3 Volumes
Medicine
New volume 2012-07-04 13:34:26 description
Nineteenth Century Philadelphia 1801-1928 (III)
At the beginning of our country Philadelphia was the central city in America.
Health: Philadelphia
New volume 2014-08-04 22:18:40 description
Philadelphia Medicine (2)
Philadelphia is where medicine began in America
Funny Toes: A Physician Viewpoint

|
| Webbed Toes |
It probably took me twenty years to notice that, unlike most people, I had an incomplete separation of my second and third toes. I thought my toes were like everybody else's, but once you start peeking, you see that webbed toes are not normal, although they are not really rare, either. After another thirty years, it became apparent that most of my numerous descendants had the same kind of toe; it was obviously an inherited condition. When the family clan gathered at the beach, it was a source of mild amusement, possibly even a little pride. A few weeks ago, I happened to mention the matter at a party, whereupon another doctor promptly pulled off his shoes and socks, and revealed fused or webbed toes of a much more striking sort than mine; obviously, he was proud of it, too. He is of an old, old Philadelphia family that owns one of the oldest, if not the oldest, a house in Germantown. His family, too, is stigmatized in the same way only more so. In Philadelphia, when you are proud of your family, you are really, really, proud of it.

|
| Ainhum |
Which brings me back to my days as an intern in the accident room of the Pennsylvania Hospital. When there is a sudden crowd of emergencies in an emergency department, the nurses get all of them undressed, put in a hospital gown, and instructed to wait for the doctor behind a curtain that doesn't quite reach the floor. For some reason, as a medical student, I had been particularly struck by a photograph in a textbook of an inherited disorder said to have been first noted on a slave ship; the disease in the native language was named Ainhum. For reasons obscure, a tight little band appears at the base of the fifth, or little, too. It gets slowly tighter over a period of months, and eventually, the little toe falls off. That's all there is to Aihnum, and all that was known about it. So, imagine my surprise and delight to walk past a row of naked feet sticking out below curtains -- and there was my first and last case of Aihnum.
I summoned my colleagues, and the visiting medical students from both Jefferson and Penn who at that time shared training in our accident room. I raced off to my room to get a camera to record this momentous event. An elderly staff physician, either Tom McMillan or Charles Hatfield, wandered past and was invited to share the excitement. Well, he says, I saw one of those forty years ago, it looked just like that; old Doctor Norris showed it to me when I was an intern. Much murmuring ensued but abruptly stopped when the patient himself rose up and started putting on his clothes. He was going home, but why? "Well," he growled, "I came here because my back hurts, and all you people do is look at my toes!" He said he was going over to the Jefferson Hospital to get proper treatment, and I guess he did.
And finally, there is Morton's Toe. Or perhaps more properly, Mortons' Toes. There were in fact two Doctor Mortons, one of them at Columbia College of Physicians and Surgeons where I went to school, and the other at the Pennsylvania Hospital where I interned. In New York, Morton's Toe refers to a painful callous, or neuroma, that forms on the bottom of the victim's big toe. In Philadelphia, such an answer would get a failing grade, because the Philadelphia Morton had noticed that some people have a big toe that is shorter than the other toes, instead of being bigger as the term would suggest was proper. The tricky thing about this relatively harmless variant is that the big toe is actually not short at all. The foot bone, or metatarsal, is short, so the toe of normal length sits back farther on the foot and just looks shorter. The main significance is for shoe salesmen since the shoe needs to be long enough to avoid crushing the other toes.
So now, you readers who were not lucky enough to go to medical school can get a feeling for what it seems like to be a doctor. The other significant shared bond within the fraternity is a sense of outrage at the way health insurance companies drag their feet paying doctors, but that's not limited to feet..
Link to PHILADELPHIA PHYSICIANS
To skip back to GENERAL TOPIC OF PHILADELPHIA PHYSICIANS, click the indicated place below:
» Click here for PHILADELPHIA PHYSICIANS «
Link to:Medical Club of Philadelphia
This concludes the general topic Medicine in Philadelphia. The more specific topic area of the Medical Club of Philadelphia (founded 1892 and still operating) can be reached by clicking on the title below. It's large, so wait a moment for it to come up:
» Click here for THE MEDICAL CLUB OF PHILADELPHIA «
Link to Nobel Prizes
To skip back to Nobel Prizes, click the indicated place below:
» Click here for NOBEL PRIZES «
Link to Academic Medicine
To skip back to the the topic of Academic Medicine, click the indicated place below:
» Click here for MEDICAL ACADEMIA «
Cost Shifting: Indigent Care Out, Outpatient Revenue, In
The CEO of Safeway Stores recently offered his company's preventive approaches as an example of what the nation can do to reduce health costs. He's undoubtedly sincere, but quite wrong; Safeway just shifted costs to Medicare. This is only one of several ways, major ways, cost-shifting is misleading us. Let's explain.
Average life expectancy is increasing at more than two years per decade, but of course, people eventually die. Since health care costs are heaviest in the last year or two of life, extending life will soon push nearly all those heavy terminal costs from employer-based insurance -- into Medicare. To die at age 64 costs Blue Cross a lot; but to die at 65 gets Medicare to pay for it. Either way, the cost is exactly the same, it doesn't save Society as a whole any money at all. Let's put it another way: dying at age 64 costs the employer and the employees, but dying at 65 costs the taxpayers. This means Medicare costs will surely rise, but in this case, it's a reason to rejoice.
Increasing longevity is constantly pushing more costs from employers to Medicare, and not just in Safeway; the prospect is that soon substantially all major sickness costs will shift into Medicare. (To explain the failure of most employer insurance premiums to fall comparably in response to this shift, one must look elsewhere). But just a minute. Medicare is 50% subsidized by the government, and the employer writes off half of the cost as a business expense. That ought to mean it doesn't make much difference to anyone involved, except for one thing. Some employers have two employees and some have two hundred thousand employees. The amount of tax write-off is multiplied by the number of employees, so some employers can only write off a little, while an occasional employer might even make a profit on using health insurance for calisthenics. Economists agree that fringe benefits eventually and proportionately come out of the pay packet, so ultimately the employed patient benefits from the reduced bill, his employer pays less, and the Medicare costs the taxpayers more.
<But instead of going down that trail, let's look at the second form of cost-shifting. Government payers and a few other monopolists are able to pay hospitals less than actual costs and get away with it. The worst offenders are state governors administering Medicaid, where the underpayment is roughly 30%, in spite of federal reimbursement to the states for most of it, at full price. The resulting profit is used for various state purposes, mainly nursing home reimbursement. For the most part, such diverted funds are used for purposes not easily eliminated, so it is unlikely there will be much cost reduction for the government if the scam is acknowledged and merely shifted to a different line in the ledger. To avoid bankruptcy, hospitals raise the rates for other health insurance plans -- and the uninsured. Employers are paying for most of it, so they stand to gain from reform, only to face higher state taxes as matters readjust. We have yet to learn where these costs will shift if the federal government takes over the costs of the uninsured; the current Obamacare plan is to shift 15 million uninsured persons to Medicaid. To a major degree, the federal government and its taxpayers are already paying for a lot of this uninsured cost, through the Medicaid shift. So its present dilemma is whether to continue to pay for it twice.
