3 Volumes
Second Edition, Greater Savings.
The book, Health Savings Account: Planning for Prosperity is here revised, making N-HSA a completed intermediate step. Whether to go faster to Retired Life is left undecided until it becomes clearer what reception earlier steps receive. There is a difficult transition ahead of any of these proposals. On the other hand, transition must be accomplished, so Congress may prefer more speculation about destination.
Surmounting Health Costs to Retire: Health (and Retirement) Savings Accounts
Consolidated Health Reform Volume
To unjumble topics
Healthcare Reform: Looking Ahead (2)
The way to make certain you have enough -- is to have too much.
Healthcare Reform: Looking Ahead (2)

|
| health care |
The Industrial Revolution crowded people together into smoky, draughty unhealthy places to live and work, and thus created ideal conditions for the spread of smallpox, tuberculosis, plague, poliomyelitis and many other infectious diseases. With better sanitation and hygiene, those diseases declined steadily for two centuries. Meanwhile, medical science developed a steady stream of expensive enhancements to health like removing an inflamed appendix, inserting pins into broken bones, utilizing CAT scans and artificial kidneys. These things each made life more comfortable and extended it a little longer, but steadily increased the cost of care. Here and there major leaps forward occurred, like the discovery of antibiotics and the prevention of arteriosclerosis, but it seldom seemed that medical care was stamping out disease, it was just making it more complicated and expensive. But if you stopping plodding forward for a moment and looked backward, the aggregate progress was astounding. Dozens of diseases either disappeared entirely or are well on the way to disappearing, like polio, smallpox, tuberculosis, syphilis, rheumatic fever, and what have you. Life expectancy for Americans at birth, which had been 47 years in 1900, was approaching 80 years in 2000. When I started as an attending physician in 1955, I was in charge of a 40-bed ward continuously full of diabetic amputees; during the last fifteen years of my practice, however, I did not attend a single diabetic amputation. At some point in this amazing medical pilgrimage I can remember realizing that for really important purposes, there were only two diseases left. Arteriosclerosis and cancer; and now arteriosclerosis mortality has declined fifty percent in ten years.
So now it is possible to have the luxury of asking: what will happen when we finally cure cancer? Oh sure, there is Alzheimers Disease, HIV/AIDS, schizophrenia and childbirth, plus an apparently endless variety of ways to produce self-inflicted conditions. Everyone will eventually die of something, so doctors will keep busy. It is not necessary to predict the end of medical care to see that some important social transformations are likely. For example, if we cure cancer around the time of financial chaos caused by the retirement of baby boomers, it is going to be hard to resist the demand that we reduce spending on medical research. Every tedious word of the impending debate on the topic could be written right now to save time because it is a very strong probability that spending on medical research will decline, once an effective cure for cancer is behind us.
Let's, however, continue our march into the future of healthcare reform. When employers became self-insured for employee health costs, they came into possession of data about what they were buying. It didn't look adequate to them to explain the sums of money they were spending, so they concluded they were being hoodwinked by hospital cost shifting, with consequences summed up as the Clinton Health Plan. Now put yourself in their shoes when the Wall Street Journal tells you cancer has been conquered. Michael De Bakey once pressured Lyndon Johnson to start a crusade against Heart Disease, Stroke, and Cancer, and now even cancer is gone. A significant number of C.E.O.s are likely at that point to decide that since Far Eastern competitors don't have this cost to contend with, perhaps it is time to declare that you have been fleeced long enough. Give the employees some money, and tell them to buy their own health insurance.
There are even some more legitimate arguments for doing so. Individually owned and selected health insurance would be portable, putting an end to "job lock", the fear of changing jobs for fear of losing health coverage in the process. Employee divorces create a different twist to job lock, and inequities jump out at you from the tangle of arguments about dual coverage for working couples. Add same-sex marriages to this issue and employers are driven to despair. Individual policies would simplify all of these issues, and open the door to life-long coverages, which we will discuss in a later section.
If medical progress makes just the right progress in the impending time interval before doomsday, it is even possible to start talking about eliminating health insurance in a practical way. If there is no threat of medical expense, why buy insurance against it? Since everybody will die of something, it is hard to envision a time without insurance. But maybe Medicare is enough. Senator Edward Kennedy (D, Massachusetts) will finally have his universal single-payer system -- by default.
What we have here are the daydreams of a corporate C.E.O., struggling to make his numbers for the next quarter, and they are pretty strong stuff. But who can doubt the power of these concepts to move the system away from an employer-based formulation?
How Do You Withdraw Money From Lifetime Health Insurance?
Four ways should be mentioned: Debit cards for outpatient care, Diagnosis pre-payment for hospital care, Transfers from escrow, and Gifts for specified purposes. The comments which follow apply to regular, old, single-year HSAs. The multi-year variety has more similarity to insurance than to retail banking and probably would favor the "cash balance" approach used to withdraw money from whole-life insurance. In the long run, that would probably lead to lower costs, but actual retail experience does produce a different culture.
Special Debit Cards, from the Health Savings Account, for Outpatient care and Insurance Deductibles. Bank debit cards are cheaper than Credit cards, because unpaid credit card payments are a loan, whereas the money is already in the bank for a debit card. It could be argued credit cards are a little safer than debit cards, because "possession is nine points of the law". Sometimes pressure has to be applied to banks or they won't accept debit cards with small balances. Somehow, the banks must be made to see that you start with a small account and only later build up to a big one. So it's probably fair, for them to insist on some proof you will remain with them. The easiest way to handle this issue is to make the first deposit of $3300, the maximum you are allowed to deposit in one year. Even better would be a family account with a $6000 deductible, which probably gets to the $10,000 threshold in less than two years. That's difficult for little children and poor people, however, so some way ought to be devised to have family accounts for children. At the moment, you just have to shop around, that's all. Unfortunately, the tendency of banks to merge into bigger entities headquartered in another city leads to powerlessness at the local level.Spending Health Savings Accounts. Spending Less. In earlier sections of this book, we have proposed everyone have an HSA, whether existing health insurance is continued or not. It's a way to have tax-exempt savings, and a particularly good vehicle for extending the Henry Kaiser tax exemption to everyone, -- if only Congress would permit spending for health insurance premiums out of the Accounts. To spend money out of an account we advise a cleaned-up DRG payment for hospital inpatients, and a simple plastic debit card for everything else. Credit cards cost twice as much like debit cards, and only banks can issue credit cards. Actual experience has shown that HSA cost 30% less than payment through conventional health insurance, primarily because they do not include "service benefits" and restore the patient to a position of negotiating individual item prices, or be fleeced if he doesn't. Not everybody enjoys haggling over prices, but 30% is just too much of a penalty to ignore.After negotiating that hurdle, you should pay your medical outpatient bills with the debit card, although we advise paying out of some other account when you can, so the balance can more quickly build up to a level where the bank allows more latitude. Remember this: the only practical difference between a Health Savings Account and an ordinary IRA, is that medical expenses are tax-exempted when paid with money proven to come from an HSA. Both debit and credit cards are tax-sheltered for deposits, and both (in normal economic times) internally generate income, un-taxed. If you can scrape together $6000, you are completely covered from Obamacare deductibles, and since co-payment plans are to be avoided, an HSA with Catastrophic Bronze plan is your present best bet. If you have a bronze plan, you probably get some money back if you file a claim form, but those rules are still in flux at this writing. The expense of filing and collecting claims forms is one of the reasons the Bronze plan is more expensive, but that's their rule. The bronze plan is thus easier to get, but harder and more expensive to use, and carries a political risk of changing rules with political motives. Another curiosity is that big banks tend to be more customer-friendly than small ones, although that may well be temporary. The tendency of traditional HSAs would be to act like banks: checking accounts with reinsurance in the background for emergencies. The multi-year approach would probably behave like insurance with occasional withdrawal privileges, very likely treating cash withdrawals as a nuisance which increases costs. Their experience is with "cash balances" which are somewhat smaller than true balances, and a preference for big-ticket hospital payments.
There are some other important things to say about outpatient vs. inpatient care, but first, it seems best to describe how inpatient care is envisioned to work in this system, before returning to the tension between one-year and multi-year approaches. Increasing ease of use might create the problem of making it a little too easy to spend money foolishly.
Payment by Diagnosis Bundles, for Inpatient care. In 1983 a law was included as a largely unnoticed section of the annual Budget Reconciliation Act, which nevertheless later proved to have a huge effect on the hospital financing arrangement. The proposal was to stop paying for Medicare inpatients on the basis of a bill for itemized services, but rather to pay a lump sum based on each patient's elaborated diagnosis. The argument was accepted that most cases of a given diagnosis were pretty much the same, so small variations soon average out. Such a casual approach to the complexity was justified by arguing any patient sick enough to be in a hospital bed, was too overwhelmed by his frightening situation to dispute what was done to him. Market mechanisms, in short, were futile is situations with such imbalances of power. Consequently, why waste money on accounting systems to arrive at prices which were actually arbitrary.
This overly simple argument prevailed in a Congress desperate about relentless cost increases. Misgivings that the hospital accounting system was a large part of its administrative information system, were brushed aside. To the extent such objections were valid, they could be addressed later. In retrospect, it can be seen the administrative and medical parts of a hospital act largely independently of each other, communicating through prices as a sort of abbreviated language. The administrative mission of bottom-line efficiency thus became even more insulated from those who saw patient satisfaction as far more important. In fact, the unresisted expedient emerged, for prices of the DRG ( diagnosis "related" groupings) to migrate toward a 2% profit margin on the bottom line, no matter how delicate the medical issues happened to be. You might suppose anyone could see a 2% profit margin was unsustainable during a 2% inflation, but normal hospital behavior is to seek uncomplaining workarounds.
The hospitals might have rebelled, or might have collapsed. Instead, they just accepted 2% for inpatients as additional administrative nonsense and set about adjusting the cost-accounting to aim for 15% profit margin on the Emergency Room, and 30% profit on outpatient services. Cost shifting of established cost accounting was difficult to achieve at first, so Emergency rooms were enlarged, and much-expanded outpatient facilities were built, requiring hospitals to purchase physician practices to keep them filled. The entire healthcare system was put under strain, and hardball became the game of the day. New lifesaving drugs were priced at $1000 per pill, less expensive institutions were merged out of existence, the office practice of medicine was in turmoil, and a year in business school could make someone a millionaire if he could appear calm in the midst of such confusion.
I tell this story to explain why, with great reluctance, I advise the management of Health Savings Accounts to base their inpatient payment system on some variation of Diagnosis Related Groups. It's a terrible system, designed for other purposes and adopted for hospital billing by Congressmen. It does protect the paying agency from being fleeced, once it gets past negotiated rebalancing of a reduced list of prices, aggregating toward a politically dictated bottom line. It chases everyone else out of attempting to understand it, with the consequence that a handful of people have brought hospitals dangerously close to quick destruction by a sudden change in the rules. Whatever it may call itself, it is a rationing system. And rationing invariably leads to shortages.
Resolving Tension Between The Two Payment Systems. Evidently, some shrewd thinking by some smart people have brought them to the ruthless conclusion that a two-class system of medical care is preferable to the way we were otherwise going. Rich people will have their way if their own health is at stake, and poor people will have their way if they exercise their votes. Both of these conclusions were correct, but they lead to Medieval monks retreating into monasteries. The cure for cancer and a few brain diseases might make monasteries unnecessary, and so would a drastic reduction in health care costs. Huge research budgets and major regimentation are big-government approaches, of willingness to accept some loss of freedom to achieve equality of outcome.
But we can't completely depend on either choice, so the remaining choice is to undermine a lot of recent culture change, by devolving back to leadership on the local level of small states and big cities. This is a small-government approach, willing to accept wider inequalities in order to find the freedom to act. Mostly using the licensing power, the competition will reappear if retirement villages and nursing homes are licensed to be hospitals. If not, nurses and pharmacists can be licensed as doctors. Some of this could become pretty brutal, and all of it leads to patchy results. But of its ability to restrain prices temporarily, there can be little doubt.
Escrow Subaccounts within HSA Accounts. Whether anything can restrain reckless spending of "found" money, is quite a different matter, however. It may be that supply and demand will balance, even if it takes generations. There is some satisfaction to be gained from watching reckless teenagers become penny-pinching millennials, but dismal reminders of improvidence will also be found in ninety-year-old millionaires marrying teen-aged blondes, further reinforced by watching the blondes run off with stable-boys. The net conclusion is that if certain portions of a Health Savings Account must be set aside for mandatory later expenses, then the money should be set aside within partitions, like an escrow account. Even that will have limits to its effectiveness, as I have noticed when trust-fund babies in my practice worked around the restraints their grandfather's lawyer took care to put in place.
Specified Gifts to be Encouraged. Only limited restraints on spending the client's own money can ever be justified, but certain types of gifts can still be better justified than others. One of them would be the special $6000 escrow fund for deductibles and caps on out-of-pocket spending. Particularly in the early transitional years, the fund's solvency may be threatened by leads and lags, where these escrow funds could save the day. Therefore, if someone accumulates large surpluses in his account by the fortuitous conjunction of events, he should be encouraged to consider donating a $6000 escrow to one of his grandchildren or other impecunious relatives. Quite often, a prudent gift to a grandchild can lighten the burdens of his parents or other members of the family. If they wish, any number of $6000 transfers to the escrow funds of others should be encouraged.
No Medicare, no Medicare Premiums. We assume no one wants to pay medical expenses twice, and will, therefore, want to drop Medicare if investment income is captured in lifetime Health Savings Accounts. Such a change of attitude might take twenty or more years, however. The major sources of revenue for Medicare at the present time fall into three categories: half are drawn from general tax revenues, a quarter come from a 6% payroll deduction among working-age people, and another quarter are premiums from retirees on Medicare. All three payments should disappear in time, but the 50% subsidy may actually block it. Therefore, the benefit available for dropping Medicare would differ in type and amount, related to the age of the individual. Eliminating the payroll deduction for a working-age person would still find him paying income taxes in part for the costs of the poor, as it would for retirees with sufficient income.
Retirees might pay no further Medicare premiums. Illnesses of the elderly make up 85% of Medicare cost, but at present only contribute a quarter of Medicare revenue. They first contribute payroll taxes without receiving benefits, and then later in life pay premiums while they get benefits, to a total contribution of 50% toward their own costs. But the prosperous ones still contribute to the sick poor through graduated income taxes. There might be some quirks of unfairness in this approach, but its rough outline can be seen from the size of aggregate contributions. At any one time during a transition, working-age and retirees would both benefit from about the same reduction of money, but the original working age people would eventually skip payments for twice as long. Invisibly, the government subsidy of 50% of Medicare costs would also disappear as beneficiaries dropped out, so the government gets its share of a windfall, in proportion to its former contributions to it. One would hope they would pay down the foreign debt with the windfall, but it is their choice. This whole system -- of one quarter, one quarter, and a half -- roughly approximates the present sources of Medicare funding and can be adjusted if inequity is discovered. For example, people over 85 might well cost more than they contribute. For the Medicare recipients as a group, however, it seems like an equitable exchange. This brings up the subject of intra- and extra-group borrowing.
Escrow and Non-escrow. When the books balance for a whole age group, the managers of a common fund shift things around without difficulty. However, the HSA concept is that each account is individually owned, so either a part of it is shifted to a common fund, or else frozen in the individual account (escrowed) until needed. It is unnecessary to go into detail about the various alternatives available, except to say that some funds must be escrowed for long-term use and other funds are available in the current year. Quite often it will be found that cash is flowing in for deposits, sufficient to take care of most of this need for shifting, but without experience in the funds' flow, it would be wise to have a contingency fund. For example, the over-85 group will need to keep most of its funds liquid for current expenses, while the group 65-75 might need to keep a larger amount frozen in their accounts for the use of the over-85s. In the early transition days, this sort of thing might be frequent.
The Poor. Since Obamacare, Medicaid and every other proposal for the poor involves subsidy, so does this one. But the investment account increasingly pays a larger share, so the cost of the subsidy is considerably reduced. HSA seemingly makes it somewhat cheaper to pay for the poor.
Why Should I Do It? Because it will save large amounts of money for both individuals and the government, without affecting or rationing health care at all. To the retiree in particular, who gets the same care but stops paying premiums for it. In a sense, gradual adoption of this idea actually welcomes initial reluctance by many people hanging back, to see how the first-adopters make out. Medicare is well-run, and therefore most people do not realize how much it is subsidized; even so, everyone likes a dollar for fifty cents, so there will be overt public resistance. When this confusion is overcome, there will still be the suspicion that government will somehow absorb most of the profit, so the government must be careful of its image, particularly at first. Much depends on allowing individuals to drop Medicare if they wish, rather than eliminating the choice, or even poisoning it with benefits reduction. Medicare now serves two distinct functions: to pay the bills and to protect the consumer from overcharging by providers. Providers must also exercise prudent restraint. To address this question is not entirely hypothetical, in view of the merciless application of hospital cost-shifting between inpatients and outpatients, occasioned in turn by DRG underpayment by diagnosis, for inpatients. A citizens watchdog commission is also prudent. The owners of Health Savings Accounts might be given a certain amount of power to elect representatives and negotiate as a group what seem to be excessive charges.
We answer this particular problem in somewhat more detail by proposing a complete substitution of the ICDA coding system by SNODO coding, within greatly revised Diagnosis Related Groupings,(if that is understandable, so far) followed by linkage of the helpless inpatient's diagnosis code, to the same or similar ones for market-exposed outpatients. (Whew!) All of which is to say that DRG has been a very effective rationing tool, but it must not persist unless it becomes generally proportional to market prices. We have had entirely enough talk of ten-dollar aspirin tablets and $900 toilet seats; we need to understand how such prices are arrived at. In the long run, however, medical providers are highly influenced by peer pressure, so again, mechanisms to achieve price transparency are what to insist on. These ideas are expanded in other sections of the book. An underlying theme is those market mechanisms will work best if something like the Professional Standards Review Organization (PSRO) is revived by self-interest among providers. Self-governance by peers should be both its theme and its reality, ultimately enforced by fear of a revival of recent government adventures into price control. Those who resist joining must be free to take their chances on prices. Under such circumstances, it would be best to have multiple competing PSROs, for those dissatisfied with one, to transfer their allegiance to another. And an appeal system, to appeal against local feuds through recourse to distant judges.
Deliberate Overfunding. Many temporary problems could be imagined, immediately simplified by collecting more money than is needed. Allowing the managers some slack eliminates the need for special insurance for epidemics, special insurance for floods and natural disasters, and the like. Listing all the potential problems would scare the wits out of everybody, but many potential problems will never arise, except the need to dispose of the extra funds. For that reason, it is important to have a legitimate alternative use for excess funds as an inducement to permit them. That might be payments for custodial care or just plain living expenses for retirement. But it must not be a surprise, or it will be wasted. Since we are about to discuss doing essentially the same thing for everybody under 65, too, any surplus from those other programs can be used to fund deficits in Medicare. But Medicare is the end of the line, so its surpluses at death have accumulated over a lifetime, not just during the retiree health program.
That outline may not be more accurate, but it displays its assumptions better. Michigan Blue Cross has calculated we calculate lifetime costs and Obamacare costs by starting with lifetime average health costs of $325,000 and subtracting Medicare. Although Medicare is reported by CMS to have average costs of $11,000 a year, for which we prefer to assume a Health Savings Account "present value" cost of $80,000 on the 65th birthday (at a 6.5% interest rate). At the same 6.5% rate, a $3300 annual deposit from age 25 to 65 (the earning years) would total $132,000 of deposits. The striking fact is, however, that Medicare alone could be pre-paid by an escrow of $150 to $350 a year, from age 26 to 65, providing it can generate 8% compounded investment income. The entire staggering cost of Medicare would hardly add any expense, within a lifecare financing system. Preliminary goals for a hypothetical average person are: To accumulate $57, 000 in the Medicare escrow fund by the age of 65, to pay off the 25-year health costs of 2.0 children per couple as a gift to them, and to pay his own relatively modest average healthcare costs from 25-45, somewhat higher costs 45-65. The Medicare goal of $57,000 is what is estimated to be what is required for a single-deposit investment fund (paid on the 65th birthday) to pay the health costs for an average person aged 65-93,(a guessed-at future average longevity), with an estimated compound investment income continuing at 8%, also guessed. Inflation is ignored, assuming revenue and expenses will inflate at the same rate. Our average consumer will have to set aside $150-350 per year from age 25 to 65, and earn 8% compounded, to do it. Different contributions at different interest rates will produce different results. We defend 8% in a later chapter.Those who disagree with the underlying assumptions should feel free to substitute their own assumptions. The interest rate of 8% is deliberately high, in order to make room for disagreements which are higher. The upper limit of life insurance ($132,000) is set to match the HSA contribution limits of 3300 times 40, becoming hypothetically the upper bound of revenue which can ever be anticipated, and from which $150-350 is escrowed for Medicare replacement. Anticipating two children per couple and full employment from 25 to 65, this revenue effectively covers one full lifetime, from cradle to grave. Childhood illnesses and elderly disabilities notwithstanding, this is all the revenue we allow ourselves in this particular example. Quite frankly, $3000 per year for age 26-65 is the weakest part of the estimation, because it is most dependent on the general state of the economy, the number of indigent immigrations we permit, and the competition of other worthy goals for the same resources.
Let us assume that an average person can start contributing to an H.S.A. at the age of 25, even though perhaps a quarter of the population at that age are burdened with college debts, etc. and cannot. We are well aware of the Pew Foundation poll that many of those under 30 are still living with their parents, and many others have college debts. The present ceiling of $3300 annual contribution is otherwise taken as the upper boundary of what is possible for the sake of example, and theoretical deficits have to be made up from whatever surplus is created by such maximums. To plunge ahead with the example, our average person sets aside $3300, starting at age 25 toward lifetime health costs. To simplify the example, he does so whether he can afford it or not, and what he can't supply himself is provided by a subsidy or a loan. Since present law prohibits spending from the H.S.A. for health insurance premiums (this should be reconsidered by Congress, by the way), an estimated premium of $300 for his own Catastrophic insurance is taken from the set-aside, and the remainder is placed in the H.S.A., paying an estimated 8% tax-free. Within this, he eventually needs to set aside a Dependent Escrow premium (remember, this example covers lifetime expenses, even though everyone has Medicare), which for twenty years (until age 45) is zero for Medicare and available for medical gifts to children. After that, it is exclusively used for Medicare, as explained in later sections.Health Savings Accounts are tax-exempt, and they can earn tax-free investment income. Except it isn't all it could be. Professor Ibbotson of Yale, the acknowledged expert in the long term results of investment classes, has regularly published data going back nearly a century. In spite of military and economic disasters of the worst sort, investment classes have remained remarkably steady throughout the past century and presumably will maintain the same relationships for some time to come. John Bogle of Philadelphia has translated that into index funds of investment classes, with negligible administrative costs. (Caution: Many index funds are sold with very high trading costs, typically in hidden charges when money is withdrawn. Be careful of your counterparty, particularly if he specifies the index fund, because he may limit it to one who gives kickbacks to him.) With this warning, there is a reasonably good chance of getting gross returns approaching 10% for investments in index funds of well-known American stocks, even though the typical HSA at present is yielding less. This investment income can grow to the point where it constitutes a fairly large part of the health revenue.
