3 Volumes
Second Edition, Greater Savings.
The book, Health Savings Account: Planning for Prosperity is here revised, making N-HSA a completed intermediate step. Whether to go faster to Retired Life is left undecided until it becomes clearer what reception earlier steps receive. There is a difficult transition ahead of any of these proposals. On the other hand, transition must be accomplished, so Congress may prefer more speculation about destination.
Surmounting Health Costs to Retire: Health (and Retirement) Savings Accounts
Consolidated Health Reform Volume
To unjumble topics
Healthcare Reform:Saving For a Rainy Day
Lifetime Health Savings Accounts
Front Stuff, Health Savings Accounts: Planning for Prosperity;SECTION ONE: HSA and its Competitor, in brief
...Also by the same author:
The Hospital That Ate Chicago, Saunders Press, 1980
Health Savings Accounts: A Handbook, Ross & Perry, Inc. 2015 (Forthcoming)
---------------------------------
Ross & Perry Book Publishers
3 South Haddon Avenue
Haddonfield, New Jersey 08033
856-427-6135
----------------------------------
Copyright: 1-2540412791
ISBN #: 978-1-931839-44-0
-----------------------------------
Acknowledgements
For advice and support about the thrust of this book, I owe spiritual debts to John McClaughry of Vermont, the late F. Michael Smith, Jr. of Louisiana, and the late Bill Niskanen of Minnesota and Washington, DC. It's heartening to remember strong support coming from wide corners of America, and from strata of society ranging from a country doctor to the former Chairman of the President's Council of Economic Advisors. All three of these men worked their way up to being either a candidate for Governor of his state, the President of his State Medical Society, or the Chairman of a famous Washington think-tank. All three brushed aside the problems they created for themselves by constantly thinking outside of the box. My fellow Philadelphian John Bogle, whom I have only fleetingly met twice, deserves a lot of credit for demonstrating in his books how to invent a complicated concept, and then simplify it for outsiders. I've adopted his investing strategy.
And for personal support and tolerance from my family editorial board, consisting of my two sons and two daughters. My son George took time out from climbing the tallest mountains in the world, to develop a computer algorithm that instantly created the answers to a multitude of math problems hidden in certain assertions I blithely make, but now have confidence in. Likewise, my CPA daughter, Miriam told me some things which may be commonplace among corporate Chief Financial Officers, but astonish the rest of us. And her siblings Stuart and Margaret, who understood my tendency to wise-crack, but having long practice with its consequences, talked me out of most of it. Especially Margaret, who persuaded me it was more important for the title to be accurate than to be witty.
CHAPTER ONE: Re-Examining the Revenue Premises of Medicare
Chapter One:
We propose a comprehensive reform of American healthcare finances, resulting in a drastic drop in costs. This is payment reform, not medical reform, although the practice of Medicine cannot escape upheavals in its finances. It must all withstand critical review, but some of the future is simply not knowable. Defense of future predictions relies on extrapolations of history, but brief explanation nevertheless forces some things out of chronological order. We must, however, begin somewhere, repeating ourselves a little when the loop is finally closed.
So, we begin with Medicare, which has worked well for fifty years. Its data are easily confirmed on the Internet. Costs are known, minor faults have had time to be been corrected. Medicare is not the central focus of this book, but it's familiar. Seeing where Medicare fits in, gets the reader a long way toward understanding the system and where it needs to be modified.
Begin understanding Medicare with how it gets paid for, in three parts. (1) About a quarter is pre-paid, originating as a payroll deduction from the paycheck of every working person and mostly matched by an equal amount from his employer. (2) A second 25% of Medicare expenditure is supplied by the retirees themselves, as various sorts of insurance premiums. (3) And the remaining half is contributed by the federal government, but it originates in everybody's graduated income tax. In recent years, national finances have been strained, so a considerable part of the subsidized half is "temporarily" borrowed from foreign countries. There is general approval of the Medicare program, but it has grown expensive, a crisis usually blamed on the approaching retirement of the baby boomer generation. In a sense, maybe Medicare is a little too popular. Everybody likes a dollar that seems to cost fifty cents.
Focus attention on the pre-paid quarter of the costs, the payroll deduction. It's to be found in a mass of other numbers on any paycheck stub, often mixed with pre-payment of Social Security, and consists of 1.45% of salary for most people, 3.8% for those who earn more than $200,000 a year. The average worker earns $42,000 per year, and thus contributes $630; half of the workers contribute less, half of them, more. Persons earning less than $200,000 are matched by equal contributions from their employer. This has been going on for so long, most people could not guess how much it costs, would overestimate the proportion of their contribution, and underestimate its full cost.
In our proposal, we ask that $360 (of this average of $609), a dollar a day per working person, be set aside in an untouchable "escrow" fund every year, $180 from the beneficiary, $180 from the employer. Essentially, that's a seventh (14%) of the matched average $1218 pre-payment already being made on behalf of the average worker, although it might constitute all of his personal pre-payment if that worker only earned $5,000 a year. (It's a flat tax, but it does not go to zero at zero income.) In forty years of working life, the escrow would total $14,400. (It currently becomes the government's money, so the transaction is a tax reduction as well as an increase in personal income. For the moment, let's skip over the people below the poverty line, who obviously have to be subsidized, and ask, "What do you propose to do with a seventh of a quarter (3.6%) of the average total cost of Medicare coverage?" We're asking for $14,400 spread over forty years, which is 7% of what a person costs for a lifetime of Medicare ($200,000), or 4.5% of what is generally guessed to be one person's health cost for an entire lifetime ($325,000). What are we proposing to do with the money?
Answer: We propose to invest the $14,800 at 8%, and offer one choice about some of it on the individual's 65th birthday, as well as a second choice about it at any time thereafter, including his will. Because we plan to earn 8% interest on it, the $14,800 has turned into $93,260, and by the way, $7400 of the $14,800 was probably contributed by the employer, who got at least $3700 in a tax deduction for it. Furthermore, most economists agree employer contributions effectively reduce the paycheck by an equivalent amount, describing all fringe benefits as just part of employee costs. We will unravel this later, but the point right now is illustrating the largely unappreciated power of compound interest. This little exercise was conjured up to illustrate the power of compound interest, which it does quite nicely; but we aren't quite through. A dollar a day has resulted in 93,260 by age 65, but by age 83 (the present life expectancy) the 93,260 has turned into $360,000, just by sitting in Medicare unused, and $360,000 is the generally accepted figure for the total lifetime healthcare cost of an individual. One conjecture is 8% interest is too high, but we devote a whole later chapter to defending that number, which is merely the highest that can readily be defended.
Remember, however, this gain. equal to Medicare's total cost was achieved by investing only $360 of the $609 actually paid in salary withholding for Medicare. There is another $249 paid to the Medicare "trust fund". At 8%, this has reached $64,505 by the 65th birthday and grows by $6054 a year until age 70. Medicare averages $11,000 a year costs until age 83, the expected age at death. If the second fund makes up the $5946 difference. The two funds are in the position of earning 8% and shrinking at a total of $11,000 per year in combination. By the age of xx, the escrowed fund is growing at more than $11,000 a year, and the surplus fund is shrinking to make up the difference between $11,000 a year and the deficits of the escrow fund. Once the escrow fund is earning more than $11,000, there is a growing surplus which at present would transfer to an IRA.
Well, obviously no one is actually going to do what's suggested in the example, at least not more than once, but it does bring out some important points. The first is that apparently Medicare could be privatized for about one-quarter of what it is now costing, just by depositing and investing what is already collected in payroll deductions. Is it really possible we could also stop collecting Medicare premiums from the beneficiaries entirely, and stop accepting its 50% federal tax subsidy entirely, which we must now borrow from foreigners? Well, sort of. It would all depend on whether you could get 8% from Wall Street, as well as an income tax deduction from the IRS. Since the government doesn't pay itself taxes, the comparison boils down to whether you can get that 8%. A later chapter is devoted to the question.
Data has not been collected to test this idea directly, but some suggestions are intriguing. Medicare reports it spends about $11,000 per year per Medicare subscriber, whose average life expectancy is to age 83. That would imply Medicare is now costing about $200,000 per subscriber per lifetime. Future longevity is unknowable in advance, but it seems plausible it will level off at 93, sometime this century. One way of looking at this is to multiply $11,000 per year, times 27 years instead of 17, and get a future total lifetime Medicare average cost of $352,000. That's quite a wallop, but revenue from compound interest of 8% would be paid longer as well, taking it from $198,000 to $726,000. Old people getting cheaper is quite a surprise. Among the various things suggested is we have no idea how much 2035 technology would cost if it's good enough to extend longevity by ten years. Take a cure for cancer, for example. Would it be $100,000 per treatment, or would it be like aspirin, just lying around waiting to be discovered lowering heart attacks by 50%, at a nickel a pill? Or take another direction: perhaps living ten years longer would result in ten more years on the golf course or bridge table, followed then by the same terminal illness. An unchanged lifetime medical cost, in other words, just spread out over a longer time. Like a tulip on a longer stem. Since we obviously don't have the faintest idea about these projections, we will just have to strike an average, and hope for the best. But to return to a deeper question latent in the discussion: Do we have to worry that living on investment income will reach a point where it can't maintain a decent living in the face of improving technology? The encouraging answer seems to be: There's nothing on the horizon to suggest it.
Choices at age 65 have therefore become more complicated. If you had already reached your 66th birthday, and your choices included taking the $180,000 in cash, of course, you can just take the money and run. You might well be required to pay income tax on the lump sum, reducing its net amount by 15-30%, depending on your tax bracket. Perhaps a better choice has already been created, to roll it over into an IRA. In that case, the tax is deferred until you take minimum distributions for retirement purposes, which start paying a gross taxable amount (calculated by dividing it by your life expectancy, which at 66 is currently 17 years) of $10,500 per year. Considering this the return on an original $7400 cash investment, that's pretty substantial. And even recognizing your employer contributed half of it, it's still pretty good.
But consider another direction, entirely. Suppose by then the laws have been liberalized to allow "grandparents" to transfer a certain limited amount (see below) from their own Health Savings Account into a child's newly-created unique Health Savings Account if the recipient child is any age less than 35. At "grandpa's" death, again if the laws then permit it, the amount (specified below) may be transferred to other accounts. In the past, a child's account would have had more than three doubling opportunities in a 26-year span, but an infant baby has no money to double, and occasionally no way to create an account.
Whereas under our proposed new hypothetical rules, the baby's HSA might contain $8,000 at age 26, if grandpa transfers $1000 at birth and nothing else is spent out of the account until the child is 26, as a hypothetical illustration. The proposal is made that special Catastrophic insurance is also needed for this situation. Nevertheless, the potential should be exploited to create a bridge which connects an age group which is often overfunded with a generation that is usually underfunded, and always incapable of managing its own financial affairs. The extra $8000 at that particular moment in a 90-year cycle would have an immense effect on the cost of the entire scheme at all ages. So immense, in fact, that it undoubtedly would require safeguards against creating a nation of perpetuities in a few generations. My own suggestion is that a surplus from inherited sources should reach its conclusion at age 35, after which any surplus from "grandpa" sources should be transferred to the U.S. Treasury, subject to appeal to the local Orphan's Court. With such a rule in place, the system would readjust its arithmetic in the great majority of cases to accommodate special circumstances. The compound investment income alone will start this cycle all over again, if it throws off $325 a year for, say, the last ten years, including consuming its principal to do so. To repeat, an estimated $6000 of the eventual $8000 is consumed by the process of paying for the baby's birth and pediatric expense, with perhaps $2000 used to fund the child's own HSA up to $3250 at age 36, getting consumed in the process. Since this hypothetical began with only $1000, the starting amount could easily be tripled without disturbing the conclusion. With actual experience, these estimates can be fine-tuned. Tax-exempt funds like this should probably not be permitted to become perpetual, but allowing them to extend to a grandchild's 35th birthday would provide very desirable bridge funding for a period of life from birth to 36, which is both medically and financially quite vulnerable, and hence requires real-life insurance data (i.e. not hospital charges). He's going to have to go out and earn a living to sustain his own health insurance (see below), but his retirement Medicare costs are already a third paid up.
Just imagine: such a scheme might encourage more women to have children at an earlier age, which would be biologically very desirable, poorer people would be able to go to college without health financing concerns, and probably with reduction of the burden of disease from untreated medical conditions. At the same time, money would remain available for grandpa's health because he got to it first. Invisibly in the background, it assures generosity in the disability costs of the increasing volume of elderly indigents, which have been widely viewed with apprehension. And although all such benefits would entail some costs, at least they could not break the national fisc, within this financing design.
Other choices for the use of this "found" money are suggested in later chapters, and still, others are readily imagined, including perhaps some undesirable ones. At this point in the narrative, we will break off in order to heighten attention to the central feature of this health "reform", perhaps better described as reformulation. The central feature of this reformulation, is to exploit the sociological changes in healthcare created by advances in science: a much longer life expectancy, with an initial period of low health expenses, followed by a shift of burdensome illness toward its far end. Such change in lifestyle is ideal for gathering compound income early in life, augmenting it while it remains idle, and spending it toward the end. Since the reformulation pushes money toward an uncertain end, it inevitably creates some surpluses, which can best be recycled to assist the difficult costs of some relative's young life that, in the larger view, are quite modest.
So far, we have only looked at reformulation as a way to generate revenue. Another proposal to choose as an alternative is to drop Medicare, and simply pay medical bills out of the health savings account plus fail-safe catastrophic coverage. While at the moment few would have the courage to make such a switch, a credible threat to do so would at least perform the public service of discouraging mission creep, cannibalism by other agencies, and/or administrative bloat. It will always be impossible to determine how much of the present cost overrun was avoidable, but it's a fact, and a source of restlessness. Its best preventative is some viable competition.
Viable competition would include both luxury care for those willing to pay extra, and bare-bones care for those who cannot afford the standard variety. Both these desirable competitors would require some mechanism for extracting a fair financial equivalent from the standard product's expense account, and transferring it to the competitive systems. Needless to say, the existing system would resist, but a proposal might additionally be devised to resolve state/federal Constitutional problems in parallel with the money.
The Constitution's Tenth Amendment is decisively opposed to any centralized national healthcare system so this issue will continue to arise. To drive a not-so-subtle point home, it is only fair to conclude that many perhaps most citizens would prefer to impair employer-based health insurance -- if the only alternative offered, is to impair the Constitution. To state the matter in a conciliatory manner, there exists a widespread consensus not even to speak critically about the Constitution, unless a sincere bipartisan effort has first been conducted, trying to work around a problem. We tried the nullification alternative in 1860, and the results proved discouraging.
So, I propose we have at least two state-based healthcare systems, and eventually, a third national system exclusively limited to interstate issues, conflicts between jurisdictions, etc. That's what the Constitution wanted, and until we give it a chance, the state/federal uproar will be recurrent. It appeals to me to envision a hospital-based system and a retirement-village-based system, taking care to restrain medical schools, the federal government, or major employers from dominating either one. That gives state governments a chance to dominate locally, but the condition of state governments makes it unlikely that more than a handful would be up to the task. Governors, possibly, but legislatures, not so likely. A unique obstacle is to discover many sparsely settled states do not have the actuarial numbers necessary to support more than one health insurance company.
