1 Volumes
Handbook for Health Savings Accounts
New volume 2015-07-07 23:31:01 description
FUTURE VERSIONS
Some ruminations about health financing, written while we wait for the Supreme Court to announce its decision on King v.Burwell.
Waiting for Roberts
It seemed foolish to publish a book on healthcare financing, just on the eve of the United States Supreme Court announcement of what it had decided about Obamacare. Why not wait a little? So I got ready for the announcement by writing half a book and imagining several potential endings. At the end of this section, I plan to add a comment about what the Court did decide, which may be a long or short commentary, depending.
First, let me summarize the book up to this point. The Health Savings Account has had thirty years to ripen and mature, and it could be described as moderate success in supplementing the existing system of employer-dominated health care. HSA saves money for most subscribers, and even makes money for a few people who are shrewd about finances.
When President Obama hammered the Affordable Care Act past a reluctant Congress in 2008, the Health Savings Account developed a new mission. It had been originally devised as an alternative to a tired old system of employer-based health insurance. With Obamacare as a new issue, it got contrasted with a new and untried system, whose direction and purpose had been left quite unclear. With dozens of flaws, the employer-based system had created a great need for reforms, but the Affordable Care Act addressed almost none of them, and it was uncertain whether it ever would. In my view, the purpose of the ACA was to seize control of the finances, after which the President would be able to reform whatever he pleased. First, defeat the enemy, and then announce what your plans are.
That left me with a quandary. I strongly believe in reform, but I strongly resist a blank check. So I decided to write down my views on Health Savings Accounts, in case the public wanted to make use of them during the period when -- by default -- we continued to operate under the old employer-based system. That was particularly vexing, because employers seemed to be the strongest opponents of the new system, and delayed its implementation by at least two years. My strongest opinion was, the public didn't seem to understand how good Health Savings Accounts were, because their best features are latent, hidden within what seem like simple ideas. Their advantages begin to emerge when you encounter difficulties with alternatives. With HSA, almost every problem you encounter seems to uncover a ready-made solution, whereas a flawed concept usually leads to more problems every time you try to fix something.
But now we have reached a point where it is natural to ask how much further we could take Health Savings Accounts. For that, we need an organizing theme. The most natural theme is that Americans would really like to give outstanding medical care to everyone, with perhaps a few points of hesitation. We are not sure the nation can afford to give the style of care we admire, to everyone. Since the employer-based system was mainly criticized for being so costly, and since what we could see of Obamacare was going to be even more expensive, it looked like the end. There seemed a significant danger that making things better for the poor would be paid for by making them worse for the rest of us. By speaking to community groups I had the feeling that elderly people, women, in particular, are not so much in love with Medicare, as fearful it will be stripped to pay for Obamacare. All fifty states have Medicaid programs for the indigent, and all fifty of them are under-funded. That raises the question of how genuinely the public wants to give good care to the poor. There's one exception, however; rich folks, the top one percent, do seem to have a genuine wish to help the poor, no matter how populists denounce them. The rest of the country is often perilously close to competing with poor people and is therefore uneasy about being upended by a leader who wants to spend their money helping the competition. There's a lot of churning between the classes in America; in Thomas J. Stanley's The Millionaire Next Door we read that most millionaires in this country made the leap upward in a single generation.
There's another obstacle to expensive universal care, which the public recognizes only dimly. The whole medical system is already riddled with cost-shifting, at every level. The family unit cross-shifts within family insurance plans. Surgeons support the "feeders" with cross-shifted hospital costs. The rich in private rooms are charged more than the middle-class in semiprivate rooms, for the same care. The doctors in blue-stocking districts pay for medical society services of free-loading doctors in poor neighborhoods. Every conceivable cost-shifting strategy has been used up to smooth out cost differences and for hardly any other reason.
