There are other ways to support retirement, but most retirement plans before the public are based on the insurance model.
Here are some insurance-like ideas to add to the discussion. The longer we dither, the more we get driven toward ways to have many healthy people support the cost of a few sick ones, the insurance model. We need a better balance. Curing disease lengthens longevity, but it also provides more opportunity to get sick again. We can't be sure what that will do to overall costs. The possibility exists that research has first selected the low hanging fruit. That is, treatment and research for the few remaining diseases may become progressively more expensive, thereby increasing costs as fast as, or faster, than extended longevity reduces them. We are forced to gamble that curing common diseases will further reduce costs, knowing it may not. Among other things, we need to make extra longevity more worth-while.
Study of Health Savings (and Retirement) Accounts was begun thirty years ago, increasing rapidly in the past five years. During that time, paying for unknowable health costs emerged as the central concern. At a recent Congressional hearing, the actuary testified his estimate of the first ten years of costs for "Medicare for everybody" to be 40 trillion dollars in addition to present costs, which will themselves require additional revenue in 5 or so years to avoid bankruptcy. Retirement costs would require even more additional revenue. Furthermore, it would take at least five years to make such a massive transition, possibly ten years.
This emergency testimony before the "Speaker's Rules Committee" seemed to be Nancy Pelosi's signaling we should lower our sights on such impossible spending proposals, no matter how many Democrat candidates for President endorse them. Paying a big chunk of health costs would be a significant achievement, paying for two issues simultaneously might just be an impossible dream. Nevertheless, paying for the whole healthcare system was something the public expected to happen quite soon, and would punish the ruling political party if it didn't sacrifice everything else to achieve it. We might afford to leave Medicare alone. But when eventually Medicare came into focus as the main impediment to solving a double problem for exactly the same age group; "saving" it becomes a relatively minor issue. New revenue must be found, the quality of care must not be injured, and -- most of all -- public opinion must be satisfied. This is a specialist's game, but avoidance of a disappointing outcome is becoming a decisive player. As Congress dithers, it only becomes clearer that deficit financing from foreign enemies cannot continue much longer.
Resource Assessment. Adding up all the economies of Health (and Retirement) Savings Accounts, but now also including the retirement costs, the conclusion is left that HSAs might somehow pay for health costs, plus some but not all retirement costs. Much of the shortfall comes from difficulty stating a "decent" retirement payment which would satisfy most people. What is enough for a Trappist monk is not enough for a movie star, and what will be called decent in 60 years is pretty hard to say. So at most, we should aspire is healthcare plus some retirement; supplementing retirement as we can. Even promising that much is a stretch, but is certainly superior to government healthcare plans without the discipline of individual ownership. Unfortunately, that forces the individual to some choices he must make for himself, versus allowing some big anonymous corporation to do it all for him at a hefty administrative markup. Let's specify the two big dangers the individual must navigate:
Imperfect Agents Theoretically, even the best anyone could provide from HSAs (we jump ahead, here) would be to give a newborn baby a couple of hundred dollars at birth, let a big corporation do the saving and investing, and pay out a million dollars for medical bills (that's what total health costs over the next ninety years might cost} on his behalf, at no charge. The long investing period could provide some astonishing returns, but it would not be entirely carefree for the customer. For example, it might actually cost that much, not just be borrowed with every intention of defaulting on the loan.
Unfortunately, experience over thousands of years has demonstrated agents -- especially governments--will eventually extract much of the resulting profit for themselves. Countless kings have been known to shave the edges of gold coins, some of them have been found to have employed inflation of the currency to pay their own bills. Investment managers are almost invariably well compensated, usually for mediocre returns, so this cost must be automated with index funds. William Penn, the largest private landholder in history, was put into debtors prison by his wayward agent, as was Robert Morris, the financier of the American Revolution. Whole-life insurance companies are the closest approximation of an agent for a Health Savings Account who might propose to get paid a level premium for decades before paying out a benefit for a dead client. They seem to survive by promising a single defined fixed-dollar benefit and counting on inflation to work for them as it sometimes does for dictators, overseen by an honest insurance commissioner. Unfortunately, they have the moral hazard of falling back on other surviving firms to bail out bankruptcies, and the political hazard of trying to force premiums downward for the taxpayer without reliable benchmarks or overgenerous recompense. Just how much they have been rescued by lengthened longevity is something only an actuary knows. Long ago, the imperfect agency situation was summarized by the question, "And where are the customers' yachts?"
Inexperienced Solo Management. If Warren Buffett had an HSA, he would have no problem managing it, and neither would a great many other savvy folks. The problem is to make the management so simple and standard that expenses can be kept low without injuring investment returns -- for the average citizen. This consideration almost drives the conclusion that lifetime health costs might be best divided into at least three component parts, with benchmarks and averages published regularly, since the medical and beneficiary problems divide into the same three (childhood, working age, and retirement) components. It begins to look as though a new profession of fee-for-service advisors needs to become educated and distributed widely, perhaps in local bank branches. As will be described in later sections, the need is for the income stream to be kept in balance with the probable expenditures, adjusted for inflation or deflation. It is not, to achieve the maximum possible revenue return, regardless of risk. That is to say, the purpose of the HRSA is not to make as much money as possible, but to be sure as much medical need as possible can be satisfied by the revenue available. Let's put it all in a nutshell: There's a big difference between designing a system to cover a public need inexpensively -- and designing a business model to make a profit. But even that's not nearly as big a problem, as trying to do both at the same time.
After Assessing Obstacles Comes Strategy. Most HSAs make payments with a debit card suitable for passive investing (utilizing total market index funds) for inexperienced investors and for otherwise undesignated accounts. However, there's a technical problem: the earning period is not the first stage of life; it's the second, following nearly a third of life in childhood and educational dependency or debt. Health expenses in the childhood third of lifespan may be comparatively small, but the earning capacity is essentially zero. This unconquerable fact leads to splitting investment considerations into three stages, the first and last thirds subsidized by the middle one. The result is, two systems feeding off the middle third in opposite ways, requiring opposite approaches, and jumping between generations. Somehow, it must all come out in balance at the end. And remember, it starts with a deficit in the obstetrical delivery room unless we re-arrange something else. There is no choice but to take things one at a time.
If you spend too much too early, you won't have anything left for later.
On his 66th birthday, a Health Savings Account owner has only one choice at present: to turn any surplus from healthcare into an IRA (Individual Retirement Account), for taxable retirement living. However, that's a step better than Medicare or employer-based insurance alone, which return unused surplus to the donor of the gift, either the government or the employer, in the guise of the reduced premium cost. However, economists agree the salary soon adjusts downward to treat the confidently expected gift, as part of wage costs. Therefore, health insurance is more expensive than it would be if the surplus were returned to the beneficiary directly. These forms of health insurance have been dominant so long, everyone feels they describe necessary features of health insurance, rather than terms of a contract negotiated by parties other than the beneficiary.
The presumption is made the individual has Medicare, so any accumulated surplus in his HSA needs to be spent after age 66, but not on health, since he assumes he will then be completely covered. This presumption is strengthened when the employees of a group plan are merged into a group, but quickly emerge when transfers are made. So any surplus is an average of the group, not specific to the individual. Data is not available to determine whether the size of this issue is enough to worry about. But a pathway probably was not created for overfunding Medicare to create retirement savings through employer-based insurance. In the first place, the surplus does not exist. In the second place, any surplus was probably expected to flow back into Medicare to reduce its cost. In 1965, it was probably expected that Social Security would fill this need, but increasing longevity has created resistance to enhancing all entitlement programs. It scarcely matters, today.
However, if changes in laws and regulations would make it possible, there might be other choices, one of which would be to overfund Medicare coverage, continue the HSA, and spend the generated surplus on retirement. But notice this: as things stand, if you don't need Medicare anymore, you don't get anything back and the government can spend the surplus on battleships. Just as, in plain fact, a commercial insurance company can spend a surplus on executive salaries. It's not fair to say Medicare will "never" have a surplus. By design, any surplus will always be used for healthcare, because that's thought to be part of "share the risk". It's a design feature common in sharing the risk programs, although not a devastating one.
In short, the designers of Medicare never imagined it would run a surplus, and at present, it is far from it. But in the long, long run, scientists will eventually cure those chronic diseases of the elderly, and then there might actually be such a surplus. It is already clear things are moving in the direction of making Social Security a larger if not more important program than Medicare -- in the short run -- and could largely replace Medicare, in the long run. Because expensive illness is often fatal illness, a great many people do not survive it. So, one ray of hope in this situation is that relatively few people will have both devastations, so the future is probably one expensive entitlement transforming into the other with relatively little overlap. In that case, dual catastrophes are best addressed by insurance. With luck, the people who drop dead without warning or cost will equal the number of overlaps, smoothing down national expense to only two groups, which eventually merge into one as science merges chronic disease into the growing group whose problem is outliving their savings. There are other ways of approaching that problem, but at least a flexible health program could provide a source of funding for it and a general outline of where it might be headed. Notice that compound interest works in favor of this solution, and could be an important component. In fact, unknown treatments will increase future expense, but by definition are not counted. Therefore, statistical projections can show a revenue surplus after the age of 90, which may in fact never materialize.
Therefore it would be easier to pass a seemingly meaningless amendment, right now, while it doesn't cost anything. We've just shown how HSA does it, and Medicare could do it too if it tried. The more likely circumstance would be to get a reduction of either payroll deductions or Medicare premiums in return for surrendering some particular benefit, like transfusions for members of Jehovah's Witnesses. At the moment, religious objectors cause lawsuits and other commotion, just because they don't want some particular feature of health insurance, and actually I can think of no reason why we should make it mandatory. In fact, doing things for someone's own good is a suspect idea, generally.
The long-range reasoning, however, is this: in 2015 the great need is for flexibility. Some of us will need to spend every dime we have on staying alive. And some of us will need to save every dime we can, in order not to outlive our retirement funds. But that probably won't be the same dilemma, fifty years from now. Almost every one of us could be threatened with poverty during extended retirement into undefinable longevity. It strains the imagination to think of ways to pay for both the present elaborate Medicare and an extended retirement in addition. So, by that time, I fully expect people to have come to the realization that Medicare must be liquidated piece by piece. Not to fund Obamacare, but to pay for their own retirement. When you go to a funeral every week, the idea doesn't usually occur that dying too early might ever become a thing of the past.
Neither employer-based nor Medicare returns an unused surplus to subscribers.
For one thing, I expect "rent-seeking" to soak up a lot of the savings from people not getting quite so sick. Rent-seeking will take many forms, like Botox injections and cosmetic surgery. Or like elaborate hospital equipment and excessive salaries, or like too much stand-by but essentially unused equipment. It may sometimes be hard to tell where the money is going, but costs will surely fail to fall as rapidly as illness can disappear. We will need a way for people to perceive this, and for them voluntarily to start saving for it by gradually opting out of Medicare. It won't be an all-or-none issue; people will perceive it at different rates. Therefore, we need to provide a way to get out of Medicare in steps, and individually one by one, over a period of decades. For political reasons, the use of a surplus should be limited to your own retirement living. All of this is called "planning ahead".
Proposal 1:At present, Health Savings Accounts are limited to age 21-66. There should be no age limits at either end, and some provision should be made for inheritance of surplus to newborn children, sufficient to cover their healthcare up to age 21. (3320)
Proposal 2: At present, contributions to Health Savings accounts are limited to $3500 per year, age 21 to 66. This should be changed to an aggregate lifetime amount, at least until latecomers have had an adequate transition to the program. (3320)
Health Savings Accounts provide the flexibility to do this, but at present many Medicare program details are awkwardly designed to anticipate the need. Right now, the program is not sufficiently modular to permit dropping one feature but retaining others and letting the funds follow the needs. And designing partial proposals is inhibited by a political terror that the public will misinterpret motives. So the first step is for people like me, who have nothing to lose, to step forward and start talking about it. The need for retirement money is looming ahead; we need to prepare Medicare for gradual liquidizing, to pay for it.
The first step is probably to design a way to buy out of Medicare, save some money by substituting an HSA for their healthcare, and buy something more appealing with the surplus. The first version will probably be crude and awkward, but it provides a platform to build on. Most politicians, whatever they may think of Medicare and its financing, regard talk of privatizing Medicare as political suicide, so we should be thinking of pilot studies, think tanks, and experimental projects. The old folks who have, or will soon have, Medicare coverage regards it as such a treasure, they tell their elected representatives that privatizing Medicare is the third rail of politics: touch it and you are dead. But a Washington sage once remarked that if things can't go on, they will stop. So, what would it require, induce potential Medicare beneficiaries to select something else, before circumstances abruptly force it on them?
That's probably not the best way to go about it. The early initiatives should be generated by scientific advances. The likelihood is great that science will cure one or two of the big five (cancer, diabetes, Parkinsonism, Alzheimer's Disease, schizophrenia) and bit by bit, Medicare will get cheaper in spite of the rent-seeking. As it does, it will seem attractive to increasing numbers of people, to consider cheaper health insurance, shifting Medicare funding to retirement income. The rules should be relaxed to let early-adopters test the changing environment. We already have a flexible funding vehicle in Health Savings Accounts, and fifteen million existing subscribers who will endorse it.
The Problem With Medicare. Medicare is 50% self-funded by payroll deductions and premiums and is 50% subsidized by the federal government. The old folks get a dollar for fifty cents and are not about to give it up. They obviously should get their own fifty cents back. It's the fifty cents of government subsidy which is at issue, and the published budget should reflect that fact. Just notice how retirees display almost no interest in the Obamacare controversy, except for one thing. Old folks are uneasy that funding for Medicare might get squeezed in order to finance Obamacare, particularly if the two were in the same budget compartment. When the conversation gets around to that point, retirees suddenly wake up and start talking loudly. If the discussion centered on the subsidy, things might subside, somewhat.
But hold on. A retiree approaching his 66th birthday has already pre-paid approximately a quarter of the costs of Medicare, and when he joins, his premiums will later amount to another quarter of the cost. That 50% is the retiree's share of the present costs of Medicare, and naturally, he doesn't expect to see it disappear. The 50% subsidy provided by the government, on the other hand, is what concerns everyone. Even the people who advocate "single payer" systems are talking about extending Medicare to the whole population, gradually perhaps, but probably including the 50% subsidy to everyone. Since healthcare now consumes 18% of Gross Domestic Product, are we willing to see 9% of GDP go from the private sector to the public sector in extra taxes? Or in increased borrowing from foreign nations? We will have to let the politicians wrestle with issues like that, but it will be hard to persuade the public to go along with it.
Meanwhile, let's see what persuasion can do if we offer a good enough deal. For a start, let's presume someone in his late fifties had invested in his HSA while he was young, and is approaching the age where he could augment his retirement income from a substantial balance in his IRA (recently converted from HSA). Then, let us say he also wakes up to the realization he gets a second tax deduction from an HSA if he spends extra retirement money on medical care, either on Medicare payroll deductions or Medicare premiums. And if he stops spending some other obligation, he effectively gets a further tax deduction from spending the money on something else which is tax-free. Potentially, that could add a few thousand dollars a year to his income from age 21 to the day he dies. It's a very attractive goal, and while it really would be legitimately spent on healthcare, Congress might well decide they can't afford to lose that much tax revenue.
So, the rumination goes, the proposal must somehow save some money for the Government, too. If the subscriber were allowed to make a deal to buy out his Medicare, he might make a payment out of his HSA of about $86,000 untaxed, which with 6.5% declining income, would repay the costs of Medicare throughout his remaining life expectancy, all from the invested lump sum. That might seem like enough on paper, but the government has been going in debt for some time to foreigners and would like to stop doing that. If possible, it would like to pay back the earlier loans. If you include this debt, the Medicare cost is revealed as greater than it seems. Furthermore, the GAO will quickly tell you, if you save tax money, you, unfortunately, make it harder to balance the federal budget. The details of all this may be hard to explain, but the general sense of it all is pretty clear.
Let's qualify the simplifications. Different people will have different payroll deductions, at different ages. To some extent, these balance out, because if you have a larger balance in your HSA, you are likely to be older, and likely to have paid more into your Medicare payroll deductions. And to some extent, averages will cancel out and vary with the economy from time to time. A change in the tax code would scramble all of these numbers, but it's preliminary. Medicare is best privatized in pieces, and for that you need prices, so preliminary pricing should be devised for those people who for religious or other reasons, would be interested. Furthermore, accumulating money of this order will require normal interest rates, not abnormally low ones as at present. Since that time is hard to predict, it is necessary to supply minimum interest guarantees, best approximated by index funds of 10-year treasury bonds. Buying out Medicare is a very delicate matter, and should be approached very slowly. The first step is to talk about it without starting a panic. The initial appeal will be found among those who perceive a greater risk from outliving their income than their risk of a major illness cost. They are rare at present, but times will change,
The New York Times devoted an entire issue of its Sunday News of the Week in Review on April 7, 2019, to variations of the theme that "Elderly People Have Surplus Spare Time." Although I have several personal connections with the editors of the Times by marriage, and other connections to the newspaper through Columbia's College of Physicians and Surgeons, I seldom agree with its New Yorkerish hunt for evil from greedy enemies. But this particular attack struck me as right on the mark. Sympathy with downtrodden unions has led to commercial forces preferring fragile cheap products needing to be replaced when broken, discouraging home repairing and the ultimately of the population's ability to repair. At the same time, a lot of old folks have time on their hands and limited opportunities to supplement their retirement income, even ultimately leading to the disappearance of the needed skills to make simple repairs. The Times doesn't suggest the two unfortunate curable ends of the Industrial Revolution could cancel each other out, but it seems to me they might fit if coaxed.
Apple seems to be the biggest offender, substituting unnecessary cheap electrical connectors for successive versions of expensive machinery. When you need to replace a thousand-dollar computer for its broken ten-cent plastic connector, the commercial motive is obvious to the consumer, and pretty annoying, too. A broken plastic connector isn't worth its twenty-dollar markup, but the expensive computer would justify its connector markup, which ultimately becomes a one-dollar markup for a Chinese imitator. The situation in the computer industry was explained to me in person by Michael Dell. When he had his nineteenth birthday, his mother gave him an expensive IBM portable computer. He took it to his bedroom with a screwdriver and found that not a single component was actually manufactured by IBM. He wrote each individual manufacturer for prices and discovered he could make an imitation (but identical) computer, selling it profitably and ultimately driving IBM out of the portable computer business. Substituting Chinese names for Michael Dell you get quite a different story, which paints quite a different description, about excessive markups by greedy Americans. Nevertheless, the moral I draw is the ultimately self-defeating nature of excessive markups, for commercial unfair motives. Smaaart when you reveal them to friends, but unwise, in the long run.
But buried in all this petty maneuvering is a solid truth. We once had a population which took woodshop in the seventh grade and metal shop in the eighth. for boys. And the girls were learning how to cook and sew in separate rooms. This system needs a little updating, but the point is that these abbreviated courses were adequate to teach the essentials of home repairing to whole generations of the population. You wouldn't need to buck the unions, who proved able to destroy the whole vocational school system of fresh competitors, in order to restore simple home repair to the whole population. The old retired folk could repair the broken plastic widgets in their simple lives. The ladies could cook a little instead of continuing plastic-wrapped dinners they now have more than enough time to play around with. Hardware stores would reappear to satisfy the need for widgets. And the retirees wouldn/t need to sit around for lack of simple things to do. It's a brilliant idea, even if it did come from the New York Times.