And so, since big changes are expensive, we need to find some extra money. As the reader will see, I believe Medicare could be paid for by reformulation at a fraction of its present cost, with a compound income of about 8%. The precise fraction and its compound income can be juggled around, but it looks achievable. If finances are tight, and 8% is unachievable, perhaps the Federal government could supply block grants which would support 8%, just as an example. However, any such expedient is a stunt that can probably only fail once, so we better study it hard. But if it can be done with Medicare, the pattern can be repeated with other age groups.
Finally, there really is a scientific end in sight, to a problem which science largely created. Just find an inexpensive cure for five or six diseases, and the main problem which will loom is spending too much money on non-serious complaints, cosmetic enhancements, and flummery. It may surely come to that in another fifty years.
Because of the extent and complexity of the problems, this first chapter only states the premises and gives a few examples; later chapters will explore more details needed to understand certain poorly understood features. But if there is doubt about the goal, let's make an explicit statement of it. We have been convulsed by health care reform since at least the time of President Theodore Roosevelt, but every ten years it keeps coming back. Let's stop thinking small and start thinking big. Let's fix it right and get on with it.
Children, 0-26
Everyone agrees there is a tangle about the rights and responsibilities which begin when childhood begins. We wish to avoid this issue as much as we can, but partitioning the costs of the average child requires stating some point or other, as its beginning.Keeping the practicalities of paying for it in mind, we hope no one will object if we say childhood begins, the day you are born.
We next consider the healthcare costs of children, from birth until age 25, linked with the costs of the elderly, for a reason. One of the points made in this book as an arguable alternative to the present employer-based system is to keep it within your family, rather than tax other people as a class. However, although the system now claims to begin with the first full-time employment, a newborn provokes about $18,000 of medical expense including obstetrics before that, right from the beginning, before the child can even feed him or her self. Age 26 might be a reasonable place to begin self-support, not because of tax deduction, but since that's typically the age group with the lowest health costs. Even that starting age has its problems because the parents are not much more accustomed to managing finances than the child is. The central question remains the same. Who is to supply the $18,000?
The Progressive movement started the idea of "family plans" about a century ago, but Henry J. Kaiser is credited with noticing an employer's gift of the insurance would supply two tax deductions, the employer's and the employee's, during World War II. That "reduced" the cost of health insurance by at least 50% (for the employer and employee), but it made a married employee seem more expensive than unmarried ones, made healthcare seem a free cost to the recipients and therefore boosted its cost, introduced a religious note by discouraging multiple pregnancies, and was unfair to unemployed or self-employed persons who were excluded from getting the gift. It is impossible to determine how much this new twist distorted employment and medical prices, but by suspicion the unfairness was major. It surely prompted a response, and this is one. If a big business can get tax deductions for giving away healthcare, why can't everyone else?
So it is proposed -- hold your breath -- HSAs give the equivalent of $18,000 at the death of an older relative, to a newborn's HSA at birth. The average childbearing mother has 2.1 children, which works out to one grandchild per grandparent, and helps smooth out the cost of multiple children. Because births and deaths cannot be forced to coincide, some sort of fund has to be created to make all this come out fairly, but the result should equal a zero balance between two generations. And because everyone who is alive has somehow already paid his birth cost, there is less urgency to begin this feature at the onset of the program--it becomes a feature of the transition. And, going back to the pros and cons of including Medicare premiums in the compounding, the more surplus is generated, the shorter the transition period should become. Ultimately, of course, the cost of health insurance for the mother is reduced; but the main beneficiary of the transfer is whoever is now paying for the mother's health insurance. That would sometimes be the father, sometimes the employer, and sometimes the Affordable Care insurance.
A few children are cursed with horrendous medical bills, which quite often predict lifetime disabilities. For the most part, however, childhood medical costs are pretty small. It would seem to produce an < b>ideal configuration for insurance, leading to mostly small premiums, affording a lot of protection against a fearful risk which is nevertheless relatively uncommon. However, a newborn is unable to walk, talk or feed him or her self, beyond even mentioning his or her lack of savings. Parents are now expected to pay such bills, and when they are very large it is common for grandparents to help out. So it sort of fits the common situation to group the two dependent periods of life (childhood and old age) together, as a continuous loop skirting the income-producing period of life entirely. The underlying purpose is to shift overfunded money to an underfunded time, compensating the childhood cohort for the fact that compound interest appreciates very little during childhood, but very greatly toward the end of life. This configuration fairly shouts "risk pool" but requires legislative action because it is more a metaphor than legal reality. It serves to explain to people why we have struggled to close the loop for twenty or more years because what is true for children is definitely not true for Medicare, where the main costs congregate. To meet the disparity, we chose to employ patchwork solutions for a single generation, counting on the enhanced generosity of the public for disabled children to meet the major expense. This appearance contrasts sharply with the deceptively low average cost of ordinary childhood healthcare. The only danger is for this temporary expedient to become a career.
Please note the fiscal dilemma. Even if subsidies or gifts provided a $100 nest egg to start health savings account at birth, 2.5 doublings at 7% would only create a fund of $525 by age 25. That's not nearly enough to fund healthcare for individuals at risk of auto accidents and HIV while trying to pay for college, home mortgages or the like. By contrast, $100 a year for forty years might well pay for all of Medicare while retaining leverage of eight dollars out, for one dollar in. Adding $1400 a year for 20 more years would be much better, at 80 to one. For lucky people, $8127 might work, but its safety margin is too narrow for launching a lifetime medical system. The actual plan proposed is a complicated variant of this approach. As the reader will see, there will be ample funds available for a lump sum donation, once the system has closed the loop, because just 8.5 extra doublings from the beginning of lifetimes to the end of other lifetimes, without supplementation, should silence any remaining doubts, at 256 to one leverage.
Once it gets underway, the two-generation process is very simple, requiring only a few amendments to existing legislation. Extend the age limits of catastrophic high-deductible insurance down to the date of birth, and allow the premiums to compound up to the date of death or 104, the length of a perpetuity. After that, allow surplus Health Savings Accounts of the parents or grandparents to flow over to the HSAs of the child, and allow surplus funds of grandparents and designated others to be transferred (from the date of death of one, to the date of birth of the other) via the HSAs of both. Gifts of this sort might even become a popular item in obituaries, in lieu of flowers.
Springing such a radically different proposal on an unprepared public is potentially to provoke ribald rejection, so it's gradually introduced here as a challenge to provoke alternative proposals. At the moment, I don't see what they would be. We are combining the advantages of two systems, for the young and for the old, which separately they cannot achieve, except through the socially threatened but biologically inescapable, concept of "family".
First Two, and Last Two, Years of Life
Before we get too deep into slicing average lives into average medical partitions, the reader should remember there is another way of viewing health care. Declaring we simply can't pay for everything because there are limited resources, we imply we agree on life's priorities when we really don't.
If this were a contest on TV, no two people might rank priorities the same way. But physicians would come closer. Reflecting common professional experience, most of them would give a special place to the first two years of life, and the last two. Health care costs concentrate there, and special reverence is paid to the patients. The rest of life has long quiet periods, but just about everyone is seeing or trying to see a doctor, during their first two and last two years. If we really must ration care, these are the years to be spared. These are the four years of maximum helplessness. We must keep it in mind. Special consideration is in order.
Fun With Numbers
The principles of compound interest are thought to have been a product of Aristotle's mind. The principles of passive investing are more recent, mainly attributed to John Bogle of Vanguard, although Burton Malkiel of Princeton has a strong claim. In the present section, we propose to merge the two methodologies, compound interest with passive investing, trying to give the reader some idea why the combination could supply Health Savings Accounts with seriously augmented revenue. Because there is so much political flux, it cannot be an actual plan until the politically-controlled numbers have some finality to them.
The proposal to accumulate funds, however, shifts responsibility to the customer to spend wisely, even resorting to employing some of the individual's taxable money to pay small medical costs, thus preserving the tax shelter. (Or to use escrow accounts, or over-deposit in some other way, such as reducing final goals.) HSA doesn't directly reduce health costs, it eliminates some unnecessary ones but provides lots of extra money to pay for essential ones. At the outset we want to state, schemes of this sort have a history of working effectively up to a certain level, and then begin to interfere with themselves as eager money rushes in. There's no sign of that so far, but it might appear. Therefore, we advise modest hedged experiments rather than attempts to pay for all of healthcare, reducing health costs perhaps by only a quarter or a half, since those smaller levels would still amount to large returns. Balancing the risks with investments outside the HSA -- is just another prudent way of hedging the bet.
 Money earning seven percent will double in ten years. 
|
In fact, we have a tragic example in the nation's pension funds. A few decades ago, pension managers were tempted to invest in stocks rather than bonds, and then the stock market crashed, stranding pensioners with low rates of return, rather than the high ones they had hoped for. I want readers to understand I am well aware of the cyclicity of markets, and make these suggestions, regardless. As long as we include a thirty-year "Black swan" contingency by limiting coverage to a quarter or a third, it should be reasonably safe, but savings would still be enormous. There are other, more traditional ways of protecting endowments from stock crashes. With people of every age to consider, the long transition period alone would almost automatically buffer out black swans.
Having issued a warning to be a conservative investor, let's now introduce some notes of reassurance. Younger people are always likely to be healthier. Those who save their money while young therefore need not use all of it for healthcare -- for several decades. Compound interest works to magnify savings, the longer its horizon the better. We'll describe passive investing later, but it too should increase the average rate of return. These investments after some successes increase the incentives to save. If no one buys Health Savings Accounts, the incentives were apparently not large enough. If everyone rushes to buy, perhaps the incentives were unwisely too attractive. Right now, the financial industry is observing a rush to passive investing; nearly fifty percent of mutual fund investors are switching to "index funds" in spite of capital gains taxes on selling other holdings. Since the marvel of compound interest has been accepted for thousands of years, a mixture of compound interest and passive investing isn't an especially radical idea.
What's radical is the idea that all those highly-paid advisors can't do better than random coin-flippers. What's radical is to discover that the main ingredient of poor performance is high middle-man fees. Low fees won't assure high returns, but high fees will assuredly lead to low returns. If that new idea gets replaced in turn, it will be replaced by something better, and everyone should switch to it. But if compound interest is here to stay, this proposal is safer than it sounds. The investment income rate or continued employment of your agent is what isn't guaranteed, which is why business relationships (between customers and managers of HSAs ought to remain portable and transparent by law. Your manager might move, or you might decide to move away, from him.
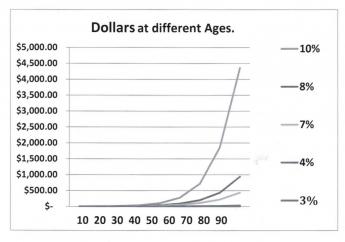
Start by looking at what happens if you jump your interest rate curve from 5% to 12%, or if you lengthen life expectancy from age 65 to age 93. That's what the graph is intended to show, and we stretch the limits to see what stress will do. Jumping to the highest rate (12%)the interest rate gets the balance to a couple of million dollars pretty quickly and lengthening the time period further enhances that gain. The combination of the two easily escalates the investment far above twenty million. The combination of extra time and extra interest rate thus holds the promise of quite easily paying for a lengthening lifetime of medical care, regardless of inflation. In fact, it gets the calculation to giddy amounts so quickly it creates suspicion.
|
Average lifetime health costs: $350,000 per lifetime
|
One person who does have practical control of the interest rate an investor receives is his own broker. The broker shares the income, but usually takes the first cut of it, himself. Covering a full century, Roger Ibbotson has published the returns on various investments, and they don't vary a great deal. Common stock produces a return of between 10% and 12.7% in spite of wars and depressions; if you stand back a few feet, the graph is pretty close to a straight line. You wouldn't guess it was that high, would you? If you don't analyze carefully, a number of brokerages offer Health Savings Accounts which produce no interest at all -- to the investor -- for the first ten years. Indeed, the income of 2% also amounts to nothing at all during a 2% inflation. In ten years, 2% approaches a haircut of nearly 20%, explained by the small size of the accounts, and by the fact that customers who know better will generally just politely look for another vendor. Since the number of accounts has quickly grown to be more than fifteen million, it might be time for some sort of consumer protection. The prospective future size of these accounts should command greater market power, quite soon. After all, passive investment should mainly involve the purchase of blocks of index funds, all with fees of less than a tenth of a percent . Much of this haircutting is explained by the uncertainties of introducing the Affordable Care Act during a recession and taking six years just to get to the point of a Supreme Court Test, to see if its regulations are legal and workable. It can be used to provide high-deductible coverage, but it's expensive.
That's the Theory. The rest of this section is devoted to rearranging healthcare payments in ways which could -- regardless of rough predictions -- easily outdistance guesses about future health costs. When the mind-boggling effects are verified, skeptics are invited to cut them in half, or three quarters, and yet achieve a worthwhile result. The purpose here is not to construct a formula, but to demonstrate the power of an idea. Like all such proposals, this one has the power to turn us into children, playing with matches. By the way, borrowing money to pay bills will conversely only make the burden worse, as we experience with the current "Pay as you go" method. By reversing the borrowing approach we double the improvement from investment, in the sense we stop doing it one way and also start doing the other. In the days when health insurance started, there was no other way possible. The reversal of this system has only recently become plausible, because life expectancy has recently increased so much, and passive investing has put that innovation within most people's reach. The environment has indeed changed, but don't take matters further than the new situation warrants.
Average life expectancy is now 83 years, was 47 in the year 1900; it would not be surprising if life expectancy reached 93 in another 93 years. The main uncertainty lies in our individual future attainment of average life expectancy, which we don't know, but probably could guess with a 10% error. When the future is thus so uncertain, we can display several examples at different levels, in order to keep reminding the reader that precision is neither possible nor necessary, in order to reach many safe conclusions about the average future. Except for one unusual thing: this particular trick is likely to get even better in the future. Even so, it is best to do only conservative things with a radical idea.
Reduced to essentials for this purpose, today's average newborn is going to have 9.3 opportunities to double his money at seven percent return and would have 13.3 doublings at ten percent. Notice the double-bump: as the interest rate increases, it doubles more often, as well as enjoying a higher rate. If you care, that's essentially why compound interest grows so unexpectedly fast. This widening will account for some very surprising results, and it largely creeps up on us, unawares. Because we don't know the precise longevity ahead, and we don't know the interest rate achievable, there is a widening variance between any two estimates. So wide, in fact, it is pointless to achieve precision. Whatever it is, it will be a lot.
|
| One Dollar: Lifetime Compound Interest |
Start with a newborn, and give him a dollar. At age 93, he should end up with between $200 (@7%) and $10,000 (@10%), entirely dependent on the interest rate. That's a big swing. What it suggests is we should work very hard to raise that interest rate, even just a little bit, no matter how we intend to use the money when we are 93, to pay off accumulated lifetime healthcare debts. Don't let anyone tell you it doesn't matter whether interest rates are 7% or 12.7%, because it matters a lot. And by the way, don't kid yourself that a credit card charge doesn't matter if it is 12% or 6%. Call it greed if that pleases you; these "small" differences are profoundly important.
If that lesson has been absorbed, here's another:
In the last fifty or so years, American life expectancy has increased by thirty years. That's enough extra time for three extra doublings at seven percent, right? So, 2,4,8. Whatever amount of money the average person would have had when he died in 1900, is now expected to be eight times as much when he now dies thirty years later in life. And even if he loses half of it in some stock market crash, he will still retain four times as much as he formerly would have had at the earlier death date. The reason increased longevity might rescue us from our own improvidence is the doubling rate starts soaring upward at about the time it gets extended by improved longevity. In particular, look at the family of curves. Its yield turns sharply upward for interest rates between 5% and 10%, and every extra tenth of a percent boosts it appreciably.