There's still a third cost-shift. In 1983, Medicare stopped reimbursing hospitals fee-for-service (itemized inpatient bills are still prepared but are meaningless fictions) and for thirty years has paid by the diagnosis, not the service, for inpatients. Consequently, per beneficiary inpatient costs have only risen 18% in five years, while outpatient costs have risen 47%. Costs are not the same as prices, which are even worse distorted. To a large extent, changes in costs are really changes in accounting practices, driving changes in actual practices. Skilled nursing and home care costs are rising even faster. When you hear fee-for-service payments attacked, it is this apparent overpayment of outpatient costs which is the source of the complaint. But to pay out-patient medical costs in any way other than fee-for-service would imply an almost unimaginable restructuring of the medical system, without any proof it would save money. It will be very interesting to learn what contorted proposal is about to emerge.
 Medicare +6% Medicaid -30% Private Insured +32% 
|
| 58% of Hospitals Lose Money |
Not only do these shifts provoke inpatient nursing shortages, but they also start a war for patients between hospitals and office-based physicians. Hospitals are winning this war for business, but are losing money doing so. If the public ever demands a stop to loss-leaders, net insurance premiums will probably rise. The difference between a hospital which makes money and one which loses money is based on whether there is enough extra out-patient revenue to compensate for the hidden tax which the state effectively imposes on hospitals in order to pay for nursing homes. The obscurity of the present payment system is quite expensive, and the present beneficiaries of it are the Medicaid nursing homes. Obamacare essentially provides health insurance to 15 million uninsureds by the process of placing them on Medicaid, so the consequences are going to be an interesting juggling act to watch.
|
5-year Change: Inpatient +18% Outpatient +47%
|
| 5-Year Hospital Costs |
Just notice, for example, that neither Medicare nor private health insurance pays below costs if you look at total national balances. Private insurers are paying hospitals 32% more than actual inpatient costs, while Medicare is paying 6% more than national cost. And yet 58% of hospitals are losing money. The magic in this formula lies in the losses incurred by state Medicaid but shifted to other payers. It could fairly be said we are just looking at a maldistribution of the uninsured, as a cost, and a maldistribution of non-inpatient revenues, as a profit, among the nation's hospitals. To what extent such maldistribution reflects uneven patient quality, as the loser hospitals claim, or provider inefficiency, as the winner hospitals would say, -- merely starts a distraction of attention which could last twenty years while we examine it.
And disruptions enough to take decades to fix.
Cataracts
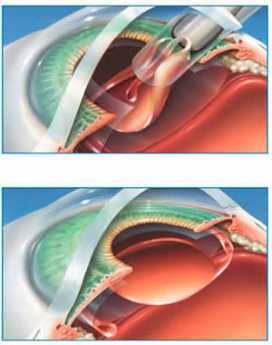
|
| Cataract Surgery |
At a social gathering of older Americans, if someone excitedly announces he has just had successful cataract surgery, the chances are good that every other person in the group will reply they have had it, too. Those who have had two eyes operated have slightly more social clout than those who have had only one, but in general soft lens implants are what everybody has. It's pretty common to meet someone for lunch who had a cataract operation that morning. What a contrast from the olde days. Until about 1970, having a cataract removed was a matter of spending two weeks in a darkened room in the hospital, with your head held in sandbags to keep you from moving. And the result, while better than nothing, was the need to wear glasses so thick they resembled the bottom of cocoa-cola bottles and narrowed the visual field to the end of a tunnel. Those who had cataract surgery forty years ago had to be nearly blind before the risk of surgery was justified.
|
Everybody gets cataracts, and almost everybody is cured.
|
| Dr. Fisher |
There was a reason for this, relating to a blinding eye condition known as sympathetic ophthalmitis. The most harrowing of dangers associated with eye surgery was the tendency for an injured eye to become allergic to itself, and hence also allergic to the opposite eye, soon leading to total blindness in both eyes. Eye surgery was nothing to fool with, and it was particularly dangerous to have a foreign body like a piece of flying glass enter the eyeball. And then, came the Battle of Britain, where so many owe so much to so few.
The British pilots were flying Spitfires, a type of airplane with a large plexiglass canopy over the pilot, allowing him to look in all directions for the enemy. The German Messerschmidt pilots would swoop down on the Spitfires, machine guns blazing. The Spitfires were not necessarily shot down when they were hit, but many of them had shattered chards of plexiglass sprayed into the cockpit, and many of the splinters went into the British pilot's eyes. If they managed to land the planes, the British doctors administered emergency first aid, stopped major bleeding, fixed major broken bones. In the heat of the emergency, no one noticed that bits of plexiglass were being left in the eyeballs.
Eventually, these survivors were being treated for scars and injuries in clinics, long after the war. One British opthalmologist suddenly had a striking insight. These eyes, with buried foreign bodies in them, were working just fine. No sympathetic ophthalmitis; that wasn't supposed to happen. Ultimately, the realization spread that plexiglass could be used as a lens implant, and many patients were successfully treated with a so-called hard lens.
The next advance was the soft lens. Someone realized that soft plastic, like a soft rubber ball, has a memory. Squeeze it out of shape, and it will soon return to its original shape. So, in effect, a soft lens of the proper size and shape can be squeezed into a toothpaste tube, injected into the right place in an eye, and it will pop back into shape. Before this can be done, of course, the rotten old lens has to be removed in any of several ways; pluck it out with eyebrow tweezers, or buzz it into liquid by lasers or other means, suck out the juice and squeeze the squashed-up soft plastic lens into place. With practice, the whole thing can be done in ten minutes. That's modern cataract surgery, and it's pretty slick, especially if you know what the struggles were, before the Spitfires.
But don't let me overstate matters. This operation still has its risks. The retina behind the lens may turn out to have been defective, so a new lens hardly helps very much. Or there can be a slip, which amounts to one drop of blood getting where it doesn't belong, and the eye or both eyes are ruined. When I had my eye fixed, I seemed to be lying on the stretcher, waiting for a lot longer than necessary. Suddenly, I heard operating room doors banging open, and several older physicians in street clothes came in, huddled around, talked with each other for a long time, walked slowly back out into the corridor. I knew exactly what that was all about, and it didn't improve my serenity. Eventually, a nurse came around and asked if I was ready for my surgery, and I said, Well yes, I guess so.
Inside the Big House