A friend of mine, treated as my contemporary but probably only sixty years old, was recently speaking of a club picnic he, unfortunately, wouldn't be able to attend. His mother was now living with him, and since she was 84, obviously neither of them could go to a picnic on a sailing vessel. The club committee, listening to this regret, chuckled that of course, we shouldn't expect him. My thoughts were somewhat different. Since I'm 94 myself, I was wondering if she was available for a date. And of course I am going to that picnic, why shouldn't I?
You can't scare me very much about the future scientific costs of medical care. But Insurance and administrative costs are something else of course. If the problem of foolish borrowing puts Medicare out of business, it's hard to see how that could be the fault of my profession, unless perhaps something or other undermines our traditional system of ethics.
Where the ethics thing comes in is in the obvious conclusion that we are spending a lot of money treating diseases we crusty old docs once wouldn't have thought were worth our time. We are fast approaching the point when substantially all the medical catastrophic costs are concentrated in the first year of life and the last year of life. Increased life expectancy is a matter of widening the interval between those two signposts. Medical care between those years consists of treating the disease successfully, preventing disease and managing complaints we once would have dismissed as 'that's nothing'. Even the cost of doing this kind of medical care should decline: patents should expire equipment should simplify treatment should become standardized or even routine. But we notice people won't leave us alone: our government has just spent $27 billion forcing office computers on doctors who don't see the need to be bothered with them. People persist in using our time to inject botulism toxin into wrinkles and to listen to complaints about
how lonesome they are. That is to say, the public is beginning to insist on substituting their own view of what they want, for what doctors have traditionally thought was worth treating. This is an expensive way to enjoy the freedom of choice and it is only a matter of time before bureaucrats figure out the least obtrusive way to curtail it. Only when forces come to equilibrium will it be feasible to extrapolate future health costs.
What should appall us is the cost of paying for a progressively protracted retirement of so many unemployed people and the absolute impossibility of paying for it by continuing on our present funding path. Maybe that's what all this obesity means. Maybe people are trying to store up enough fat when they are forty, so they can go without eating from age sixty to ninety.
Unions teach their supporters: never retreat. Yell, shout, threaten, roll on the floor in simulated agony, denounce and declaim -- but never give back a single concession you have previously won. The hallmark of ratcheted positions about givebacks, is they are not negotiable.
Raising average retirement ages to 75 would quickly cure the financial problem.
By having some personal contact with union officials, who are generally decent enough fellows when not in their negotiating stance, I have learned that, to them, advancing the retirement age is absolutely not negotiable. Some of this intransigence is fake, having to do with negotiating traditions, and some of it has to do with the equally traditional stance that work is some dreadful thing which has been inflicted on the working man by unfeeling employers, or management, or the rich aristocracy or somebody. Reflex belligerence is therefore triggered immediately by suggesting that people are going to have to work more than they expected to. Much as I hate to offend people in their deeply held religious beliefs, I bring the news that retiring later would immediately solve the problem of affording to retire and that no other proposal under the sun has greater chance of solving that problem. But it's like the Law of Gravity. When dealing with demographics, to declare that something is off the table, or unacceptable, or a giveback -- is just bombast. With the present data, we are going to have to re-set the retirement age to 70. If medical and demographic trends are unexpectedly extreme, we may have to go to 75. If you think someone has promised you can retire at 55, you had better be in an iron lung or drinking your meals through a straw.
Retirement Later
It's easy to see that later retirement cuts lifetime costs in two ways: it increases the duration of earning and saving. And it shortens the years of retirement payout. The later you retire, the better it is. So the less you save, and the more lavish your lifestyle, the older you will be when you can afford to retire.
A lot of things can be debated, and a lot of clever ideas can be worked with. But it is going to take an atomic attack or something similar to modify this particular prediction about the future. And even doomsday predictions just make the future look worse, not better. Because as the insurance salesman tells you, you can have it one way or the other. You can die too soon or you can live too long. Since you can't know in advance which it will be, you would be wise to work a little longer, just in case.
To hope to retire is to hope to be prosperous without working. Those who must work can grow sullen about it.
Dr. Fisher
Rentier income is passive income, such as interest on savings accounts. Lord Keynes gave the term a nasty rap by defining rentiers as "functionless investors". That suggested Keynes shared some sentiments about passive investing with Karl Marx, who seems to have invented the term; both authors apparently judged the rentier class by the standards of novels by Jane Austen and Edith Wharton, or perhaps movie stars depicted in the novels of F. Scott Fitzgerald. That is, not gainfully employed, mainly occupied with debaucheries and expensive luxuries. This envy-based image dies hard but may subside if rentier life becomes everyone's goal. Or it may turn vicious, if a majority of voters see themselves as Jacobins in the water with the sharks, looking hungrily at the lucky few in the lifeboat. Guillotine, anyone?
Lord Keynes
To a certain degree, these attitudes can be managed, as possibly illustrated by bankers. After all, bankers extend credit to financially secure borrowers at the lowest interest rates and refuse credit to the penniless clients who need it most. It is thus frustrating to discover that you can't have any borrowers unless you have some lenders, too. In the main therefore, the public remains tolerant of the differential cost of taking risks. However, the public is often intolerant of the true value of a banker's role: simultaneous exchanging of capital between those with a surplus, and those with a need. That's unforced barter; forced relief of need requires the use of political majorities, responding to political viewpoints. If votes were all that mattered, however, the growing proportion of the population in retiree status could afford to be more complacent than they are. So 30-35% of American GDP would now qualify as the spending of passive income, although the varying degrees of risk within such investment are hard to evaluate. The risk is sure to rise as more labor-intensive work gets globalized away. Observers notice a paradox: passive income seemingly increases as the labor to achieve it diminishes, quite the opposite of the 19th-century Communist idea of work as the source of all wealth. Rentiers are never far from the need to defend the value of non-work income, at the same time everyone seeks to avoid hard labor, except as recreation. Our inconsistency does need some fine-tuning.
F Scott Fitzgerald
In the future, one thing seems certain: a greater proportion of our population will be retired persons, living on pensions, rentier income from savings, and government handouts. As it becomes the universal expectation of everyone that thirty years of rentier life awaits in the retirement stage of life, there will be less chance for Keynes, Marx, and Fitzgerald to seem so congenial to the voting class. But take care; young people, particularly unemployed young people, are never far from asking, "And what have you done for us, lately?", as if fairness were something to be measured with a spoon.
Karl Marx
Curiously, one implication about rentier income has almost disappeared. Interest is paid by a debtor to a creditor; as Marx would have it, the poor workingman is paying the rich rentier. Dividend income represents the profit from a business to its owner or a farm to its farmer. But emotionally, that is hardly so. We have so sterilized the investment process that we seldom think of debtors and creditors but speak of "fixed income" and "fixed income investors". The income from ownership, or "equity", is now thought by economists to bear a definable relation to the "prevailing return from fixed income". To them, it's all the same thing. Future attitudes can be hard to predict, but although everyone seems destined to be both a creditor and debtor at the same time, the two are surely not the same thing.
It's also hard to predict Americans attitudes if passive income becomes say eighty percent of GDP. Or fifty percent of the population become rentiers. Eighty percent rentiers, if you exclude children. Americans worship work; even labor leaders cry out, "Jobs, jobs, jobs." Western Europeans, however, seem willing to sacrifice luxury in order to live without work as threadbare rentiers. Is that the product of brain-washing, or have they discovered some evil in work that Americans are unable to see? The ancient Romans once aspired to more luxury, fewer soldiers. Unsympathetic barbarian neighbors then wiped them out. Better do some thinking about this because the Law of Gravity will not save the situation, any more than history lends much comfort to it.
Prior to the Second World War, old-age homes were almshouses, slightly modernized. Since few people lived very long after they retired, the old-age home took care of a few stranded old folks unable to care for themselves. The places were depressing and sparse, with a characteristic odor of urine and poorly-ventilated kitchens. But when time spent in retirement lengthened to twenty or more years, a new dynamic had to be considered. The dingy old single rooms changed into multi-room apartments, the dining room went upscale, and the infirmary changed into a skilled nursing facility. The idea was, you could graduate to more specialized medical care when you needed it, and be visited by your friends in the community who would someday be in the nursing facility themselves. They were paying to keep it up, and they would raise a ruckus if the infirmary service began to look uninviting. Whether the community was paying for it collectively or the younger generation was supporting it, the Retirement Village provided a more civilized way to grow old and die.
THe CCRC falls somewhere between a college dormitory and a resort hotel.
People chose these places for a variety of reasons, depending in large part on what they could afford. Widows are often overwhelmed by maintaining a house, widowers are often overwhelmed by cooking. And retired couples are often simply tired of both chores, or sufficiently crippled or befuddled enough to look for a way to give those tasks to younger people. One system grew up, of acquiring a second home in a vacation area and then replacing the main house with an apartment in a retirement community. If you stay in the vacation home for six months and one day each year, certain combinations can lead to appreciable tax savings. Sometimes a married couple is in perfect health and uses a retirement community as a comfortable suburban apartment complex, "just going on living the way we always did". The idea in their mind is the folk wisdom that you need to get used to a place and develop a circle of friends there; to do that, you ought to be less than eighty years old. When that's a general idea, it can be self-defeating to join a group of friends with pooled meal tickets. Thirty friends, or fifteen couples, can each host a party for thirty, once or twice a month. Unfortunately, they are quickly sequestered and disliked by everyone else as they make the regular rounds of nightly parties; but this sort of thing happens in upscale places, the kind of retirement community where some apartments have servants' quarters, and nobody much cares what anything costs. For people in this circle, the most detestable thing about a retirement community is the pressure to have dinner at 5 PM. Early dinner is ordinarily the surest sign the place is managed primarily for the convenience of the employees, but it can also mean there is nothing else to do except watch prime-time television.
Retirement Funds
For most people, however, even having ample funds for retirement is constrained by the uncertainty of how long the retirement will have to be, how much must be held in reserve, even at age 100. The gallows humor continues to repeat some version of trying to plan a way to spend your last dollar on the last day of your life. It isn't just how long you will live, it is how. If you or your spouse become blind, or bedfast, or in chronic pain, your level of living is going to change and your daily expenses may rise dramatically. Even if you never gave such gloomy things a moment's thought, the experience of eating in the same dining room with several hundred elderly acquaintances soon teaches all the lessons of unexpected illnesses and weekly funerals. Some people cannot bear the idea of living in such a community, for precisely the reason that it becomes impossible to kid yourself. And one thing no one can kid himself about is the reality that you have to have one awful lot of money before you can ignore the need to watch your pennies. And it isn't just your spending money; it's also the lack of a basement, attic, and garage in which to expand or from which to draw reserves, or just to enjoy old books and mementos buried in dust.
Retirement communities seem to have developed independently in the Quaker suburbs of Philadelphia, and along the California coast. Except for the climate, there isn't much difference. More tennis in California, more trips to the theater on the East Coast. The early communities had a strong focus on finances, which assumed a lifetime retirement fund derived from selling the family home. The fancier the house, the more elaborate the apartment it would finance. As the duration of retirement grows progressively longer, roughly three years every decade, it is certain that the sale value of the average American family home will get progressively stretched to extend to the average age at death -- especially if you focus on the average age of the second of a couple to die, or become blind, or become bedfast.
CCRC, Continuing Care Retirement Community)
So, the patterns of financing are changing, at least experimentally. Some retirement communities (the term is are purely rental, partly room and board, extra charge for the nursing facility, or a la carte for all services. People who enter any sort of community are often planning to move to a different one after a period of time, either to adjust to their reduced physical capacities or changes of location of their families. Some of them actually say they plan to live luxuriously and then move into their children's houses when the money runs out, although it is usually hard to know how seriously to take such comments.
Obviously, what is needed is some sort of insurance mechanism to pool everybody's risks, but there is a fundamental problem. Insurance companies make a big profit on life insurance in two ways: either from clients who drop the policy before they cash it in or from premiums which underestimate the actual age of death compared with the average experience at the time the policy was taken out. But in the retirement case, essentially all policies mature at death and the duration for compounded investment is brief. So such insurance is either overpriced or unobtainable. The same underlying phenomenon affects Medicare and explains its impending insolvency. Those early retirement communities which based their charges on the assumption that Medicare would continue unchanged are repeatedly stranded when Congress cuts back on Medicare benefits. Someday, demographic trends will level off and insurance can be restored to practicality, but that time is certainly two or more decades away. Many states, including Pennsylvania, have passed laws that residents of retirement communities may not be evicted if they become impoverished, so the communities are forced to be strict about advance funding. Ultimately, the danger is that the community will be forced out of business, stranding the occupants. With so much time available to discuss such matters in a common dining hall, occupants of these facilities can become obsessed with the need to save for the future, and no one can be certain they are wrong about it.
The legislation removes the hampering restrictions of the 1995 Law. What follows is a brief outline of the main features of the HSA/MSA clause in the 2003 law,
U.S. Capital
as published by the main authorizing committee, the House of Representatives, Committee on Ways and Means. From this point forward, more specifics of the program will probably be written by the Executive Branch and published in the Federal Register. The Ways and Means Committee will continue to exercise oversight authority, however, in conjunction with the Senate Finance Committee. As a consequence, statutory modifications of the program are likely to appear in future annual budget reconciliation acts, or else in any new Medicare amendments. The legislative route map becomes more understandable when it is recalled that Medicare itself is considered to be an amendment (Title XVIII) of the Social Security Act.
Working under the age of 65 can accumulate tax-free savings for lifetime health can needs if they have qualified health plans.
A qualified health plan has a minimum deductible of $1,000 with $5,000 cap on out-of-pocket expenses for self-only policies. These amounts are doubled for family policies.
Preventive care services are not subject to the deductible.
Individuals can make pre-tax contributions of up to 100% of the health plan
deductibles. The maximum annual contributions are $2,600 for individuals with
self-only policies and $5,150 for families (indexed annually for inflation).
Pre-tax contributions can be made by individuals, their employers, and family
members.
Individuals age 55-65 can make additional pre-tax "catch up" contributions of
up to $1,000 annually (phased in).
Tax-free distributions are allowed for health care needs covered by the insurance policy. Tax-free distributions can also be made for the continuation
coverage required by Federal law (i.e., COBRA), health insurance for the
unemployed, and long-term care insurance.
The individual owns the account. The savings follow the individual from job to
job and into retirement.
HSA savings can be drawn down to pay for retiree health care once an
individuals reach Medicare eligibility age.
Catch-up contributions during peak savings years allow individuals to build a
nest egg to pay for retiree health needs. Catch-up contributions allow a married
couple to save an additional $2,000 annually (once fully phased in if both
spouses are at least 55.
Tax-free distributions can be used to pay for retiree health insurance (with no
minimum deductible requirements), Medicare expenses, prescriptions drugs, and
long-term care services, among other retiree health care expenses.
Upon death, HSA ownership may be transferred to the spouse on a tax-free
basis.
Contain rising medical costs- HSA's will encourage individuals to buy health plans that better suit their needs so that insurance kicks in only when it is truly needed. Moreover, individuals will make cost-conscious decisions if they are
spending their own money rather than someone else's.
Tax-free asset accumulation- Contributions are pre-tax, earnings are tax-free, and distributions are tax-free if used to pay for qualified, medical expenses.
Portability- Assets belong to the individual; they can be carried from job to job and into retirement.
Benefits for Medicare beneficiaries- HSA's can be used during retirement to pay for retiree health care, Medicare expenses, and prescription drugs. HSA's will provide the most benefits to seniors who are unlikely to have employer-provided health care during retirement. During their peak saving years, individuals can make pre-tax catch-up contributions.
John Maynard Keynes invented the science of macroeconomics after the First World War, and since then everybody seems to hate the subject. But after proposing a radical change in medical finance which involves eighteen percent of the gross domestic product, it is time to reflect on where it might go.
Politically, a spread of Health Savings Accounts would make everybody an investor, and therefore more sympathetic toward investing. But the same idea was applied to affordable housing, and it caused a major economic crash in 2007, with real estate getting the worst of it. It taught us if there is a crash, it's hard to sell your house, so it's hard to move to a place where jobs are plentiful. So it follows if everyone is an investor, people will love you when the market is up, hate you when the market is down, but the worst part of it will probably be quite unexpected.
For example, executives are clearly overpaid because the stockholders are too remote to have their vote matter. A spread to stock index investing might reawaken legislation to give the stockholders more power, or it might stimulate the German system of placing union members on the board of what is often a family-owned business. It's hard to know what to think about that outcome.
My own prediction is increasing ownership by patients will act as a counterweight to drug and medical device prices, but will also restrain government regulation of those industries. The public wants low prices, but it will in time want higher profits in those companies. Perhaps some way can be devised to put those motives into balance for the benefit of all.
The same conflict exists with health insurance companies and other corporate medical enterprises. And yet, with the quick passage of the McCarran Ferguson Act, the insurance companies emphatically endorsed state regulation over federal for insurance. Would the public be the pawn of big corporations, or would the reverse happen? Hard to say, so we might as well just watch to see.
Cost shifting has come to describe something evil, something to be eliminated. Perhaps it is not illegal, but the common view is that at least it represents "rent-seeking", an economist term for reaping unearned or undeserved profits, and getting away with it. This attitude must be revised; a modern healthcare system cannot function without a certain amount of cost-shifting. The funds to
Pennsylvania Hospital, Nation's First Hospital, 1751
Healthcare institutions may well have mission statements, but the main force visibly shaping hospital mission is third-party reimbursement. One must be sympathetic with institutions which really prefer their own mission to the pressures from third parties, particularly when the "second party" -- the patient -- also likes the original mission better. Teaching hospitals surely would prefer to concentrate on streamlining tertiary care, retirement villages on enriching the lives of elderly residents, etc. And they could probably make a better case for what they prefer than third-parties can. When one-size-fits-all health insurance is imposed on institutions which must survive by internal cost shifting therefore, insurance mandates invisibly prevail. It is not always strictly a matter of "Who pays the piper calls the tune", as it is "Who pays the most can run the place."
Considering these invisible forces of control at work, it seems highly desirable to search for situations in which the incentives of the third-party do not run parallel to the incentives of the provider community. In the case of government third-parties, the goals of the agency may not even be parallel to the will of Congress. The public clearly prefers to pay for private rooms and private duty nurses if it can afford to, but those are mainly relics of the past. Doctors used to work out of offices in their homes, but you seldom see that, now. There once were twenty hospitals in Philadelphia which were owned, paid for and operated by churches, but now at most, the church name is a relic on the front door surviving from a former era. If these changes were a response to public preference it would be another thing, but they are usually not even traceable to a written mandate which might be appealed. So it becomes all the harder to defy a mandate which grew out of the hospital's surmise as to what the third party would probably prefer. Perhaps some examples of social pressures at work would be useful.