Grandpa Gives a Gift to Grandchildren. But one vehicle for cost-shifting hasn't been analyzed very well. Almost all money in the medical system ultimately depends on a single age group, from age 21 to 66. Parents almost always pay for their children, and the elderly plan to fall back on their working children if resources run low, although they hope not to. To a limited extent, the pricing of health insurance premiums shifts money around, but holds back uneasily, when it comes to shifting between family units. The Scandanavians regard whole language groups as "family" to a much greater degree than we do, explaining most of their different attitude about nationalizing health costs. Through most of these schemes runs the idea of taxing the necessary money into a government pool, and then redistributing it to the worthy poor. The resistance to this approach mostly concentrates on the political step in the middle, easily denounced but leaving true public attitudes unclear. A more serious concern would be the cost of an extra layer of administration, but most substitutes just seem to add one of their own.
So it seemed only natural to ask whether some of the unused surplus generated by the conservative elderly might be used to fund the costs of having grandchildren. Perhaps a grandchild would be better accepted than a stranger. Some resistance comes from misjudging longevity, but most of it is an underestimation of the way earnings accelerate during late-stage interest compounding. True, it might take eighty years to break even with generational transfer, but even that could be turned to the advantage of eight doublings @ 7%. Since we are dealing with paying childhood costs in the range of 10% of $350,000, the investment of one dollar (doubled eight successive times) should pay for it all in eighty years, and it really doesn't have to pay for all of it, in order to be a big deal. A variation of this line of musing follows shortly, but it isn't an easy concept and must be studied to be understood.
Buying Out of Medicare. The other group who paradoxically often need the support of some sort of cost-shifting, are the elderly, among whom the variation in wealth is wide. It might appear otherwise because Lyndon Johnson took care of them with Medicare. Except he really didn't. The Medicare budget, according to its own reports, is supported in quarters: one quarter from payroll deductions from young workers, one quarter in premiums from the elderly themselves, and two quarters from general taxpayer funds, because it's a subsidized deficit. In this case, the "general taxpayer funds" are the pool, currently replenished by foreign borrowing, mostly from the Chinese. The voting public is shielded from this deficit at the moment, but this program is destined to suffer badly unless something is done. Politicians may tell you that tinkering with Medicare is the third rail of politics (touch it and you're dead), but alternatives would plainly be welcome. It is difficult for an average layman to obtain reliable data on government operations, and they are indeed quite bulky. Therefore, the amount of accumulated foreign debt attributable to Medicare is unclear, as is the yearly or current state of it. Nevertheless, the Medicare program might well be a bigger problem than Obamacare; it is certainly quite large. Putting a stop to further borrowing, not to mention paying off previous years' debt, would be a major achievement. Unacknowledged perhaps, but particularly welcome to elected politicians.
Someone just has to make the suggestion of making it possible for some people to buy their way out of the Medicare program. Don't gasp. Depending on what age was made eligible, and depending on the effective interest rate the HSA was able to earn, there are ways it might be possible to do it and save appreciable money. The ultimate goal would be to make the program self-sustaining, and to shift its costs from those in retirement to those still in the 21-66 age group, (plus the interest income on the residual buy-out fund during retirement). No group likes to have costs shifted to it, but as we mentioned, all revenue ultimately derives from the working age group. Aligning costs and revenue almost always clarifies and, for the most part, reduces the cost of any program, by reducing "moral hazard". For an idea like this, it makes it simpler to assume the HSA fund was earning income from birth to death at age 93. Some of this is double-counting because it is uncertain whether the future is a sole new program or if it is part of a cradle-to-grave project. It might start out as one, and evolve into the other. As a quick guess, either one might become feasible with the assumption that a voluntary program would have a gradual rather than abrupt rise in costs.