|
| Medical care inside a prison |
The Right Angle Club was highly honored recently to be addressed by Peter Binnion, MD, the former Chief of Cardiology at the Pennsylvania Hospital, distinguished librarian of the Shakspere Society, and well-known former Main Line physician. Peter is now, hard to believe, Associate Director of a state prison medical program. One of the members of the audience asked him straight out, "Why are you there?"
At a time when prison medicine is widely, and correctly, regarded as a generally deplorable system, it is hard for the public to understand the sense of duty which impels at least a few of the profession to try to improve matters. And it is particularly difficult for the lay public to understand the attraction for a well-trained academic physician to work in an environment of severely ill patients. In a sense, it's like the old days.
And Peter slyly pointed out, it may be somewhat like the future if we aren't careful. He artfully repeated the anti-medical care harangues which are now commonly issued by various liberal politicians, denouncing the extravagant care we are supposed to provide, and the uncaring attitude toward the uninsured sick. Having resonated with any left-leaning members of the audience, he proceeded to describe what things are like when the government provides the care, and how it feels to observe the limitations of a real bureaucracy. Just for a start, he isn't allowed to call himself a doctor. He's a provider of care. And to go on, not only are the prisoners three to a room designed for two but one-quarter of those without cells, sleep on the bare floor,

|
| Delaware State Prison Patch |
Over ninety percent of the prisoners are taking illicit drugs; their ingenuity in smuggling simply passes belief. What's called drug detoxification among new inmates gets briskly to the goal. Our speaker delicately avoided the disagreeable notion that study after study has shown that illicit drugs in prison are almost invariably smuggled in and sold by the guards. For them, it's just a source of supplemental income, justified in their minds by low pay for unpleasant work. Lots of the prisoners have HIV infection, although not as many as depicted in rumor. Unless a disease is life-threatening, treatment is not encouraged. Hernias are not repaired, for example. And so a physician working in this environment is intended to spend all of his time with life-threatening conditions. Most physicians would shame-facedly have to admit this makes for an exhilarating professional experience, and it is indeed the sort of environment in which post-graduate medical training once took place, almost everywhere. Up until now, Peter had never seen a case of Hepatitis C. In the past two years, he has treated six cases. Diabetes is almost always out of control because it is absolutely forbidden to allow the prisoners to have the needles to give themselves insulin. Sharps, you see, is prohibited.
It's a little disconcerting to be given lectures on how to behave if you are being held hostage, but the fact is that the prisoners universally treat the doctor with great courtesy. You know they are always looking for drugs, and you know they regard the medical system as a soft spot in the security system so it's a good place to launch an escape attempt. But regardless of the motivation, Peter observes at least as much civility in these patients as in the Main Line office. The doctor really doesn't want to know the reasons for imprisonment, and the prisoner certainly doesn't volunteer it, so the topic just doesn't come up.
Three goals are maintained, above all others, by the prison authorities. The suicide rate is regarded as a measure of the prison system, so extreme measures are taken to prevent it, or to prevent suicide from being successful when attempted. There is a very high rate of schizophrenia among the inmates, which probably reflects the deplorable state of psychiatric hospitals following the 1983 Budget Reconciliation Act. The second overriding goal is to protect the guards ("officers") from attack, so that scissors, hypodermics, and things which could remotely be described as a "sharp" are scrupulously sought out and eliminated remorselessly. The final goal, of course, is to prevent escapes, which have become the public measure of whether or not it's a good jail. The precautions taken to prevent, thwart and punish escape attempts hang heavy in the air.
All legislatures hate prisons; they cost too much. Since budget restraints lead to many of the nastiest features of prison life, budget restraints enhance the punishment. How much these two ideas reinforce each other is hard to say, but one thing is clear. Individually, people are pretty decent; collectively, Society is a bum.
Reforming Health Reform, New Jersey Style
 |
| Congressman Robert Andrews |
A single e-mail to constituents, and no other communication visible to the general public, announced a town hall meeting with our Congressman, Bob Andrews, on the campus of Rowan University, from 6 to 8 PM, August 24, 2009. The subject was to be Health Care Reform Legislation. On arrival, it was hard to find the auditorium in the square mile of new college campus, and only a small sign entitled "Event" indicated the place to park. Lots of cars.
By counting seats in a row and multiplying by the number of rows, the University Auditorium held 3000 people, but at 6 PM it was difficult to find a vacant seat. The doors were almost blocked by two lines of people standing to speak at microphones in the center of the hall, snaking all the way out past the television cameras and then out the door. These people were strangely silent, preoccupied but not rude, apparently rehearsing their speeches. In the lobby outside the doors, several workers were distributing posters showing "Thank You!", checking people off on lists of some sort. Many of those who got posters were wearing red T-shirts emblazoned with something or other.
 |
| Rowan University |
When I finally got a seat inside, it was behind a whole row of such T-shirted poster-holders, mostly but not entirely of the black race. The Congressman was giving a little speech to the effect that he was one of the committee members who wrote the bill, so of course, he had to support it. Strange, that as a member of Commerce and Labor he was working on a bill which traditionally is the province of the Subcommittee on Health, of the Ways and Means Committee. In any event, that gave him the ability to explain some of the languages which were a little too hard to understand. Several in the audience shouted out something unintelligible at that point, but mostly the audience sat in silence, waiting for the questions. He soon opened it up for questions, because he wanted to know what his constituents were thinking.
Although a few inevitably wandered off the point, questioners were confident, moderately deferential, remarkably effective. No matter how it was stated, and no matter how it began ("I have always voted for you, Congressman"), they were at the microphone to run a sword into him. To some extent, posting the entire bill on the Internet had changed politics. One old man, reading from his papers, said that page 343 says, etc; to which the harassed Congressmen blurted out, "That isn't true!" But the old man held his ground, "Oh, yes, and what else isn't true, that's written in the bill?"
Our congressman represents a working-class district, as clearly illustrated by his previously running for Congress without opposition. In searching for the reason this solidly Democrat audience was so antagonized, one gathers they generally have Unionized health benefits and feel threatened that ensuring the "illegals" will be paid for by impairing their own insurance. Somehow they feel that anyone who denies it is lying to them. ("It isn't what's in the bill, it's what will be in the bill ten years from now.") Except for college professors, Union members have the most luxurious health insurance coverage in America and are accustomed to boasting of it. Somehow, this privileged position drowns out their envy of rich people. When told that only the top x% of the country would have its taxes raised, one man bore right in on the Congressman. "You never heard anyone asking a poor man to give him a job". (Yeah, right, right on, Yeah.)
Although the people in red shirts holding posters put up a fight for fifteen minutes or so, they soon subsided out of recognition of who "owned" the room, and the remaining three hours of "questions" were almost uniformly negative. After an hour, the television cameras left the room, and at that signal, the people in front of me wearing red shirts also left. After a succession of speakers praised physicians somewhat excessively, a couple of physicians got up and made a poor showing at the microphone. One of them, a fat woman, had the poor judgment to tell these folks that many diseases like diabetes were self-inflicted, but was to hear back that it would help if our President would himself stop smoking and leave the rest of us to mind our own business. Two women who proclaimed themselves single mothers were no better treated..
At 9:30, a meeting scheduled to end at 8 PM still had a thousand people in the audience, and fifty at the microphones. But I had enough. They made their point. All that remains is to see how fairly the television editors extract significant clips and to find out how the rest of the nation feels.
LATER FOOTNOTE: As matters turned out a few months later, this national legislation had more of a local New Jersey effect than the audience could have guessed. Mandating health insurance for 30 million uninsureds, Obamacare accomplished it for 15 million of them by forcing them into the state Medicaid program, which is widely acknowledged to be the worst program in American medicine, because it usually is the most under-funded. New Jersey residents are firmly opposed to anything which raised their already high local taxes and will focus intently on the attempt in the coming lame-duck session of Congress (November 2010) which intends to transfer federal money to states to pay for Medicaid, and which is given only the narrowest chance of success. Republican Governor Christie deftly split the industrial unions from the public sector unions with the remark, "Every time they get a raise, you get a tax increase." It was hard to answer.
Time To Care
|
| Dr. Norman Makous |
It sometimes seems as though Medicare has been a standard part of the scene for so long it now needs major reform, but when a doctor has practiced Medicine for sixty years he has seen a lot of contrasts between the old way and the new way, not all of them favorable to the new -- which we are now tired of, and trying to repair. That's particularly true if the doctor practiced at America's first and oldest hospital, because it sustained many traditions from two centuries before, and was among the last to yield to the imperatives of newcomers for the last forty years, their hands grasping for the purse strings. Dr. Norman Makous must either have a remarkable memory or a thick, detailed diary. He tells three hundred pages of fast-reading anecdotes about sixty years of his own medical practice, before summing up in fifty pages of reflection. One by one, he describes the innovations in his field of cardiology and how they affected him and his patients. Thiomerin, one of the first of many easy ways to pump out excess body fluid accumulation, transformed the treatment of congestive heart failure. Synthetic digitalis claimed to but probably did not much improve things over dried digitalis leaves; it certainly raised the cost. Cardiac catheterization, electro-shock resuscitation, ultra sound diagnostics, MRI and CAT scans, cardiac surgery using the heart-lung machine, and finally cardiac transplants -- all started out as headline-news spectaculars, evolved into cutting-edge advances, and then settled down into the Standard of Care that you obtained a plaintiff lawyer to sue about. All in one medical lifetime, supposedly prepared for by one Medical School course, followed by one residency apprenticeship, the specialty of Cardiology was completely transformed at least six times.
Meanwhile, the leadership of the medical profession was tenaciously resisted by those who supposedly followed its direction. Hospital administration.
Only Three Things Wrong With American Healthcare

