounding interest as long as there is money in it, which will turn into an IRA (Individual Retirement Account) when he joins Medicare. It's the only plan with that feature, as well, and the American Academy of Actuaries found it was 30% cheaper than regular insurance.
Part of the savings came from the tendency of HSAs to pay small bills with a debit card, working on the assumption the depositor will not spend his own money as freely as he spends an insurance claim. Since health insurance averages 17% costs, the main claim to process, it taught everyone the lesson that the expensive claims processing costs could be avoided by giving the subscriber some "skin in the game." When you compound these two savings for several decades, a surprising amount of income is generated, which ultimately is available to spend in retirement. And if you spend it for healthcare, you probably won't survive quite as long. The serious disease is being pushed steadily later in life, to the point where half of the sickness cost is paid by Medicare, and half of that covers the last four years of life. Longevity, in short, has increased by nearly thirty years in the past century. At the rate this is going, retirement costs will soon exceed healthcare costs, and a dual-purpose Health Savings Account is the only health insurance which covers both purposes.
Therefore, this program is available as a fall-back, in case of a sudden collapse in the Affordable Care Act. The incoming President won the election as a change agent, and he may have other plans. But the House of Representatives has voted to repeal the ACA many times, only to be thwarted by the threat of a filibuster in the Senate or veto by the former President of the opposite party. Very shortly, we may find ourselves without ACA, and nothing ready to replace it. Since the HSA is owned by the subscriber, and innumerable financial institutions are able to supply it, it makes for a quick replacement. A very short technical amendment would repair the few flaws to appear in thirty years, like expanding the age, occupational and contribution limits, and allowing a tax deduction for the insurance component by permitting the tax-exempt account to purchase the catastrophic insurance, currently forbidden. Given a week or two, Congress could improve on that, but it makes a swift substitute very simple.
However, the HSA has been around for thirty years, and bigger ideas have emerged. The retirement feature is the first feature to appear, inadvertently thwarted by the mandatory roll-over on attaining Medicare coverage. The roll-over is a good idea, but it should be optional up to a somewhat later age. We will return to that unexpected twist in the next section. Because Medicare is beginning to accumulate the most serious illnesses, the bullet will have to be bitten; Medicare really ought to be the first existing health plan to join the Health Savings Plan network. Unfortunately, retirees are particularly wary of change to their plan, and must be persuaded.
Since other health insurance needs to share in this feature as well, provision ought to be made to add their finance stream to the Health Savings Account pattern, like adding pearls to a necklace. As long as they remain revenue neutral, there would be no objection to adding them to the Health Savings Accounts in order to share in the retirement incentive. This might be considered if new programs for prison inmates, illegal immigrants, etc. want to get started rapidly, and would greatly facilitate the transition. Great overhead savings are possible through merging operations permanently, but permanence is not as essential as a speedy onset. Just as Medicare is accumulating the bulk of serious chronic disease, employer-based health insurance, and ACA contain the bulk of the money generation. A very expensive transfer system, using the government as a bank, has been virtually constituted for the purpose of uniting the money with the disease cost, across age barriers. This problem is expensive, and getting worse. However, no one wants to subsidize some other insurance, so every ship on its own bottom -- revenue neutrality, -- is a price that must be paid for the independence of the various delivery systems. These are the steps on the staircase., which may take decades to complete. The very least which can be required is to keep any windfall scientific breakthroughs, permanently within the healthcare realm, untouchable by regional, governmental, industry or legal encroachment.
Because very large amounts of money must be held by a custodian for many decades, special precautions must be constructed to keep it from wandering to unintended purposes, such as aircraft carriers, to say nothing of imperfect agency of the usual type. The awkwardness of the Tenth Constitutional Amendment must be satisfied, possibly through the court system, possibly legislatively. All these things require time to resolve, and a full implementation cannot be expected during many changes of political control. Neither the outcome nor the cost can be precisely predicted. But if we rescue healthcare from earlier blunders, and avoid new ones in retirement funding, we can be very proud of ourselves.
Now, let's take a look at the age limit for surplus funds in the account.
Law of Perpetuities
It may be a surprise, but the concept of a Limiting Factor (the Law of Perpetuity) may once again intrude the U.S. Supreme Court into the Affordable Care Act. It may also be a little hard to follow, so pay attention to what would ordinarily be regarded as a dry subject.
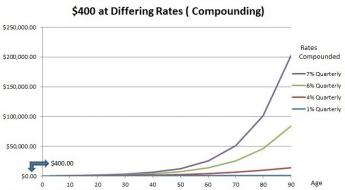
The concept of a limiting factor makes modern law, and possibly modern economics, possible. Several centuries ago, well before the US Constitution was written, lawyers came to see that many things are only possible if you don't carry them too far. The operation of compound interest is an example. In ordinary human commerce, the tendency of compound interest to rise over time leads to an eightfold rise over one lifetime of 84 years (48 in 1901 to 84 in 2017). A 200-year lifetime would lead to even more rise, to the point where one dollar invested at birth at 7% would pay for the entire average medical cost of a lifetime of $350,000 expressed in the year 2000 dollars. But quite obviously, if some scientist discovered a drug which lengthened life that much, something in the law would have to be changed to hold the economic world together.
So, about three hundred years ago, some English judge laid down the Law of Perpetuity, stating that Trust Funds may not endure for more than one lifetime, plus 21 years. It's proved to be a useful limiting factor, not likely to be changed easily. Congress might feel empowered to change it, but too much of modern commerce revolves around this definition of perpetuity, for the public to permit tampering without huge uproar. Notice the flexible wording: 21 years plus one life expectancy. Changing life expectancy would not invalidate the law.
A century ago, life expectancy was thirty years shorter, five doublings at 7%. And now it is more than eight doublings or in effect (2,4,8,16,32,,64,128,-->)256 times the original number. But that doesn't matter, because the law only effectively states its limit is 2 doublings (four times as much) more than the life expectancy at birth. A century ago, that implied two hundred-fifty-fold increase more than the starting amount at birth, and today it implies a thousand times. Inflation chugs along at 3% simple interest in both cases, at a growth rate doubling in 24 years (72/3). That's three doublings at simple interest a century ago, versus four doublings today. The important present difference is the thousand-fold compounded gain, compared with only 256-fold compounded at 7% a century ago, a seven-hundred-fold difference in the base price. The problem we have nevertheless still threatened less than forces opposed to changing the Perpetuity age limits.To summarize, compound interest on Medicare-linked investment has gained six or seven hundred-fold over inflation in a century, as a result of medical progress bumping against mathematical principles. This difference is not likely to change in the coming century, because longevity at birth would have to increase to age two hundred to overwhelm the judges into changing the age limits of such a fundamental law. If net Medicare-linked costs rise to approach that level, moreover, this revenue opportunity might disappear.
There is no reason to avoid exploiting this opportunity while it lasts. It presents a quick and dirty solution to the present urgent problem, which is to find alternative proposals for reforming transition to healthcare financing, in case the Affordable Care Act is suddenly repealed. At the present time, the opportunity to reduce the effective cost of transition lies in the gap between the average age of death and the Law of Perpetuity -- about twenty years. At 7%, that's two doublings or four-fold profitability. The question becomes whether to raise the term limit of the Health Savings Accounts above its present level of the age of Medicare attainment. The natural instinct would be to terminate the HSA at death, but the Perpetuity law would permit 21 years more. Since the life and health of the depositor has very little bearing on this subject, Congress has the opportunity to allow Trust funds to continue to earn investment interest after death, until either its Medicare funding debts are extinguished, or the birthdate of the deceased depositor reaches 104 and is terminated by the unchanged Law of Perpetuity. The effect of doing this would multiply the funds for the transition by 400%, and largely solve the problem if the Trust applied all funds to the debt incurred when offered the opportunity to choose. When we get to that subject, the transition is the big obstacle for three reasons: 1) There may not be enough money to do it. 2) The transition may take too long if it is constrained by available funds. 3) And the courts may find some reason to block it.
As a non-lawyer, I can see no technical reason why this could not be done, but some reason might be invented for political reasons. Unanticipated problems might arise, but under present law the challenge would probably come through the State courts, using the Tenth Amendment as a basis. If the adoption of the idea is voluntary with the States, or if demonstration projects are employed, a conflict between jurisdictions is very likely, and the U.S.Supreme Court would have to settle the conflict. This split approach might satisfy both State and Federal proponents enough to remove the obstacle, because the Wickard v. Fillmore decision still rankles after eighty years, and after much longer than that from the Civil War, memory of which still greatly affects the regional popularity of federalism.
Several other ways to pay for the transition costs, or shorten the transition time, will be offered in later chapters. But only this simple change is required early in the process, and so only this proposal will transform transition from a plan to a process. It has always bothered me for a complete transition to take nearly a century, during which interval there would be many changes of political control of Congress. In turn, those transitions offer a chance to smother central concepts in a welter of obfuscation. And that applies to all transitions, suggesting original planning should always be followed. To a certain degree, that has sometimes proved useful, but the transition in this particularly vexed case is going too far with it. So having major alternative approaches, and thus creating opportunities for later innovation, seems on balance a worth-while addition.
The Plan
It is time to present an outline of the proposal for replacing the Affordable Care Act with a cheaper payment design, owned by the subscriber himself. We first described its chief obstacle, paying for transition to it, not just because the proposal has to be shaped around that obstacles solution. It quickly becomes apparent people are so incredulous about overcoming a century-long year transition, they lose interest in details of it. Essentially, the solution consists of borrowing from trust funds after death, or possibly in anticipation of birth. This, in turn, generates income from extending the period of compound interest, which actually increases with a longer time period. Once it is accepted the protracted transition can be shortened into reasonable time periods, people are more willing to look at the overall proposal..
Most health insurance depends on overcharging healthy young people, using that accumulated surplus to pay for expensive old folks. Because people often change jobs, it becomes difficult for employer-based insurance to do that, so employer control of the system depends on the contortion of giving insurance as a gift to the employee. That allows the employer to set the terms while increasing funds with a tax deduction. This questionable approach is only tolerated because it works, and nothing else seems to. However, in the long run, it increases costs, and we are reaching the point where it has to end. With a plausible transition, we can at least look at alternatives.
The beginning of earnings happens to coincide with the least expensive period of life, around age 25. Children can get expensively sick, but someone has to give them the money for it. The period from childbirth to age 25 is a sort of no-man's land, neither self-supported nor assuredly funded by solvent parents. So let's assume children's health costs are donated by someone else, and the system really starts with approximately the 26th birthday. With the first paycheck, the new employee begins to contribute 3% of his earnings to Medicare. That's right now, and the employment period lasts approximately until the 65th birthday, followed by 20 years of Medicare premiums, until age 85, the present life expectancy. We suggest the payroll tax be paid into the individual's Health Savings Account instead of the Medicare "Trust Fund". If Congress would permit it, it would generate much more money if the premium expectancy were paid first, followed by forty years of the payroll deduction. That leaves 21 more years for a postmortem Trust Fund to make up any difference caused by starting later than at birth, reducing the implicit debt by 75%. Any surplus can be used for retirement purposes, any deficit remaining at age 104 can be written off. A table will show this system could supply ample funds for Medicare, and a variable amount for retirement. There are five special considerations, more or less optional in timing a phase-in:
1. Scientific Attrition of Healthcare Costs. We presently experience a period when new curative drugs costing pennies to manufacture, are being sold for eighty thousand dollars per treatment. Presumably, this will be a brief period because no government can tolerate it for long. After turmoil is overcome, we can expect a series of scientific discoveries will eliminate many health costs, often preceded by a brief period of raising them, first. It may be tumultuous, but the eventual outcome will be substantial lowering of before-inflation costs of medical care. It might require a century, although probably will be considerably sooner before we see health costs approaching those of the first-year and last-years of life. Executives of pharmaceutical companies may have other plans, but I have confidence in scientists' love of fame, driven by thirty or forty billion a year of research dollars, to sweep contrary trends aside. In the coming century, you can share my confidence that after-inflation health costs will come down. It will be up to Congress to be sure such savings are retained within the health system and not spent on battleships, or new substitutes for sickness care.2. Not a Single-Payer System, but Pearls on a String, Linked by Escrowing. This is essentially the same problem the Constitutional Congress faced in 1789. One side justifiably wanted a powerful central government for taxes and defense. In time, the central government was given a few enumerated powers by the Tenth Amendment to accomplish these goals, but everything else remained locally controlled. The dual problems were resolved with a dual ("federalized") system, which lasted 80 years until slavery and the Civil War broke it apart. Applying the same principles to Healthcare financing faces the same sort of issue, with the major difference that Healthcare financing is destined to get easier in spurts, constantly illustrating hope for the future. What holds it together is escrow a binding agreement to do what you promised unless some third party custodian decides you need an exception. The present four components are held together by escrow accounts, each ship on its own bottom, with a court system to allow for occasional special circumstances for one component to subsidize another. Other entities could add pearls to the necklace as desired. It has its fragilities, but it ought to last a century. If it doesn't seem to be working, a single payer's flaws can still be re-examined. But that's why we must wait to see what Obamacare really costs, with subpoena power to be sure the data reflects the complexities. The working age population in ACA really ought to produce surplus revenue, but indications are it wants to be subsidized. For the present, approximately revenue-neutral would suffice.
3. Component-shifting, Replacing Hidden Cost-shifting. The lifetime cost curve of healthcare is J-shaped from birth to death. Both the balancing problem and the revenue solution revolve around keeping revenue and cost manageably in balance at each stage, so transfer systems are minimized, not exaggerated. As a generalization, our proposal depends on moving payment compartments to other stages of the J-shaped curve. Obstetrical-pediatric costs are shifted from the mother to the child. The child's cost is shifted to investment-overfunded Medicare; male-female costs are equalized by removing them from the mother. The overall effect is to transfer obstetrical/childhood costs from single mothers and employers to Medicare (from the far end of the J-shaped curve to the opposite end), which is overfunded by the tail end of the compound interest curve. It's inevitably a little lumpy, and the final result must be smoothed out with the familiar tricks of accountants. It may seem difficult to persuade a dozen industry executives to shift business components like checkers, but it's a whole lot easier than persuading millions of customers to rearrange their health insurance habits. The new source of revenue is investment income from the currently indolent revenue stream , so there's considerable extra revenue to pacify a few losers.
The specifics are: transfer obstetrics/pediatrics from mother to child, donate that cost (supposedly $18,000) at birth to the Health Savings Account of the child, and eventually to his Medicare voluntary buy-out escrow at age 65. Any surplus is used for retirement, less buy-out costs for last-year of life re-insurance and childhood costs. (By the way, I bet we will find it doesn't cost $18,000 to bear and support a child; much of that big-ticket cost must be cost-shifted accounting maneuvers for malpractice, bad debts, etc.)
4. Computers: Finance Industry Suffers, Amateur Investors Prosper. Burton Malkiel showed a Random Walk Down Wall Street was mostly superior to the sharp-penciled judgment of experts, while John Bogle made economy-wide investing practicality, with index funds. Adjusted for fees, it was pretty hard for an investor to improve on low-cost total market index funds, just buy 'em and forget 'em.
Bogle's funds now total in the trillions of dollars, still growing fast, with only the crooked ones left to worry about, although the year you were born and the year you happen to die will affect the result beyond anyone's control. Otherwise, this approach will suddenly give millions of people superior results cheaply. When you compound the results for most of a century, a few tenths of a percent difference in return make a big difference in final outcome.
On the other hand, risky investments offer higher returns, so total market index funds must be chosen with care. The narrow index funds, by industry, for example, are not what we are describing. Our present calculation is that a steady 6.7% average return will suffice for a medical lifetime. Professor Ibbotson of Yale reports the stock market has averaged 10-11% for the past century, and inflation has averaged 3%; the result is 8% real return to be split between Wall Street and the investor, When you consider who is taking what risk, the investor has a reasonable argument he deserves (but often does not get) 6.7%. And when you observe the violence with which lobbyists reject mandatory fiduciary (the customer's interest ahead of the intermediary's) relationships where 1% is at stake, it won't be an easy settlement.
5. First Year and Last Year of Life Re-insurance. Two things make this transition idea possible. Not only is 50% of health cost concentrated in Medicare, but 50% of that is concentrated in the last four years of life. Secondly, the two halves of Medicare revenue stream can be separated by paying cost components into different escrow funds, reunited after death and/or borrowed, as seems expedient.
Effectively, this can remove half of Medicare cost from the mainstream, and it's the half which will shrink from scientific advances of the future. The terminal care half is more resistant to shrinking, is payable after death, and therefore puts less pressure on transition, demanding expediency only for half the costs. Essentially, this dual approach is an alternative or supplement, to Postmortem Transition Trust Funds. If both methods are employed, the transition phase can be considerably shortened. If half of Medicare cost is already "in the bank", it should also reassure many older subscribers of its safety.
It's presently difficult to know what to do with First Year of Life Insurance until we are more certain of its real cost. It's held in reserve until we can judge what its urgency is.
Well, What About Catastrophic Health Insurance, All by Itself?
To have a Health Savings Account, you must also have a high-deductible insurance policy by law, and naturally, there are premiums for it. Since I favor just about everyone having a Health Savings Account, I also favor everyone having Catastrophic insurance, as Scott Gottlieb and James C. Capretta advocate in a recent Wall Street Journal Op-ed article. Unfortunately, it is not entirely clear what that might cost, but we could find out by learning what it must cover.
Salesmanship. It's true the vendors of catastrophic insurance have been reluctant to advertise prices or even quote them over the phone. That's an unfortunate feature of many big-ticket items sold on commission. Desiring to save price for the last item of discussion, salesmen frequently leave room for discounting their commission against the customer's guess at the lowest possible price. Everyone who has bought an automobile is familiar with the issue; it's not in the salesman's interest to be up-front with his best offer. When it's included in the Bronze plan of the ACA, they quote the minimum price at about a hundred dollars a month. But that is not the whole pricing problem with Health Savings Accounts.
Boundaries. It comes down to rules for the product's boundaries. I fought hard for the HSA law, and am proud of it. Unfortunately, it contains a clause requiring customers to be employed, which cuts out policies for children. It also terminates at age 65, when Medicare ends your cost worries, but creates the unique ability to roll unspent HSA money into retirement funds. Essentially, "employment" limits health insurance to the middle third of an average lifetime, where only a third of health expense is found. Without a transfer mechanism, that makes life insurance difficult. So within the fixed limits, there also exists an unnecessary second uncertainty about its permanence. In the past, a significant portion of insurance profit comes from people who drop their policies. Why wouldn't they drop them, when they threaten to lose usefulness? People do make wrong choices, but in general, they know their best interests. Make it an option, and price it accordingly.
Compound Interest Grows with More Time. When allies want to make catastrophic insurance universal, apparently without required linkage to Savings Accounts, one has to worry it might pass in a form making other proposals politically more difficult. It considerably reduces attractiveness to subtract years from compound interest that way. Especially during sixty years of employer-based insurance, where custodial costs might be 0.1%. The proponents of catastrophic alone probably would not object to widening its age and employment limits, but you never know how negotiations could turn out. Custodial cost isn't hard to fix, but meanwhile, a final price must be stated, so I have a proposal.