Other assumptions are: an average investment income of 5% net, for 93 years of life, and a steady inflation rate of 3%. We accept a lifetime medical cost of $350,000 and that Medicare will continue to be half of it. Let's take it in two steps. In order to cover a cost of $175,000 from age 66 to 93, an individual account with a net income of 5% must achieve a $90,000 escrowed balance by age 66. And, in order to have a balance of $90,000 at age 66, the individual must start with a "gift" of $4000 at birth. That is to say, an individual can buy his way out of Medicare for a single payment of $4000 at birth. That's not the exact story, but it establishes the framework.
The calculation assumes an individual will still pay half his costs, (one quarter as payroll deductions, and one quarter as premiums). Including the interest on these sums, the single-premium cost of buyout at birth would be reduced to either $3000 or $2000. Remember, the Government stops going deeper into debt, but the outstanding debt is unchanged. Let's call that a wash because a good deal is a good deal for everyone involved. Yes, the Government is losing the tax income from the individual's HSA tax deduction, but on the other hand, it doesn't have to keep paying so many administrators in Baltimore, on Social Security Boulevard.
Lifecycle Health Savings Accounts. So there's a plan for children, and another for the elderly. They consist of a Medicare buy-out, and an inheritance. Some of the latter derives from unused balances after the buy-out. For working people, there remain employer-sponsored plans, Obamacare, and Health Savings Accounts. Everybody's covered by one of these five variations, somehow. But let's explore going further in the opposite direction, by having a unified plan, cradle to grave. The superiority of one big unified plan over three smaller ones has yet to be demonstrated, and I would personally challenge anyone to defend taking such giant steps for no particularly good reason. That is, the default position is to reduce or eliminate cost-shifting, rather than add to it.
The final step would be to develop Lifecycle Health Savings Accounts, combining the gift from Grandpa, the Medicare buyout, and Health Savings Accounts -- all under one big tent. Some of that has been explored in a separate section, but what hasn't been defended is the advantage of doing it all at once, instead of step by step. As long as we are talking Blue Sky, let's explore the advantages and disadvantages of a unified Whole-life Insurance Company which even absorbed the functions of the Health Savings Account, internally, with a guaranteed rate of return. A century ago, some major companies devised this arrangement for life insurance, and I would advise talking to such companies to learn what they think of it. In short, you pay a regular premium, the company invests the premiums and waits for you to die. This proposal would then substitute a Health Savings Account for the death benefit, but why not, let's include that, too. In Sherman antitrust terms, that's called vertical integration, but vertical integration has now been deemed appropriate in the State Oil v. Kahn case. You'd probably find yourself in a tangle of state insurance regulations, administered by people untrained in all the added skills, but let's just say we found a reason to overcome such obstacles. Essentially, this proposal would be to transfer a group of quarreling government agencies from the public sector to the private one, using income guarantees instead of passive investing. The experience might resemble watching a train wreck, but perhaps it would demonstrate some overall advantages for the combination of conservative investors and adventuresome insurers.
Without stating a preference, that seems to be the range of possibilities.
Better, but More Complicated: Lifetime HSAs
Health Savings Accounts are a big improvement over traditional health insurance, and this book stands behind them -- as is, without major adjustments. Go ahead and get one right now, regardless of what other coverage you have. Let me repeat: Their secret "economy" lies in keeping everyone spending insurance money as carefully as he would spend his own -- but not being too dictatorial about it. No one washes a rental car, as the saying goes, so you can't act as if someone has committed a crime, just because he doesn't do everything for you. But just you let the individual keep what he saves, and millions of HSA owners will find ways by themselves to save up to 30% of traditional healthcare costs. HSAs provide an incentive for the medical consumer to shop more carefully, and consumers seem to respond. The difficulty is, some people are too sick to worry about rules. So, substitute a catastrophic high deductible for your present coverage if the law lets you do it (which is presently uncertain) but go ahead with a Health Savings Account and add to it when you can.