|
| American Healthcare |
Although Congress is offering several thousand pages of proposals for healthcare "reform", none of them even mentions the three main difficulties, to say nothing of fixing them. Let's be terse about this:
1. Health insurance is fine, but if you make it universal, there is no impartial way to determine fair prices. Somebody must haggle with the vendor in order to introduce the issue of what is the service worth? The customer doesn't care what it costs to make, or whether the vendors are being paid fairly. If everyone is insured, no one cares what it costs. Not only do all costs rise, but they rise without coordination, without a sense of what each component is worth, relative to alternatives.
2. Employer-based insurance is fine, but it ends when employment ends. You just can't stretch employment-based insurance because you can't stretch employment.
3. State Medicaid programs are fine, but just about all fifty states are going broke trying to pay for it. Extending it to more people by raising the income limits just makes things worse. Items 2. and 3. are related. Trying to do both -- expand Medicaid as employment shrinks -- during a recession is incomprehensible. Item 1. (price confusion) gets drawn into this because the States try to pay less than it costs, hoping to shift the deficiency through hospital cost-shifting, utterly confounding the information which prices provide. The doctors have no way to tell which is the cheapest approach to a problem, so they don't try. Without control over prices, we can only control volume.
That's really all there is to this mess. Not one word of the current legislation even mentions these problems, so of course the legislation blunders. Even a child can see that compulsory expansion of benefits to universal coverage will fail if you can't pay for what you already have. No one will make sacrifices for a new system if the sacrifices seem futile. They are futile, so leave me alone.
The current administration has been compared with bank robbers who see they are trapped and decide to shoot their way out. Let's see them try to shoot their way past the first Tuesday after the first Monday in November.
Christmas Reflections
My father in law, a prominent obstetrician in Binghamton, New York, regularly took his family to New York City sometime between Thanksgiving and Christmas. The three-day junket was described as a visit to do Christmas shopping. Another relative made similar trips from home in Tyler, Texas. Several of my patients made such visits to Philadelphia from their homes in West Virginia, stopping by to make a medical visit to me during the same trip. From the seasonal crowds in Penn Station and in the shops on Chestnut Street, it was clear that an annual visit to the big city was a common custom in the upper crust of small to medium-sized cities, for whom the more expensive shops of the bigger city provided big-ticket items bought infrequently, and the distinctive luxuries which made them stand out from the socially less-enlightened back home.
These shopping visits were not confined to purchasing, although that was the main focus. It was a time to go to the theater, orchestra and opera, maybe an occasional ballet and art exhibit. The choice of a large city might be related to returning to the University, or another period of professional training for a drop-in visit because these associations made it possible to observe the latest trends and innovations, a useful issue in the smaller towns. The ladies could observe the trends in fashions, and everyone would have a chance to dress up in the better hotels and restaurants. This recirculation between the small towns and the big one at the hub unified the region, establishing hierarchy rather widely. And it hardened traditions in the big city, since islanders tend to return to the same hotel, restaurants and social gathering spots even more than the local residents do; there isn't time in a brief visit to shop for new venues, unless the trip itself reveals that times and places have somehow changed in an important way.
 |
| Wannamakers Pipe Organ |
That's all changed, today. The pipe organ at Wannamakers, the cluster of department stores around Eighth and Market, the theater district, Caldwell's and Bailey Banks and Biddle upscale jewelers, the fancy women's clothing shops on Walnut and Chestnut Streets, and the bespoke men's tailor shops -- have disappeared in a slew of retail despond. The excited crowds of upscale shoppers have dwindled, at least in the center city shopping area. Students of sociology point to the decline of the department store as a central commotion in the center of this phenomenon, blaming that in turn on the spread of national brand names by television and more electronic forms of advertising. The department store did your comparison shopping for you, putting its brand name on the product and placing its reputation behind the choice. If Wannamaker could determine that a Japanese radio was of high quality, it became Wanamaker's radio. Today, Samsung and Sony do their own advertising, sell their products through outlets in the suburban malls. Philadelphia residents enjoy as much retail choice and pricing as ever, they just shop in the malls located along the Interstate circumferential highway, just outside what used to be the outermost suburbs. So the volume of retail shopping among Philadelphians probably hasn't changed a great deal; it has merely shifted to the malls where there is parking for your car to transport goods which the department stores used to deliver. It is the annual visits from the subordinate small cities at moderate distance that has disappeared. Small cities now have their own shopping malls, carrying national brand name merchandise. Losing this source of business, the associated entertainment industry has declined to a point below sustainability for most of them -- in the center city hub. Along with the disappearance of this regional recirculation, small cities have lost their sense of affiliation with a bigger one. The small-town professional class which was the biggest participant in this annual migration is professionally more isolated but so are their clients. The upper crust of the small town now must constrain its horizon to the smaller town professionals, with their lesser claim to distinction. For a while, the disparity can be overcome by specialization, but ultimately the distinction of the big-city specialist rests on assembling a richer experience from wider drawing power. In Medicine at least, the insistence of Medicare on paying the same fee for the same service lessens the economic incentive for self-repair of the system.
 |
| Wannamaker's Christmas Light Show |
Meanwhile, nature of Christmas itself is becoming standardized. Fewer people make their own Christmas presents, whether through knitting or baking. If the process of commercial gifts goes the full distance, eventually the joy of searching for exactly the right gift will seem more like paying your taxes. These things already cost too much, are worth too little, and neither the process of giving a gift nor the process of receiving a welcome gift will retain much joy. Or significance. What was until recently a Christian religious celebration has become diversified into a generic "Happy Holiday", presumably in order to avoid offense to other religious groups who themselves likely persist in their old traditions of ritual greeting. The assault on Christmas is however not primarily cultural, but commercial. The silent ostentation of elaborate outdoor lighting and the secular versions of Christmas carols endlessly replayed over loudspeakers in stores, probably have a more destructive effect on the community winter solstice ceremony than any competition for religious adherence.
The coming next step in the modification of the Christmas season is dimly visible in the assault of pocket telephones on the suburban shopping mall. After enjoying only a few years of victory over the center city department store, malls must now confront shoppers with portable telephones containing a camera and GPS geographical locator. Seeing something he likes, the shopper of the future can photograph its bar code in the shop display, and be immediately told of all the neighboring stores which sell the same product for a lower price. Electronics are thus about to turn Christmas shopping into an electronic auction, no doubt making it eventually easier to do the shopping from home.
What Christmastime means to me is a recollection of what it once was like at the nation's oldest hospital, and not so terribly long ago, at that. Before 1965, the Pennsylvania hospital had been staffed for centuries with unpaid student nurses, working under the direction of unpaid doctors in training, supervised by volunteer attending physicians. Of the five hundred beds, only forty were filled with paying patients and the rest were housed in long communal halls. On Christmas morning at 7 AM, the drowsy patients were astonished to be awakened by a procession of very pretty student nurses, led by Miss McClellan the grim-looking Directress of nursing, and followed by a handful of internet and residents, all singing Christmas carols and carrying lighted candles in the dark. Miss McClellan herself was never heard to utter a note, but the student nurses had been trained in four-part harmony, and the interne doctors were enthusiastic followers. The faces of the poor old indigents in the beds were filled with pure delight as we traipsed past, chanting of the travels of Orient kings, the pregnancy of virgins, and other miracles of the occasion.
Lumpers In Constant Combat With Splitters
|
| James Boswell's Book |
Some colleges produce managers by teaching management theory, but in certain Ivy League colleges it is thought to be more useful to teach how to dominate a committee, eventually perhaps a board of directors, or a board of trustees. The handbook of instruction is James Boswell's Life of Johnson which is a rather large book of verbatim notes that Boswell took of his many lunches at a London club in the 18th Century. Boswell was a quiet mouse privileged to sit in the company of the great Dr. Samuel Johnson, surrounded by the most eminent intellects of the Enlightenment. Boswell carefully manages the background of each episode, describing the issue and the various arguments, and then -- Sam Johnson's booming voice settles the matter. After he speaks, the meeting is over.

|
| Dr. Samuel Johnson |
"Why, sir", says Johnson, and then look out for the one-liner to follow. We get the impression that Dr. Johnson used that "Sir" signal to indicate he had enough of these dumb arguments, and soon would come the growled epigram that scatters any token resistance. Boswell may have neglected to record instances where the great Johnson was defeated in debate, who knows. We are left with the distinct impression that if you engaged in lunch table conversation with Sam, you were almost certain to lose. So that's what Ivy League students are being taught: how to win a debate at a committee meeting, in the expectation they would spend much of their lives in committees, boards, and even cabinets. That's how the English-speaking world gets its work done and its decisions made. That's what lunches at the Franklin Inn Club, or the club tables of the Union League, are trying to do for the education of neophytes.
As the goggle-eyed student of the great Chauncey Tinker, who gave young Pottle his start in life, it was an awesome performance for me to watch. But the rules of this game never became entirely clear to me, I'm afraid, until the other evening when I listened to Peter Nowell describe in a half-dozen brief paragraphs how he had revolutionized prevailing theories of the cause of cancer. The Franklin Institute then followed the award ceremony by putting on an all-day symposium of notables who run elaborate enterprises in cancer research, essentially funded by the National Institutes of Health, your tax dollars at work again. Last year, the NIH dispensed thirty billion -- you heard me -- dollars in research grants to internationally known research entrepreneurs, and if you can stay awake during their talks, there must be something the matter with you. So far as I could see, they were painstakingly describing every grain of sand on the beach, whereas Peter Nowell made the whole beach electric and clear in ten minutes. Essentially, he was saying that each patient's cancer is caused by a long chain of events, starting with a single mutation within a single cell. All the other cancer cells of a patient are descendants of that first one, which triggered the cascade of chemical events now repeated by the descendants. To stop the process, you probably only have to find a way to break the chain at one vulnerable point. Then you have a cure, without necessarily understanding every other link in the chain.
Peter Nowell described himself as a "lumper", admitting that most scientists are "splitters". A splitter quite reasonably attacks a complex problem by isolating one small piece of it at a time; that's really a pretty good way to address overwhelming complexity when you encounter it. But you can be sure that people of that mindset should not be found in a President's cabinet, deciding how to save the world from impending disaster. Whether by their own genetic predisposition or as a result of peer pressure in their profession, they are habitual splitters. And it suddenly occurred to me why Sam Johnson's one-liners always won the argument; he was a lumper. Usually right, sometimes wrong, never in doubt. Witty as a Frenchman, but as quick as a rattlesnake. Cordial, perhaps, unless you disagreed with him.
We need more lumpers. If they get that way from the likes of Chauncey Tinker, we need to print more copies of The Life of Johnson. If they are born that way, maybe we need a breeding farm for lumpers, which is what the Assembly Ball amounts to. But don't get me wrong, we need more splitters, too. They just have to learn their place at the table.
Atlantic City, Brigantine and the N.I.H.

|
| Dr. William Osler |
It would only be honest to say that Atlantic City was a rundown mess after World War II, cheap, sleasey and dispirited. But for academic medicine during a period of thirty or forty years, one small nook of A.C. was the most exciting place in the whole world. Only during several days at the beginning of May, however. The reason it was so attractive to scientists was that beach hotels were cheap and dilapidated; Atlantic City probably contained the worst on the East Coast. The Haddon Hall was an exception, rather elegant and far too expensive for most physicians in training; research is a young doctor's game. The medical profession's annual beauty contest for medical research was headquartered in Haddon Hall next door to the Steel Pier, surrounded by hundreds of cheap lesser hotels. The professors all stayed at Haddon Hall, but few others could afford it. Indeed, resident physicians from Philadelphia mostly found it cheaper to commute from home for ninety minutes than to stay overnight, residents and fellows from more distant cities stayed in the dumpy hotels. Nobody in that age group had much money to spend, so the commuting Philadelphians didn't miss out on much nightlife at the shore by going home every night.