Now, hear this. In the past century, inflation has averaged 3%, and small-capitalization common stock averaged 12.7%, give or take 3%, or one standard deviation (One standard deviation includes 2/3 of all the variation in a year.) Some people advocate continuing with 3% inflation, many do not. The bottom line: many things have changed, in health, in longevity, and in stock market transaction costs. Those things may have seemed to change very little, but with the simple multipliers we have pointed out, conclusions become appreciably magnified. Meanwhile, the Federal Reserve Chairman says she is targeting an annual inflation rate of 2% of the money in circulation; the actual increase in the past century was 3%. If you do nothing at 3%, your money will be all gone in thirty-three years. If you stay in cash at 2%, it will take fifty years to be all gone.
But if you work at things just a little, you can take advantage of the progressive widening of two curves: three percent for inflation stays pretty flat, but seven percent for investment income starts to soar. Up to 7%, there is a reasonable choice between stocks and bonds; but if you need more than 7% you must invest in stocks. Future inflation and future stock returns may remain at 3 and 7, forever, or they may get tinkered with. But the 3% and 7% curves are getting further apart with every year of increasing longevity. Some people will get lucky or take inordinate risks, and for them, the 10% investment curve might widen from a 3% inflation curve, a whole lot faster. But every single tenth of a percent net improvement will cast a long shadow.
But never, ever forget the reverse: a 7% investment rate will grow vastly faster than 4% will, but if people allow this windfall to be taxed or swindled, the proposal you are reading will fall far short of its promise. Our economy operates between a relatively flat 3% and a sharply rising 4-5%. In other words, it wouldn't have to rise much above 3% inflation rate to be starting to spiral out of control. Our Federal Reserve is well aware of this, the public less so. A sudden international economic tidal wave could easily push inflation out of control, in our country just as much as Greece or Portugal. On the other hand, as developing nations grow more prosperous, our Federal Reserve will control a progressively smaller proportion of international currency. Therefore, we would be able to do less to stem a crisis that we have done in the past.
To summarize, on the revenue side of the ledger, we note the arithmetic that a single deposit of about $55 in a Health Savings Account in 1923 might have grown to about $350,000 by today, in the year 2015, because the stock market did achieve more than 10% return. There is considerable attractiveness to the alternative of extending HSA limits down to the age of birth, and up to the date of death. It's really up to Congress to do it. If the past century's market had grown at merely 6.5% instead of 10%, the $55 would now only be $18,000, so we would already be past the tipping point on rates. In plain language, by using a 10% example, $55 could have reached the sum now presently thought by statisticians -- to be the total health expenditure for a lifetime. By achieving a 6.5% return, however, the same investment would have fallen short of enough money for the purpose. Like the municipalities that gambled on their pension fund returns, that sort of trap must be avoided. Things are not entirely hopeless, because 6.5% would remain adequate if our hypothetical newborn had started with $100, still within a conceivable range for subsidies. But the point to be made provides only a razor-thin margin between buying a Rolls Royce, and buying a motorbike. If you get it right on interest rates and longevity, the cost of the purchase is relatively insignificant. That's the central point of the first two graphs. For some people, it would inevitably lead to investing nothing at all, for personal reasons. Some of the poor will have to be subsidized, some of the timid will have to be prodded. This is more of a research problem than you would guess: a round-about approach is to eliminate the diseases which cost so much, choosing between different paths of research to do it, or rationing to do it. Right now we have a choice; if we delay, the only remaining choice would be rationing.
Commentary.This discussion is, again, mainly to show the reader the enormous power and complexity of compound interest, which most people under-appreciate, as well as the additional power added by extending life expectancy by thirty years this century, and the surprising boost of passive investment income toward 10% by financial transaction technology. Many conclusions can be drawn, including possibly the conclusion that this proposal leaves too narrow a margin of safety to pay for everything. The conclusion I prefer to reach is that this structure is almost good enough, but requires some additional innovation to be safe enough. That line of reasoning will be pursued in a later chapter.Escrow Accounts and Over-Depositing. The main unpredictable feature of these future projections is you can't predict when you will get sick and deplete the account. Money withdrawn early is much more damaging than money withdrawn late in the cycle. Catastrophic insurance will somewhat protect against this risk, but the safest approach is to use segregated, somewhat untouchable, escrow accounts for future heavy expenses. That, combined with deliberate over-depositing, is the safest approach. If Obamacare would settle down, it might serve that function, as well, but the political situation is pretty unsettled until a large-group design is made final, and that seems to mean November 2016 at the earliest.Revenue growing at 10% will rapidly grow faster than expenses at 3%. As experience has shown, it is next to impossible to switch health care to the public sector and still expect investment returns at private sector levels. Repayment of overseas debt does not affect actual domestic health expenditures, but it indirectly affects the value of the dollar, greatly. Without all its recognized weaknesses, a fairly safe description of present data would be that enormous savings in the healthcare system are possible, but only to the degree, we contain next century's medical cost inflation closer to 2% than to 10%. The simplest way to retain revenue at 10% growth, on the other hand, is by anchoring the price to leading healthcare costs within the private sector. The hardest way to do it would be to try to achieve private sector profits, inside the public sector. This chapter describes a middle way. It's better than alternatives, perhaps, but not miraculous.
Cost, One of Two Basic Numbers. Blue Cross of Michigan and two federal agencies put their own data through a formula which created a hypothetical average subscriber's cost for a lifetime at today's prices. The agencies produced a lifetime cost estimate of around $300,000. That's not what we actually spent because so much of medical care has changed, but at such a steady rate that it justifies the assumption, it will continue into the next century. So, although the calculation comes closer to approximating the next century (than what was seen in the last century) it really provides no miraculous method to anticipate future changes in diseases or longevity, either. Inflation and investment returns are assumed to be level, and longevity is assumed to level off. So be warned. This Classical HSA proposal, particularly with merely an annual horizon, proposes a method to pay for a lot of otherwise unfunded medical care. The proposal to pay for all of it began to arise when its full revenue potential began to emerge, rather than the other way around. If a more ambitious Lifetime HSA proposal ever works in full, it has a better chance, but must expect decades of transition before it can. Perhaps that's just as well, considering the recent examples we have of being in too big a hurry. Rather surprisingly, the remaining problem appears merely a matter of 10-15% of revenue, but all such projection is fraught with uncertainty.
Revenue, The Other Problem. The foregoing describes where we got our number for future lifetime medical costs; someone else did it. Our other number is $150,750, which is our figure for average lifetime deposit in an HSA. It's the current limit ($3350 per year of working life) which the Congress applied to deposits in Health Savings Accounts. No doubt, the number was envisioned as the absolute limit of what the average person could afford, and as such seems entirely plausible. You'd have to be rich to afford more than that, and if you weren't rich, you would certainly struggle to afford so much. To summarize the process, the number amounts to a guess at what we can afford. If it turns out we can't afford it, this proposal must be supplemented, and the easiest expedient is to raise the contribution limits. Other alternatives are pretty drastic: to jettison one or two major expenses, like the repayment of our foreign debts for past deficits in healthcare entitlements, or the privatization of Medicare. Not privatizing Medicare sounds fine to most folks, but they probably haven't projected its coming deficits. It would leave us considerably short of paying for lifetime health costs for quite a long transition period, but it might be more politically palatable, like Greece leaving the Euro, than paying more. Almost anything seems better than sacrificing medical care quality, which to me is an unthinkable alternative, just when we were coming within sight of eliminating the diseases which require so much of it.
CHAPTER TWO: Fitting Employer-Based Health Insurance Into an Individual-based Framework
Chapter Two:
No history of American healthcare finance is complete without acknowledging the deep debt of gratitude we all owe to Big Business. Negotiating stormy waters, they created a workable insurance system and held it together for decades. Their legal premise was good health care for employees was essential for modern business. Society has now decided good health care is essential for life. This extension of the mandate has been awkwardly arranged. The main function of this chapter is to ease the transitions between employer-based health care and the other half of life, before and after forty years of employment. In the process, we would like to see Health Savings Accounts become a voluntary alternative for working people, both of them changing enough to co-exist. As a start, I can see no reason to prohibit anybody from having an HSA, with or without employer insurance as well. Nor can I see the slightest justification for unequal income tax treatment. Yes, health insurance companies must make some major changes, but after all, we're talking about changing health insurance.
History. Theodore Roosevelt had proposed a system of national health insurance, probably based on the example of Bismarck's German system, and Teddy nearly pulled it off. The American Medical Association considered the reform idea quite favorably until some physician leader (legend relates it was Morris Fishbein) had a change of heart and denounced it. Legend also has it that Fishbein was influenced by the bad treatment the Mensheviks received at the hands of the Bolsheviks in Russia. Fishbein was related to many Mensheviks, and this is said to have influenced his thinking, although its connection to Bismarck and the Flexner Report is a trifle hard to understand at this distance. Word of mouth history also blames this episode for the alienation of academic medicine (medical schools) from organized medicine (the AMA), dating from this issue. Somehow or other, this has to do with the Flexner Report of 1914, favoring the affiliation of medical schools to research universities. Much of this is gossip, and much of it is possibly quite wrong. It is related here to help the reader understand why many present political alignments exist, even if they do not explain why they persist. The fact that hardly anyone alive can recount precise details, does not diminish the intensity with which some present partisans hold their (possibly mistaken) beliefs.
Big Business was obviously drawn into a dispute of this magnitude, but in view of Teddy Roosevelt's past activities as a trust-buster, business leadership was unable to unite its constituents into taking one side or the other, openly. That division continues to this day, although it is fair to say the leadership of Big Business leaned in the direction of "reform" of the healthcare system, even while many heavy hitters in their ranks still remain violently opposed. Businessmen lean heavily on their lawyers for advice about non-business issues, and there can be no doubt it makes Big Business uneasy to read the plain language of the Constitution, especially the Tenth Amendment, and the McCarran Ferguson Act of 1945. The Constitution firmly proclaims the Federal Government is to have only a limited role in most areas, so medical care is therefore regulated by state governments. As a reminder, the states license hospitals, universities, medical schools and physicians, and the entire structure of organized medicine revolves around state control. As well as upon the Constitution, for which all this stands. The President of every county medical society in the nation takes his inaugural oath, with the wording of great similarity to those of George Washington, to uphold the Constitution. Not the Governor, or the State, but the Constitution. Medical Schools, nursing societies, hospital administrators and all similar officers are expected to take much the same oath, although many feel free to disregard it. When they do so, they meet the glares of many physicians and many lawyers. A corporation is only a creature of the state legislature, and all lawyers know what danger lies in flouting the courts.
With all this background of stern rules and bitter recollections, it must have taken skill and courage for Big Business to act as negotiator and peace-maker in constructing the collection of compromises and invisible unity, now called employer-based health insurance. The edifice was negotiated in the 1920s and rescued the health system from near-dissolution after the crash of 1929. Much of its strength lay in family-controlled corporations with close associations to local hospitals and other members of civil society. As family-held businesses gave way to stockholder-controlled corporations, American business became much less local and more national, with hired managers much more congenial with government bureaucrats and university presidents, than self-made entrepreneurs ever felt. The stage was set for "reform", and for several decades things seemed to work very well. Its legal high point was probably Franklin Roosevelt's court-packing confrontation, which Harry Truman tried but was unable to exploit. In 1965 Lyndon Johnson succeeded in some patchwork, successful for old folks, a failure for poor people. Hillary Clinton tried again and failed, with rumors circulating that Big Business had ruined her plan. Then Barack Obama tried the same plan; whether he succeeded or failed is yet to be made clear. In all these efforts, the issue was the same: take control of healthcare away from the States, and give it to the Federal Government. The decisive argument for business to avoid total war was also the same: if you ignore the Constitution for medical care, you may find you have opened the door for federal conquest -- of all corporate independence.
That's a capsule history of healthcare reform, confessing it must contain many omissions about closed-door arrangements. And leaving to last mention, Henry Kaiser's tax-avoidance scheme during World War II. In an effort to move steelworkers from the East Coast to build ships in his West Coast shipyards, Kaiser found wartime wage controls prevented him from paying workers to move. So he persuaded the War Production Board to look the other way from his healthcare scheme, devised as a non-taxable inducement. After the war ended, Congress continued to include employer-donated healthcare as a necessary business expense for the employer, while excluding it from the taxable income of the employee who got the "gift". Furthermore, the same tax exclusion was denied for the same expense unless it was donated by an employer. For seventy subsequent years, the tax abatements have repeatedly defied Congressional repeal, in spite of the denial of the same tax abatements for competitors. In this case, competitors are foreigners without voting rights, uninsured persons, and self-insured. The critical legal issue was health insurance had to be donated by the employer to qualify. Management would have everyone believe they are powerless to persuade unions to be reasonable. In the next section, we explore other motives and suggest a different solution.
Corporation Tax Deductions Support Our Health System.
This is the last anecdote, I promise you. It has to do with Ireland, the Emerald Isle, in 2000. In an effort to attract corporations to move there, the Irish Republic lowered its corporate income tax to 12.5%, an unheard-of low rate. To Irish delight, corporations in Sweden, Scotland, Germany and many other nations, promptly moved to Ireland to enjoy the low taxes. Since Ireland is mostly rural, there was a migration of Irish workers from the country to the city, causing a housing shortage in Dublin. A taxi driver, in passing a little Dublin shack, was pleased to tell foreign visitors the shack had just sold for a million dollars. That, in turn, set off a building boom, bringing construction workers to Dublin, and causing a shortage of mortgages, leading to boom-time rates. Irish bankers were delighted that little banks could be so top-heavy with imported mortgage money. The little Irish banks became overextended, and promptly collapsed, taking the stock market with them.
The moral of this little Irish tale is clear: lowering corporate taxes will definitely attract businesses to relocate to your shores, but if you lower them too much, too fast, it can cause a disaster. Some people conclude from this you should never lower corporate taxes; other people conclude you should lower taxes, but do it carefully and slowly. In the American case at present, it is tempting to try it to stimulate the economy, but we owe a powerful moral debt to the Europeans, who are in bad economic condition. If only we could devise a way to punish our enemies but not our friends, it would seem perfect. Selecting certain manufacturers but skipping others would do the trick nicely. By the way, our federal corporate tax is 35%. That's the highest in the developed world, so our hands are tied -- we're sorry, but we just have to do it to keep our own corporations from moving to Ireland. Other nations, like Japan and Switzerland, would be sure to notice we have this power, even if we don't use it against them. Yet. We hold a powerful international weapon, providing we use it sparingly, but gracefully.
And our own corporations? Well, that's the whole point. We would like them to take the pressure off health insurance, either by allowing other health insurance to be tax-exempt or by telling their lobbyists to look the other way while we remove Henry Kaiser's little gimmick. There's even a compromise, for those who admire bi-partisanship. Lower the tax exemption for existing corporations, but extend them to other companies and people in general. We're not looking to lose or gain revenue, we are looking for equal treatment under the law. And finally, the best way of all would only require one sentence. Just amend the Health Savings Account Law to permit the premiums for mandatory Catastrophic high deductible to be paid out of the account. Since the Accounts are tax-exempt, the reinsurance premiums would be, too. The level playing field for health insurance is restored in an instant. Only after the inequality resistance is removed, can you consider lowering the exemption.