 Looking ahead to what might follow HSA, is one of the main reasons for doing it. 
|
One further simple idea: costs not prices. We have all assumed that catastrophic coverage is basic. If everybody ought to have something, he ought to have a very high deductible for a bare-bones indemnity policy. But just consider an addition: insurance for the health costs of the first year of life, plus the last year of life. That's technically simple to do retrospectively, although it takes most people a few moments to get it. And 100% of the population would receive both benefits, at a restrained cost by remaining uncertain just what the last year of life is until it is too late to run up its cost. Indeed, transition costs would be minimized by eliminating the historical part of costs for the transitioning population and phasing in the ongoing expense. Ask your friendly actuary; he'll get it, immediately.
Revised DRG coding and Methodology. Either way, if you guarantee to provide something for everyone, you better have a plan for controlling its boundaries. Inpatient costs affect patients too sick to argue about price, so hospital bed patients might as well be presented with some different options. They are more or less suitable for the DRG approach, but we have gone to some length to show what's wrong with the DRG coding methodology. The coding, among other things, must be fundamentally modified. As informed doctors will tell you, ICDA-11 isn't it.
DRGs ("Diagnosis Related Groups") is something Medicare started, which with more precise coding could be made ideal for the catastrophic insurance part of Health Savings Accounts. Medicare now contributes half of average hospital revenue, so its rules effectively dictate most other methods of hospital reimbursement. There are many problems with Medicare, but paradoxically, escalating inpatient cost is not one of them. Inpatient billing has been so muddled, most people do not realize that DRG has been a somewhat overly-effective rationing device. Like all rationing schemes, it causes shortages, as inpatient care is shifted toward the outpatient area. Office and hospital outpatient costs are quite another matter, so the whole hospital accounting system has been turned on its ear. In particular, components of inpatient costs must be re-linked to identical outpatient charges, in the instances where they are really market-based. Then, a system of relative values needs to be applied to that base. For that, we will need a Google-like search engine for translating the doctor's exact words into more precise code.
|
Single payer is not a solution, it is pouring gasoline on the flames.
|
Furthermore, both catastrophic insurance and last year of life insurance are more similar than they sound. What most people don't appreciate is the risk of a catastrophic health cost is rather remote in any given year. But in a whole lifetime, it is almost certain to happen at least once, which is often the last year of life. When you consider an entire lifetime, you cannot delude yourself it won't happen. Someone must plan for it, and the books must roughly balance.
Add Many Years to Lifetime Compound Income. Mathematically, it is fairly easy to show that healthcare costs will go down at the end of life; it's cheaper at 95 than at age 85. But that's probably a trick. We don't know what diseases will terminate life a century from now, so we can't count them. They are not cheaper, they are just unknown, and so we record the cost of the survivors of the race of life, not the average runner who will take time to catch up. If we are looking for lifetime healthcare revenue, recognize that practically all revenue is now generated by members of the working-age 21-66. A lifetime system needs to extend its revenue even further to other lifetime age groups. It seems only right that everyone's longevity should be included, but laws may currently block the way.
It would help a lot to include the first 21 years, adding several doubling-time periods. It would also be useful to let HSAs run for a full lifetime instead of mandatory rolling-over to IRAs at 66. Obviously, the idea behind terminating at age 66, was that Medicare would take care of everyone's medical needs. But with time, Medicare has consistently run big deficits, to the point where it is 50% subsidized by competition with other federal funds, or by international borrowing. Adding forty years would multiply extra investment returns by four doublings at 6%, and at little cost to the government. This would be particularly useful during the transition, when many people start their Accounts at zero balance, but at a more advanced age. It would be a significant improvement to all these programs to end them with at least one optional alternative; terminating a health program at a fixed age is something to avoid.