|
| New Atlantic City Skyline |
Before the spring meetings got popular after World War II, a hundred members of the most elite society of academic research professors on the East Coast assembled in Haddon Hall, all of them quite able to afford to stay in the headquarters hotel. This had been going on since William Osler founded it in 1885, at first in Washington, and then migrating to Atlantic City. As medical research began to flourish, the society grew a little, but at a pace too slow to keep up with the growth of medical scientists, so a second group of "Young Turks" formed a competitive society which met the next day, and ultimately a third group, the "Young Squirts", felt excluded by the old has-beens, and met on the third day of what eventually turned into a week-long parade of scientific presentations, each ten or twelve minutes long, starting before normal breakfast time, lasting until 10 PM, with occasional breaks. That is to say, the medical papers that everybody wanted to hear grew from thirty or forty a year to nearly a thousand. If a young fellow did well, the older professors would notice, and he would get employment offers. That kept the eminent older doctors around for the whole session and provided an informal ranking of the worth of the program. Everybody wanted to advance up the ranks of prestige, and this system roughly sorted them out. However, it was an exhausting experience just to sit through all that and listen; the old professors tended to drop out and go home a little early. No matter how many outstanding papers were clamoring to be heard, no one could endure more than a week of straining for attention. It was strictly forbidden to present a paper which had been published or presented anywhere else, so it was usually difficult to guess in advance whether a paper was likely to be exciting. You could go home early if you wanted to, but at the risk of missing the real blockbuster of the year, tucked away on the program with a bewildering scientific title. The younger wise-apples had a formula, that if one paper in three was outstanding, you were having a good meeting; you just had to grit your teeth and try to stay awake during the other two-thirds. Still, that got to mean that the reward for pursuing this grinding ordeal was to go home after learning about three hundred outstanding scientific advances that no one else knew about; knowing three hundred cutting-edge things that other doctors didn't know really did put you well ahead of the pack. Keep that up for ten or twenty years, and notable differences among colleagues would relentlessly emerge.
|
| Old Steel Pier |
From the lounge of the Haddon Hall, with non-members forced to stand in the back, the meeting moved to the 2000-seat movie theater in the Steel Pier, at about 1950. Things then came to equilibrium; the movie theater was never completely full. We were told there were seven or eight even larger auditoriums on the Steel Pier, but it was never necessary to move to them. The first four years I attended these sessions I was being paid no salary at all, and most of my contemporaries were only getting token amounts beyond room and board. The eminent professors who were real members of the top society would find their way to front-row seats where they could ask questions, having had a chat with colleagues at breakfast in the Haddon Hall. But they had once been impecunious, too, and wore their brand-new Ivy League plaid jackets rather uncomfortably. Doctors who (gasp) worked for drug companies also gave signs of affluence, but they tended to drift over to the barber shop and have a shoeshine, where they picked up the gossip for their employers. Over a period of fifty years, I can recall first hearing of the wonders of several new antibiotics, a strange chemical called cortisone which seemed to cure rheumatoid arthritis, the introduction of the birth-control pill, the introduction of polio vaccine, the first drugs in the treatment of tuberculosis, and a vast array of novel explanations for disease phenomena that had seemed mysterious for centuries. In those days, a year without a new medical miracle was a very lean year, indeed. During this interval, the basis for curing at least thirty common diseases was first presented at the Spring Meetings in A.C., and since then medical practice looks nothing like it did in 1947.
Gradually the audience changed, too. At first, the people presenting papers came from at most ten medical schools, and mutterings of discrimination could be heard. In fact, it was plainly true, because only about ten schools had any extra money to fund research. When this news reached the U.S. Senators from the Mid and Far West, federal research money started to be spread around more evenly, just like the distribution of Senators. It was the appointment of one of the members of the original small nest of clubs to the Directorship of the N.I.H., the National Institutes of Health in Bethesda, Maryland, which really got the research spigot to flow. The point man was James Shannon, who knew what was what in cutting-edge research, and he sat there in the audience making up his mind who was who. For all the time of his directorship and for long afterward, he enforced, really enforced, the rule of "no political influence in research grants". Lots of congressmen came to the N.I.H. with the news that their relatives had such-and-such a disease, and so they thought more money should be diverted to research in that area. Nothing doing. Shannon held the keys to the kingdom, and he knew it. He had a deft feel for how much money the research industry could usefully absorb, and then he went to Congress and demanded it. The purity of this process has frayed at the edges somewhat as the amounts of money grew to what is now thirty billions of dollars a year. Most experiments, unfortunately, fumble or fail, so a lot of money gets spent on blind alleys before someone gets it right. It takes a tough-as-nails idealist like Jim Shannon to survive the temptations of an N.I.H. Director, and among the temptations is just to give up and give out money indiscriminately to people who want to count all the grains of sand on the beach. If your idea was a good one, you got all the money you could possibly spend; if the idea was mediocre, in those days you got nothing at all. On the other hand, the estimation of overhead costs is something other mortals can quibble about. Shannon demanded and got about a third of the grant money to be given to the medical school administrations. That was barely enough in a research establishment emerging from the Depression of the 30s, and the World War. However, now that the pipeline is filled, it is increasingly doubtful that ten billion a year needs to go to administrators; the bean-counters took over, and the results are more open to criticism. After all, after someone finds a cheap cure for cancer, some disadvantages of perpetuating an aging retiree population start to emerge and may outweigh the arguments for spending quite so much doing it. That may well be what the advisors to President Obama are growling at, but for now, the example of his nose poked into the hornet's nest of favoring research for certain population (voter?) groups will restrain others who were once inclined to agree. After cancer is cured, perhaps then everything will seem different.
|
| Dr. James Augustine Shannon |
Well, let's tell one story out of many that could be told. Around 1965 there were two competitive polio vaccines rumored to be in the pipeline. Jonas Salk had an injection method, and Albert Sabin had an oral vaccine. Anyone who had watched children run shrieking from a needle knew that Sabin had the preferred method, but Salk got to Atlantic City two years earlier than Sabin. The auditorium was filled with rumors of very dubious precision to the effect that Salk had used unfair methods to get to the stage of public announcement. For example, it was growled he gave the vaccine to the Russians to test, but they were afraid of it and gave it to the Poles. Regardless of such scurrilous gossip, which is here repeated only to show how hysteria can occasionally agitate even scientists when Salk gave his paper at the Steel Pier, the standing ovation was thunderous. And so, as the meeting broke for dinner the crowds migrated over to a huge seafood restaurant named Hackney's and watched the new scientific hero get a little tipsy in public. That seemed to revive the rumors which became even less factual. But there is no doubt that by the time Sabin stood at the same podium and gave his presentation of the oral vaccine, the crowd had switched to his side, the ovations were unlike anything the scientists had ever heard. Anyway, as emotions now settle down in retrospection, we are all pretty happy that polio is nearly eradicated from all but a few corners of the earth, and these two men are both responsible for it. But so is Jim Shannon responsible for it, and he never got the ovations he deserved.
|
| Mr. Peanut |
When the gambling casinos came to A.C. the cheap boarding houses were swept away, doctors in the research were incidentally better paid, and the Spring Meetings migrated back to Washington. The dumps on the beach have been replaced by gleaming multistory hotels, the place looks much more prosperous. Doctors are in a position to know about the drug and alcohol addiction, the venereal disease and crime among the casino employees, and the personal tragedies among the gamblers. But anybody can see the new buildings and clean streets. When a group of eight of us took a nostalgic trip to revisit the place, no doctor even mentioned the idea of going in to drink and gamble -- even the suggestion was preposterous. So we wandered over to Brigantine where there appears to be a large retirement community, where gambling and drinking seem equally unlikely. The elementary school in which we heard a talk about the old days was splendid beyond anything I remember in an elementary school. Among the audience, the questions revealed there were many former employees of the old A.C., people who ran shops to sell salt water taffy, fudge and the like to crowds on the boardwalk. Some of them may have once driven Jitney buses or pushed sightseeing wheelchairs. But not one of them showed the slightest sign of recognizing that on the first weekend in May, every year, a crowd of nerdy-looking serious fellows would move into familiar boarding houses for a few days, remaining mostly invisible during daylight hours. That was the academic doctor crowd if anyone had bothered to ask, pouring into the Steel Pier movie theater, having the time of their lives listening to medical history being made. After a week they all went home, and nobody in A.C., later Brigantine, paid any attention to any of it. After all, A.C. is about salt water taffy, right?
Cataracts and Deference to Seniors
Last week I had a cataract extraction; it went well. I now see like an eagle, there was no pain at any time, and it only interrupted my life for about six hours, including travel time. While I suppose there is a chance of complications during the next month after surgery, I'm an optimist and statistics are on my side. As they say in South Philadelphia, faced about it.

|
| Cataract Extraction |
Those were of course not the serene thoughts I had in advance of the surgery, which carries certain risks. Persons with myopia like me often have a mismatch in the size of their eyeball and the size of the retina inside so the retina can tear or detach during the first few days after the eyeball's integrity has been pierced. The lens can get stuck and break apart as it is being removed, hemorrhage can occur. The surgeon's hand can slip; he can sneeze at the wrong moment. So, bad things could have happened to me, making my twinge of anxiety entirely justified. But that's all behind me now; I even forgot to ask the surgeon what type of lens he intended to implant so I could argue with him. Let the Captain run the ship. I was surrendering my fate to the largest eye hospital in the country. They perform between fifty and a hundred of these procedures every day, and my surgeon is the chief of the cataract department.
And yet, and yet, I have a few grumbles, leading to some generalizations about health care for the elderly. In the first place, I was told by an administrator who sounded terribly fierce that I had to be there at 8:15 AM, in the company of the person who would drive me home, or they wouldn't do my surgery. I told her I doubted that, so we got off to a poor start. The procedure ought to take less than ten minutes to perform, perhaps twenty if you count the formalities. Furthermore, I was a consultant to that hospital once, and still had a certain amount of standing in the Philadelphia medical community, having once been a trustee of almost everything you can be a trustee of. Sure enough, when my driver and I arrived at 8:15, there were more than fifty others waiting. They finally called my name at 1:30 in the afternoon, and by roughly 2 o'clock I was out of there. I was by no means the last one waiting to be called, and it sort of felt as though we were all treated like logs of wood. While I was inside the operating room, a couple of nurses were chattering, and one said she much preferred to work on weekends because there were no administrators around. I could see what she meant.
To keep this essay from sounding like constant whining, let me tell a little of the history of this operation. Until perhaps twenty years ago, a cataract extraction involved keeping the patient in the hospital after the operation with the head in sandbags, for two full weeks. Now, it takes ten or twenty minutes, and you are free to have lunch with a friend in an hour unless you give in to your driver who has been waiting five hours and wants to go home. The results are far superior, and you don't have to wear glasses that look like the bottom of Coke bottles afterward; in fact, I already see pretty well without any glasses before a week is up. In the past, the great fear was a complication known as sympathetic ophthalmitis, in which disturbing the lens of one eye would set up a sort of allergy which could also make you blind in the other, good, eye.