It happens my own first office experience was in the home of an older doctor on vacation. The location of that family residence was a careful triangulation of convenience, expense, distance to the hospital, and the preferences of the patients. It was a grand experience to put aside the breakfast coffee, walk into the next room, and see the first patient of the day. Or to interrupt office hours for an emergency in the neighborhood for less than an hour and to have your excuses readily accepted by the waiting patients upon return. My colleagues had explained the financial advantages of sharing a roof and heating system with a tax-deductible business. But my accountant explained that the Internal Revenue Service didn't like offices in the house, and would surely audit any doctor silly if he persisted. So I spent fifty years in an office across the street from the hospital, commuting and seeing patients who had to commute to see me; the extra expenses of parking and the rest of that arrangement are easy to imagine. True, it was easier to visit the hospital patients, and nice to eat lunch with other doctors in the hospital cafeteria. But all of these decisions were not my own first choice. I never got a letter from the IRS or heard a murmur from them, but I always believed I was responding to their mandate. When an IRS agent finally wandered into my office as a patient, he admitted the IRS prejudice but said he believed it grew out of fear the business expenses reported would really be the expenses of a hobby, not a business.
A second relevant experience occurred when I was a resident physician. A staff physician at the hospital had a heart attack, and the Chief of Medicine asked me to take a few days off to tend to the problems in the stricken doctor's practice. His home and office were in the midst of a row-house district of town. When I arrived, the office was empty of patients, but the nurse was waiting with an umbrella. "Before we see the office patients, we must make rounds to see the bedridden patients at home." To my amazement, within a three-block radius of his office, there were nearly twenty patients in hospital beds at home. Some of them had oxygen tents, several of them had intravenous fluids dripping into their arms. The nurse told me that she drew blood for pickup by a laboratory and that with a little argument a portable x-ray machine could be brought to the home. At the foot of each bed was a hospital chart, all up-to-date with notes and reports. It might not be possible to run such a show in many other neighborhoods, but the city row house neighborhood was ideal. Or, not ideal perhaps, because there must have been many problems. But it was clear why Blue Cross had slow progress making sales to the people accustomed to this arrangement. And it even made clear why patients were content with open twenty-bed wards in a hospital, for at least ten years after Medicare would have gladly paid for a semi-private room. No private duty nurses, however, it might set an unwise example.
Two things are at work, here. Things happen to medical care which is undesirable, so someone needs to complain about them, and complainers must be provided with a place to appeal. The reverse is also true; good things which ought to happen, don't happen. So in addition to providing an appeals system, we somehow have to provide a wise and unbiased ombudsman to suggest what new initiatives ought to be undertaken. And the two functions, negative and positive, need to commune with each other. Parenthetically, since everybody gets involved in health care to some degree, adversary roles must be filled in this process, containing representatives of patients and also providers (both institutional and individual), as well as guardians of the purse. Since the process quickly becomes unwieldy, it needs to be associated with a special committee of Congress and needs to be able to summon both witnesses and experts. An annual convention in some pleasant spot might enhance the concept.
Institutions are another matter since quite often the personal opinions of the spokesman are constrained by the incentives of the institution. It must be made clear to them which opinion is desired.
Institutions choose their location for other considerations, chief among which is cheap land, but the location near public transportation is another factor. Whatever the thought process underlying it, nursing homes and retirement villages are almost always in the far suburbs. A related problem is a vexing difficulty for a center-city hospital to find a nearby nursing home for convalescents. These annoyances are protracted by the licensing rules in a round-about way. When a corporation is formed, typically a lawyer with a yellow pad asks two questions: "What are you going to name this organization?", and then, "What is its purpose?". Presumably, he then completes some forms and files the necessary applications. The stated purpose may well have other uses, but it defines the sort of license needed, and eventually either match or does not match the rules some third-party reimbursement agency has laid down for what sort of institution is eligible for reimbursement. After that, the system becomes much more rigid than it needs to be. As long as the institution remains defined as a hospital it will be paid by the third-party, and without that designation, it won't. Effectively, the state licensing board acquires the power to shut off the revenue of some institution which displeases it. But what displeases it (let's say, mice in the kitchen) usually bears a scant relationship to whether or not the institution is capable of performing additional tasks. It does not take long for these issues to get blurred and forgotten; the retirement village can't receive hospital reimbursement because it doesn't have a hospital license. A hospital license would permit it to do a lot of things it doesn't want to do. While the general idea is sound enough, the rigidity it imposes is excessive, particularly when you consider the penumbra of reluctance it provokes from employees. Obviously, the interpretations vary greatly between jurisdictions. It leads to hospitals which may perform heart transplantations but may not run a day-care center for the children of their employees.
There are many simple solutions to this simple problem, but because so much of it is buried in-laws, it would probably require a special court to be appointed to oversee it. How busy that court would be would depend on how vigorously competitors would resist it, which would probably vary with the region.
In any event, Society has a legitimate interest in preserving the quality of care, but it does not fulfill that duty by transferring it to reimbursement agencies. During wars, surgery is satisfactorily performed in tents, for an extreme example of how expendable much oversight can be. Another principle would be to ease impediments to overlaps of functions between institutions, particularly including the backward sharing of component services and records toward the lower-level institution. Since such sharing is often observed to occur without objection within vertically integrated institutions, there is every indication it is both desirable and feasible between competitors.
Going much farther back to the town meeting form of oversight, the most radical departure from present custom would be to encourage a shift of the center of care from inpatient hospitals toward retirement villages. The simplest definition of the center of care would be the location of primary physician offices, and the most important step would be to discourage mandatory links between referring physicians and particular acute care hospitals. Doctors left to themselves will locate where the patients are, and increasingly it is possible to see a shift of patients requiring chronic disease management and terminal care into the retirement village. The tendency of doctors and laboratories to cluster around hospitals impedes this natural shifting together. If doctors shift their offices and are allowed a choice, laboratories and x-rays will soon follow them. Before Medicare, the center of care was found near the high-rent districts of cities. In London it was Harley Street, in Philadelphia it was Spruce Street. As reimbursement changed, it shifted toward the hospital campus, where the parking problem is also solved. Nowadays, early discharge and reimbursement shifts have made it unattractive for a primary care physician to visit his patients in the hospital, so hospitalist and emergency room specialties are flourishing, with computerization feebly bridging interruptions to the continuity of care. The primary care physician would find the retirement village solves the parking problem; pharmacies and laboratory pick-up are often already in place, and non-surgical specialists would soon follow primary care physicians. Patient transportation, at present crippled by expensive municipal monopolies, would be greatly eased by such shifts of medical interaction. The ultimate shift of the center of care would be for the more mobile younger population of suburbs to shift allegiances toward the retirement village location, a change mostly affecting pediatricians. It would take some time, and it would always be a partial migration. However, the infirmaries of retirement villages offer convenience and comfort near home.
The most effective force maintaining standards for this level of care, have no doubt of it, is the ease with which friends within the community drop in for visits. They have time for it, especially to and from the dining room, and all of them keep a watchful eye on how they would likely be treated there themselves when their turn comes. In retirement communities, client consensus is a powerful force. What is lacking is a willing sharing of reimbursement with acute care hospitals. Therefore, the idea of brief hospitalization followed by longer recovery near home is now only realistically available to the affluent. But their choices show the way, as they always did before third-party insurance dominated the scene. For a while, little children may think it is funny to get their shots at the old folks home, but they will soon get over it.
Inflation-targeting, unless someone is keeping a big secret from us, is the only arrow in the quiver of a nation's central bank, in our case the Federal Reserve. A strong case that the Federal Reserve should acquire no other duties, rests on the fear that any new duty might conflict with holding inflation on target (at present, 2% per year). The recent adventure of the present Chairman, Ben Bernanke, into "Quantitative Easing" illustrates that diluting and confusing the role of the Federal Reserve will tempt the Executive Branch to poach on its independence. In this particular case, the adventure was the purchase of vast amounts of bad loans in order to remove them from the economy, never mind the future problem it will create of re-selling those loans to someone. Mr. Bernanke is lending credibility to the outcry of Representative Ron Paul (R, Tx) that the Federal Reserve should be abolished entirely.
Kenneth S. Rogoff
Maintaining price stability (Inflation targeting) rests on Alan Greenspan's simplification of Milton Friedman's "monetary" theory that you can combat inflation or deflation by appropriate adjustments of interest rates and the money supply. Greenspan's further insight was that you needn't measure "monetary aggregates", you just have to measure inflation itself and react like a helmsman with a compass. Until 2008 it looked as though Greenspan had won the argument, by avoiding a deep recession for seventeen years, in the so-called "Great Quieting". Inherent in this helmsman theory is a deeper theory that all episodes of deflation (depression, recession, whatever) are merely over-reactions to inflation; avoid inflation and then forget about deflation. Still further behind this analysis is the observation that all governments at all times are pushing toward inflation, count that as an immutable law. The blunder of holding interest rates too low in 2001-3, for example, has been blamed as deliberately inflating in order to combat the Dot-Com crash of 2001 for political reasons; by this reasoning, the rescue of the DotCom dip led straight to the 2008 Subprime plunge. There is thus evidence that monetary effort by the Federal Reserve is powerful enough to control inflation, provided other branches of government abstain from political interference. In the long run, however, the Fed can only smooth out wobbles in the main trajectory. As Rogoff has shown, all crises whether of currency, banking, commodities or securities, are pretty much the same and caused by unwise borrowing. Avoiding inflation is enough to prevent a recession since government pressure to inflate can be counted on. Paul Volcker may have proved the issue in another way in 197_. During the Carter Administration, the country experienced "stagflation", we had inflation and unemployment at the same time. Improving one might seemingly make the other worse. But, dismissing the whole mess as inflation in disguise, Volcker promptly jacked up interest rates a great deal -- and both inflation and unemployment then went away. What seems proven is that stagflation is just a variant of inflation and should be treated by sharply raising interest rates.
If inflation targeting is as powerful as that and as simple as that, what could go wrong? One present worry is that so much American money has fallen into foreign hands that the Federal Reserve could lose control. There is a second source of danger. Broadly speaking, this concern is that public opinion might demand inflation -- or policies which would surely cause it -- and in a democracy, the time might come when the Federal Reserve would have to give people what they demand. James Madison warned us about that. In a democracy, it's their country to ruin if they please.
Fringe Benefits
New Jersey increased the number of state employees and their fringe benefits. As is so often the case, these state employees and their union became the core voting bloc for the party in power, usually Democrats. Not only are there a remarkable number of employees in each of the local offices for the Bureau of Motor Vehicles for example, but New Jersey included the local municipal and school employees (mainly police and school teachers) in the state health and pension system, a decidedly unusual step. These were not trivial costs. Longer life expectancy makes pensions and health care more expensive. Just how a ten-mile ambulance ride gets to cost $1700 is a related story, passed over here. And then, a few years ago it seemed like clever bookkeeping to float a bond issue to bring the state pension system up to full funding. Long term full funding tends to mean a stock portfolio, buying stocks with a bond issue is like buying stock on margin. By a stroke of timing, the booming dot-com stock market promptly crashed, taking New Jersey's margined stocks down even faster. In a sense, not only has the state raised the reimbursement of its workers, it has guaranteed them for life.
New Jersey has always had high real estate taxes, now painfully high. But Jersey residents once could console themselves they had no sales tax and no income tax. Now, NJ sales and income taxes are nearly the highest in the country, and just about every other form of state taxation is at unsustainable levels. Doesn't matter, the state is running a $5 billion deficit and will run a greater deficit for as long as anyone can predict. Forbidden by the courts to borrow money, it's not easy to see what the Governor can do except raising taxes some more. Well, perhaps there is one thing if the unions will let him. He can extend the retirement age of state employees from the present age 55 to age 75. Having retired at age 81 I have little sympathy and have even written a long essay praising the joys of late retirement.
But let's see him try to do that without anyone noticing.
Most Americans alive in 2020 will live to be ninety
Dr. Fisher
During the Twentieth century, average life expectancy for Americans at birth extended from a little less than age fifty, to a little less than age eighty -- roughly thirty years. Looking ahead to the next century, it's entirely reasonable to expect a cure for cancer and Alzheimer's disease to extend life expectancy to ninety-five. It's also reasonable to expect that somewhere along this path we will find such retirement expectations are more than the nation can afford. Everyone will have to go back to work.
Working ten years longer means ten years less time in retirement, and it also means ten years more time to accumulate sufficient savings for whatever time is left. Some people who are already working more than they want to, won't like that. There will be attempts to make retirement cheaper and to extract savings from novel sources, but further improvements in health care will wipe out all those efforts. The normal age for retirement will have to move to at least age seventy, probably seventy-five. If employers have problems with that, the solution will have to be second careers. So, let's shift our attention to people who are lucky enough to afford a thirty year vacation. They must go back to work, too.
A moment's reflection reveals that everyone must have a life goal of accumulating more money than is needed to live out his life. Once average life expectancy levels out to a stable point, ingenious life insurance design could bring us to the point of spending the last dime on the last day, providing we consider it worthwhile to spend the extra insurance administration cost. More likely, human psychology will always demand a little extra comfort from a little extra financial cushion, and there's a relationship with the age of retirement. The later you retire, the more likely it is you will have money to spare. For physical or mental reasons there will be people who can't work, but everyone else knows a simple solution to the problem of being able to retire: don't stop working until you can afford to quit. And by the way, the later you start saving, the longer before you can quit.
We have so far not worried much about the lucky, talented, or just miserly few who achieve life's normal goal of saving just a little more than they need; but that must change, they need to go back to work, too. Philanthropy, a very important part of American life, is struggling and needs their talent. It's likely that our business and economic success as a nation is responsible for diverting our energetic and imaginative talent toward the for-profit sector. The general attitude has been that if things are worthwhile, people will pay for them; businesses run not-for-profit can't really be worth much. That's very wrong, of course, but there's enough truth to it to require some changes.
Nonprofit organizations are often inefficient because efficiency is partly the consequence of seeking a profit. But the analysis must not stop with this hopeless truism; the manageable problem is to find new goals for efficiency which do not directly require profit-seeking. One approach would be for non-profits to create for-profit subsidiaries, later selling them off to enhance their endowment. The tax authorities would want to examine this approach to avoid harming competitive tax-paying entities, or sham arrangements in which the purported subsidiary dominates a nonprofit shell.
However, this and similar approaches merely continue the present mindset about the role of the donors and the volunteers. Nonprofit organizations tend to gravitate toward a professional staff with nominal trustee oversight, relegating the donors to the function of giving or getting donations. If philanthropy is to acquire a new drive toward efficiency to supplant the absent profit motive, the donors must be actively employed in the organization, noticing any waste or inefficiency, sharing the gossip, and appreciating the triumphs. To some degree, a form of this model is found in the auxiliaries of hospitals and museums, where staff administrators generally chafe in private about the class distinctions and disruptive ability to cut across management hierarchies. If this system is to work effectively, it needs to be studied for ways to be less threatening to the younger employees, and to get more useful work from the older ones.
At a recent meeting of the Right Angle Club, Stephen C. Bennett an administrator, and Alix Esposito a social worker, kindly addressed the club about the Veterans Hospital where they work. The federal government pushes its mass produced products into every city, but gradually a local flavor starts to creep in; how this process works is illustrated by the fact that Steve's grandfather Claude was once the manager of the Bellevue Stratford Hotel. The VA hospital may be a piece of Washington D.C. planted on Philadelphia soil, but Philadelphia will surely absorb it with the passage of enough time. The VA was once a part of the Veterans Administration, but now it is a part of Department of Veterans Affairs, run by a Cabinet Secretary, no less. It's the second largest department of the federal government, and since the only bigger department is the Department of Defense, the combination of the two shows you how far we have come from the nation's original opposition to "standing armies". The fact that these two components of our war machine are separate, on the other hand, surely symbolizes some hidden tensions between our regular armed forces and the American Legion, or the hidden frictions between two congressional committees, or else some other mystery of bureaucratic politics.
The Veterans Administration was founded in 1930, the Philadelphia VA Hospital was built in 1950. Originally, it was designated as a Deans Hospital, signifying the intention to confer prestige and lessen friction with the medical schools. Originally, Philadelphia's VA was affiliated with several medical schools, but in time its proximity to the University of Pennsylvania led to the elimination of ties with other schools. Although the bed capacity is growing in reaction to America's successive wars, its open wards converted after 1960 to more semi-private style, and its focus of medical activity shifting with changes in medical science, the VA remains isolated from the rest of the city and the rest of Philadelphia medicine. Part of this is physical; the hospital is confined by the University of Pennsylvania, the parking complex next to the Amtrak line, and the Woodland Cemetery, so there is little room to grow. And comparatively little commonality with the neighbors. There are 2000 employees and a $30 million budget, marooned in a sea of automobile traffic going elsewhere in a big hurry, too big to ignore but too small to influence the local culture.
Vietnam War
The patients are distinctly different from those you find in other hospitals. There is a great deal of chronic mental disorder a heavy influence of alcohol and substance abuse and rehabilitation, and even some residential apartments for patients. On a national level, between a third and a half of homeless people are veterans, but for some reason in Philadelphia, only a tenth of the homeless are veterans. During the Vietnam War, the system of draft avoidance through educational exemptions resulted in that generation of veterans coming from an unusual concentration of low income and low educational subgroups. The system of government pensions and promotions tend to retain employees in the system for a lifetime. It's true that informal transfer arrangements allow a certain amount of migration to Florida (in the winter), or Maine (in the summer), or California (to see what LaLa land is all about), but those who do this stay within the VA system. Consequently, the interchange of ideas and techniques that professionals carry with them between hospitals is curtailed, confined somewhat to variations within the VA system, conforming to its social norms. An archipelago, although not exactly a gulag archipelago.
Veteran
But by far the greatest source of distinctiveness in the VA hospitals comes from the byzantine eligibility standards for the patients. The reimbursement systems of Medicare, private insurance -- which more or less copy each other -- changed around 1988 in a way that more or less eliminated psychiatric inpatient care in the community, especially if it lasts more than a month. The VA, on the other hand, was forced by circumstances to increase its attention to this area. Consequently, all social workers everywhere inquire immediately whether an addict or a schizophrenic might be a veteran. A differential sorting process quickly gets underway, with the VA as the preferred place to send such patients if at all possible. Non-veteran victims of the same conditions tend to have a worsened time of it, because the pressure on state and local governments to make some provision, has been relieved.
Walter Reed Hospital
At the other extreme, the social elite of the armed forces are not admitted, either. President Eisenhower was unquestionably a veteran, but he had his famous hospitalizations at >Walter Reed Hospital. There's an income limit for VA admission, which automatically cuts off 20-year veterans above a certain rank, possibly major. And there are overlapping disability classifications for military hospitals and veterans facilities, with considerable latitude available to uniformed boards of three serving officers, only one of whom is a physician. The result is a general perception that if you have any influence at all, you can generally avoid the VA and be treated in a military hospital, probably in a VIP unit. Good for them; I'd take advantage of it if I had a chance, too. But by siphoning off the top brass, a lot of pressure to improve quality is removed as well. If a VA hospital had eight or ten Admirals and Generals as patients, with academy classmates coming to visit, it's safe to assume that courtesy, orderliness, and cleanliness would instantly improve. And take it from me, the quality of care would improve, as well.