PIECES OF THE LIFETIME PIE
Instead of starting at birth and ending at death, this book reverses the process for financial reasons. For social and political purposes however, that may not be where further expanding the program can make the most difference. Let me explain. During the first two years of life, it seems likely excellent care would do the most enduring good. The same can be said of the last two years of life because they contain the highest proportion of mortal illness. But after the first two years, there are many decades before healthcare makes the same difference. The same is true of terminal care in reverse; it's preceded by decades of golf, bridge, and television. If we must concentrate expenditures, these four, bookend, years of a lifetime are where to do it most effectively.
There is also a big transition problem in alternative proposals, since voters will be of different ages, and the system must work without gaps. It will take decades to prove any of them have much effect. Concentrate in these four years, however, and changes will be both prompt and wide-spread, a politician's dream. Everybody has already been born, and for a long time to come, everybody will have a piece of his life behind him that he does not want to pay for. The time has passed when Lyndon Johnson could solve the transition problem by simply giving a gift of many years free coverage to most of the new entrants to his system. So, although it will probably spook a number of old folks just to hear the discussion, let's begin with Last Year of Life Coverage, where the data is most accurate. Two years may be a little safer. Next, for political reasons, we would jump to First Two Years of Life coverage. If it is planned to have anything permanent, these are the two minimum goals you would start with. In our wildest dreams, after we have cured just about everything, these are the two features which would remain. Both of those apply to 100% of Americans, and in one sense would be basic coverage. Other end-games are possible, like universal health insurance, or universal good health, or universally top-notch quality care for everybody. But only the year of birth and the year of death are universal and finite. Only these two would be essential to any other scheme of healthcare reform, and therefore teach us the most. If we had to retrench, these two would be the last to disappear. If any health insurance should be universal, these four years have the strongest medical arguments. Unfortunately, right now, they seem to have the least chance of political success. Therefore, it is likely that they will be voluntary and self-pay if they are adopted at all.
Footnote:That isn't quite the case however. Since third party (insurance) payers were placed in the middle of the transaction, and after electronic computers arrived, piles of individual payment data made analysis irresistible. That approach was repeatedly discredited when everyone with a computer found out that increasing the volume of useless data never improves its lack of relevance. The watchword of the 1960s became GIGO, garbage in, garbage out. Expanding the dataset with large volumes of medical data is nevertheless a dream lingering on, eventually running up against a new stone wall. It makes no economic sense to shift the clerical data-entry burden to a physician, the most expensive employee in the system. Although the Affordable Care Act mandates something close to that, it is safely predicted we will restrain the impulse when the cost is fully appreciated. Meanwhile, the utility of just applying more reasoning to aggregate data opened up the vista of a reversed health insurance system. In a sense, this book is a product of that line of thinking; more pieces of data contribute very little, but a new concept changes everything. Unfortunately, although a radical idea can be developed in six months, it may take decades to prove it had the predicted effect.The Deal Breaker
Much ink has been spilled by arguments about Obamacare, compared with almost anything else. That's a pity, because the Affordable Care Act ends up as only a variant of how it originally started, with correcting the defects of employer-based health insurance. No matter how the Obamacare dispute turns out, it fails to address the central cost problem. So, without getting into a detailed history, let's focus on what needs to be addressed, hoping it will help the present cost escalation.
If an employer gives health insurance to his employees, the insurance necessarily terminates when the employee changes jobs. The employee, in short, doesn't own his own policy. The result is "job lock" where an employee dares not change jobs for fear he might lose the renewability of the insurance he paid for, along with the associated hospitals, doctors, etc. with whom he affiliated during the course of his employment. Either that, or go through the grief of re-assembling his medical care under new insurance with new attachments he either fears or has good reason to reject. And all this, at a moment when he is applying for a new job and is necessarily reluctant to make demands.
His employer's grandparents created the problem for benevolent reasons, but the present generation of employers now finds itself blamed for its details, largely steered by his finance department exploiting tax loopholes. Discovering the tax loophole -- remembering the income tax itself was started at about the same time as Blue Cross -- it really is pretty hard to devise a system which is paid for by employers, and tax-deductible by them as a corporate business expense, while still respecting the interests of the rest of the community. Naturally, the employer resists arrangements which would either absorb costs growing out of illnesses occurring before employment ("pre-existing illnesses"), or after an employee is terminated, becoming pre-existing illnesses for the following employer. Furthermore, ever since World War I, family domination of businesses has become unusual.
While the employer community, now largely selected by head-hunters, had a century to devise a cross-generational pooling system, a satisfactory one has trouble emerging in an intensified antitrust atmosphere, involving huge expenses by employers whose stockholders regard healthcare as a minor concern. The Obama Administration was determined to take a stab at it. At first, their solution was essentially to have the government pick up the cost above a certain level (now about $7000), and the opposition Congress became equally determined to frustrate this doorway into eventual total cost control by the government. The business sponsors were also indifferent or displeased with this maneuver because they had devised ways of having the government pay most of the bills by tax deductions of a "gift" while leaving effective control in the hands of business management. And anyway, a recession was not the best time to add new cost centers.
Buried among these details was a dominant payment system based on "service benefits" instead of indemnity, or cash, benefits. Everyone understands that ten dollars is less than a thousand, but not everybody agrees a blinding migraine headache deserves less attention than a hopeless brain tumor. The indemnity system had its flaws, but over the course of a century, labor negotiations readjusted to insurance coverage focused increasingly on illness episodes, rather than on the itemized price of treatments. This was much more advanced in hospitals than doctors' offices, but it fitted specialization better than general practice. To a certain extent, this arrangement originally did make it possible for employees to choose their own doctors and hospitals, regardless of price variation. Fine points could be overlooked, but the ability to draw a line could never be surrendered to a counterparty in wage negotiations. "Service benefits" were particularly unable to migrate into a blank check for the illness, regardless of when it had been contracted. That still left high-cost outliers, particularly those extending after employment had been terminated. If the employee left his employer on bad terms, the line could still be invoked, even if it was often ignored.
Two responses ensued: The government made assurances to insurers they would stand as re-insurers to cover cost over-runs ("risk corridors"), a feature which the political opposition greeted with great suspicion. And secondly, luxury treatment was able to exploit the tax-shelter, eventually becoming sufficiently expensive to permit less reckless insurance to undercut it. Younger employees were cheaper than older ones, certain geographic locations, ethnic groups, and employer advantages became health advantages as well; a ruthless employer could injure a more generous competitor by concentrating on health costs by indirect approaches. In other words, a benevolent system imposed disadvantages on a benevolent employer, and retained customer control in the hands of employers. Over time, employers lost control of a major cost center and had to stand by, while the interests of employees and employer took different directions. Over time, employers solved their cost problem by taking a tax deduction at higher tax rates than individuals, shifting much of the cost problem to the government without losing control. The government promptly responded to accepting more of the cost by demanding more of the control. Underlying much of this evolution was the decline of the family-owned business, gradually replaced by much less benevolent stockholders and headhunter-selected managers.
Let's summarize the evolution, to state that patients will not tolerate it when decisions about what is important are made by his employer, his insurance, or his government. In turn, those entities can not tolerate a blank check. The only solution left was for the third party to set a price limit and leave other decisions to the patients and their doctors. That is, patients, doctors, and insurance companies were better off with an indemnity insurance system and should return to it. Unfortunately, the twists and turns of the process have left all three participants without much say in the matter. This is what you get when you allow lawyers to describe your employer's tax dodge, as a gift.
Lots of other things changed materially in the course of a century, and a variety of approaches might mitigate the bad things. Giving health insurance to everyone might solve matters, but it would surely cost more, and the present Obamacare controversy is already largely whether we can afford it at 16% of Gross Domestic Product. You can blame 16% on the haste of Lyndon Johnson and Wilbur Cohen, to the extent, it isn't 8%. It's that extra 8% this book is struggling to recover, the rest of the waste is often transfers, not real expenses.
Mr. Obama's abandonment of the limitation on pre-existing conditions, however, additionally undercuts a traditional expedient the insurance industry, one it suspects it cannot cope without. Insurance companies were given assurance of government support in case an alternative didn't work. That might be a separate issue. None of these, however, prevented standard care from migrating from wards to semi-private rooms, and semi-private to start to migrate toward single rooms. It's rather chilling to imagine what would happen if events continue in that direction. Expanding Medicaid to cover all poor people might facilitate this particular flaw in the present system, but falls foul of the Tenth Constitutional Amendment, which was the original basis for fifty Medicaid programs rather than one national one. And so it goes. The proposal I make is far simpler and is admittedly not a total solution to any problem except pay-as-you-go. And even pay-go existed for fifty years before 1965.
Market-Based Outpatient Costs as a Cornerstone. It is to try to approach a cash or debit-card system for paying for outpatients at market-set prices, thereby greatly reducing processing costs, while constraining insurance payment and review to the helpless inpatient -- with an improved DRG coding system, related to true costs by overlapping with the market-based outpatients. The dual nature of the Health Savings Account readily suits itself to a dual system of this sort. As far as the insurance is concerned, if cost and portability are seen as the main problems, the change with least disruption seems to get back to indemnity insurance with a high front-end deductible, which coordinates better with a second more or less invisible, reinsurance. That's such a concentrated summary it will take the rest of the book to explain its reasoning. So, let's come back to the re-insurance part in a later chapter, and concentrate on the indemnity insurance for ordinary hospital costs. Should the hospitals be consulted? Obviously, yes. Should they be given veto power? No, because they have a rather daunting conflict of interest. You can't blame hospitals for preferring a blank-check approach to any alternative which isn't a blank check for hospitals. But the nation is more or less united on the idea, we now have to be more careful with public money -- because in the long run, it's our own. High-handedness destroys this image, so they would do well to act humble.
The case for indemnity insurance also boils down to this: the premiums are collected in cash, and the providers are paid in cash. All that expensive processing in the middle is on trial as redundant, time-consuming, and ultimately ineffective in suppressing costs. The burden of proof is on it, that it can justify its own costs, let alone restrain an army of bill-collectors. Demonstration projects are welcome, stonewalling is useless. I suspect it has a minor utility for preventing fraud.Medical Reform Through Payment Reform, not Payment Reform as a Club. Affordable Care, the nation's current "healthcare reform" really concentrates on the payment mechanism for healthcare. It may nurse grander ambitions, but it directly confronts only one of many problems with healthcare delivery -- whether poor people can afford it. Much is made of the electronic medical record but its impact is mostly one of user annoyance with increased overhead. Instead of calling doctors rigid resisters, consider their point of view: The electronic record adds four hours a week to the doctor's limited time. The extra overhead cost means more employees, which means the doctor never takes a vacation. Working harder means he can quit, but he can't slow down. After six years, EMR still hasn't justified itself. And so it remains in a class with driverless cars -- it's coming, but it isn't here. The fundamental structures of hospitals and medical practice, growing out of the much older employer-based system, are pretty much unchanged. The configuration remains mainly the employer-based system.In the far future, control of payments may eventually be used as a hammer to control healthcare, but that goal has never been articulated, and the slow pace of the past six years suggests any such goal is distant, indeed. For practical purposes, the Affordable Care Act (ACA) reduces to a payment mandate -- universal health insurance for everyone regardless of cost, subsidizing those whose insurance costs exceed 8% of income (presumably, a pretty elastic number). Opponents reply: Since 87% of the people who bought insurance on a Federal Exchange did so with subsidies, the cost could seemingly bankrupt the country, at least crippling more important priorities. In general, I sympathize with both emotional responses (care for the poor but don't wreck the economy), except for one essential point. In almost every foreign health plan, the government becomes generous with trivial items and stingy with expensive ones. Plenty of cough drops, but not many chest x-rays. Or plenty of chest x-rays, but woefully few MRIs. When you see what others have done, you get a clearer idea of what we might be facing.
The deal-breaker for me is the kind of insurance selected to be mandatory. Catastrophic (high-deductible) health insurance without frills would be far more suitable, and considerably cheaper. Linking it to a tax-exempt savings fund makes it even more flexible with first-dollar coverage, and doesn't raise the cost of the insurance standing behind it by one penny. Somewhat to my surprise, cash overfunding leads to retirement income and creates the incentive for the patient to be frugal.
Its bare-boned catastrophic insurance has both a top limit and a bottom limit and uses money as an indemnity measure, not elastic definitions like "service" benefits. (Indemnity pays for your itemized bills, not your disease.) Without prior experience, new insurance entrants cannot guess at their risks, either individually or collectively. Service benefits might be considered after the long and stable experience, but for a beginning new program, they tilt the balance between patient risk and insurer risk, entirely too much in favor of patients whose real client is the elected politician. If diagnostic payments have any utility it is in detecting odd-ball charges, but it would take a lot of persuading to convince me the fraud in the system amounts to 8% of GDP.
The problem with the Affordable Care Act is not that it excludes too much, but that it scolds too much, improves too little, and never comes even close to identifying the central problem. By utilizing the principle that the higher the deductible, the lower the premium, the flexibility of catastrophic coverage could almost rest its case. By adjusting the premium, anyone might afford it; by adjusting the deductible, anything might be a covered service. But the final philosophy we would hope for is to cover no non-essentials until the last essential service has been covered. But let's settle for less. The choice of deductible threshold defines the coverage by simultaneously defining the premium, allowing both the paying public and the subsidizing public to bid in the same auction. Deficit financing is much harder to conceal if you play by indemnity rules, and is a whole lot more difficult to prevent than allowing your relatives to sit on your bed. Nothing else I know of can make a similar claim. I tend to resist anything with the word "mandatory" in it, but high-deductible indemnity health insurance offers a flexibility which might justify an exception.
The deal-breaker for me is the type of insurance made mandatory.
Of course, flexibility is only valuable if you use it. With its high deductible, catastrophic coverage excludes small-cost items. Like birth control pills, I'm sorry to have to say. High-cost automatically means expensive but relatively infrequent health issues, which in present circumstances leans toward inpatient hospital care. Defining low-cost benefits as "service" benefits usually undermine the high-deductible part of Catastrophic insurance. It converts the ACA into scarcely more than a collection of small mandatory benefits, all of which combine to defeat the purposes of a high deductible.
The higher the deductible, the lower the premium.High-Deductible Catastrophic Insurance The effect of all this seems to suggest high-cost items are the enemy, but in fact, they are the most important benefit to insure. Collecting all small benefits into Health and Retirement Savings Accounts substitutes patient choice for unlimited bureaucracy, shifting the selection burden to the subscriber, and if uncertain, his doctor. High deductibles make them turn to their doctors for advice when they are worried. That's quite different from requiring a slip of paper from a doctor whenever things are expensive.
All Right, Hippocrates. So What's the Basic Problem?

Affordable Care Act It took me a chapter to describe what went wrong with the Affordable Care Act. Five chapters to describe what should be done about it, in whole or in part. But the best final goal of it all, one which has the best chance of making medical care affordable, can be described in a few words. Until we decide where we want to go, we are unlikely to go there. and I simply can't believe that modification of health insurance is worthy of all this uproar. Health insurance executives may be forgiven for thinking so, but it is hard to imagine the rest of the nation has such priorities. Without stopping to argue that unprovable point, I offer what I believe is a self-evident, and better, goal. One paragraph more of history is needed.
AMA Medical turmoil in its present form seems to have begun in the Progressive Era, sometimes called the Gilded Age, which briefly preceded and probably had something to do with, the First World War. It certainly involved President Teddy Roosevelt, who first proposed National Health Insurance, generating considerable appeal within the American Medical Association. After a brief flirtation, the Association then changed its position and has been more or less opposed ever since. At that time, the AMA turned its attention to the so-called Flexner Report of 1914, which advocated the physical and managerial relocation of medical education into the existing Universities. Out of this grew an unexpectedly vigorous medical research environment, responsible in time for the amazing transformation of medical care which characterized the 20th Century. This transformation which in turn probably generated the idea that Medical Schools were the natural center of the profession, a suggestion which greatly annoyed the AMA, triggering an unfortunate power struggle between medical school faculty and their practicing alumni. Since this battle divided those who were paid salaries from those whose income came from patient fees, parochial teaching issues were allowed to migrate into conflicts about how all doctors should be paid. From that the two groups soon split over the payment arrangements of health insurance, which also seeped out into questions of how all "health" care employees were to be paid, especially nurses, and thus who should manage them. In short, the subject material for a restructuring of medical payment wandered around for a century, getting further and further from resolution as new voices were heard, times changed, and the new arguments had little to do with the old ones. To summarize this century of argument in a few sentences leaves everyone confused about the topic, but certainly leaves no participant in a position to criticize the others. It is even possible to claim this bickering was good for the profession, because, for all the scolding, medical care has undeniably flourished in the meantime. I only picked up the trail, joining the profession during the Second World War. I was a practicing physician for fifteen years before Medicare made its appearance. My viewpoint may be narrow, but I have been at work in Medicine before, during, and after most of the major changes in the medical care of the last seventy years.
To come to the present concluding point, I believe the American medical system actually does have its own unique plan already for the future of health care. Never mind what the rest of the world does; they never had the resources to do what comes naturally to Americans. It goes like this: We resolved without saying so, to pour tons of money, in amounts the Europeans cannot even imagine, into a medical system populated by the best students we could identify. This somewhat pampered priesthood has one main mission: eliminate the disease, and thereby eliminate the cost of disease for everyone, rich or poor, the world over. Some physicians are more idealistic than others, and there is some grumbling. But scarcely anyone dares to challenge the results, summarized by thirty years of increased life expectancy achieved in a single century. Arithmetic alone makes it impossible to repeat that performance.
Sounds pretty grandiose, doesn't it? As to costs, how much do we spend, today, on polio, tuberculosis, rheumatic heart disease, and thirty other diseases I once spent my time with? And how little will we soon be spending on Hepatitis C and HIV? A lot, at first, but in ten years, probably very little. The great killers of my medical student days, like syphilis, subacute endocarditis, heart attacks, and strokes, are declining fast, so probably no more than a quarter of what they used to be. People have their gall bladders and appendices removed, but they don't even go to the operating room to do it. Improved longevity is taken for granted. Doesn't anyone want to live an extra thirty years? Doesn't everyone want his cataracts and knees replaced? The list goes on so long it is ineffective to recite it. We got our orders, and we delivered. No other nation on earth could even dream of such a project, and yet someone still occasionally challenges me with statistics about infant mortality in Luxembourg. Our inpatient psychiatry is a disgrace, yes I will give you that. But wipe out disease, that's the way to reduce health care costs for everyone. We're going to do it, and nobody else has a prayer of a chance. It is remarkable that costs keep rising while disease keeps disappearing, but even that trend must come to an end. Inevitably, there will be a reckoning of details.

NIH, Jim Shannon It's probably fair to ask who told us to do such a thing. Everybody did, and nobody did. As much as anybody, my contemporary at the NIH, Jim Shannon exemplified this dream of the conquest of disease, and was in a position to do something about it. Maybe it was Vannevar Bush, who was the same sort of scientific evangelist. But somehow that search doesn't feel like the right one. What feels right is that the generation of Americans who conquered the armies of the world just pushed us onward to conquer a little thing like a disease. American exceptionalism did it, and right or wrong is going to get it done. It's true that I worry we will keep people on thirty-year vacations, which our grandchildren will take at the beginning of life instead of the end of it. It begins to sound as though Reverend Malthus may have been right about feeding all these people, and maybe there will be problems with employment. But that isn't our mission. We feel the nation wanted very badly for us to do what we did, and they are just going to have to whip up a generation of environmentalists, or sociologists, or banjo players -- if there are to be new directives. Passerby, go tell the Spartans: We lie here, forever obedient to their laws.

Vannevar Bush Since I am about to launch, in closing, a proposal for revising the goals of American health care, it seems appropriate to begin it by recalling a remark of one of my medical school teachers, delivered at the close of the Second World War. "The goals for medical research,' said this pathologist, "are relatively small. When we've found a cure for cancer and arteriosclerosis, we're about done." Since the current generation of students would regard anything known before 1945 as not worth knowing, and the treatment of cancer has not advanced much since the time of this prophecy, we had best be modest about what we already know. It is widely stated that fifty percent of drugs currently in use, was totally unknown only seven years ago. That may well be true and may continue to be true for centuries to come. The limits of knowledge for medical students were once defined in a study by Howard Becker called Boys in White and go as follows: First-year medical students are determined to learn it all. By sophomore year they have decided you can't possibly learn it all, so you only try to learn what is important. By Junior year even that seems impossible to learn, so you only try to learn what is going to be on the tests. Essentially what this says is that the faculty finally gets control of things by Junior year, and their selectivity defines the horizons of what students pay any attention to.
This is a strangely limited selection of topics, which is finally set straight by the training directors of postgraduate Residency programs. Having played each of these roles in my time, I feel the residency directors have it about right, but only for inpatient care. Outpatient care is now the source of nearly half of hospital revenue, and the proportion is rapidly growing. The inpatient faculty reasserts control by writing the Board Examinations, and the final mixture is defined as the present state of medical knowledge, but it remains strangely neglectful of the outpatient half of medical care (notice, I did not say health care, which has become a rapidly growing world as non physicians assert control over funding sources).
But even an assessment based on all these biases may still not be a good measure of where Society stands in its search for scientific progress. For one thing, we haven't been serious about science for very long. The first course in science, of any sort in any American university, was only offered at the time of the Civil War. Although I had already decided to enter the Medical Profession by the Second World War (eighty years later), I nevertheless chose a college major more suitable for a gentleman. English literature, now that was the thing. In a few elite colleges, it still is. A bachelor in engineering is a degree for people who invent things; a bachelor in science was for those who would discover things. But a bachelor in the Arts was a degree for someone who planned to run things. Until that witticism loses its bite, we haven't really become serious about how much we can depend on the average patient knowing what he needs to know, to assume cost-effective control of his health. Young women and mothers chatter about pediatric topics quite a lot, but for the rest of the population, the state of medical information remains what the physician priesthood understands and has the time to communicate.
In 1945, the limits of medical knowledge were thus only two: how to cure cancer, and what to do about atherosclerosis. Today, we finally discover that sleep has a lot to do with the circulation of spinal fluid through the brain, which sounds about as advanced as Harvey's discovery of the circulation of blood in 1642. This year it became possible to see that protein synthesis is like a zipper in thousands of ribosome molecules inside zillions of cells inside you, me, Eucalyptus leaves, and dinosaur bones. Since cellular chemistry is pretty much protein chemistry, the potential for drug synthesis, to say nothing of understanding cell activities, is immense. I have had a reasonable acquaintance with a couple of dozen Nobel Prize winners, and mostly I don't know what they are talking about. The point is this: right now, it is practically impossible to know how much more there is to know, and therefore what discoveries are possible in the next twenty-five to fifty years. My pathology professor was obviously pitifully ignorant in 1945 about what lay ahead, and we haven't even cured cancer yet. How long it will take for a lot of billionaires to be created after they discovered a cure for something, isn't known and isn't knowable. But God bless them all, because the money they will save us in the cost of medical care, simply staggers the mind. Who will care about the cost of health insurance, when every disease the present generation of medical students will learn about, has disappeared? On the other hand, perhaps the scientific opportunities which are uncovered will trivialize the new pharmaceuticals of only seven years ago, which are half of the drugs presently in use. As long as the music keeps playing, we will have to keep dancing and hope for the best.