Cost. There's no price mentioned for just leaving an account in the background whenever it shows zero spending activity for minor custodial cost. Remember, it provides an access route to retirement funding and greatly enhances yield. It's thus a valuable feature for both parties if dual coverage is permitted. In fact, a base price for zero spending activity, plus additional surcharges for months in use, might significantly improve present premium structures, which depend too much on sharing profits with a broker in order to reduce premium cost. The suggested option would approach charging ten dollars a month without activity, twenty-five dollars a month for outpatient spending, plus five hundred dollars a month for hospitalization. Internal subtraction from account balances could eliminate new billing costs; a short period of experience would restore predictability, as it does in banks.
Taxes. Dual coverage is commonplace in coinsurance, supplemental insurance, etc. so there is little reason to prohibit it here. Instead of catastrophic insurance firmly outside a tax-exempt savings account, as at present, the configuration might better become catastrophic with tax exemption, included within an HSA twin package. That would make an HSA equal with employer-based insurance as a matter of Constitutional tax equity. Instead of potentially offering everybody a chance to become a virtual millionaire if he is frugal, stripping the two apart in the suggested way might only leave coverage for the ultimate benefit of hospitals, the most expensive component of our present system, it is true. But that would eliminate year-to-year carryover, thus crippling innovations which greatly outweigh the nuisance.
Playing it Safe. and Shooting for the Stars. The proposal inadvertently implies: No funding for retirement, no removal of obstetrics from employer coverage, no male-female equalization, no Medicare buy-out option, no mechanism for lifetime coverage. It's a retreat, not a courageous advance, to split the Health Savings Account and discard such enormous potential. At the very least, we should all be fighting to permit HSA as a dual optional addition to any health plan, at any age, disregarding employment status. When we first find out what its mandated extent would be, we'll be able to estimate its cost.
And something else needs to be said. All of the first part of this book concentrates on using HSAs to transfer funds from the profitable age groups to the expensive ones. Without the linkage to an account, there is no way left to substitute for hospital cost-shifting, a growing evil. At the same time, it is necessary to restrain medical prices from rising. As Justice Cardozo observed, sunlight is the best disinfectant, so hidden cost-shifting tempts honest people into crooked behavior. Open-book accounting is better. Saving for your own old age is better than using the government as a bank to subsidize people you never met.
Preliminary Summary
Let's stop for a moment to review where we are. Several books ago, I announced my conviction that Health Savings Accounts are just about the only alternative to the Affordable Care Act to have completed all the steps of legislation, and many of the steps of establishing a national network. It has been tested over a period of thirty years and has probably discovered and corrected most of the many minor flaws to surface in testing actual operations of a big project. HSA could be implemented nationally during the sort of insurance crash which has been widely predicted. Unless it faces a national last-ditch rebellion by millions of people, a few corrective technical amendments could be added in a week, and the rest of its implementation would be temporarily solved. I'm sure I don't want to see such a thing actually happen, but if it does, I think HSA would get us through the crisis. Perhaps for that very reason, the crisis won't occur because it wouldn't accomplish much except further polarizing people. After all, most people are not desperately sick all at once, and Health Savings Accounts could patch something together for the many who are not desperately sick, while hospitals are full of administrators who know what to do. Without hysteria pushing us, of course, we could do better.
A Necklace of Pearls. A much better approach would be to continue a slightly modified Health Savings Account while we study how to add pearls to the necklace, one by one. It could be done in a year, although two or three years would be better. There are several alternatives available for demonstration projects if there is time to implement several, picking out the best ones. If our Congressmen didn't spend so much time commuting, or in the telephone call center soliciting, they might conduct a surprisingly large amount of legislation. In that sense, adding an atmosphere of urgency might be a good thing. I believe calculations demonstrated there could be plenty of money available to mount a full implementation, with only political and psychological resistance. From Pearl Harbor to Hiroshima, we fought an entire World War in that much time.
Topple the Finance System? In fact, I believe the Federal Reserve would be horrified at the prospect of giving thirty million dollars to every citizen, and resistance from their direction would overall be useful in redirecting 18 percent of GDP. We don't operate on a monetary standard anymore, and yet we do. You can't be certain any printing press money would assuredly be redeemed in gold, but on the other hand, we own multiple tons of gold bullion in Fort Knox and similar places. Something could be patched together.
Start with Cost Accountants. My advice would be to start with a large team of accountants, to fan out and assess where the bodies are buried, and how bad the damage might have been. For example, I would love to know what the tangled motives could be, for hospitals to overcharge so drastically for drugs, knowing full well the insurance companies will disallow the majority of such overcharges, and their own business office will discount most of the uninsured bills. There must be some financial motive, probably rooted in some overlap between independent laws, but all I ever got from hospital accountants was a smirk when I questioned it. A whole nation has become infuriated with such billing practices which seldom result in much revenue. It took me years to figure out why outpatient charges tend to be so much higher than inpatient ones for the same service, and why business executives force employees into captive insurance policies in spite of "job lock" and associated unpleasantness resulting from employer ownership of the policies. And so forth. The basic question is, what is preventing market forces from holding prices down. Please don't just give up and ask for more stringent price controls. Just take a hard look at indirect overhead costs, for example. Health insurers surely must know some of the answers; shake tips out of their accounting retirees.
And so we come to reversing the payment flow. If you only increase the revenue, don't be surprised if prices rise to wipe out the profit margin. The first part of this book solves a lot of problems by providing more money to the patients. We must establish a balance between fluctuating costs and cash flow which creates a competition between retirement income and health provider income, each of which is unrestrained. Instead, they should restrain each other if we design the system to encourage it.
Unfinished Business
Two things remain to be addressed: the cost of the catastrophic insurance, and the sort of agency which should sell the HSA service. Because both of these issues contain a strong political flavor, and because of the uncertain cost of the Affordable Care Act without subpoena power which the incoming administration will possess if it needs it, it is not possible to integrate these two features just yet. The power to delay action, inherent in the federalized system of governance, makes it difficult even to predict when these obstacles will be cleared away. Presumably, the Scalia vacancy on the Supreme Court will clarify much of this, but a time table is difficult to predict. Nevertheless, it is possible to outline the shape of what is needed.
Catastrophic healthcare insurance is "term" insurance, both in the sense its premium can be changed yearly, and in the sense that individual policies can negotiate their premiums to the degree, the agent is allowed to discount part of his sales commission in order to lower the premium. Thus to be fair, it must be admitted a general premium is difficult to state for a lifetime. The closest I have been able to find for a national insurance company is an offer of a $2000 yearly deductible, for $55 a month premium. But is it automatically renewable? The agent didn't know. What is covered? The agent didn't know.
Anticipating the Need from the Beginning
When you touch a hot stove, the signal makes a round trip to and from your brain in a fraction of a second. But we have been told the tip of a dinosaur's tail is so far from its head, its slowed signals required a second brainlet in the tail of the dinosaur to retransmit in a useful time period. Whether the example is accurate or not, the fable illustrates the utility of speedy information. If we construct a system of paying for Medicare with revenue derived from childhood, we can't wait for the signal to travel for sixty years to those expensive Medicare patients. It would be a useful feature for the two ends of the payment system to communicate instantly. That would only be possible if those two ends were in existence from the beginning of the system. Therefore, it might be important to reorder the sequence more or less simultaneously and to establish communication from the outset. That's true throughout the cycle, but it is particularly important for the two ends of it. The "pearls on a string" design concept might take care of this problem fairly simply.
It's preferable, for instance, to insisting all "pearls" should be revenue neutral and then forgetting about it. Doing that would raise the question of what to do if they don't all prove to be neutral. Evict a member of the circle? Impose a reserve requirement and tax it when ends don't meet? Does one pearl borrow a deficit from another pearl with a surplus? Tax the incoming receipts for last year's deficit? What should be done if some pearl is chronically out of balance, year after year? All of these possibilities may well be encountered, and solutions are more likely to be imposed if they are agreed in advance. Such arrangements are somewhat more secure if agreed as a condition of entry, since that forces revenue and spending to be pretty close at the start, making maintenance easier to continue. But what should the others do if one age group consistently produces a surplus? You wouldn't want to discourage that. What if they all produce surplus?
Inevitably, a more ideal solution is to impose or award a monetary solution, either paying an interest rate or awarding one, for internal borrowing. The problem is a monetary one and should have a monetary solution. For a start, the actually achieved investment return of the depositors seems like a good rate to begin. If the problem becomes a chronic one in spite of a common interest rate, some consideration should be given to modifying the content of the investment portfolio. With millions of individual HSAs owned by amateurs, they should be faced with an idealized solution as a default, trying as hard as possible to avoid doing it by regulation, but probably reserving regulation as a fall-back from market failure.
The starting concept is to invest in the whole economy, prospering or suffering as the whole nation does. A penalty fund composed of drug companies, scientific equipment makers, or makers of other medical products, could be constructed to divert the profits of such industries back to the patient population which supports them. If the effect of HSA deficits is to speculate on insider information, such profits might be refluxed back to the HSA as a means of discouraging speculation with the depositors' money. Or encouraging it for that matter, so long as the effect is to recycle speculative profits back to the people being gouged. Eventually, a system might be imagined of the patient population creating a venture capital fund, whose purpose is to stimulate research in products which transform speculators' profits into products which benefit them even more than in financial ways. We're getting close to government control of private industry when the discussion turns in this way, but perhaps some small experiments would be harmless, or definitions could be devised to distinguish venture capital investment from insider trading. We do seem to have a problem with establishing market prices for medical care, and perhaps there is some value in this type of approach. While we are at it, we might also have a look at the Food and Drug Administration, which seemed to be working well until Senator Kefauver meddled with it.
After a Long Tour of the Transfer Escrow, a Return to the Old Health Savings Account
The Escrow subaccount within Health Savings Accounts now stands unveiled for what it is -- a transfer system between plans. It pays for health insurance, usually not for current care but designated for underfunded future care. Regular Health insurance sometimes contains similar communication-and -funds transfer channels, but informal ones, patchwork for adding new features to existing ones, as in adding federal funds to state-controlled Medicaid. We here offer the escrowed Health Savings Account as an individually owned policy, specifically incorporating specific finances of a string of pearls to new ones with independent delivery- system regulations. As long as the pearls are careful, they can have a neutral transfer system, like the state-national one for the rest of the economy. Disputes are regulated by the courts under a common Supreme Court. The Court might be a new medical one, or use the one we already have.
This tripartite system not only conforms to the Constitution but restrains mission creep. That's historically why we have a Bill of Rights, although the document doesn't say so.
If the escrow subaccount is purely a transfer system between Pearls on a String, what is the function of the non-escrow portion? It is to permit each Pearl to fund separately and independently, and to make it easier to keep one Pearl from subsidizing another inadvertently. An argument can be made that New York now subsidizes Mississippi within the Federal Reserve monetary system, but that was for facilitating the approval of the various states -- the states which badly wanted a Federal Reserve would be taxed extra to get it -- but it is uncertain whether the same considerations apply to healthcare. The absence of cross-subsidy may be seen as an advantage in Healthcare, and therefore the issue should be decided by Congress. Perhaps decision could be delayed until the public gets a sense of what it wants after some defined period of experience.
When Health Savings Accounts were first discussed, it was assumed they would be funded by employer contributions, so and so many dollars per month or per quarter per employee. Tax deductibility would be decided once, and probably continue indefinitely for a class of employees or a certain type of employer. Actually, that proves to be the most difficult method to determine, because health insurance is given to the employee as a gift, and therefore has already been made tax-exempt. The potential for double tax exemption is raised, and various strategies could be adopted to simplify the tax status.
The double tax exemption might well be re-examined, but much of its unfairness traces to employer's inequitable tax exemption in the first place, which we have repeatedly suggested Congress equalize. It might be compared with using the income from municipal bonds, also tax exempt and tangled up in the minimum tax provision as well. If the amount of questionable deposits is overall fairly small, the matter can be taken up in a general revision of taxation and passed over for the present.
The Arithmetic Behind Our Claims, With Commentary
Knowing how to calculate is less important than knowing what to calculate. Any computer's search engine has several free examples of compound interest calculators. It is also useful to know a few short-cut ways of calculating approximate answers in your head, just to keep a check on computer calculations going off the rails. Be careful, because calculators can have bugs (or the computer's memory cache may not unload), but the commoner mistake is to calculate the wrong components.
The chief short-cut to know is a $100 fund of money earning 7% will double to $200 in ten years. Its related fact is, in fifty years a hundred dollars at 7% will equal (2,4,8,16,-->32) times a hundred dollars, or $3,200. With compound interest, the result is not linear. The 7% in 10 years shorthand is a subset of the "rule of 72", which says you can divide 72 by the compound interest rate, to get the number of years it takes to double. So while 7% doubles in 10 years, 6% doubles in 12 years, 10% doubles in 7 years, etc.
It's true, $100 at 10% will double every seven years, (as in 2, 4, 8, 16,--> 32x) in 35 years, or to $3200, reaching the same value as 7%, but in fifteen fewer years. Our economy contains more examples of 7% interest charges, than of 10%. The difference between 7% and 10% is surprisingly great and surprisingly meaningful in reverse. The 10% figure is often applied to impaired credit, or galloping inflation and therefore higher rates are often a warning signal, not an opportunity. Approximations permit the reader to recognize anomalies or to verify accurate calculations without repeating them.
Both approaches, short-hand and the Internet calculator, are recommended for verifying the following calculations, involving advance predictions which cannot be precise. One method of signaling approximation is to round off the answers to three or more digits of zeroes (2,400,000 is most probably an approximation, for example). We prefer fully calculated numbers, not to imply an accuracy which isn't present, but to allow the reader to follow arguments by recognizing components as they jump from line to line without elaborate identification.
-----------------------------------------------------------------------------------------------------------------------------------
Summary of the Math, With Caveats. This proposal is not free, it mainly substitutes investment income for government borrowing. The government thus benefits, but the patient benefits as well because he ends up owning the investment. This is an essential feature, since without it the consumer may see the proposal as benefitting the government, without benefitting himself. The calculations are necessarily rough ones, and 7% may prove optimistic, but the system is self-balancing. Borrowing is reduced, so in the example, the consumer gets the same product for roughly half its present net cost. "Roughly half" is approximate; the actual saving will be determined by market forces, both when he buys the investment, and later when he sells it.
To be explicit, this proposal involves passing early savings into the individual's own savings account, and immediately investing them. The consumer can measure his savings growth and later can watch his own bills being paid with them. He keeps any savings for his own retirement, and even more, if he is frugal enough to generate extra savings. Furthermore, he lives longer, which is largely only possible if his government has the money freed up to spend more billions on basic research to cure the diseases he might have died of. It is, therefore, possible to describe this whole system as a shrewd investment, growing out of cold, hard self-interest. Which, as the owner of the investment, visibly improves the individual's private benefit. So to return to the point we were making in the last chapter, hold off on ridiculing the idea of a newborn babe contributing money to it, it just looks that way at first.
To resume the arithmetic discussion, a deposit in a Health Savings (and Retirement) Account of $1650 1 yearly from birth to age 20 (from diverted Medicare premiums not yet authorized by Congress to be diverted) would result, invested at 7% in an escrow balance of $72,192 at age 20. If, at age 20, contributions of $825 yearly 2 for 40 more years (Source of revenue: diverted average Medicare withholding tax) were then substituted, both contributions firmly placed in escrow against college expenses and the like, might result in a balance of $1,260,000 at age 60. If investments realize less than 7%, this balance will be less. At age 65, 7% interest alone for five more years, generates a balance of $1,772,351. After subtracting a Medicare buy-out at age 65 of $134,000 3 plus $30,000 (income tax), a balance is left for retirement of $1,608,351. That hypothetical balance could provide a pretty reasonable retirement fund starting at 65, and eliminate additions to the Medicare debt, and by age 84 (average life expectancy) still allow for extraction of $18,000 4 to a designated member of the child or grandchild generation, at birth.Footnotes.For persons in transition with less than a full lifetime to work this out, a postmortem Trust Fund could continue to earn interest from average age of death (84) to the legal limit of a perpetuity, dedicated to paying Medicare shortfalls even though the subscriber is dead, until the age of 105 5 when further debts are extinguished. Meanwhile, the $18,000 legacy recirculates in a child or grandchild's Health Savings Account, replenishing the fund for a new generation. It should be emphasized this escrow fund is for Medicare, to which major illness is increasingly migrating. (We here suggest Congress waive the Catastrophic insurance requirement during the sixty years when no medical withdrawals are being made.) Current medical costs for younger people, balancing the Medicare migration, should diminish, and be revenue-neutral for the lifetime system. In any event, they do not include either surplus or deficit from Obamacare.
This condensed example is given to answer the question: is there enough money in the system? There probably is, and the trick is to find ways of getting it out. The difficulties are political and cultural, not financial. Other programs can join the system like pearls on a string, so long as they individually remain revenue-neutral, or subsidies are created to make them so. Success depends on achieving 7% returns from passive investing 6 , and revenue-neutrality among newly added programs. In a century, scientific discoveries might even reduce overall costs to the first year, and the last year, of life.
1 For its own reasons, this is entirely credited to Medicare Part B, and Part A gets none of it. As a further twist, it is deducted from Social Security checks rather than billed.
2 The allowable amount is $700 per year, with an income tax deduction at the end of the year.
3 This is my own guess as to the probable buy-out price of Medicare, age (65) to average life expectancy (84)
4 The is the CMS estimate of childhood costs, birth to age 25.
5 A perpetuity is defined as one "life" plus 21 years.
6 My own portfolio averages 6.7%. I have it from John Bogle personally that 7% is a stretch, selected because of its calculating ease.
Comments.
It is not intended to follow this outline strictly. For example, the transition period to it must be somehow shortened, avoiding transitional bond issues whenever possible. One additional twist would be to take advantage of the population continuing to live longer. Half of Medicare expenses are devoted to the last four years of life, so the transition period can be cut in half by dividing the revenue into two escrow funds, one of which is funded by the compound interest for 84+ years, and reimburses Medicare for the last 4 years of life it has already paid for. This puts the burden in half for the second fund, a particularly useful feature during the transition period.
If the public will not stand for using old-age premium money to fund childcare, or if there is resistance to shifting obstetrics cost from mother to child, either the retirement must be reduced, or new sources of revenue found. If there is significant resistance to other generation-shifting of funds, it is usually less important financially than socially.
Without any government changes, passive investing is gaining on active investing, by almost a trillion dollars a year. The financial community can be expected to resist the shift to passive investing. Whether they will stiffen their resistance or adapt to the change, remains to be seen.
Further, if the ownership of index funds can be tolerated, perhaps a segment could be directed to venture capital funds for cost-reduction of medical corporations, or even to transforming medical industry profits into cost-reduction for its products. When the health industry consumes 18% of the gross domestic product, it must consider new financing methods if it is to avoid either government ownership or a purely for-profit orientation. Perhaps healthcare could consider its place as an export industry.