Except for Social Security, most retirement funds are not required to be tax-sheltered ("Federally Qualified"), but one would be foolish not to take advantage of the option where possible. Ordinarily, just about every other form of saving must first net out federal taxes. The debts of state governments ("municipal bonds") are free of federal but not state taxes, but reflect that benefit by paying a lower interest rate; any overall advantage must be calculated individually, and quite often it is non-existent. Mandatory taxable income, more-or-less mandatory tax-exempt income, and optional; that's your choice, except for the decision to put them in a federally qualified pension fund. Most people just throw the ownership certificates into a safe-deposit box and forget them. This article suggests you create three funds, whether in a lock-box or brokerage account and mentally rename them by overall purpose. There's not much you can do about tax status, but you have a little latitude about how and when you spend the money. It can make a certain amount of difference because increasingly it is true that investment performance is affected by taxes and fees. Friends, neighbors, and classmates may tell dazzling stories about astonishing investment luck, but if you want to have the best performance in your social circle over the very long haul, you would be well advised to focus on taxes, transaction costs, and fees. Especially fees.
Saving Bonds
When Grandpa gives a brand-new grandchild a hundred dollars, it can be spent on a new rattle or it can be invested. Rattles usually win, but occasionally it gets invested; what it's worth when the newborn finally dies will mostly depend on two things: how old he is when he dies, and how young he was when he started the investment. To make it easy to calculate, let's assume a life expectancy of 85 years, and an interest rate of 7%; that seems to imply a value of $40,000 at the time of death. That seems to imply a value of zero if he dies without spending any of it, and value somewhere around $30,000 if he pays current income taxes. But if he pays $100 a year for the lock-box, he will only have $20,000 left after expenses. And if he pays fees for his checking account, or receives only nominal interest for a savings account, he may end up with nothing at all. Since that's the usual outcome of most cases of Grandfather gifts, perhaps the choice of a rattle isn't so reprehensible. The whole investment process is too expensive to bother with until the sum involved is several thousand dollars. At fifty times the hundred dollar gift we started with, the investment is $5000, and its final result is a retirement fund of two million dollars. Yes, the arithmetic can be argued with, and yes, lots of things can go wrong in 85 years. Maybe a one-million dollar benefit is more likely, but no one can dispute that it's a pretty easy way to die a millionaire instead of a paper.
All right, that's your Contingency Fund. It's taxable, but almost everyone can start it pretty young and forget about it for long periods of time.
Tax Fund
The Tax Exempt Fund gets created when you start to work, even for a few days as a teenager. Several percents of your earnings will be withheld for the Social Security program, which requires that you apply for a Social Security number. If you wish, you can start depositing up to a set limit of your earnings as a tax-exempt fund for retirement, currently called an IRA or a 401-k fund. Your income taxes for the current year will be tax-sheltered, up to the amount taxed on the amount you contribute. It's a good thing to get one of these funds started as soon as you are legally able to do it, so the mechanics are completed while the amounts are still small. The suggested funds are the ones with the smallest administrative costs, which will probably be no-load index funds; if the fund you choose has more than a trillion dollars under its control, you are probably reasonably safe. Try to keep depositing automatically, right up to the maximum amount allowed by the law, right up to the day you die if they will let you, and select the option of automatically re-investing any dividends. Until these vehicles were created, just about the only tax-exempt investments anyone could buy were tax-exempt municipal bonds and life insurance. Both of these vehicles have some major disadvantages; the IRA and 401-k mechanisms allow you to apply the tax exemption to just about any investment you choose, so they are just as good as anything you can buy, plus having the advantage of being tax sheltered. If anyone proposes investments other than IRA/401-k before you exhaust the limits of these, that person has some serious explaining to do; at the very least get a second opinion. It will be a rare person under the age of forty, perhaps an entertainer or professional athlete, who has money left to invest after fully exhausting the tax exemptions. That's because the typical young person takes on the burden of buying a house or paying for private education for children, and there just isn't enough money to go around.
Life Insurance
Life Insurance is a comparatively poor investment, and it is an even worse investment if it is purchased without investigation or comparison shopping. Some insurance companies, like Northwestern Mutual, have considerably better results than the average, and some other very large, very famous "leading" life insurance companies have pretty inferior results. Life insurance does provide some tax exemption, however, which varies a little between states as a result of the McCarran Fergusson Act of 1945. However, the legislation does produce tricky features, like tax-exempting either the owner or the beneficiary of the policy, but not both. The entire first-year premium is ordinarily paid to the salesman as a commission, and sometimes the commissions continue for life. But that is only part of the incentive which the life insurance salesman has for selling excess coverage. The other incentive is worth serious pondering: the main source of life insurance profits derives from a large number of clients who pay premiums for a while and then drop the policy without collecting on it. The deplorable national statistics on temporary job loss, personal bankruptcies, and divorce carry implications of considerable weight for the purchase of life insurance; investment is limited to what you happen to have, but life insurance is based on projections of what you hope to have, or what you fear.
Benjamin Franklin was able to retire from the printing business at the age of 42. His partners bought him out in eighteen yearly installments. In the Eighteenth century, it was unusual to live past the age of 60, so Ben felt pretty well fixed. Unfortunately for this planning, he lived to be 82, so when he did reach the age of 60 he was forced to look around for postmasterships and other ways to survive, for what proved to be 22 more years.
This is the other side of a coin; on one side is written, "Protect your family in case you die young". On the opposite side is written, "Be careful not to outlive your savings", relying on the old Quaker maxim that the best way to have enough--is to have a little too much. For centuries, life insurance was sold to people who mainly feared the first, commonest, possibility, but never completely addressed the opposite contingency, which was growing steadily commoner. Annuity insurance ordinarily is sold for a fixed number of years, so insurance commissioners ordinarily require what is most probable. Unfortunately, this response shifts the risk of guessing wrong onto the subscribers' shoulders. Since science has unexpectedly lengthened average life expectancy (by thirty years since 1900, or by five years in the last ten), experience rather like Ben Franklin's has become a commonplace, but rather poor business judgment. The business remains solvent only as long as the decision to drop the policy is later than the life expectancy.
Retirement Saving Debt
There may exist insurance policies to address this issue, but few companies offer it. We will briefly describe this sort of policy, in case it becomes more widely available, but it is primarily described here to illustrate the issues to consider. If you can get it for a reasonable price, or if you can get it at all, the outline of the policy would be to set a premium and promise to pay 6% for the rest of your life. Underneath the promise is the reality of paying 6% for eighteen years as a non-taxable return of principal. Following that, you don't need to get a postmastership, you are paid a taxable 6% until you die. Presumably, the insurance company has actuaries to help with the math, so the company makes money if you live less than your life expectancy, and loses money if you live longer. If life expectancy suddenly extends much longer (let's imagine a cure for cancer appears), the insurance company is going to go broke. That's why insurance commissioners are uncomfortable with the concept, even though it is obvious how desirable it might be. So that's why annuity insurance typically states a fixed number of guaranteed years and expects the subscriber to shoulder outlier risk.
Any insurance has an administrative cost, so everyone must consider some non-insurance solution to the whole problem. Therefore, we propose you re-examine the old saw about "never dip into principal". If you don't have enough money, you can't do very much except depending on the government, your family, or your fairy godmother to help you out, although it must be obvious that all Americans would be wise to consider retiring five or ten years later than they hoped. Very likely, the government is going to have a difficult time sustaining even the present tax exemption of retirement funds, medical insurance, and social security. Those are called entitlements, but if the government eventually can't afford them, it won't matter what you call them. If entitlements keep getting extended, we can expect our nation to resemble the ancient Chinese and Indian nations -- able to build palaces in their golden era, but eventually crumbling into a gigantic slum in centuries afterward. So please, if you are able to do it, try to keep gainfully employed for a few extra years. If you do it (and some people can't) you may be able to realize the American Dream.
Inheritance Tax
The traditional American dream was to accumulate enough money to live off the income from it indefinitely, never touching principal, and then exposing the principal to destructive estate taxes after you finally die. Unless you are unusually wealthy, there isn't much left for the next generation after estate and inheritance taxes and expenses. It's a little inefficient to accumulate more than you actually need, but the government gravitates toward the least painful methods of collecting taxes. By confiscating this safety surplus, however, it declares that "Every ship (generation) must sail on its own bottom." And therefore it must acknowledge responsibility for what inheritances ordinarily pay for, like charity and good works. But there remains a quirk to this.
If Ben Franklin's partners had arranged to invest the money until he needed it, they could at least have afforded to finance two or three extra years. After inflation and expenses have eaten away at your retirement income, your principal may not generate enough income to last forever, but it is still big enough to pay for several years of retirement, which may in fact be longer than you are destined to live. Remember two things: 1) a principal sum, big enough to support you indefinitely, must be roughly eighteen times your yearly expenses. If it is only big enough to support you for fifteen years, it will seem too small until you realize you are probably actually going to live, say, five years. And 2) as far as leaving an inheritance to your children is concerned, there is a realistic probability that the government will consume most of the estate before it ever gets to the kids. These fundamental truths are presently obscured by the Federal Reserve artificially forcing interest rates to less than 1%. But if you can just hold out for a few years, it seems entirely likely that interest rates will return to 6% (meaning your principal will once again produce eighteen equal installments). But such a return of interest rates to normal levels will force the government to pay a comparable amount as interest on its bond debts (meaning it will get hungrier to escalate your estate taxes.) This isn't nearly as satisfactory a solution to the life expectancy quandary as retiring five years later than you once expected to, but you can't say we didn't warn you.
And as for what happened to Ben Franklin, you can read his will. He died a very rich man as a result of shrewd investments, later in his life. Ben left eight or nine houses, several thousand acres in several states, a gold-handled cane, and a portrait of the King of France surrounded by hundreds of diamonds. But it would not seem wise for the rest of us to count on accumulating that much new wealth, after attaining the age of sixty. The way things are going, once you attain your life expectancy, everyone should have some non-insurance plan for supporting himself for two or three extra years.
Over thirty Quaker retirement villages scatter through America, more than twenty in the suburbs of Philadelphia -- "under the care of the Yearly Meeting", as their expression has it. But for some people, community living seems unattractive. It does not speak to their condition.
For one thing, it may not be affordable.
Friends Lifecare
Or the style of may seem too fancy, or too plain, for some tastes regardless of cost. The increasing emotional rigidity of growing older is a factor; by the time people get to be seventy-five, they had better make this decision or forget it. Plenty of people are hale and hearty at ninety, but they establish pretty firm ideas about the sort of person they want for neighbors while they are still in the workforce. Quite often it's just a habit, people have lived in their home for several generations and cannot imagine another neighborhood, lifestyle, or environment. This is home, and they intend to die there.
So, to address this need, or market, a group of Quakers conceived of a retirement village without walls. Live in your own home and someone will come to oversee things, will know what to do if there is an emergency, and may eventually make the decision for you that you absolutely must go somewhere else. All of this is wrapped within an insurance vehicle, to recognize the fixed incomes of retired people, the inevitability of terminal illnesses, and the occasional risk of monumental medical expenses. At present, about 1600 people in Philadelphia are enrolled in the unique plan of Friends Lifecare at Home, making it one of the largest retirement communities in the country. The organization receives universal praise for its imaginative responses, as well as the dependability and high quality of the people it sends out to the homes of subscribers. Friends Lifecare is a pioneer, and it is gradually weeding out the ideas that didn't work and adding new features that were not originally contemplated. One of its greatest challenges is the need to adapt to unexpected and uncontrollable changes in the Medicare program. Slashes in the Medicare program could bankrupt Friends Lifecare, and even sudden windfalls like the Medicare Drug Benefit create management problems. There can be no doubt that one element of trust exists for which there is no substitute; Philadelphians know that the invisible support of the community and its Quaker core is behind them. If anyone can possibly preserve a moral commitment to the elderly, it will be the Quakers.
Ultimately, the commitment is not so much to 1600 subscribers as to the notion of finding out what works. Life expectancy has extended by three additional years, during the past ten; that's a joy, but it's a problem to finance. The optimum size of the organization is also an unsettled question. Although this program is relatively large by comparison with individual retirement villages, it may not be large enough to have spare capacity to cope with influenza epidemics or record-breaking spells of bad weather. Since it's the only one of its kind, it is vexed by the popularity in ever-widening geographic areas. It must grow to some reasonable size in one area before it can spread its resources to another. By the same reasoning, it must have a reasonable number of prosperous subscribers if it is to accept even a limited number of poor ones.
The idea of creating a seamless partnership with the residential-type retirement villages is certainly attractive, but Friends Lifecare must be careful to avoid becoming too much of a life raft for other people's problems. When the resale price of residential housing rises in a housing bubble, people wish to cling to a rising investment. During the same economic period, the entry and rental price of residential villages also rise. With a great many uncertainties that are specific to this pioneering effort, it is hard to know what policies to develop to insulate the lifecare environment from speculation in the mortgage and housing markets. Or, right now, high-rise apartment development. All of this creates a need for clear minds in the governance, determined to see and acknowledge difficult reality. If anyone can do it, Quakers can.
Before we get too deep into slicing average lives into average medical partitions, the reader should remember there is another way of viewing health care. Declaring we simply can't pay for everything because there are limited resources, we imply we agree on life's priorities when we really don't.
If this were a contest on TV, no two people might rank priorities the same way. But physicians would come closer. Reflecting common professional experience, most of them would give a special place to the first two years of life, and the last two. Health care costs concentrate there, and special reverence is paid to the patients. The rest of life has long quiet periods, but just about everyone is seeing or trying to see a doctor, during their first two and last two years. If we really must ration care, these are the years to be spared. These are the four years of maximum helplessness. We must keep it in mind. Special consideration is in order.
Last year of life insurance is life insurance, retrospectively paid after the death of the subscribers to his health insurance company. Although theoretically reimbursement could be made for actual individual expenditures, it is a more powerful idea to reimburse in the amount of the calculated average last-year costs of the community. It could loosely be said this approach constitutes 100% reinsurance of a selected peril, in order to suggest possible variations, such as 105% reinsurance (to transfer administration costs), 80% reinsurance (to encourage case management ), etc.
The last-year-of-life concept should be regarded as a tool for coping with certain problems inherent in the system of basing health insurance on employer groups. Employer-related health insurance is tax-favored, reduces marketing costs, and almost eliminates risk to the insurers; it is far easier to modify such a system than to reform it. However:
Non-random perils like AIDS may cause insurers to withdraw from ensuring particular companies or even whole industries.
Employees who retire early for reasons of health may find themselves unable to obtain health insurance after the COBRA protection period.
There is presently no method available for young people to guarantee their insurability before they enter permanent employment, or for employees of any age to guarantee their insurability in the event of company insolvency.
The risk of losing insurability is present in every change of employment; job immobility is created when fear of health insurance problems is on the employee's mind. Early retirement may be rejected for fear of exposure to loss of health coverage between the time of retirement and the onset of Medicare coverage.
Serious dilemmas for corporate funding of post-retirement health benefits have been created by a fear that voluntary pre-funding such obligations may create cash targets for corporate raiders. An employee has no legal rights to the prefunded reserve even though he may have legal claims for the eventual benefit obligations
Consequently, the most conservative present estimate of unfunded post-retirement health insurance obligation is $100 billion, and it may be four times that.
Since last-year-of-life insurance is life insurance, it might be provided as either term insurance or cash-value insurance. Although cash-value insurance has obvious advantages for the problems listed above, it would not enjoy the same tax-sheltering which term insurance would have, and consequently would require legislative relief to be fully effective. However, term insurance might well offer some relief for the AIDS problem.
Insurers are leaving the Washington DC area because of prohibitions against screening for AIDS, and Massachusetts also has a law against testing. The obvious first resort of an insurer is to withdraw from covering companies involved in the arts, design, theater, etc, and this tendency is paralleled by rapidly increasing detox and rehab costs for cocaine abuse, which have led to harsh exclusions for psychiatric care. The point is that employer-based insurance seldom includes a premium provision for risk, and if a particular peril cannot be excluded then a general class of service or a particular sort of employer is excluded as a proxy for it.
In this particular instance, it is proposed that insurers explore the willingness of their group markets to shift coverage of last-year costs from company-specific to community-rated premiums while continuing to be experience-rated for all other perils. If the various trade-offs were favorable, then insurers might be willing to discontinue offering last-year coverage except through the community-rated life insurance route. At present, the experience is probably insufficient to judge whether a market-driven voluntary approach would be effective. In the event, most companies proved willing to adopt the approach but insurers feared non-compliant competitors who saw an opportunity to steal business, then the public-interest need for legislation to protect the health insurance industry from disruption by the AIDS problem would have to be debated. For those who dislike compulsory solutions, it is exasperating to discover that the insurance industry generally prefers to be compelled by law since to move ahead in a cooperative manner is to invite anti-trust action.
In this particular instance, it is proposed that insurers explore the willingness of their group markets to shift coverage of last-year costs from company-specific to community-rated premiums while continuing to be experience-rated for all other perils. If the various trade-offs were favorable, then insurers might be willing to discontinue offering last-year coverage except through the community-rated life insurance route. At present, the experience is probably insufficient to judge whether a market-driven voluntary approach would be effective. In the event, most companies proved willing to adopt the approach but insurers feared non-compliant competitors who saw an opportunity to steal business, then the public-interest need for legislation to protect the health insurance industry from disruption by the AIDS problem would have to be debated. For those who dislike compulsory solutions, it is exasperating to discover that the insurance industry generally prefers to be compelled by law since to move ahead in a cooperative manner is to invite anti-trust action.
The preceding, or "term-insurance" approach has the advantage of gathering useful information about the last-year concept without requiring extra tax sheltering or even the formality of separate policies or insurance subsidiaries. It could be retrospectively tested on paper without much cost or any risk, and it might be held ready as a potentially useful tool for the eventuality of the AIDS epidemic provoking serious disruption of health insurance. However, much more important benefits might grow out of the cash-value life insurance or refunded, approach to last-year-of-life coss. Since last-year expenses come at the end of a 70+ year life expectancy, the opportunity for compound interest to work is at a maximum.
Under this approach, the initiative would lie with life insurers, who would be induced to include a standard beneficiary clause in their policies. That clause would assign the community-average last-year health cost reimbursement to any health insurance company which had assumed those costs and had previously provided the beneficiary with appropriate consideration for making the assignments. (At the moment, the various secondary adjustments between employer, employee, health insurer, and tax collector can be left to the marketplace to work out. If no one makes an adequate offer, the beneficiary simply has some life insurance).
The cost of such insurance might turn out to be fairly modest. Although average last year-of-life health costs might be guessed to approach $20,000 per death, the comparatively low death rate before the age of 65 means that an average life insurance policy of less than $5000 (with proceeds exhausted at 65) could conservatively be guessed to cover that need. After age 65, every person can reasonably expect Medicare to have a last-year obligation. Using a 65 investment assumption, the present value of such policy would be $250 at birth; a 3% assumption would only be $500 and would allow general inflation the economy to be ignored. (The $5000 figure would seem to allow generous room for potential innate health-care cost inflation, inasmuch as last-year coverage does not require any provision for recovery from one formerly-fatal condition only to die later of a second fatal condition, which is the main cause of "innate" health cost inflation.) Presumably, the best protection against future health cost escalation is to purchase more insurance than is thought to be needed, expecting any surplus to flow into the estate. Even taking a conservative view of the health-cost escalation problem, its possible to imagine premium costs of $100 per year during thirty years of working life.