Reducing Health Care Costs, by Reorganizing Them (Lifetime Health Savings Accounts)
Lifetime Insurance: Deriving National Health Costs Indirectly.
It's traditional to estimate future health costs by listing the ingredients of cost, then adding them up. How many physicians do we need? How many hospitals? What diseases will have expensive cures, which ones will disappear entirely? And so on. For a century these questions have produced a single answer: It is impossible to foresee the volume or price of ingredients, so it must be impossible to predict overall costs.
Footnote:That isn't quite the case however. Since third-party payers were placed in the middle of the transaction, and particularly after electronic computers arrived, piles of payment data made analysis irresistible. That approach was soon discredited when everyone with a computer found the increased volume of the wrong data never compensates for its lack of relevance. The watchword became GIGO, garbage in, garbage out. Expanding the dataset with large volumes of medical data is a dream lingering on, but eventually runs up against a new stone wall. It makes no sense to shift the clerical data-entry burden to a physician, the most expensive employee in the system. Although the Affordable Care Act mandates something close to that, it is safely predicted it will restrain the impulse when the cost is fully appreciated. Meanwhile, the utility of just applying more advanced mathematics to simple data opened up a vista of revising the health insurance system. In a sense, this book is a product of that sort of thinking. Its difficulty is a radical idea can be developed in six months, but it may take decades to judge if it had the predicted effect.Let's start with the final answer to the test. In the year 2000 dollars, the average American spends an average of $325,000 on health care in a lifetime. Women spend about 10% more than men. To ensure the whole lives of 340 million Americans, the cost would be trillions of dollars. That's 110,500 trillion, in fact, give or take a few trillion, or 110 or whatever is one thousand times bigger than a trillion. These mind-boggling figures were developed by Michigan Blue Cross from its own data and confirmed by several federal agencies. By the end of this book, we will have suggested it should be possible -- to cut that figure in half. It is entirely legitimate to be skeptical, since a ninety year lifetime involves a great many diseases we don't see anymore, afflicting many people who would have been readily cured with present medications except they weren't yet invented. It would involve predictions about the health costs of people who are still alive, destined to be treated with drugs we don't yet have. It is roughly estimated that fifty percent of the drugs now in use, were not available seven years ago. Since we have to go back ninety years to get the data about the childhood illnesses of our presently oldest citizens, the unreliability of looking ninety years forward from 2014 is pretty clear. But some things change slowly, so the problem is how to select.The value of these calculations is considerable, nonetheless. They give us a technique which the statistical community agrees is reasonable, which tells us lifetime insurance would require something like $300,000 per person. Future trends can be calculated, indicating whether costs are going up or down, and roughly by how much. When you consider they had to account for inflation, you begin to appreciate the achievement. A penny in 1913 money is worth a dollar today, just for illustration. Naturally, we then assume a dollar today will be worth 100 dollars, a century from now. Regardless of numbers games, we have an accepted tool to estimate the general magnitude of health costs, and by how much they will likely change. It's useful, even if its answers are appalling.
Indeed, at first, the health insurance industry skipped the computer details and invented "Risk Adjustment", essentially just basing next year's premium on last year's results. If future medical care changes direction drastically, its payment system might be forced to change. But if health care doesn't change much, the payment system won't need to predict the future. That reasoning reflected the insurance industry's own history, where the marketing department eventually asserted dominance over the actuaries, by declaring it was more important to predict usefully, than with precision. With increasing longevity, all life insurance has to be like that.
The approach has its limits. Insurance did underestimate how much the payment system could warp the medical one over long periods because it gradually misjudged who its customers were. Payment methodology was relentless in affecting its true customers, who were businessmen in the human relations departments of large corporations. Looking back over an expedient system designed for short-term goals, a shocking realization dawns: most current "reform" thinking is about how to twist the medical system to fit some unrelated budget. Even more shocking is that the business customers discovered how modified tax laws could let them buy health insurance with a sixty-cent business dollar. When passed to the employees, another 15 or 20 cents could be clipped off.
Gradually we reach the point of rebellion; if it is legitimate for insurance executives to tell physicians how to practice medicine, it must be equally legitimate for physicians to re-design the payment system. So let's have a go at it.
Footnote: In the thirty years since I wrote The Hospital That Ate Chicago about medical costs, the newspapers report physician reimbursement has progressively diminished from 19%, to 7% of total "healthcare" costs, so perhaps now it's legitimate for some other professions to answer a few cost questions, too.As patient readers will gradually see, considerable extra money is already in the financial system, leaving difficult problems of how to get it out and spread it around. This isn't snake oil or a mirage. The beneficiaries would scarcely see any difference in medical care if Health Savings Accounts fulfilled their promise. But frankly, the insurance providers would have to make some wrenching changes. Since millions make their living from the present system, it is undoubtedly harder to design a new system which would please them.Medical care now costs 18% of Gross Domestic Product (GDP) and 18% is pretty surely crowding out other things we might prefer to buy. In a sense, the political beauty of the premium-investment proposal we are about to unfold lies in its primary aim of only cutting net costs by adding new revenue.
Lifetime Health Insurance: General Idea Behind the Proposal.
Let's get more specific than GDP, which is a pretty vague concept. A new primary goal of the Lifetime Health Savings Account proposal is to collect interest on idle insurance premiums, as has been done for decades whenever whole-life insurance replaces one-year "term" life insurance. If the recovered money flows to the management, it increases profits. If it goes to lower prices, the recovered money flows to the consumer. Since this tension always exists between the two counterparties, the final direction of funds-flow begins with subtle differences in the whole design of the insurance, made right at the beginning of the program.
The longer we wait to make drastic changes, the more difficult they become, and more proof of benefit will be demanded. In the proposed case of switching health insurance from term insurance to whole-life, almost a century of health insurance development is threatened. But remember, the past fifty years have seen plenty of dissatisfaction come to the surface, only to be dashed by a (generally correct) opinion that the gain was not worth the pain; the old system was working better than the proposed one. So this time, let's start in advance with establishing a monitor center where our control data is extensive -- the cost of terminal illness in the last year of life. It happens that every American has Medicare, and every American must some day die. It also happens that nearly everybody who dies does so as a Medicare recipient. Not quite, but in a population of 350 million people, it's close enough for information needs. Conversely, in a population this large, enough people of younger ages will also die; so we could still extrapolate what difference our proposals are making to costs, for the beneficiary to have attained almost any age. At least then, the public could base its opinion on what is currently happening, and actually happening, instead of having to rely on the anguished pronouncements of political candidates.
Footnote: An experience forty years ago makes me quite serious about this monitoring issue. While I was on another mission, I discovered that Medicare and Social Security are on the same campus in Baltimore, with their computers a hundred yards apart. So I proposed to the chief statistician that the Medicare computers contained the date and coded diagnosis of every Medicare recipient who had, let's say, a particular operation for particular cancer. Meanwhile, the Social Security computer contains the date of everybody's death, with the Social Security number linking the two data sets. So, why not shuffle one data set against the other, and produce a running report of how long people are living, on average, after receiving a particular treatment or operation. He merely smiled at the suggestion, and I correctly surmised he had no intention of following up on it. This time, I resolved to write a book about it, and see if that has more effect.
SOME BASIC QUESTIONS
No matter what payment system we use, the accounting system has to be clear on a few facts. For example, who produces revenue, who gets subsidized? At least in the healthcare system, it is unwise to assume that everyone pays for what he spends. Even if he does, he may well pay at one age and receive subsidies at other ages.
Answering the revenue question starts out pretty easy, but quickly gets harder. Children under roughly age 25 are subsidized by their parents, and retirees over 65 are living on their pensions and savings. Working people, roughly between the age of 25 and 65, are paying for the entire medical system, directly or indirectly, even though the money comes from the employer, who controls the terms through health insurance family plans. Legally speaking, parents are making an untaxed gift to their children when they pay for the child's healthcare bills. But it often gets further muddled by divorce and orphaning, and divorce at least is getting pretty common. For our purposes here, it is unnecessary to get into biological and legal complexities, to make a broad statement: the whole medical system is in some way supported by people with a paycheck, who are therefore aged 25 to 65. That's the healthiest component of society, so it can be increasingly unstable to base healthcare costs on family values, in a divorce-prone society, further clouded by payment of insurance by employers. Because of the tax laws, employers intrude their wishes, and may sometimes act as pawns for labor unions. But even with all this intrusion, society seems to feel the parent or parents are the best overseers of the kind of healthcare to use for all three living generations, even though effective employer and government control is perilously close to the surface. To some extent, this may reflect the fact that every sick person could become dependent on the assistance of others, and to that extent needs their consent. An employer-based health insurance system may not be the best, so the looser the family control, the more unstable employer-basing may become. Nevertheless, it is also reasonably accurate to say the upper limit of healthy revenue is ultimately traceable to people 25 to 65 and is probably going to remain that way.
Footnote: For children, medical costs can usually be traced to some sort of gift or loan from the pool of working people. And in a general sense, the revenue which pays for Medicare beneficiaries is also indirectly derived from the pool of working people, in this case, themselves at a younger age. In the case of divorce, should the new father or the actual father be assigned these costs? It might simplify things if childhood costs were assigned to the mother. This is the sort of issue we assign to judges in the Orphan's Court, but there is an even more perplexing issue: what do we do with the costs of a pregnancy, share it one way, two ways, or three? If there is a reimbursement, who should get it? Is that a cost to the child, leading to a debt to the mother, or is pregnancy a cost to the mother, unshared by the child? It was not so long ago that all pregnancy costs would have been legally assigned to the father. From the way things are going, it looks as though the insurance ought to regard pregnancy costs as a cost of the child, with a loan or gift coming from one or both natural parents. But in reality, the legislature or the Congress will make the best decision it can, and tell the insurance company what they decided. In considering it, the Congress or Legislature might remember that insurance companies have generally preferred to use family-plan insurance, reimbursing whoever paid for the family insurance at the workplace; and thus it gets back to the employer, even though that is not a socially useful outcome.Since we confess we are here trying to demonstrate how universal lifetime Health Savings Accounts might support the whole system, let's skip over the sensitive issues and temporarily agree to impose the revenue limits of the maximum HSA deposits permitted under present law. Anyone 25 to 65 are permitted to contribute $3300 a year to a Health Savings Account. They are also permitted not to contribute that much or even anything but suppose for present purposes that everybody did. Ignoring any periods of illness or hardship, the average person is therefore permitted to contribute a maximum of $132,000 in a lifetime. Suppose for further example sake, there is no other source of medical revenue. Would that amount of money suffice to carry the entire nation's health costs, from cradle to grave? To that, the astounding but gratifying answer is a qualified Yes. So with that mildly reassuring news, let's look at the issues related to selecting a new HSA account.
Tax Exemption First of all, every bit of HSA deposits, both contributions, and compound income. is tax-exempt to the individual owner. That immediately makes it possible for anyone to claim the discriminatory tax exemption for health costs which Henry Kaiser devised for employees of profitable corporations. True, unless it is contributed by an employer, employer deductions are still omitted, although that is a separate issue. Big solvent business employers can take a 60% corporate tax deduction in addition to what the rest of us non-employees have been denied for seventy years, by purchasing HSAs for employees. If the employer is already struggling to meet the payroll, of course, he won't do it. Extending this deduction to HSAs makes employers more likely to offer them, although the present confused state of the employer mandate under the ACA makes it uncertain. To a certain extent, it continues to be unfair to confer such a huge tax advantage to a corporation based on the number of employees it has, although even this feature can be overlooked during periods of high unemployment.
A related mathematical issue is that a deposit when you are young is much more valuable than the same deposit later. Since young people are relatively healthy, while older ones are relatively sick, a deposit by a young person has many decades to grow before it is used for health care. True, young people have colleges and cars and houses to compete for their savings but just listen to this: If it were allowed by the fund managers, you could pay for a 90-year lifetime with a deposit of less than $100 at birth. The contrast is so staggering, that even raging hormones cannot compete with it in any rational analysis. Therefore, pay for administration and trivial medical expenses from some other account (in order to build this tax-sheltered one up), whenever you can do so without running up high-interest charges. By the same reasoning, discounted tax-exempt bonds might lock it up until an investment manager would charge reasonable fees to manage it as a fair-sized HSA. But let's not exaggerate. The main financial differences between an HSA and an IRA, are that an HSA is tax-exempt when you withdraw it for health purposes, whereas the IRA has a top limit of $6000 (for persons over age 50, $5000 below that age), not $3300, for annual contributions. The big obstacle is that IRA contributions are limited by the amount of money paid by an employer in that year, something a newborn obviously cannot match. Therefore:
(Proposal 7a) Waive the limit to annual HSA contributions for underaged subscribers, for single-premium contributions of less than a thousand dollars. While resistance to this provision might focus on class distinctions, the subsequent benefit to Medicare and/or Medicaid might ultimately be so large as to overcome it.Portable, without Job-lock. No matter where you move, or where you work, this fund moves with you. Or leave it where it is, and communicate by mail.Individually owned and selected. If you don't like one advisor or his results, choose another.
Investment Control. Here, we advise caution. If you surrender control of investments, there is some danger the broker could select an investment that gives him a kickback. Although they should be, stockbrokers are not fiduciaries. A common overcharge is an excessive commission for liquidating withdrawals, which ought to be no more than $7.50 per trade. Your goal should be to get a 10% annual return, safely, before making withdrawals to pay medical expenses, which will be discussed separately. (Unless you control fees, or deal with a fiduciary, you will be lucky to get 1%) Even during an economic recession with negligible interest rates common stock total return is 5%, and a recession is an especially good time to buy stock and hold it, where 30-50% becomes conceivable. In a tax-exempt fund, ignore dividends. Buy and hold, is the thing, with no commissions above $10 a trade (either buy or especially on sale), highly diversified for safety, index funds of common stock. Either hold back a little cash for medical issues or pay small medical bills with other funds. At least until you are sixty, try not to spend HSA money unless you have no other source of funds.No advice is absolute, but the reasoning behind this little homily appears in other sections of the book.
(Proposal 7b) Limit eligible investment agents who handle HSAs to legally defined fiduciaries. Needless to say, the brokerage industry will oppose this, and should be asked if they can suggest alternatives.Pooling of funds. Pooling is what you only partially get with the present H.S.A as provided by present law. The law requires that an H.S.A. be accompanied by a high-deductible or "catastrophic" health insurance, which is expected to pool the experience of subscribers. But really suitable low-cost high-deductible policies are not provided by Obamacare. For cost comparisons, we initially pretend that you do not have Catastrophic re-insurance, although in real life and for the present, the best available alternative is the Bronze plan. For outpatient expenses, you are expected to pay out of your own funds, or else draw on the H.S.A. to cover them. When the law was written, the big expenses were hospital expenses, but the prepayment system enacted in 1983 limited their profitability, so hospitals have tended to shift from inpatient toward outpatient care where profits are more unconstrained. There was a time when fixing hernias and removing gall bladders as an outpatient was unheard of, but that has changed, so a pooling system for outpatient costs would be a desirable addition. There might be plenty of money in this approach which could be pooled, but a comfortable average will still be disrupted by an occasional high-cost outlier. For example, major auto accidents might run up a very high accident room cost which would not be covered, even though the average was well in surplus. A credit card would cover such eventualities, but their interest rates are high, and it might be better if investment houses provided loan funds for this purpose at a lower cost. If you must borrow, liquidate the loan at the earliest possible moment.Compound Investment Income. Here, we have the heart of the whole arrangement. It's not a bonus, it is the source of the new revenue to pay for burdensome health care expenses. Call it the Ben Franklin approach, that allowed him to retire at the age of 41 and live comfortably for another forty years. John Bogle's discovery of buy-and-hold index fund investing is safe and effortless. It makes it unnecessary to rely on a high-commission stock picker to achieve first-class results. So trust, but verify. If you are prudent, a cash deposit of $132,000 spread over 40 years, can pay for $325,000 of lifetime health care, the present national average. That's not exactly free, but it represents an average saving of $192,000, multiplied by 350 million people, which seems to mean $68 trillion in health revenue released for medical use. These back-of-the-envelope calculations are so dizzying that, pick all the nits you please, and the same conclusion would emerge. We'll return to that after going into more description of how the proposal should work.
Caution About Averaging. Remember, it does you no good at all to have $10 in your account and receive a bill for a $1000. That is just as true if the national average of HSAs contains $50,000, which unfortunately isn't yours. Money to pay your bill is in the system, but you can't get at it. The first thing to point out is that the national curve of health accounts shows most expensive illness takes place after the age of 60, when chronic diseases and terminal disease makes an appearance, and where funds in HSAs ought to be ample. Therefore, you are cautioned to pay medical bills from any source of money you have, in order to avoid depletion of the HSA later in life, when it really ought to have money to spare. And within reason, even borrowing (short-term, and at low-interest rates) is usually better than depleting the account for diseases that won't kill you soon. Since most high medical bills are caused by hospital care, the catastrophic insurance requirement was added. Ordinarily, that feature has been fortuitous, but the migration to outpatient surgery caused by DRG payment is threatening, and the inflation of normal outpatient prices, as well as monopoly new-drug pricing, threaten to upset the payment system before it can adjust. Short-term loans from a premium pool, or else a new layer of semi-catastrophic insurance inserted between the two existing classes appear to be a coming necessity. In the meantime, short-term borrowing at what we hope are bearable rates, seems to be the only available expedient.
SOME BRIEF EXAMPLES, EXPLAINING LIFETIME HSAs .
Obamacare does not include Medicare recipients. However, it is a familiar topic, and its data are fairly accurately available in a unified form. So future Obamacare costs are readily understood by subtraction of Medicare costs from lifetime totals, and future changes can be more readily integrated. The average lifetime medical costs are roughly $325,000, as calculated by Michigan Blue Cross, who devised a system for adjusting costs to the year 2000. The results have been verified by several Federal agencies, although the method includes diseases and treatment which we no longer see, and adjusts for inflation to a degree that is startling. Medicare data are more precise but have the same trouble adjusting for the changes of half a century. By this method, we get the approximation of $209,000 for Medicare. By subtraction, we get the data approximating what Obamacare would cover, slightly confounded by including the small costs of children. That is estimated by subtraction to be $116,000. The revenue to pay for these costs is assumed to come entirely from the working years of 25 to 65. In the examples which follow, the Health Savings Account data are the maximum annual allowable ($3350) multiplied by 40, representing the working years, so they represent the maximum contribution, adjusted for compound investment income at 6.5%, and paying for lifetime costs. The aggregate cash contribution is thus $134,000, which without being disturbed by withdrawals, at 6.5% would hypothetically grow to the astonishing figure of $3.2 million by age 93. A more conservative interest rate of 4% would reach nearly a million dollars. The conclusion immediately jumps out that there is plenty of money in the approach, with the main problem remaining, somehow to devise a way to get it out in adequate amounts when the average is adequate but an occasional outlier cost is extreme. In these examples, inflation in revenue is assumed to be equal to inflation in costs, an assumption which is admittedly arguable.HSA and ACA BRONZE PLAN: A FIRST LOOK. Although a catastrophic high-deductible plan must be attached to a Health Savings Account, and the Affordable Care Act provides a catastrophic category, those plans are not available after age 30 except in hardship cases. Therefore, at the present writing, it is necessary to select the plan with the highest deductible and the lowest premium, which happens to be the Bronze plan. "Lifetime" coverage with this, the cheapest ACA plan, would amount to $170,000, or $38,000 more than the most expensive HSA allowed by law. That's about a 22% difference. And furthermore, the bronze plan does not allow for internal investment income accumulation, which could amount to five times the actual premium revenue if held untouched until the end of projected life expectancy.A more conservative analysis would end at age 65 because that is where the Affordable Care Act presently ends. Stopping the investment calculation at age 65 would lead to the same $170,000 for the bronze plan, compared with an adjusted price of HSA of $132,000, less a 6.5% gain of $xxxx, or $xxxx. To be fair about it, the gain would have to be adjusted for inflation, which at 2% would amount to $xxxx, an xx% difference. Let's make a more dramatic assertion: The difference between the most expensive HSA and the cheapest Bronze plan would be $xxxx. In a minute we will discuss the reasoning applied to Medicare, but it will show that a deposit of $80,000 at the 65th birthday would pay for the entire average lifetime of twenty years as a Medicare recipient. In a manner of fast talking, you get a lifetime of Medicare coverage free, somehow buried within the HSA approach. That's an exaggeration, of course, but at a quick glance, it could look that way. We haven't accounted for Medicare payroll deductions or premiums. Or government subsidies. And we haven't depleted the fund for the medical expenses it was designed to pay.
HSA AND MEDICARE. Medicare Part A (the hospital component) is free, and the system while generous, is pretty ramshackle. Furthermore, it isn't free, since it collects a payroll tax from working people, and collects premiums from the beneficiaries. Almost no one understands government accounting, but it has the unique feature that its debts are often described as assets. That is, transfers from another department are assets, so money which is borrowed, from the Chinese, let's say, is placed in the general fund and transferred internally, so such debts are assets. And the annual report (available from CMS on the Internet) shows that 50% --half-- of the Medicare budget is such a transfer asset, otherwise known as a subsidy. Medicare is a popular program because a fifty percent discount is always popular; everybody likes a fifty-cent dollar. Unfortunately, the elderly Medicare recipients perceived the Obamacare costs were underestimated and became suspicious Medicare would be raided to pay for it. Therefore, every elected representative regards Medicare as the "third rail of politics" -- just touch it, and you're dead.
THE OUT-OF-POCKET CAP FUND. The Affordable Care Act contains two innovative insurance ideas for which it should be given full credit: the electronic health insurance exchanges which unfortunately caused such havoc from poor implementation, nevertheless have great potential for reducing marketing costs with direct marketing, and should be given full credit. And secondly, the cap on out-of-pocket payments is really a form of reinsurance without the cost of creating a re-insurance middleman. It is this which is the present focus. Three of the "metal" plans have deductibles of about $6000, and two of the plans have $6000 caps on out-of-pocket cash expenses by the beneficiary. How these two features will be co-ordinated is not yet clear, and does not concern the present discussion.