|
| Spitfire |
In the famous Battle of Britain in the Second World War, the British pilots to whom so many owe so much were covered with a plexiglass canopy in a fighter plane called the Spitfire. Enemy machine gun fire would often shatter this canopy, and among a lot of other damages, shards of plexiglass got lodged in the eyeballs of the pilots. For the most part, it was left in place because other injuries needed tending more urgently. Long after the Battle, it finally dawned on a British ophthalmologist that this wasn't supposed to happen, it was supposed to cause sympathetic ophthalmitis and the pilots were supposed to go blind. From this, it was finally deduced that plexiglass was safe to use as a lens implant, a so-called "hard implant". You can still see people walking about with these lenses, recognizable because their eyes seem to glow when the light shines into them, like crocodiles along the Amazon at night.
The second step in the migration to modern cataract surgery was the insight that soft pliable forms of plastic retain a memory of the shape they were molded into. So, the old lens can be scooped, lasered or sucked out of place, and a squeezed-down soft lens can be shoved into the vacated space. Retaining its shape-memory, it springs back into the correct shape for a lens, and you are all set.
And finally, there was the stitch. If you cut into the side of the cornea, you have to stitch it up after you are through. And then later you have to remove the stitch. An eye surgeon who should be more famous if he were more popular then invented a form of curved incision which did not requite a stitch because the pressure within the eye held it closed. It was a simple and brilliant idea, which took scarcely a few extra seconds but eliminated one of those sources of complications which dogged the statistics. There was only one problem. This surgeon decided to apply for a patent for his invention, and the medical world had a fit; not only did he patent the curved incision, but he also sent bills for royalties to every eye surgeon he could prove was using it. I happened to be seated the House of Delegates of the American Medical Association when this matter came up, and the uproar was considerable, including some ribald limericks which were read the House "as a matter of personal privilege". Shortly afterward the courts did the right thing and disallowed the patent.
So that pretty well summarizes how cataract surgery became a modern miracle, with a great many elderly people now playing demon bridge when they would otherwise be fed with a spoon. Somehow, the national gratitude is not quite equal to its obligations, and we hear people grumble that eye surgeons make too much money. When the achievements of politicians match those of the average eye surgeon, perhaps they will have a point. But not sooner.
But I'm allowed to complain, and perhaps obliged to issue a warning to my fellow elders about the true source of our discontent. It seems to start with eye drops, but it's more than that. There's a simple technique for instilling eye drops, which involves pulling down the lower lid, creating a pocket, and putting the drop in the pocket, after which the subject blinks his eye and spreads the drop around. Works slick takes no extra time, and little trouble. And while a half-dozen nurses put drops in my eye, and must put fifty drops in fifty eyes every day, not one of them did it right. The drops were spattered on the eyelids and eyelashes, much of them running down my cheek. One extra-large nurse with an attitude put her thumb on my upper eyelid and spread the lids so painfully apart that I cried out in protest. It's supposed to hurt, was the unwelcome answer. I resolved then, and soon carried out the threat to scold the surgeon and the Physician-in-Chief about the responsibilities of supervision, but there are two other more serious issues behind this indignity.
In the first place, the reimbursement mechanisms were modified so that hospitals were no longer paid for maintaining a school of nursing. Within a few years, all hospitals had trimmed this expense, and nurses went to college to be trained in nursing, miles away from the nearest hospital, and eventually trained by other nurses who had themselves had scant experience with patients. Although it is boasted that they now have bachelor's' degrees instead of mere diplomas, their skill with patient care is far inferior to that of the generations which went before them. Instead of being well trained, they are rule-ridden.
The other underlying issue lies with us, the patients. In France people retire at fifty I hear, and in this country, we retire at sixty-five. But we sit around, essentially quite healthy, until eighty-five or later. Everybody knows we have nothing important to do, so they waste our time. Or rather, whenever there is a choice of wasting a minute of working-person's time or an hour of a retired person's, it is the retired person who is dumped on, and it's only going to get much worse with time. Hey, folks, it's degrading to be so useless. Go to work and accomplish something. Don't let the younger generation treat you like logs of wood.
Christmas Reflections (Podcast)
Lazaretto

|
| David Barnes |
DAVID Barnes, professor at the University of Pennsylvania, kindly visited the Right Angle Club with an interesting talk about the Lazaretto, the oldest quarantine station in the Western hemisphere, and the sixth oldest in the world. It was built in 1800 responding to the Yellow Fever epidemic of 1793, followed by those of 1797, 1798, 1799, 1820, 1853, and 1870. If an incoming ship had a case of Yellow Fever on board, the patient was institutionalized at the Lazaretto and the ship captain had to pay for the care until the patient recovered, or until he didn't. Since we now know that Yellow Fever is transmitted by mosquito bites, it probably didn't do much good, and by locating the Lazaretto in a swamp, it may actually have promoted the spread of the disease. It thus fits into the story of Dr. Benjamin Rush hastening the death of his Yellow Fever patients by bleeding them of several pints of blood, as well as the construction of the Philadelphia Water Works to purify the drinking water, which we can now she had nothing to do with the disease, either. However, the waterworks were a marvel of engineering and must have saved many lives from Typhoid Fever. As recently as 1970, I can remember cases of anthrax being brought to the port on Pakistani ships, so quarantining and quarantine stations are useful ideas, some of the time.

|
| Philadelphia Lazaretto |
The first Lazaretto was built on the Aegean Sea at Venice, around 1450. There is some dispute about the name, which is said to come from the patron saint of lepers, St. Lazarus. The followers of St. Nazareth maintain the present name is a corruption of Nazaretto however, since St. Lazarus was the name of the church on the island where it stands. It seems most likely that the original Venetian quarantine hospital was responding to the plague, which would have benefitted greatly from isolation, although the rats and mice probably quickly found a way around their problem. Benjamin Rush thought that Yellow Fever was transmitted by the overpowering stench of rotting coffee beans, which is quite wrong as Walter Reed later showed, but at least it would lead to the idea that quarantine might be useful. Historically, the rumors and suppositions about this matter were useful to the Virginia delegates to the Constitutional Convention, who used it to promote their campaign to move the national capital to Washington, D.C.
The Schuylkill empties into the Delaware River at a sharp bend in Delaware, which slows the river and causes silt to be dumped there. William Penn had earlier decided to locate his new colony at Chester, just below the bend. However, he soon saw that it was more defensible to locate Philadelphia on the upstream side of the mud flats, as it proved to be in the Revolutionary War. Fort Mifflin was located just above the mud flats and could be kept supplied by flatboats coming down the Schuylkill from Valley Forge and Reading, the arsenal city of the Revolution. On Benjamin Franklin's suggestion, the channels between the mud flats were blocked by the chevaux de fries, underwater spiked contraptions which were much like the blockages to the entrance of parking lots. On the Jersey side of Delaware was Ft. Mercer at what is now called National Park. It was a formidable defense which almost ended the War by starving the British troops who had occupied Philadelphia from the rear via Germantown but were long unable to get past Fort Mifflin with their fleet, coming upriver. Most of South Philadelphia was a swamp, and there are many reports of flocks of swans paddling around the entrance of the Schuylkill. Hog Island became a shipyard, then a Naval Base. And then the airport was built on the mudflats, pretty much-obliterating everything else. There is the talk of making this area into the main intermodal transportation hub of the east coast, since ocean shipping, air transport, interstate highways, and railroad are all crowded together, quite close to the urban centers.
|
| Benjamin Rush |
Benjamin Rush, a signer of the Declaration of Independence, was still active at the Pennsylvania Hospital in 1800. It was still the only general hospital in America and the model for much of subsequent American medicine. One striking memento of that connection at the Lazaretto is the cupola on the center building, which is very similar to the cupulas on the roof of the building at 8th and Spruce Streets. The brickwork is also Flemish bond. The ten-acre site of the Lazaretto is very accessible, except perhaps for the suspicious Tinicum Township police. However, it has long been a tradition to have a banquet and picnic at the Lazaretto at the beginning and end of the quarantine season, roughly June 1, and October 1. Yellow Fever shots are not required.
Wistar Institute, Spelled With an "A"

|
| Dr. Russel Kaufman |
The Right Angle Club was recently honored by hosting a speech by Dr. Russel Kaufman, the CEO of the Wistar Institute. Dr. Russel is a charming person, accustomed to talking on Public Broadcasting. But Russel with one "L"? How come? Well, sez Dr. Kaufman, that was my idea. "When I was a child, I asked my parents whether the word was pronounced any differently with one or two "Ls", and the answer was, No. So if I lived to a ripe old age, just think how much time and effort would be wasted by using that second "L". In eighty years, I might spend a whole week putting useless "Ls" on the end of Russel. I pestered my parents about it to the point where they just gave up and let me change my name". That's the kind of guy he is.