Well, fine, what about corporate taxes? Since I am a single-issue voter, it isn't in my interest to declare a position on unrelated issues. But I stay within my medical mandate if I point out one thing about the politics of this. You don't have to be a magician to guess some corporations would like to have a tax reduction, because a tax reduction is a money in the bank. Other corporations might persist in the party line that it serves our interest to leave things alone. So, the leadership might just have to stand by, while a newly elected hothead makes a name for himself by introducing a bill to eliminate corporate taxes, entirely. Just what would the consequences be?
A tax deduction of 35% is a tidy sum, all right, but many states have a 10% tax, so it's really 45%. But look at what happens when you give your employees health insurance. It's a business expense, so a $10,000 health insurance policy only costs the company $5500. And then, remember the first chapter of this book. Every employee gets a payroll deduction of 2.9%, up to $117,000 of salary. That's another $3000, per employee. Some companies have hundreds of thousands of employees. And if you've got high-priced employees over $200,000 in salary, it's another $3800, but notice this: there's no top limit to the taxable salary, so if you've got a $10 million president, he's generating a $380,000 deduction for the company. Many companies positively love expensive health insurance, which includes extremely dubious Flexible Savings Accounts with a use-it-or-lose-it feature, leading to prescription sunglasses toward the end of December if the employe hasn't used it. All of those other deductions on a pay stub except the income tax withholding are probably eligible for tax deductions, too. It isn't too hard to imagine a resourceful accountant who could make the whole donation of health insurance a free gift, when you remember all employees are getting a tax deduction of several thousand dollars, too. The higher the premium the better, which isn't at all a good thing for market prices for the rest of us. The only thing which limits more and more deductible items is the company runs out of taxes to deduct from. Who wants lower corporate taxes? Not us, think a lot of companies.
And then, there's Greece. We can't lower corporate taxes more than 10% at a time, for fear of bankrupting Greece and sending the financial world into a tailspin. So even the most rabid populist can be persuaded to limit the size and pace of the deductions. Therefore, we have some other things on our wish-list while we wait to watch how low corporate tax can safely go. That being the case, there are some other things on the wish-list while we watch what gradual corporate tax reduction can do. I would like to see every Flexible Spending Account roll over its end of year surplus into a Health Savings Account. That would immediately create several million new HSAs, meanwhile getting some good for the money. I'm really serious about Health Savings Accounts. Everybody ought to have one, so remove the prohibition on having more than one health policy. What we mean to prohibit is taking two tax deductions, so say so, and let people have as many accounts as they want. This is particularly important if you want to reap compound interest for newborns for an extra 26 years, but there are probably lots of retirees who are healthy and want to store up their benefits for later, but now have nowhere to put them. Of course, we should allow everyone to have both an Obamacare policy and a Health Savings Account, with the proviso you can't take a double tax deduction. Not everyone will do it, and of those who do, not everyone will use both. But as long as they don't game the system, why not? It's a lot easier to defend freedom of choice than prohibitions.
Good Ol' Health Savings Accounts
In 1981 at what was then called the Executive Office Building of the Reagan White House, John McClaughry and I conceived the Medical Savings Account, later known as the Health Savings Account. John was at that time Senior Policy Advisor for Food and Agriculture, but he had read my book The Hospital That Ate Chicago, and it inspired him to think about a better way of financing health care. He asked me to come down to Washington to discuss the issue. We met and fleshed out the idea. Little did we then suspect how many delightful features would pour out of the simple little invention with only two moving parts.
It was patterned after the tax-deductible IRA (Individual Retirement Account) which Senator Bill Roth of Delaware was bringing out the following year. But with two major variations: our account contained the unique feature of a second tax exemption, given on condition the withdrawal was spent on health care. Otherwise, a regular IRA subscriber pays the usual income tax on withdrawals and gets only one tax deduction, the one he gets when he deposits money into the account. Bill Roth later produced his second kind, the Roth IRA, which allowed a tax-exempt withdrawal but took away the tax-exempt deposit. Only the Health Savings Account gives you both. In Canada, by the way, they do allow both deductions in their IRA, but in America only the HSA offers it.
Garlands of Unexpected Good Features. So the first part of a Health Savings Account is just that, a tax-exempt savings account, obtainable in the same way you get an IRA or a Roth IRA, although a few eligible outlets were slow to take ours up. And the second combined feature was to require a high-deductible, "catastrophic", stop-loss health insurance policy -- the higher the deductible, the cheaper the premium gets.
Further, the more you deposit in the account, the higher is the deductible you can afford, so you save money going either way and get extra benefit in your account for having a tailor-made insurance program. The industry term for this kind of insurance is "excess major medical", which the two of us wanted to avoid because of its implication it was somehow frivolous or unnecessary, when in fact it is central to the whole idea. Linked together, the two parts enhanced each other and produced results beyond the power of either, alone. The savings account was first envisioned to cover the deductible, but nowadays it also commonly attaches a special debit card to purchase relatively inexpensive outpatient and prescription costs. That led to further administrative savings to the subscriber if he shopped frugally for optimum proportions of deductible insurance. Right now, it's a little uncertain what the current Administration will permit in the way of catastrophic health insurance, so, unfortunately, it is just about impossible to give concrete examples of what the ultimate cost will prove to be. But we do know that in the old days, a $25,000 deductible was available for $100 a year. Nowadays, a $1000 premium is more likely. When we get to explaining first year and last year of life insurance, it will become clear that this premium can be appreciably reduced.
But while the savings account allowed someone to keep personal savings for himself, the insurance spreads the risk of an occasional heavy medical expense at what ought to be a bargain price for bare-bones insurance. You needn't spread any risk for small expenses because you control them yourself, but no one can afford some of those occasional whopper expenses. There's no reason why you couldn't set the deductible level yourself, weighing your own ability to withstand bigger risks. In practice, the actual savings were reported to approach 30% (compared with "First-dollar" health insurance), quite a pleasant surprise. But because of the younger age group of the early adopters, much of this saving was achieved in the out-patient area.
(Let's start using the present tense to talk about it, although right now it's hard to know what politics will permit.) So, hidden in this bland dual package are lower premiums, less administrative red tape, less moral hazard, but complete coverage. Right now, that's somewhat subject to change. It provides complete coverage in the sense that the insurance deductible can be covered by the savings account, but contains the option to be saved, invested or used for small outpatient expenses. Furthermore, the account carries over from year to year and employer to employer. So it eliminates job-lock, use-it-or-lose annoyances, and allows a healthy young person to save for his sickly old age. Curiously, many of the subscribers have elected to pay small expenses out of pocket, in order to make the tax deduction stretch farther.
In one deceptively simple feature, many of the drawbacks of conventional health insurance have been removed. The bank statement from the debit card can even do the bookkeeping. The first part of the two-part package, the savings account, creates portability between employers, opens up the possibility of compound interest on unused premiums, eliminates pre-existing conditions even as a concept, and creates a vehicle for transferring the value of being a "young invincible" forward into age ranges when the money really is likely to be needed for healthcare. Maybe some other features can be added later, but introducing an unfamiliar product is always greatly assisted by having it all appear so simple. The HSA only has two features, but they solve a dozen pre-existing problems.
To return to its history, nearly 15 million accounts have been opened, containing $24 billion. John McClaughry and I (neither of us received a penny for any part of this) were seeking a way to provide a tax exemption to match the one which employees of big business get when the employer buys insurance for them. That is, Henry Kaiser inspired us to do it. Although we got the general tax-free savings idea from Bill Roth, we did him one better by giving a deduction at both ends, provided only -- you must spend the money on healthcare to get the second tax relief. An additional novelty at that time was a high deductible, which permits a "share the risk" feature unique to all insurance, but invisibly limits it too expensive items. It wasn't the original idea, but it turns out you get spread-the-risk and limits to out-of-pocket patient costs in the same package. Who could have guessed?
Volume control versus Price Control in Helpless Patients.We did know a third automatic advantage, not fully exploited so far: it seems possible the hateful DRG system (with its codes restructured) could become a useful tool for dealing with a major flaw in the Medicare system. Professional peer review has become pretty good at controlling the volume of services, but prices still escape effective control. No amount of volume control can, alone, address the price issue. Controlling vital services for helpless people is a delicate matter.Other than two variations (double tax deductions, and incentives if used for health care), a Roth IRA would be nearly the same as an HSA, with independently purchased Catastrophic backup. But the assured presence of low-cost, high-deductible insurance provides security for another needed feature: Using individual accounts with year-to-year rollover , we could introduce the notion of frugal young people pre-paying the healthcare costs of their own old age. For all we knew, there weren't any frugal young people, but we were certainly pleasantly surprised. And catastrophic insurance added the ability to share the opportunity of that feature -- subsidizing the poor at bearable prices. As we will shortly see, it also offers an incentive to save for retirement. Think of it: almost nobody can afford a million-dollar medical bill, but almost everybody welcomes low premiums. Catastrophic coverage offers the only chance I know, of approaching both goals at once. And it offers the fall-back, that if you are lucky and don't get sick, you can use it for your retirement.Quite a few of those services match (or contain) identical items in the outpatient area. The outpatient area faces outside competition from other hospitals, drugstores or vendors. Instead of letting helpless inpatients generate unlimited prices for the outpatients, why not let competition in the outpatient area define standards of prices for inpatient captives? Outpatients and inpatients overlap in the ingredient components, considerably more than most people suppose. Inpatients may have higher overhead because of the need to supply their needs at all hours, but a standard extra markup around 10% ought to take care of that. No doubt some services are unique to the inpatient area, but a relative value scale is then easily constructed, thereby linking unique costs to other services which are exposed to competition. Ultimately, provable relationships to market prices might even discipline big payers demanding unwarranted discounts. This last is a deal breaker, provoking suspicions of abused power by a fiduciary. The government in the form of Medicaid is often the worst offender, so we need not imagine laws will prevent discounts so long as law enforcement remains crippled. Every business school teaches that discounts below cost are a path to bankruptcy, but business schools have apparently not had enough experience with governments to suggest an effective remedy.
As the only physician in the room, I also pointed out another pretty gruesome fact: either people end their lives have a lot of sicknesses, or they end up paying for a protracted old age. Only infrequently, do real people encounter both problems. It can happen of course; breaking a hip after long confinement in bed would be an example.
|
People end their lives with sickness, or else they must pay for protracted old age.
|
A tax deduction is a tax deduction, but this one has two: An incentive to save, and a later option to spend the savings on either healthcare or retirement. That's nearly specific enough. Furthermore, it offers a choice between saving preferences -- you can have interest-bearing savings accounts, or you can invest in the stock market, or a mixture of both. The HSA automatically converts to a regular IRA (for retirement) at age 66 when Medicare appears; that should be optional for all health insurance, but isn't. The IRA up in Canada includes both front and back features, but in the United States the HSA is the only savings vehicle to have dual deductions, so it's more flexible. As the finances of Medicare become shaky, it may be time to provide additional alternatives. At least, we ought to consider extending age 66 to a lifetime coverage option.
This harnessing of two familiar approaches makes a deceptively simple package which ought to be considered in other environments, unconnected with medical care. In most public policy proposals, the deeper you dig, the more problems you turn up. In this one, we found the proposal already had hidden answers to most concerns we could discover. It's possible to fall in love with an idea that does that for you. It lets you sleep at night, secure in the knowledge you aren't mucking things up for people.
Another surprise. Overall, the Affordable Care Act has probably helped sales of HSAs, since all four "metal" plans of the ACA contain high deductibles, serving in a (rather over-priced) Catastrophic role. This may be a way of covering the bets in a confusing situation. The ACA is a needlessly expensive way to get high-deductible coverage because it pays for so many subsidies. Frankly, it baffles me why subsidies swamp the costs of Obamacare but are made unworkable for HSAs. Many of the details of the subsidies are obscure, including their constitutionality, so we have to set this aside for the moment.
One good motto is don't knock the competition, but we must comment on a few things. The Bronze plan is the cheapest, therefore the best choice for those who choose to go this way. But uncomplicated, plain, indemnity high-deductible, would be even cheaper if its status got clarified. The good part is, the current rapid spread of high deductibles suggests mandatory-coverage laws may, in time, slowly go away. At first, the ACA looked like a bundle of mandatory coverages, all made mandatory at once. But they may be learning a few basic lessons as they go. Mandatory benefits are an example of mixing fixed indemnity with service benefits, with the usual dangerous outcome. Like many dual-option systems, they create loopholes. The HSA seems to avoid this issue by effectively being two semi-independent plans, for two separate constituencies -- who are the same people at different ages. Once more, we didn't think of it, the features just emerged from the plan.
That's about as concise a summary of Health Savings Accounts as can be made without getting short of breath. But of course, there is more to it, particularly as it affects the poor. For example, there is an annual limit to deposits in the Health Savings Account of $3350 per person, and further deposits may not be added after age 65. They can be "rolled over" into regular HSAs when the individual gets Medicare coverage, and supposedly has no further financial needs. So plenty of people have health care, but can barely support their retirement. These plans are absolutely not exclusively attractive to rich people, but it must be admitted, poor people start with such small accounts that companies can't operate profitably unless the client sticks with them for a long time. If people possibly can, they should scrape together one $3300 maximum payment to get a running start.
The problems of poor people can nevertheless be eased, within the limits of the plan's design. Since people will be of different ages when they start an HSA, it might be better to set lifetime limits, or possibly five-year limits, to deposits, rather than yearly ones. Some occupations have great volatility in earnings, and sometimes a health problem is the cause of it. To reduce gaming the system, perhaps the individual should be permitted to choose between yearly and multi-year limits, but not use both simultaneously. As long as the self-employed are discriminated against in tax exemptions, that point could certainly be modified. There remains only one major flaw, which we propose should be fixed:
Proposal 6: Congress should permit the individual's HSA-associated Catastrophic health insurance premiums to be paid, tax-exempt, by Health Savings Accounts, until such time as elimination of the present tax exemption for employer-based insurance is accomplished by other means.Subsidies for the Poor? Here's my position. If poor people could get subsidies for HSA to the same degree the Affordable Care Act subsidizes them, Health Savings Accounts should prove at least as popular with poor people as the Administration plan. Mixing the private sector with the public one is always difficult. Why not make subsidies independent of the health programs? There is no point in having the poor suffer because someone prefers a different health system. Quite often, a subsidy program is mixed with a public program, in order to make its passage more attractive; that's not necessary.
Proposal 7:That health care subsidies be assigned to patients who need them, rather than attached specifically to one or another health system that happens to serve them.Let's just skip away from all those digressions, and return to the poor in other sections. If the concern is, health care is too expensive, why in the world wouldn't everyone favor the cheapest plan around? Part of the answer, politics aside, is that young people have comparatively little illness cost, while old folks have a lot. Since Medicare, therefore, skims off the most expensive healthcare segment of the population, the fairness of any health subsidy program is difficult to assess. Evening out the tax deduction for the catastrophic portion equalizes the unfair tax deduction for self-employed and unemployed people. Perhaps the equality issue should be re-examined after each major revision since many moving parts get jostled, every time.