The point which emerges is the original Health Savings Account was based on the concept of a high deductible, matched with enough money in the fund to pay it. Effectively, it provided first-dollar coverage without the cost-stimulating effect, and experience in the field showed it worked out that way. However, the forced match of HSA with one of the metal plans interfered to some unknown degree with the comfort of virtual first-dollar and the cost reduction of a psychological high deductible. The premium is higher, because an increased volume of small claims is covered, and may be exploited. And an increased pay-out means less cash is available for investment. The result could be either higher costs or lower ones. And therefore, the idea arises of a single-payment fund of initially $6000, deposited at age 25 (Since that might well be a hardship for many young people, an additional feature is required). But the power of compound interest is such that this reserve would eventually become seriously overfunded. If the hypothetical client deposited $6000 at age 25, he would have accumulated $80,000 from this source alone. That's enough so that if it were paid to Medicare on the 65th birthday, it would pay for Medicare for the rest of the individual's life. But since it would not be needed from age 50 to age 65, further compounding (at the arbitrary rate of 6.5%) to $320,000 or some such amount, at age 65. Therefore, the following uses can be envisioned: ( 1.) Lifetime health insurance without premiums after 65. (2.) Since Medicare premiums would not be required, the Medicare premiums would not be required and should be waived. Money which flows in from earlier payroll deductions could be diverted to paying off the Chinese Medicare debt. (3.) We have glossed over this matter, but everyone was born at someone else's expense and should pay off his debt for the first 25 years of his own life. (4.) If circumstances permit, the client should be able to transfer $6000 to other members of his family for the same funding as he got it. (5.) Surpluses might persist in exceptional circumstances, and the option to supplement his own retirement funds might be offered. Eventually, it seems inevitable that the premiums for "metal" plans would be reduced.
At the very least, one would hope that this dramatic example of the power of compound investment income would encourage wider use of the principle.
How Certain Numbers Were Derived
These are important numbers to know, but difficult for most people to understand what they mean. That will, of course, depend on how they are derived, a subject of much less interest to many people. Therefore, the more controversial numbers are discussed in this chapter, which the reader may skip if he chooses.
WHAT IS THE AVERAGE LIFETIME HEALTH CARE COST, PER PERSON, AT PRESENT RATES?
Most people in the past did not live as long as they do today, so the "average person" is a composite of older people who had illnesses as children which we seldom see today, plus some who may well live beyond recent expectations, but who live beyond the age of death of their parents. One surmises this tends to include among "average" some or many hypothetical people who had both more illnesses as children, and who will have more illnesses as retirees. This would lead to an average with more illness content than the future likely contains.
Prices in the calculation have been adjusted to 2000 prices, slightly less than in 2014. Furthermore, there has been a 2% inflation adjustment, which reflects that a dollar in 1913 is now worth a penny, so we expect the penny to be worth 0.0001 cents in 2114. It is hard for most people to wrap their heads around such calculations. There is a $ 25,000-lifetime difference between the sexes, but the highly hypothetical result is this statement: The Average Person Can Expect Lifetime Health Costs of $325,000. Since most assumptions lead to an overestimate of future real costs, this number is conservatively on the high side. Comparatively few people would think they can afford that much. That is, plenty of people are going to feel stretched to adjust their savings to that level of inflation. It's the best estimate anyone can make, but by itself alone it seems to justify organizing a government agency office to match average income with average expenses, and to make the ingredient data widely available to many others outside the government on the Internet, to maximize the recognition of serious errors, unexpected financial turmoil, the development of new treatments, and changes in disease patterns. Inevitably, these calculations will be applied to other nations for comparison, but that is a highly uncertain adventure.
HOW DO YOU CALCULATE CHILDREN'S HEALTH COSTS?
Like Archimedes announcing he could move the World if he had a long enough lever and a place to stand, accomplishing this little trick could arrive at impossible assumptions. Our basic assumption is that paying for your grandchildren is equivalent to having your parents pay for you, even though the dollar amounts are different. It's an intergenerational obligation, not a business contract, and you are just as entitled to share good luck as bad luck when the calculation is shaky at best. Since children's costs are relatively small, little damage is anticipated from taking present costs, adjusted for inflation, for both past and future.
Is it reasonable and/or politically possible to lump males and females together, when females include all the reproductive costs, and have a longer life expectancy? How do we apportion the pregnancy costs between mother and child, with or without including the father? What is fair to those who have no children? What costs do we include as truly medical? Sunglasses? Plastic Surgery? Toothpaste? Dentistry? The recent hubbub about bioflavonoids threatens to convert what was mainly regarded as a fad, into a respectable therapy for allergy. When allergists and immunologists agree it is a fad, you don't pay for it; if substantially all of them think it is medically sound, pay for it. The opinion of the FDA informs the profession, it does not substitute for that opinion. Quite aside from cost issues, all of these issues affect the statistical ground rules, and may not have been treated identically among investigators. Unverifiable 90-year projections must be thoroughly standardized to be useful, and that's one committee I shall be glad to avoid because I do not believe the improved accuracy is worth the dissention. When somebody discovers a cure for cancer or Alzheimers, rules may have to be revised, net of the cost of the treatment, and net of the increased longevity. Government accounting, private accounting, and non-profit accounting are three different schools of thought for three different goals; when a government borrows outside of its accounting environment to reimburse providers of care, misunderstandings of the "cost" consequences result, in the three definitions of medical costs. In short, only broad qualitative trends can be credible at the moment.
CRUCIAL FINAL QUESTION: FUNGIBILITY (Shifting money around)
Some of the foregoing examples are lurid, and perhaps a little dramatized for effect. But the effect of compound investment income is so impressive, that there really is a little question there is plenty of money to do just about everything which needs to be done in health financing. The problem, however, is how to get enough money to pay the right bills, at the right time. The temptation to steer the money into the wrong places has been present since Isaac and Esau, and while the pooling principle of insurance (and government) solves that problem, excessive use of that flexibility is what mainly got us into the present mess. The intrusion of government can be traced to the "pay as you go" system, which amounts to paying long-term debts with current cash flow. This money has been present right along, but political considerations created pressure to begin the government system, right away, and for everyone right away. The citizens are partly responsible since they have taught politicians they must respond to people taking off their shoes and pounding the table with them. So, yes it's true that compound interest gives an advantage to frugal people, and to some extent to people who are already prosperous. But egalitarianism doesn't justify refusing to do what is in the general interest of everyone. We are currently in a pickle because we took egalitarian short-cuts in 1965, and have preferred to borrow money for healthcare, ending up paying many times what we need to pay, rather than yield to mathematical principles discovered by Euclid, or perhaps it was Archimedes.But while Health Savings Accounts, individually owned and selected, have more investment flexibility to take advantage of the necessarily higher returns of the private sector, and the flexibility to choose superior investment techniques as they are invented, and the flexibility to adjust to personal circumstances rather than universal absolutes,-- they lack the flexibility to pool resources between different persons and times. Perhaps this flexibility could be extended to whole families since there are shared perplexities of pregnancy, age group, and divorce which must be addressed in a communal forum, and perhaps churches or clubs could fill that role. But in our system sooner or later you get mixed up with a lawyer, judge or investment advisor. And therefore must contend with moral hazard and disloyal agents. By this time, I hope we have learned the weaknesses of that new branch of government, the government agencies. As Adlai Stevenson quipped, "It used to be said, that a fool and his money are soon parted. But nowadays -- it could happen to anyone."
So I recognize that although some people in a Health Savings Account system will have barrels of money, while others will be desperately in need, the fact that on average there is plenty of money to fund everybody isn't quite good enough. Somewhere a pooling arrangement must be created, and the fact that the people running it will be overcompensated must be shrugged off as inevitable. But since the people who trust it will be fleeced, they might as well be the ones to create or select it.
------------------------------------------------------------------------------------------------------------------------------------------How Do I Pay My Bills With These Things?
To summarize what was just said, on the revenue side of the ledger, we noted the evidence that a single deposit of about $55 in a Health Savings Account in 1923 would have grown to more than $300,000, today in the year 2014, because the economy achieved 10% return, not 6.5%. Therefore, with a turn of language, if the Account had invested $100 in an index fund of large-cap American corporate stock at a conservative 6.5% interest rate, it might have narrowly reached $6000 at age 50, which is re-invested on the 65th birthday, would have been valued at $325,000 at the age of 93, the conjectured longevity 50 years from now. No matter how the data is re-arranged, lifetime subsidy costs of $100 can be managed for the needy, the ingenuity of our scientists, and the vicissitudes of world finance-- within that 4% margin. We expect that subsidies of $100 at birth would be politically acceptable, and the other numbers, while stretched and rounded, could be pushed closer to 10% return. Much depends on returns to 2114 equalling the returns from 1923 to 2014, as reported by Ibbotson. At least In the past, $55 could have pre-paid a whole lifetime of medical care, at the year 2000 prices, which include annual 3% inflation. An individual can gamble with such odds, a government cannot. So one of the beauties of this proposal is the hidden incentive it contains, to make participation voluntary, and remain that way. No matter what flaws are detected and deplored, this approach would save a huge chunk of health care costs, even if they might not be stretchable enough to cover all of it.
And if something does go wrong, where does that leave us? Well, the government would have to find a way to bail us out, because the health of the public is "too big to fail" if anything is. That's why a responsible monitoring agency is essential, with a bailout provision. Congress must retain the right to revert to a bailout position, which might include the prohibition to use it without a national referendum or a national congressional election.
This illustration is, again, mainly to show the reader the enormous power of compound interest, which most people under-appreciate, as well as the additional power added by extending life expectancy by thirty years this century, and the surprising boost of passive investment income to 10% by financial transaction technology. The weakest part of these projections comes in the $300,000 estimate of lifetime healthcare costs during the last 90 years. That's because the dollar has continuously inflated a 1913 penny into a 2014 dollar, and science has continuously improved medical care while eliminating many common diseases. If we must find blame, blame Science and the Federal Reserve. The two things which make any calculation possible at all, are the steadiness of inflation and the relentless progress of medical care. For that, give credit to -- Science and the Federal Reserve.Our innovative revenue source, the overall rate of return to stockholders of the nation's largest corporations, has also been amazingly steady at 10% for a century. National inflation has been just as non-volatile, and over long periods has averaged 3%., perhaps the two achievements are necessary for each other. Medical payments must grow less than a steady 10%, minus 3% inflation, before any profit could be applied to paying off debt, financing the lengthening retirement of retirees, or shared with patients including rent seekers. But if the profit margin proves significantly less than 10%, we might have to borrow until lenders call a halt. No one can safely say what the two margins (7% + 3%) will be in the coming century, but at least the risks are displayed in simple numbers. Parenthetically, the steadiness of industrial results (in contrast to the apparent unsteadiness of everything else) was achieved in spite of a gigantic shift from control by family partnerships to corporations. Small businesses (less than a billion dollars annual revenue) still constitute half of the American economy, however, and huge tectonic shifts are still possible. Globalization could change the whole environment, and the world still has too many atom bombs. American Medicine can escape international upheavals in only one way -- eliminate the disease. Otherwise, the fate of our medical care will largely reflect the fate of our economy. To repeat, it is vital to monitor where we are going.Blue Cross of Michigan and two federal agencies put their own data through a formula which creates a hypothetical average subscriber's cost for a lifetime at today's prices. All three agencies come out to a lifetime cost estimate of around $300,000. That's not what we actually spent because so much has changed, but at such a steady rate that justifies the assumption, it will continue for the next century. So, although the calculation comes closer to approximating the next century than what was seen in the last, it really provides no method to anticipate future changes in diseases or longevity, either. Inflation and investment returns are assumed to be level, and longevity is assumed to level off. So be warned.
The best use of this data is, measured by the same formula every year, arriving at some approximation of how "overall net medical payment inflation" emerges. That is not the same as "inflation of medical prices" since it includes the net of the cost of new and older treatments and the net effect of new treatments on longevity. Therefore, this calculation usefully measures how the medical industry copes with its cost, compared with national inflation, by substituting new treatments for old ones. Unlike most consumer items, Medicine copes with its costs by getting rid of them. Sometimes it reduces costs by substituting new treatments, net of eliminating old ones. It also assumes a dollar saved by curing disease is at least as good as a dollar saved by lowering prices, and sometimes a great deal better, which no one can measure. Our proposals therefore actually depend on steadily making mid-course corrections, so we must measure them.
Revenue growing at 10% will relentlessly grow faster than expenses at 3%. Our monetary system is constructed on the gradations of interest rates between the private sector and the public sector. It would be unwise to switch health care to the public sector and still expect returns at private sector levels. Repayment of overseas debt does not affect actual domestic health expenditures, although it indirectly affects the value of the dollar. Without all its recognized weaknesses, a fairly safe description of present data would be that enormous savings are possible, but only to the degree, we contain last century's medical cost inflation closer to 3% than to 10%. The simplest way to retain revenue at 10% growth is by anchoring the leaders within the private sector.
How Do You Withdraw Money From Lifetime Health Insurance?
Four ways should be mentioned: Debit cards for outpatient care, Diagnosis pre-payment for hospital care, Transfers from escrow, and Gifts for specified purposes.
Special Debit Cards, from the Health Savings Account, for Outpatient care. Bank debit cards are cheaper than Credit cards, because unpaid credit card payments are a loan, whereas the money is already in the bank for a debit card. Some pressure has to be applied to banks or they won't accept debit cards with small balances. Somehow, the banks have to be made to see that you start with a small account and only later build up to a big one. So it's probably fair, for them to insist on some proof you will remain with them. The easiest way to handle this issue is to make the first deposit of $3300, the maximum you are allowed to deposit in one year. That's difficult for little children and poor people, however, so some way must be devised to have family accounts for children. At the moment, you just have to shop around, that's all.Spending Health Savings Accounts. Spending Less. In earlier sections of this book, we have proposed everyone have an HSA, whether existing health insurance is continued or not. It's a way to have tax-exempt savings, and a particularly good vehicle for extending the Henry Kaiser tax exemption to everyone, if only Congress would permit spending for health insurance premiums out of the Accounts. To spend money out of an account we advise a cleaned-up DRG payment for hospital inpatients, and a simple plastic debit card for everything else. Credit cards cost twice as much like debit cards, and only banks can issue credit cards. Actual experience has shown that HSA cost 30% less than payment through conventional health insurance, primarily because they do not include "service benefits" and put the patient in a position to negotiate prices or be fleeced if he doesn't. Not everybody enjoys haggling over prices, but 30% is just too much to ignore.After that, you should pay your medical outpatient bills with the debit card, although we advise paying out of some other account if you can, so the balance can more quickly build up to a level where the bank quits pestering you for more funds. Remember this: the only difference between a Health Savings Account and an ordinary IRA for practical purposes, is that medical expenses are tax-exempted when paid with money from an HSA. Both of them give you a deduction for deposits, and both collect income without taxes. If you can scrape together $6000, you are completely covered from Obamacare deductibles, and since co-payment plans are to be avoided, an HSA with Catastrophic Bronze plan is your present best bet. If you have a bronze plan, you probably get some money back if you file a claim form, but those rules are still in flux at this writing. The expense of filing and collecting claims forms is one of the reasons the Bronze plan is more expensive, but that's their rule at present.
There are some other important things to say about outpatient vs. inpatient care, but it seems best to describe how inpatient care is envisioned to work in this system, before returning to the tension between the two. As will then become apparent, increasing the ease of use might create the problem of making it a little too easy to spend money.
Payment by Diagnosis Bundles, for Outpatient care. In 1983 a law was included as an unnoticed part of the annual Budget Reconciliation Act, which nevertheless later proved to have a huge effect on the health financing system. The proposal was to stop paying for Medicare patients on the basis of the itemized services each patient received as a bill, but to pay a single lump sum for the main diagnosis of each patient, using the argument that most cases of a given diagnosis were pretty much the same, and what variation there was, would soon average itself out after a few cases. Such a meat ax approach to the complexity was justified by the argument that a patient sick enough to be in bed in a hospital, was too overwhelmed by his frightening situation and too uneducated in its issues, to be able to dispute what was done to him. Market mechanisms, in short, were futile is situations with such imbalances of information and power. Consequently, a great deal of money was being wasted on accounting systems to arrive at prices which were ultimately set in an arbitrary way.
This argument prevailed in Congress, which was becoming desperate about relentless cost increases in Medicare, even sweeping aside the grossly primitive details of a system defining the solvency of vital institutions. The misgivings from economists that the accounting system was a large part of the internal hospital administrative information system, were also treated like mutterings of pointy-heads. To the extent these objections were valid, they would probably lead to a collapse of the experiment, so why worry about it. In fact, the expedient emerged that the prices of the DRG ( diagnosis "related" groupings) were simply revised to result in a 2% profit margin on the bottom line, no matter what the medical issues happened to be. It was a highly effective rationing system, not terribly far removed from a lump sum payment with a 2% markup, so live with it. Since the Federal Reserve targets 2% annual inflation, 2% profit is no real profit at all.
The hospitals might have rebelled, or might have collapsed. Instead, they accepted 2% for inpatients and set about adjusting the subsidies, aiming for a 15% profit margin on the Emergency Room, and a 30% profit on outpatient services. Subsidies from such accounting were difficult to achieve at first, so Emergency rooms were enlarged, and much-expanded outpatient facilities were built, requiring hospitals to purchase physician practices to keep them filled. The entire healthcare system was put under strain, and hardball was the game of the day. New lifesaving drugs were priced at $1000 per pill, institutions were merged out of existence, the office practice of medicine was in turmoil, and a year in business school could make you a millionaire if you could appear calm in the midst of confusion.
I tell this story to explain why, with great reluctance, I advise the management of Health Savings Accounts to base their inpatient payment system on some variation of Diagnosis Related Groups. It's a terrible system, designed by rank amateurs, which results in distortions of a noble profession. But there is no other rational choice. It does protect the paying agency from being fleeced, once it gets past negotiation of a small list of prices which aggregate to a profitable bottom line. By protecting the payment system, it protects the patients from a chaotic price jungle which, unchecked, will rapidly destroy health care. If we experience more than 2% inflation, the destruction will be quicker.
Resolving Tension Between The Two Payment Systems. Evidently, some clear thinking by some smart people have brought them to the ruthless conclusion that a two-class system of medical care is preferable to the way we are otherwise going. Rich people will have their way if their own health is at stake, and poor people will have their way if they exercise their votes. Both of these conclusions are correct, but they lead to Medieval monks retreating into monasteries. The cure for cancer and a few brain diseases might make monasteries unnecessary, and so would a drastic reduction in health care costs. Huge research budgets and major regimentation are big-government approaches, of willingness to accept some loss of freedom to achieve equality of outcome.
But we can't completely depend on either choice, so the remaining choice is to undermine a lot of recent culture change, by devolving back to leadership on the local level of small states and big cities. This is a small-government approach, willing to accept wider inequalities in order to seek freedom to act. Mostly using the licensing power, the competition will reappear if retirement villages and nursing homes are licensed to be hospitals. If not, nurses and pharmacists can be licensed as doctors. Some of this could become pretty brutal, and all of it leads to patchy results. But of its ability to restrain prices, there can be little doubt.
Escrow Subaccounts within HSA Accounts. Whether anything can restrain reckless spending of "found" money, is quite a different matter, however. It may be that supply and demand will balance, even if it takes generations. There is some hope to be gained from watching reckless teenagers become penny-pinching millennials, but there remain dismal reminders of improvidence to be found in ninety-year-old millionaires marrying teen-aged blondes, further reinforced by watching the blondes run off with stable-boys. The net conclusion is that if certain portions of a Health Savings Account must be set aside for mandatory later expenses, then the money should be set aside within partitions, like an escrow account. Even that will have limits to its effectiveness, as I have noticed when trust-fund babies in my practice worked around the restraints their grandfather's lawyer took care to put in place.
Specified Gifts to be Encouraged. Only limited restraints on spending the client's own money can ever be justified, but certain types of gifts can still be better justified than others. One of them would be the special $6000 escrow fund for deductibles and caps on out-of-pocket spending. Particularly in the early transitional years, the fund's solvency may be threatened by leads and lags, where these escrow funds could save the day. Therefore, if someone accumulates large surpluses in his account by the fortuitous conjunction of events, he should be encouraged to consider donating a $6000 escrow to one of his grandchildren or other impecunious relatives. Quite often, a prudent gift to a grandchild can lighten the burdens of his parents or other members of the family. If they wish, any number of $6000 transfers to the escrow funds of others should be encouraged.
No Medicare, no Medicare Premiums. We assume no one wants to pay medical expenses twice, and will, therefore, drop Medicare if investment income is captured in lifetime Health Savings Accounts. The major sources of revenue for Medicare at the present time fall into three categories: half are drawn from general tax revenues, a quarter come from a 6% payroll deduction among working-age people, and another quarter are premiums from retirees on Medicare. All three payments should disappear if Medicare does, too. Therefore, the benefit of dropping Medicare will differ in type and amount, related to the age of the individual. Eliminating the payroll deduction for a working-age person would still find him paying income taxes in part for the costs of the poor, as it would for retirees with sufficient income.
Retirees would pay no Medicare premiums. Their illnesses make up 85% of Medicare cost, but at present, they only contribute a quarter of Medicare revenue. However, after the transition period, they first contribute payroll taxes without receiving benefits, and then later in life pay premiums while they get benefits, to a total contribution of 50% toward their own costs. But the prosperous ones still contribute to the sick poor through their income taxes. There might be some quirks of unfairness in this approach, but its rough outline can be seen from the size of their aggregate contributions, in this scheme. At any one time during the transition, working-age and retirees would both benefit from about the same reduction of money, but the working-age people would eventually skip payments for twice as long. Invisibly, the government subsidy of 50% of Medicare costs would also disappear as beneficiaries dropped out, so the government gets its share of a windfall, in proportion to its former contributions to it. One would hope they would pay down the foreign debt with the windfall, but it is their choice. This whole system -- of one quarter, one quarter, and a half -- roughly approximates the present sources of Medicare funding and can be adjusted if inequity is discovered. For example, people over 85 probably cost more than they contribute. For the Medicare recipients as a group, however, it seems like an equitable exchange. This brings up the subject of intra- and extra-group borrowing.
Escrow and Non-escrow. When the books balance for a whole age group, the managers of a common fund shift things around without difficulty. However, the HSA concept is that each account is individually owned, so either a part of it is shifted to a common fund, or else frozen in the individual account (escrowed) until needed. It is unnecessary to go into detail about the various alternatives available, except to say that some funds must be escrowed for long-term use and other funds are available in the current year. Quite often it will be found that cash is flowing in for deposits, sufficient to take care of most of this need for shifting, but without experience in the funds flow it would be wise to have a contingency fund. For example, the over-85 group will need to keep most of its funds liquid for current expenses, while the group 65-75 might need to keep a larger amount frozen in their accounts for the use of the over-85s. In the early transition days, this sort of thing might be frequent.
The Poor. Since Obamacare, Medicaid and every other proposal for the poor involves subsidy, so does this one. But the investment account pays 10%, the cost of the subsidy is considerably reduced. HSA makes it cheaper to pay for the poor.