|
| The Wistar Institute |
The Wistar Institute is surrounded by the University of Pennsylvania, but officially has nothing to do with it. It owns its own land and buildings, has its own trustees and endowment, and goes its own academic way. That isn't the way you hear it from numerous Penn people, but since it was so stated publicly by its CEO, that has to be taken as the last word. It's going to be an important fact pretty soon since the Wistar Institute is soon going to embark on a major fund-raising campaign, designed to increase the number of laboratories from thirty to fifty. The Wistar performs basic research in the scientific underpinnings of medical advances, often making discoveries which lead to medical advances, but usually not engaging in direct clinical research itself. This is a very appealing approach for the many drug manufacturers in the Philadelphia region, since there can be many squabbles and changes about patents and copyrights when the commercial applications make an appearance. All of that can be minimized when fundamental research and applied research are undertaken sequentially. Philadelphia ought to remember better than it does, that it once lost the whole computer industry when the computer inventors and the institutions which supported them got into a hopeless tangle over who had the rights to what. The results in that historic case visibly annoyed the judge about the way the patent infringement industry seemingly interfered with the manufacture of the greatest invention of the Twentieth century.
Patents are a tricky issue, particularly since the medical profession has traditionally been violently opposed to allowing physicians to patent their discoveries, and for that matter, Dr. Benjamin Franklin never patented any of his many famous inventions. But the University of Wisconsin set things in a new direction with the patenting of Vitamin D, leading to a major funding stream for additional University of Wisconsin research. Ways can indeed be devised to serve the various ethical issues involved since "grub-staking" is an ancient and honorable American tradition, one which has rescued other far rougher industries from debilitating quarrels over intellectual property. You can easily see why the Wistar Institute badly needs a charming leader like Russel, to mediate the forward progress of our most important local activity. From these efforts in the past have emerged the Rabies and Measles vaccines, and the fundamental progress which made the polio vaccine possible.
It was a great relief to have it explained that there is essentially no difference at all between Wisters with an "E" and Wistars with an "A". There were two brothers who got tired of the constant confusion between them, see and agreed to spell their names differently. When the Wistar Institute gathered a couple of hundred members of the family for a dinner, the grand dame of the family declared in a menacing way that there is no difference in how they are pronounced, either. It's Wister, folks, no matter how it is spelled. Since not a soul at the dinner dared to challenge her, that's the way it's always going to be.
"They Don't Make That, Anymore"
They Don't Make That, Anymore These words from the nice young lady in the drug store, left me astonished, baffled, bewildered, and angry.
Although I am retired from the practice of medicine, my limited license permits me to prescribe ethical drugs for myself. I had not realized, until that very moment, that to some extent it also isolated me from the experiences of my fellow patients. Let me explain.
The drug involved was tetracycline, which I had surely prescribed a thousand times, and to which I had a sort of loyalty growing out of the fact that I took it myself. In the days when I was a college student, I came down with a form of pneumonia that involved a lot of coughing, like whooping cough. It was then called virus pneumonia because it was somewhat different from ordinary pneumonia, even though it was called Primary Atypical Pneumonia in polite academic circles. Eventually, we learned that its cause was neither a virus nor a bacterium, but rather something in between in size, called Mycoplasma. All of this is important to know, because it tends to appear as a question on a certification examination, but the fact of the matter is, it was a disease for which there was no effective treatment. We could cheer up a little to know that of four hundred recruits at an Alabama training center who came down with it, only one died. On the other hand, Legionnaire's Disease is also caused by a Clamydia and lots of them died, probably because most of them were older. But no matter, in 1944 there was no treatment, and I can tell you it is very unpleasant for a very long time, no matter how young you are.

|
| CAT Scan |
In 1950 I got it again, but this time I was a doctor and knew there was a good treatment. It sounds strange to say so, but I was sort of happy to be able to try out the new medicine, which was then called Aureomycin because the powder was golden yellow. Aureomycin was a trading name, with a patent, and when the patent expired the generic form was called Tetracycline. It worked just fine, and in three or four days I was out of the hospital, perhaps a little weak and shaken, but cured. Incidentally, I discovered an interesting feature of the disease which I believe has not been previously reported. It had long been observed that the chest x-ray showed pneumonia while the stethoscope perceived very little abnormality, a feature which disconcerted those of us who were concerned with the cost of medical care, particularly members of a generation who felt sniffy about the dependence younger physicians displayed for x-rays, and nowadays for CAT scans and MRIs. Unfortunately, in this particular instance, x-rays are clearly superior to stethoscopes.
My third time around for "viral" pneumonia was a few years later; I was sitting on a park bench near the hospital when I recognized the old symptoms were coming back again, so I went straight to the x-ray department and had a chest x-ray less than an hour after the symptoms appeared. I planned to have an x-ray to prove it, go get some tetracycline and be all better over the weekend, with a rollicking anecdote to tell doctor friends about. Unfortunately, the x-ray was normal, so I was admitted into the hospital to see what was wrong. The next morning the x-ray showed a densely consolidated lung, so it had been viral pneumonia all along. And so my old prejudices were vindicated; it was possible to be too quick to order x-rays after all. Unfortunately, the extra twelve hours without treatment allowed me to get a lot sicker than I had to be. I think I know this because, doggone it, I developed the same disease several decades later, took no shortcuts to the drug store, and was fine in a couple of days after I immediately started taking tetracycline. You could say this strange recurrence of Mycoplasma pneumonia over one-lifetime sort of illustrates how medical care of the disease has become progressively cheaper. Instead of a month in the hospital with no treatment, it was now a matter of skipping the stethoscope, skipping the x-ray, skipping the hospital, and just swallowing some cheap tetracycline capsules. You have to have the nerve to do it, of course, and ethically you probably only have a right to do it to yourself, knowing the risks and being willing to accept them. There is, however, one flaw in this story.
When Aureomycin first emerged from the clutches of the FDA (and well before that accursed Kefauver Amendment), it seemed astonishingly expensive. Because I knew what it weighed (250 milligrams per capsule), and I knew what gold cost ($35 an ounce), it was easy for an idle mind to calculate that Aureomycin cost more than gold. Gold now sells for $1700 per troy ounce, so you could take this story in the direction of inflation. I rather prefer to take it in the direction of nominal dollar amounts, because Aureomycin retailed for $5 a capsule the third time I had the disease, and $1 per capsule when it lost its patent and became tetracycline. The fourth time I had the disease, I bought a container of fifty capsules for 76 cents. But as you have already heard, by the fifth time I couldn't buy it for any price, because everybody had stopped making it. Since my view of the economics of useful commodities is that low prices will only cause shortages if there is artificial market interference, the usual cause of shortages is rationing. Somebody who understands the 2500 pages of Obamacare better than I do will have to tease out the way rationing has caused shortages of tetracycline. And when they are done confusing the public, let them explain why you also can't buy KMnO4 crystals (potassium permanganate), which has cured more cases of athlete's foot for twenty cents, than all those cans of stuff in spray canisters.
Psychiatry: Last Cow in Philadelphia
The present problem with PSYCHIATRY can be summarized as follows: At the suggestion of the American Hospital Association, Congress introduced the DRG system of paying for inpatients by diagnosis, rather than itemized services. It worked well except for psychiatry, where the diagnosis usually implies little relation to the later costs it generates, so an exception was made. The dual system of payment created loopholes which unfortunately overpaid psychiatric hospitals and were described as exploitation. Congress over-reacted in a way that was unsustainable, and essentially all of the psychiatric hospitals of the nation were forced to close. This is not a history for anyone to be proud of, and the lack of outcry is also a disappointment. However, after twenty years without reform, evidently, nothing is going to be done without an outcry.CONVENE BLUE RIBBON COMMISSION TO REPAIR PSYCHIATRIC INPATIENT CARE. The 1983 BRA switched hospital inpatient reimbursement to payment by diagnosis (DRG). Abuse of the psychiatric exclusion then led to "corrective" legislation which has essentially reduced American's psychiatric inpatient care to an underfunded national disappointment. The problem is not an easy one, so a commission should devise a workable methodology for psychiatric hospitals, relying neither on present approaches nor on DRG. But overpayment is a better outcome than no care at all. Homeless people sleeping in cardboard boxes on downtown steam grates are the consequence any visitor to the area can observe at night after the commuters go home. Psychiatric social workers readily recognize their daytime patients in the boxes.
* * * * *