The government is going to have trouble affording the existing subsidy, so it may not endure, particularly at 400% of the current poverty level. But if we can subsidize one plan, we can subsidize the other, instead. The government would then be seen, and given credit for, saving a great deal -- by inducing destitute people to use HSA as an alternative option, equally subsidized by an independent subsidy agency. As for single-payer, the government for fifty years borrowed to continue Medicare deficit financing and got it to 50% universal subsidy without much notice. That's like boiling the frog too gradually to be noticed until it is too late. But suddenly expanding the 50% subsidy to the whole country at once, would definitely be noticed. Extending such levels to the whole country should anyway be buttressed with accurate cost data. Administrative cost savings are just a smoke screen. Total costs are the real cost. Other people also point out Medicare was financed after we had won some wars, but now we seem to be losing wars.
Spending Rules--Same Purpose As Escrow Accounts
Useful features are buried in the spending-rule idea. A portfolio would never go to zero if spending is held below a certain level; an endowment on auto-pilot. This magic number was once 3%, now is thought to be 4%. In trust funds for irresponsible "trust fund babies", spending rules are particularly common. In taxable circumstances, it is a vexing complication for non-profit institutions that federal tax rules require minimum annual distributions of 5%, somewhat more than a taxable account can sustain indefinitely, at least according to present theory, and assuming present costs. Every effort should be made to reduce middle-man costs, and the present rate of progress is encouraging. As long as medical progress continues to depend on a top level of talent, efforts to attack the cost of care itself may prove counter-productive.
In my opinion, a spending rule is pretty much the same as a budget, and the same goals can be accomplished with an escrow account, permitting no expenditures at all until a certain date, and then only for a stated purpose. And furthermore, there can be several spending rules, just as there are several lines in a budget. There surely ought to be both a discretionary spending rule and an inflation spending rule, for example, since inflation is beyond citizen control. As a practical matter, planning will generally mean 5% discretionary, and 3% inflation, for a total of 8%. Until recently, it was generally assumed if the Federal Reserve instituted, or Congress mandated, an inflation target of 2%, it would mean 2% was dependable because the Fed had unlimited power to print money. However, in 2015 the inflation rate is 1.5%, in spite of heroic efforts to use "Quantitative Easing" to bring it to 2% by buying two or more trillion dollars worth of bonds. Inflation has remained at 1.5%, resulting in much wringing of hands. So spending rules help establish responsibility for deviations.
It is not useful to engage in political arguments over why this is so, it must be adjusted for. The consequence is we have an Inflation Spending Rule of 3% and actual inflation of 1.5%, leading to a national inflation surplus of 1.5%. If a Health Savings Account has an Inflation Spending Rule of 3% only because that is what we have seen in the past century, our inflation is 1.5% under budget, which could easily be misinterpreted as an extra 1.5% to spend. When we figure out what this means, we can puzzle what to do with it, but until that happens, no spending allowed. Another precaution would be to have two spending rules, totaling 8%, only 5% of which is actually spendable. If we create special escrow funds for buying out Medicare or passing to our grandchildren -- the same thing.
|
If you don't limit yourself, Others will limit you.
|
| Spending Rules |
In the case of Health Savings Accounts, a spending rule of 6.5% within an investment yielding a net of 9%, is a special case, but a good one. The central purpose of the whole HSA idea is to lower the effective cost of medical care, by generating funds to pay for it. The more income generated, the lower the effective price of medical care, so why impose a spending rule? In fact, a spending rule for an HSA does not reduce the income, it only delays the spending of it, because either the funding account gets exhausted by the time of death, or it is rolled over into an IRA. Either way, there is no final end to HSA spending, only postponements. When spending is postponed, it eventually earns more income; the ultimate effect is more availability for health care. If a cash shortage forces the HSA to curtail health spending, the bills must be paid from other sources, usually taxable ones. So even in this situation, there is more health spending power ultimately generated, but it is generated by not spending tax-sheltered money. It could even be argued that diseases later in life tend to be more serious. Indeed, if a spending rule is under consideration for an HSA, it could be voluntary as long as there is no way to game it. Unfortunately, that can lead to coercion for someone's own good, always a dubious idea.
If a portfolio generates 8% but only spends 5%, there's a safety factor of 3%, almost exactly matching the long-term effect of inflation. We hope moreover, the inflation issue is addressed by using the theory that inflation of expenses should match inflation of revenue, but you never can be sure of it. It is, in fact, more likely they won't match. A spending rule increases the power to shift surplus revenue to years of high medical cost, which will be later years, and will, by compounding, actually increase the total amount of it. This consequence is not necessarily obvious. The spending rule guards another easily forgotten thought: the purpose of an HSA is not to pay for every cent of health care. It is meant to pay for as much of it, as it can. It is likely, to invent an example, to encourage skipping cosmetic surgery, so there will be money enough for cancer surgery at a later time.
The purpose of this soliloquy is to justify the establishment of escrow accounts within Savings Accounts, to keep the fund from wandering from its purposes, or at least to recognize it early if it does. There should be a Medicare buy-out escrow fund, with a suggested budget calculated to make it come out right. And a Grandparent's escrow fund, and Permanent Investment Escrow fund, budgeted to pay for a future lifetime of care, alerting the owner how much it is below budget. These escrow funds are intended to be flexible but intended to serve their purpose. HSA Account managers are encouraged to use them and to explain them. By making certain escrows mandatory and uniform, big data monitoring is facilitated. Other government access should be minimized.
Health Competitors for Windfall Money
A bank account earning interest will contain more money than a bank account earning no interest. How much the interest will be, depends on circumstances, but earning interest beats no-interest every time. In the case under discussion, the account is a Health Savings Account, and the alternatives for spending are healthy alternatives. Because the volume of money passing through the system is estimated to be huge ($325,000 per lifetime), the interest to be earned on 316 million Americans is staggeringly huge. In the following discussion, it is assumed the comparatively easy decision has been made to accept the money, but the highly contentious decision remains: how to spend it. The following choices immediately come to mind:
Pay off the health entitlement debts of the past.The U.S. Treasury reports our foreign debt to be $4.5 trillion, of which one trillion is owed to China, and one trillion to Japan. The Treasury does not issue data any more detailed than the national total, for the interesting stated reason that all Treasury bonds are general obligations. Some of this debt originated as Medicare subsidy, but it is not easy to learn more than that. In addition, it would only seem fair to devote some of a windfall for health to paying off its past obligations. For these two reasons, it would be possible to run an appreciable surplus without seeming to affect current balances.
Universal Entitlement. Obamacare was enacted on the proposition of universal entitlement to health insurance. Implicit in that claim was the idea that many Americans did not have and could not afford health insurance, and that insurance coverage represented some minimum level of healthcare entitlement, even if it had to be subsidized. Persons who did not have health insurance were regarded as jeopardized, even if they were in perfect health, and even if they did not regard health insurance as worth its cost. This uninsured risk within the population was covered by providers absorbing the cost, along with traditional health charities, and other levels of government. Somehow the idea was included that it was superior to have the federal government cover these costs, or perhaps it was superior to cover these costs with a graduated income tax. Although in the early stages there was some talk of reducing healthcare costs by federalizing them, it was eventually acknowledged, extra insurance coverage implied higher costs for everyone, except those who received government subsidies, derived from graduated income taxes, and identified as entitled by government regulation. It is a great curiosity of this campaign that employers were never pointed to as having a burden lifted when the existing system was still described as employer-based. As proposing to devote a huge windfall to the purpose tends to bring out, the cost of healthcare was being shifted from employer tax-deductions to individual taxation of the upper-bracket sort.
After three years of Obamacare, the two clear beneficiaries are health insurance companies and employers who donate the insurance to their employees. It is not clear either of these two groups was particularly suffering, so it is not obvious why a windfall should benefit them.
Half-Started HSAs
There's another quirk in the law, which may or may not endure. You don't need a linked high-deductible insurance policy to withdraw money from an HSA, but you do need it, to deposit more money. If you take advantage of that, watch out for the rule that you can't have two government plans at once, including Obamacare, Medicare, Medicaid, and Veterans Health Benefits. So it's best to take out the HSA first, then the other insurance. This is such a complicated process, it might very well change, so be sure to ask before taking any action.
In any event, the suggestion seems valid at the moment, that the worst to happen to you is to acquire a tax-deductible account which you aren't entirely free to liquidate until you retire. And it has a health insurance feature which is also tax-deductible to the extent it has been funded, but which can be used to empty the account if you are strapped for money. If you have other sources of funds, it probably would be best to spend the first, since doubly-deductible health insurance is hard to find.
Direct Premium Payments, Constitutional Issues
In earlier sections I said I like computerizing a health insurance exchange. But confessing does not suggest the difficulties are trivial. To enroll by computer implies access to a computer. Since millions of people are still frightened to touch a computer, it implies an army of instructors to guide newcomers through the process. And since the insurance choices confront applicants with a bewildering set of choices, some person they trust must explain the choices to them. Since no insurance system imaginable could satisfy every reluctant hesitater, a considerable complaint and re-assignment process would probably be necessary for years to come. Many people will choose the wrong policy, regret it, and ask to transfer. To continue, you wouldn't expect a person to trust his private data to a system, without a personal password. Fine, but what do you do with seven million passwords? People will forget them, leave them lying around in public, and disremember them. The crooks in the cyber underground will get seven million opportunities to break into the system and steal things. If insurers of older policies undertake passive resistance, things could get tangled for years. So why undertake all these headaches?
There may be other answers to this question, among which is likely to be a set of imperatives contingent on making it mandatory. We will let others make their own arguments since once the vague mandatory feature is dropped, related conjectural problems diminish or disappear. The Affordable Care Act does not proclaim health insurance is mandatory; it only states a tax is required if you don't meet its requirements. The language really does suggest you have a choice between taking the insurance and paying the penalty tax. The Supreme Court mandates the tax must be small, to avoid being coercive to the states. The Constitution forbids the federal government to regulate the business of insurance, a provision heavily emphasized by the McCarran Ferguson Act. If the Health Savings Account with an attached high deductible is allowed to substitute for minimum requirements, any medical requirement is satisfied if someone has the money, and the HSA provides the money. True, it would allow someone with the money to reject the medical requirements, but what objection can there be to that?
There is a legitimate need to facilitate interstate health insurance. That means a minimal set of information exchange items is useful. The person must be confidently identified, and the terms and limitations of one state's policies must be matched with those of a second state. The credit status must be roughly described, and the current premium payments verified. If there is a current illness, its previously related history must be exchanged. Subsequent communication should be conducted between insurance companies, not between 300 million subscribers. Having established the basics, a communications channel(client to-and-from insurance company) must be provided for later use, particularly for expenses, even diagnoses, which might apply. And while this list may not be complete, it is close to adequate and can be expanded a little. It is nearly enough to get travelers, transferees and money exchanges to be organized. It will be sufficient for current needs and can be supplemented between particular states at conferences. And it would satisfy the Constitutional issue without needlessly inflaming it. If the Obama Administration expresses a willingness to compromise, these are the lines it might follow. On the other hand, if the issue is forced to the Supreme Court, the Court might be persuaded to follow these lines. We present three other liberalizing proposals for Electronic Insurance Exchanges:
One. Let a Thousand Flowers Bloom. The Affordable Care Act provides for selling high-cost health insurance products, meeting certain specifications, on the Electronic Health Insurance Exchanges. It's not obvious why the government has a legitimate interest in promoting one kind of health insurance over another, but perhaps a case can be made. Uniform interstate protocols are legitimate between insurance companies, along with standardized codes. And a website is a legitimate means for citizens of one state to communicate with insurance for sale in another state. Beyond setting standardized definitions, the communication between customer and insurer can be left to the individual companies. The case for excluding many existing types of policies has not been made, and this has particularly infuriated the subscribers of such policies, particularly those cheaper than the preferred variety. So why not enable or even facilitate the construction of such exchanges in every state which wants them, privatize the electronic programming and operations, possibly even subsidize them. And then permit every one of them to set its own rules for the products to be sold across state lines, setting its own prices as long as the prices clearly relate to the same products for every state-licensed insurance client who wants to utilize a particular product. Nobody must use the system, but everyone may use it. If no one uses it, it needs improvement. There could be multiple exchanges in each state, but the state may set limits, and no state is required to have any. In return for federal assistance, the federal government is limited in its involvement in setting rules which guarantee access to every system for every insurance company, and every citizen.Two. Specify That Health Savings Accounts are Acceptable Options. In fact, if Health Savings Accounts (linked to a matching high deductible), were available as an option among many other options in the Electronic Insurance Exchanges, only the worth of the option would be in dispute. The claim of HSAs to being listed, is they are cheaper than any other option. That's a feature which is certainly desirable for a Law which puts emphasis on helping the poor. It could potentially add tax-free investment funds to a pool which helps fund the program or fund its deficit. Such windfall income could provide revenue for the costs of educating and coaxing people into making better choices, and is much less apt to provoke the irritation of mandating people to do unpleasant things for their own good.
|
| Tenth Amendment |
Three. Be brief(in requirements), and let who will be clever(in details). The threat of the Tenth Amendment hangs over all federalizing initiatives, not just the Affordable Care Act. If Electronic Health Insurance Exchanges would limit their scope to the flexible enlargement of interstate insurance sales, the insurance would clearly be part of interstate commerce, and thus safe from any revival of the Court-packing disputes of the 1930s. There is almost no justification for interposing the Federal Government into the middle of most communication between subscriber and insurance company. Permitting smaller states to enlarge their markets might by itself relieve many of the indirect pressures now limiting competition as a force to suppress healthcare prices; and could limit the damage to established insurance carriers, who will probably need time to recover from the changes it would force on their marketing.
Proposal 6: Congress should mandate the licensing to sell health insurance to be widely inclusive, including Health Savings Accounts and Catastrophic Coverage, and subject to regulation in the state of corporate domicile, subject to objection by the state of residence of the insured. When there is conflict, an appeal may be federal.Furthermore, the spread of computers has reached a point where people are sensitive about being commercially manipulated by computers. Fifty years ago, the department store had a computer and the customers didn't. Nowadays, even children have them, and just about everyone is touchy about the way early-adopters try to bamboozle the innocent, putting their own products on the first page, in big letters, and "all others" under a button that doesn't work. Considering all the compromises needed to satisfy a common denominator, it seems very likely some other products would be more suitable for some people. "Hogging the limelight" and forgetting to mention other alternatives have become such common practices, people are on the lookout for them. The term "user-friendly" is now a part of the English language, people immediately bristle at signs of high-handedness, of which there is great plenty in the computer world. It is no secret businesses will tolerate most taxes or indignities, just so all of their competitors are seen to endure the same. It was once a common experience to have one competitor offer to design a computer program for the industry, quietly slanting the terms of entry to favor its own products. Was this just another example of it?
Therefore, allowing privatized insurance exchanges to become available for all variants of health insurance might have allowed time for discovering other features which might require special adjustments. After all, health insurance would remain half-state and half-federal, and undiscovered problems may yet surface. Even if the President planned to run healthcare like an Egyptian Pharoh, a gradual switch to individually owned and selected life insurance would have-- in time -- eliminated the need for pre-existing condition exclusions. It might even have provided an opportunity to reduce premiums for insurance which protects against the cost of appendices, indirect hernias, cataracts, uteri, prostates, and gall bladders --that have already been removed. Not everyone would want such features, but that's a small price to pay for the freedom to want them. A long-term shift to lifetime health insurance might very well require other adjustments, but it would be best to wait to see what they are. Meanwhile, the public will get the idea, teach each other, and get where it wants to be in a few years. That's at least as quick as a mandatory system can respond to industry lobbying, and still, get wherever it wants to go.