Why Should I Do It? Because it will save large amounts of money for both individuals and the government, without affecting or rationing health care at all. To the retiree, in particular, he gets the same care but stops paying premiums for it. In a sense, gradual adoption of this idea actually welcomes initial reluctance by many people hanging back, to see how the first-adopters make out. Medicare is well-run, and therefore most people do not realize how much it is subsidized; even so, everyone likes a dollar for fifty cents, so there will be some overt public resistance. When this confusion is overcome, there will still be the suspicion that government will somehow absorb most of the profit, so the government must be careful of its image, particularly at first. Medicare now serves two distinct functions: to pay the bills and to protect the consumer from overcharging by providers. Providers must also exercise prudent restraint. To address this question is not entirely hypothetical, in view of the merciless application of hospital cost-shifting between inpatients and outpatients, occasioned in turn by DRG underpayment by diagnosis, for inpatients. A citizens watchdog commission is also prudent. The owners of Health Savings Accounts might be given a certain amount of power to elect representatives and negotiate what seem to be excessive charges.
We answer this particular problem in somewhat more detail by proposing a complete substitution of the ICDA coding system by SNODO coding, within revised Diagnosis Related Groupings,(if that is understandable, so far) followed by linkage of the helpless inpatient's diagnosis code to the same or similar ones for market-exposed outpatients. (Whew!) All of which is to say that DRG has been a very effective rationing tool, but it cannot persist unless it becomes related to market prices. We have had entirely enough talk of ten-dollar aspirin tablets and $900 toilet seats; we need to be talking about how those prices are arrived at. In the long run, however, medical providers are highly influenced by peer pressure so, again, mechanisms to achieve price transparency are what to strive for. These ideas are expanded in other sections of the book. An underlying theme is those market mechanisms will work best if something like the Professional Standards Review Organization (PSRO) is revived by self-interest among providers. Self-governance by peers should be its theme, ultimately enforced by fear of a revival of recent government adventures into price control. Those who resist joining should be free to take their chances on prices. Under such circumstances, it would be best to have multiple competing PSROs, for those dissatisfied with one, to transfer allegiance to another. And an appeal system, to appeal against local feuds through recourse to distant judges.
Deliberate Overfunding. Many temporary problems could be imagined, immediately simplified by collecting more money than is needed. Allowing the managers some slack eliminates the need for special insurance for epidemics, special insurance for floods and natural disasters, and the like. Listing all the potential problems would scare the wits out of everybody, but many potential problems will never arise, except the need to dispose of the extra funds. For that reason, it is important to have a legitimate alternative use for excess funds as an inducement to permit them. That might be payments for custodial care or just plain living expenses for retirement. But it must not be a surprise, or it will be wasted. Since we are next about to discuss doing essentially the same thing for everybody under 65, too, any surplus from those other programs can be used to fund deficits in Medicare. But Medicare is the end of the line, so its surpluses at death have accumulated over a lifetime, not just during the retiree health program.
That may not be more accurate, but it displays its assumptions better. Michigan Blue Cross has calculated we calculate lifetime costs and Obamacare costs by starting with lifetime average health costs of $325,000 and subtracting Medicare. Although Medicare is reported by CMS to have average costs of $xxxx, for which we prefer to assume a Health Savings Account "present value" cost of $80,000 on the 65th birthday (at a 6.5% interest rate). At the same 6.5% rate, a $3300 annual deposit from age 25 to 65 (the earning years) would total $132,000 of deposits. Preliminary goals for a hypothetical average person are: To accumulate $80,000 in the Medicare fund by the age of 65, to pay off the 25-year health costs of 2.0 children per couple as a gift to them, and to pay his own relatively modest average healthcare costs from 25-45, somewhat higher costs 45-65. The Medicare goal of $80,000 is what is estimated to be what is required for a single-deposit investment fund (paid on the 65th birthday) to pay the health costs for an average person aged 65-93,(a guessed-at future average longevity), with an estimated compound investment income of 4%, also guessed, but conservative. Inflation is ignored, assuming revenue and expenses will inflate at the same rate. Our average consumer will have to set aside $1250 per year from age 25 to 65, and earn 4% compounded, to do it.Those who disagree with the underlying assumptions should feel free to substitute their own assumptions. The interest rate of 4% is deliberately low, in order to make room for disagreements which are higher. The upper limit is set to match the HSA contribution limits of 3300 times 40, becoming hypothetically the upper bound of revenue which can ever be anticipated. Anticipating two children per couple and full employment from 25 to 65, this revenue effectively covers one full lifetime, from cradle to grave. Childhood illnesses and elderly disabilities notwithstanding, this is all the revenue we allow ourselves in this example.
Let us assume that an average person can start contributing to an H.S.A. at the age of 25, even though perhaps a quarter of the population at that age are burdened with college debts, etc. and cannot. We are well aware of the Pew Foundation poll that xxxx% of those under 30 are still living with their parents, and that xxxx% have college debts. (Congress ought to examine this condition, which could apply at any age, and provide for make-up contributions later.) The present ceiling of $3300 annual contribution is otherwise taken as the upper boundary of what is possible for the sake of example, and theoretical deficits would have to be made up from the $68 trillion dollar surplus created by such legal maximums. To plunge ahead with the example, our average person sets aside $3300, starting at age 25 toward lifetime health costs. To simplify the example, he does so whether he can afford it or not, and what he can't supply himself is provided by a subsidy or a loan. Since present law prohibits spending from the H.S.A. for health insurance premiums (this should be reconsidered by Congress, by the way), an estimated premium of $300 for his own Catastrophic insurance is taken from the set-aside, and the remainder is placed in the H.S.A., paying an estimated 4% tax-free. Within this he eventually needs to set aside a Dependent Escrow premium (remember, this example covers lifetime expenses, even though everyone has Medicare), which for twenty years (until age 45) is zero for Medicare and available for medical gifts to Children, and after that is exclusively used for Medicare, both of which will be explained in later sections.Starting with the Medicare example. Notice that forty years of maximum contributions would amount to far more than the necessary $40-80,000 by age 65. We haven't forgotten that the individual is at risk for other illnesses in the meantime, so in effect what we need is an individual escrow fund for lifetime funding intended (at first) only to replace Medicare coverage. (We are examining lifetime coverage, piece by piece, trying to accommodate an extended transition period.) Depending on a lot of factors, that goal could cost as little as $100 a year deposited for forty years at high-interest rates, or as much as the full $1000 per year with low rates. It all depends on what income you receive on the deposits in the interval. In a moment, we will show that 10% return is not impossible, but it is also true that a contribution of $1000 per year would not seem tragic, compared with the present cost of health insurance (now averaging over $6000 a year). I have unrelated doubts about the current $325,000 estimate of average lifetime health costs, but that is what is commonly stated. For the moment, consider these numbers as providing a ballpark worksheet for multi-year funding, using an example familiar to everyone, but not necessarily easy to understand after one quick reading.Health Savings Accounts are tax-exempt, and they can earn investment income. Except it isn't all it could be. Professor Ibbotson of Yale, the acknowledged expert in the long term results of investment classes, has regularly published data going back nearly a century. In spite of military and economic disasters of the worst sort, investment classes have remained remarkably steady throughout the past century and presumably will maintain the same relationships for some time to come. John Bogle of Philadelphia has translated that into index funds of investment classes, with almost negligible administrative costs. (Caution: Many index funds are sold with very high trading costs, typically in charges when money is withdrawn. Be careful of your counterparty, particularly if he specifies the index fund, because he may limit it to one who gives kickbacks to him.) With this warning, there is a reasonably good chance of getting returns approaching 10% for investments in index funds of well-known American stocks, even though the typical HSA at present is yielding much less. This investment income can grow to the point where it constitutes a fairly large part of the health revenue.
SIX PIECES OF THE LIFETIME PIE
Instead of starting at birth and ending at death, this book will reverse the process. Let me explain. There is a big transition problem in a proposal like this, since the readers will be of different ages, and the system must work without gaps. Everybody has already been born, and for a long time to come, everybody will have a piece of his life behind him that he does not want to pay for. The time is past when Lyndon Johnson could solve the transition problem by simply giving a gift of many years free coverage to most of the new entrants to his system. So, although it will probably spook a number of old folks just to hear the discussion, let's begin for completeness with the Last Year of Life Coverage, and end up with the First year of Life coverage. Both of those apply to 100% of Americans in a theoretical sense, and in a sensible system would be the basic coverage. If any health insurance should be universal, these two have the strongest arguments. Unfortunately, they have the least chance of political success. Therefore, it is likely that they will be voluntary and self-pay if they are adopted at all.
FOREWORD, written June 28,2015
This book was originally based on a notion, on a dream if you will. A whole lifetime of healthcare might be purchased, for what now only covers a quarter of a half -- those scarcely-noticed payroll deductions for Medicare, listed on everybody's payroll stub. But then politics and Supreme Court decisions came along. Turning over each pebble on a new heap, it nevertheless seems that amount might still stretch to cover all of the nation's average lifetime costs, although payroll deductions wouldn't resemble the way to do it. Reducing prices by 28% of $350,000 is a ton of money, particularly when multiplied by 300 million people. Let's lower expectations by saying the new narrower proposal might only reduce prices by 14%. That would be $39,000 times 300 million, or twice the combined fortunes of Bill Gates and Warren Buffett. The $39,000 is a substantial amount for anybody, and $ 11.7 trillion is an astonishing aggregate for the nation. That's once in a lifetime, but it's still $140 billion a year.
I decided to ignore the 42% of historical costs which Obamacare covers (age 21 to 66) until its facts emerge. Just add the cost of the earning segment (21 to 66) to estimate whole lifetime costs. That does leave a gap of one third in the middle of life. If you don't know what the Affordable Care Act will eventually cost, you can't be confident what lifetime healthcare will cost. I'm confident lifetime Health Savings Accounts would cost much less. The Affordable Care Act has not yet convincingly described any cost reductions. But to be fair, neither do Health Savings Accounts. They reduce the price by adding revenue.
The issue is how to transfer $238,000 from individuals in one group, to another group.Quick calculation now follows. Average lifetime healthcare expenditure (in the year 2001 dollars per person) is in the neighborhood of $350,000. That's the estimate of statisticians at Michigan Blue Cross, confirmed by Medicare. Medicare takes half of the annual cost, from birth to age 21 takes another 8%, and we don't know the cost of the unemployable of working age, but they are 10% of the population. So, the new segment we assigned ourselves, involves at least 68% of national health costs, and probably somewhat more. That represents the basis for saying the working population 21-66 must pay its own costs and somehow transfer at least 68% more to what we will call the dependent sector. At a minimum, that's 68% of $350,000 per lifetime, or $238,000. Don't take it too seriously, but that's the ballpark.
Endowment funds traditionally aim for 8% annual return (3% from inflation, 5% net). The stock market has averaged 12% gain for a century, so 4% isn't exactly missing, but its disappearance requires convoluted explanation, later in the book. Starting with those bits of information and adding a few more, just re-arranging payments would get to the same final result-- by spending one-third as much money. The cost of separating employer-based insurance from all the rest of it exceeds my abilities, so it will have to dangle. How we got to that conclusion isn't rocket science, but it isn't obvious, either. So let's make the conclusion easier: you can make a ton of money doing what is suggested. Don't complain it isn't two tons or only half a ton, it is what it is. You can put this data through a big data computer, or use a slide rule, but you are still dealing with predictions about the future, which will contain lots of uncertainty. Although it will not make healthcare free, it implies savings of about $38,000 per person, per lifetime. View that saving in two ways: it's only about $500 per person, per year. Or, viewed as a nation of 316 million inhabitants, it saves $150 billion per year. Skeptics could attack the math as exaggeration, and still get an answer in billions per year. Tons instead of billions would be even more accurate, just sound less precise.
Next might come nit-pickers. You can't get 8% investment income returns a year, unless this, or unless that. Very well, just say this is the top limit of what is possible as an average, using average investment advice. The Federal Reserve confidently promised to keep inflation at 2%, but actually experienced 3% over the past century. Chairman Bernanke tried his best to "target" inflation up to 2% but inflation just resisted going up that far, and it's pretty hard to get any agreement about why it resisted. Accuracy just isn't possible when you are predicting the economic future. That's why the unit of measurement is in tons. Tons of money. Who will save it and who will steal it, is much harder to predict.
Some doctors, deans, drug companies, financiers and politicians will always try to increase their spending to equal any available revenue. About forty percent of the public will line up at the same trough. All that is beyond my control. You won't find one word in the accompanying book to suggest I endorse such behavior. All I did was write a cookbook. The cooking is up to you.
George Ross Fisher, MD
Philadelphia
June 28, 2015
Summaries for the Book Jacket and Elsewhere.
Short Summary for Book Jacket:
This book presents a physician's viewpoint on a specific healthcare Reform. Much of the hidden economics of healthcare, a major topic of the first book, was omitted. In its place is an expanded description of Health Savings Accounts as they stand right now -- a dual provision linking medical advances with the expanding need for retirement income, the need for which is mainly the consequence of better health care. It is put to the public in two different ways: take care of your health or you won't get much retirement. Alternatively, invest your healthcare savings wisely, or you will never be able to afford retirement.
Most people don't really like to save, they like to spend. And to a degree, what you save reduces the income of those who need to help you. They aren't evil, but they will take your money if you offer it to them. Because of these two obstacles, I have come to feel spreading present Health Savings Accounts is all that can be accomplished in a decade. But improving the Account system could probably generate much more savings than the present one. Having some idea of where it all would lead, would greatly enhance the incentive to do some things the public ought to do, anyway. So a second section is added, for future generations to modify its future if they please, and if the whims of circumstance permit.
Once again, I express my gratitude to John McClaughry, the former Republican leader of the Vermont legislature and Senior Policy Adviser in the Reagan White House, for suggesting basic features. The flaws in such future features are all my own.
But remember, the classical form only needs a little tweaking. All you have to do is buy it and urge Congress to tweak its tax exemption to be level with every other plan. Removing small mandated benefits (which reduce the market power of high deductibles) might also help.
Lifetime Health Savings Accounts:How Much is Enough?
The Duchess of Windsor was reported to say, a woman can never be too rich or too thin. Perhaps, but with insurance you state -- in advance -- how much insurance you can buy, best not expect more. In healthcare, it's my hunch something drastic would have to change before the American public voted an assessment for more than $3300 per person, for every working year from age 26 to age 65. In fact, if it went much higher, many people would probably look for a way to escape the burden. Perhaps we could supplement 3% per year, the historical rate of inflation for the past century. That's fair because although it would reach $10,000 at age 65 instead of $3300, everything else would have readjusted to give it the same financial impact. Similarly, asking people 26-65 to pay for all ages is more palatable if it's arranged as your own childhood and retirement to be supported.
Excluded: Past debts and Custodial Care. In any event, any payments for past debts, for health or otherwise are not envisioned in the following plan. The term "fixed income" reminds our debt and equity obey different rules, and the premise is the income supplement of this calculation will be based on equity, common stock. Furthermore, we know the National Debt, but how much of it once paid for health services, is fuzzy. When I started this analysis, I really never dreamed all of the current healthcare costs might be covered by investment income from common stocks, and it's going to take some experience to be sure even that is reasonable. It allows us to take a stance: if it won't pay current costs, at least it will pay for some of them. If it more than pays for them, annual deposits should be reduced, never confiscated. To avoid circumvention by changing definitions, it might be well to state custodial care costs are not included, either, because they are treated as retirement income.
Medicare. Making it easier to explain, let's begin at the far end of the process, the day after death, looking backward. This proposal didn't initially include a Medicare proposal, but the accumulation of its unpaid debt has become so alarming, considering Medicare within Health Savings Accounts could fast become a national priority having no other solution. In addition, most factual health data come from Medicare, so the reader gets accustomed to hearing about it. So, while the Medicare situation is fraught with political obstacles, we might have to risk them. While debt overhang from earlier years continues to grow, Health Savings Accounts cannot be confidently promised to rescue Medicare by itself. But perhaps at least the Savings Account discussion could put a stop to going deeper into debt. Even a stopgap would have to get started pretty soon, but there is also a chance an improving economy might partially reduce the indebtedness.
Medicare-HSA Overlaps. At present, Catastrophic coverage is required for Health Savings Accounts, but its premiums are not tax-exempt. To extend HSA for the life expectancy, therefore, requires an additional average of 18 years of after-tax premiums. We have split lifetime HSA into two parts at age 65 and assume a single-premium ($80,000) exchange for Medicare, possibly traded for partial forgiveness of premiums and rebate of payroll taxes. It is important not to count the $80,000 twice if it assumed to be self-financed. One quarter from payroll taxes, one quarter from premiums, and a half from the $80,000 which used to be from the taxpayers. If pre-payment begins at an early age, Medicare costs might be quite modest after growth from income. Even when we show all the costs, including double payments, using an HSA at conservative rates like 4% will reduce the Medicare cost by 75%. Better performance depends heavily on approaching 12.7% by passive but hard-boiled investing. To pay down the existing debt back to 1965 is not contemplated by this proposal. At present, it grows by 50% of annual costs by addition; and an unknown amount by compounding. The amount of debt service is probably going to depend on the national ability to pay it down, regardless of its written terms. The same is likely to be true of subsidies for the poor. Ultimately, both of these decisions are political, limited by the ability to pay. Because of the long time periods, comparatively modest interest rates could convert this impending disaster into a manageable cost, but it should not be contemplated until net investment returns approach 12.7 %. The outcome of these intersections is that the terms and benefits become largely a matter of political choice. That has been true for a long time, yet no effective corrections have been made. It is perhaps unbecoming of a citizen to say so, but the political system needs some steps taken to increase its sense of urgency.
Disintermediation of Investment Returns. By this reasoning, the rescue of Medicare depends on the political choice to do it, and the avoidance of a collision with the financial industry. Without a solution to the Medicare problem, a solution to paying for healthcare at younger ages becomes quite feasible, but it would be useless. Conversely, solving Medicare would be possible if the problems of younger people were ignored, but that is equally unlikely. To solve healthcare financing for all ages depends on introducing some new feature, and the easiest solution to imagine is to raise effective net interest rates. Interest rates are unusually low at present, and the Federal Reserve probably feels it would be dangerous to raise them. However, that's the easy part, because interest rates are certain to rise, eventually. What's much harder to envision is to flow the improved rates and the transaction-cost efficiencies through the financial system without wrecking it. What's hard to imagine is not hard to seem feasible, however. It is to take investments averaging 12.7%, flowing 10% past the intermediaries to the investor; and keeping it up for a century. Disintermediation, so to speak.
Rationalizing Fragmented Payments The transition to a solvent system could be greatly eased by the present premiums and payroll deductions, which are largely age-distributed, and can, therefore, be forgiven in a graduated manner for late-comers to the program. Most redistribution of high-cost cases should be handled through the catastrophic insurance, which is well suited for invisible and tax-free redistribution. Because of hospital internal cost-shifting, inpatients are overpriced, rapidly heading toward underpricing. This distortion of prices is achieved by squeezing inpatient prices with the DRG to shift costs and overpricing to hospital outpatients. In the long run, distorting prices has the effect of raising them. This will more immediately affect the relative costs of Catastrophic and Health Savings Accounts and should be more carefully monitored, with an eye toward re-achieving equilibrium.
Dual Reimbursement Systems are Better Than One At present costs, statisticians estimate average lifetime healthcare costs at about $325,000 in the year 2000 dollars; we could discuss the weaknesses of that estimate, but it's the best that can be produced. Women experience about 10% higher lifetime health costs than men. Roughly speaking, how much the average individual somehow has to accumulate, eventually has to equal how much he spends by the time of death. At this point, we must work around one of the advantages of having separate individual accounts. On the one hand, individual accounts create an incentive to spend wisely, but it is also true that pooled insurance accounts make cost-sharing easier, almost invisible, and (for some) tax-free. Therefore, linking Health Savings Accounts with Catastrophic insurance provides a way to pool heavy outlier expenses, while the incentive for careful money management resides in the outpatient costs most commonly employed (together with a special bank debit card) to pay outpatient costs. Such expenses are much more suitable for bargain-hunting anyway because dreadfully sick people in a hospital are in no position to bargain or resist.
Internal Borrowing. Furthermore, there is a significant difference between mismatches of aggregate revenue-to-expenses of an entire age group, and outliers within the same age cohort, the latter much likelier to be due to chance. To put it another way, somebody has to pay these debts, and the plan has been designed to break even as an entirety. Surely we must have a plan about who should pay them when enough revenue is not yet present in a new account. Surely some groups are always in surplus, other groups are always in arrears; the two should be matched, at low or zero interest rates. Borrowing between sick outliers and lucky good people within the same age cohort should pay modest interest rates, and borrowing between different cohorts for things characteristic of the age (pregnancy, for example) should pay none. Unfortunately, some people may abuse such opportunities, and interest must then be charged. Until the frequency of such things can be established, this function of loan banking should be part of the function of the oversight body. When it's limits become clearer, it might be delegated to a bank, or even privatized. While it is unnecessary to predict the last dime to be spent on the last day of life, incentives should be identified by the managing organization, separating structural cash shortages from abusive ones. Much of this sort of thing is eliminated by encouraging people to over-deposit in their accounts, possibly paying some medical bills with after-tax money in order to build them up. Such incentives must be contrived if they do not appear spontaneously. User groups can be very helpful in such situations. People over 65 (that is, those on Medicare) spend at least half of that $ 325,000-lifetime cash turnover, but just what should be counted as their own debt, can be a matter of argument (see below.)
Proposal 10: Current law permits an individual to deposit $3300 per year in a Health Savings Account, starting at age 25, and ending when Medicare coverage appears. Probably that amount is more than most young people can afford, so it would help if the rules were relaxed to roll-over that entitlement to later years, spreading the entire $132,000 over the forty-year time period at the discretion of the subscriber.Bifurcated Health Savings Accounts. When Health Savings Accounts were first devised, it never seemed likely that Medicare might be supplanted. However, Medicare has grown both highly popular and severely under-funded, probably running at a large loss. The rules should be modified to permit someone who has health insurance through an employer to develop a Health Savings Account which the funds but does not spend while he is of working age. The funds would then build up, enabling him to buy out Medicare on his 65th birthday or thereabout, with a single-premium exchange at present prices, (exchanging about $100,000 funded by the forgiveness of Medicare premiums and some portion of payroll deductions from the past). He would have to purchase Catastrophic coverage at special rates. If this approach proved popular, it might supply extra funds for loaning to HSA subscribers in the outlier category. While there is no thought of phasing out Medicare against the subscribers' will, Congress would certainly be relieved to have subscribers drop out of a program which must be 50% subsidized.Proposal 11: The present closing age for HSA enrollments at the onset of Medicare should be extended a few years older. And single-premium buy-outs of Medicare coverage, including the possible return of payroll deductions where indicated, should be permitted as an option.Single-Premium Medicare, age 65 Hypothetically, if anyone could live to his 65th birthday without spending any of the accounts, a prudent investor would have accumulated $132,000 in pure deposits on his 65th birthday. He only needs $80,000 to fund Medicare as a single-payment at age 65, however, so he can even afford to get sick a little. If he starts later than age 25, he has already paid for Medicare somewhat, with payroll taxes. That could be considered payment toward reduction of the Medicare debt.Proposal 12: Congress should create and fund a permanent Health Savings Account Agency. It should have members representing subscribers and providers of these instruments, with the power to hold hearings and make recommendations about technical changes. It should meet jointly with the Senate Finance Committee and the Health Subcommittee of Ways and Means periodically. It should be involved with the appropriate Executive Branch department, to review current activity, detect changing trends, and recommend changes in regulations and laws related to the subject. On a temporary basis, it should oversee inter-cohort and outlier loans, leading to recommendations concerning the size and scope of this activity.