Although the marketplace could be expected to determine how much reduction in health insurance premium would be accorded for the lifting of last-year risks, the main value of this coverage would appear in the case of someone who was uninsurable (? ie unemployable?) without it, or who would have been afraid to switch jobs without it. When individuals sustain periods of loss of income, the possession of this insurance might be regarded as a form of catastrophic health coverage, which for the temporarily unemployed might be an absolute minimum coverage. The reasoning is that this type of coverage can be switched on or off; a treaty of assignment need only be signed if the individual finds it advantageous to use it, and is later revocable at will. The policy, in short, is his not his employer's but can be made to coordinate with employer benefits.
Medicaid programs are rather dubious candidates for this approach but even they might be induced to be more generous with last-year coverage (probably under either a term-insurance or waiver-of-premium approach) than they have typically been with full health insurance, the becaused potential for abuse is eliminated.
Finally, the relationship with Medicare needs to be explored with HCFA. After all, Medicare is the main health insurers of fetal illness costs. Far from ever escaping these costs, Medicare has a major concern that it may also have to assume long-term custodial and nursing home costs. Far from ever escaping these costs, Medicare has a major concern that it may also have to assume long-term custodial and nursing home costs. In this matter, Nature provides a certain trade-off. Dying young and outliving your income are both tragedies, but few people have both of them. There is a need to consider ways of transferring costs between the two largely-exclusive problems. The aggregate community cost of fatal illness after age 65 is much heavier than it is up to age 65; possibly $20,000 average coverage would be necessary. Since compound interest would have longer to operate, however, the premiums or present-value costs would not necessarily be proportionately larger. A premium of $40 (1988 dollars) could be imagined; there is no reason why premiums could not be inflation-adjusted on a yearly basis as an alternative to making overly conservative interest-rate assumptions.
The proposal is to explore with HCFA he attractiveness to them of providing some degree of long-term care coverage in return for surrender to them at age 65 of paid-up life insurance adequate to cover fatal-illness costs.
QUESTION: If the health insurer agrees to lower his premium, and subsequently pays the last year costs for the subscriber, how can he be assured the life insurance will eventually reimburse him?
Since health insurance is mostly in employer groups, covering only expenses n the current year, the health insurer can limit his concern to the current year. The health insurance annually needs a slip of paper guaranteeing payment by a life insurer, in the event of client death. Three main methods are available, each with implications about who owns and controls the process:
One method is to follow the reinsurance model strictly; the employer pays the health insurer, who then pays a life insurer for "reinsurance". In this case, the health insurer controls the process, which is almost invisible to the employer an employee.
Where the employer already has a group life insurance benefit, he might well wish to send the check directly to the life company for a somewhat larger benefit(simultaneously reducing the payments to health insurer). While this approach gives control to the employer, it also gives him the headache of negotiating the premium adjustments.
Both of two foregoing approaches would be administratively very convenient, but neither one provides the employee with portability between employers, bridging of episodic gaps in employment, etc. For the employee to take advantage of portability, carriers other than the company carrier must be utilized. The employer's health carrier would then need yearly slips of paper from a number of life carriers, most easily obtainable as part of the yearly premium billing process for the life insurance. Such a paper would amount to a rebate coupon, issued by the life insurers, honored by the health insurer.
It is essential to keep paperwork simple for an estimated premium of about $100 a year for a term an $400 a year for cash-value life insurance (of course, only$100 of either would be transferred to the health insurer). Consequently, insurance management would want to look into bulk communication: "Dear Health Insurer, Our records show the following clients have exclusively assigned the average last-year health benefit to your company for deaths which might occur during the period between A and B. Yours Truly, Life Insuror"
Because of the problem of differing premium dates, the insurance industry might further wish to agree on a calendar or other standardized year definition for this type of coverage. The administrative issue can be stated in the plainest possible term: the extra administrative cost of this approach is the price of portability.
QUESTION: No underlying health insurance.
Although an individual with cash-value life coverage could borrow against it to pay health costs, terminal or otherwise, the issue has been raised as to how someone would employ the life insurance mechanism if he did not have any underlying health insurance, but did have term life insurance. Alternatives would be:
He could purchase health insurance with a front-end deductible equal to the face value of the life insurance. MONY sells a $25,000 deductible policy for about $200 a year family premium, with a $1,000 top limit. Such a combination would protect for more than just terminal illness, but it would not protect against more than one heavy cost. For what would presumably be a very low extra premium, he would need another reinsurance policy to cover multiple illnesses. Such reinsurance might have two parts: one part to cover the remote possibility of exceeding the deductible more than once, and another part to cover the deductible on what proved to have been a non-fatal illness. This degree of coverage goes considerably beyond the last illness concept and would naturally cost more.
The main problem with this life-insurance-to-pay-off-the-high-deductible approach is that it presumes the beneficiary would pay his bills in cash and contains no way to spread the risk. Therefore, everyone ends up either overinsured or underinsured. A smaller issue is that he would pay full charges without a way to negotiate volume discounts at hospitals. Taken together, this approach would be unnecessarily expensive.
An approach more narrowly related to the cost of terminal illness would be for the life insurer to pay last-year costs, large and small, but only reduce the net death benefit to the estate by the average community terminal illness cost rather than the actual case-by-case expense. Once the average rate had been established, it would become possible to tailor the insurance coverage, leaving a suitable margin for year-to-year inflation and other contingencies.
The degree to which carriers could pool claims data in arriving at the average cost is an anti-trust question; the definition of a covered expense is purely a question of practicality within claims administration. However, differences of opinion about the feasibility of different coverages might make data sharing less practical.
QUESTION: What if there are multiple carriers involved?
On examination, this question relates mainly to carelessness, misunderstanding or incompetence on the part of the subscriber. Even if the individual has multiple life insurance carriers, he would be foolish to execute a last-year beneficiary clause with more than one of them. Consequently, no such clause should be permitted unless it defines the primary carrier for last-year purposes as that carrier with the earliest date of execution of such a clause which is still valid at the time of death.
With regard to multiple health carriers, the life carrier would generally take the position that he is only going to pay so much, and the health carriers can work it out among themselves. The reasonable division of the award would be in proportion to the degree the health insurers had paid out the actual health costs. No doubt there would be instances of multiple health insurance coverages of someone who dropped dead with no medical costs at all. If the reimbursement were on the basis of average community costs, lawyers for the health companies would no doubt exercise their imaginations in court, but the life insurer would be serene, and the situation would soon clarify itself with case law.
It is somewhat more difficult to contend with the possibility that the life insurance clause would authorize payment of actual individual costs, only to discover that the beneficiary had over insured himself with multiple health carriers, without coordination of benefits clauses. The life carrier would thus be in a poor position to know just what the actual payments by the two contending health insurers had been, and how much overlap or legitimacy there was to them. It follows that the subscriber who requests that individual actual reimbursements rather than average community ones be made, must also be required to specify whether he wants all carriers reimbursed, or only the primary, or only the largest, payor. With the life carrier thus immunized, it becomes the responsibility of health carriers not to reduce their premiums or make other concessions to the subscriber in return for a last-year treaty unless the subscriber can satisfy them that their agreement meshes with the life clauses, or that the subscriber agrees to the coordination of benefits.
In a love song written by T.S. Eliot, the character named J. Alfred Prufrock complains that as he grows old, he wears the bottom of his trousers rolled. College freshmen who encounter this line are apt to glide over it, uncomprehending, but the allusion will eventually grow clearer. The old man tends to find his legs have apparently grown shorter because he has to roll up his pants to keep them from dragging on the ground. Although the cartilages in his knees, hips and the lower spine may have compressed a little, the shortened legs are more apparent than real. The pants seem longer because his belt line has dropped. Dropped below his pot belly, that is.
No medical textbook that I know contains much discussion of pot bellies, even though they are almost universal, and universally noticed. The muscles of the belly wall relax, allowing the guts to bulge forward over the pubic bone.
Even doctors don't know enough about this disorder of old age
The aging lungs tend to enlarge, pushing the guts downward. The spine bends forward, and of course, the fat tends to increase inside the abdominal cavity. If there has not been too much weight gain, the pot belly tends to flatten out when its owner lies down on his back; if the weight has been gained, the pot sticks up like a pregnancy, obscuring the lower edge of the rib cage, bulging out at the sides. Normally, a young person's abdomen is described as "scaphoid" or hollowed out like the inside of a rowboat. A skinny young woman has wider flaring hip bones, exaggerating this scaphoid appearance, and making the waist narrower by allowing the guts to drop down into the larger pelvic cavity. Younger people are more active, with more muscle tone holding things together somewhat better.
Anyway, when the older person rolls over in bed, the innards of the belly cavity get squashed against the mattress. The old man's prostate leads to a fuller bladder, which means he gets up earlier when he rolls over it and gets up a lot earlier if he is overweight and has more pot belly. Or it may be the upper stomach that gets squashed, forcing the acid stomach contents up the esophagus and resulting in heartburn, burping, and even cough or hoarseness if the acid gets up into the throat and back down the windpipe. With weight gain, the pressure of lying prone can press against the main leg veins as they cross the brim of the pelvis, resulting in swollen ankles. Since the large intestines are coiled and kinked, external pressure against them causes a minor degree of obstruction which can be experienced as constipation or sometimes bowel urgency. Since the bowels contain a fair amount of gas, pressure on them causes small gas bubbles to merge into larger bubbles, with resulting flatulence which can reach startling proportions in the early morning hours. For all these reasons, people with pot bellies tend to sleep on their backs, causing a lot of snoring. If they snort and waken, they may have night time insomnia, daytime drowsiness. One sure sign of this is that the bed partner flees to a separate bedroom.
Victims of this affliction may, if they choose, imitate Scarlett O'Hara in that famous scene in Gone With the Wind with the slave girls pulling a tight corset even more painfully tight, but corsets are currently out of fashion. Or they can take purple pills to correct the heartburn, or regular laxatives for some of the other problems. In general, however, leg-lifting exercises strengthen the belly wall muscles (abs, I believe they are called), and losing weight by eating less does the rest. Losing weight is never easy, but in this case, a few pounds can make big differences in belly circumference, as measured by the belt size. Nothing will shrink the enlarged lungs pushing down, however, and arthritis of the spine may maintain the forward stoop. Very few older people are complete without some signs of this common affliction. Even so athletic a person as the ramrod-straight George Washington developed just a little pot. And Benjamin Franklin, of course, had a hopeless case.
The Duchess of Windsor was reported to say, a woman can never be too rich or too thin. Perhaps, but with insurance you state -- in advance -- how much insurance you can buy, best not expect more. In healthcare, it's my hunch something drastic would have to change before the American public voted an assessment for more than $3300 per person, for every working year from age 26 to age 65. In fact, if it went much higher, many people would probably look for a way to escape the burden. Perhaps we could supplement 3% per year, the historical rate of inflation for the past century. That's fair because although it would reach $10,000 at age 65 instead of $3300, everything else would have readjusted to give it the same financial impact. Similarly, asking people 26-65 to pay for all ages is more palatable if it's arranged as your own childhood and retirement to be supported.
Excluded: Past debts and Custodial Care. In any event, any payments for past debts, for health or otherwise are not envisioned in the following plan. The term "fixed income" reminds our debt and equity obey different rules, and the premise is the income supplement of this calculation will be based on equity, common stock. Furthermore, we know the National Debt, but how much of it once paid for health services, is fuzzy. When I started this analysis, I really never dreamed all of the current healthcare costs might be covered by investment income from common stocks, and it's going to take some experience to be sure even that is reasonable. It allows us to take a stance: if it won't pay current costs, at least it will pay for some of them. If it more than pays for them, annual deposits should be reduced, never confiscated. To avoid circumvention by changing definitions, it might be well to state custodial care costs are not included, either, because they are treated as retirement income.
Medicare. Making it easier to explain, let's begin at the far end of the process, the day after death, looking backward. This proposal didn't initially include a Medicare proposal, but the accumulation of its unpaid debt has become so alarming, considering Medicare within Health Savings Accounts could fast become a national priority having no other solution. In addition, most factual health data come from Medicare, so the reader gets accustomed to hearing about it. So, while the Medicare situation is fraught with political obstacles, we might have to risk them. While debt overhang from earlier years continues to grow, Health Savings Accounts cannot be confidently promised to rescue Medicare by itself. But perhaps at least the Savings Account discussion could put a stop to going deeper into debt. Even a stopgap would have to get started pretty soon, but there is also a chance an improving economy might partially reduce the indebtedness.
Medicare-HSA Overlaps. At present, Catastrophic coverage is required for Health Savings Accounts, but its premiums are not tax-exempt. To extend HSA for the life expectancy, therefore, requires an additional average of 18 years of after-tax premiums. We have split lifetime HSA into two parts at age 65 and assume a single-premium ($80,000) exchange for Medicare, possibly traded for partial forgiveness of premiums and rebate of payroll taxes. It is important not to count the $80,000 twice if it assumed to be self-financed. One quarter from payroll taxes, one quarter from premiums, and a half from the $80,000 which used to be from the taxpayers. If pre-payment begins at an early age, Medicare costs might be quite modest after growth from income. Even when we show all the costs, including double payments, using an HSA at conservative rates like 4% will reduce the Medicare cost by 75%. Better performance depends heavily on approaching 12.7% by passive but hard-boiled investing. To pay down the existing debt back to 1965 is not contemplated by this proposal. At present, it grows by 50% of annual costs by addition; and an unknown amount by compounding. The amount of debt service is probably going to depend on the national ability to pay it down, regardless of its written terms. The same is likely to be true of subsidies for the poor. Ultimately, both of these decisions are political, limited by the ability to pay. Because of the long time periods, comparatively modest interest rates could convert this impending disaster into a manageable cost, but it should not be contemplated until net investment returns approach 12.7 %. The outcome of these intersections is that the terms and benefits become largely a matter of political choice. That has been true for a long time, yet no effective corrections have been made. It is perhaps unbecoming of a citizen to say so, but the political system needs some steps taken to increase its sense of urgency.
Disintermediation of Investment Returns. By this reasoning, the rescue of Medicare depends on the political choice to do it, and the avoidance of a collision with the financial industry. Without a solution to the Medicare problem, a solution to paying for healthcare at younger ages becomes quite feasible, but it would be useless. Conversely, solving Medicare would be possible if the problems of younger people were ignored, but that is equally unlikely. To solve healthcare financing for all ages depends on introducing some new feature, and the easiest solution to imagine is to raise effective net interest rates. Interest rates are unusually low at present, and the Federal Reserve probably feels it would be dangerous to raise them. However, that's the easy part, because interest rates are certain to rise, eventually. What's much harder to envision is to flow the improved rates and the transaction-cost efficiencies through the financial system without wrecking it. What's hard to imagine is not hard to seem feasible, however. It is to take investments averaging 12.7%, flowing 10% past the intermediaries to the investor; and keeping it up for a century. Disintermediation, so to speak.
Rationalizing Fragmented Payments The transition to a solvent system could be greatly eased by the present premiums and payroll deductions, which are largely age-distributed, and can, therefore, be forgiven in a graduated manner for late-comers to the program. Most redistribution of high-cost cases should be handled through the catastrophic insurance, which is well suited for invisible and tax-free redistribution. Because of hospital internal cost-shifting, inpatients are overpriced, rapidly heading toward underpricing. This distortion of prices is achieved by squeezing inpatient prices with the DRG to shift costs and overpricing to hospital outpatients. In the long run, distorting prices has the effect of raising them. This will more immediately affect the relative costs of Catastrophic and Health Savings Accounts and should be more carefully monitored, with an eye toward re-achieving equilibrium.
Dual Reimbursement Systems are Better Than One At present costs, statisticians estimate average lifetime healthcare costs at about $325,000 in the year 2000 dollars; we could discuss the weaknesses of that estimate, but it's the best that can be produced. Women experience about 10% higher lifetime health costs than men. Roughly speaking, how much the average individual somehow has to accumulate, eventually has to equal how much he spends by the time of death. At this point, we must work around one of the advantages of having separate individual accounts. On the one hand, individual accounts create an incentive to spend wisely, but it is also true that pooled insurance accounts make cost-sharing easier, almost invisible, and (for some) tax-free. Therefore, linking Health Savings Accounts with Catastrophic insurance provides a way to pool heavy outlier expenses, while the incentive for careful money management resides in the outpatient costs most commonly employed (together with a special bank debit card) to pay outpatient costs. Such expenses are much more suitable for bargain-hunting anyway because dreadfully sick people in a hospital are in no position to bargain or resist.
Internal Borrowing. Furthermore, there is a significant difference between mismatches of aggregate revenue-to-expenses of an entire age group, and outliers within the same age cohort, the latter much likelier to be due to chance. To put it another way, somebody has to pay these debts, and the plan has been designed to break even as an entirety. Surely we must have a plan about who should pay them when enough revenue is not yet present in a new account. Surely some groups are always in surplus, other groups are always in arrears; the two should be matched, at low or zero interest rates. Borrowing between sick outliers and lucky good people within the same age cohort should pay modest interest rates, and borrowing between different cohorts for things characteristic of the age (pregnancy, for example) should pay none. Unfortunately, some people may abuse such opportunities, and interest must then be charged. Until the frequency of such things can be established, this function of loan banking should be part of the function of the oversight body. When it's limits become clearer, it might be delegated to a bank, or even privatized. While it is unnecessary to predict the last dime to be spent on the last day of life, incentives should be identified by the managing organization, separating structural cash shortages from abusive ones. Much of this sort of thing is eliminated by encouraging people to over-deposit in their accounts, possibly paying some medical bills with after-tax money in order to build them up. Such incentives must be contrived if they do not appear spontaneously. User groups can be very helpful in such situations. People over 65 (that is, those on Medicare) spend at least half of that $ 325,000-lifetime cash turnover, but just what should be counted as their own debt, can be a matter of argument (see below.)
Proposal 10: Current law permits an individual to deposit $3300 per year in a Health Savings Account, starting at age 25, and ending when Medicare coverage appears. Probably that amount is more than most young people can afford, so it would help if the rules were relaxed to roll-over that entitlement to later years, spreading the entire $132,000 over the forty-year time period at the discretion of the subscriber.
Bifurcated Health Savings Accounts. When Health Savings Accounts were first devised, it never seemed likely that Medicare might be supplanted. However, Medicare has grown both highly popular and severely under-funded, probably running at a large loss. The rules should be modified to permit someone who has health insurance through an employer to develop a Health Savings Account which the funds but does not spend while he is of working age. The funds would then build up, enabling him to buy out Medicare on his 65th birthday or thereabout, with a single-premium exchange at present prices, (exchanging about $100,000 funded by the forgiveness of Medicare premiums and some portion of payroll deductions from the past). He would have to purchase Catastrophic coverage at special rates. If this approach proved popular, it might supply extra funds for loaning to HSA subscribers in the outlier category. While there is no thought of phasing out Medicare against the subscribers' will, Congress would certainly be relieved to have subscribers drop out of a program which must be 50% subsidized.