In the meantime, healthcare must pay its own bills. Almost immediately I would establish a large force of accountants, to throw some light on central issues which are now conducted as either state secrets or business secrets. For example, I do not understand why hospital prices to uninsured patients are allowed to be so unrelated to their underlying costs, frustrating efforts to becoming market-oriented. Insurance companies have almost figured out how to protect themselves, but the public is appalled and unprotected. Perhaps the motive is the protection of indirect overhead as a mechanism of cost-shifting. The only self-interested group I can think of are the trial lawyers, who base their settlements on "seven times the medicals". But I have trouble believing they have enough power over the state legislatures and judiciary to whip-saw the public into tolerating sixty thousand dollar charges which the insurance companies discount to six thousand, and the hospitals write off willingly, knowing their real inpatient cost is limited by the DRG7 . And which I suspect cost the drug company much less than that to manufacture. If sunlight is the best disinfectant, let's have a lot of it.
7 Here, I am quoting my own personal health insurance EOB.
And I would like to see the true costs after taxes, of health insurance to various clients, particularly big business. It is possible to see two tax deductions, one to the employer and one to the employee, leading apparently to incentives for business to prefer high taxes on itself. There must be more to it than that, and one component is overworked congressmen. Each one of them has a million constituents and spends a lot of time on the phone.
Estimated Cost of Medicare Buy-out.
The data in this analysis are usually condensed to a single average individual, in anticipation of use in individual Health Savings (and Retirement) Accounts. The number of individuals enrolled in Medicare (55,504,005), obtained from the Internet figures published for 2015 by Centers for Medicare & Medicaid Services (CMS), is divided into the total 2014 budget of the program ($373 billion) =$6,720 Medicare cost per person per year for 20 years average life expectancy at 65, or restated as roughly $134,400 per person per Medicare lifetime. As a check, Medicare cost is said to be half of lifetime medical costs of $350,000 or $175, 000. This is the ballpark guess of a Medicare buyout cost.
The accuracy of this figure would improve by excluding 9 million recipients under the age of 65 eligible by reason of disability, not by age. However, figures were not provided separately to distinguish costs of the disabled from the 46 million who became beneficiaries by attaining age 65. Assumed here to be roughly the same, disability probably costs more.An important side point is not the exact amount of cost, but rather that this composition includes everyone, rich or poor, who is over 65. These figures therefore definitely include the indigents, and if anything includes a disproportionate number of them. This should be attractive to single-payer enthusiasts, who wish to extend Medicare coverage to everyone, and who find that employing extra eligibility based on age rather than income simplifies their task of persuasion. The calculations which follow are therefore not a "rich man's proposal" at all because Medicare is not a rich man's proposal. Its fault is being funded by pay-as-you-go for several decades.
A second non-obvious fact of regional variability is readily inferred by comparing $6,720 per year (the overall Medicare average cost) with the $18,000 annual premium for New York employer health plans cited in the newspapers. Quite obviously New York prices are higher than those in a small rural district, but not three times as high. The New York employees, like the Medicare beneficiaries, must include a large subsidy of non-paying clients by paying ones, because of New York laws and demography, and are thus "conservative" estimates of revenue requirements in a limited sense. That the average is an overestimate is still further suggested by the $5700 annual premium charged for Medicare Part F for the highest income bracket, including a profit margin for the contractor. (Medicare sells coverage at wholesale prices and allows the Part F vendors to discount them, while still making a profit by constraining provider reimbursement.) Counting on the tacit reinsurance of the "risk corridor", some contractors lost money, but evidently, not all of them did. It should be comparatively easy to calculate a more accurate estimate of costs by excluding under-65 beneficiaries, but the prediction-- that wholesale is less than $6720-- will almost certainly be borne out.
The underlying principle of our proposed example is equality with the present Medicare public charges. That's a rhetorical boundary, not an actual one. And an example, not a rule. Congress can set these charges where ever it pleases. Eventually, the charges must reflect an underlying need for them. For the present, current charges will suffice as an example.
Current revenue comes in two approximately equal components. The first comes from the withholding tax on the employment of people aged 25-65, the amount of which is specified as 2.9% of the wages, 1.45% from the individual paycheck, and 1.45% from the employer. From the Medicare annual report, it comes to an average of $700 per year for 40 years = $28,000. The other half, comes from the Medicare premiums (applied to reduce the benefits of Social Security checks by $1400 a year) from age 65 to the date of death, on average of 20 years = another $28,000. Some accountant should explain attributing all this to Medicare Part B, and why Part A is not attributed to hospitals at all. It seems entirely arbitrary, but you never know. Since contributions to Health Savings Accounts are tax-deductible, their value increases. We use the 18% flat-tax figure offered as a weighted average of real income taxes, so the HSA annual deposits are effective $825 and $1650, ignoring the attributions. That's another example; does it make sense? To repeat, total average lifetime spending by Medicare is $6720 per year times 20 years = $134,000 ($2580/yr left for retirement). Is this a reasonable price for a buy-out? I doubt it, but even this figure is surmountable.
Transition Costs.Investment Income.
There are two ways to increase investment income: invest the same at a younger age, or invest more over a longer period of time. Depending on the sequence of investing, these previously collected sums should produce enough to buy out Medicare, with some left over to finance a moderate retirement -- without increased debts to bondholders. Of course, you can't spend it twice, but this is in an escrow account. The alternative is to have a separate account, and it is hard to say which is simpler. Although its internal distributions and cross-subsidies remain perhaps a little unclear, the over-65 retirement benefits are likely overestimated. The reader must weigh these approximations for himself, keeping one principle foremost. If the approximation does not comfortably dwarf the projection, it is too close for comfort.
In any event, the entire Medicare program must at most borrow $78,000 times 55,500,000 beneficiaries divided by 20 years of the collection -- each year -- or roughly $200 billion of a 373 billion budget -- for a transition from one system to a better one. Moreover, alternative proposals for transition are suggested in later chapters. Even Wall Street veterans concede the U.S. Treasury has an outstanding reputation in bond issues for wars and depressions, so their advice is worth consulting. Once again, that figure is high to the degree the 9 million disabled on average have different costs than the 46 million elderly, low to the degree inflation becomes rampant and largely unpredictable in sum. As far as frightened investors are concerned, the escrow rules should actually lessen the risk of panic illiquidity. Whether they see it that way or not, they are investing in the durability of the entire long-term American economy by investing in total stock market indices. It is safe to respond the Medicare deficit is made wildly unsustainable by pay-as-you-go financing, whether privatized, or not, and the proposed approach might actually help quite a bit. Furthermore, starting with a contingency fund of only $100 yearly from birth calculates to reach the same number with a little margin of error built in. But it includes no pension, and probably less elimination of debt.
The Health Saving Account law already provides potential revenue relief to the beneficiaries in two main ways: a tax deduction for deposits, and the freedom to invest deposits, tax-free, in any way agreeable. Furthermore, it collects no tax on withdrawals for medical purposes. (There is one exception which might be changed: taxes are not collected from medical expenditures, but are collected on HSA to IRA conversions.) Medicare, on the other hand, collects an average of $700 yearly for 40 years (25-65) in salary withholding, and $1400 a year for 20 years in Medicare premiums. That's about half its cost, another half is a deficit which must be borrowed. Using the rule of thumb of 7% doubling in ten years, an investment return of 7% in an HSA of the same money which resulted in an unsustainable deficit by pay/go, would be worth $825 per year (700 from Medicare + $126 extra value from the tax exemption) or $185,000 at age 65 (or even more, if Medicare costs are substantially less than $6720 for over-65 subscribers). That would buy out Medicare with $161,459 or so to spare, which after taxes would be $132,396 by subtracting the real average income tax of 18%. That much ought to provide approximately $8,000 annual retirement for the 20 years 65-85, the average life expectancy at birth. We can do better than that, but some money will have to be spent on the transition costs, so it's a maximum, providing an individual HSA can earn 7% on its investment. And worse than that if it can't. At least, we can sustain the point that, alone among health insurance programs, HSAs transform any surplus after taxes into retirement income in the form of Individual Retirement Accounts, (IRA), and provides a way to generate potential surplus which is then likely to be under-stated.Future Projections.
It will be noticed we have left two features of HSAs unexploited, and one fly in the ointment unmentioned. In the first place, you have to be younger than 25 to take full advantage of what we have described, and you have to wait 40 more years to receive any tangible benefits. Secondly, the $3400 per year voluntary contribution deposit limit to HSA is unused and we suggest those who can afford it, spend it all on looming transition costs. These are both artificial limitations on the simplified example, a standing invitation to exploit new features. For example, look at what a hundred or so dollars would do, if deposited at birth. Of course, you can add more, up to a $3400 limit per year. The result would probably be in the millions. Age and contribution limits should first be expanded, and the employment requirement eliminated. By expanding the time available for recovery, these features would actually enhance the safety of the investment.
An important stickler is, the law requires a high-deductible Catastrophic backup throughout the life of the HSA but makes scant mention of overlapping insurance. When age and employment limits are removed, this needs to be addressed by "or it is equivalent", and possibly then more specifically, since it leaves the HSA at the mercy of ambiguities its competitors can manipulate.
The Importance of Solving Childhood Health Costs.Let's be frank about projections so far in advance. They are meant only to distinguish areas where funds are "comfortably adequate" from other numbers which are more dangerously "barely adequate". The imagined precision is retained as a way of following particular numbers through the argument. Combining the two, a modest sum of $100 added to the account at birth would slowly grow to $542 (at 7%) by age 25. But that relatively small amount would be added to the withholding tax contribution at age 25, and even singly might grow to be $8,127 by 65. By age 84, without any withdrawals, it would grow (single) to $31,450. Combined with $825 a year , however, starting at age 25 with $825 (withholding tax equivalent) added yearly, it would grow to $180,500 at 65, and subsequently without withholding tax addition, might re-grow (without withdrawals for retirement) to $166,000 by age 85. It would be in an escrow fund for Medicare, so it could not be spent for other purposes until age 65. There would be a withdrawal, however, to buy out Medicare at age 65, of $134,000. So the reduced value to $41,500 might re-grow in 20 years (age 65-85) to be $166,000. Using it up for retirement, however, would provide an annual pension too small to depend on for distant calculations. For the retirement to be a real incentive, it would have to last as long as projected longevity. The person would have to supplement it with private savings and investment along the way, a normal situation for rich people, but a frightening novelty for most people. Another step is required before such a lifetime venture is undertaken. Therefore, what is presented is not the best case. It will be improved upon later, especially with cutting the numbers in half with the Last Years of Life approach.The HSA act was originally intended to appeal to young people, whose current medical needs were often small ones, and whose distant retirement looked utterly remote. Since the Affordable Care Act has considerably confused matters for this age group, we have decided to avoid discussion of the working age group, at least until after the 2016 Presidential elections give us some indication of where things are likely to go. The proposal does cover Medicare, retirement, and newborns -- substantially everything except what Obamacare covers. When the future of ACA becomes clearer, it will be necessary to write another book to integrate the issue of filling in such gaps. The HSA law does permit individuals to contribute up to $3400 annually to the accounts, but solvency seems temporary unless the age group 25-65 can produce a surplus to subsidize other groups. Here, we only contrast the HSA with about 100 to 250 dollars per year, from birth. That makes calculation easy, and small, but it grows relatively slowly and well might have to be supplemented at later ages, particularly during the transition period.
That venture would be a rearrangement of revenue streams. The earlier a sum is invested, the larger it will grow; in meaningful terms, it is worth far more for retirement if you start the same contribution twenty to sixty years earlier. In order to get the most out of the same investment, Congress might remove the employment requirement and extend the age limits, both up to death and down to birth. Maximum revenue could then be extracted if the financial equivalent of the Medicare premium began at birth, and twenty years later was followed by forty years of payroll deduction. Essentially, this means moving the equivalent of Medicare premiums to some form of a trust fund, and re-directing the payroll deductions to the Health Savings Account as described. These sixty years of investment leave five years unfunded, so if the Medicare age limits remain fixed at 65, the trust fund could begin as late as the fifth birthday.
Such rearrangement of the payment stream would generate a fund in the millions at age 65, allowing for much more comfortable slack in the investments, and supplying ample funds to transfer to a grandchild. Funding the health needs of children is the greatest single unaddressed problem in all health planning. It gets little attention because it seems so impossible to pre-fund the birth costs of a newborn. And it even stimulates misinformation, such as the mistaken belief that health costs of newborns are trivial. They are not as great as the cost of dying, but the financial resources of the parents are more strained. They spill over into grievances about the higher health premiums of women, in an era where feminism has had hidden effects on politics and even Supreme Court decisions. The transfer of Medicare premium funds to grandchildren has synergy with grandparent funding of obstetrics, and the Health Savings Account provides a vehicle to do them both. This particular caper is a political issue, requiring Presidential leadership; it is definitely not a financial issue just waiting around at the end of a lifetime of compound interest.
Any greater results would have to rely on additional donations to the contingency fund, or spectacular good luck in the stock market. This is therefore just about the limit of what a favorable arrangement could provide; except for outside contributions, any other arrangement would provide less. For example, switching Medicare premiums to fall between 65 and 85 (the current arrangement) would reduce the benefits by a third, as might a bad decade in the stock market. Suffering both reverses at once might wipe out all retirement benefits. But short of an atom bomb attack, it is hard to see how the average investor would lose money by doing it. Most of this plan requires changes in present law, although the growing national debt will create pressure to do something major to change the future trajectory of Medicare. The finance industry, already under strain, may resist. Consequently, the opportunities and drawbacks of Medicare Part F for employers also ought to be scrutinized, particularly as long as large employers recoup so much from their various unshared tax exemptions.Long periods of unemployment could destroy this tempting dream, as could a protracted poor investment experience. The ordinary person would have trouble finding an institution which would accept amounts smaller than $100 without long-term contracts allowing the institution to trade short-term losses for long-term benefits. In the next section, we must, therefore, take a moment to reflect on the finance industry. And then we will return to this lifetime plan, by adding the Ends of Life approaches.
Imperfect Agency: HSA Administrators
Particularly if Congress amends the HSA act to broaden its scope, some serious thought should be given to establishing the rules for selling and administering the Health Savings Account itself. Just about all likely candidates have some conflict of interest which cautions us about distributing monopoly positions, or pay to play, as it is sometimes called or nepotism as the form it sometimes takes. Nevertheless, when there are monopolies, kick-backs, formal or (usually) informal, proliferate at the expense of the customer, who then must "pay rent" for non-monopoly (arms-length or fiducial) behavior. It would be nice, for example, to feel if the customer detects churning or front-running, the customer would have recourse to some court, and not necessarily to have the issue foreclosed by involuntary arbitration agreements. A change in culture is always to be preferred to an imposed system of control.
The present structure traces back to the Constitution's Tenth Amendment, essentially telling the Federals they can deliver the mail, issue the currency, and police the borders, but anything else is to be conducted by state governments. In the early Nineteenth century, when corporations took their present form, that meant every new corporation had to have an individual state law, enabling and defining its rules. When it became obvious the proliferation of corporate charters made this system unworkable, states mostly converted to Uniform Corporation Acts, defining the rules for all for-profit and nonprofit corporations within the state.
By the end of the Nineteenth century, even this move toward uniformity became cumbersome for interstate corporations, and the push was on for uniform national laws, the Tenth Amendment be damned. The Civil War had discredited states rights enough to make nationalized corporations a viable entity. The first railroad, the Camden and Amboy RR in New Jersey, was given a perpetual monopoly on railroads in that strategically located state, and it took most of a century to untangle this complexity. Federal agencies slowly filled the gap for big corporations, but almost all corporations continue to start out small and state-regulated. So the result is informal flouting of the Tenth Amendment by the Courts, reaching out for a one-size-fits-all solution. Strangely, the State of Delaware moved into this chaos with its Court of Chancery, to decide controversies where there is an obvious injustice, but no law exactly fits it. This history would seem to suggest that agents for Health Savings Accounts will have to be state-regulated, even though they grow from Federal law. But if they are to be evaded, eventually another way will have to be found to make interstate HSAs viable and efficient. One thing standing in the way is the McCarran Ferguson Act, which lays out that no state need to be hampered by the orders of any federal agency, concerning the "business of insurance." It does not improve the rest of the world's opinion of us, to be observed flouting our own Constitution.
We'll leave untangling this mess to others in the future, and concede that as long as HSA administration remains a small business, its regulation would speed along faster in fifty state legislatures, providing big corporations leave it alone and their lawyers ignore McCarran Ferguson. The consequence of all this is to relegate Vanguard, Fidelity and the rest of Wall Street, to the status of vendors to small businesses who in turn mainly respond to available services and fees without flagrant kickbacks to Wall Street, placing the customer's interest ahead of their own. If our arithmetic is accurate, the volume of business should grow into custodial accounts in aggregate of billions of dollars worth of stock certificates. But they would essentially remain small businesses, eventually requiring some nation-wide consistency governed by the House Ways and Means Committee and the Senate Finance Committee. And yes, some Federal agency to oversee the paperwork.
The structure outlined above has the effect of leaving the packaging of the index and other securities to Wall Street, but the recommendation of which one the customer should buy should be delegated to local small businesses or professionals. At present, computerized consolidation of stocks into an index stock, conducting an IPO, etc., are complex tasks requiring professionals, whereas the advice as to the best one to buy for a situation, is a mom and pop custodial function, requiring a small staff, a large lock-box at the bank, and a knowledge of customer needs. By and large, it requires no great talent to select among products (indexing took care of that), but in time it will require the talents of an accountant, and the integrity of a saint. Over time, these mom-and-pop small businesses will grow through franchises and other mechanisms familiar to business in general, and perhaps require a different system of regulation, with a re-examination of the forces at work.
This overview of the probable business future argues for as much choice as possible. At the moment, we are being treated to the spectacle of brokerage houses violently resisting fee-only arrangements, so it is up to them to suggest a better resolution for the customer. Their eventual capitulation is not a foregone conclusion, they could drag out the change for quite a long time. Nevertheless, this business ought to explode if the middle-men took less of a cut from their monopoly, and customers could approach a 7% investment return with more confidence. Turning in the opposite direction, I find a doctor friend of mine is unable to retire because a stockbroker churned the trust fund account of her mentally retarded brother into extinction. The court question, of what sort of court should set similar things right for the HSA, should be settled early during the period when the decision between state or federal overall control, still remains fluid.
As a footnote, a reversal of fiducial requirement was slipped into the 2016 lame-duck period, so this issue must be quickly addressed.
Re-Arrangements and Addition of Childhood
Preliminary Totals
Actuaries have one way of totaling up the average lifetime cost of healthcare, which comes to $350,000 per person, in the year 2000 dollars. Their method of the cost estimate is to ask insurance companies to tell them how much they spend at each yearly age. That potentially has three flaws, although perhaps some of the flaws cancel each other out.