However, after all the uproar about the introduction of computerized direct-pay insurance has subsided, a great many opportunities are probably lost for decades, and any suggestions are probably futile. One thing remains, however, in view of the likelihood the issue of the Tenth Amendment will soon arise. How can we preserve the Constitution and still take advantage of our continent-wide marketplace?
The Argument Against National Uniformity of Prices.
It is abundantly clear the Founding Fathers were concerned with unifying a collection of thirteen sovereign states and had to make concessions. Furthermore, it is also clear no other nation in two hundred years has been able to match the achievement, even with massive wars and millions of casualties. So the instinct is strong to leave our Constitution alone. If it was not originally clear, the Civil War made it so. Nevertheless, the nation is laced with successful interstate corporations, for the most part, regulated by the state, not national, law. It seems to have been accomplished by establishing stock exchanges in a few states, operating under a few states' regulations, and otherwise allowing each corporation to choose a state of domicile, where the corporation can be regulated by the laws and courts of that state. The arrangement lasted for two centuries, and only later is starting to bend, under the pressures of electronic innovation. We seldom hear much uproar about the corporate arrangement under the state-federal problem. Why can't health insurance companies accomplish the same thing without federal oversight?
Well, for one thing, some states are still so sparsely settled, they cannot assemble the actuarial minimum numbers to have more than one viable health insurance company, or more than one HMO (Mrs. Clinton please note). Other states are densely populated enough to have several viable insurance companies, so the two-state sizes resist changes made to accommodate each other. The two have a great many dealings with the major corporations in their states, allowing them to pressure state legislatures into favoring state "champions", or else resisting the power of large insurance companies to dominate one state marketplace.
However, this is all pretty small peanuts, and it would seem fairly simple to separate the buying and selling of insurance companies from the buying and selling of insurance. After a while, one or two state exchanges would come to dominate and cluster in one area; while a handful of companies would start to dominate national health insurance business, and therefore migrate their health insurance operations into some different legal climate. In particular, our history of the migrating frontier made local communities restless about the distribution of doctors and hospitals. They could, of course, pass a law if one cabin is built on Pike's Peak, there must be two neurosurgeons within a hundred feet of it. The futility of such laws was soon apparent, and almost all resorted to some sort of incentives to attract medical resources found to be in short supply. State licensing was sometimes a way to create a local monopoly as a reward for a hospital to locate, or some specialist to open an office. But the development of health insurance provided an ideal way to attract specialists in short supply, by the simple expedient of overpaying them. Naturally, such communities resist the proposal to have national uniform fees, as interfering with the laws of supply and demand. Large cities, on the other hand, see national uniform fees as a way to suppress high fees. Our Founding Fathers recognized what was going on, and responded by letting anything commercial be regulated by the local states, flying the flags of states rights or state sovereignty. Franklin Roosevelt, a big-state resident, thought he could accomplish the big-state goal by calling it "court packing", but the nation soon told him his landslide electoral victory had some limits if it had that kind of result. Although Roosevelt largely accomplished his goal by other means, repeated attempts to make medical care nationally uniform has resulted in some kind of Presidential disaster. Things like medical care should become nationally uniform when the country becomes nationally uniform, but not sooner. Actuarial facts change pretty rapidly, as the discovery of gas shale in the Dakotas recently demonstrated. Any fixed but ideal arrangement will eventually fall victim to an agile and geographically flexible competitor.
Two personal examples have emphasized the point to me. In 1947, the Society for the Study of Internal Secretions (later known as the Endocrine Society) held its international meeting in a single lounge in a Chicago hotel. Nowadays, seven thousand national members meet in three concurrent ballrooms, and the shortage of Endocrinologists is over. To my surprise, a gentleman who looked like a Roman Senator approached me after a speech, and invited me, first to dinner, and then to become a paid consultant in his state which had no Endocrinologist. The other example was being approached by a lady in a pink hospital volunteer's uniform, asking me if I would like to become the sole doctor on a resort island of very rich folk, an hour from New York City. I accepted the first offer and declined the second, but the point is, people, protect their own personal needs when national health insurance is under discussion. And they often do not mean to be thwarted by supposed needs for national uniformity.
Congress and the Supreme Court are urged to view the Tenth Amendment as a compromise between big and small states which still enjoys wide support. Big states desire uniformity in order to suppress prices, while sparsely populated states reject uniformity in order to maintain control of local interests.Proposal 5: Congress is urged to permit the domicile of health insurance corporations to be in one state chosen by the corporation. But all health insurance should be freely sold interstate, subject to regulation by the state of domicile.(2611)
Lifetime HSA and Whole Life Insurance: A Basic Difference
Over the years, much experience and lore have accumulated about running a life insurance company. Because the managers ordinarily are responsible to others who have risked private capital, more latitude can be extended to them than to taxpayer-owned entities. Consequently, it may be wise to obtain experienced counsel to suggest some business limits and latitudes which need to be authorized by law. The following is meant to suggest some areas which may need attention. And a lifetime Health Savings Account has at least one unique difference with whole-life insurance. A moment's thought about Lifetime Health Savings Accounts immediately highlights it. Life insurance has only one benefit claim, the death benefit. Once the flow of premiums begins, only one liability by a life insurer has to be made, the length and risk of individual longevity. The relationship goes on autopilot and a rough match can be made between the pool of bonds and the pool of policies at any time, adjusting only for policy additions and subtractions, or for fluctuations in the bond market. A Health Savings Account, on the other hand, must anticipate a possibly constant stream of deposits and withdrawals.
It is probably true, more money will be deposited in whole-life insurance in response to a fixed annual premium billing, than if deposits are optional in date and amount, so it probably would be wise for the manager of a lifetime Health Savings Account to calculate annually what deposit is needed, for each client to meet his goal, judged by his age and past progress. He should send reminder notices for the "suggested" amount. The purpose of health insurance is to provide money for healthcare when absolutely needed, building up a fund for potentially even more urgent future emergencies. We have partially surrendered the right to mandate the amount, in favor of creating incentives to save it. Consequently, there will be a more constant drain on the investment reserves, matched by a somewhat greater inflow needed from outside sources. The Law of Large Numbers will smooth this out as it does with bank balances, but some volatility is unavoidable.
Since the general inclination is to limit the Catastrophic health coverage to hospitalizations, the attrition to their independent reserves in the account balance should be constrained (not limited) to paying at least one deductible, by adding one deductible to the escrow section, to reassure the hospital it is available. The non-escrowed balance would then more closely reflect the growing retirement savings earned by the arrangement. Since the Catastrophic Insurer is ordinarily an independent company, coordination is essential for long-term coverage. We can get more specific, but for now, the risks to be managed are outpatient costs, less frequent but larger inpatient deductibles, and what for now we can call "all other". All three could usefully use reasonably independent escrows, which repeated display would encourage.
Overdrawn Claims. Since any client might be hit by a truck within a week of establishing an account, new customers present the biggest problem with getting escrowed reserves established. A large front-end payment can be required, and eligibility for benefits can be delayed. Lines of credit may have a place. Otherwise, established customers must fund and be compensated for the risk of early claims. Most organizations will probably elect some combination of the several approaches, with some combination of selecting which phase of the combined insurance should or should not subsidize the others, and how it should be repaid, and at what age. Bond issues are a possibility.
Overestimated Reserves. In the long run, solvency will depend on deliberate over-reserving, gradually reduced as experience accumulates. The basic premise is young people are comparatively healthy, whereas most of the heavy sickness costs will appear as the client approaches and attains retirement, many years later. Compound investment income will grow over time. There may be periods of mismatch between accumulating and invading reserves, so there should also be a provision for intergenerational borrowing and repayment, the size of which will be established at the onset. Every effort should be made to reduce these shortfalls by overestimating the need for them, possibly based on archived statistics from the term-insurance era. Nevertheless, future shortfalls and future bubbles will both be steadily predictable, and unexpectedly volatile, so over-reserving must be seen as permanently advisable. The consequence of all this is a continuing need for some allowable non-medical use of surpluses, such as conversion to retirement accounts, in order to generate reluctance to invade the reserves. The importance of this easily overlooked necessity is very great.
Proposal 8: Congress should state the principle that necessary Health Savings Account reserves should be somewhat overestimated at all times, linked to the incentive that individual non-medical uses of surpluses should be permitted at times when they are generally unneeded for health purposes.Underestimated Reserves. And almost of equal importance is the need for early warning when reserves are threatening to become inadequate, in spite of every effort to overestimate them. Some sophisticated body must be created to oversee the growth of aggregated reserves, mandating increased contribution rates from subscribers. Since some subscribers could discover an increased contribution rate is a hardship, the oversight body must have the right to reduce benefits to uncooperative subscribers. That is, instead of reimbursing at 100% of the cost, they may have to impose a seldom-used rate of less than that. In order to perform this unpopular task, the oversight body must have access to better information than the public does, to be in a position to impose small steps rather than big steps. Under all these unpleasant circumstances, Congress could make the upper limit for contributions more flexible. At the moment, it is $3300 a year. However, while that amount now seems adequate enough, the figure is entirely arbitrary, probably set to prevent speculators from abusing the tax exemption. Therefore, if the upper limit is raised to address underestimated reserves, money might well be forthcoming to address the underestimate, which by then might have proved to be no underestimate at all.
Proposal 9: Congress should authorize the Executive Branch to raise the upper annual limit for deposits to Health Savings Accounts, whenever (and for such time as) average HSA reserves fall below an advisable level.
Some Ruminations About the Far Future.
George Washington soon learned he couldn't defend the country without taxes, so in time the Constitutional Convention lodged firm control over taxes in Congress. If we must have taxes, the people must control them. Except for defense, Congress has ever since been cautious about imposing taxes. Reducing taxes is quite in accord with this attitude, except net reduction of taxes, after raising them first, maybe a little tricky.
Net reduction of taxes is an important argument in favor of tax subsidies for Health Savings Accounts, using them as incentives to healthy people to "tax" themselves while they remain young and healthy. Investing the money internally, the subscribers can meanwhile protect it for their own use when they inevitably grow old and sickly. If interest greater than the rate of inflation is paid, the money returned should exceed the money invested. Investing the money tax-free further helps the process. If people get back more than they contributed, they recognize it as frugal, saving for a rainy day, and so on. Lifetime Health Savings Accounts were designed as a way to enhance this thinking, and are described in Chapter Two. Over thirty years have elapsed since John McClaughry and I met in Ronald Reagan's Executive Office Building in Washington, but there has been a continuing search for ways to strengthen personal savings for health while avoiding temptations to tax our grandchildren, or to make money out of harmless neighbors. Many of the financial novelties naturally derive from models in the financial and insurance industries. This book in largely a result of such thinking.o
But the biggest advance of all has nevertheless come from medical scientists, who reduced the cost of diseases by eliminating one darned disease after another, and meanwhile increased the earning power of compound interest -- by lengthening the life span. We thus luckily encountered a "sweet spot", where conventional interest rates of 6% or better take a sharp turn upward, while 3% of inflation still remains fairly constant. My friends warn me it must yet be shown we have lengthened life enough, or reduced the disease burden, enough to carry all of the medical care. That may well be true, but we seem close enough to justify giving it a trial as a partial solution. Before the debt gets any bigger, that is, and class antagonisms get any worse.
While Health Savings Accounts continue to seem superior to the Affordable Care proposals, you can seldom be quite sure about details until both have been given a fair trial. The word "mandatory" is, therefore, better avoided at the beginning, and awarded only after it has been earned. As a different sort of example, the ERISA (Employee Retirement Income Security Act of 1974) had been years in the making but eventually came out pretty well. In spite of initial misgivings, ERISA got along with the Constitution and its Tenth Amendment, and the McCarran Ferguson Act which depends on them. We had the Supreme Court's assurance the Constitution is not a suicide pact. So with this general line of thinking, and still grumbling about the way the Affordable Care Act was enacted, I had decided to hold off and watch. The 1974 strategy devised in ERISA, by the way, turned out to be fundamentally sound. The law was hundreds of pages long, but its premise was simple. It was to establish pensions and healthcare plans as freestanding companies, substantially independent of the employer who started and paid for them. Having got the central idea right, other issues eventually fell into place. Perhaps something like that could emerge from Obamacare.
Nevertheless, growing costs are ominous for a law proclaiming it intends to make healthcare Affordable. After several years of tinkering, this program stops looking like mere mission-creep and starts to look like faulty reasoning, maybe even the wrong diagnosis. While waiting for the Obama Administration to demonstrate how the Act's present deficiencies could justify rising medical prices and greatly increased regulation, I brushed up seven or eight possible improvements to Health Savings Accounts, just in case. They had been germinating during the decades after Bill Archer, of the House Ways and Means Committee, got Health Savings Accounts enacted. However, my proposed new amendments wouldn't change the issues enough to cause me to write a hostile book. More recently, some newer variations grabbed me: Health Savings Accounts might become lifetime insurance, and thereby save considerably more money, without the fuss Obamacare was causing. Furthermore, in 2007 the nation immediately stumbled into an unrelated financial tangle, almost as bad as the Great Depression of the 1930s. A depression might lower prices, but if it provoked accelerating deflation, we could be cooked. And thirdly, the mistake of the Diagnosis Related Groups was such a simple one, failure to understand it might not be a complete description. Seen in their best light, unrecognized mistakes were about to disrupt a functioning system, while simple solutions were sometimes ignored. Maybe the problem was trying to spend our way out of extravagance, made worse by massive transfers from the private sector to the public one -- actually, just the opposite of what Keynes proposed. And finally, individually owned and thus portable policies, always held the potential for a small compound investment income. But the recent thirty-year extension of average life expectancy is what really changed the rules. The potential for much greater revenue from compound interest made an appearance, simply waiting for the recession to clear, and to be given a chance to prove itself with normal interest rates.
Cost is the main problem. The Affordable Care Act might be making the wrong diagnosis, even though it used the right name. Employer-based insurance did create pre-existing conditions, and job-lock; losing your job did mean losing your health insurance, and often it was a hard choice. If employer-basing caused the problem, why didn't the business community fix it? Is the only possible solution to pass laws against pre-existing conditions and job lock? Maybe, even probably, a better approach was to break, soften, or change the link between health insurance and the employer. Sever that linkage, and the other problems just go away; perhaps less drastic modification could even achieve the same result. ERISA had discovered such a new concept, forty years earlier. Employers might well bristle at the obvious ingratitude, but real causes were creeping up on them unawares. Generations of patronizing legislators had found it easier to raise taxes on the big, bad corporations, than on poor little you and me. Employers had always received a tax deduction for giving away health insurance to employees, but now, aggregate corporate double taxation made it approach fifty percent of corporate revenue. Nobody gives away fifty percent of his income graciously; for its part, the Government thought it couldn't afford to lose such a large source of tax revenue. Big business prefers to avoid the subject, while big government tends to mislabel things. It's mainly a difference in style.Another issue: the approaching retirement of baby-boomers slowly revealed that Medicare, wonderful old Medicare with nothing whatever wrong with it, had been heavily subsidized by the U.S. Treasury, which was now paying its 50 percent subsidy out of borrowing from foreign countries, notably Communist China. Medicare's companion, Medicaid, subsidized by an elaborate scheme of hospital cost-shifting, transferred most of its losses back to Medicare. And, guess what, the Affordable Care Act transferred 15 million uninsured people into Medicaid. By this time, Medicaid had become hopelessly underfunded and poorly managed, and 15 million angry people were about to find out what they had been dumped into. Other maneuvers affecting the employees of big business are delayed a year or two, so we may not discover what they amount to, until after the next election, four or even five years after enactment. Meanwhile, the Federal Reserve "solved" the problem of mortgage-backed securities by buying three trillion dollars worth of them. That may not seem to have anything to do with Obamacare, except it pretty well crowds out any hope of buying our way lose of this new trouble. And it sure underlined our central problem. There was nothing all that bad about the quality of a fee-for-service healthcare system which gave everybody thirty extra years of life in one century. Two extra years of life expectancy even emerged in the past four calendar years, in fact. Our problem is lack of money. Lack of money, big-time, and Obamacare was going to cost even more. Health Savings Accounts, new style, emerged from all this confusion as a possible rescue for the cost problem. All this, helped me decide to write this book.