Proposal 11: The present closing age for HSA enrollments at the onset of Medicare should be extended a few years older. And single-premium buy-outs of Medicare coverage, including the possible return of payroll deductions where indicated, should be permitted as an option.
Proposal 12: Congress should create and fund a permanent Health Savings Account Agency. It should have members representing subscribers and providers of these instruments, with the power to hold hearings and make recommendations about technical changes. It should meet jointly with the Senate Finance Committee and the Health Subcommittee of Ways and Means periodically. It should be involved with the appropriate Executive Branch department, to review current activity, detect changing trends, and recommend changes in regulations and laws related to the subject. On a temporary basis, it should oversee inter-cohort and outlier loans, leading to recommendations concerning the size and scope of this activity.
Single-Premium Medicare, age 65 Hypothetically, if anyone could live to his 65th birthday without spending any of the accounts, a prudent investor would have accumulated $132,000 in pure deposits on his 65th birthday. He only needs $80,000 to fund Medicare as a single-payment at age 65, however, so he can even afford to get sick a little. If he starts later than age 25, he has already paid for Medicare somewhat, with payroll taxes. That could be considered payment toward reduction of the Medicare debt.
If someone makes a single deposit of $80,000 on his/her 65th birthday, there will accumulate $190,000 in the account over the next 18 years, the present life expectancy if he spends nothing for health and invests at 5%; and $190,000 is what the average person costs Medicare in a lifetime. Since the average person spends $190,000 during 18 years on Medicare, enough money will accumulate in Medicare to pay its expenses, and after some shifting-around, this should make Medicare solvent, in the sense that at least the debt isn't getting bigger because of him. Furthermore, index funds should be returning 10-12% over the long haul, so there should be some firm discussions with the intermediaries about some degree of dis-intermediation. Please don't do the arithmetic and discover that only $40,000 is needed. That seems plausible, but that's wrong because the costs remain the same , and previously the government has been borrowing half the money from foreigners. In effect, the subscribers have been paying the government in fifty-cent dollars, while claiming the program is entirely self-funded. There has been an exchange of one form of revenue for another, so the required revenue actually does demand $80,000 for a single deposit stripped of payroll deductions and perhaps premiums. An end would be put to further borrowing, but the previous debt remains to be paid. I have no way of knowing how much that amounts to, but it is lots. All government bonds are general obligations, mixed together, while access to Medicare reports back to 1965 is not easily available. What we can more confidently predict is the limit young working people can afford for the sole purpose of paying off the Medicare debts of the earlier generation. If there are other proposals for paying off this foreign debt, they have not been widely voiced. And the debt is still rapidly growing.
Escrow the Single Premium A young subscriber would have to set aside an average of $850 per year (from age 25 to 64) to achieve $247,000 on his 65th birthday, assuming a 5% compound investment income and relatively little sickness. This might seem like an adequate average, but occasional individuals with chronic illnesses would easily exceed it in health expenditures. Assuming a 10% return, he would have to contribute $550 yearly. It is not easy to estimate the size and frequency of expensive occurrences in the future, so someone must be designated to watch this balance and institute mid-course adjustments. As an example, simple heart transplants costing $200,000 are already being discussed. To some unknown extent, the cap on out-of-pocket expenses would have to be adjusted to pass these cost over-runs indirectly through the Catastrophic insurance. Insurance does greatly facilitate sharing of outlier expenses, but usually requires a time lag whenever new ones appear.
It does not require much political experience to know taxpayers greatly resent paying debts that benefitted earlier generations. They complain, but complaining does not pay off the debts of the past. To double required deposits in order to pay off past debts, as well as using forgiveness of payroll deductions and premiums, would require an additional $120,000 per year escrow, for each year's debt accumulation. At present, roughly $ 5300 per beneficiary, per year, is being borrowed, and there are roughly twice as many current beneficiaries as people in the tax-paying group, but for only 18 years, as compared with 40 years as a prospective beneficiary. So that comes to liquidating roughly $1300 a year of debt to balance the two populations or $2600 a year to gain a year. That's for whatever the debt happens to be, which surely someone can calculate. To accomplish it, one would have to project an average of ??% income return. That's definitely the outer limit of what is possible, and it probably over-reaches a little. Therefore, to be safe, one would have to assume some other sources of income, a change in the demographic patterns, or an adjustment with the creditor. Assuming inflation will increase expenses equally with inflation seems a possibility. And it also seems about as likely that medical expenses will go down, as that they go up. You would have to be pretty lucky for all these factors to fall in line over an 80-year lifetime.
Medicare: Optional, Mandatory, or Third Rail? It is this calculation, however rough, which has made me change my mind. It was my original supposition that multi-year premium investment would only apply up to age 65, and that would be followed by Medicare. In other words, it should only be implemented as a less expensive substitute for the Affordable Care Act. It seemed to me the average politician would be very reluctant to agitate retirees by proposing a plan to eliminate Medicare. They would feel threatened, the opposing party would fan the flames of their fears, and the result would be a high likelihood of undermining the whole idea for any age group, for many years. Better to take the safer route of avoiding Medicare, and confining the proposal to working people, where its economics are overwhelmingly favorable.
But when the calculations show how close this proposal under optimistic projections would come to failure, and when nothing remotely close to it has been proposed by anyone, the opportunity runs the risk of passing us by. So, I changed my mind. The moment of opportunity is too fleeting, and the consequences of missing it entirely are too close, to worry about the political disadvantages of doing the right thing. The transition to a pre-funded lifetime system will take a long time to get mature, and the political obstacle course preceding it is a daunting one. However, there is another way of saying all this, which is perhaps more persuasive that Medicare must be changed. It begins to look as though the unfunded and accumulated debts of Medicare are such a drag on our system of government, that very little can be accomplished by anyone, until this central problem is addressed. In that sense, our problem is not the uninsured or the illegal immigrants, or an expensive insurance system. Our problem has become Medicare underfunding, and our second problem is that everyone loves Medicare.
The "simplified" goal is therefore for everyone to accumulate $80,000 in savings by the 65th birthday, remembering that savings get a lot harder when earned income stops and definitely remembering that people approaching retirement are not likely to part readily with $80,000. With the current law, you would have to start maximum annual depositing in an HSA of $3300 by your 52nd birthday, to reach $80,000 by age 65, and you would still need 10% internal compounding to make it. With a 5% return, you would have to start at age 48. But notice how easily $200 a year would also get you there, starting at age 25 (see below) but it immediately gets questionable to assume $700 a year deposit for a 25 yr-old receiving 5% returns. We are definitely reaching a point where the ideas proposed in this book will no longer bail us out of our Medicare debt. Because -- the most optimistic of these projections are achieved by assuming there will be no contributions at all from people aged 25-65, for their own healthcare, babies, contraceptives and whatever. Many frugal people might skin by with looser rules; But the universal goals of the past are just that, the goals of the past. If we are going to cover lifetime health costs instead of just Medicare, many more will need $80,000 to do it and have something left to share with the less fortunate. But to repeat, that still compares very favorably with the $325,000 which is often cited as a lifetime cost. Unfortunately, that just isn't enough, the Chinese will have to wait for repayment. This book was not written to propose a change in Medicare, but in writing it I do not see how we get out of our healthcare mess without addressing Medicare. If politicians can be persuaded of that, at least we will no longer need to invent reasons for urgency.
Starting with the Medicare example. Notice that forty years of maximum contributions would amount to far more than the necessary $40-80,000 by age 65. We haven't forgotten that the individual is at risk for other illnesses in the meantime, so in effect what we need is an individual escrow fund for lifetime funding intended (at first) only to replace Medicare coverage. (We are examining lifetime coverage, piece by piece, trying to accommodate an extended transition period.) Depending on a lot of factors, that goal could cost as little as $100 a year deposited for forty years at high-interest rates, or as much as the full $1000 per year with low rates. It all depends on what income you receive on the deposits in the interval. In a moment, we will show that 10% return is not impossible, but it is also true that a contribution of $1000 per year would not seem tragic, compared with the present cost of health insurance (now averaging over $6000 a year). I have unrelated doubts about the current $325,000 estimate of average lifetime health costs, but that is what is commonly stated. For the moment, consider these numbers as providing a ballpark worksheet for multi-year funding, using an example familiar to everyone, but not necessarily easy to understand after one quick reading.
The Cost of Pre-funding Medicare. Rates of 10% compound income return would reduce the required contribution to $100 per year from age 25 to 65, but if the income were only 2% would require $700 contributed per year, and at 5% would require $300 per year. Remember, we are here only talking of funding Medicare, as a tangible national example, Obviously, a higher return would provide affordability to many more people than lesser returns. Let's take the issues separately, but don't take these preliminary numbers too literally. They are mainly intended to alert the reader to the enormous power of compound interest. Let's go forward with some equally amazing investment discoveries which are more recent, and vindicated less by logic than empirical results.
Joseph Schumpeter's famous slogan "Destructive Innovation" fails to mention an important feature: sometimes, the cost of destruction can be greater than the profits from the innovation. The destructive effect makes its appearance early when the innovator is likely to have the insufficient startup capital to overcome a stagnant but politically powerful existing alternative. A suspicion arises that undeveloped markets, lacking "national champions", might actually have an advantaged location to perfect and exploit an innovation.
Kenya seems to present examples of several of the issues. Regardless of whose idea it was, the British but Los Angeles Headquartered Qualcomm Corporation seems to have recognized the potential of electronic banking and hired IBM to develop the technology. Ignoring the British and American markets, they started the M-Pesa Corporation in Kenya and Tanzania, where they quickly assembled 15 million customers producing a 27% profit margin, in spite of a 10% rate of attrition by fraud. Competitors are experiencing similar mixtures of success and failure in India. After the kinks are worked out in Africa, Qualcomm presumably might then be in a position to exploit its experience toward defeating conventional banking competitors in the developed world. Its recent stock market decline may suggest fierce competition even in darkest Africa, or it may suggest an investment bargain. But it illustrates the changing issues within technology innovation.
According to reports, M-Pesa eliminates the cost of branch banks by combining the ideas underlying Bill-Pay and Pay-Pal. Others can do the same. Africa may have few strong banks but has millions of wireless telephones. The customers deposit money by phone by increasing the phone charges and then direct its payment by phone. Leverage is developed by outsiders depositing extra money to lend, and thus the basics of banking are assembled inexpensively. A charge to use the system is added, with a surcharge for paying the bills of non-members. The system attracts fraud, but apparently, there are enough honest people starved for banking services, that profits absorb the cost. Bitcoin employs different technology but many of the same concepts, so conventional branch banks are not the only competition. Unless they change ancient ways, somebody is eventually likely to upend conventional banks in developed nations, although it may not necessarily be Qualcomm.
So, many of the objections to substituting new currencies for higher-cost branch banking are surely going to be tested by some system, anyway. Branch banking has been successful for a long time, so it is not likely to collapse because of internal contradictions alone. Innovative competitors are going to have a rough time overturning a useful system, need not be addressed here, so we confine this overview to the peculiarities and specific advantages of a currency replacement by index funds. Are they here to stay?
It may be a surprise, but the concept of a Limiting Factor (the Law of Perpetuity) may once again intrude the U.S. Supreme Court into the Affordable Care Act. It may also be a little hard to follow, so pay attention to what would ordinarily be regarded as a dry subject.
The concept of a limiting factor makes modern law, and possibly modern economics, possible. Several centuries ago, well before the US Constitution was written, lawyers came to see that many things are only possible if you don't carry them too far. The operation of compound interest is an example. In ordinary human commerce, the tendency of compound interest to rise over time leads to an eightfold rise over one lifetime of 84 years (48 in 1901 to 84 in 2017). A 200-year lifetime would lead to even more rise, to the point where one dollar invested at birth at 7% would pay for the entire average medical cost of a lifetime of $350,000 expressed in the year 2000 dollars. But quite obviously, if some scientist discovered a drug which lengthened life that much, something in the law would have to be changed to hold the economic world together.
So, about three hundred years ago, some English judge laid down the Law of Perpetuity, stating that Trust Funds may not endure for more than one lifetime, plus 21 years. It's proved to be a useful limiting factor, not likely to be changed easily. Congress might feel empowered to change it, but too much of modern commerce revolves around this definition of perpetuity, for the public to permit tampering without huge uproar. Notice the flexible wording: 21 years plus one life expectancy. Changing life expectancy would not invalidate the law.
A century ago, life expectancy was thirty years shorter, five doublings at 7%. And now it is more than eight doublings or in effect (2,4,8,16,32,,64,128,-->)256 times the original number. But that doesn't matter, because the law only effectively states its limit is 2 doublings (four times as much) more than the life expectancy at birth. A century ago, that implied two hundred-fifty-fold increase more than the starting amount at birth, and today it implies a thousand times. Inflation chugs along at 3% simple interest in both cases, at a growth rate doubling in 24 years (72/3). That's three doublings at simple interest a century ago, versus four doublings today. The important present difference is the thousand-fold compounded gain, compared with only 256-fold compounded at 7% a century ago, a seven-hundred-fold difference in the base price. The problem we have nevertheless still threatened less than forces opposed to changing the Perpetuity age limits.
To summarize, compound interest on Medicare-linked investment has gained six or seven hundred-fold over inflation in a century, as a result of medical progress bumping against mathematical principles. This difference is not likely to change in the coming century, because longevity at birth would have to increase to age two hundred to overwhelm the judges into changing the age limits of such a fundamental law. If net Medicare-linked costs rise to approach that level, moreover, this revenue opportunity might disappear.
There is no reason to avoid exploiting this opportunity while it lasts. It presents a quick and dirty solution to the present urgent problem, which is to find alternative proposals for reforming transition to healthcare financing, in case the Affordable Care Act is suddenly repealed. At the present time, the opportunity to reduce the effective cost of transition lies in the gap between the average age of death and the Law of Perpetuity -- about twenty years. At 7%, that's two doublings or four-fold profitability. The question becomes whether to raise the term limit of the Health Savings Accounts above its present level of the age of Medicare attainment. The natural instinct would be to terminate the HSA at death, but the Perpetuity law would permit 21 years more. Since the life and health of the depositor has very little bearing on this subject, Congress has the opportunity to allow Trust funds to continue to earn investment interest after death, until either its Medicare funding debts are extinguished, or the birthdate of the deceased depositor reaches 104 and is terminated by the unchanged Law of Perpetuity. The effect of doing this would multiply the funds for the transition by 400%, and largely solve the problem if the Trust applied all funds to the debt incurred when offered the opportunity to choose. When we get to that subject, the transition is the big obstacle for three reasons: 1) There may not be enough money to do it. 2) The transition may take too long if it is constrained by available funds. 3) And the courts may find some reason to block it.
As a non-lawyer, I can see no technical reason why this could not be done, but some reason might be invented for political reasons. Unanticipated problems might arise, but under present law the challenge would probably come through the State courts, using the Tenth Amendment as a basis. If the adoption of the idea is voluntary with the States, or if demonstration projects are employed, a conflict between jurisdictions is very likely, and the U.S.Supreme Court would have to settle the conflict. This split approach might satisfy both State and Federal proponents enough to remove the obstacle, because the Wickard v. Fillmore decision still rankles after eighty years, and after much longer than that from the Civil War, memory of which still greatly affects the regional popularity of federalism.
Several other ways to pay for the transition costs, or shorten the transition time, will be offered in later chapters. But only this simple change is required early in the process, and so only this proposal will transform transition from a plan to a process. It has always bothered me for a complete transition to take nearly a century, during which interval there would be many changes of political control of Congress. In turn, those transitions offer a chance to smother central concepts in a welter of obfuscation. And that applies to all transitions, suggesting original planning should always be followed. To a certain degree, that has sometimes proved useful, but the transition in this particularly vexed case is going too far with it. So having major alternative approaches, and thus creating opportunities for later innovation, seems on balance a worth-while addition.
Among the many things we don't know about the future, is the average longevity eighty years from now. The whole-life insurance industry prospered when they sold policies assuming American longevity of 47 years in the year 1900, and it turns out to be 83 today, still growing fast. If longevity should get shorter, as it recently has in Russia, life insurance would go out of business. Since we can't rely on projections, we have to rely on early observations and make mid-course corrections.
President Lyndon Johnson both underestimated how much Medicare would cost, and how politically successful it would be. He was in no position to multiply 50 million Americans times $11,600 per year per person, times 22 years per person. That simple sentence tells you all you need to know about current Medicare costs, but who knew? Nor could he know how fast longevity would grow, or how fast the cost would rise. But we can monitor the trend, extrapolate, and revise the extrapolation. Medicare was a medical success, which had to be paid for; and President Johnson's successors might have found that out a little sooner, and changed course. If we must find fault, failure to readjust early would be my candidate.
So, who is counting?
Quis custodiet custodies?
For reasons obvious or not, the nation would be well served to create a monitoring agency for the guidance of future Congresses in charge of the type of Health Savings Accounts we already do have, and maybe some related issues. When we start envisioning lifetime coverage, it becomes even more vital to have a permanent agency to sort out what is happening. This is particularly important when the Branches of the Federal Government are divided between the two parties. Informally, the subcommittees of the Appropriations Committees have assumed much of the burden of overseeing agencies. They are the only Congressional Committees to review every program every year. However, the Agencies have grown to be the largest bureaucracies in the government, and tend to become jealous of their independence, as the Appropriation Committees grow too burdened to bother with them. It begins to look as though we need more Congressmen if we want Congress to maintain closer control of the agencies. Each Congressman now represents a million constituents, and simply cannot do all we would like him to do. As much as anything, we need a core group who worry about issues in advance and have the prestige and access to make their views be heard. Rather than design a blueprint, let's review some issues that such a body might explore.
Proposal 8: Health Savings Account Age Limits Should be Extended, from the Cradle to the Grave. A few extra years might be a minor improvement in special cases. The real benefit would be to create a continuous account, which could grow over long periods of apparent inactivity.
Proposal 9: Instead of annual contribution limits, the limit for HSA should extend over several years, or even be a lifetime limit. When deposits must be skipped for health or occupational reasons, there should be an opportunity to catch up. Athletes and similar occupations tend to concentrate on earning power in a few years.
Since the HSA is increasingly accustomed to augmented retirement income, thought should be given to extending the idea to amounts of money which could encourage that use. Furthermore, there are special circumstances, like a partial Medicare buyout, in which a limit to deposits forces a choice between two desirable uses for the same money. If the individual has the money for more than one purpose, it seems wrong to force a choice. For example, it's considerably safer to over-deposit more than you believe you will need, planning to return the excess. As a practical matter, the usual danger is overoptimistic revenue projection. Someone who sells his business at age 63 might have enough cash, but still, encounter trouble with the $3300 per year limit because he once needed the income to run the business. It seems pointless to squeeze through such a narrow window, and much better if the window were at least enlarged to permit lump-sum deposits up to a $ 132,000-lifetime limit. With that sort of cushion, plus a stretch of reasonably good health at the right time of life, it would become considerably safer to take risks. At age 65, a lifetime of health costs is already in the past, but the curve of health expenses starts to bend upward at age 50, at a time when college expenses for children may be persisting, and the house isn't quite paid for. It seems a pity to cripple a good idea with pointless contribution limits that almost stretch far enough, but leave people fearful. If Congress develops a serious interest in lifetime insurance, the yearly contribution limit should be revisited. The optional side use for retirement should be examined in parallel, including its potential for being gamed.