Proposal 13: Health Savings accounts should include the option to be individual rather than family-oriented, and therefore should include an option to extend from the cradle to the grave, rather than age 21-66, as at present, and consider options for Medicare buy-out and transfers within families between accounts.Permit Tax-free Inheritances of Funds Sufficient to Fund One Child's Healthcare to Age 21. In other words, we should make some sort of beginning to the knotty difficulty of making The State responsible for what used to be the family's responsibility. A second adjustment would recognize that essentially all children are dependent on their parents for healthcare support until they themselves start to work. Children's health costs are relatively modest, except for costs associated with the first year of life, and the bulge would be even greater if insurance shared obstetrical costs better between mother and infant. Even as we now calculate it, the baby's health costs, from birth to age 21, are 8% of lifetime costs. A cost of 3% for the first year of life alone, makes lifetime investment revenue essentially impossible for many young families to support lifetime costs because any balance would start from such a depleted level. So, the idea occurs that a considerable surplus appears when many people become older if grandpa could effectively roll over enough of his surplus to one grandchild or designee. The average American woman has 2.1 children, so it comes close to a 1:1 ratio of children to grandparents. Young parents often have a big problem financing children, whereas in a funded system, the transfer from grandparents could be supported by a fraction of it, by application of compound interest.
With two statutory adjustments along these lines, financing of lifetime healthcare by its investment revenue becomes considerably easier.
Whole-life Health Savings Accounts. (WL-HSA) It has developed in my mind that Lifetime Health Insurance would become even better for cost savings, with the addition of one more feature, copied from life insurance, and combined with the needed DRG revision. It is, broadly, the difference between one-year term life insurance, and whole-life insurance, which offers lifetime coverage as a variant of multi-year coverage. Life insurance agents frequently argue that whole-life is much cheaper in the long run than term life insurance. What they may not tell you is that most of the apparent profitability of term insurance derives from so many people dropping their policies without collecting any benefits at all. Comparing apples with apples, whole-life insurance is not just cheaper, but vastly cheaper.
For those who don't understand, one-year term insurance covers illnesses for a single year and then is open for renegotiation. By contrast, a whole life policy covers a lifetime of risk, overcharging young people for it in a certain sense, meanwhile investing the unused part for later years when health risks are greater. Does that start to sound familiar? The client is seemingly overcharged at first, but in the long run, his life insurance cost is far cheaper. Not just a little cheaper, but just a fraction of what a chain of yearly prices would cost.
It doesn't mean you must enroll at birth and remain insured until death; it means any multi-year insurance becomes cheaper, depending on the age you begin and the age you cash out -- often at death but not necessarily. What makes the saving so astonishing is the way life expectancy has lengthened. We have been so uneasy about rising medical costs we didn't much notice that people were living thirty years longer than in 1900. As a rule of thumb money earning 7% will double in ten years; in thirty years, it becomes eight times as big. If you lose half of it in a stock market crash, you still end up with four times as much. This is what would be new about lifetime accounts, and it can be easily shown that overall savings for everyone would be more than anyone is likely to guess.
Let me interject an answer before the question is asked. Why can't the government do the same thing? And the answer is, maybe they could, except two hundred years of history have shown the American public is extremely averse to letting anyone be both a player and an umpire. For more than a century at first, there was a strong political suspicion of the government running a bank, or even borrowing money with bond issues. Yes, the government could invest in businesses, but we would then be guaranteed a century of rebellion if we tried to have the government do, what any citizen is free to do on his own. Indeed, a review of Latin American history shows what disaster we have avoided by retaining this negative instinct to allowing the camel's nose under the tent. The separation of church and state is a similar example of how our success as a nation has been based on gut feelings. The separation of business and state is at least as fundamental as separating church and state. And for the same reason: we instinctively avoid having the umpire play on one of the teams.
Proposal 14: Congress should authorize a new, lifetime, version of Health Savings Accounts, which includes annual rollover of accounts from any age, from cradle to grave, and conversion to an IRA at optional termination. Investments in this account are subject to special rules, designed to produce a maximum safe passive total return, and limiting administrative overhead to a reasonable, competitive, amount. The account should be linked to a high-deductible catastrophic health insurance policy, with permanently guaranteed renewal, transferable at the client's annual option. The option should also be considered of linking the HSA to a policy for retrospective coverage of the first year of life and last year of life, combined. These two years are disproportionately expensive, and they affect 100% of the population. Subtracting their costs from catastrophic coverage should greatly reduce catastrophic premiums.