If someone makes a single deposit of $80,000 on his/her 65th birthday, there will accumulate $190,000 in the account over the next 18 years, the present life expectancy if he spends nothing for health and invests at 5%; and $190,000 is what the average person costs Medicare in a lifetime. Since the average person spends $190,000 during 18 years on Medicare, enough money will accumulate in Medicare to pay its expenses, and after some shifting-around, this should make Medicare solvent, in the sense that at least the debt isn't getting bigger because of him. Furthermore, index funds should be returning 10-12% over the long haul, so there should be some firm discussions with the intermediaries about some degree of dis-intermediation. Please don't do the arithmetic and discover that only $40,000 is needed. That seems plausible, but that's wrong because the costs remain the same , and previously the government has been borrowing half the money from foreigners. In effect, the subscribers have been paying the government in fifty-cent dollars, while claiming the program is entirely self-funded. There has been an exchange of one form of revenue for another, so the required revenue actually does demand $80,000 for a single deposit stripped of payroll deductions and perhaps premiums. An end would be put to further borrowing, but the previous debt remains to be paid. I have no way of knowing how much that amounts to, but it is lots. All government bonds are general obligations, mixed together, while access to Medicare reports back to 1965 is not easily available. What we can more confidently predict is the limit young working people can afford for the sole purpose of paying off the Medicare debts of the earlier generation. If there are other proposals for paying off this foreign debt, they have not been widely voiced. And the debt is still rapidly growing.
Escrow the Single Premium A young subscriber would have to set aside an average of $850 per year (from age 25 to 64) to achieve $247,000 on his 65th birthday, assuming a 5% compound investment income and relatively little sickness. This might seem like an adequate average, but occasional individuals with chronic illnesses would easily exceed it in health expenditures. Assuming a 10% return, he would have to contribute $550 yearly. It is not easy to estimate the size and frequency of expensive occurrences in the future, so someone must be designated to watch this balance and institute mid-course adjustments. As an example, simple heart transplants costing $200,000 are already being discussed. To some unknown extent, the cap on out-of-pocket expenses would have to be adjusted to pass these cost over-runs indirectly through the Catastrophic insurance. Insurance does greatly facilitate sharing of outlier expenses, but usually requires a time lag whenever new ones appear.
It does not require much political experience to know taxpayers greatly resent paying debts that benefitted earlier generations. They complain, but complaining does not pay off the debts of the past. To double required deposits in order to pay off past debts, as well as using forgiveness of payroll deductions and premiums, would require an additional $120,000 per year escrow, for each year's debt accumulation. At present, roughly $ 5300 per beneficiary, per year, is being borrowed, and there are roughly twice as many current beneficiaries as people in the tax-paying group, but for only 18 years, as compared with 40 years as a prospective beneficiary. So that comes to liquidating roughly $1300 a year of debt to balance the two populations or $2600 a year to gain a year. That's for whatever the debt happens to be, which surely someone can calculate. To accomplish it, one would have to project an average of ??% income return. That's definitely the outer limit of what is possible, and it probably over-reaches a little. Therefore, to be safe, one would have to assume some other sources of income, a change in the demographic patterns, or an adjustment with the creditor. Assuming inflation will increase expenses equally with inflation seems a possibility. And it also seems about as likely that medical expenses will go down, as that they go up. You would have to be pretty lucky for all these factors to fall in line over an 80-year lifetime.
Medicare: Optional, Mandatory, or Third Rail? It is this calculation, however rough, which has made me change my mind. It was my original supposition that multi-year premium investment would only apply up to age 65, and that would be followed by Medicare. In other words, it should only be implemented as a less expensive substitute for the Affordable Care Act. It seemed to me the average politician would be very reluctant to agitate retirees by proposing a plan to eliminate Medicare. They would feel threatened, the opposing party would fan the flames of their fears, and the result would be a high likelihood of undermining the whole idea for any age group, for many years. Better to take the safer route of avoiding Medicare, and confining the proposal to working people, where its economics are overwhelmingly favorable.
But when the calculations show how close this proposal under optimistic projections would come to failure, and when nothing remotely close to it has been proposed by anyone, the opportunity runs the risk of passing us by. So, I changed my mind. The moment of opportunity is too fleeting, and the consequences of missing it entirely are too close, to worry about the political disadvantages of doing the right thing. The transition to a pre-funded lifetime system will take a long time to get mature, and the political obstacle course preceding it is a daunting one. However, there is another way of saying all this, which is perhaps more persuasive that Medicare must be changed. It begins to look as though the unfunded and accumulated debts of Medicare are such a drag on our system of government, that very little can be accomplished by anyone, until this central problem is addressed. In that sense, our problem is not the uninsured or the illegal immigrants, or an expensive insurance system. Our problem has become Medicare underfunding, and our second problem is that everyone loves Medicare.
The "simplified" goal is therefore for everyone to accumulate $80,000 in savings by the 65th birthday, remembering that savings get a lot harder when earned income stops and definitely remembering that people approaching retirement are not likely to part readily with $80,000. With the current law, you would have to start maximum annual depositing in an HSA of $3300 by your 52nd birthday, to reach $80,000 by age 65, and you would still need 10% internal compounding to make it. With a 5% return, you would have to start at age 48. But notice how easily $200 a year would also get you there, starting at age 25 (see below) but it immediately gets questionable to assume $700 a year deposit for a 25 yr-old receiving 5% returns. We are definitely reaching a point where the ideas proposed in this book will no longer bail us out of our Medicare debt. Because -- the most optimistic of these projections are achieved by assuming there will be no contributions at all from people aged 25-65, for their own healthcare, babies, contraceptives and whatever. Many frugal people might skin by with looser rules; But the universal goals of the past are just that, the goals of the past. If we are going to cover lifetime health costs instead of just Medicare, many more will need $80,000 to do it and have something left to share with the less fortunate. But to repeat, that still compares very favorably with the $325,000 which is often cited as a lifetime cost. Unfortunately, that just isn't enough, the Chinese will have to wait for repayment. This book was not written to propose a change in Medicare, but in writing it I do not see how we get out of our healthcare mess without addressing Medicare. If politicians can be persuaded of that, at least we will no longer need to invent reasons for urgency.
The Cost of Pre-funding Medicare. Rates of 10% compound income return would reduce the required contribution to $100 per year from age 25 to 65, but if the income were only 2% would require $700 contributed per year, and at 5% would require $300 per year. Remember, we are here only talking of funding Medicare, as a tangible national example, Obviously, a higher return would provide affordability to many more people than lesser returns. Let's take the issues separately, but don't take these preliminary numbers too literally. They are mainly intended to alert the reader to the enormous power of compound interest. Let's go forward with some equally amazing investment discoveries which are more recent, and vindicated less by logic than empirical results.
The Coming End to Ink Blots.
Medicare spends about $56 billion a year. The National Institutes of Health spends $30 billion, rising at a rate of 3% a year, or about the national inflation rate. Full disclosure: I was an employee of the NIH for two years, and think highly of the place. The Director of NIH at that time was James Shannon, who had been in charge of the New York division of Goldwater Hospital on Welfare Island in New York harbor, while I was a medical student on the Columbia division of the same hospital. I didn't meet Shannon in New York, but I heard everyone who knew him, speak with awe. The big news when I was a student was that he had accepted a job in the commercial drug industry, which was deemed a degrading sell-out. There was much cluck-clucking, which medical students intended as giving the drug industry a not-so-subtle warning from us their betters, that we would never, ever, consider such a sell-out to the money-changers. Shannon persisted in the drug industry for a few years and then turned up as Director of the NIH.
He never confided his goals to me, but it was widely reported he only accepted the political job, on condition Congress would absolutely never introduce political goals into the research process. No scientist would ever be forced to study a project because some Congressman's wife had a disease, or thought she did. Grants would absolutely never be awarded a geopolitical bias, and the consideration of favoring a particular drug company's research leads would absolutely never be tolerated. And indeed, the NIH was pretty much run on such starchy principles for at least fifteen years. By the end of that period, its reputation was immense.
During that period, the grounds of the NIH in Bethesda grew from an expansive, golf course-like, estate with only a billion or so budget, into an extensive little city of research buildings, with traffic lights and uniformed policemen to direct traffic. And, a $30 billion budget whose composition is not easy to come by, but only 10% of which is reported to be spent in-house. The greatest proportion of the budget is now dispensed to far-flung academia in the form of grants. The emphasis of current research can be inferred from its list of specified targets, which concentrate on cancer, antibiotic resistance, brain disorders, and Alzheimer's disease. A few years ago, HIV/AIDS was targeted, and so successfully, it dropped off the targeted list. Let me tell you a trade secret about research: most proposed research is a waste of money, accomplishing little. The art of selecting which proposal to fund is, therefore, a difficult one, but there is no doubt some scientists are better at both selecting it and doing it than others; only about 20% of grant requests are selected to be funded. How many potential Nobel prizes are in the rejected 80% is unknown, but there must be some.
Successful researchers quite often prove to be high-stakes gamblers, and some people seem to have better hunches than others. Some people just don't have the right temperament, but it's pretty hard to identify just what that is. On the other hand, some people only flourish when surrounded by others with the "right stuff", while others work best when left alone in solitude. I hate to say it, but a few people also excel at the fine art of stealing the ideas of others with less drive and energy. Some people burn out at an early age, others keep producing good work past the retirement age. All in all, it's probably remarkable that 20% who are selected, produce so much. But since so much time and money comes to nothing, the environment is a dangerous one, rather glibly leading to a conversational conclusion that someone else should have got the grant. On the other hand, we have made it possible to become a billionaire before you are thirty, so some real pirates get attracted to research. Observations of this general sort lead me to believe, if we should suddenly get the announcement of a cheap effective cure for cancer, there would immediately be a chorus of voices, demanding next year's NIH budget be cut in half. And the frustrating thing would be, no one could be entirely sure that was wrong.
That summarizes one way this promenade could end; not with a whimper, but a bang. A famous success, with prizes and speeches and even statues -- followed by a steep budget cut. The other way would be the slow exhaustion of contemporary protein chemistry, followed by nothing which could match it for glamor. For the past twenty years, the five hundred peer-selected papers chosen for presentation at prestigious three-day research seminars-- have overwhelmingly shown slides displaying ink blots.
 What will follow protein chemistry?
|
Let me explain. Until twenty years ago, most successful new drugs and biochemical discoveries have involved small molecules. It seemed clear most of the remaining secrets were hidden in the coils and recesses of protein chemistry, but protein chemistry was just too hard to do quickly. We spent a billion dollars exploring the human genome, only to find it explained no more than 2% of disease. So we doubted the research and repeated it, spending another billion to no avail. Almost all these experiments involved chromatography, so almost all of the experiments showed their results as blots on a piece of paper, rather uniformly resembling ink blots in a psychiatric personality test. Either a novel bulge appeared, or two sets of bulges (amazingly) showed no difference in bulges. After twenty years of watching slides showing ink blots, I retired from the scene and started clinical practice and writing books.
When a new miracle is discovered, its particular ink blot will probably look a lot like other ink blots, so why go to so many meetings. It looks to me as though ink blots of mitochondria or ink blots of Golgi bodies will demonstrate the new miracle, or else every conceivable ink blot will be performed on those particles, and nothing striking will turn up. Somewhere, some cure for cancer and Alzheimer's disease will exist, but its effect need not be demonstrated in its protein chromatography. But at least until the cure is found, or every imaginable ink blot has been photographed, the ink blot parade will continue, and then it will gradually wear out. At least to me, it seems incredible the present approach can continue much longer. What I'm saying is we need a new cure fast, or else we need a new experimental tool.
There's another danger I haven't mentioned. Like the cost overruns of clinical practice, the best place to direct the accountants who count the beans of research grants is the indirect overhead. It's characteristic for grants to come as direct and indirect costs, and the indirect costs are approximately 70% of the direct ones. Research institutes who operate on a for-profit basis all agree that 70% is if anything far too little, and the non-profits nod in agreement. It sure doesn't feel appropriate to give the administration of academia a 70% cushion for the library, air conditioning, etc, necessary to sustain these billions of dollars for research. Sooner or later, someone will apply the old government technique for dealing with an expense account you don't understand: Cut its indirect overhead budget 10% and see what happens. If nothing bad seems to happen, cut it 10% more. And so forth until you have starved it to death, forced it to commit suicide, or identified its legitimacy. No, don't do it. Either you do research or you don't, and if you want the right answer you must do it the right way. But if Shannon's rules are egregiously flouted, disaster will more likely be the consequence.
After the Second World War, America decided to do what only America could afford to do. We decided to spend astonishing amounts of money, curing disease. The unproven theory for gambling this enormous fortune was -- in the long run, it would cost less than subsidizing everybody to be treated in old-fashioned ways. And it really has been shown to work. In 1950 we had 500,000 state and municipal hospital beds for a mental disorder. Today, we only have about 40,000. Can you imagine how much money that has saved? Or the 100,000 beds for tuberculosis? Or the fifty thousand beds for polio? What is left to do is treat about five diseases of late-life onset, and there is a reasonable chance to do it in the next two decades. Just double those numbers, and you still have a bargain. Yes, it's true we have not resorted to expedients every other civilized nation in the world has resorted to, and yes it is true the medical profession will never be the same. But this is America, right? We plan to give it away to all those other civilized nations, mostly free, to foreigners who might never dream of doing the same for us. That's part of the overachieving American character, too.
Methods in the Madness
Even today, many people are uncomfortable about psychiatric illness in their family. In the Nineteenth century, this feeling was much more pronounced, so wealthy families sought out luxurious psychiatric hospitals where wealthy patients were kept out of sight. Rich families also sought out psychiatrists of their own class to be in charge; not only keeping matters out of sight, but they were also likely to be discreet in their outside discussions. Sigmund Freud wrote a whole book to the effect that getting richer brings on mental disorders.
Snake Pits. By contrast, saying institutions for indigent psychiatric patients were once substandard, is quite an understatement. Indigent cost to society must have been a considerable burden fifty years ago, with over 500,000 licensed beds nationally in 1955, even though society is a notorious pinch-penny with indigents in any era. When Thorazine made its appearance as the first really effective antipsychotic drug in 1953, it was prematurely followed in 1955 by President Kennedy announcing a plan for cutting the number of inpatient psychiatric beds by half. This goal was quickly and drastically achieved, cutting beds in "psychiatric snake-pits" to 40,000 by the year 2000. To a certain degree, however, we have simply moved mental patients from snake pits into prisons at a higher cost. In all this turmoil, upper-class institutions at first were much less affected.
Rest Cures. During the last half of the Nineteenth century, psychiatry itself had become a distinctly upper-class specialty. To what extent this class isolation was a cause of the profession's later troubles is hard to say, but it probably was a factor. In the early Twentieth century, this social situation was upset by a pell-mell rush of enthusiasm by psychiatrists to follow the teachings of the Austrian doctor, Sigmund Freud, introducing psychoanalytic methods of treatment at a significantly higher cost.
The Analysts. For a while, no academic psychiatrist could expect promotion unless he was an analyst, and this attitude spread out into the practicing profession, too. But its time was brief; psychiatric drugs starting with Thorazine swept the scene. Soon, anybody with a fountain pen and a prescription pad could be a psychiatrist; seven years of specialist training were no longer required. Hope was soon raised that psychosis would next follow the example of tuberculosis, first with effective patient treatment, and evolving later into the closing of highly expensive specialty hospitals.
Fads and Fashions. Many of these changes did result in general savings. In each step in the therapeutic process, the leadership of the specialty was thrown into disarray by radically new treatments requiring many years of re-training to master. Brash young physicians displaced the experienced older ones; the older ones never quite got it, and the younger ones never quite got over it. The ultimate outcome of this uproar was what you can now see in the center of many cities: "homeless" people living in rags on steam grates, because there are few psychiatric hospitals for chronic indigents, anymore. And basically, no good ways to define and reimburse psychiatrists.
Trust Fund Babies. The effect on upper-class "trust fund baby" patients are harder to notice, but inevitably young people of any class will outlive their parents, and often outlive the trust fund as well. What did further disrupt the vulnerable changing treatment scene, was the introduction of large numbers of addicts to recreational drugs, which tended to affect those who could afford the cost, sooner than those who could not. The system was disrupted from the top down at first, and then it became a regular feature of the youth scene for young people of any social class. The closing of upper-class inpatient facilities is particularly disruptive when the signs of addiction first make their appearance, encountering a distraught family having no familiarity with what to expect, or whatever treatment facilities are available, however abundant or scarce, good or bad.
Non-Relatedness of Psychiatric Severity to Hospitalization. There is an old saying in psychiatric circles: "People aren't hospitalized because they have psychiatric conditions. They are hospitalized because they are bothering somebody." Because psychiatry at the time was regarded as a state responsibility rather than a federal one, there were enormous disparities in treatment adequacy. It should be recognized that interstate disparities are part of the force behind the move to federalize. It's actually one of the pressures by interest groups to upgrade spending in poor states, which in time will correct the imbalances between states which James Madison envisioned as a driving force for change. Because California was particularly generous, it was punished by attracting large numbers of psychiatric patients. The response of neighboring states was quite the opposite; they closed what few state facilities survived, and the patients drifted to California. In both cases, local politicians found something to boast about, and their opponents found something to complain about.
The Rather Drastic Philadelphia Method. One place they couldn't quite boast of, was the relative absence of drug addiction in Philadelphia, for quite a long time. The local Mafia chieftain declared anyone selling drugs in his territory wouldn't even live to regret it. His methods were easy to notice, and for a number of years, Philadelphia was "clean". The proof that this was the cause was easily demonstrated by an upsurge in drug addicts soon after a neighboring Mafia tribe "bumped him off".
Cycles. One psychiatric social worker looked on the scene with disgust and offered this explanation. "These psychiatric fads come and go, and they always will. We see patients on steam grates and we say they must be hospitalized to get better treatment. After a while, we call those hospitals 'snake pits' and then say the patients should be integrated back into society." That was her view of it, and everybody else except me may be right. But I feel blame for the present mess is partly shared among many forces: To over-enthusiasm for a new treatment, partly stimulated by a desire to save a lot of public money which encourages a suspension of disbelief, and adverse decisions made by public officials, with other priorities being pressed upon them. Increasing longevity caused adverse de-selection to emerge from state governments funding nursing homes for the indigent elderly, for example. We, unfortunately, do need some bad examples to trigger improvement, but too many of them will overwhelm a government into seeing no way out except hunkering down.
|
John Kennedy closed the Snake Pits. Who will close the steam grates?
|
The End of the Dream Economy The shift in American international trade payments from positive to negative, which took place around 1966 reminded us we weren't as rich as we thought we were, while the recreational drug scene shifted attention to different clients for psychiatric care. The two movements have a certain amount in common. In other words, the nation shifted charitable priorities away from chronic psychosis. It was a result of a whole host of pressures independent of the inclinations of the psychiatric patients and psychiatric doctors. Psychiatry is an extreme case because the patients always surrender a certain amount of autonomy. But it is a warning to everyone that it is dangerous to surrender the remaining control of your fate to people who have limited incentive to look out for your interests. I have been convinced by the arguments that the closing of high-class, high-cost psychiatric hospitals for the rich, did not start this trend. But when wealthy powerful people cannot find an institution they are perfectly willing to pay for, (as is now true in the case of chronic adult psychosis), it is a remarkable development. And it raises a question how much further this trend might go.
That Dratted DRG, Again. Hospital payment by diagnosis makes a reasonable assumption that hospitalization costs are somehow related to the diagnosis, but while that's often true it is seldom precise. The less the precision of the diagnosis, the less precision it will have in determining the cost. When it reaches the extreme of two million diagnosis categories lumped into two hundred diagnosis-related groups, it is inevitable that some diagnoses are unrelated to the mean, in the services they require. Furthermore, some patients with identical diagnoses have complications involving fresh departures in treatment. Or they will be affected by unusual manifestations of illness requiring them to run up special costs. Variations are sometimes enough to bankrupt a family, sometimes they are so extreme they bankrupt a hospital. Bigger hospitals find the law of large numbers often takes care of the problem, but combined with local environmental or politician problems, sometimes even a very big hospital can be shaken by an epidemic.
Outliers. That is, "outliers" will be found, where the DRG payment is not even remotely appropriate. But the main reason DRG is adequate for most hospitals is the payer wills it to be so, and the hospital then devises some workaround which the payer chooses not to notice. In the case of psychiatry, whole disciplines of illness are occasionally found to have little association between diagnosis and cost of treatment. No matter what his diagnosis may be, a person who thinks he is Napoleon can stay in a hospital for one day, or his whole life, depending on circumstances. So the DRG law at first provided outliers should be paid the old way, by itemized services, for psychiatry and other outliers. That was once the way we paid for all hospitalizations, so why wouldn't it continue to suffice for outliers to be treated as exceptions? The flaw in this reasoning, of course, was prices of individual services were discretionary, and pretty much limited to exceptional cases, plus psychiatry. That led to two clusters of prices in the chargemaster lists, one for outliers in conventional general hospitals, and a second one for psychiatric hospitals. Either way, it seemed a good precaution to set the prices high.
Strained State Budgets. In government circles, there is a standard sort of behavior, usually tolerated as a normal part of the negotiations. To get a bill passed in Congress without delay, technical adjustments can come later. In retrospect, it is unclear whether readjustments were bungled or whether the problem was unsolvable; the payers' fuse did seem to have been rather short. In any event, when the number of psychiatric beds fell toward 40,000 from an earlier 500,000, many gave up and went out of business.
Windfall, Then Disaster. And so it came about in those days that general hospitals were chafed by low prices set for DRG, while psychiatric hospitals were effectively given blank checks, and prospered notoriously. A movement was even under discussion, to move non-psychiatric patients into psychiatric hospitals, but events headed this off. It took some time for all of this to work through the system, but eventually, three situations survived. Prices were drastically reduced for psychiatric DRGs, to the point where hospitals of this type were driven out of business. Secondly, the DRG system proved to be a highly efficient rationing system, eventually moving toward a pattern of 2% profit margins within a 2% national inflation rate. And thirdly, the Chargemaster rates remained high, discouraging hospitalization and encouraging outpatients. One by one, famous established psychiatric facilities closed their doors, to the point where indigent patients are found on steam grates, and some affluent ones, too.