|
| Daniel Blain, M.D. |
Daniel Blain, M.D. (1898-1981) was just about the most important psychiatrist in America. He was the Physician in Chief of the Institute of the Pennsylvania Hospital at 49th and Market, the first and in many ways the most prestigious psychiatric hospital before it was closed. Before that, he was the first Medical Director of the American Psychiatric Association, itself the first (1844) medical society in America. His fame rested on organizing the disorganized psychiatry of the Veteran's Administration into a chain of advanced "Dean's Hospitals", a huge and very important achievement. Before that, he had achieved considerable fame as the man who took the dilapidated State Psychiatric Hospitals with a reputation as "snake pits" and made them a respectable part of the medical community. And before that, he had been born in China as the son of missionaries. As a matter of fact, even before that, he was a descendant of General Mercer of Revolutionary War fame.
Dan was an outstanding example of the peculiar fact that Psychiatry was dominated by social upper crust psychiatrists in Philadelphia for a very long time. In fact, Benjamin Rush of the 8th Street branch of the Pennsylvania Hospital is known in some circles as the "Father of Psychiatry", while in other circles he is known for signing the Declaration of Independence. That isn't true in other cities, and it definitely isn't true in New York City, where the psychoanalytic school of Sigmund Freud took that city by storm, and essentially drove every other school of psychiatric thought out of town, out of medical schools, out of psychiatric hospitals. The famous sixteen-year psychoanalysis of Woody Allen is an example of the extremes of that fad. Every profession has petty civil wars of that sort, best left undiscussed in public. But in the case of psychiatry, it was indirectly a material contributor to the present disappearance of inpatient psychiatry, and the related appearance of lots of homeless people on steam grates. Let me give a biased view of what is a massive human tragedy, which someone else can "rectify" if he chooses.
|
| APA |
It starts with a Budget Reconciliation Act of the 1980s, which brought us the DRG (Diagnosis-related) system of paying for hospitalized patients. The idea was that appendicitis resulted in essentially 7 days in the hospital, give or take a couple of days, and the bills for admission for appendectomy were for more or less the same amount. If you had fifty or a hundred cases a year in your hospital, the high bills balanced the low bills, and the overall hospital reimbursement was essentially the same without itemizing the bandages and whatnot. Congress bought this package, and after it got going, just about all hospital bills were reimbursed at one of three hundred prices, the cost to the government was the same, and there was a whole lot less bookkeeping and accounting cost. It was a success, except for a few cases where the costs did not closely line up with the diagnosis, and psychiatric hospitals were where they concentrated. So, psychiatric hospitals were excluded, and psychiatric bills skyrocketed. This experience has been carelessly cited as an example of the evils of payment by service ("fee for service"), when in fact the duration of psychiatric hospitalization is related to features of the condition, like danger of suicide, rather than the diagnosis itself. Psychiatric leadership at the time contained many in a subset of physicians who did not think much of inpatient psychiatry in the first place and even less of lobbying, and they underestimated the severity of the assault on the specialty. Apparently, no workable formula for pricing inpatient psychiatry has since been brought forward to be approved by a Congress which is more accustomed to getting its lobbying in the form of one-liners. And would you believe it, psychiatric inpatient care soon disappeared.

|
| Pennsylvania Hospital |
That's right, if someone in your family needs psychiatric hospitalization, I wouldn't know where to tell them to get it -- at any price. From considerably overpaying for psychiatry inpatients to paying scarcely anything for them, this little change of the regulations caused every psychiatric hospital I know of by name, to close. It helped balance some state budgets, but it also was a considerable factor in filling the steam grates of American cities with people who sleep on cardboard boxes. And what it illustrates is that this is what political society always seemed to do, before Dan Blain and a small group of upper-crust psychiatrists were temporarily able to shame them into something better. In fact, if there is any tattered remnant of good inpatient psychiatric care left in America today, it is in the Veterans Hospitals that Dan was able to straighten out.
Dan Blain will probably eventually be bypassed as a curiosity, like his wife. She was a Wister Logan Blain, descended from families who ruled Philadelphia a hundred years before even General Mercer came along. So the Blain couple lived on an enormous farm plot, centered at 20th and Olney right next to LaSalle University, which is built on their property. It also contains the Peale House, where Charles Willson Peale lived as the elected president of the rebel faction of the American Revolution. Peale didn't know what he was supposed to do, so he resigned and painted portraits of people. The Blains enjoyed keeping a cow on their land, the last cow in Philadelphia, and the LaSalle students enjoyed stealing the cow and leaving it on the top floor of a dormitory, for laughs. Meanwhile, the Blain couple had cocktail parties on their front porch for visiting dignitaries. They usually wore blue jeans, and Mrs. Blain, the absolute Queen of Philadelphia society, was occasionally observed to pour vodka into her glass of beer. That sort of background may well have been useful when psychiatry needed to be built up and humanized, but it became a liability when the rest of inpatient psychiatry failed to appreciate what was knocking on its door.
| Posted by: Karen Lawrence | Jun 12, 2017 11:20 PM |
| Posted by: Karen Lawrence | Jun 12, 2017 11:20 PM |
| Posted by: Karen Lawrence | Jun 12, 2017 11:09 PM |
20 Blogs
Funny Toes: A Physician Viewpoint
Most people either ignore funny toes, or hide them in their shoes. Here are one doctor's idle thoughts about them.
Link to PHILADELPHIA PHYSICIANS
.
Link to:Medical Club of Philadelphia
In 1992, it's Executive Director summarized the century-long history of this last surviving club of physicians, devoted exclusively to non-medical affairs.
Cost Shifting: Indigent Care Out, Outpatient Revenue, In
 Hospitals probably shift costs ten or more ways; here are three ways. Picture yourself as a Congressman trying to modify this mess, and then you try to do it in a couple of weeks. Probably Galen, not Hippocrates, first said Primum non-nocere -- don't make things worse.
Hospitals probably shift costs ten or more ways; here are three ways. Picture yourself as a Congressman trying to modify this mess, and then you try to do it in a couple of weeks. Probably Galen, not Hippocrates, first said Primum non-nocere -- don't make things worse.
Cataracts
 The modern miracle of cataract surgery began when a Messerschmidt fired a machine gun into a Spitfire, during the Battle of Britain.
The modern miracle of cataract surgery began when a Messerschmidt fired a machine gun into a Spitfire, during the Battle of Britain.
Inside the Big House
Medical care inside a prison is some sort of extreme case of government health care.
Reforming Health Reform, New Jersey Style
U.S. Representative Robert Andrews (D, NJ) had a night he won't soon forget on August 24, 2009. Facing 3000 constituents angry about Health Reform, he practically had a public stoning.
Time To Care
A physician who practiced for sixty years, before and after Medicare, has a lot of stories to tell about how Medicine has changed and been changed.
Only Three Things Wrong With American Healthcare
What needs to be fixed in American healthcare can be very simply stated as three fundamental problems.
...
Christmas Reflections
It once was a tradition to go back to the big city for Christmas shopping..
Lumpers In Constant Combat With Splitters
 The home dinner table is no longer the place most families teach the rules of conduct to each other, probably because of the invasion of homes by television. But there are places where friendly debate is still conducted and social issues are settled. In Philadelphia, newcomers are still taught what's what, in this manner.
The home dinner table is no longer the place most families teach the rules of conduct to each other, probably because of the invasion of homes by television. But there are places where friendly debate is still conducted and social issues are settled. In Philadelphia, newcomers are still taught what's what, in this manner.
Atlantic City, Brigantine and the N.I.H.
Great scientists in crowds look and act pretty much like everyone else.
Cataracts and Deference to Seniors
Cataract extraction is now the commonest surgical operation in America. It doesn't receive the deference it deserves.
Christmas Reflections (Podcast)
George Fisher narrates one of his favorite reflections, "Christmas Reflections," on the changing face of Christmas and Christmas shopping in Philadelphia.
Lazaretto
The oldest quarantine station in the Western hemisphere is located next to the airport on Tinicum Island, quite easily visited by car. It dates from Philadelphia's famous Yellow Fever epidemics of 1793.
Wistar Institute, Spelled With an "A"
The Wistar Institute is properly pronounced "Wister", but in fact it's all the same family. Its fame in biomedical research makes that quite irrelevant.
"They Don't Make That, Anymore"
 Pharmaceutical drugs seem to follow a trajectory of fifty years, from new and expensive, to cheap, old and eliminated.
Pharmaceutical drugs seem to follow a trajectory of fifty years, from new and expensive, to cheap, old and eliminated.
Psychiatry: Last Cow in Philadelphia
Daniel Blain, just about the most famous psychiatrist in America, lived at 20th and Olney, West. Not only was that the place he lived, but he also kept a cow there. And this was within living memory.