The first comes from getting reports from insurance companies, which might well minimize the cost of insurance itself, sometimes estimated as high as 17%, sometimes as low as 2%, for Medicare. The Medicare figure is surely on the low side, with much of its cost attributed to other sources than CCS -- the cost of Treasury and Congressional involvement, for example, or military administration. But as a preliminary guess, let's say 2-17% is a possible statement about this source, or $7000-$59,500 per person, per lifetime.
The second is medical research, which is $33 billion a year, or $1000 per person-year, $84,000 per lifetime, or 4% extra, for the National Institutes of Health, alone. University and pharmaceutical expenditures overlap somewhat, but surely double the research cost to 8%. Research cost is part of the overall equation, as the companies loudly complain. Training professionals is similarly mixed-source, but certainly another 2%.
And finally, depending on how you figure it, there is an uncompensated subsidy of one subgroup by another. The cost of Obamacare is difficult to measure, but surely seems a major cost to the people who pay extra to support it. For the present, we treat the Affordable Care Act as tentatively revenue neutral, which is to say: adding nothing to the non-escrow portion of the Health Savings Account of the age group 26-65, and/or costing no more than inflation adds at 3%. Inflation lends a working supposition to the idea that total lifetime healthcare cost is somewhere around $500,000 in 2017 dollars, plus 2-17% for health insurance, 2% for training, and an unknown amount for ACA. Call it $600,000 a year, with research entirely funded by independent sources. Total revenue expended for health might easily reach a million dollars per lifetime per person by the end of the decade, by this method of calculating.
Bottom Line. Calculating the expenses-consumed we reach about the same conclusion, but both approaches are confounded by cost-shifting. Let's skip ahead to approximate where the new proposal places us. From childbirth to age 25 we estimate $18,000 cost, having shifted $10,000 of obstetrics from the mother to the child, and donating the remaining $10,000 from the grandparent. From age 26 to 65, starting at an HSA balance of zero, we break even by assuming a shifting balance between current expenses and subsidy from other generations; that is, the escrow account keeps growing while non-escrow also grows but falls behind by age 65. We thus project a net voluntary transfer (of $65,000 for a Medicare buy-out) leaving $ 135,000 for retirement. They would surrender $10-18,000 of childhood expenses when the same $10-18,000 is transferred from the working generation and then later re-transferred from retiree surpluses to one grandchild's HSA.This is America, built on several centuries of optimism, or risk-taking. No one needs to warn us of the possibility of miscalculation. We have sometimes, indeed, experienced miscalculation and over-optimism. But if all goes well, we could end a century of risk with bills paid, longevity further lengthened, and money in the bank from betting on the American economy. If things go badly in the stock market and laboratory, or if they go bad in wars and epidemics, our reserves will suffer and planning will work out wrong. Obviously, in a gloomy future, plans must be curtailed. We count on the stock markets to be our banker, but if they appear to be based on a miscalculation, we may once again blame it on the bankers. But let us hope we have the sense to modify our plans, particularly by adding the First and Last Years of Life reinsurance system and dipping into our reserves sooner than expected. That's for volatility. For real miscalculation, major modifications of the delivery system may be needed, but it's difficult to imagine wanting anything more than longevity.Up the time of death (average age 84) scarcely any new money has been added to the medical system, except for money previously uncomplainingly paid during working years from working-age people toward Medicare, plus Medicare premiums paid by seniors. These funds, which currently produce unmanageable deficits, would now be paid into the Health Savings Accounts for age 26-84 deficits from awkward timing. For the most part, the surplus should replace hardship, for deficits anticipated for age 66-84 in the form of $65,000 for a Medicare buyout at 66 and a $10-18,000 Childhood buy-in at age 84. Surplus or deficit may arise between the HSA and Medicare at age 65, or again between the HSA and Children's funds at 84. If any deficits appear during this interval, they could be paid by extending Trust Funds to age 104 regardless of whether the depositor is still alive, and only then must the remainder being written off as national debt. At that duration, compound interest grows quite surprisingly. During the early transition, these deficits might appear large, but many of them could later be written off easily against looming reductions in Medicare costs caused by a century of research discoveries, or stock market returns multiplied by compound interest.
Last Four Years of Life Reinsurance
Half of lifetime medical expenses are reimbursed by Medicare. And half of Medicare represents the cost of the last four years of someone's life.
Having got middle-men off our chest, we return to a search for other ways to introduce greater efficiency into the medical financing system. That might be accomplished by reducing medical prices or eliminating medical problems with the research. Rationing, however, never seems to work without distorting resource allocation, and medical research is best left in the hands of the scientists. Here, we offer a third method, which is to increase the revenue by modifying its structure, while minimizing changes to the medical system it pays for. The National Institutes of Health (NIH) research budget is already $33 billion a year, and somehow that seems like enough. Right now, our mission is seeing what might be done with the payment system to fit its purpose.
Up until recently, paying for medical care has been treated as just part of paying for anything else, but it has some special features. For example, because of a welter of scientific advances, it is possible to imagine a future when nothing except the first and last years of life will contain any substantial medical costs unless they are self-inflicted to some degree. The American public seems consistently adverse to subsidizing self-inflicted conditions, which it views as a disguised form of suicide. Since homeless, addicted males seldom have children because females avoid them, non-cohabitation of the Lizistrata sort is a hidden way of punishing them for failing to support their families. With exceptions of this sort, medical care is an expensive need which will gradually become less essential. Except the system should be arranged to accommodate unexpected changes because change itself is confidently expected to occur.
What's Reinsurance for the Last Years of Life All About? Ends of life concepts were designed to take advantage of the permanently J-shaped curve of medical costs to increase with age. They divide revenue into two investment classes maturing at different rates. The longer the period of compounding, the more we should want to save it for heavier expenses. (And the less we should be interested in spending a valuable resource on age groups with little to fear.)
Start by cutting escrowed Medicare costs into two subaccounts, differing in content and thus in timing. Overall, while all curves of lifetime health expenses are J-shaped, skewing progressively toward old age, containing roughly half of the expenses in Medicare, and half of that (one-fourth of total costs) concentrates in the last four years of life. (Later on, we will apply the principle to cover the increased cost of being born, addressing that initial upswing of the J.) There are six or eight variations, but our version has Subaccount A starting at age 25, the least expensive health year for the typical person, but also the time when Medicare withholding tax begins its forty-year climb. Our Subaccount B, by contrast, begins at birth with a major obstetrical expense, but currently must abandon this opportunity to achieve maximum compounded interest because of a newborn's lack of income. (The age group from 25 to 65 is temporarily abandoned to the Affordable Care Act until the nation decides whether to continue ACA, change its scope, or abandon it.) What follows is a description of financing everything except the Affordable Care Act, while temporarily accepting the implausible assumption ACA will seem revenue-neutral, until after the public gains full access to its books. The big data approach should speed up this examination.
Therefore leaving out ACA, and examining only what is left, Subaccount A buys out Medicare voluntarily, paying for retirement (which usually begins at the same time) with what is left over, in return for the hope of retirement income. Subaccount B pays for the last four years of life, thus removing half of Medicare cost from part A, as well as funding one grandchild equivalent until he or she reaches age 25. In effect, Account B pays for childhood, later materially helps buy out Medicare by re-insuring the last four years of life and eventually becomes the basis for First and Last Years Insurance as a pre-paid substitute for pay-as-you-go Medicare. It may take a long time to get there, but that's the goal. Meanwhile, it effectively cuts the cost of Medicare into two equal parts and thus makes it more digestible for a buy-out. (By applying different revenue sources, its timing is different in the two pieces.) During the long transition period, the payments for Medicare are divided between the two funds to satisfy obligations, one of them is extinguished, the other continuing to fund retirement costs until the death of the subscriber. It amounts to shifting the costs and revenue around, taking advantage of longer compounding for heavier costs. Ultimately, it raises questions of how far the public is willing to go with all that, including donations to another generation, and being educated it's a sensible thing to do. By accomplishing many things at once, it acquires what mathematicians call elegance, but the public may regard it as too complicated unless it is accomplished in steps.
If, during the transition phase, there still remains a deficit, consideration might be given to establishing postmortem trust funds as a fall-back to continue the interest compounding until its debts are paid, and/or conceivably pre-birth trust funds anticipating childhood costs (see below). At the moment, mandatory conversion into an IRA would be subject to tax. However, we hope Congress can be persuaded to defer the taxes until the date of death. In this way, unpaid taxes could be utilized to extend retirement benefits until they are needed, and taxes can be discontinued if they aren't needed. Meanwhile, savings continue to gather investment income. During the transition, there might be several revenue/cost mismatches which require expediency and/or bond issues, and there is no reason to see it as shameful.The substance of the following table is that the investment of $250 at birth would result in $21,714 cash for retirement at 65, plus the present value of $28,000 in Medicare premiums, plus an uncertain value for the improved structure. But this improved structure assumes no interest is gained on the premiums, and in fact, they would probably be discounted to present value. So, it seems better to sacrifice the structure for improvement in cash flow. That would be summarized as follows:
The last four years of life are not the same as the last four years of Medicare. It is only possible to establish which four years are someone's last ones after the date of death is known. The proposal here is to set one half aside as a special fund for the last four years of life because old-age health and retirement funds will generally not be needed for decades, but costs will eventually be heavy. When costs can finally be known, the Last Years fund reimburses Medicare. Some funds must be constantly consumed for medical care, and they should utilize funds which are soon to expire, and not be escrowed. Escrowed funds are usually set aside for distant medical costs, and like Odysseus bound to the mast, keep him from yielding to the temptation to use them prematurely. Meanwhile, a third, non-escrowed, subaccount is free to manage current expenses, and need not be dealt with further in this section. Medicare doesn't know when you are going to die any better than you do, so it reimburses every cost at the time it is incurred, spending revenue about as fast as it is received. Account A was designed for future healthcare costs in all but the last four years, a burden considerably lightened by removing those last four years and letting the revenue grow. The switch isn't exactly insurance, it is re-insurance. The beneficiary is then dead, and even his relatives would scarcely notice this transfer has taken place, except by auditing receipts.
When costs can finally be known, the Last Years fund reimburses Medicare.
As a matter of fact, Medicare needn't reimburse the particular costs for specific last-four-years clients, since there are only two parties directly involved, both of the insurance companies. By maintaining aggregate books, Medicare merely needs to determine the average cost for all its dying patients, to emerge with equal aggregate reimbursements for everyone who dies. Whether this bookkeeping short-cut can actually be utilized, however, depends on whether variations in regional cost are too substantial for local politics to tolerate. Even then, statewide averages might serve. This detail is an accounting efficiency which the two parties could sort out with Congress.

|
 Everybody is born, everybody dies, and nobody does either thing twice.
|
Eventually, the taxpayer under present law might pay long term capital gains tax of 25% on withdrawals from tax-free accounts; revising such tax laws is under discussion. The present value of such revenue is difficult to estimate, but it would likely be offset by the reduction of interest rates paid on the indebtedness, which is also hard to predict. And all of this would be offset by a long term rise in the stock market, also subject to capital gains tax. Since a rise in bond, rates seems almost certain at present, and thus a long-term rise in stock market averages is likely, it seems reasonable to suppose the government would make a huge profit on an expanded Health Savings Account. Only a major prolonged recession or a war would reverse this judgment, and even that would see bond revenue mitigating the stock market loss. The private purchase of huge amounts of stock would certainly raise stock prices and might put any qualms of the IRS to rest. It is true, stock market exuberance can lead to a bubble which collapses, but this observation never seems to restrain a bull market.
To review the matter, splitting Medicare payment into two escrowed subaccounts and one non-escrowed one, has simple purposes related to transitioning between systems, and really isn't that hard to understand.
1) Technically, it allows longer-term funding to avail itself of compound interest for longer periods, largely by devoting more attention to the matter and ignoring the original assignment of the funds.
2) Secondly, a transfer of $18,000 out of a million-dollar retirement fund would not meet with nearly the same resistance as it would from a fund scraping the barrel to survive. We take this intergenerational transfer up in a later section, but here it should suffice to summarize, this transfer would solve a number of problems which hitherto have been treated as issues one simply has to endure.
2) Part of a spectacular revenue enhancement comes from adding twenty years of compounding a rather large sum ($1650 annually for 20 more years) onto the end of a long period (40 years) of compounding a smaller contribution, of $825 a year. Reversing the sequence (Medicare premiums first, payroll withholding subsequently) would generate even more revenue, and advancing Medicare premiums to childbirth-to age 25, would generate the most. Furthermore, any one of these sequences follows the design of original Health Savings accounts by ultimately depositing left-over funds into the individual's retirement account, as a sort of reward for being frugal. Acquiring revenue for other insurance components, what had previously been a unique feature of HSAs for retirement, it discourages early diversion of these funds to unrelated government activities (aircraft carriers, etc.), recurring anxiety of beneficiaries. Perhaps more to the point, it gives the client a tangible reason to be frugal, at an age when such ideas are not entirely natural.
3) The proportions of the public who have already consumed, or paid for, parts of Medicare will vary with their demographics, largely related to the year they happen to have been born. But a rising proportion of cost in one compartment means a decline in the other half. Because revenue often has unexpected connections to cost, this will always be a rough proportion, but it ought to help placate the sense of helpless public disenfranchisement which attends all major transitions.
4) And finally, this new configuration approximates the way things are probably going to go anyway, with ever-increasing concentrations of medical cost pushed toward the end of life. Not everybody dies at Medicare expense right now, but the universal trend is for people to die later, eventually making it approach 100%. Further, as we describe later, it provides a framework for first year-of-life coverage as well. That is to say, the trend is for health insurance to narrow down to the beginning and end of life, as science gradually eliminates the disease. One day in the far future it might be said, nothing else is left of major health costs. Everybody is born, everybody dies, and nobody does either thing twice. Insurance as we currently think of it will slowly become a thing of the past, replaced by what is more frankly a pre-payment methodology on a much grander scale. And eventually, the public will see it happening, which eases political resistance considerably
Buying Into Medicare, Several Decades Early
Campaigning for President, Hillary Clinton brought up a proposal in 2016 to permit the uninsured to buy into Medicare coverage between the ages of 55 and 65. Eight years earlier, the Congressional Budget Office estimated such coverage would cost about $7600 a year per added client. The appeal is particularly strong for divorced women because employer-based coverage ends when employment does. Nevertheless, the CBO estimate would make this segment the most expensive component of Medicare, so gradualism may have to wait for some enhancements.
It happens I was working on similar calculations for this book; the CBO estimate of what medical care once cost this 55-65 age group before 2008, seemed reasonable. The shape of the curve has probably not changed much in eight years. Nevertheless, there are now several reasons present estimates may be underestimated. The Consumer Price Index for medical care has jumped around but increased 3.4% a year, or over 30% more than the level eight years ago. Health insurance costs have probably exceeded overall costs for fifty years, so forecasting health insurance premiums has always included some guesswork. The cost curve for 55-65 is at the high end of a rising rate. Including more sick people also means fewer well ones, so there is leverage. The data is based on aggregating claims data from still earlier years, so insurance costs tend to struggle to catch up with community costs. The cost of care inflates, but this portion of the population is at the high end of commercial coverage, so it probably escalates disproportionately.
In addition to statistical underestimation, there are probably invisible sources of confoundment. With Medicare just ahead, these people hold back on elective expenses, with lack of insurance exaggerating the tendency. If the experience with Medicare in 1965 or the ACA more recently, is used as a guide, we can expect a backlog of untreated gallstones, varicose veins, perforated eardrums and the like, to make an appearance once they regain insurance. That's quite different from pre-existing diabetes, heart failure or strokes, and will take longer to appear because it is more deferrable. It would not be surprising to find that post-insured costs are 50% higher than the 2008 CBO estimate, and will remain abnormally high for a decade. Finally, the method of data collection almost guarantees a low result. The published papers relate insurance companies were asked to report their claims, but no mention is made of insurance overhead, while the deductible and copayment ingredients are merely estimated. What seems to be implied is the data does not include insurance costs, probably for competitive reasons. And all of this is before we debate how much to subsidize, or how much it will encourage unemployment if we are too generous.
I surely do not know what is fair and proper to subsidize and can see no good way to estimate it. Medicare is already financed by about 50% government subsidy from the general fund, as well as another 25% from payroll deductions, which have already been collected at a probably lower level. With inflation at 3%, a 3% payroll deduction is less than it seems. No mention was made of the revenue sources for this proposal, but hidden extra subsidies of $5000-6000, per person per year, would seem to be buried in it for someone to pay. While no one disputes the genuine hardship this group experiences, this proposal would only be a bumpy introduction to the practical difficulties of the "single payer" idea.
There is little doubt working women are handicapped in many ways by higher health care costs attributable to pregnancy, and this handicap results in a number of undesirable social consequences. My suggestion has been to shift the cost of obstetrics from the mother's insurance to the baby's, which usually amounts to saying they should be shared by the father's employer through the father. While this shift would have the undesirable feature of shifting costs from the working age group to a childhood group which requires some sort of compensating cost-shifting, it mainly lengthens the period for compound interest to generate investment income, thus lowering the effective cost. A glance at the following chart clearly shows the bump in female costs between ages 15-45, transfer of which would go a long way to bringing the costs of males and females to much the same level. Since this cost would ultimately be born by a transfer of surplus revenue from the Medicare group, it would heighten the attractiveness of the First year of Life Insurance, which will be our next topic.
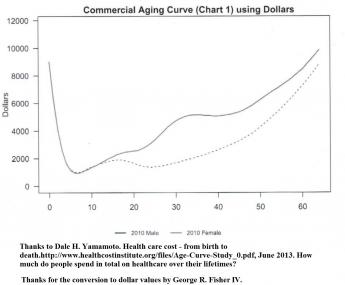
|
Children, 0-26
Everyone agrees there is a tangle about the rights and responsibilities which begin when childhood begins. We wish to avoid this issue as much as we can, but partitioning the costs of the average child requires stating some point or other, as its beginning.Keeping the practicalities of paying for it in mind, we hope no one will object if we say childhood begins, the day you are born.
We next consider the healthcare costs of children, from birth until age 25, linked with the costs of the elderly, for a reason. One of the points made in this book as an arguable alternative to the present employer-based system is to keep it within your family, rather than tax other people as a class. However, although the system now claims to begin with the first full-time employment, a newborn provokes about $18,000 of medical expense including obstetrics before that, right from the beginning, before the child can even feed him or her self. Age 26 might be a reasonable place to begin self-support, not because of tax deduction, but since that's typically the age group with the lowest health costs. Even that starting age has its problems because the parents are not much more accustomed to managing finances than the child is. The central question remains the same. Who is to supply the $18,000?
The Progressive movement started the idea of "family plans" about a century ago, but Henry J. Kaiser is credited with noticing an employer's gift of the insurance would supply two tax deductions, the employer's and the employee's, during World War II. That "reduced" the cost of health insurance by at least 50% (for the employer and employee), but it made a married employee seem more expensive than unmarried ones, made healthcare seem a free cost to the recipients and therefore boosted its cost, introduced a religious note by discouraging multiple pregnancies, and was unfair to unemployed or self-employed persons who were excluded from getting the gift. It is impossible to determine how much this new twist distorted employment and medical prices, but by suspicion the unfairness was major. It surely prompted a response, and this is one. If a big business can get tax deductions for giving away healthcare, why can't everyone else?