There are some who persuasively argue our even bigger problem is Constitutional. Perhaps because I'm a doctor rather than a lawyer, I don't consider the Constitution to be our problem, I consider it to be Mr. Obama's problem. Because the 1787 Constitutional Convention was convened to unite thirteen sovereign colonies into a single nation -- and splitting it into more pieces wasn't on anybody's mind at all -- they reached a compromise, brokered by two Pennsylvanians, John Dickinson, and Benjamin Franklin. The small states wanted unity for defense, but they also wanted to retain control of their local commerce. They knew very well big states would control commerce in a unified national government unless something fundamental was done to prevent it. Speaking in modern terms, a uniform new health insurance system risks being designed to please big cities who mostly want to hold prices down and wakes up. Sparsely settled regions want -- or need -- to be able to raise prices, here and there, when shortages appear, of neurosurgeons or something like that. The full algorithm is: price controls always cause shortages, so shortages are only cured by paying a higher price. Eventually the Constitution was engineered to give power over all commerce to the several states; otherwise, the small states declared there would be no unified nation.
That's how we got a Federal government with only a few limited powers, reserving anything else to the states. Absolutely everything else was to be a power of the states, except to the degree the Civil War caused us to reconsider some details (which Franklin Roosevelt's Supreme Court-packing enlarged). So, that's why the 1787 Constitution effectively lodged health insurance regulation (among many other things) in the fifty states. Furthermore, The Constitution in the later form of the 1945 McCarran Ferguson Act thereby definitively insulates health insurance from federal regulation, reinforcing the point in a very explicit Tenth Amendment. This may regrettably create difficulties for interstate businesses, and for people who get new jobs in new states. Many states have too small a population to support the actuarial needs of more than one health insurance company, thus creating monopolies in many states and consequent resentment of monopoly behavior. So, work it out. But don't give us a uniform national health system.
There, in a nutshell, you have a brief restatement of the Constitution's commerce issue in the language of the Original Intent point of view. The Constitution as a living document is all very well, but there must be some limits to stretching its plain language; otherwise, it becomes hard to understand what in the world people are talking about.Lifetime HSAs could solve the problem of differing state regulations by allowing the individual subscriber to select a managing organization domiciled in "foreign" states, and thus indirectly if the individual chooses, select a different home state for its regulatory climate. After all, the nation has changed in two centuries from a culture of farming in the same local region most of your life, to one where it seems normal to change home states almost yearly. Businesses tied to local laws like insurance, do not move easily. The consequence for lifetime Health Savings Accounts might be a niche market for health insurance in small or sparsely settled states, or others which reject specific California or New York State regulations. Paradoxically, California presently has over a million HSA subscribers, so we must not underestimate the ingenuity of necessary workarounds. Eventually, local pressure mounts to change local regulation, doubtless balanced by the attractiveness of acquiring disaffected customers from out-of-state. All of this could be accelerated by internet direct billing. Consequently, to avert this, we propose:City dwellers have trouble imagining anyone in favor of either higher prices or lower wages, let alone negotiable prices as the central bulwark of a different way of life. The Civil War toned it down a little, but if it is nothing else, our system is tough-minded and realistic, doesn't surrender easily. The U.S. Supreme Court may soon make the Constitution and its central compromises into the central issue of the day, or they may wiggle and squirm out of it. But as long as they keep squirming, cost containment will remain the central commotion of the Affordable Care controversy. In certain parts of the country, price controls are seen as just one step before shortages appear. That's not entirely unsophisticated. As we will see when we come to it, lifetime Health Savings Accounts could materially reduce the sting of the cost issue, and thus made the final decision for me to write this book. The Constitutional issue, possibly, lurks for another day.
The case in point. On the particular Constitutional point, I would comment whole-life insurance companies in the past seem mainly to have addressed the Federal-State issue by obtaining multiple licenses to sell their products, state by state. Which might bring the Constitutional issue right back, because most insurance companies in practice attempt to be compatible with the largest states, just as John Dickinson predicted they would. In effect, the smaller states are forced to accept whatever regulations the big states have chosen first, or else they might have to do without some new product. Whole-life insurance seems rather less subject to the problem of conflicting regulations because that industry inadvertently acquired another trump card. Life insurance mostly uses bonds in its portfolio, matching fixed income with fixed liability. That's a noble thought, but the additional practicality has surely occurred to insurers that state governments issue a lot of bonds, and insurance companies are major customers for bonds.
Proposal 6: Companies which manage health insurance products, particularly Health Savings Accounts, should be permitted to select the state in which they are domiciled, but must, therefore, accept the domicile-state's regulation of corporations. Such licensed corporations may sell direct billing products into any other state; but products sold in another state must mainly conform to the regulations of the state in which the particular insurance operates, even to the point of disregarding any conflicting regulations by the state of corporate domicile.Changes in Future Cost Volatility. At an advanced age, illnesses are more severe and more sudden. Right now, increasing longevity also mostly affects elderly people who live longer toward the end of life, by widening the interval between the last two major illnesses. You can never be entirely sure that will continue to be the case because medical care and its science constantly evolve. Furthermore, the cost of care often has more to do with the patent status of a drug or device, than with its manufacturing cost, sometimes turning a cheap illness into an expensive one.Comment: Fifty years ago, the main function of any State Insurance Commissioner was to assure the continued solvency of insurance companies, so insurance would be available when the customers needed it. In the past few decades, however, many insurance commissioners with populist leanings have viewed themselves as protectors of the public against price gouging. That is, they adopt the big-city, big-state, point of view. One Insurance Commissioner attitude might thus insist on high premiums, Commissioners with another attitude might reward low premiums. Insurance companies should, therefore, welcome laws which make it easier to switch the state of domicile, since the attitudes of insurance commissioners can change very quickly.
Comment: Lifetime insurance was pressed forward by discovering the investment world's computer-driven innovations might make lifetime coverage far easier, less chance, and considerably more financially attractive, than coverage in self-contained annual slices. It is common knowledge in insurance circles that most term life insurance would be unprofitable, except so many people drop their policies. Therefore the attitudes of different states are not completely predictable. Some states are more aggressive than others in adopting new technology, for example.
One thing you can be sure of, restructuring health insurance in the way to be suggested in Chapter Two, would result in a general reduction of health insurance markup, by exposing local insurance to the more nationwide competition. Health costs themselves might skyrocket, or they might largely disappear, but in any event, will probably end up cheaper than by using other payment methods. No doubt critics will find large numbers of nits to pick since states retain the right to design idiosyncratic regulations, but new regulations would remain semi-optional for residents to the extent some neighboring state disagreed with them. No matter what else turns up, it will be pretty hard to match the cost variation from national marketing, demonstrated by ten minutes of internet cruising. In fact, the great obstacles to an effective system in the past, like "job lock" and "pre-existing conditions", present no obstacle at all to lifetime HSA within an HSA regulatory framework. Many problems would stand exposed as artificial creations of linking health insurance to employers, at least as long as health insurance remains modeled on term life insurance. Just change to a more natural system tested for a century as whole-life insurance, and such technical problems might simply vanish. Even slow adoption, based on public wariness about a new idea, has its advantages.
Although prediction of future sea change is uncertain, a brief review suggests future healthcare financing could very well become highly volatile, in both frequency and costliness. Therefore, spreading the risk with insurance gets more attractive to age groups unable to recover from major financial setbacks. Planners would do well to consider such things as last-year-of life insurance, or some other layer of special reinsurance. Immediately, such ideas raise the question of multiple coverages, with multiple tax exemptions providing room for gaming the system. No doubt, this was the thinking behind imposing regulations prohibiting multiple coverages with HSA, and probably eventually ACA as well. There must be a better way to handle this dilemma than forbidding multiple coverages. Multiple coverages are very apt to be exactly what we will need to encourage. Since living too long and dying too soon are mutually exclusive, consideration should be given to placing tax-deductibility at the time of service, and permitting deductions for the one that actually happens to you. It is thus possible to envision having four or five different coverages, but only one tax deduction. Since the purpose is to spread the risk, we might even go to the extreme of limiting the number of policies that charge premiums, into the one that actually happens to you, but paid out of a common pool. Planners with a more conventional background might well snort at such ideas. Until, of course, they themselves need a life-saving drug costing ten thousand dollars an injection for an extremely rare condition, under a patent which will expire in a year.
So, Let's Get Started with Pilot Experiments in the Willing States. The original idea of modestly improving the original Health Savings Accounts, continues to stand on its own two feet. It's what I would point to right away if you feel unsuited to the Affordable Care Act, or even to ERISA plans. Right now, anybody under 65 (who does not have, or whose spouse does not have) other government health insurance, including Veteran's benefits can enroll in an HSA, and any insurance company can offer a product containing minor variations of the idea, within the limits of the law. A number of Internet sites list sponsors for HSAs. For ease of understanding, we present this idea as if we had two proposals, term and whole life.
Actually, the term-insurance version is the only one which is currently legal, whereas the whole-life variety remains only a proposal. It seems necessary to regard the whole HSA topic as one proposal for immediate use, and a second proposal as a goal for future migration. In fact, almost 12 million people already are subscribers to the term variety, having deposited a total of nearly 23 billion dollars in them. The internet contains brief summaries of their policy variations. At this early stage of development, it is only possible to conjecture that small and sparsely populated states will probably develop more liberal regulations, while bigger and more densely populated states will probably develop bigger and more sophisticated sponsoring organizations. Anyone of the fifty states, however, might someday change its regulations to make itself attractive as a "home state", and at present, it is possible to transfer allegiance.
Unfortunately, current regulations exclude members or dependents of government health insurance programs including veterans' benefits, from depositing new funds in HSAs. It's easy to see why loopholes might allow an individual to get multiple tax exemptions in an unintended way. But loopholes are a two-way street. The early subscribers tend to be younger, averaging about 40 years of age, and probably of better than average health because it would probably require a horizon of two or three years to build up the size of an account to the point where an individual feels adequately protected. That's a result of a $3300 annual contribution limit, and a scarcity of variants of affordable high-deductible catastrophic coverage. This is one instance where "the lower the deductible, the higher the premium" puts the subscriber at risk for the first few years. And that, rather than loophole-seeking, is the reason early adopters are younger, healthier and wealthier; the regulations give them an incentive to be. Let's stop saying, "My way or the highway." If there is a reasonable fear of double tax exemption, the regulation ought to state its real purpose. Otherwise, "Let a hundred flowers bloom", regardless of oriental origins, is a better flag to fly. If a national goal is to get more people to have health insurance, we should be hesitant to impose impediments on it.
Streamline Health Insurance?
Let's review the logic. Mandatory health insurance was considered to be necessary because we wanted Universal health insurance. And we wanted universal insurance in order to extend health insurance to those who had pre-existing conditions. In a sense, we don't have a mandatory insurance problem, we have a pre-existing condition problem. Is there no other way to solve this?
Perhaps, and perhaps not; but let's take up this critical point at the end of the discussion. Right now, it is pretty clear that 10% is a pretty big price for someone else to pay your bills. Most of us would not pay so much to have someone buy our groceries, pay our utility bills, or put quarters into a parking meter for us. We very definitely would not pay such a fee to someone who proposed to do it with a system of three insurance policies (one for 80%, one for 20% copayment, and the third one for Major Medical policies for gaps in our policy coverage). Nor would we compensate a payment agent to pay for coverage which is riddled with cash demands for escalating deductibles and copayments, every time we go to the drugstore, to the accident room, to the doctor's office. Something surely is wrong when we surrender the convenience of third-party payment, pay heavily for this service anyway, and they are hounded and confused by a myriad of partial payment demands, or bewildered by undecipherable itemized bills with an astonishing total at the bottom -- but nevertheless marked "patient responsibility, zero". Something is very definitely wrong when hardly anyone can explain the payment system to us, and no one is willing to quote a price in advance of service. So, let's start by considering what would happen if we eliminated co-payments entirely, and confined deductibles to out-patient services.
In the past, it might have been theorized that prices would go up because patient participation puts a brake on prices. But now we would have to contend with the question, "How would you be able to tell the difference?" The patient in a hospital bed is incapable of haggling about prices, while the hospital is mostly reimbursed in an approximated lump sum, called the DRG (diagnosis-related group). Even those insurances which are reimbursed by items are subject to secret discount systems, which vary from 40% discounts for state Medicaid to overpayments of 30% of costs for private insurance, and up to 400% for payments by list price. This system led one very famous Philadelphia surgeon to growl, "The main purpose of having health insurance is to keep the hospital from fleecing you." The bad public relations of asking the public to endorse this summary would make the problems of changing the system seem minor. For public relations alone, the system must be made more transparent. Most hospital administrators would make the irrelevant response that, after it all shakes out, hospital inpatient care only generates about a 2% profit margin.
That may be true but fails to emphasize that emergency room services generate a 10-15% profit margin, and hospital out-patient and satellite clinics approach 30%. If you drive past a nearby hospital, you are very likely to see a construction crane in operation. But just take a guess in advance at what type of building is being built.
Since hospitals are obviously responding to prevailing profit margins, they would be wise to agree on negotiations with insurers based on audited profit margins, assigning the margin to individual departments to divide up after internal negotiation. For inpatients, a refined object of negotiation with insurers should be an agreement on the variation of reimbursement to be tolerated between insurers for substantially similar inpatients, essentially some variation of Diagnosis Related Groups. A later chapter discusses improvements needed for DRG determination. The central point is: no attempt should be made to bargain prices with a patient who is sick enough to require inpatient hospitalization.
For emergency room services , it is possible to imagine a sort of DRG, and if the patient subsequently requires hospitalization, that should be the ideal approach. However, most emergency patients are not admitted, and there are usually nearby competitors for them. Therefore, some sort of hybrid should be constructed, partly an Emergency DRG, but also modulated by comparison with neighborhood facilities.
For outpatients, competition should rule, and any insurance accommodation should reflect that fact. Ideally, small outpatient services should be cash transactions, but the trend lately is for increasingly expensive procedures to be performed in the outpatient area. The most suitable outpatient payment would be the option of using a Health Savings Account. Optional, because it is desirable to encourage those who are able to protect their HSAs for other uses, to be described in later chapters.
The ambulatory patient is fully capable of loud and insistent bargaining over prices, ultimately threatening to go elsewhere or just to refuse the pay the bill. In the last extremity of disagreement, the provider will be very glad to accept an HSA, so it serves as sort of a distorted re-insurance, and it is useful to have a central reporting mechanism to determine how the market is faring. Since everyone is now entitled to have an HSA, everyone should sign up for one. The uproar over the Electronic Exchanges has demonstrated that almost everyone is coming to the conclusion that high deductibles are desirable. The reasoning is not so self-apparent, but it is nevertheless also true, co/pay is something to be discouraged.