The Veterans Administration. As a matter of fact, there is one place left to treat inpatient psychiatric patients -- the Veteran's Administration hospital system, if you can find an empty bed. The bed capacity is small, but at least they do not segregate by the ability to pay. Social workers desperately looking for somewhere to place psychiatric patients, quickly learned to ask the most important question first: "Have you ever been a veteran?" If so, regardless of income, but somewhat dependent on locality, it is one lucky patient. All of the inadequacies of the VA informal rationing system soon come to light, however; the long waiting lists, the remoteness of the location, the recreational drug epidemic, the demoralized staff. With thousands of patients on their outpatient waiting lists, it was just not possible to cover all this up, to say nothing of fixing it before newspaper reporters arrive. Newsmedia has generally been ardent supporters of Obamacare and government-run medical care, but even they have been chastened by the example of it encountered in the Veteran's Administration. Let me help them with their outrage. The Armed Forces themselves will have nothing to do with VA, running an independent system of military hospitals for active-duty military, and politicians they wish to court. When President Eisenhower had a heart attack, he went to Walter Reed Hospital, Franklin Roosevelt and a host of other presidents went to the Naval Hospital in Bethesda. Even Senator Joe McCarthy died in the Naval Hospital, where the first thing a VIP says is, "No one must know I am here." That's the motto of military hospitals. But if any important government official is ever cared for in a Veteran's Hospital, by contrast, it will be very big news, indeed.
Academia Gets Its Share of Blame
In 1910, Abraham Flexner produced a book-long report on reforming medical education, under the sponsorship of the American Medical Association and the funding of the Carnegie Institution. The report was a product of the progressive era of reform which ended the Gilded Age, and can fairly be described as the handbook of a revolution in American medicine. The book had an impact on closing 106 of the 160 medical schools in the United States and Canada. To Flexner that was a disappointment; he thought only 31 were worth saving. To be a good doctor, in his opinion, required between six and eight years of scientific training. The quality of student, as well as the quality of schools, was important, justifying a vast shrinkage of the student body. He liked research and unleashed an avalanche of medical research which subsequently transformed medical care in a hundred ways.
Having said all that, it must be acknowledged, Abe Flexner had been educated in Germany, and his efforts mainly crystallized the transfer of German academic medicine to America, and from here onward to the world. What's being acknowledged is that for a time, German Medicine was far ahead of us, in an environment where we aspired to be the leaders.
Flexner was a charismatic figure, supported by American Medical Association reports from its Council of Medical Education, the wealth of the Carnegie Institution, and the enormous resources of the Rockefeller Foundation. American academic medicine pointed to the example of the Johns Hopkins Medical School, formed before the ferment of pre-World War I, and now being given prominence by Teddy Roosevelt, Woodrow Wilson and the rest of the muckraking era who aspired to replace the Gilded Age with something better. America was aching to take charge of something, had great gobs of philanthropic money at its disposal, and the wind in its sails. Abraham Flexner was a towering figure, all right, but he was not a physician, an academic, or a scientist. He was more the agent of revolution than its originator, ending up as the patron saint of several political factions, individually fighting academic wars with each other. He was, in short, a rain-maker.
|
Abe Flexner, the Rainmaker
|
| German Model for Medical Schools |
Abe Flexner and his book aimed to reduce the number of medical schools from 160 to 31, demanding the survivors look like German schools. This was not so strange; like Japan and China today competing with America, Flexner wanted to compete with Germany more than he wanted to worship it. The students of his dreams were required to be college graduates, the curriculum was to be four years along with two years of science followed by two years of hands-on learning. If the school could afford it, the professors would be on a full-time salary, free of any need to practice in order to make a living. On this last point, many begs to differ, arguing you have to get on a boat to learn how to sail one. There were many echoes of the ferment to come, in the upheavals of the 1960s, and the Humboldt's University of Berlin was the source of quite a few, in both cases.
Immediately there arose a town-and-gown competition. The gown group had the point they could afford the time to do some research. The town group had the point you couldn't teach doctors if you weren't one, yourself. The distinction is probably best understood by comparing medical students with law students. Both were originally taught by practitioners; schools were late arrivals. Many lawyers have remarked that a law school graduate now knows almost nothing about the practice of law until he joins a firm which teaches it to him. A medical student (post-Flexner) can do a pretty good job with most medical problems, the day he graduates. The practicing physicians have retreated into specialty training; a doctor has trouble becoming a specialist if he didn't have the right residency. The rest of the awe-inspiring march of medical progress in the Twentieth century, is the consequence of pouring unbelievable amounts of money into the system, thereby attracting a glittering array of talented medical students. Some of the talents are unbelievable. My own medical school, as an example, has a symphony orchestra made up of students in their spare time, performing on a truly professional level for their own amusement. In a sense, all of this was due to Flexner. In another sense, Flexner himself had little to do with originating it.
Now, forget the yellow journalism, or muckraking, quality of what I am about to relate. A book was recently published relating that a particular medical school was able to support its operations without touching a penny of medical student tuition for ten consecutive years. Instead, the tuition money was transferred to the University's undergraduate schools, and the medical school subsisted on research and other funds. The undergraduates continue to protest about rich doctors, while the medical students complain about going a hundred thousand into debt -- to pay their tuition. But forget that part. The most undesirable situation it reflects is that for ten years, the school was totally able to exclude any parent and student influence in an area that unfortunately has a growing power over events, the school's finances. If the students, families, and alumni of a university have no power to influence its decisions, who do have such power?
Healthcare, A Much Simplified Overview
Let me say at the beginning, what could be repeated in a summary: The present healthcare dilemma has three interlocked parts, scientific, financial, and political. The scientific component is capsulized by three symbolic life expectancies: in 1900: age 47, today: age 83, and fifty years from now: age 100. We're living a lot longer, and soon expect the population to divide into thirds (one third getting educated, one third retired, and one third working to support the whole population. It probably won't work very well. Most health reforms amount to finding some way to shift income from the working third to the other two thirds.
The main scientific problem in the past was to avoid dying too young. But the problem in the far future will be living too long, running out of savings. Right now we can imagine having both problems, and few can guess which problem to fear. Maybe there is enough money for one of those two life terminations, but we don't have enough money for both of them, for everyone. We would have to give up something else, like national defense. Let's try to use the same money twice, if we can.
Finance. The payment systems need to be more interchangeable for alternative uses. But be careful. This could seemingly lead to merging Medicare and Social Security (someday) into one interchangeable program. Interchangeability of funds might plausibly seek to be at the family level instead of over-reaching to the level of demographic groups of whole thirds of the population. We do need to devise ways to transfer from one stage of a person's life to another, Saving for a Rainy Day, as it were. Some solutions will inevitably turn into problems. Proposals to integrate all health care into one vertical single-payer medical system would likely clash with more useful integration of Medicare and Social Security. These arguments can possibly wait for a later time, but only if we recognize they remain undecided. Generally speaking, they translate into recognizing that it is easier to shift money than people. Governments regard such as shifting with indifference, but we train children from birth to be possessive about their own money. And we elect politicians to see the difference.
Both the insurance spread-the-risk approach and the government pooling process skirt the difficulty there is not enough money to cover both possibilities for everyone. Either to borrow or insure postpones repayment for a while, that's about all. Meanwhile, healthcare costs are subject to more sudden changes in greater ranges than the economy as a whole.
Finally, let's see if we can put these shifts to work, and get some extra money from investment income, with compound interest working its magic over the whole expanse.
Politics. Meanwhile, we move toward a time when voters who earn money aren't sick, and the sick voters don't earn money. But they all have a vote. Already, we conduct transfers of money on a scale people may rebel against. It must become their own money, in their own accounts, spent later on themselves -- rather than forced transfers between demographic groups. At most, we might try extending that to the family unit, and even that should be kept as voluntary as possible.
|
Constitutional equal justice tends to make political solutions resemble one-size fits all.
|
So that's the general nature of our problems. Healthcare does become less expensive in the long run, even though more expensive in the short run. And through recent advances of financial management, Health Savings Accounts can generate surprising amounts of extra money on their own, overall helping with the other problems. The abstruse issue of inflation also arises here, where you might not expect it, because if trillions of dollars eventually migrate into passive investments through Health Savings Accounts, the elderly will hold shareholder voting rights they would be unwilling to surrender. The course of further inflation, the main concern of the elderly, would shift toward the hands of savers, away from borrowers. Unfortunately, what the proper balance is, isn't yet clear.
Health Savings Account, Classical Version
Well, it's all called the Health Savings Account, Classical Version. John McClaughry and I invented it as the Medical Savings Account in 1981, and we both consider it to be on the short list of things we want to be remembered for. The central feature of these accounts is they pay your medical bills with a special debit card, and they get every tax deduction we could find, except one.
Proposal 79: The law says they must be linked to catastrophic health insurance but are forbidden to pay the premium. This omission should be repaired, by changing the law or regulation; with this change, they would become superior to the discriminatory employer-based tax abatement discussed below, because that could extend the income tax relief equally to everyone, regardless of employer.Since almost everyone would agree, why not adopt it and get on to other business? The essence of the whole remaining debate is how to pay for comparatively low-cost care, especially for people with low incomes, neither impoverished nor affluent. Some people will have to be subsidized, and the rest are mostly able to save enough to pay their medical bills. We can ease things for borderline cases with tax deductions, and the rest is mostly a routine drawing of lines. The concept is discussed in greater detail in later sections of this book. Right now, all it immediately needs is a revision of those two regulations of the Affordable Care Act.
|
An HSA should be overfunded. Any surplus can be used as a retirement fund.
|
Instead of confronting, let's out-bid them, with a Lifecycle Health Savings Account (L-HSA). The dreams of the future usually include legalizing a few radical advancements which become normal parts of the landscape in time. By adding passive investing and the power of compound interest, the HSA becomes a Lifecycle (multi-year) Health Savings Account, providing the balance can be legally carried forward for a lifetime or even longer. The out-bidding already takes the form of adding a new revenue source, not by reducing the benefits.
Proposal 80:At this point, it probably would be wise to add some legislation clarifying the ground rules since several professions would have to cooperate in allowing a new line of business for whole-life insurance.In effect, it could become a do-it-yourself whole-life insurance company, which pays for health insurance instead of funerals. I'd love to see the whole-life insurance companies adopt the idea, which comes close to imitating their business model. There's no reason why stockbrokers and/or investment managers couldn't do much the same thing in competition--it all depends on what the enabling statutes happen to enable. Whole-life insurers could manage the money professionally and would create much-needed competition for old-style health insurance companies, now operating on the "use it or lose it" principle. The large amounts of money the savings account approach would generate, seemingly almost discredit the idea as exaggerated; we'll, therefore, let the reader do some of the math. Perhaps you do need to dangle astonishing incentives to get people away from the something-for-nothing term-insurance approach which is now threatening to shoot itself in the foot. The full transition is a fifty-year project, but long-term progress usually doesn't seem so long looking back on it, and it gives everybody a chance to claim some credit. Remember, it's only long-term lack of progress you really need to fear.
Let's not quibble. It might even be legally or financially possible to adopt one approach, year by year, or the other, spread over a life cycle; and hurry it all up by making it into a mandatory monopoly. But it is inconceivable for half of a whole unwilling country to tolerate a mandatory health system they widely resent. However, it seems possible to implement parts of both approaches voluntarily right now, without major disadvantages except extra cost. You can do that, or you can read the Lifecycle-HSA as just an alternative proposal to consider. The main dream offered here prefers to cut average lifetime health costs in half ($175,000) but might be expanded to full lifetime coverage of $350,000. Or reduced by individual vendors to some more affordable fraction, such as by a reduction of average costs by only a quarter ($85,000) or a tenth ($35,000). To do this requires some legislation, but $35,000 times 300 million population is scarcely trivial. Even Bill Gates isn't worth half of that.
Over-investment in Health Savings Accounts -- The Retirement Alternative. Because it's a new program, with financing uncertainties, we advise everyone with an HSA to consider overfunding it as a precaution. If you could use resulting surpluses for something else, it should reduce the hesitation to overfund. One alternative is to use Medicare exclusively after age 66 and transfer the surplus to your IRA retirement fund. That's legal and essentially cost-free. Consider all the foregoing to be a short introductory look at the theory of Health Savings Accounts; we next display an actual example, using actual numbers which just came across our desk from a large and local insurer. To keep it simple, we assume the client had no serious illnesses at all and paid for minor illnesses out of pocket. That will rarely be the actual case, but its use here is to illustrate the safety of over-investing in the product in order to fund a healthy retirement with the overflow. Although it will provoke extensive discussion later, we assume the deposits into the HSA will earn 6% compound interest.Read on, to see how the passage of a few relatively harmless laws, might offer poor people a way to get a rich man's health care. Getting rich in this sense amounts to funding your medical bills in a radically new way, but it does not imply any change in the kind of care you receive. Otherwise, it certainly will cost somebody $350,000 per average lifetime, as calculated by Michigan Blue Cross, verified by Medicare.Example One. Assume an average employee aged 21 receives $750 yearly from the employer and deposits $3300 into the HSA account, adding the personal supplement permitted of $2600 extra, until age 66. Deposits earn 6% compounded. After age 66, income tax is paid and the remainder rolled over into an IRA. Subsequent to retirement, the minimum retirement is paid annually, while the balance continues to earn 6% after tax.
Example Two. Assume an average employee aged 21 receives $750 yearly from the employer and deposits $3300 into the HSA account, adding the full supplement permitted of $2600 extra, until age 26 when he/she retires to get married. Deposits earn 6% compounded. After age 66, income tax is paid and the remainder rolled over into an IRA. Subsequent to retirement, the minimum retirement is paid annually, while the balance continues to earn 6% after tax.
Example Three. Assume an average employee aged 61 receives $750 yearly from the employer and deposits $3300 in the HSA account, adding the full supplement permitted of $2600 extra, until age 66. Deposits earn 6% compounded. After age 66, income tax is paid and the remainder rolled over into an IRA. Subsequent to retirement, the minimum retirement is paid annually, while the balance continues to earn 6% after tax.
You pay income taxes when you make the transfer to the IRA and on IRA withdrawals. Most of the investment return is tax-sheltered, however. Assuming 6% tax-free earnings and a 15% blended income tax rate, your investment of $132,000 would be worth $698,000 pre-tax, and $482,000 after income tax, at age 66. At that point, suppose you pay your HSA tax and re-invest the proceeds in an IRA. Assuming a life expectancy of 88 years at that point, you would leave $1,638,000 when you die, or $1,493,300 after income tax. That's assuming you actually spend nothing out of the account, but since it's a surplus, it also represents how much you could have spent without affecting the retirement. Be careful of this point, however, because the age at which you spend it will markedly affect the outcome. That's unlikely to be sure, but if you consume it all you have paid for all your lifetime healthcare, as best we can estimate it. The point of this calculation is not to make everyone rich, but to demonstrate the financial power of the approach. With a little management, it easily covers the actuarily projected lifetime cost of health care of $350,000 per person and leaves enough slack to be comfortable about it. In case anyone questions the ability of a poor person to save $3300 per year, lifetime savings would amount to $440, per dollar invested at the beginning. That's too attractive to brush aside on the grounds you might never be able to do it, even for brief periods. It's quite honest and legal, starting today, but an additional reason to show it here is to demonstrate how little anyone has to lose by investigating it today. In fact, over 12 million people have already started such arrangements. If the rudiments of the plan are that attractive, just imagine what a few legal clarifications could accomplish.
What's the secret? Instead of paying 10-15% to service your bills, you earn 5-6% interest by pre-paying them. The swing between those two is the difference between comfort and worry. There are other swings, but that's the main one.
But it doesn't imply that no one will be worse off. There are 1,500,000 employees of health insurance companies, but there are only 800,000 licensed physicians. Doesn't it seem excessive that for every doctor you see, there are two insurance employees handling the bills? It's probably conservative to guess that every doctor hires another insurance employee, and every pharmacy hires several. Every hospital probably hires a hundred, and every laboratory or x-ray laboratory hires more; it just seems to go on, and on. Five or six clerical insurance employees per doctor don't seem like a wild guess since a lot of doctors aren't actually practicing. Those who want to continue with this sort of thing can pay for it. Surely, the rest of us deserve some other choice.
Because this book is written during a confusing period where both Health Savings Accounts and Obamacare have been enacted, but the position of the Supreme Court has not been clarified, nor the regulations coordinated, -- what an individual should do is highly specialized to his age and situation. We cannot predict what upsets the November 2016 elections will bring, or what the result of their reconciliation will be.
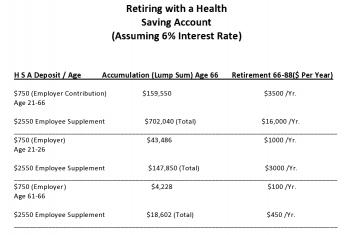
Essentially, this particular health plan offers its groups the choice between an Obamacare with, and Obamacare without, a Health Savings Account. Into the HSA version, the employer effectively contributes $750 but gets a lower premium from raising the deductible. Never mind the economic argument that the cost ultimately comes from the paycheck; most people will say it feels like a gift. The compound interest in the future dictates that every young person should enroll in an HSA at the earliest possible moment, and supplement the employer contribution to the limit of his ability. A young lady, for example, should go to work immediately after graduation from school, even though she plans to drop out of employment when she gets married. An older employee, on the other hand, is far less expensive to the employer than he appears to be if the retirement benefits are considered. If a person reaches age 61 without provision for retirement, there is little to be done about it.
Commentary. The high deductible portion of Obamacare serves as the catastrophic link required by the HSA enabling act. The employee is annually allowed to contribute up to $2600 to the savings account additionally. (There's a family plan, with different contribution rates.) There's no way to know how long an employee will remain with the same employer, or whether a new employer would continue the same coverage; but at least an individual's HSA has been established, provided you go ahead and do it. If an employee starts this plan at age 21 and continues it to age 66, the outside potential is to transfer $159,550 to a regular IRA at age 66, assuming 6% interest, but no personal supplement, and only out-of-pocket health withdrawals. Never mind theoretical economists; it's a very good deal, and it almost feels free.
But don't get carried away; you can't spend the money twice. The example shows the financial benefit of being lucky with your health; it could also be said to reflect the cost of being unlucky or careless if your health is bad. Its success depends on young healthy people saving their money and generating extra income before they become older people getting sick and having to spend their savings. Meanwhile, scientific progress will exaggerate both the savings and the attained age before the spending begins. In the past century, that added thirty years of longevity, and hence thirty years of compound interest. If some scientific miracle should add more cost than longevity, a mid-course correction might have to be applied. Some future generation might have to answer the question, "Didn't you want to live an extra ten or twenty years?" I would have to say the medical profession has been pretty good with this juggling act in the past when we were in control of it; one of the ponderable dangers of upsetting the system is the danger of upsetting this balance in the future if control of the payment system falls into other hands.
The foregoing should suffice as a summary of this book's proposal. The next section describes some of the other serious problems with healthcare and how they got that way in the past century. Sometimes more funding will help these problems, sometimes it won't. The section following that will describe some of the nuts and bolts of Health Savings Accounts, and sketch in some more elaborate variations which might be possible. By far the most important new concept to be thoroughly absorbed is the approaching wrestling match between the health industry and its finance partner. Recall that we have estimated the Health Savings Accounts would earn 6% compound interest income during the long lifecycle between healthy youth and sickly elderly. Actually, that is likely to be an under-estimate.
Stock Market Issues.For the past century, the foremost student of the matter, Roger Ibottson, has shown the equity stock market has averaged about an 11-12.7% total return. Investors in index funds of the same stock have received about 5%. Three percent of this attrition is ascribed to inflation, leaving another three percent unaccounted for. Money managers use the residual 3% for expenses and to buy bonds as a safety measure. While the law of large numbers will ordinarily account for the ordinary jiggles of the stock market, there is some other cycle at work causing a severe crash every 25-30 years. It is thought wise to set aside 25-40% of the portfolio in bonds to ride out such "black swan" storms. This, in essence, is the central issue of the third section. The final section describes other variations of the Health Savings Account concept, particularly as it involves transitions from other funding mechanisms.
The Wedding of Computers and Medicine: First Annual Fuller G. Sherman Lecture George Ross. Fisher, M.D.
The Wedding of Computers and Medicine:
First Annual Fuller G. Sherman Lecture
George Ross. Fisher, M.D.
October 1, 1987
Fuller G. Sherman, M.D. was born August 15, 1894, graduated with academic distinction from Jefferson Medical College in the class of 19** with his second doctorate degree, was certified by the American Board of Internal Medicine, practiced for many years in Woodbury New Jersey, and retired from practice in 19** to live in his native state of Maine.
The competitive strengths of Dr. Sherman’s character have actually been easier to see during the so-far thirty years of his retirement from medicine. Past the age of 90, he attended Bowdoin College, taking courses in Shakespeare and geology, plays par golf, holds a Masters’ certificate in tournament bridge, is a distinguished cabinet maker, and does creditable work in oil painting. Two notable achievements were once, on the day after his graduation, to have flattened an Associate Dean of this Medical School with a single punch; and secondly to have consistently outperformed the Dow Jones Industrial Average on the New York Stock Exchange. Because of the latter, of course, he was able to endow the lectureship we inaugurate today. In both of these adventures, he illustrated the truism that in life, everything is a matter of timing.
He has been my teacher, employer, referring physician, and friend. He is now my patient, allowing me to judge he has as good a chance as any of us to live another thirteen years. If he does, he will have the almost unheard-of opportunity to observe the practice of medicine in three different centuries. There can be little doubt he will study the next century harder than any of us, as his patronage of computer science demonstrates today.
My subject has three parts: yesterday, today, and tomorrow. The exhilarating nature of the computer world lies in only a little yesterday, a little of today, and a great deal of tomorrow. For our purposes, yesterday began about thirty-five years ago when the Chairman of the International Business Machines Corporation, Thomas Watson, made the decision to gamble the whole future of his successful typewriter and tabular company on mass-producing computers. There were then only a few dozen of those machines in existence, mostly owned by the military. They cost millions and were expensive to operate. Typically, a bushel of worn-out vacuum tubes were replaced every day. You could walk around inside them without stooping over. By 1960, IBM was selling a thousand of these machines a month to large corporations for about $ 4 million apiece. Technology in 1960 had greatly reduced the maintenance cost, but the University of Pennsylvania still had to rent them for $300 an hour at the academic rate. Machines of equal power can today be purchased for a thousand dollars, and are the size of typewriters. I own five of them; there are about twelve million others in existence, up from nine million last year. One surgeon recently told me he bought one of the best, about a year ago, but had not yet had time to take it out of the box. The cost of these miraculous machines was thus trivialized in a single generation, and each year the Sunday supplements have promised us that within two years, five at most, such things as a medical diagnosis would be relegated to computers. It never happened, of course, because science fiction writers had not heard Dr. Sherman’s professor Thomas McCrea (Dr. Maddrey’s predecessor by seven) repeatedly intone that “most diagnoses are missed because the doctor didn’t look not because he didn’t knowâ€. The problem of diagnosis today, as then, is one of information gathering, not information manipulation.
A generalization can be offered. If you hear a prediction about computers, be fairly certain it will never happen, unless it already exists. So many brilliant minds are at work, with financial rewards providing unlimited resources, that the immediately achievable is achieved immediately. Mr. William Gates, a self-made billionaire at the age of 31, illustrates how among people who are successful in this field, there is no motivation for idle chatter.