So it is proposed -- hold your breath -- HSAs give the equivalent of $18,000 at the death of an older relative, to a newborn's HSA at birth. The average childbearing mother has 2.1 children, which works out to one grandchild per grandparent, and helps smooth out the cost of multiple children. Because births and deaths cannot be forced to coincide, some sort of fund has to be created to make all this come out fairly, but the result should equal a zero balance between two generations. And because everyone who is alive has somehow already paid his birth cost, there is less urgency to begin this feature at the onset of the program--it becomes a feature of the transition. And, going back to the pros and cons of including Medicare premiums in the compounding, the more surplus is generated, the shorter the transition period should become. Ultimately, of course, the cost of health insurance for the mother is reduced; but the main beneficiary of the transfer is whoever is now paying for the mother's health insurance. That would sometimes be the father, sometimes the employer, and sometimes the Affordable Care insurance.
A few children are cursed with horrendous medical bills, which quite often predict lifetime disabilities. For the most part, however, childhood medical costs are pretty small. It would seem to produce an < b>ideal configuration for insurance, leading to mostly small premiums, affording a lot of protection against a fearful risk which is nevertheless relatively uncommon. However, a newborn is unable to walk, talk or feed him or her self, beyond even mentioning his or her lack of savings. Parents are now expected to pay such bills, and when they are very large it is common for grandparents to help out. So it sort of fits the common situation to group the two dependent periods of life (childhood and old age) together, as a continuous loop skirting the income-producing period of life entirely. The underlying purpose is to shift overfunded money to an underfunded time, compensating the childhood cohort for the fact that compound interest appreciates very little during childhood, but very greatly toward the end of life. This configuration fairly shouts "risk pool" but requires legislative action because it is more a metaphor than legal reality. It serves to explain to people why we have struggled to close the loop for twenty or more years because what is true for children is definitely not true for Medicare, where the main costs congregate. To meet the disparity, we chose to employ patchwork solutions for a single generation, counting on the enhanced generosity of the public for disabled children to meet the major expense. This appearance contrasts sharply with the deceptively low average cost of ordinary childhood healthcare. The only danger is for this temporary expedient to become a career.
Please note the fiscal dilemma. Even if subsidies or gifts provided a $100 nest egg to start health savings account at birth, 2.5 doublings at 7% would only create a fund of $525 by age 25. That's not nearly enough to fund healthcare for individuals at risk of auto accidents and HIV while trying to pay for college, home mortgages or the like. By contrast, $100 a year for forty years might well pay for all of Medicare while retaining leverage of eight dollars out, for one dollar in. Adding $1400 a year for 20 more years would be much better, at 80 to one. For lucky people, $8127 might work, but its safety margin is too narrow for launching a lifetime medical system. The actual plan proposed is a complicated variant of this approach. As the reader will see, there will be ample funds available for a lump sum donation, once the system has closed the loop, because just 8.5 extra doublings from the beginning of lifetimes to the end of other lifetimes, without supplementation, should silence any remaining doubts, at 256 to one leverage.
Once it gets underway, the two-generation process is very simple, requiring only a few amendments to existing legislation. Extend the age limits of catastrophic high-deductible insurance down to the date of birth, and allow the premiums to compound up to the date of death or 104, the length of a perpetuity. After that, allow surplus Health Savings Accounts of the parents or grandparents to flow over to the HSAs of the child, and allow surplus funds of grandparents and designated others to be transferred (from the date of death of one, to the date of birth of the other) via the HSAs of both. Gifts of this sort might even become a popular item in obituaries, in lieu of flowers.
Springing such a radically different proposal on an unprepared public is potentially to provoke ribald rejection, so it's gradually introduced here as a challenge to provoke alternative proposals. At the moment, I don't see what they would be. We are combining the advantages of two systems, for the young and for the old, which separately they cannot achieve, except through the socially threatened but biologically inescapable, concept of "family".
Consulting Agency for Medicare Buy-out Issues
Proceeding on the assumption Congress might authorize a system of Medicare buy-outs similar to the one outlined, some contractual obligations and procedures need to be established. Individuals need a fair opportunity to transfer payroll deductions, and later, Medicare premiums, in return for promising to re-direct payment to Health Savings Accounts to fund a buyout, and subsequently to do so. That's a single sentence, with several clauses. Essentially, since you can't move sickness to a different time, concentrate on moving revenue around to match the sickness.
As it happens, a conflicting principle emerges, that the greatest revenue comes from investing the most money, in the hands of as young an investor as can possibly be chosen. Remembering of course, that during transition some people are too old to start young. It reminds me, in reverse, of my father's observation the "best thing to happen, is to lose some money while you are young." At least, there may be time for a youngster to make up a loss, but it's still better if he also avoids losses when he is young. Making that choice favors both compound interest, and avoiding even the low health costs of the young. If the largest revenue source comes from Medicare premiums then it follows, newborn babies ought to be investing funds derived from grandparents on their deathbeds. Such twisting of original purposes probably will be motivated by knowing a dead donor will never notice. Supreme Court advocacy might argue the original purpose really was to finance Medicare painlessly, so this particular twisting results in the greatest revenue for the least complaints. The fact is, it is indeed advocated to take advantage of the greatest revenue for the least pain, but the benefit is directed to someone who was largely unanticipated. And therefore the loyal opposition may oppose. We merely display the arithmetic.
If it is agreed the two primary sources should be Medicare premiums and Medicare withholding taxes, then the greatest revenue by sizeable amounts will result from assigning the Medicare premium source to age zero to age 25, followed as before by the Medicare withholding taxes, from age 25 to 65. Gifts to the HSA, presently limited to $3400 a year to employed persons, should be accepted at any time, whether employed or not, and gift limits should be raised to encourage it. The potential is in the millions of dollars per person. If objections are raised by doing such a thing, the revenue could be substantially less. It will be interesting to see how this is dealt with.
Most likely, many individuals would get this choice during the 40-year period of payroll withholding and request a payroll change after a few years of having partially paid in some other sequence. Should any portion of an escrowed account already paid, be refunded? A similar but different situation can be anticipated after age 66 when the question will be raised whether paid premiums should be repaid, but by that time the buyout should be accomplished. Since the two payment methods are of the same total amount, forty years for payroll deduction, and twenty years for Medicare premiums, the premiums are twice the size of the deductions. For present purposes, there will be some people who recognize a bigger amount will grow at a faster rate and be a better investment, while other people either cannot afford the higher price or else cannot live long enough to collect the benefits. So, if the sixty years of paying for Medicare are switched around, there will be five different twenty-year sequences with different prices and different outcomes. Among the predicted outcomes will be better investments at higher prices, and worse investments at lower prices. Presumably, Congress does not want to get into the weeds of such details, but leaving it to the bureaucracy is the first step toward losing control. Congress needs an oversight subcommittee, but it also needs an executive body within the bureaucracy. Since there will eventually be a need for such a body, its skeleton should be started before the legislation is passed.
Each year of the transition will see somewhat smaller differences, some of which are inconsequential and some are not. If the cost and consequences of these entry points are worked out and explained, most people should have no difficulty recognizing their optimum sequence. Quotas may have to be imposed to keep the system in balance, but in general, a voluntary choice would self-select the best choice. Generally speaking, a larger deposit is most suitable for early selection and longer compound interest. If you are in your nineties, you may not care, or you may care a great deal. On the government side, it is in everybody's interest to have the transition cleared as soon as possible, with disputed choices referred to a specified court system.
Obviously, Medicare should be consulted about what it sees to be the most appropriate procedure, and in reply, Medicare will probably describe some problems with starting Social Security in the absence of Medicare premiums, as a deduction from Social Security checks. Again, a temporary transition team, with appropriate membership, should be established to iron out such issues. The number of clients involved suggests there will be numerous unanticipated administrative problems to be resolved, so Congress should not allow the basic decisions to get beyond its control.
The donation of surplus retirement funds to infants poses a similar problem, triggered by getting the revenue from Medicare buy-outs. It would seem the creation of separate escrow accounts within Medical Savings Accounts might be the simplest way to keep track of this segregation since the child would be expected to require its own HSA to receive the funds, and later to distribute them. There are likely to be a number of incompetent elderly and newborns, whose custodians would be arguing for negotiations, and more rigid uniform procedures. After initial transition problems have mostly been resolved, there surely will remain a need for a permanent consulting agency for clients and a need for a special court of appeals. This all sounds like a lot of trouble, but comparatively simple when compared with switching millions of people from one program to another, and then listening to their outcries.
This isn't as hard to understand as it sounds. We return to it later, when resolving the Obamacare transition is actually before us.
Transition Problems
Transition Issues
Sickness costs have migrated toward the end of life and will continue to migrate, as we have repeatedly mentioned. That's what makes pre-funding so attractive, but unfortunately, the sequence is reversed for a simple transition, placing the biggest costs temporarily at the head of the line to be paid first, not last. If we can't fully afford one set of beneficiaries, we certainly cannot afford two sets on top of each other. For twenty years, people would be showing up for Medicare coverage, protesting they have either already paid for it, or have no means of earning the cost of it.
Bond Issuance. At first, there seems no way to cover the transition except by a bond issue of twenty or thirty years, and then there still remains the problem of paying off the bonds. Or waiting forty years for the revenue to catch up with expenses, a proposal which is unappealing to people who have to be re-elected before the fruit ripens. But both reactions are too dismissive. Eventually, there will be an enormous fund of money building up in the accounts, and therefore plenty of money to pay off bonds. Just when that will occur is a matter of complicated mathematics, but I hope I have convinced readers it will happen.
Voluntary. Therefore, it is at least essential to make the transition voluntary and perhaps even a little unattractive for the first generation of beneficiaries who have already achieved Medicare eligibility, inducing them to shift some of the burden of transition (limited in the Medicare case to the escrowed funds) until later when the country can afford it. A quota system may even be necessary, but more probably the conservatism of old age will impel most Medicare beneficiaries to ask why they should bother to demand something they have already been given. The issue largely goes away in twenty years, unlike pay as you go, which stretches to infinity. And the funds required to begin at only half of what they originally were, before removing the expense of the last four years of life.
But on the other hand, not every elderly person has ferocious medical expenses. The trick is to figure out how many there will be at each stage of transition, figure out what proportion they represent, and phase in the cheap ones first. That calculation, which is beyond my capability without dependable ACA data, will establish the point at which it is safe to phase in the expensive residual people. Or the sort of disorders it is advisable to delay. There's a risk in this, that the scientists who discover cheap cures will, instead, be overruled by the administrators of the drug and insurance industries, who feel their charge is to produce business plans to make a profit. That is, a combination of circumstances may thwart a fixed transition plan. At this point, our only hope is to use force, negotiation, and pleas -- essentially, to delay profits in return for enhancing them later. A dull refunding plan might then suddenly transform into a skillful negotiation of conflicted self-interests. Unfortunately, we must first determine the hidden costs incurred by the Affordable Care Act.
Cutting the Problem in Half With Last-years Reinsurance. A big hurdle is the group of people who are just stepping into Medicare, and an equal hurdle is a group just entering their last four years of life. Those people will cost the bulk of transition money but have no way left to repay it after death. That's where the reinsurance to repay Medicare for the last years of life really serves a purpose, and the concept of post-mortem trust funds might have to test its viability, including any bad precedents it might set. Repayment would then be guaranteed, so there is thus likely to be less objection to removing it from transition planning. And if it is sufficiently foreseen, terminal care might already be pre-funded.
Staggered Transition.If, after we pay off both the first and last years of life, we then divide a lifetime of health financing into five twenty-year segments, it should be possible to complete the transition in twenty years. That assumes we start everything at once, placing everyone into the system simultaneously, at whatever stage the person's last birthday determines. That approach is pretty disruptive, as Lyndon Johnson discovered in 1965, but cowboy that he has just plunged ahead and eaten the costs. His method was the one we are trying to escape, which is to adopt a pay-as-you-go approach and kick the can down the road. Eventually, the borrowed interest cost builds up, and people start talking about never paying anything back. So, if a transition of even half of Medicare is too much to absorb, the transition can be further segmented, waiting for compound interest to build up in the last 4 years of life funds but holding off the number of transitions until it does.
If we do plan to start everybody's transition all at once, we must plan to pay each year as it comes along. That amounts to twenty mini-transitions every twenty years because that's how people were born. Although we start with a plan which pays for itself, it does so by diminishing the cash cost through investing in total stock market index funds. Some years you make 20%, and other years you may lose 20%, but at the very least, taxing investment funds in anticipation of a financing gap before reserves build up.
Forty-year Transition Segments.Just to remind everyone, the evolution of this process over a century could be shown in a single table, which displays phases of a single life, with the exception of dividing the 40-year working period into two 20-year segments--except for the fact we cannot be certain how the Affordable Care Act and employer-based insurance are to be handled. That uncertainty segregates the low-cost age 25 to 45 segment from the somewhat higher-cost segment from 45 to 65; balanced roughly by increased income from salary raises, promotions, etc. The cost difference between the two segments will be heightened if the cost of obstetrics is shifted from the "family" to the infant, as we suggest, and shifted a second time from employer-based years to the retirement ones when our plan finally reaches a surplus. The result is the virtual creation of two mega-segments which, combined, are roughly two segments of about forty years apiece, one low cost and the other high cost.
Twenty-Year Transition Segments.The contrasting advantage of suggesting a twenty-year transition is that each twenty-year segment has about the same cost, once the whole system reaches a steady state. That is, each segment is expected to borrow, as one compartment, the full income earned. Any shortfalls can be covered by segmenting the bond issue we mentioned. The medical cash costs will balance internally in each segment, except the first one must find the cash to prime the pump for twenty years. During that first twenty years, the stock market has to behave itself and produce at least an average return. So that's the proposal to a lender: if we encounter a normal twenty-year market, the loan is easily paid off, on time. Otherwise, the loan must extend into a second segment. Selling the HSA program voluntarily to early adopters lessens the transition impact, but stretches out its resolution. If lenders rebel at these conditions, we await their counter-proposals.
So, what we are describing can be fit into a twenty-year bond issue, but thirty years is more comfortable. It's a whopper, all right, coming to roughly a half million dollars for each of millions of people for several years paid back over perhaps thirty years. At the moment, bond interest rates are at historic lows, so the timing would probably never be easier unless some major diseases happen to find an inexpensive cure in the meantime. That's not impossible, but the longer we stretch the bond issue out, the likelier it becomes. Meanwhile, the population gets older, and expensive sickness is pushed later, too. In the meantime, we can expect a profit, from a spread between 3-4%, and the 7% we need to strive for, in the stock portfolio. This is an expensive buyout of a faulty system, but in the long run, it should prove to be a sound investment, just by itself. We financed bigger issues in each of our last few international wars, so there is a good deal of history to review and consult about, with investment bankers. And consult with the Treasury Department, which does a very credible job of funding bonds.
But the awkward fact remains, you cannot devise a comprehensive transition without knowing the true financial condition of ACA, and employer-based health insurance. Except for Medicare, so we start with eliminating the biggest hurdle, first. You might discover this data with subpoenas, but cooperation is preferable.
Reflections on Full Transition
Up this point, the reader has been exposed to a rather deadpan description of where available data seems to lead us. Experience with discussing the matter with friends at local clubs has been the members of the audience either sit in bewildered silence, or they interrupt with imagined discoveries of flaws in the reasoning. Most of the interruptions are misunderstandings, requiring a lengthy digression to explain the point to someone unfamiliar with the particular topic which upset him. Since readers cannot speak out, but often have the same points of misunderstanding, let me pre-answer some common sources of agitation:
Some Common Misreadings 1) "This is a rich man's plan, which does not focus on the poor man's problems. "No, it accepts the ground rules of Medicare to include everybody, rich or poor, of a certain age; and we follow Medicare's data, so we accept their rules. The data per average beneficiary takes Medicare's data and divides them by the number of beneficiaries. Since Medicare data has age limits, not income limits, including 46 million persons over 65, plus 9 million disabled persons under 65, the average is probably somewhat more conservative (higher) than even the average rich man would actually pay, but the benefits are universal for the age group.
2)"Where is a poor single mother going to get $100 to start a contingency fund?" You mistake the purpose. The $100 is an example, not a mandate. It saves us repeating endless calculations for every year from birth to death. It illustrates the power of compound interest, implies that things which are entirely free are not taken seriously, and provides a point for the subsidy, when a subsidy is needed.
3)"These calculations are preposterous." You may be right if I have occasionally miscalculated or miscopied some numbers. But I tried hard to avoid that. The main purpose of the effort was to point out that increased longevity (caused by medical care) has brought the far end of the curves into an area where the tail of compounding turns upward. We have long since ignored this feature, which greatly bothered the ancient Greeks who discovered it. Since the tail, except for the transition phase, of the curve stretches ahead nearly a century, we mostly haven't adjusted to the practicalities of the proposal, quite yet.
4)"Nobody can earn 7% in the stock market for extended periods of time." I looked over my own and some other accounts, and find I have averaged 6%. A recent article in the Wall Street Journal estimates that switching the stock manager to a fee-only arrangement (instead of participation in the profits) would add one percent to the average investor's final return. If we get serious and exploit computers and other efficiencies, I have no doubt another percent investment return is feasible. Naturally, the finance industry doesn't want to agree, but that's the nature of creative destruction.
5)"What's good to me, to wait nearly a century to get healthcare cheaper? The government or my agent would probably steal it, anyway." Yes, the problem of the imperfect agency is a real one, and prevention must become part of the design. But the transition might take twenty years, not a century. Medicare itself was created in 1965, and you could have raised the same objection, then. You have to start somewhere, and you have to expect mid-course corrections.
The Real Practical Issues to be Confronted. At my age, I have no desire to start a company and make a fortune, so I leave that to my grandchildren. So I might as well be frank about the matter.
This plan cannot go ahead without some Congressional amendments. Not many, but there would be sufficient to cripple the idea if it provokes opposition which has no motive except political ones. The age and employment requirements of HSA must be eliminated, and other government programs should be modified to adjust to changing life circumstances. Bare-bones catastrophic insurance should be standardized by some mechanism. If there were problems with the ACA, surely there must be flaws in catastrophic insurance companies because they are accustomed to a one-year term format, and this proposal requires a longer horizon. A huge nation-wide system requires local offices and personal advice about how to handle changing investment environments, plus issues like investing for newborns, and for divorces. A totally new approach will require a lot of explaining, and all of this requires investment.