Rollover of Unspent Flexible Spending Accounts
A Change in Direction
For whatever reasons, much of the Affordable Care Act is still shrouded in mystery. After three years, an employer-based system is still predominant, and it remains unclear where a big business wants it to go, or perhaps what makes business reluctant to go ahead. It is even conceivable big business just wants a vacation from healthcare costs, hoping to go back to the old system of supporting the healthcare system by recirculating tax deductions. Once an economic recovery restores profits enough to generate corporate taxes, it will once again be worth saving them by giving away health insurance and taking a tax deduction. Otherwise, it is hard to see what value there is, in a year's respite. Under the circumstances, it begins to seem time to look at some new proposal, neither sponsored by an opposition party nor motivated by antagonism to the Administration initiative. Let's reverse its emphasis, testing how much it is true the financing system now drives the health system, not the other way around.
Both big business and big insurance have been remarkably silent about their goals and wishes for the medical system, while quite obviously agitating for some sort of change by way of government, and quite obviously leaving their own agendas off the visible negotiating table. Let's illuminate the situation, with the medical system speaking out about how employers, insurance, and investment should change while leaving the medical system alone until we better understand the finances which are driving it. The proposed way to go about all this is to harness Health Savings Accounts, with its two different ways of paying for healthcare (cash and insurance), with two-time frames for the public to explore (annual and lifetime), and passive investment of unused premiums versus concealed borrowing. So yes, it's technical, and necessarily it's been simplified. Two important features, multi-year insurance and passive investing, are outlined in this book. But one theme runs throughout: the customers, individually, should have choices. Nothing should be mandatory, everything possible should be left for individual customers to select.
Don't take on too much at once. Health Savings Accounts have grown to over 12 million clients, so it isn't feasible to do more than repair a few loopholes, and let it grow. The next logical step is to get rid of "first-dollar coverage". Not by eliminating insurance, but by making high-deductible the normal standard for health insurance. If we must make something mandatory, it ought to be ensuring big risks before insuring small ones. Catastrophic indemnity insurance is a well-established, known quantity; it's not likely to need pilot studies to avoid crashes. It doesn't need government nurturing; it needs big insurance companies to see the writing on the wall. So let's get along with it, without any mandatory coverage rules. If the old system of employer-based and tax-warped coverage can get its act together, that's fine. Because as I see it, the main danger in Catastrophic coverage is it will penetrate the market too quickly; let people have a level playing field to watch the game unfold. When we have two viable competitive systems, the customers can decide between them, and both will emerge healthier.
An observation seems justified. In a system as large as American healthcare, changes should be piecemeal and flexible; win-win is strongly preferred to zero-sum. Sticking to finance for the moment, we slowly learn to avoid zero-sum approaches, while strongly applauding aggressive competitors. Napoleon conquered Europe, and Genghis Khan conquered Asia by smashing opposition, but it isn't an American taste. Since everyone would prefer saving for when he needs that money for himself, (compared with being taxed to support someone else's healthcare), let's see how far and how fast we can arrange that. The recent extension of life expectancy creates a long period between healthy youth and decrepit old age. About 20% of those born in the lowest quintile of income, will eventually die in the highest quintile. That's a good start, but the process can't go much faster just because someone beats on the table with his shoe.
Nevertheless, a larger proportion of people could save a small amount of money when they are young, and by advantageous investing in a tax-sheltered account, accumulate enough money to support their healthcare costs while old. Some people will never be self-supporting, of course, but the idea is to shrink the size of the dependent population as much as we can. We can at least try it out, on paper so to speak. And if it produces good numbers, perhaps we are ready for pilot projects. That ought to be the next step in our long-term plan to reform the health system without attacking it -- switching from one-year term insurance, to multi-year whole-life insurance. The underlying insurance principle is called "guaranteed re-issue". We aren't ready for that yet, but we are ready to call in the experts in whole-life life insurance and ask for their guidance while setting up information gathering systems to navigate the reefs and shoals. The exercise does seem feasible and is partially explored in the rest of this book. Meanwhile, medical science is steadily reducing the pool of acute illness and lengthening the average longevity. Actuaries are my best friends in the whole world, but I think they are wrong about one prediction. Like retirement planners, both professions assume future taxes and future health costs are going to go up. But I am willing to predict, net of inflation, they will go down as longevity increases. Just wait until you see an enthusiastic medical profession attack the problem of chronic care costs. The nature of retirement living must change. Both things will change because of changes in the nature of investing and finance, the lowering of transaction costs, and the effect it has on the economy. Because: investing is based on perceptions, and a general disappearance of the acute disease will certainly re-direct perceptions of what is important.
Over thirty years have elapsed since John McClaughry and I met in the Executive Office Building in Washington, but a search for ways to strengthen personal savings for health marches on, trying to avoid temptations to shift taxes to our grandchildren, or make money out of innocent neighbors. Most of the financial novelties to achieve better income return originated with financial innovators and the insurance industry. But the central engine of advance has come from medical scientists, who reduced the cost of diseases by eliminating some darned disease or another, greatly increasing the earning power of compound interest -- by lengthening the life span. My friends warn me it must yet be shown we have lengthened life enough or reduced the disease burden, enough. That's surely true, but I feel we are close enough to justify giving it a shot. Before debt gets any bigger, that is, and class antagonisms get any worse.
While Health Savings Accounts continue to seem superior to the Obama proposals, there is room for other ideas. For example, the ERISA (Employee Retirement Income Security Act of 1974) had been years in the making but eventually came out pretty well. In spite of misgivings, ERISA got along with the Constitution. And we had the Supreme Court's assurance the Constitution is not a suicide pact. So, still grumbling about the way the Affordable Care Act was enacted, I eventually stopped waiting to describe an alternative. The long-ago strategy devised in ERISA, by the way, turned out to be fundamentally sound. The law was hundreds of pages long, but its premise was simple and strong. It was to establish pensions and healthcare plans as freestanding corporations, more or less independent of the employer who started and paid for them. Having got the central idea right, almost everything else fell into place. Perhaps something like that can emerge from Obamacare, but its clock is running out.
HSA Lifetime Payments: Limits of Feasibility
The two traditional ways to pay for healthcare are paying directly with cash, or paying indirectly with insurance. Each has advantages, and we return to them later. This book proposes a third payment method which ought to be cheaper, while medical care itself ought to be unaffected. The payment idea grows out of a quirk of modern health care: Children up to age 20 consume only 8% of current medical costs; 92% of healthcare expenses arise decades later. Most families of young people could save up money during the long low-expense period, adding extra compound interest to use later. If this approach reduces overall costs, some of the saving could be used to subsidize the poor. No one doubts some extra interest could be gathered. The really critical question then sharpens: Is it enough to be worth the trouble?
The calculation is not an easy one. In the past century, the nature and cost of healthcare changed dramatically and will change more in the future. Nevertheless, attempts are often made to estimate national health costs; lifetime costs are now widely accepted to range around $350,000 per person, in the year 2000 dollars. Women cost about $50,000 more than men. That's partly a result of the statistical convention of attributing all costs of pregnancy to the mother, and it also reflects females living longer than males. These are daunting amounts of money, but at least we can estimate some upper limit to costs from them. At the other boundary, we know some interest could be earned on almost any balance. So the problem has a solution. The real feasibility issue is whether it produces enough savings to be worth the trouble.
The ability to save varies considerably between families, interest rates vary, longevity increases; no one can know precisely what health care will cost when newborns of today live to be a hundred. On the other hand, estimating national totals is often easier. Dividing national data by the size of the population generates individual averages, which are more natural to comprehend. Furthermore, sometimes we know the available revenue but not the costs. It seems a little cynical to say so, but since one limits the other, they are often (roughly) interchangeable. The rest is a little speculative, and sometimes you just have to make an educated guess.
What a hypothetical average person could afford to pay is one of those speculative matters, and what the average person would willingly pay is even harder to guess. But there are limits to reasonableness; some boundaries can be recognized. So, let's now test what the plausible limits might be, starting with a range of interest rates. As a further preliminary, present longevity is to age 83, and one plausible guess about where it might go next century is age 93. The limit to what almost everyone could afford for a newborn child is guessed to be $500; it seems to be a bargain the government would readily accept as a subsidy to the poor, in order to cover a $350,000 expense. Table # 1 displays the first stab at an estimate. It leads to a conclusion: the proposal of pre-funding health care seems feasible enough under certain circumstances, to justify further investigation.
Interest Return According to Roger Ibbotson, the acknowledged authority on investment statistics, inflation has closely approximated 3% per year for the past century. United States stock market assets have appreciated in a range from 10% (large-cap stocks) to 12.7% (for small-caps) for a century. Growth stocks and value stocks have followed different cycles, but over a span of a century have generated almost identical returns. This table makes the hypothetical assumption that average parents already contribute as much as they can at the birth of their child, and all further additions to the child's fund our investment income. Can the cost of a lifetime of health care be supported by a $500 contribution at birth? Under certain imagined circumstances, the answer seems to be a tentative "Yes" -- if the fund can be invested at 7 to 8%, or the average longevity is between 83 and 93 years. Although it may take a little explanation, these do not seem like unreasonable expectations. It might, therefore, be said that if there are no interruptions or withdrawals (a totally unreasonable expectation by the way), the presently expected cost of an average lifetime of healthcare could be accumulated from the investment of $500 at birth. With no further expenditures than the original $500, although it may be a little too early in the discussion for a skeptical reader to accept that. How about this for an alternative: Although the devil is most assuredly in the details, the goal of paying for a substantial amount of healthcare in this way, is at least conceivable.
Having said that, it should also be firmly stated that paying for all of healthcare costs this way, is neither necessary nor probably even desirable. In the first place, when you make things totally free, they lose their perceived value in the eyes of the recipient. He treats the gift as worthless and is induced to spend money even more carelessly than he does with insurance. Secondly, by placing a cap on the upper bound, we adopt indemnity principles of shifting the risk to the person in control of them. It thus removes the temptation to favor inflation as a way of escaping from debts. Third, the explanation acquires specific numbers to replace vague promises. So, let's set the far more realistic goal of paying for half of it, and seeing if that seems even more feasible by using somewhat reduced limits.
The achievement of $175,000 cannot be made by simply cutting one of the ingredients in half, because that reduces his balance(and its resultant later income) by half, also. The result is the recipient soon gets into a downward spiral, just as the miraculously enhanced income sent his spiraling balance upward. We develop a family of curves (figures 2a to 2d) for different contribution levels in the next chapter, but must first digress to meet an unexpected development There's a sweet spot, and we are already close to it. To test this point, we have some very rough estimates from the AHRQ (the Agency for Healthcare Research and Quality) of the distribution of average health costs by age. If we subtract these costs from the data already mentioned, we would choose 8% as the most likely income, and age 88 as the most likely average longevity. The results are seen in Graph #1 and summarized in Table #2. To assist in the verification, the AHRQ data show that 8% of costs are in the age group 0-20; 13% in age 21-39; 31% in the age group 40-64; and 49% are over 65. The preliminary results are seen in Figure 1a.
Whoops! It is immediately obvious our preliminary description has forgotten something important. We will correct the graph in a minute, but first, we must explain something about paying for healthcare. All of the revenue for healthcare must be generated during the working years of, roughly, 18 to 66 years of age. Ignoring a few trust-fund exceptions, the costs of childbirth, neonatal costs, and childhood are currently borne by the parents of a child. To some extent, the fall-back costs of the grandparents are also covered by people in the working age group. To go even further, when the government pays for dependent healthcare, this too is covered by taxes, which are generated by working people. To summarize, no matter what the direct source, ultimately all healthcare costs are derived from working-age earnings.
In table 1b, we remove the 8% of health costs generated by children, as well as the $44 in revenue which is their portion of the $500 seed money, and redraw the graph; we move the beginning of the revenue curve to the time of birth, gaining three doublings of revenue. The anomalous excess of costs over revenues is reduced but not eliminated. The expected surplus appears as promised, but at the end of life, where it becomes considerably enhanced. The general financial idea is vindicated, but what of the children? Their costs are incorporated into an independent Health Savings Account. The legitimacy of doing so, and the financial consequences, are discussed in the following section. For the present, we can see from Figure 3a. that this approach helps but does not entirely reconcile the financing.
The revenue for that account is introduced at age 35 when health costs are predictably low, and ownership is transferred from the parents to the child. That is, we recognize the validity of such a transfer of responsibility, but during the transition from one system to the next, must yield to the requirements of transition. Because of the overlaps, it may well be desirable to keep the two funds separate for quite a long time. It would seem premature to anticipate dynamic effects on the culture of marriage, divorce, and multiple family health insurance plans, and let the consolidation of accounts remain optional until much later in the unfolding of this scheme. Figure 1b illustrates the effect of consolidating accounts in figure 5c, and considerable experience with this issue probably exists within the life insurance industry. A reverse case can even be made for splitting the account into smaller age subgroups by logical age groups, as a way of easing the entanglements which people get themselves into.
18 Blogs
CHAPTER ONE: Re-Examining the Revenue Premises of Medicare
New blog 2015-01-05 21:38:20 description
Children, 0-26
Everyone agrees there is a tangle of rights and responsibilities about the beginning of childhood.
First Two, and Last Two, Years of Life
Medically speaking, the four most eventful years of almost anybody's life.
CHAPTER TWO: Fitting Employer-Based Health Insurance Into an Individual-based Framework
New blog 2015-01-06 22:24:59 description
Corporation Tax Deductions Support Our Health System.
If you eliminate a tax, you also eliminate tax deductions from it.
Good Ol' Health Savings Accounts
Possible fixes in health savings account to adjust to Obamacare. HSAs remain available and have millions of pleased subscribers. A debit card pays (tax deductible) medical expenses, and does the book keeping. High-deductible health insurance is also required, mostly to cover hospitalizations, but primarily to smooth out the unevenness of disease. Bronze plan is the cheapest Obamacare option, but private catastrophic coverage would be cheaper.
Spending Rules--Same Purpose As Escrow Accounts
Invisibly, a corporate spending rule is a way to increase the size of the reserve fund.
Health Competitors for Windfall Money
New blog 2015-01-27 20:27:09 description
Half-Started HSAs
If you create a mandatory high deductible, you must create a way to pay for it.
Direct Premium Payments, Constitutional Issues
 New blog 2014-01-02 19:15:22 description
New blog 2014-01-02 19:15:22 description
Lifetime HSA and Whole Life Insurance: A Basic Difference
Lifetime Health Savings Accounts resemble whole-life insurance, but there are significant differences.
Some Ruminations About the Far Future.
Streamline Health Insurance?
Maybe the simplification of health insurance selection could save appreciable amounts of money, but it looks as though it might create too much uproar
to do it all at once. Compared with this, perhaps we should review the imagined advantages of one-size fits all.
Rollover of Unspent Flexible Spending Accounts
Flex Spending is use-it-or-lose-it. Employer-based insurance, only. So, wasteful things are bought at year-end. It made some sense when it was the employer's money. But now FSAs surplus is mostly the employees own money, the option to roll-over, as in Health Savings Accounts, seems only fair.
A Change in Direction
Health Savings Accounts take a new direction, adds some features borrowed from other professions, and sets sail.
HSA Lifetime Payments: Limits of Feasibility
New blog 2015-02-12 18:46:07 description