Revisited by whom? Someone should be empowered to travel, and talk to people in the field. Maybe hold hearings, maybe just interview. A simplified goal is, therefore, to accumulate $80,000 in savings by the 65th birthday, intending to make a single-premium buy-out. That clarifies costs, but is it practical on a large scale? Remember that savings get a lot harder when earned income stops. With the current law, you would have to wake up and start maximum annual depositing of $3300 by your 50th birthday, to reach $80,000 by age 65, and you would need generous internal compounding to make it. But notice how easily $100-200 a year would also get you there, starting at age 25 (see below), even justifying somewhat less optimistic investment income returns until age 65.
Many more frugal people might skin by with looser rules; It even could rather easily be subsidized for poor people and hardship cases. If you are going to cover lifetime health costs instead of just Medicare, many more will need $80,000 to do so and have something left to share with the less fortunate. But to repeat once again, that still compares favorably with the $325,000 often cited as a lifetime cost. That's all we care to promise in public, but secretly we know it may not be enough. The plain fact is, if longevity or inflation get out of hand, someone must have the authority to raise the contribution limits and to do that, there should be some research by a trusted house actuary.
Proposal 10: Instead of the present annual limit of contributions to Health Savings Accounts of $3300 per year, Congress should permit a lifetime limit of $132,000, with annual deposit limits adjustable to bring accounts at their present age, up to what they would have been if $3300 annually had been deposited since age 25.
Proposal 11: Congress should reserve decisions to itself for changing the lifetime contribution level, and review final appeals from contract terms which seem to threaten imminent major adjustment to the general public lifestyle.
The Cost of Pre-funding Medicare. Rates of 10% compound income return would reduce the required contribution to $100 per year from age 25 to 65, but if the income were only 2% would require $700 contributed per year, and at 5% would require $300 per year. Remember, we are here only talking of funding Medicare, as a tangible national example,
It is this calculation, however rough, which has made me change my mind. It was my original supposition that multi-year premium investments would only apply up to age 65, and that would be followed by Medicare. In other words, HSA should only be implemented as a less expensive substitute for the Affordable Care Act. It seemed to me the average politician would be very reluctant to agitate retirees by proposing a plan to eliminate Medicare. They would feel threatened, the opposing party would then fan the flames of their fears, and the result would have a high likelihood of undermining the whole idea for any age group, for many years. Better, I thought, to take the safer route of avoiding Medicare, and confining the proposal to working people, where its economics are overwhelmingly favorable.
But when the calculations show how close this proposal under cautious revenue projections could come to failure, and when nothing else remotely close to it has been proposed by anyone, the opportunity runs the risk of passing us by. So, I have changed my mind. The moment of opportunity is too fleeting, and the consequences of missing it entirely are too close, to worry about the political disadvantage of doing the right thing. The transition to a pre-funded lifetime system will take a long time to get mature, and the political obstacle course preceding it is a daunting one. At least we should allow it as a demonstration option, where some fears will prove unwarranted, while others can be corrected.
So we make the guess of the average life expectancy where things will eventually flatten out, will then be about 91. (Be careful, most census figures are for life expectancy-at-birth.) But many people would have to be lucky in all details: a favorable investment climate for the right ten-year periods, plus a favorable health situation which avoids expensive illnesses just at the age when they begin to threaten. Some life-saving scientific advances would be a big help, too. Using a lower goal of $80,000 and an interest rate of 7% is considerably easier to conjure, but the barrier which might be reached first is the $3300 yearly contribution limit. Some unfortunate individuals might be forced to pay all medical expenses out of pocket in order to make the investment fund stretch, even before the average becomes affected. The individual who came up short might still remain considerably ahead of where he would be without an HSA, but we are using a precise match of revenue and expense, to simplify the examples.
Someone who sells his house or business at age 63 might have the cash, but still, have trouble because of the $3300 per year deposit limit. It seems pointless to squeeze through a narrow window, and much better if the window were enlarged to permit lump-sum deposits up to a $ 132,000-lifetime limit, adjusted for inflation and compound income returns. With that sort of cushion, plus a stretch of reasonably good health at the right time of life, it would become considerably safer to take the risks. At age 65, a lifetime of health costs is nearly in the past, but the curve of health expenses starts to curve up at age 50, at a time when college expenses for children may be persisting, and the house isn't quite paid for. It seems a pity to cripple a good idea with pointless contribution limits that almost stretch far enough, but leave people fearful. If Congress develops a serious interest in lifetime insurance, the yearly contribution limit should be revisited.
The simplified goal is, therefore, to accumulate $80,000 in savings by the 65th birthday, remembering that savings get a lot harder when earned income stops. With the current law, you would have to start maximum annual depositing of $3300 by your 50th birthday, to reach $80,000 by age 65, and you would still need generous internal compounding to make it. But notice how easily $100-200 a year would also get you there, starting at age 25 (see below) and less optimistic investment income returns until age 65. Many more frugal people might skin by with looser rules; poor people and hardship cases could more easily be subsidized. If you are going to cover lifetime health costs instead of just Medicare, many more will need $80,000 to do it and have something left to share with the less fortunate. But to repeat once again, that still compares very favorably with the full $325,000 which is often cited as a lifetime cost. We have already imposed an extra $80,000 internal savings requirement in order to include Medicare; here is the place it would be a hardship. That's about as far as concentrated thought will carry you. It leads to the conclusion that it might be better to modularize Medicare and let the public pick and choose what it wants to buy its way out of.
The Cost of Pre-funding Medicare. Rates of 10% compound income return would reduce the required contribution to $100 per year from age 25 to 65, but if the investment income were only 2% would require $700 contributed per year, and at 5% would require $300 per year. Remember, we are here only talking of funding Medicare, as a well-understood national example, Obviously, a higher return would provide affordability to many more people than lesser returns. When $100 competes for the investment income from 10%, it's much easier than $300 competing for 5% income. Let's take the issues separately, but don't take preliminary numbers too literally. They are primarily intended to alert the reader to the enormous power of compound interest, and the big difference made by relatively small changes in it. Let's go forward with some equally amazing investment discoveries which are more recent, and vindicated less by logic than empirical results.
A transition from term insurance to pre-payment of Medicare is greatly eased by forgiving the premiums and payroll deductions, which are roughly age-distributed, and can, therefore, be forgiven in a graduated manner for late-comers to the program. Most cost-redistribution of high-cost outlier cases should be handled through the catastrophic insurance, which is well suited for invisible and tax-free redistribution. Because of hospital cost-shifting, inpatients are temporarily overpriced but are quickly becoming underpriced as a result of hospitals gaming the DRG to shift costs to outpatients. This will in time affect the relative costs of Catastrophic and Health Savings Accounts and must be carefully monitored for mid-course adjustments. This changing horizon of cost shifting reinforces the need to create a special agency to keep track of it. And to report its findings to Congress, who can consider the broader political implications, once they know the facts.
Proposal 12: Congress should create and fund a permanent Health Savings Account Agency. It should have members representing subscribers and providers of these instruments, with the power to hold hearings and make recommendations about technical changes. It should meet jointly with the Senate Finance Committee and the Health Subcommittee of Ways and Means periodically. It should have extensive access to the appropriate Executive Branch department, to review current activity, detect changing trends, and recommend changes in regulations and laws related to the subject. On a temporary basis, it should oversee inter-cohort and outlier loans, leading to recommendations about the size and scope of inter-subscriber loan activity. At first, it might conduct the loan activity itself, with an eye toward eventually overseeing a commercial vendor.
Cost Sharing with Frugality.At present costs, statisticians estimate future healthcare costs of about $325,000 (in year 2000 dollars) for the average lifetime. We could discuss the weaknesses of that estimate, but even though it's breathtaking, it's the best guess available. Women experience about 10% higher lifetime health costs than men. Roughly speaking, how much the average individual somehow has to accumulate, eventually must equal what he spends by the time of death. The dying individual himself has little interest in what is left unpaid at his death, so Society must do it for him, in order to survive as a Society. At this point, we, unfortunately, must also work around one of the great advantages of having separate accounts.
On the one hand, individual accounts to create an incentive to spend wisely, but it is also true that pooled insurance accounts make cost-sharing easier, almost invisible, and tax-free. Cost sharing induces reckless spending of other people's money, however, while individual accounts induce frugality with your own money. Therefore, linking Health Savings Accounts with Catastrophic insurance provides a way to pool heavy outlier expenses, while the incentive for careful money management remains in the outpatient costs most commonly employed (together with a special bank debit card) to pay outpatient costs. Such expenses are much more suitable for bargain-hunting anyway because dreadfully sick people in a hospital are in no position to argue or resist.
But a cautionary reminder: linking individual accounts to frugality through outpatients, as well as linking heedless spending to insurance through inpatients -- induces hospital administration to game the system we have here imagined. There's no doubt a system can be gamed by shifting medical care to the outpatient area, but we must expect the DRG to be attacked, in order to reverse such incentives, which run in the hundreds of billions of dollars. A well-informed monitoring system simply must be created and funded, if we ever expect the decision to hospitalize patients to rest on whether the patient needs to lie down, instead of on what kind of payment system we happen to fancy. At the same time, the present DRG coding system must be considerably improved to withstand being subverted. These are not tasks which congressmen typically enjoy, but they must be done within the legislative branch if we expect it to function.
Standard Deviation within and between age cohorts.Furthermore, there is an important distinction between a mismatch of revenue to expenses caused by chance within one age group and a revenue mismatch between two age cohorts. To put it another way, somebody has to pay off these debts, and we must have a plan about who should pay them when revenue is not present in the account. Borrowing between subscribers within the same age cohort should pay modest interest rates to forestall gaming, but borrowing between different cohorts for things characteristic of their age level (pregnancy, for example) should pay no interest if at all feasible. Unfortunately, people sometimes abuse such opportunities, and interest must then be charged. Until the frequency of such things becomes better established, this function of loan banking policy should be part of the function of the oversight body, rather than the executive agency, which tends to want to retain the function. When its limits become clearer, it might be delegated to a bank, or even privatized, but the policy must be monitored by specialists who understand what is happening "on the ground". While it is unnecessary to predict the last dime to be spent on the last day of life, incentives should be understood by the managing organization, separating routine cash shortages from likely abusive ones. And looking at all such activity as potentially having been caused by payment design. Much of this sort of thing can be minimized by encouraging people to over-deposit in their accounts, possibly paying some medical bills with after-tax money in order to build the fund up. Such incentives must be contrived if they do not appear spontaneously. User groups can be very helpful in such situations. People over 65 (that is, those on Medicare) spend at least half of that $ 325,000-lifetime cash turnover, but just what should be counted as careless overspending, can be a matter of argument.
Proposal 13: Current law permits an individual to deposit $3300 per year in a Health Savings Account, starting at age 25, and ending when Medicare coverage begins. Probably that amount is more than many young people can afford, so it would help if the rules were relaxed to roll-over leftover entitlements to later years, spreading the entire $132,000 over the forty-year time period at the discretion of the subscriber.
Finally, an observation. The classical Health Savings Account will save a big chunk of money, but who gets it will depend heavily on the health of individual subscribers because it is term insurance, year to year. Two concepts loom over it: (1) The nation may want to distribute the good and bad luck more evenly, and (2) It would be much easier to cut down an over-funded project than to supplement an under-funded one. If we can think of some ways to improve the product, we should start with as generous a benefits package as we can easily devise. Therefore, the rest of this book is devoted to making the returns more generous, and the outcome more predictable, sooner.
A point which cannot be emphasized enough is that a Health Savings Account is just about the best way to invest, if you have given little thought to investing. The deposits are tax-deductible, and the withdrawals are tax-free if they are medical in nature. Even if they aren't medical, they can be anything at all after you reach 66. You probably ought to give a lot of thought and investigation to the particular agent you choose, because they aren't necessarily legal fiduciaries, no matter how friendly they may be. They have no obligation like a doctor or lawyer to put the client's interest ahead of their own, and they can later hire partners you don't care for, so make certain you can terminate the arrangement and switch to someone else without penalty.
Be careful to choose a representative carefully. But whether to choose an HSA, at any age and stage of advancement, always leads to the same answer: Yes, do it. That being the case, a certain number of HSA owners will find themselves with an account they don't know what to do with. There's almost always an exit strategy, although you may need professional advice to judge which one is best for you.
If you started your account near or after retirement, you may have the idea you will never have surplus funds. But if Congress can be persuaded to make it legal, one of your options might be to roll the surplus over to a grandchild or grandchild-like person. If this suits your situation, please notice that a newborn child has some special medical problems. In the first place, the first year of life is unusually expensive; in the aggregate, 3% of all medical expenses are spent on the first year of someone's life. To anticipate a little, 8% of health cost are spent before age 21, which is generally held to be the beginning of the earning period. Children are generally pretty robust, but when a child is sick, he is vulnerable to lasting disabilities of a very expensive sort, so you don't like to see a family cut corners on child care.
But newborns have no earning power, their future is in someone else's hands. The average woman has 2.1 children today, two women thus have 4.2. Four grandparents roughly have one apiece. The way the law of averages is working out, if every grandparent took care of the health costs of one grandchild, things would be close to solved. Things would have to be adjusted for the non-average case, but they would be close to being solved by adding one grandchild's cost to each average Medicare cost for the elderly.
In this case, however, the legal and political problems are greater than the financial ones, so it would suffice for a beginning, just to permit those who want to volunteer, to be permitted to leave unused leftovers in their HSA to children under the age of 21. If there is concern about dynasties and perpetuities, it might be left to the child's HSA, to be exhausted by age 21, or transferred to the HSA of a second child. The sum in question might be around $8000.
One of the best ways to wreck a good plan, is to fail to provide for success. Most innovators spend so much anxiety over possible failure, they never get around to planning for the problems created by the plan's roaring success. So, let's voice some concerns about where the Lifetime Health Savings Accounts might stand if everything worked perfectly.
In the first place, there could be a conflict between the small investor's best interests. On the one hand, he will undoubtedly do better for himself by purchasing index funds than individual stocks. He gets diversification and low fees, supported by mountains of evidence that only a rare investor will do better with stock-picking and market-timing, no matter who is advising him. But if myriads of people do the same, index funds could overwhelm the market. Already, they represent several trillions of dollars and show no signs of slowing the pace of advancement. The proportion of stockholders who actually vote their shares will steadily shrink, and ultimately we can expect the few shares that are voted, to be in the hands of managers and insiders of the company. Now it is probably true that the average small investor knows so little of what is going on, that both he and the companies are better off if he doesn't exercise an uninformed vote. A more likely danger is imperfect agency on the part of the managers of the funds. Wall Street periodically circulates rumors of fund managers offering to vote the fund proxies, in return for the selection of their fund for the affected company's pension fund assets. It doesn't matter whether this is true, what matters is it is believed. Sooner or later, Congress will get wind of such rumors and pass inhibiting legislation. The nature of such regulation and/or legislation is ultimately to impair the value of the stock. The salaries of CEOs may go down, and some Wall Street predators may be thwarted, but overall return on investment will be lessened by the suspicion.
The bond market is much larger than the stock market because leverage is the basis for a great deal of profitability. No one knows what the optimum ratio of bonds to stocks should be. In 2007, the ratio of bank leverage was fifty to one, and few people complained it was too much. In the depths of the 1930 depression, it was far lower, and few people complained it was too low. In retrospect, fifty times is insanely high, while if you bought any stock at all in 1939, you probably made a ton of money. The herd instinct always seems to drive this relationship to extremes, but in fact, the optimum ratio will also go up and down with the times. Any law setting limits will be meaningless for long periods of time, and then suddenly be a serious impediment to the economy. The problem lies in the reality that bond trading is, with few exceptions, a zero-sum game. For you to win, someone else likely has to lose. By contrast, the stock market represents company ownership, and it is possible for both sides of a trade to be highly satisfied with their outcomes. It certainly isn't guaranteed, but the environment is more favorable for a passive investor. The long-run hazard lies in the possibility that nearly all investors will go to school and learn these aphorisms, thereby undermining the bond market except for insurance companies, banks and other long-term investors, who can hold a thirty-year bond to maturity. A flight from bonds would inevitably make their prices drop, followed by a shortage of bonds, which would then make their prices soar. Carried to an extreme, and protracted for a decade, a disturbance of this sort would cause the buy-and-hold stock investor to lose the faith, and ultimately to lose his shirt.
You have to feel sorry for the traditional stockbroker and investment advisor. The advent of the computer and of low-cost diversified funds have badly shaken what has long been an honorable and respectable profession. However, stockbrokers have resisted adopting the legal role of fiduciary, pledged to put the customer's interest ahead of his own. Most of the major stockbrokers started as private offices to handle the affairs of one rich family, who essentially didn't care about the fees and commissions. As a favor to rich friends, they enlarged the business and utilize economies of scale. In consequence, almost all stockbrokers could hope to get rich from trade secrets. With the advent of computers and high-speed trading, the broker trade became an investing profession, graduates of business schools and even mathematics majors from Ivy League Universities. The secret of success in that environment was volume, not trust-fund babies as friends and former classmates. Pension funds in particular aggregated a large number of obedient clients for them; the salary scale was still opulent, but the clientele was no longer their equals in sophistication.
As the brokerage house with walnut panels and oriental rugs began to fade away, the social level of the broker was no longer so important, and high fees interfered with maintaining high volume. It is only a matter of time before the personal financial manager discovers a small volume of potential clients, including trust-fund babies with some investment training of their own. The surviving financial advisors are only cogs in a big machine. In the meantime, be careful of whose advice you take, especially if he steers you away from index funds. There is a significant risk the advice is really coming from the sales manager, unloading the firm's inventory. The most lurid example is what has happened to 401(k) pension plans, where the investment return is heavily consumed by fees, altogether too often. It would certainly pay to browse through a book by Ibottson, containing all of the statistics you need about the last century. Since 1926, large-cap stocks have averaged 10% total return, while somewhat riskier small-capitalization stocks have averaged 12.5%. Your interview with an advisor can't be considered finished until you are told what the 15-year experience has been at that particular fund. Unless you are determined to get the data, you probably won't get it. Because of this behavior, the famous investor Warren Buffett tends not to buy stocks and bonds at all. He buys the whole company. The results of his investment fund, Berkshire Hathaway, are a rather close match to the returns which Ibottson reports.
Ok, ok, got that. But suppose everyone gets it? In that case, one would suppose the prices of common stocks would fall, and the prices of bonds would rise to a new level. At that point, the advice would be to buy funds which hold huge amounts of bonds of all maturities and hold them to maturity. Remember, investors in Health Savings Accounts would effectively be investing for the next sixty to eighty years. Someone must be found to change the composition of the portfolio rather drastically and to do so gradually enough to avoid convulsing the market. Panics are essentially what happens when everyone tries to get out the door at the same time. Are we to risk the entire savings of the nation for healthcare, based on that sort of opinion? It seems pretty clear to me that we have to trust someone, but it is not clear to me how we can assure ourselves that the person or persons with authority, will be sufficiently unaffected by politics -- to be trusted.