But mainly I have strictly left the working age group (age 25-65) out of the narrative, until the full facts are known after January 2017 and we can learn whether it is to be revenue-neutral or regularly sustains a big loss. When Donald Trump gets control of the department and its books, I worry that deficits will prove to be far worse than even he thought they would be. His temptation to "expose the rascals" will be strong but must be held back for better, more strategic, political uses. One important use would be to punish efforts to stonewall the new program. The Affordable Care Act took two years to emerge with regulations, Medicare in 1965 was an administrative mess for five years -- their computers didn't work, either. So, it might be wise to start modestly, with the program of 1980 to which a few essential parts are added. Just for a taste of what's coming, read Robert Wachter's book, The Digital Doctor to learn how 30 billion dollars was recently taken from the Stimulus Package to finance the Electronic Medical Record, which eventually overwhelms just about every physician who must use it without crippling shortcuts. It often employs MUMPS, an interpreter language, largely given up as obsolete in 1985, so patching it is just about impossible.
At least we don't have to usher in 2017 with a trillion dollar bond issue, after all. Let the program be voluntary, possibly with demonstration projects in various states. The secret of its effectiveness is that savings build up early for expenses which are greatest at the far end. But in a reversed transition, the oldest people must be served first, so you just can't afford to let an unlimited number of the older, expensive ones get in at the beginning. If we must have bond issues, let's start with patching up the cracks as they appear, and keep the bond issue from suddenly looming in the trillions of dollars. The best I can foresee is a twenty-year transition, during which there may be opportunities for wounded ACA supporters to get even. So let's be nice, and not be over-eager with eliminating all of ASA with a single stroke of a pen.
But let's not be timid, either.
Exit Strategy: Medicare as the First Pearl in the HSA Necklace
Placing a termination point for Health Savings Accounts was originally occasioned by recognizing the overlap created in 1965 by Medicare for everyone. At the time, it seemed pointless to be covered by Health Savings Accounts in addition to Medicare, and there was confusion with Health Spending Accounts with their "use it or lose it" features. Pouring remaining HSA surpluses into a regular IRA retirement fund, seems in retrospect the most effective way to create some incentive to save as much as you can in the Accounts. You couldn't lose it and might well need it. To a certain degree, the size of the resulting retirement package is determined by the frugality of the individual client during his whole medical lifetime long before, but also during, the time he is on Medicare.
He would, however not be in the position of needing to do that, if he had been born earlier. The subscriber to an HSA could continue to deposit extra tax-exempt money in the roll-over IRA for his retirement, giving the appearance of laundering it. Unfortunately, he would first have to drop out of the healthcare benefits, so he would lose the laundered tax exemption for health benefits on withdrawal. You would now have to view the extended tax exemption as repairing that unintended inequity. As Medicare began to be less generous, there were increasing gaps in coverage, and there may be many more in the future.
In what follows, we extend the retirement roll-over idea to several other medical entitlements without suggesting it be required as a universal rule. The time-honored old approach was to use an insurance surplus to reduce costs by recycling its surplus, but there are other things to consider. The first would be to imagine a theoretical sharp drop in the cost of Medicare, itself. Since 80% of Medicare is now spent on five or ten diseases, the possibility of a sudden cheap cure of one of those diseases is raised. The astonishing savings in the cost of strokes and heart attacks, created by taking a daily aspirin tablet -- shows what it might be possible to imagine as happening again. Not to promise, but to imagine.
On the other hand, it is also possible to imagine less desirable priorities getting into the competition for such a financial windfall. Confronted with the issue, the average person would likely suspect such a windfall might as likely pay for aircraft carriers as Medicare deficits. But another opinion would emerge and should be the default position. The Medicare program and its members had experienced the unexpected -- and expensive -- a consequence of more protracted retirement than they planned on (five times as expensive, by one estimate). A more just assignment of such windfall would be to pay for the extra-long retirement cost it had provoked. If other emergencies seemed more pressing at the time, they could always be given priority on the money, but by default, Medicare should first pay for its own consequences. In fact, nothing of the sort occurred.
In a sense, President Obama later created the same political problem for himself with the original budget for Obamacare. He did not need to make any speeches directing attention to the diversion of Medicare money to help pay for Obamacare costs, because plenty of Republican opponents were studying the budget. And plenty of Republicans remembered Richard Nixon's advice, "Watch what I do, don't listen to what I say." Having spoken to many groups of retirees about healthcare financing, I am acutely aware that retirees are watchful for any move to strip Medicare funds for Obamacare's benefit. It's about their highest priority.
And indeed their anxiety would be heightened by discovering Medicare is already 50% subsidized by general taxation, and then unsustainably maintained by borrowing money (selling US Treasury bonds) to foreign countries like China. And still more to the point, medical costs have been and will continue to migrate from working-age people to retirement age people in the future. Just about everyone who dies right now dies at Medicare expense. Even more than that, the effect of medical science has tended to eliminate terminal medical costs for people under 65, shifting them to people who get sick when they are over 65. It can be predicted a major cause of future Medicare cost increases, compared with the cost of living, lies in this shift of disease cost to the elderly. So it's a little hard to project whether Medicare costs will go up or go down, even if the cost of illness remains the same.
Recipients will change insurance compartments. Many attempts have been made to shift Medicare costs to the non-stick working population, such as through the payroll tax deduction and hospital internal cost-shifting, but the trend continues. A more sophisticated thing for the retirees to worry about, is the instability of a system which depends for its financing on that one-third of the population who are at work -- but who are themselves becoming progressively more healthy -- to support the medical finances of the other two thirds of the population, who are sick.
Taken in summary, there exists a great political opportunity for both political parties to put a stop to this "third rail of politics" talk. And to amend the Medicare Law immediately to provide that any declines in Medicare costs be immediately transferred to Social Security, for the purpose of paying for further increases in longevity. That provision should not cost much for some time to come. But the incentive it would give to the retirees to reduce their health expenditures might be considerable. Just as the comparable position Health Savings Accounts achieved, once Medicare coverage was attained.
But its real benefit might be tested on that fateful day in the future. The day you pick up the morning newspaper and discover someone has cured cancer.
Health and Retirement Savings Accounts: to Privatize Medicare and Save Money, Too
As earlier sections outlined, Health Savings Accounts were developed by John McClaughry and me in 1981, as a bare-bones health insurance scheme for financially struggling people. The package consisted of the cheapest insurance we could imagine (a high-deductible catastrophic indemnity plan with no co-pay features), attached to what others have aptly described as a tax-sheltered Christmas Savings Fund. That's essentially what you get if you sign up, today. What was this linkage supposed to accomplish? The Account part was intended for folks who must accept a high deductible to lower the cost of health insurance, but who then struggle to assemble the deductible. A combination package thus became the cheapest healthcare coverage we knew how to devise -- the higher the deductible, the lower the premium.
As deposits build up in the account, the remaining deductible falls toward zero, but the premium of the insurance does not rise because the extra cost is excluded from the insurance part. At that point, you could easily describe it as "first-dollar coverage for a high-deductible premium." Stepping through the process should clarify for anyone, how expensive it had always been to include the deductible costs inside the insurance! It certainly compares well with so-called "Cadillac" plans, where the underlying motivation really was to include as many benefits as possible, money no object, with someone else paying for it and then writing off its cost against artificially high corporate tax rates -- which were then eliminated by the same healthcare deduction. If the government elected to subsidize our plan to provide it even more cheaply to poorer people, inter-plan subsidies could easily be arranged for seriously poor people, just as the Affordable Care Act does, by offering to transfer the same subsidy to it. Although HSA is itself absolutely the cheapest, neither it nor the Affordable Care Act is completely free of any cost, so additional features like charity must be supported by additional revenue from somewhere. Cheaper is simpler, simple is easier to understand. But cheaper doesn't mean free.
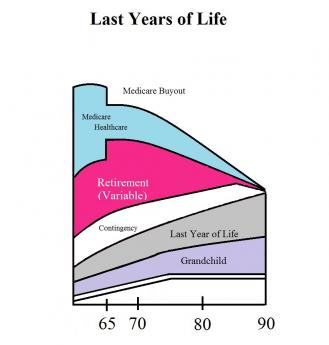
|
First-dollar coverage by any mechanism generates the danger of spending health money unwisely. That undesirable feature was neutralized by letting subscribers keep what is left over at age 65, thereby generating (and greatly increasing) retirement income. Retirement income is generally in short supply, and there may exist a future danger, that well-meaning attempts to supply generous retirements would destroy this incentive to be frugal. But right now it isn't a worry.
Other Incentives. One thing we didn't immediately verbalize was, making it a bargain entices people to save, even when they are sort of inclined to consume. We didn't think to include regular paycheck withdrawals, but that's another common savings incentive with proven effectiveness. Having loose cash does seem to create a vague itch to spend. But the Health Savings Account specifies an invitation to save for health care, using any surplus for retirement, a much more specific appeal. With that addition, it became a more attractive program, appealing to a larger segment of the population without reducing its appeal to the original ones. Our reaction was that everyone was complaining about high health costs, so the more people Health (and Retirement) Savings Accounts appealed to, the better.
The real game-changer was this: When a subscriber later acquires Medicare coverage, anything left in the fund is automatically turned into a tax-exempt retirement fund, an IRA. As enrollments in HSAs began to boom, it was realized this provision creates an unmatchable retirement fund if someone puts extra money into the account. I wish I knew whose idea originated that. So you might as well say the basic package has three parts: high-deductible health insurance, a spill-over retirement fund, and a Christmas savings fund to multiply savings with compound interest -- useful for both purposes.
It's amazing how many people think HSA has only one feature. It is a double savings vehicle for two sequential stages of life, with the tax advantages of the first stage getting it on its feet. The separation of the account from its re-insuring catastrophic health insurance, also identified the incentive to save, distinguished from a natural desire to share the risk like a hot potato. Adding compound interest adds particular attractiveness for the later stages of life because compounding takes a long time before it means much. It connects two benefits end-to-end, lengthening the time for compound interest to become meaningful for the second one, as it would not if it waited for retirement to begin. We eventually realized the deductible-funding and overlapped retirement-funding package, was the most attractive investment vehicle most ordinary folks could find. Beating it as a retirement fund alone was therefore nearly impossible.
Hence the double-strong incentive to save, sadly missing from every other form of health insurance. We strongly suggest adding this feature to Medicare, which badly needs some such incentive, although retirement is parallel to Medicare, not sequential. Experience shows this unique set of double incentives to buy HSA was effective, so a 30% reduction in premiums for total health insurance began to emerge among pioneer clients, not merely claimed in theory. The recognition of all these advantages led millions of frugal people to sign up without an expensive marketing effort. Everything seemed to fall in place. Even though mandated coverage might have speeded up acceptance, slower adoption avoided the catastrophes of taking on more than could be handled.
So that's where HSA stands today -- the best little health insurance idea available anywhere, unless someone monkeys with it. Even the remote possibility of getting very sick very often was covered by adding the feature of a top-limit to out-of-pocket costs, paid for by dipping into a small portion of savings generated by other features. Anyone who thinks of a better health insurance plan than this one is welcome to offer it. Every addition added to its complexity, but every feature added to its cost-saving.
Let's whisper a reminder to resisters: the policy is owned by the individual rather than his employer, so it doesn't suddenly stop when you change employers or move between states. To a different audience we could whisper, it could bring a second bad feature closer to an end, the business of paying for Medicare with debts which have to be borrowed from foreigners. The Account gathers interest, instead of costing interest. The best part is: it induces the subscriber to hold back from using the account, saving it for more distant requirements, which inconveniently come without warning. Paying for your old age is wonderful, but starting to save while young is vital, and more likely to work. Most plans now maintain an upper limit to the subscriber's out-of-pocket costs, protecting against a second illness with its second deductible. When we say, "That's all there is to it," we really mean that's all the advantages which have so far emerged. It's ready to be renamed HRSA, the Health (and Retirement) Savings Account.
Technical Amendments, Needed at Present.
Now, let's pick the nits, noticing how hard it gets to improve on it. If Congress could pass a few amendments, the following flaws could be more or less immediately repaired:
1. Full Tax-Deductibility. Attractive as it is, HSA still isn't as fully tax-deductible as the health insurance many employed people are given at work. The savings and retirement portions are indeed tax-sheltered, but unlike some of its competitors, the high-deductible health insurance itself stands outside the funds (as what insurance experts might call re-insurance) and isn't covered. Employers get around this difficulty for their employees by buying the insurance themselves and "giving" it to the employees. Without monkeying around with this rather dubious maneuver to maintain tight control, we propose the premiums for the Catastrophic health portion of the HRSA might instantly become tax-exempt if the Savings Account paid the premium. That would appear cheaper for the Treasury, than proposing to make the whole package deductible. Because the other parts are already tax-exempted.As an aside, it's true the subscriber to a Health Savings Account is not fully covered in his first few years, until the account builds up to the deductible. That makes a very good argument for starting the accounts while you are quite young. At first, that was a concern, but it has proved largely unnecessary to provide for it, among young healthy subscribers. Apparently, by the age hospital-level illness becomes common, the ability to meet the deductible has mostly been achieved. Nor has it proved necessary to resort to sliding-scale deductibles hidden in the slogan, "the higher the deductible, the lower the premium" -- probably because lower premiums immediately transform into more money for saving. These features might be reviewed when self-selected frugal applicants taper off since HSA enrollment has so far attracted younger enrollees. For the moment, sales incentives seem adequate; everything else may be indirectly changed by HSAs, but very little is changed directly.To permit something like that would require a one-line amendment to the HSA enabling act, but would restore fairness to the system, and bring out how much cheaper the Health Savings Account really is. Making it cheaper means more people could afford it, thus relieving the Treasury of the need to subsidize those people under the Affordable Care Act. That would compensate for some of the loss of revenue to the IRS for making the Catastrophic Health Insurance tax-exempt. Regardless of how the CBO scores this complexity, it should be remembered that poverty is not a lifelong condition for most poor people; after a temporary period of poverty, many if not most of them rise toward becoming tax-payers. Equal treatment under the law is itself a valuable asset; it could paradoxically be provided by lowering the corporate income tax since many corporations already eliminate the corporate tax with the healthcare deduction. But that's not so self-evident, and politically hard to explain. If the Congressional Budget Office would extend its dynamic scoring to include retirement taxation on the HSA's eventual compound interest (instead of limiting its horizon to ten years), it would visibly be better to choose the compromise of letting the Accounts by the reinsurance.
2. A better Cost of Living Adjustment for HSA deposit limits. There is presently an annual limit of $3400 for deposits into Health Savings Accounts, whose limits have seldom been raised very much. This new COLA should be formalized into a continuing cost-of-living adjustment which is somehow related to the current rate of inflation in the medical economy, and perhaps takes account of a potential transition to HRSA by people over age 60. These late arrivals simply do not have sufficient time to catch up within the present deposit limits, even should they possess the savings to do so.
3. Age Limits for HSAs It is a quirk of compound interest (originally noticed by Aristotle) that interest rates rise with the duration of the investment. Consequently, much or most of the revenue appears after forty years, and consequently HSAs get more valuable with advancing age. To put it another way, young people contribute more time for interest to grow, old people must contribute more money to catch up. At present, HSA age limits are set to match employment, but the HSA will inevitably focus on funding retirement. Removing all age limits might go a little too far, but would substantially increase the amount of investment income generated, at almost no extra cost to the government. It might also supplement the platform for funding childhood health costs, a problem age group which stubbornly resists improvement. It might greatly enhance revenue for older subscribers as well (by reducing their health insurance cost), the surplus from which could be used at their death for the grandchildren generation.
Young people contribute more time for interest to grow, old people must contribute more money to catch up.
Extending the age limits would potentially also serve as a platform for re-adjusting dangerous imbalances in the healthcare financing system. We are fast approaching demography of thirty years of childhood and education, followed by thirty years of working life, followed by thirty years of retirement. Substantially all of the revenue comes from the middle third, while the remaining two-thirds of the population contains most of the health costs. To some extent this is unavoidable, but the whole health financing system becomes a dangerously unbalanced transfer system for well people to subsidize sick ones. It is possible to foresee the beginnings of class warfare, based on age alone. Consequently, society would be well served to create the more stable system of subsidy between yourself as the donor and yourself as the beneficiary. The alternative is to continue the process of having one demographic group collectively subsidize two other groups of strangers who generate most of the cost. Eventually, this could induce well people to dump the burdensome sick people. I hope I am unduly concerned, but to extend the age limits for individual self-financing seems a very cheap way to begin stepping out of that particular mud puddle.
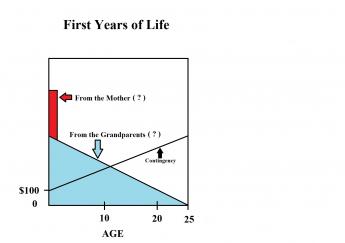
Finally, there is a conflict with inheritance laws. By extending the age limits for the funds to the legal boundary of perpetuity (one lifetime, plus 21 years), the ability to transfer funds between generations is enhanced without the perplexities of inheritance. It would be particularly useful to permit the fund to remain active until a grandparent's death, or even extend to the birth of the designated grandchild's 25th birthday. Like a trust fund, it could gather interest after the death of the owner, leaving the selection of heir to the last possible moment.
To return to the subject narrowly at hand, it is easy to see so many projects are made possible, you end up with an aggregate of goodies which eventually sink the lifeboat. Something must be chosen, something must be deferred, and the choice should be a delayed one, left to individual choice as much as possible. It can be commented in advance that retirement costs potentially dwarf sickness costs, and small single payments held at interest for long stretches have the greatest efficiency. There seems little choice but to constrain retirements to what the individual can manage independently, rather than permit retirements to absorb all the benefit of a new windfall. The theme is and should be, one step at a time.
Future Expansions.
How far these three short amendments would extend retirement solvency, is hard to predict into the future, but it would be considerable. Aside from any improvement never seeming like enough, it is almost impossible to guess the future timing of health costs, even when you can see them coming. But while the amendments might assure a comfortable future for Health and Retirement Savings Accounts, they do seem unlikely to address the full over-expectations of retirement. So the problem for many, many afternoons' deliberations, would be to expand the potential of HSAs until they become objectionable to competitive concerns. For that, I have four additional proposals which might work but inevitably collide with professions who would be quick to suggest narrower limits. Let's describe them, meanwhile waiting to assess objections from those they would discomfit:
1. A re-insurance scheme (insurance company to insurance company), called First and Last Years-of-Life Re-Insurance.This has already been described.2. Medicare should be modularized but without other basic change, so recipients need only buy pieces they need, using the invested proceeds for retirement. Obstetrical coverage immediately comes to mind. Sometime during the next fifty years, it can be predicted at least one of the five most expensive diseases (Alzheimer's, diabetes, cancer, psychosis, and Parkinsonism) will be inexpensively cured, once the initial cost increase is absorbed. We need a way to fine-tune the transfer of such medical savings into retirement income, understanding many competitors will hope to divert a windfall to themselves. Redirecting the Medicare withholding tax makes an easy way to channel the funding, as would reductions of Medicare premiums. Scientifically, Medicare is eventually destined to shrink as we find cures, but funding the resulting longevity must be given the first call on the savings.
