Related Topics
Science
Science
Old Age, Re-designed
A grumpy analysis of future trends from a member of the Grumpy Generation.
Whither Alzheimer?
|
| Dr. John Q. Trojanowski |
The Right Angle Club was recently treated to a sophisticated movie and a polished presentation by Dr. John Q. Trojanowski, Professor of Geriatric Medicine at the University of Pennsylvania. Among other posts, he holds the Truman G. Schnabel, Jr. Chair, which particularly endears him to me since Nipper Schnabel was an old friend. Dr. Trojanowski has kindly given permission to use his slides on Alzheimer's Disease.

|
| Dr. Alois Alzheimer |
When Dr. Alzheimer published his description of the disease which bears his name, in 1906, it was treated as a rather esoteric or even insignificant accomplishment. The average life expectancy at that time was age 47, so although some people did live to an advanced age, most people didn't. A newly-identified disease which crippled and shortened the lives of old folks was pretty well brushed aside. Doctors were too busy treating tuberculosis, rheumatic fever, syphilis and typhoid fever -- diseases which were part of ordinary practice. As things turn out, however, life expectancy nearly doubled in the ensuing century, so both the number of old folks has vastly increased, and they are dying even later, disproportionately increasing the prevalence of Alzheimer's disease, to the point where it is now the sixth most common cause of death. At present, nearly half of people who achieve the age of 65 will eventually develop Alzheimer's, and most of them will die of it. It's a protracted fatal disease, requiring a great deal of expensive care. One rough rule of thumb is that when patients reach the point of being unable to recognize the spouse or nearest relative, they will probably still live another two years.
With conventional nursing care, utilizing home nursing aides, it will likely cost more than $50,000 to take care of any patient during a perfectly dreadful terminal experience. One of the more imaginative ideas for relieving this financial burden has been to store up credits for volunteer work as nursing assistants after retirement, but before infirmity, say between 65 and 85. Those credits could then be used later to pay for the care of that same volunteer when he or she becomes incapacitated. The tax authorities have been unsympathetic, however, fearing any system of barter undermines the income tax mechanism. Since there presently is a huge pool of unused labor in the early years after retirement, this idea should be revived, and at least given a trial as a pilot experiment.
Experience with trying to treat this growing epidemic brings out features which somewhat seem to support the idea of "intellectual reserves". Educated and intellectually active people tend to develop the condition less frequently, or at least later in life; aboriginal cultures develop the condition much younger than advanced ones, head injuries and sports which promote them provably increase the prevalence. It looks as though persons with greater educational attainments have some kind of reserve capacity to be used up before the disease finally overtakes them. And strange things happen; the incidence on the island of Guam is now only a tiny fraction of what it was a century ago. Unfortunately, all of these anecdotal experiences contain the chance that it is actually the early onset of the disease which lessens social skills, rather than the other way around. Unfortunately, exercise does not seem to improve cognitive functioning, although it improves other functions.
|
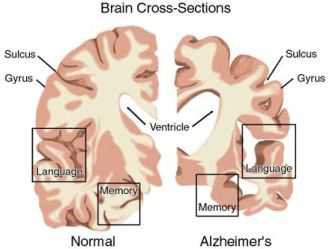
| What is Alzheimer's |
Naturally, there is a great hope for scientific improvement in the treatment of this condition. After all, the percentage of persons over the age of 80 who are disabled from any condition is only half of what it was in 1982. However, the most discouraging feature of Alzheimer's dementia is that it is a degenerative disease. The estimate is made that when the first symptom of Parkinsonism appears, roughly 40% of the substantia nigra has already been destroyed. That sort of observation leads to the very discouraging possibility that a new treatment for the condition, even one that is completely effective, may never do any patient's symptoms any good. At least, research workers in the field may have to give up the approach of treating patients to see if they get better because the damage has already been done. Very likely, vast numbers of apparently normal persons may have to be treated for years, in order to see whether the disease is eventually delayed in its onset. That's quite different from defining the value of a drug for pneumonia, where all you have to do is treat a hundred patients to see if it works. Delaying the onset of this disease would be no small achievement, however, because of the average age of the patients. A delay of five years in the onset would reduce the overall quantity of impaired persons by 50%. So, an effective drug for Alzheimer's would be enormously valuable, but it would be far more expensive to determine potential delays in onset, the potential toxicity of years of preventive therapy would be greater, and the public disappointment on behalf of existing patients would be something to deal with. All of these discouragements tend to inhibit drug manufacturers from spending vast sums to develop a treatment, particularly in an era where cost concerns are prominent. But we all better get used to it: delaying the onset of degenerative diseases is likely to be more expensive, and much more difficult to prove, than the medical miracles of say infectious disease we have grown accustomed to looking for.
Originally published: Friday, July 09, 2010; most-recently modified: Sunday, July 21, 2019