Which brings up the Federal Reserve. It would be hard to find a group of more serious people, generously infused with a strong sense of duty and fidelity. But strong differences of internal opinion regularly surface, not necessarily following a political ideology, as much as creating it. After all, some of this stuff is really hard. In the full century since the 1913 creation of the Fed, the dollar has declined a thousand percent, from the value of one dollar to the value of one penny. John Kenneth Galbraith, one of the wittiest civilized men on earth, loudly and earnestly advocated a deliberate 2% inflation in the value of the dollar. Well, we have it, and the dollar has completely severed its connection to gold and silver or any other commodity. The currency has now just become a computer entry when thousands of years of experience speak to the hazard of doing so.
When the dust settles, there remain two reasons why we should take such risks. The first is the rather good possibility we can indeed extricate ourselves from a looming health finance disaster, by taking this risk. The second is to reflect on the growing possibility that medical research can eliminate enough disease, and reduce the cost of caring for what is left, to give us the room to ease into sustainable finances. If that's our grand strategy, only America, using American bravado, could pull it off.
We propose the development of a lifetime health insurance product, for the main purpose of gathering investment income on the insurance premiums. It reduces the cost of health care by adding that new revenue source, which at the moment is simply lost. The longer compound interest is allowed to work, the more income will be produced, to the point where it can be imagined that this income source would more than cover the cost of health care. For the most part, it would really only cover a portion of the cost, but a very large one. If things are cheaper, more people can afford them, so the problems of the uninsured are eased. This system would take many years to make the transition to wide-spread coverage, so many features of the Affordable Care Act might be temporarily useful. Many people who resist Obamacare are unable to see an end to it. As a transition, Obamacare would become a success if some other program is a success, first.
First, the law requires two things to be purchased at once: an investment account, and catastrophic health insurance. Deposits into the Account are tax-exempt. Withdrawals are restricted to health costs, not including the premiums of the catastrophic insurance, but the internal investment income on the deposits compounds tax-free. The framers of the enabling act apparently did not anticipate that many or most children would, under Obamacare, already have mandatory coverage on their parent's policies up to age 26, under their parents' policies, so the overlap is a little ambiguous. Apparently, however, there is no limitation to single health policy, so dual policies appear to be allowed. As long as the law requires money to be withdrawn from an Account only for health expenses, many people during the transition will find they already have health insurance, but not enough money in the account to cover the required minimum deductible. Unless they can make a deposit and see it grow, they will never be able to start an account. So, especially for children, the required deductible should match the amount in the account, not the other way around. It scarcely matters which it is, except the child rarely has control over the parent's policy, so the law should be amended to allow an HSA to be created without catastrophic coverage, until such time as some flexible minimum deductible is reached, even if it is necessary to prevent all withdrawals until the minimum is reached.
Perhaps this issue could be addressed for children with a single-payment deposit. It seems a great pity to prevent lifetime accounts which could be made for a nominal single payment, simply because the parent has a low-deductible policy and cannot or will not change it. Alternatively, it is an equal pity to require a child to have two other health insurance policies, when the reality is the healthiness of such children seldom requires even one policy. Since lifetime health coverage is within reach for a single payment of less than a thousand dollars, it is much easier to envision subsidies for the poor of that amount. Lifetime average health expenditures in the range of $300,000 are largely made up of inflation costs which reduce a dollar to the value of a penny, over an ensuing century. There are few ways for the poor to escape inflation, but this would be one of them.
That gets us to age 26 when employer-based insurance makes an appearance. Or makes a disappearance, replaced by Obamacare; we must wait to see what happens. Present law permits a deposit of a maximum of $3300 in the accounts, until retirement at age 65, when Medicare takes over. That could result in a deposit of $128,700 at age 65, which with 7% compound income within the account would amount to $610,000 total in the account, but an unknown amount subtracted for exceeding the insurance deductible. Since additional deposits are not permitted to people receiving Medicare benefits, $610, 000 will have to last for the duration of life expectancy, calculated to be age 90 by then. Assuming the same 7% return on investment, that amount is short of the $3 million single payment deposit which would be required (at age 65) to pay for average health costs to the end of that life at 2014 prices. And probably not nearly what year 3004 prices might become.
To achieve that, 10% compounded income would be necessary, both to reach the end of life, and to augment those deposits of $3300 yearly to $4.5 million, the point where they and their investment income would meet the need. Although Ibbotson's curve encourages the hope that 10% return might persist for a century, there is little doubt that long periods of 1% income would bankrupt the system, resulting in only $156,000 gross before illness expenses at age 65, and unguessable effects on medical costs after that. Large numbers of people would not even be able to afford annual $3300 deposits into their Accounts. But there are two ways out of this trap.
In the first place, no one claimed that 99% of future medical costs must be met by this approach. The claim is only that large amounts would be "found money", not found at present; don't be greedy, since not a penny of this money is being utilized at present. And secondly, it would be manifestly unfair for Medicare to continue to collect payroll taxes from one age group, and Medicare premiums from another, if the plan is for this individual to bear his own costs. Accordingly, these payments could partly be waived, and partly deposited directly into the Accounts rather than into the U.S. Treasury. The Treasury itself would be amply compensated by putting an end to the present 50% subsidy of Medicare costs by the taxpayer, assisted of course by foreign loans, mostly Chinese. There is a political risk, of course, that opposition politicians would encourage the elderly to believe that Medicare is about to be taken away from them. Almost everyone enjoys getting a dollar for fifty cents and is suspicious of claims that, otherwise, they will get a penny for a dollar. It would thus seem better timing to begin at the other end of the age spectrum, building up a constituency for compound interest, the Ibbotson curves, and Health Savings Accounts, and meanwhile waiting for competitive proposals to flop. It would take six months of intensive publicity to convince people who don't want to believe it, that Medicare is 50% taxpayer subsidized. It would take another six months to iron out all the unsuspected technical flaws in the proposal.
And it would take time to create a bipartisan think-tank, to collect the necessary data and make the necessary calculations. Perhaps some philanthropists will offer to do it privately, saving us from the criticisms of agencies like the Federal Reserve, which are accused of being less "independent" than they claim to be. The first step would be to put it somewhere other than Washington DC since there is no need to be seen as close to those who threaten your independence. The divergence between costs and revenues must be monitored and adjusted to; sudden changes in direction must be responded to.
Independence Blue Cross (of Philadelphia) has imaginatively designed a Health Savings Account product for retirement purposes, by allowing the employer or the employee to overfund an HSA with $750 annual contributions, looking ahead to the employee's retirement. The HSA part is presented as an add-on to conventional Blue Cross, although it is unclear whether that is required. Independence Blue Cross should be given credit for a good idea. Whether it supplements health insurance before retirement, is apparently left up to the employee, but of course, it does supplement any other after-retirement arrangements the employee may have because the HSA continues on after Blue Cross itself terminates at age 66.
Since employers may soon face an un-suspended requirement to provide health insurance meeting ACA requirements, the high deductible from the government plan might simultaneously supply the high-deductible requirement for the HSA. This seems an efficient way to address present uncertainties and could provide the basis for compromise discussions between the two political parties on the whole subject of fringe benefits. High-deductible is good; adding subsidies confuses the intent. Keep them separate.
Savings unused for healthcare are available for retirement living.
Overfunding is always a good idea for subscribers to HSA, whatever their other program features. Politicians avoid overfunding anything because of voter reaction, so private plans are generally more flexible than public ones, while voters tend to complain that instead of overfunding, taxes should be reduced. The program is so new, and its time periods so distant, that unintentional gaps in coverage are always possible. If worries prove unfounded, overfunding leads to more money for retirement, hardly a tragedy.
Over-investment in Health Savings Accounts -- The Retirement Alternative. Because it's a new program, with financing uncertainties, we advise everyone with an HSA to consider overfunding it as a precaution. Just about everyone could readily use surpluses for some of his retirement. Although the employer only donates $750 per year, the law allows a total of $3350 as a maximum, and so a $2600 personal supplement is required in the following three hypothetical but typical situations. At this level, the employer contribution is a small factor; what really matters are inflation and interest return. And starting at an early age.
Example One. Let's say an employee starts the program at age 21 and remains with the company until retiring at age 66, contributing $3350 per year to the HSA (in the Blue Cross plan, $750 comes from the employer, and the employee must supplement $2600 from personal funds). (It makes no difference whether the employee rises through promotions or remains at an entry level; the maximum is the same.) Result: the employee receives a taxable retirement income at age 66 from the HSA to IRA transfer of $81,616 per year until age 83, dropping to 66,642 with 3% inflation. If the life expectancy of 93 is anticipated, the yearly annuity drops to $65,621, dropping to 48,595 with inflation..
Example Two. Another employee enrolls at age 21 but retires to get married at age 26. At age 66, until death, there is a yearly $23,423 retirement income assuming a life expectancy of 83, and dropping to 19,125 with 3% inflation. Assuming 93, the annuity is $ 18,832 with and $ 13,946 without 3% inflation.
Example Three. An employee joins the firm at age 61 and remains until age 66. His retirement income is $1,886 per year, dropping to $ 1,540 with inflation, Assuming expectancy of 93, he gets $1,516 yearly, or $1,123 after 3% inflation.
In the examples, many things jump out. The first is the large disparity between what five years of work will get you, starting at age 21, compared with the almost pitiful amount a person age 61 will get for the same absolute, and maximum allowable, contribution. The difference between examples is the difference between whole social classes. That difference, of course, is made up out of the income compounded internally for 40 years. And the moral is clear, a small steady investment at an early age is worth far more than the same investment at the end of working life. It happens to cost the employer the same, either way, and he may not realize it. His viewpoint will depend on what value he places on maturity and experience in an older employee, as compared with vigor and strength in a younger one; the pension costs would be the same.
However, this is a major change in pension design, and people should familiarize themselves with it. The employer can make far more difference in an employee's life with the selection of savings plan, than with salary. Perhaps another way of looking at it is the employee gets to keep the interest compounding in an HSA, whereas in other plans the employer gets to keep it. Or, depending on how the contract is written, some middle-man gets to keep it. The old defined benefit plans placed much more emphasis on training and experience and much less on the age and duration of enrollment. It's a new ball game. For example, there is no reason why an employer couldn't have two plans, with an optional choice, one for young people, the other for latecomers.
The second point revolves around the interest rate being paid. The investment manager, whether in-house or by way of a vendor, is able to earn and should be able to earn, 12% on an index fund of the common stock of the whole American market. Inflation at a steady rate of 3% for a century, reduces that return to 9%, net of inflation. How much is the employee entitled to?
Much depends on whether inflation is pre-deducted in advance, or calculated at some later time. If an employee is paid less than 3% per year for his HSA, he actually loses money on the exchange. If he is paid 7.5% gross, he only receives 4% net of inflation, in spite of surrendering half of the net gain (4.5% of 9%) to the broker or manager.
In this example we have arbitrarily assigned him 6.5%, which is 3.5% net of inflation, yielding well over half of the margin to the broker. I have to wonder whether the services provided are really worth more than 1% (for example, one nearby trillion dollar firm only charges a tenth as much), so it seems as though a fair return to the investor/subscriber should be 5%, net of inflation, net of fees, or 8% gross. So, be careful to identify whether inflation is anticipated, or only calculated after it happens. Sometimes, both approaches are adopted, and someone is seriously affected by not noticing it.
That means the price debate ranges between 3% (no profit to the investor at all) and 8% (essentially the wholesale price). Throughout this book, I have generally adopted 6.5% as an average, mainly to be safely conservative and avoid arguments. The marketplace will eventually settle on the "right" price, but if it's less than 3.5% net of inflation, it's less than a quarter of the wholesale price. Eventually, I expect the price to be knocked up to 8%, net of inflation, or 11% gross. The ultimate effect of this price pressure on the cost of health care would be considerable, indeed. Sustainable retirement would come into sight, and as we have mentioned, the price of healthcare is linked to it.
Now, I don't want to be accused of starting a revolution, but my calculator tells me if the passive investment could achieve 6.5% income return, the first of the three examples cited above would receive a retirement income of $81,616 per year. And the old fellow who decided to work for a few years to build up his retirement would receive $1,866. The youngster who worked for five years and then quit could look forward to a pension of $23,423 per year. Something tells me this is too destabilizing, so I'm not going to get impaled on the barricades discussing it. Ultimately, it probably reflects a reduction of transactional costs by electronics, which has not yet worked its way through to retail consumers. So, one way or another, something is going to happen, and it's up to all of us to make sure it is benevolent.
Overfunding health insurance by one means or another is a very good idea if you can afford it -- and you keep your wits about you.
We have begun the exploration of Health Savings Accounts, out to the edges of the potentials for the idea. Somewhat to our surprise, the idea has the potential for generating surpluses if carried out long enough, at a high enough interest rate. The immediate reaction is how to control this feature so that even if it all works out as anticipated, it does not wreck our rather fragile system of controlling the currency. The suggested technical solution lies in forcing the account to come nearer to a zero balance more frequently, a result rather easily accomplished by constraining the permissible balance transferred between existing programs, possibly even forcing it to zero. After a certain amount of experimentation, it should be possible to retain the compound interest feature for desired intervals, but imposing more zero balance constraints if it starts to get out of control. But there are other approaches.
There is always the rather simple-minded approach of forbidding what you fear, imposing fines or the threat of imprisonment for violations. Any physician would recognize that approach as merely treating symptoms, rather than getting to the root of the matter. It would seem, if the desired outcome of a surplus is achieved, it would be better to suggest a different use than health care, rather than permit potential hustlers from diverting the surplus to their own purposes. The obvious need is to fund retirements with it. There is going to be a great need for assisting retirements if improvements in health care continue to lengthen life expectancy. Still, further down the road, there is even a limit to this need, but it seems better to let signs of it appear in future generations before we actually take steps toward constraining it in some foolish way
In the meantime, the need to guard against the consequences of too little disease, death, and disability is just starting to appear, and it is huge. In the language of Congress, it makes its appearance as a deficit in the Social Security program which needs to be repaired in some way. When that need appears more imminent, it might be well to demand improvements in Social Security, or even its total replacement with a new program, rather than adopt the expedient of dipping into some other program with a? temporary? surplus. The South American approach of privatized Social Security investments was apparently bungled, but it might be re-examined for repair and revival. Much will depend on relative size; if living too long ever becomes a bigger problem than dying too soon, it would be a pity to allow the smaller program to dominate the larger one, because of tradition. It is probably not too soon to be thinking about these potential problems, but it may well be too soon to act on our plans.
Redesigning Old Age The authors of the Bible believed human life was designed to end at age 70. The revised scientific guess is 100.
Retire Later In the social entitlement environment, like the union environment, "givebacks" are never acceptable. But accepting a later retirement age than you planned on is one certainty, utterly beyond debate.
Rentier Class Eventually, everyone can hope to be a member of the rentier class. Ideally, they will have first spent equal time as workers.
Retirement Communities Retirement communities are fairly new ideas, still experimenting with the ideal model, so it is hard to generalize about them. But they look to be a possibility for everybody's future.
Health Savings Accounts In late 2003, Congress passed and the President signed, legislation enabling tax exemptions for contributions to Medical Savings Accounts. This monumental reform was included in a law which created a number of Medicare prescription drugs benefits which received more attention in the press. Such accounts were renamed Health Savings Accounts, which was the original terminology in 1980 when John McClaughry of Vermont and George Ross Fisher of Pennsylvania, shortly joined by Michael Smith of Louisiana, first introduced the concept.
Increased Potential for Retirement Villages Third-party insurance is blocking certain patient preferences, as demonstrated by what rich people prefer to do when they are sick.
Starving the Beast of Early Retirement New Jersey may be about to demonstrate that taxpayers should be on the lookout for too many government employees, not too much government spending.
Retiring to the Workforce Most Americans alive in 2020 will live to be ninety before they die. Forget about lock boxes and other schemes to pay for a thirty-year vacation. These people will have to keep working at least until age 70.
Veterans Hospital In spite of much effort and expense, Veterans hospitals are not typical of American healthcare.
Designated Lifetime Funds Nowadays, the government incentivizes most investment funds to be taxable, but curiously certain funds are forced to be tax-sheltered, while personal latitude exists for others. Since most people are eventually forced into having three types of funds anyway, some thought might be given to which purposes are most suitable.
Friends Lifecare at Home Philadelphia Quakers run over twenty retirement communities for the elderly in their region. One of them is a virtual village, one without walls.
What Price Success? If everybody buys diversified stock funds, and never votes at the annual meeting, who owns and controls the company?
Lifetime Health Coverage, Summarized in Advance Lifetime coverage cannot be envisioned without some changes in existing law. Most people need to see the goal before they will inconvenience themselves to get it.









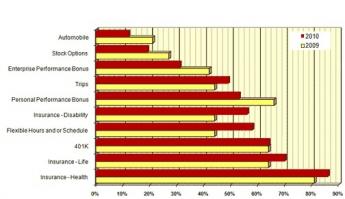









 The authors of the Bible believed human life was designed to end at age 70. The revised scientific guess is 100.
The authors of the Bible believed human life was designed to end at age 70. The revised scientific guess is 100.
 Eventually, everyone can hope to be a member of the rentier class. Ideally, they will have first spent equal time as workers.
Eventually, everyone can hope to be a member of the rentier class. Ideally, they will have first spent equal time as workers.
 Retirement communities are fairly new ideas, still experimenting with the ideal model, so it is hard to generalize about them. But they look to be a possibility for everybody's future.
Retirement communities are fairly new ideas, still experimenting with the ideal model, so it is hard to generalize about them. But they look to be a possibility for everybody's future.
 In late 2003, Congress passed and the President signed, legislation enabling tax exemptions for contributions to Medical Savings Accounts. This monumental reform was included in a law which created a number of Medicare prescription drugs benefits which received more attention in the press. Such accounts were renamed Health Savings Accounts, which was the original terminology in 1980 when John McClaughry of Vermont and George Ross Fisher of Pennsylvania, shortly joined by Michael Smith of Louisiana, first introduced the concept.
In late 2003, Congress passed and the President signed, legislation enabling tax exemptions for contributions to Medical Savings Accounts. This monumental reform was included in a law which created a number of Medicare prescription drugs benefits which received more attention in the press. Such accounts were renamed Health Savings Accounts, which was the original terminology in 1980 when John McClaughry of Vermont and George Ross Fisher of Pennsylvania, shortly joined by Michael Smith of Louisiana, first introduced the concept.
 New Jersey may be about to demonstrate that taxpayers should be on the lookout for too many government employees, not too much government spending.
New Jersey may be about to demonstrate that taxpayers should be on the lookout for too many government employees, not too much government spending.
 Most Americans alive in 2020 will live to be ninety before they die. Forget about lock boxes and other schemes to pay for a thirty-year vacation. These people will have to keep working at least until age 70.
Most Americans alive in 2020 will live to be ninety before they die. Forget about lock boxes and other schemes to pay for a thirty-year vacation. These people will have to keep working at least until age 70.