3. The investment component of Health Savings Accounts should be dis-intermediated, partially if not completely.Ibbotson reports the stock market has produced--for a century--10%-11% long-term returns on large-cap stocks and less steadily, 4-5% on bonds, minus 3% inflation. You might not expect that judging from the returns investors often receive; investors are definitely absorbing most of the risk. The volatility is much less than most people imagine, and there is every reason to suppose Index funds of these entities should perform better with less volatility at far less cost, perhaps 0.1-0.3%. The days fast fade, when the public will continue to surrender the present level of stockmarket transfer costs and fees, which now sometimes erode investor return to as low as 1%. The fast-growing and simpler system is "passive" investing with index funds, and its goal should be an average return to the retail customer of at least 6.5% after inflation and costs. The struggle will be a fierce one, but the retail finance industry must re-examine who is at risk, and who are rewarded for taking that risk.
4. The center of medical care should migrate from medical centers toward shopping centers attached to retirement villages. Architects report it will always be cheaper to build horizontally than vertically. Since we seem destined to spend thirty years in retirement, and the principal occupation of retired people is taking care of their own medical needs -- the wrong people are doing the medical commuting. Teaching hospitals were located close to the poor, in order to use them for teaching material. But now "meds and eds" are fast becoming the principal occupations of high-rise cities. If there is ever a good time to place medical care closer to the patients, this is it.
The wrong people are doing medical commuting.And if ever there is a way to put the doctor back in charge of medical care, decentralization is the way to do it smoothly. We will always need tertiary care, but we don't need indirect overhead, skyscraper construction, or multiple layers of overcompensated administration. Even continuing-education is becoming a revenue center. No one can claim the present centralization made things cheaper, and the disadvantages of medical silos certainly call the quality issue into question. The Supreme Court failed us in the Maricopa Decision; so let's see what Congress can do with reconciling the Sherman Act with the Hippocratic Oath.
Commentary
Questions about Health Savings Accounts
Pertinent Questions: Three Current Tweaks to HSA.
1. Tax Equity. An alternative way to achieve more equitable taxation is to reduce corporate income tax rates since the tax deductions for donated employee health insurance is a way of making health benefits cheaper for the employer than wages would be. And health benefits are a reason corporations pay so little of the published corporate tax rate. Once benefits become equal they can be reduced, as eighty years have demonstrated. Tax equity first, then reduction, may be the best way to get corporate taxes reduced.
2. The transition-to-a-cheaper-system needs help, time, and more brackets for those who are already close to retirement. The private sector is inherently more flexible than the public sector in dealing with inflation, stock market volatility, and changing occupations. However, the public sector could readily be streamlined a great deal.
3. Longer durations for compound interest add flexibility and far greater returns without added cost to the government or client. In long duration, 6.5% returns rise far more rapidly than 3% inflation. This spread is an inherent feature of compound interest and can be enhanced by lengthening the duration. The historic spread between the curves at 11%/3% underlined by Professor Ibbotson is astounding -- and so costless it long seemed unachievable to shift its benefit a percent or two by John Bogle.
Pertinent Questions: Four Future Deep-Rooted Changes For Health Care, using HSA.
1. Although the whole-life insurance industry managed to accomplish it, a 90-year transition period is very difficult to plan for. As they say, life insurance is not purchased, it is sold. The last year of life proposal cuts the transition period to a manageable size, thus providing funding flexibility from the start. The first-year of life addresses the otherwise impossible task of pre-funding the year of your birth -- without help from somewhere. The present extended period of education before employment is being "addressed" by a declining birth rate, thus straining immigration policy. National defense alone argues this is an unwise policy to pursue in a present way. Luckily, the anti-perpetuity laws allow inheritance up to one life-span plus 21 years, an adequate period. The great danger in this is a revenue-starved government. Unfortunately, if public sector revenue became 100%, they would still claim to be starved, so their argument appears discredited. No strong argument is improved by exaggeration.
2. The public does not realize that Medicare is 50% subsidized, and therefore a single payer system aspires for the same treatment. We are already borrowing from the Chinese to pay for Medicare. As long as we have nation-states, this is too dangerous to continue. Although Medicare is regarded as sacrosanct, anything which cannot continue will stop, one way or another.
3. The balance between the harmful effects of having a rentier class must be balanced against the harmful effect (of overtaxing them) on the incentives of elderly rich people. So the proper balance probably varies with the state of the economy. When two-thirds of the population is to some degree rentiers, the situation must be approached with care. More retired people must be employed at home, while the finance industry must make more effort to prove its worth.
4. The business school and the law school are fast replacing the medical school as the preferred route to control medical care. The computer industry is not yet ready to join them. Controlling the hours and conditions of the workplace is not an acceptable route to control of a service industry, and in the long run, is self-defeating. The only way to gain respect from a professional is to be able to do what the professional does, only better and overall cheaper. Just how you accomplish that without going to medical school has not yet been explained, and "price fixing" is not an adequate description of its essence. The Professional Standards Review Organization (PSRO) devised by Senator Wallace Bennett of Utah comes pretty close, and although the AMA narrowly rejected it, reconsideration is recommended.
Suggested Additions.

|
| Lanhee J. Chen |
Soon after the release date of the first edition of this book, an article appeared in the Wall Street Journal by Lanhee J. Chen and James C. Capretta of Stanford University, entitled Instead of Obamacare: Giving Healthcare to the People. The authors were in general sympathy with the Health Savings Account approach and made three other suggestions with which I more-or-less agree. But they add a fourth which makes me unhappy :
1. Continuous Coverage Protection. They rightly notice many mandatory auto insurance recipients take out insurance, pay a single month's premium, during which time they obtain their drivers' license. And then no further payments are made for the insurance. The authors propose higher premiums for those who do the same thing with healthcare insurance, but presumably waive the higher cost if insurance is continued for a full year. There are many people who are suspicious of making anything mandatory, but if it's mandatory, it's unfair to allow obvious loopholes of this sort to persist.
2. Medicaid Reform. The two commenting authors are evidently aware of the unsatisfactory quality of many state Medicaid programs and propose splitting Medicaid into two parts, one for able-bodied adults and their children, and another for the disabled and elderly. Essentially, this is a rewording of high-risk pools, partially achieved by splitting Medicaid from federal plans. While this division might mesh more easily with existing workers and their families in the event of universal coverage (under a single-payer system), by itself it would not address much else.
A more useful split would be between inpatients and outpatients. That would match Medicare A and B, as well as the underlying Blue-Cross/Blue Shield organization of paperwork. Moreover, splitting helpless inpatients from ambulatory outpatients could surprisingly enable the marketplace to influence inpatient costs. Since a large number of outpatient and inpatient services are identical, it would establish a comparison framework for approximating inpatient to outpatient prices through a two-step market mechanism, which ultimately approximates market prices. For those inpatient services which have no outpatient match, a relative value system would provide a more stable way to set prices for the remainder of helpless inpatients. Doing this would close a loophole commonly employed to cost-shift inpatient costs to the outpatient area, resulting in vast confusion between two pricing systems for identical procedures. Hospital administrators would resist losing the ability to shift prices, so ultimately this is an argument about who is to dominate prices, the consumers or the providers. The "market" is a compromise between the two.
3. Medicare Reform. The main reason Medicare is often preferred to Medicaid is, it is potentially available to everyone regardless of income. But Medicare itself is 50% subsidized by the general taxpayer. No wonder Medicare doesn't need to mandate coverage. Effectively Medicare is subsidized more generously than Medicaid and thus is the main source of healthcare deficits. You might subsidize Medicaid more generously, or you could apply a 50% subsidy to a single-payer system. Either way will cost more, not less. Speaking politically, it is a question of whether you wish to offend the elderly Medicare patients or the younger indigent ones. Essentially, Congress has already chosen sides once and is unlikely to change its preference for current voters rather than potential ones. Finally, there remains one suggestion in the article which does make me uncomfortable, because of what it fails to say.
(4.) Retaining Employer Coverage. It still costs less to provide health insurance for employees, than to pay them wages and let them buy the same health insurance with what is left. Employers are therefore better off giving health insurance as a gift, even though recent inflation has held back wages more than health costs. Presumably, this anomaly would not survive tax reform, because employer-basing has turned into one big tax dodge.

|
| James C. Capretta |
But if it should survive, it presents the alternative to rectify the injustice to the other half of (small business) employees, whose employers usually cannot donate the coverage and then make it up at a spuriously higher corporate tax rate. Persisting eighty years after World War II which created the pretext, this is an unnecessary reminder of the many irregularities in the tax code. However, a one-line amendment to the HSA Law would suffice to extend the same tax exemption to outsiders, allowing other issues to remain dormant. This simple amendment would permit the premiums of a catastrophic health plan to be paid by the Health Savings Account itself, thereby extending its own tax shelter to HSA owners, at less additional commotion to the Treasury than a full exemption. The present inflation distortion should not be missed as an opportunity to restore fairness, which almost everyone now recognizes to be nothing but a lobbying plum.
Some Strategies in Reserve
1. Temporarily forget about retirement funding, just finance healthcare. A smaller sum is easier to handle. I certainly hope this is merely a transition expedient.
2. Forget about death. Just keep re-investing the remaining money until its debts are paid off, and then have it terminate. The model is a trust fund.
3. Forget about childbirth. Start a trust fund in anticipation of having at least one child, and if you don't, provide for a legal contingency. The model is a "Bride's Hope Chest", which sometimes ends in funding spinsterhood.
4. Forget about living trusts. If you anticipate or even want to anticipate, having children, start financing for it by saving money, investing it, and transferring it to its purpose without taxation of the transfer. But since we recoil at government ownership of the means of production, the model is a trust fund, not Socialism. Lawyers are puzzled about trust funds without living owners, so there must be a legislative approval of whatever we do that hasn't been done, before.
5. At present, we do all of our post-graduate medical education as "residencies" in hospitals. The consequence is twin silos with impaired communication. And then, our graduates (except surgeons) spend the rest of their lives working out of their offices. The consequence is the greatest flaw in the system comes from "hand-overs" of the patients from hospital to office practitioners who can't know what happened in the hospitals. The reverse is also true, from office to hospital, although it makes some sense to do a complete work-up when the patient is sick enough to warrant admission -- as long as you also make it available to the referring physician. The reason behind this is the desire of hospitals to maintain a monopoly silo for the transfer of information, lest they lose control of the patient himself. In Switzerland, almost all medicine is practiced in 15-25 bed "clinics", but that goes too far in the opposite direction.
|
If doctors get good at typing, they are spending too much time at it.
|
6. My suspicion is the electronic record would make more progress if it were limited to laboratory, etc. data, and deliberately excluded doctor communication in favor of tape-recorded communications or even video recordings. But not composition or typing. If doctors get good at typing, they are spending too much time at it.
In time, of course, this is a technical issue which will be solved. However, it exaggerates the time spent reading the stuff, so a major project of automatic periodic summarization is urgently needed. Presumably, that should grow out of an expanded search and retrieval system, which records whatever doctors have been interested in seeing, in similar cases, and at what stage. The basic fact is that if no doctor ever looks at it, it isn't worth including in the archive. Conversely, if doctors go after it like a dog after a bone, it should be highlighted.
Health Savings Accounts: Bare-bones Brief Summary
Health Savings Accounts
Enacted 2003. Subscribers as of Jan.1, 2015: 17 million.
Provisions: Briefly stated, any approved high-deductible indemnity health insurance plan, when attached to an approved tax-deductible saving account for the accumulation of the insurance deductible, or payment of other medical expenses. Deposits are limited to $3,400 tax-deductible annually and are not taxable on withdrawal for medical purposes. Accounts presently may not be used to pay the insurance premium. The account is exchanged for a regular IRA at the time the subscriber begins Medicare coverage. (In this sense, an overfunded account earns interest until age 66 when unused funds are taxed but exchanged for any Individual Retirement Account which may then be used for any purpose. Up until that time, there is a 20% penalty for funds used for non-medical purposes.)
Suggested technical amendments: 1. Permit the account portion to pay the premiums for the insurance portion, making the entire Health Savings Account tax exempt. 2. Improve flexibility by eliminating age and employment limits. 3. Relax the deposit limits with a COLA and switch from annual limits to lifetime limits.
Suggested regulatory changes: 1. Limit costs and charges for deposits, withdrawals, and investment income to 1%, applying all the rest to the customer's account. The main purpose was not rationing, but to block expansion from Congressional intent of before-tax funding of deductibles, health expenses, and retirements. 2. Permit subscribers the option to purchase index funds and take delivery on the certificates into defined escrow sub-accounts.
Suggested Areas for Future Expansion:
1. First/Last Years-of-Life Re-insurance. (To shorten the transition but extend the period for compounding interest, plus reduction of Retirement cost.) These four years consume 50% of medical costs. They are seldom paid by the patient himself and affect 100% of the population. The present system is largely a transfer system to these four years, paid for by people who are not themselves sick.
2. Study how the savings from future disease cures could be applied to retirement (rather than misapplied to battleships, etc) by flowing such savings into HSAs. The planning should contemplate eliminating Medicare gradually as its need disappears, a feature seldom included in the design of entitlements.
3. Study the Dis-intermediation of HSA investing. Privatization creates complicated agency problems, sometimes with excessive costs. Savings are possible from investing rather than borrowing, but the savings should reflect the risks better. The problem is how to invest several percents of GDP without using price controls.
4. Decentralize. Centralization of medical care has led to running it at great intermediary cost, unlike most businesses which become cheaper if centralized. Old people have most of the disease and do most of the medical commuting. The effective way to restore physician control is to decentralize from urban silos to suburban retirement communities. To do so gracefully requires protracted planning. Begin with the Maricopa case of the U.S. Supreme Court.
Traps, Pitfalls and Fallacies in Insurance Alternatives
As a general statement about insurance: it's a little surprising any of it works as well as it does. Most of us know the storyline of Shakespeare's Merchant of Venice . It boils down to describing how a fairly decent merchant got into big trouble by pledging his life (in effect) to fulfill the terms of his maritime insurance, which of course he never should have signed. There have always been terms of insurance no one should agree to, and no court should enforce; this was certainly one of them. However, there has long been a real need for maritime insurance, so over a period of several centuries, an honorable, profitable and workable scheme was gradually patched together. Today it is possible for a shipowner with doubtful finances to make enforceable arrangements with insurers thousands of miles away, under terms of a contract written by shrewd lawyers, to pledge substantial sums derived in turn from investors who know very little about insurance, ships or navigation, to cover ships sailed by captains over whom they have no physical control, commanding crews who are often of the worst sort. It actually seems to work, if everybody involved is careful. And the same thing is true of health insurance. A workable system can be constructed, but some schemes forget their premises.
Regulations vs. Incentives. There was once a time for example when the State Insurance commissioner was expected to protect the customer from claims against an insolvent insurance company. Insurer insolvency is a risk in buying any insurance. In recent years, however, insurance commissioners have appeared to have the main goal of protecting the customers from being overcharged. The two goals are in conflict, one pushing premiums up, the other pushing premiums down. Accounting procedures have grown arcane, dual systems of cost accounting are imposed, reserves are hidden. Many states require solvent companies to bail out an insolvent one, so an occasional slick operator escapes with a quick profit before the surviving competitors can protest. And so forth. When the state Medicaid program becomes an abuser it is difficult to trust the state's insurance commissioner to protect anybody. This resembles the environment which existed before the business community organized the non-profit Blue Cross plans. The deficiencies of service benefits and rising costs then seemed a small price to pay for a workable system. After a century, unfortunately, the employer-based system has trouble defending them.
Dread Diseases. And there once was a time when newsmedia agitated worries about certain diseases, so Dread Disease policies quickly appeared, ensuring against polio or cancer, or whatever else was in the news. When hysteria subsided, people dropped these policies, and the insurance company could legally walk away with unpaid claim reserves. As a matter of fact, much of the profitability of life insurance even today resides in expired policies of those who drop their policies; like exercise clubs for the flabby, who could never actually accommodate the number of subscribers they vigorously enlist.
|
It is not possible to separate insurance for the other stages of life until you stabilize the ACA since the employed third originates most of the revenue.
|
On the other hand, it raises a question of whether employer-based health insurance would also be dropped by good persons who get into non-medical financial difficulties -- except they mostly don't own their policies. Set aside the tax dodge and its inequity for small employers, prevention of employees dropping term insurance is still most likely the underlying purpose of businesses giving health insurance to employees. They want to make sure their employees are treated for illness before the business itself gets disrupted by absenteeism. They can't give lifetime coverage, because today most employees change employers frequently. It's important to see this motive is legitimate because it must somehow be modified without the use of brute force.
Employees who own their policies might very well drop them, so the potential value of having insured employees with improved health must be balanced against its evident unsatisfactory features. As costs rise, at some point almost any IRS agent would question the imbalance of purposes. What seems to have tipped the balance was the discovery that tax exemption without loss of control could be created by giving it to employees as a gift, where the higher tax rate for corporations actually creates even higher tax exemptions for the employer than the employee. Times and attitudes change, but the argument that volume purchasing and other features secondarily make the health insurance cheaper for the employee seems to have been persuasive. The fact that non-union employees of competitors were treated unfairly, was highly unpersuasive until job mobility significantly increased. And converting high corporation taxes into high corporate tax deductions is increasingly seen to be just a step too far.
The time increasingly moves toward corporate willingness to surrender the tax inequity, with only unions belligerently opposed. The easiest way to accomplish it is for HSAs to be able to purchase it since the rest of HSA is also tax-exempt. Employers might possibly prefer to use surrender as a bargaining chip in general tax reform legislation. At this point, it scarcely matters which approach is adopted, either giving tax exemption to everyone or denying it to everyone. In the present climate, giving it to everyone probably has the edge. The price of not extending the tax shelter to the catastrophic insurance portion of an HSA is an unnecessary price for everyone who signs up for an HSA. The cost in Treasury revenue now begins to be less of a consideration than restoring fair play to the basic economy. Revenue can be restored by other means, but regaining a general atmosphere of equity is much more difficult.
Aside from this issue, catastrophic indemnity insurance continues to be confused with dread disease insurance. Let's ensure cancer, but not indigestion would be a general idea. One supposed alternative is: Let's insure illness, regardless of cause. But our goals have become confused; we should be advocating insurance against major health costs, regardless of medical cause. When you come right down to it, the underlying reason behind all this medical investigation of claims is to prevent providers and patients from milking the insurance company. And a better way to accomplish that is to have the patient pay cash and beat subsequent risk seeking reimbursement for his payment. The relative cost of the two approaches needs to be re-studied. In particular, it would be important to seek ways to separate direct from indirect costs, since the system of burying research in indirect overhead essentially makes research and teaching into beneficiaries of reimbursement abuse. In the outpatient area, however, the experience of HSAs has been the issue is not a significant one. For helpless patients in a hospital bed, a more sensible revision of diagnosis-related payment still makes sense.