The amazing drop in the cost of computers has made it possible to have a personal computer that is those dedicated to use by a single person. Personal, or stand-alone computers, can now do almost everything a large main-frame computer can do except cope with multitudes of users. But, having only a single master, they cater solely to his needs and undergo an unexpected transformation into tools not appropriate to big shared machines, becoming extensions of one user’s brain. Word-processors and spreadsheets transform the way we think and work; such generalized mind-expenders prove to be more powerful than programs which merely calculate acid-based balance or remind us of potential adverse drug interactions.
Word processing is a utility as revolutionary as Guttenberg’s invention of movable type; it can be expected to raise the standards of thought just as much as the standard of typing. A program costing less than $200 permits preliminary display on the cathode ray tube, where prose can be corrected and modified repeatedly before it is printed on paper. The machine will find all spelling errors and most grammatical errors, permit any character, paragraph or page to be replaced, repositioned or erased. It will index the material, automatically insert hyphens place footnotes and references in place, and allow unlimited experimentation with different margins, page size or paragraphing. When finally printed on paper, the right margin can be automatically justified, and the words become unified into important than these aesthetic advantages, word processing permits the author to revise repeatedly until what he writes finally says what he means.
A second innovative creation on a personal computer is a hybrid of two steps, the generalized data management system, and the spreadsheet. Many small stored globlets of information are aggregated on request, meaningful. If the unit of data is a single patient, with blue eyes can then be effortlessly linked with any other glob of information, such as antibodies to retroviruses. The spreadsheet concept then organizes such data cells into rows and columns which can be fed into formulas which operate serially on every row in a column, generating a new column of derivatives. The user need not, in fact commonly does not know statistical theory, but for example, can process anyway to command regression analysis on eye color and AIDS or any more plausible hypothesis in clinical research. These programs will then transform selected numbers into colored graphs on request (slide). The ability to use statistical tools without understanding them will, of course, create abuses of this system, which in the case of regression analysis would be to overemphasize the validity of 95% confidence limits. Ultimately, the value of the computer product will depend on the brainpower of the individual user. When convincingly packaged data can be processed in massive amounts by chimpanzees at the keyboard of $1000 machines, it is a little daunting to await the misinformation which will be generated by the 5% error content of mountains of data. By the rules of regression analysis, one conclusion in twenty will be reached by the operation of chance alone. Since editors are intrigued by papers which reach unexpected conclusions, thoroughly documented spreadsheets research which later turns into smoke will someday be their proper torment. The exciting future of computers is thus not to replace doctors in some profession-threatening way, but rather to extend the capabilities of their minds in powerful ways which continue to reflect the personality of the user. As has been said of corporations, the dedicated personal computer projects the lengthened shadows of the man.
Early steps in that direction would please Adam Smith, producing exalted results from trivial and mercenary motivations. Whether you like it or not, and whether cost-effective or not, the of medical practice with insurance and reimbursement is making it essential for every practicing physician to employ a computer; those who avoid it have done so out of fear of the disruptions, not because they deny the value of the office machine. Once the machine is installed, word processing is seen as a free bonus, and the financial affairs of the practice become raw materials for database program and spreadsheets. In this way, the practicing physician acquires a mind-expander when he merely sought to reduce his clerical expenses. He also, by way, merges into the mainstream of business computing, and like everyone else, will find that the new IBM model 50 has become the modern standard, just as the IBM Selectric typewriter became the business standard thirty years earlier.
To understand why this is so, notice that IBM continuously spends $5-6 billion annually on research but withholds most new products from the market. Then, about every seven years, a bundled package of innovations is released as a “new generation†which then makes existing machines obsolete and dominates the field for the next seven years. Throughout the seven-year gestational period, other companies also bring forward innovations but must recover their costs by releasing them immediately. IBM watches market reactions, preparing to submerge would-be pioneers in a tidal wave of releases. In effect, other companies test the market for IBM to exploit. Almost every component of the 1987 new generation is new and very little of it is unique to IBM (slide). However, an irresistible market standard is created when many innovations are released at once by the largest volume producer. The new 1987 machines seem mainly designed to permit for the first time several personal computer users to share one octopus machine, a mildly useful thing for the doctor and his secretaries. The main importance of using 32-bit technology lies in the fact that the doctor’s personal computer uses the same system and thus can talk the same language as the mainframes in hospitals, laboratories, insurance companies, and the Internal Revenue Service. The profession must not let itself get lost in the chatter of intercomputer communications; while he must adapt to the equipment that is available, the physician mostly needs many different mind-expanding applications on a single machine. The creation of a market standard will almost surely prove to be a dominant force even for physicians. The IBM model 50 will be what to buy until 1993, as will IBM stock, but physicians need to establish their own culture within the commercially available environment.
1993 will not, of course, be a far enough horizon for Dr. Sherman’s third century, so we might look across the valley over two intervening mountains. Fourteen years from now, the new 2001 models will also be composed of standardized refinements of whatever exciting advances may accumulate in the meantime. By that time, computers should be able to accept voice dictation since they can already understand a spoken vocabulary of about 1000 words. Computer scanners can now read pages of typing with 90% accuracy, so we can except much less typing for accession of much larger volumes of day-to-day information. I understand x-ray films require a resolution of 2000 by 1600 pixels; since advanced computer screens already achieve 1600 by 1200 pixels, the silver-coated films we use now should likely disappear.
In the shorter term, it would be a fair prediction that the exciting programs of the next seven years coming up will exploit the telecommunication power of 32-bit processing and the vast storage capacity of CD ROM’s. Large Multimillion dollar mainframe computers operate in units of 32, but personal computers now mostly use units of 16. Declining prices of transistor chips make 32-bit technology affordable for personal computers, so we can expect to see the doctor’s computer talking on equal terms with the big computer in the hospital, the drug store, and the Library of Medicine. It is exciting to predict role reversal, with once imperious mainframe owners outmaneuvered by users of agile PCs. Organizational whales like hospitals, department stores, banks, and the Internal Revenue Service have had their day of forcing everyone else to conform to their convenience; the little piranha fish will grow sharp teeth.
Since the profession of Medicine is after all in the knowledge business, it is breathtaking to contemplate the migration of medical journals and libraries from paper to electronic medium and the dissemination of libraries to the doctor’s consultation room. Compact disc technology is already the cheapest form of information storage, whose inevitable price decline has scarcely begun (slide). Grolier’s encyclopedia is now available on a plastic disc you could put in your shirt pocket; the entire encyclopedia only takes up 20% of the disc. This unerasable form of storage is sometimes called WORM (write once, read many). Inexpensive scanners can convert pages of print to a computer file in 20 seconds; rather accurate programs can convert foreign language to pidgin English. Between the two processes, whose only present limitation is price, whole libraries will surely soon be swallowed up on plastic disc, and medical journals may appear in that form as soon as someone figures out how to incorporate drug advertising. However, don’t run out and buy a CD-ROM just yet; there are twenty different types and they are incompatible with each other. The exasperating power of IBM is well illustrated by the fact that this titanic information storage revolution will not take a step forward until someone like IBM is able to impose a standard which will disciple the present Tower of Babel.
In closing, the point must be made that the main hindrances to adoption of computers by the medical profession will not be technical, they will be sociological. “Not in my back yard†is the Spirit with which most new things are greeted, even in the learned professions. A plain fact of human behavior is that how you stand is determined by where you sit. For years, banks have transferred patient payments to physician bank accounts without the creation of a single piece of paper. But electronic funds transfer has made very limited progress in 20 years, primarily because the payers and their banks do not wish to surrender the interest float which develops during the delay of transfer. Blue Shield of Pennsylvania has over a million floating dollars earn interest at all times while the obsolete paper check depositing process limps on. The videotape machines which are everywhere provide a warning example of how technical potential is easily frustrated. Instead of ten thousand college professors giving mediocre lectures on Hamlet, it is clear that some professor at Oxford could give the very best lecture on videotape which all students everywhere could watch at home without even paying tuition. Since it hasn’t happened, and it won’t happen, perhaps the point I am striving to make becomes clear.
Try to image the resistance which pharmacists would create to electronic drug ordering; indeed, the nursing profession is very resistant to physician orders which come in any way except handwriting on the floor chart. While I cannot identify the economic incentive which explains the delay, Jefferson Hospital has just installed a system in which laboratory results are instantaneously transmitted to the clinical floors. However, a similar system was installed at the old Philadelphia General Hospital in 1965. These and many other examples of apparently irrational delays most likely have their explanations in the motivation of people rather than the limitations of machines. Therefore, in predicting a revolution in medical information handling we must not, for example, underestimate the capability of printers and typesetters at the New England Journal of Medicine to hold up electronic publishing, or the librarians of the world to resist the destruction of their careers by plastic disks. IBM is in the business of setting bridal supplies and has repeatedly proved to be a shrewd judge of bride psychology. They obviously believe 1993 will be soon enough for the real wedding of medicine and computers; maybe it can wait for the year 2000. Meanwhile, it will not matter much that the bride’s father can easily afford the wedding, or the groom is anxious to perform. Medicine, the bride-to-be, hasn’t yet said “yesâ€.
HSA: The Cruz Transition Proposal
Whatever any unrelated purposes might be, Senator Cruz' compromise proposal (to merge the point-of-sales of the two partisan types of health coverage), has merit. It directs healthcare choice toward the customer, away from the public's elected representatives. Skirting the Constitution, it softens partisan issues into something both sides might accept. It shifts the marketing from the management to an outside broker. Essentially, Cruz proposes that any insurance company selling Obamacare (annual term insurance with subsidies) may also sell the Republican replacement for it. It thus allows Obamacare to continue in existence, but it also permits individuals to dump it. That leaves a lot of detail to be argued over, but at least it gives the customer a choice instead of forcing him to accept some feature he abhors, one size fitting all. Many would think this is a step forward, although it permits everyone to imagine options which may not materialize. It even permits customers to demand new features later, and some company to introduce them, without struggling over something Congress is afraid to touch. A healthcare-coverage supermarket or its electronic equivalent is what seems to be proposed.
The Constitutional Tenth Amendment gives healthcare jurisdiction to the states, ERISA and Medicare make some of it federal without saying so. In either case, it still allows some form of government to license or regulate an industry, instead of leaving it to the customer and vendor to work things out. The government might even foreswear the ability to tax it, as its own contribution to peace. In any case, it discourages the forms of government from pre-empting territory, merely in order to keep others away from it. Checks and balances do somewhat encourage unnecessary government interference, as we might as well acknowledge.
The present arrangement tends to relegate certain vital participants to a lobbying role and confers advantages to some who have excessive lobbying leverage, in this case, the insurance companies, unions, and identity groups. The ability to affect taxes and trade counts for more in this struggle than it should. Obscure alliances combine to unite school lunches with sugar subsidies on one side or the other of healthcare subsidies for the disabled. The history of this sort of thing traces back to the Roman Republic, but it need not be so flagrant and politically divisive.
Apparently, the largest unwarranted purchase of Congressional votes was by large corporations, following the example of Henry Kaiser, eighty years ago. By seeming to give health insurance to employees they retained control of it, largely abandoning control to unions between crises. In time, pay packets readjusted and it cost business very little. In return, they get two tax deductions, one of which is given to their employees, effectively leaving them with more generous wages at a lower cost to everyone except competitors, who are in turn denied equal treatment. Since essentially all health revenue can be traced to the working age group from age 18 to 64, they have control of 70% of visible health revenue, and effectively of all of it, by controlling taxpayer subsidy and bondholder leveraging. This even affects Congressional consideration of capital gains tax reduction, since this largest of tax loopholes is paid for by tax reductions. It largely eliminates the cost of health care for many corporations, reducing if not eliminating, the incentive of business to have its own taxes lowered. It's a convoluted contrivance, making a variation of "too big to be allowed to fail". It really is too indirect to address a major factor in 18% of GDP by removing 70% of the largest block of customers from ownership control, even by simply changing policies.
It is equally convoluted to describe the potential advantage of this Cruz proposal for the equally important issue of pre-existing illness. Since the average worker changes jobs every 3.5 years, and when you change jobs you must change health insurance, the accumulated pre-existing conditions rise steadily with age, as well as for biological reasons. The premiums must, therefore, rise steadily with age. When the young are then forced to subsidize the elderly, the young drop out, and only a limited age subsidy becomes practically possible. Whenever a sharp cut-off separates two forms of insurance, a steep step is imposed at the border. When the incidence of expensive disease is comparatively rare (as it is in the young), the step is so steep it causes a public uproar and healthy young people decline to participate. Since future projections suggest this J-shaped curve will get progressively steeper, the sooner it is addressed, the better. One way to do this is to combine healthy young people with the 30 million uninsureds which even President Obama saw no way to ensure, rather than combine them with the relatively healthy component of the elderly, as at present. After the foreseeable wrangles about prison inmates and illegal immigrants, the effect of this would be to suppress somewhat the age-based cost differential and increase the willingness of healthy young people to save for their own retirements. Meanwhile, science will probably push health costs toward higher age groups. The overall result would be an improvement in longevity, reducing the proportion of people willing to gamble on indefinite good health. The inherent advantage of compound interest over inflation should make trends of this sort easier to finance. Some of this optimism is conjectural, but almost all of the pessimistic alternatives are certain. I warm to the Cruz proposal.
Supermarket Insurance Exchanges Assist Transition from One-year Term to Lifetime Coverage
Lifetime Health Savings Accounts generate surprising amounts of money, and therefore solve lots of problems. However, they leave three problems unsolved, all of them having to do with the administrative agent. The first is trusting some stranger to hold most of your assets for a century, acting supposedly on your behalf in the meantime. The second is to obtain a fair return on your investment, which is to say, you must not overpay for honest service. The remaining problem is a transition from an old system to a better one, for hundreds of millions of different ages, different-wealth, different health. It seems to me Senator Cruz' proposal might ease all three issues, although it lacks details.
The Federal government could seem like an ideal immortal to handle long-term deposits until you look at its record. Watering the currency, shaving the edges of gold coins, and spending money earmarked for one thing, but spent on another, are things which pepper a history more attuned to getting votes than providing service. The motor vehicle office is a symbol of it. In a century, the Federal Reserve has turned a dollar into a penny of value and bought a lot of battleships with money held in trust for pensions. Politicians constantly accuse banks of stealing, but their own record is no better. Private institutions are expected to hold money for a century, but the person in front of you will probably retire, quit or retire in twenty years, to be replaced by a succession of strangers. Mergers, corporate raiders, and outright bandits teach the only generality you can trust is diversification, not consolidation. Insurance is a mixed blessing. In six corporate embezzlements I have been forced to watch, all six were overlooked by management who were easily satisfied with the insurance benefits. What that means is the insurance premiums are too high, mostly designed to save the directors from embarrassment.
In this way, most sane people eventually come to the conclusion the only person you can trust is yourself, and protections will probably only make you careless. Somewhere, this cost is built into the system, and it is hard to say how much it costs. The ancient Quaker doctrine is only a variant of it, "The way to make sure you have enough, is to have too much." Working backward from present longevity, the average person needs to save for retirement, tax-free, about 3% of average income, for about fifty years. And he needs to compound those savings at an average of 6-7% per year, so the first fifteen years are the crucial ones. That goal should accumulate enough to pay for a lifetime of healthcare, plus thirty years of retirement, plus a Quaker cushion of too much. But it needs to reckon with a general obligation of 10% unemployable, plus a one-time transition cost which might be as much a 50% of one lifetime's accumulation. There are other variables, like Korean bombs and Wall Street crashes, minus cures for cancer and automation, but we simply cannot predict all that. It's bad enough without such variables, implying the American public gets serious sooner than its history suggests. Let's project a doubling of savings, or 6% for fifty years, average savings including hardship cases. Actuaries can arrive at more precise calculations, but this is close enough to know it will be a struggle but achievable.
The struggle part is to navigate the jiggles of a continuation of the 12% average annual rise of the stock market over the past century smoothed out for annual volatility, and to assume we can wrench 6% from the finance industry out of limiting inflation to 3% inflation and their own retention factor to 1% . The first step in that process is to transfer the 3% inflation risk to where it belongs, with the customer, not his agent, by isolating and constraining storage costs. Another step is to see what we can wrench from the undeveloped 80% of the world becoming developed, minus the part they can wrench from us. That is profit growth averaging 3% per year for a century. There will be bumps on this road, you can be sure.
The other industry with which the customer must contend is the insurance industry. Their profit is also the customer's loss. It may turn out that the services of the insurance industry are quite fair, and any lessening of producer profit will eventually lead to shortages of their consumer product. But the European taunts at our costs, plus staggering glimpses of insurance reserves, suggest transaction costs plus insurance costs are appreciably overpriced and have been so for decades. Perhaps they are over-regulated, perhaps overpaid, but it seems likely a percent or two can be squeezed away. It is a certainty they over-insure the risks. We should be earning interest on what we now pay interest for, only ensuring what we cannot afford to spend. That may well imply we should spend less on some things, and our problem is to identify which ones they are. To some extent, this is a universal struggle. But most of its excess would surface after a two-year study by impartial experts.
The alternative to this steady grind is to create a market-place and then let the competitors wring the wet washcloth of costs on their own terms. What does the customer care about the technical details, he knows what he wants and for a while will be satisfied with it. The profit margin of a healthcare supermarket defines the cost of doing things that way, providing the signals for change of emphasis when the environment inevitably changes. The chances are good this approach will prove cheaper than continuing down the present path, hoping for a miracle without knowing where it might come from: funds administrators, investment administrators, insurance administrators, hospital administrators, or government administrators. Essentially, we have specialized ourselves into this mess, and the agents have themselves prospered excessively from the design. Whether they were always good at math or not, individuals have been given thirty years of new longevity to cope with the mess their institutional specialist agents have created.
A Gradual Transition, Not a Steep Step
Insurance companies announce premiums in September or October, giving themselves a few months of constant premium prices while they sell policies with a January renewal date. That provides time for the hesitant buyer to look over the competition but is an unnecessary inefficiency for a lifetime insurance, where it is likely to disappear. During the introductory period, experimentation should be made with charging for the ten-year incidence of certain conditions like appendicitis or gallstones, and allowance made for previous removal of the organ in question. A much larger database would be required to make the same adjustments for annual renewals, and there would be considerably less tendency for the patient to game his own health history. The incidence may be the same, but the risk of shopping behavior is much reduced. The possibility of introducing an elective surgery rider exists.
But a transition can be gradual in more ways than just one, changing annual renewal into once per lifetime marketing. Actuaries calculate the average lifetime healthcare cost to be around $130,000 in the year 2000 dollars. Retirement and Medicare begin at the same time, but retirement is continuous rather than episodic. A comfortable retirement to average age 84 might cost four times as much as the healthcare which created it. We may thus be talking about an average lifetime cost of $650,000 in the year 2000 dollars. At 3%, inflation could increase to nominal average cost of $ Assuming we continue yearly premium adjustments, we should at least make yearly adjustments to the premiums for lifetime coverage. That promotes a yearly decision between the present one-year term insurance and a smoothed-out lifetime price, mostly based on considerations other than price. It probably starts with a variable price band for the company to set, within which the employee is allowed a choice to switch to permanent insurance, or not, with a small price variation depending on the calendar date of switch-over. Age and perhaps other variables would affect the changing price. But the main consideration would be transferability between employers, so several large employers would have to agree on the schedule of prices. If the employer declines to participate, he also declines to pay for it, so he must adjust his pay packet accordingly. It must already be obvious why the employer is inclined to follow industry standards, and why special anti-trust exemptions may be necessary. However, once an employee makes a switch, he is likely to remain with that company for a lifetime, so the incentives are mixed.
To assist that decision, a brief overview of the insurance company position is in order. On the one hand, marketing costs are small for an existing company. The negotiation is with a single personnel office rather than hundreds or even thousands of employees. The concept of permanent insurance is probably unfamiliar to most employees, and most of them would have questions. On the other hand, insurance administration is simpler and cheaper, and some innovative clauses could make it still cheaper to run. It would create a permanent customer for many years of coverage with fewer loopholes. And just look at the money involved.A lifetime policy, once it gets started, aims to create an individual $2 million reserve at age 65, which is run down to zero in twenty years by payments until average longevity of 85. But half of the clients will live longer than that, so there is a strong probability of payouts from a trust fund for another 21 years. Whether the insurance company services these expenses itself or farms them out to a vendor, this is a very appreciable amount of business. Multiplying such numbers by 350 million Americans, the sums are in the trillions, approaching the total now invested in index funds. What's involved is the destruction of a medium-sized industry, in order to create a mammoth-sized one.
17 Blogs
Healthcare Reform: Looking Ahead (2)
Spending for health care will just grow and grow forever. Oh, yeah?
How Do You Withdraw Money From Lifetime Health Insurance?
New blog 2014-11-18 20:55:08 description
The Deal Breaker
A brief synopsis of the argument.
All Right, Hippocrates. So What's the Basic Problem?
Such goals unite us, unlike directionless strategies like universal health insurance; and partial success remains a total success in governance.
Reducing Health Care Costs, by Reorganizing Them (Lifetime Health Savings Accounts)
Instead of estimating future health care costs individually, we calculate what is now spent on health care and extrapolate its future trajectory. Working backward from an overestimate, we likely come closer to the true outcome, than by using traditional approaches. Health Savings Accounts return an unused surplus to the beneficiary, consequently, there is less resistance to aiming a little too high in estimated returns. Extracting more revenue from invested premiums provides a second layer of safety to estimates. (www.philadelphia-reflections.com/blog/2682.htm)
FOREWORD, written June 28,2015
Obamacare and Health Savings Accounts briefly summarized.
Summaries for the Book Jacket and Elsewhere.
Left jacket fold-over.
Lifetime Health Savings Accounts:How Much is Enough?
There's an old Quaker saying: The way to be certain you have enough, is to have too much.
The Coming End to Ink Blots.
Overhead, direct and indirect, is shifted by shifting floor space, educational areas, and training costs. The pawns in this game are architects, Resident Physicians, and various student groups.
Methods in the Madness
Another outgrowth of the DRG was the destruction of inpatient psychiatry. For all the public uproar about the Veteran's Hospitals, they are the only psychiatric facilities left.
Academia Gets Its Share of Blame
Academia acts as though it wants to control the whole medical empire, and shares in the corruption as long as it remains profitable. It's sort of like the newsmedia -- we badly need them, but they are pretty unattractive, up close.
Healthcare, A Much Simplified Overview
Health Savings Account, Classical Version
New blog 2015-06-26 23:15:54 description
HSA: The Cruz Transition Proposal
Senator Cruz may have something else in mind, but his proposal makes a realistic compromise.
Supermarket Insurance Exchanges Assist Transition from One-year Term to Lifetime Coverage
New blog 2017-07-13 21:21:42 description
A Gradual Transition, Not a Steep Step
A healthcare supermarket rather than a Congressional dictate.