Disability Insurance Has been praised by some as an alternative to funding health insurance and amounts to concentrating funding into diseases which entail extended disability from employment. It is true the really astounding health costs have usually included a big dose of disability rehabilitation, and in fact, organized health groups have concentrated considerable attention to it. However, these efforts have largely been subsidized experiments, and they have yet to demonstrate overall cost-effectiveness, themselves. When teams of six to eight professionals devote up to two months to a stroke patient, the cost can be overpowering at any income level, and only 4% of stroke victims currently receive fibrinolytic therapy. Extending the same generosity to 96% of stroke patients would be ruinous to this approach. Important standard of care conclusions can only be reached when 80-90% are treated, at least in a few regions, followed by 80-90% rehabilitation, followed by observation of the cost-effectiveness for some time afterward. You almost don't need to do the experiment.
When the net benefit to the patient is often meager, the question is whether the rehabilitation approach must change or disappear when the current research subsidy does. Extending it to a helicopter and police rescue, we do not have even preliminary data to encourage this essential rehab approach as a cost saver, but it certainly sounds expensive within the present state of the art. The current price of ambulance service suggests this is an area of considerable abuse. At a recent medical symposium on the topic, the audience was asked how many would prefer a disabled outcome in 30%, to dying of the disease, and very few hands were raised. These investigations must be conducted before final decisions can be made, but the early results are a warning. The advanced age of most stroke victims suggests this noble effort at best will not cause much economic improvement unless the rehab becomes much less elaborate. We hope treatment advances will appear quickly, but national cost-effectiveness changes are so far, only partially encouraging.
Home Health Care is also quite expensive, but most people would prefer it to institutional care. At the moment, home health care insurance encounters its main problems from government caprice. If Medicare cannot be depended on, or if a benefit can be removed at the stroke of a bureaucrat's pen, the finances of this sort of insurance will remain precarious. The retirement village is probably a more viable approach, because most of them are located in suburbs, and could also serve the suburb as a partial substitute for hospitals, with doctors' offices, laboratories and radiology serving a dual community. They are not cheap but are probably cheaper than holding on to oversize, underused, private homes, inconveniently located for medical service. By far the greatest problem with out-of-hospital settings is the instability of rulings by insurance companies and governments. Whatever problems the teaching hospitals may have caused, they have historically been reliable in this one.
The Subsidy Issue: Crossing the Line Between Private Sector and Public Sector
Although they seem to have the same design, employer groups don't fit the ACA plan very well. You will notice in current reports of 20% boosts in the individual health insurance contracts because of the Affordable Care Act, there was scant mention of employer groups. Their rates are negotiated privately, and usually at lower rates. They usually pay a different share of subsidies, too. In fact, it can be easier to deal with a plan with no subsidy at all, than with one which requires fitting several partial pieces together. Employer groups are often further subsidized by state and federal income tax deductions, with puzzling circular dependence. Employers make young employees subsidize older ones, while the ACA emphasizes rich ones subsidizing poor ones. (Young employees are seldom richer than older ones, so there's a mismatch, somewhere.) Young employees think of buying protection against unexpected illness, while older employees think of buying necessities at what they hope is a discount.
Some employed subscribers then find they are better off switching to Medicaid, which has historically been quite substandard. Others conclude their health risks cost less than the penalties for having no insurance at all. Some genius may be able to reconcile these issues, but at some point, it seems better to start over. An important fact to remember: many poor persons are eligible for Medicaid, but haven't applied for it. That's a job the hospital social worker usually supplied in the Accident Room as they were being admitted. When it was decided to give ACA insurance to poor people, this awkwardness suddenly surfaced, in the form of implicit subscribers who were sicker than was planned for.
|
Mixing the subsidy with the service package usually causes trouble, lumping too many sick people with too few well ones.
|
Since Health Savings Accounts were begun independently of subsidies, they sometimes face the unjustified taunt they "do nothing for the poor man." If equal subsidies were distributed, the subsidy issue could become independent of the type of health care someone happens to have. It's too bad this wasn't examined from the beginning since it definitely hampers the Affordable Care Act more than it helps it. Competition paradoxically does the opposite, no matter how hard that is to accept.
|
If you want to extend the same health subsidy to the HSA as is extended to ACA, go ahead, but stop using the addition of subsidy as a reason to prefer one payment system to the other, or one proposal to another.
|
Perhaps, poverty should be treated as economists treat unemployment -- a net absence of affluence, imitating unemployment as a net absence of employment. That says it might be temporary, which is not implied by saying it's a class of people or a particular form of thinking. The Biblical description once implied both unemployment and poverty were two classes of society, quite likely permanent ones. But that was hundreds of years ago and in a foreign land. A small demonstration program in several states might clarify whether this difference of viewpoint might actually lead to an improved subsidy approach. For a long while, I thought eliminating poverty would eliminate the sense of being poor. But it doesn't. Somehow we must get over the idea that the way we were born is the way we must remain, overlooking the plain fact that just about everybody is going to live thirty years longer, and that's generally a good thing. In fact, it's hard to think of anything most people would rather spend money on, than longevity.
Epilogue, January 6, 2017
Epilogue, January 7, 2017
Understanding What We Can Afford. My advice for early Presidential action would be to convene a group of accountants. They should acquire subpoena support, fan out, and tell us where health care stands financially, reporting back in six weeks. I trust experts know how to proceed, but would start with some recently-retired medical cost accountants. They probably already have an idea how things stand, and if retired some are eager to talk. Including a few actuaries and other experts would also be helpful. In a business merger, something like this would be called "due diligence".
The nation divides into three health groups within a massive funds-transfer system.While children and retirees produce most of today's health cost, they generate too little income to pay for it. Only the employed central bracket, aged 25-65, produces more income than an expense, and they aren't very sick. (Savings by other groups don't count because their savings originate during working years.) Notice the Affordable Care Act happens to concentrate low-income sub-groups within the only age bracket which reliably produces surplus revenue, subsidizing the pre-employment and post-employment groups. Unfortunately, employer-based insurance also competes for much of this transferable revenue, by recirculating it. Consequently, it is difficult to guess how much is really available for subsidy purposes.
Both the Affordable Care Act and employer-based insurance have incentives to obscure their effects. The ACA hopes for an image of success, while employers recirculate potential tax revenue into multiple tax exemptions. So much, in fact, that few companies actually pay the high corporate tax they complain about, since taxes are a business expense, too. The public is thus unclear how much room is left to reform healthcare. The two subgroups who might know the answer are reluctant to share it.
The issue boils down to the size and elasticity of the potential surplus from working people, available to subsidize health costs of the other two-thirds of the nation. If the surplus is small, our future should be one of cost-cutting. If it's elastic, perhaps we should postpone reform until there is a greater recovery of the economy. If it's large, well, spend away. We will hear a lot of impassioned rhetoric in the next few months, but nothing will affect the decision as much as -- understanding what we can afford.
Eliminate Duplicate Coverages. Returning to Health Savings Accounts, the existing HSA is adequate to get us past insurance collapses, even if HSA only gets a few tweaks of its limits. High deductible, non-copay, with a cap on out-of-pocket costs, is the most health insurance anybody ever needs. However, if an employer or some other program already provides more generous coverage, there is absolutely no sense in adding cheaper insurance on top of it for the same coverage. Inflationary first-dollar coverage may have been a bad idea from the start. But even it becomes affordable for poor people by attachment to a tax-free Christmas Savings Fund, called a Health Savings Account. (Because you see, once the deductible builds up in that account, first-dollar coverage is effectively created, but the independent health insurance premium is unaffected. Frugal people will save it for retirement.)A final note on the net cost of adding new revenue. Astute critics will complain about (unmentioned) costs of catastrophic coverage. During the time Health is used as health insurance, of course, bare-bones insurance is necessary to create stop-loss protection because Medicare insures everybody over age 65, rich or poor. Some people are poor so there will be losses. However, when the plan expands to Medicare pre-payment, there is no loss potential during the up to sixty years it is acting as a Christmas Savings conduit for later expenses. Consequently, there is no need to pay for loss protection during this interval. Whether you treat it as an escrow or a Christmas Saving Fund, should depend on whether it is at risk. Since at that stage the subscriber is not even a member of Medicare, Medicare is at no risk. I recommend removing high-deductible health insurance from HSAs unless they pay claims. Insurance is potentially unnecessary during the first sixty years of a Medicare reform because the primary health insurances are expected to break-even (after subsidies) or are excluded. Thus, from birth to age sixty only custodial and banking functions are needed, describable as taking delivery of index certificates and storing them in a bank lockbox, but more plausibly as part of an IRA. Meanwhile, banks collect deposits and invest them, a function many banks or brokerage houses perform for a little charge, making their profit on the float. It might cost something, but not enough to change the narrative.The rest of HSA is an expandable blueprint, to be implemented as circumstances and politics permit. It could amount to a few tweaks for the cost of living, or it could march through additional medical modules added to HSA like beads on a string, as they prove or disprove successive concepts. After all, the basic concept is this is a cheaper way to accomplish the same goal. If it doesn't reduce costs, why bother with it? Almost by definition, prisoners in detention, for example, are quite different from the mentally retarded for another example, and there are a dozen other such outliers. You almost never know if they mesh until you try to mix them. The people who lose coverage by ACA repeal are mostly refugees from a crippled Medicaid program, and they were eligible all along but didn't realize it. There is absolutely no sense in merging anything unless it works. The pearls on a string design permit the addition of new programs one by one, as they become urgent. They only need to break even after subsidies.
If Medicare gets into the trouble we predict, we have outlined a plan to transition out of it. There are thirty million people in some sort of offbeat situation, right now. If longevity should extend to age 104 as some predict, I believe HSA could adjust to it; if not, it must be modified. The investment management and "disintermediation" features seem to need re-negotiation fairly soon. Once it can be decided whether to remain state regulated, a minimal federal oversight structure could be created to acknowledge interstate sales are a modern requirement. There is enough money to do many of these things, but the political latitude needs to be tested. The essence is to rearrange them and keep the savings within healthcare. There are lots of things to be done, without doing them all at once. The software industry, for example, should be able to get the electronic record into useful shape by eliminating physician notes until voice recording becomes usable, and when automatic summarization materializes. Everything worthwhile has a cost attached to it, so creating a sensible accounting design is the first big step in medical computerization, anyway. .
Typos
Blog 3632(replaced);Blog 3676 (added to end); Index
Page 2, Line 18 So, its flaws just had to
page 3. line 18 not publish but "write"
page 4, line 13 has been plunging ahead
page 4 line 38 transition to it pushes
page 5 line 4 will depend upon circumstances.
page 5, line 12 that's only part
Page 6, line 1 Privatizing Medicare?
page 11 line 3 delete the whole duplicated line
page 12 linw 28 Now (add comma) focus (Now, focus)
page 13 line 4 delete "a year"
page 13 line 11 delete "than there seems to be"
page 14 line 31 a long-term net improvement
page 26 line 2 delete "act"
page 40 line 34 delete "to"
page 41 line 2 females to much the same
page 42 line 7 defining some point or other
page 42 line 15 this book as an arguable
page 42 line 30 employer's
page 42 line 40 employee), but it made a married
page 43 line 5 but the suspected unfairness
page 43 line 25 compounding, as more surplus gets generated,
page 44 line 3 but requires legislative
page 44 line 35 birth,and the premiums
page 44 line 36 of death or 104,the length of perpetuity.
page 45 line 4 unprepared public is potentially to provoke
page 46 line 8 subsequently to do so.
page 46 line 37 it is indeed advocated
page 46 line 6 need a fair opportunity
page 47 line 5 taxes, from age 25
page 47 line 4 before by Medicare
page 47 line 20 some people who recognize that a
page 48 line 15 Medicare premiums, as a
page 48 line 18 involved suggests there
page 51 line 40 perhaps even a little
page 55 line 4 has been that the members
page 56 line 20 have to expect mid-course
page 56 line 30 but they would be sufficient to
page 57 linne 30 At least, we don't have to
page 58 line 30 deposit extra tax-exempt
page 60 line 30 achieved, once Medicare
page 61 line 35 the same healthcare deduction>
PAGE 63 LINE 15 retirement fund when someone
page 63 line 37 Medicare, not sequential
page 73 line 15 published corporate tax rate
page 74 line 10 "addressed"
Martin Feldstein Does It Again: Eliminate Tacit Tax Exemption for 70% of Workers Denied To the Rest
Headlines in the Wall Street Journal announced collapse of Congressional healthcare reform. In the same edition, a small short article buried in its depths described a possibly major step toward its reform. Martin Feldstein calmly observed, a tax exemption for healthcare insurance of 2.9% really amounts to a wage increase whose elimination might go a long way toward paying for the eighty-year mess Henry J. Kaiser had created. (In fact, it was effectively taxable income of 4%.)
It was all so simple: healthcare extended longevity, created thirty years of new retirement cost. In turn, exempting the premium for healthcare became a tax-exempt increase in wages -- for the 70% of employees getting insurance as a gift. Maybe not at first, but wages adjust to expect it during eighty years. Social Security could not cope with an extra thirty years, so SSA was going broke, while health insurance was actually the main cause of increased longevity.
But notice how unused Health Savings Accounts automatically turn into retirement accounts (IRAs) for Medicare recipients. So if you are lucky and prudent with healthcare, or if you overfund an HSA, unused healthcare money makes a reappearance in retirement funds where it belongs. If you have used up the money, you have probably been sick, and maybe won't need so much for a shortened retirement. Increasingly, expensive healthcare hits the elderly hardest, so there are many years during which compound interest overcomes inflation. At the rate things are going, retirement may become four times as expensive as Medicare, so let's consider that future.
Medicare doesn't save its withholdings, it uses "pay as you go" and spends the money on other things, like battleships. Therefore, to make any use of this windfall, it is necessary to save it, invest it, and use it for retirement. Just doing that much might redirect the other 30% of the withheld tax to its intended purpose. So the economic effect would be considerable, just by stirring around in that corner of it.
Relationships: Bankruptcy and Bond Prices
The price of borrowed money includes a provision to pay for defaults on the loan. That is, the interest rate demanded includes a default provision assessed by the banker against what he thinks is the risk of bankruptcy. Since he wouldn't make the loan if he thought the risk was high, he insures a little more accuracy by assigning a general rate of risk for the class of debtor. But what of the creditor who wouldn't suffer much, no matter what the risk of default? Or who ignores the risk of default because he sees very little? That man would have no interest in supporting loans, except to obtain an adequate rate of return; a pure investor, who has the money and is looking for a place to earn a return. If you don't give him a fair return, he will simply pass bonds by, and invest in something else. If the banker feels the risk is greater than the offered return, he too will let the opportunity pass. The consequence is for a fair price to emerge from the marketplace for bonds. The debtor may cry and protest, talking about the unfairness of it all, and telling his wife that bankers are a greedy bunch of knaves. But in a modern bank, he would merely be offered a Kleenex for his performance. There are just times when loans are expensive, and this particular debtor has encountered one. Sometimes, a disappointed debtor visits his congressman, and sometimes the law is adjusted for him to borrow at a substandard rate. James Madison felt that debtors would always outnumber bankers, so there would be a tendency for interest rates to creep upward in a voting republic. Consequently, a mixture of strategies is employed to suppress interest rates. Sometimes the government subsidizes non-market prices, sometimes the risk of default cost is buried in the overall interest rate, sometimes the bank subsidizes the cost out of more obscure profits, usually by raising the rates for wealthier clients if they are numerous. If these simple strategies go on long enough, the default occurs and its cost is assessed as taxes from the bankruptcy courts. In a modern bankruptcy, the defaulted debtor may be entirely stripped of his other assets. If that's not sufficient to cover the loss, either the banking system collapses, or the government does.
There's another big player in this game: insurance companies. Insurance companies buy lots of bonds, trying to match their interest cost with their other expenses, notably their insurance liabilities. If the insurance commissioner of the state permits it, they may even issue some bonds to cover a shortfall. In recent years, they usually buy stock equities, and if they overdo it, the stock market may get them. The crooks in this business take in the premiums in the early years, and sell the company as the aging liabilities grow older, particularly if the Insurance Commissioner is friendly. Fortunately for them, the population has added thirty years to the life expectancies of their clients, so they have not had to resort to any of these strategies as much as they originally did. Insurance companies have been very profitable, and so bond rates have developed a great deal of slack. Whether they take advantage of their opportunities is not for me to say, but it would not be surprising if bond prices, hence bankruptcy laxness, have been both profitable and slack. The two are huge pools of money, operating in largely independent markets, which can operate comfortably and separately, for long periods of time. The last two stock market crashes have been real estate collapses, and real estate is all about mortgages, banks, and interest rates. And the Federal Reserve has responded to both crashes by artificially manipulating mortgages, banks and interest rates.
36 Blogs
Paying for Medicare Transition with Trust Funds.
Since Medicare finance isn't affected by the Affordable Care Act, there's a short-term temptation to forget it. But its deficits and poor design are at the heart of the Medicare problem, and persist in its descendants. At the end of this short book, the reader will realize it covers lifetime health insurance, except it left a big hole in the middle. Obamacare can only be absorbed after we see how much of it will survive, and uncover what it really costs.
Two Central Mistakes In The Design of Medicare.
Modifying Medicare Early, Using It Later
Pay/Go Becomes Prepaid
The mistake was made in 1965, but there was little choice.
Steps in the Staircase, Extending for Decades.
Law of Perpetuities
New blog 2016-12-22 19:52:29 description
Well, What About Catastrophic Health Insurance, All by Itself?
Anticipating the Need from the Beginning
After a Long Tour of the Transfer Escrow, a Return to the Old Health Savings Account
The Arithmetic Behind Our Claims, With Commentary
The average reader can check an approximation of these assertions in his head by assuming money at 7% will double every decade. More precision can be found by using one of the compound interest calculators found on Google. But be careful, since some of them have bugs.
Imperfect Agency: HSA Administrators
Re-Arrangements and Addition of Childhood
Last Four Years of Life Reinsurance
Half of lifetime medical expenses are reimbursed by Medicare. And half of Medicare represents the cost of the last four years of someone's life.
Buying Into Medicare, Several Decades Early
Children, 0-26
Everyone agrees there is a tangle of rights and responsibilities about the beginning of childhood.
Consulting Agency for Medicare Buy-out Issues
Reflections on Full Transition
Exit Strategy: Medicare as the First Pearl in the HSA Necklace
Health and Retirement Savings Accounts: to Privatize Medicare and Save Money, Too
.
Questions about Health Savings Accounts
.
Health Savings Accounts: Bare-bones Brief Summary
.
Traps, Pitfalls and Fallacies in Insurance Alternatives
The Subsidy Issue: Crossing the Line Between Private Sector and Public Sector
Martin Feldstein Does It Again: Eliminate Tacit Tax Exemption for 70% of Workers Denied To the Rest
The Henry Kaiser tax exemption for health would pay toward Social Security, indirectly paying for retirement, which health insurance prolonged.
Relationships: Bankruptcy and Bond Prices
 Bond prices help pay for bankruptcies, but their pricing is fairly independent.
Bond prices help pay for bankruptcies, but their pricing is fairly independent.