Lifetime Health Savings Accounts (L-HSA) would differ from ordinary C-HSA in two major ways, and the first is obvious from the name. In addition to meeting each medical cost as it comes along, or at most managing each year's health costs, the lifetime Health Savings Account would try to project whole lifetimes of medical costs and make much greater use of compound income on long-term invested reserves. The concept seeks new ways to finance the whole bundle more efficiently, and one of them is health expenses are increasingly crowded toward the end of life, preceded by many years of good health, which build up individually unused reserves and earn income on them. Since the expanded proposal requires major legislation to make it work, it must be presented here in concept form only, for Congress to think about and possibly modify extensively. This proposal does not claim to be ready for immediate implementation. It is presented here to promote the necessary legal (and attitudinal) changes first needed to implement its value. And frankly, a change this large in 18% of GDP is better phased in gradually, starting with those who are adventurous. By the time the timidest among us have joined up, the transition will have become routine. As a first step, let's add another proposal for the present Congress to consider:
Proposal 15. Tax-exempt Hospitals Should be Required to Accept the DRG method of payment for inpatients from any Insurer, although the age-adjusted rates should be negotiable based on a percentage surcharge to Medicare rates. The DRG should be gradually restructured, using a reduced SNOMED code instead of enlarged ICDA code, and intended to be used as a search engine on hospital computers rather than printed look-up books, except for very common hospital diagnoses. Also to be considered for those who are too sick for arms-length negotiation of hospital costs, are uniform reimbursements among insurance carriers and individuals, and between inpatients and outpatients, including emergency rooms, as well as a major expansion of specificity in DRGs.Overfunding and Pooling. Lifetime Health Savings Accounts, besides being multi-year rather than annual, are unique in a second way : they overfund their goal at first, counting on mid-course correctionsto whittle down toward the somewhat secondary goal of precision -- amounting to, "spending your last dime, on the last day of your life". To avoid surprising people with a funding shortfall after they retire, we encourage deliberate over-estimates, to be cut down later and any surplus eventually added to retirement income . For the same reason, it is important to have attractive ways for subscribers to spend surpluses, to blunt suspicions the surpluses might be confiscated if allowed to grow. An acknowledged goal of ending with more money than you need runs somewhat against public instincts and is only feasible if surpluses can be converted to pleasing alternatives.
Saving for yourself within individual accounts is more tolerable than saving for impersonal groups within pooled insurance categories, but probably must constantly defend itself against the administrative urge to pool. Pooling should only be permitted as a patient option, which creates an incentive to pay higher dividends for it. The menace of rising health cost at the end of life induces more tolerance of pooling in older people, whereas small early contributions compound more visibly if pooling is delayed. Young people must learn it gets cheaper if you don't spend it too soon. The overall design of Lifetime HSAs is to save more than seems needed, but provide generous alternative spending options, particularly the advantage of pooling later in life. Because it may be difficult to distinguish whether underfunded accounts were caused by bad luck or improvidence, the ability to "buy in" to a series of single-premium steps should both create penalties for tardy payment, as well as create incentive rewards for pooling them. This point should become clear after a few examples.
Smoothing Out the Curve.There is a considerable difference between individual bad luck with health costs and systematic mismatches between average costs of different age groups. Let's explain. An individual can have a bad auto accident and run up big bills; as much as possible, his age group should smooth out health costs by pooling within the age cohort to pay the bill. On the other hand, compound investment income sometimes favors one age group, while illnesses predominate in a different experience for another. It isn't bad luck which concentrates obstetrical and child care costs in a certain age range, it is biology. No amount of pooling within the age cohort can smooth out such a systemic cost bulge, so the reproductive age group will have to borrow money (collectively) from the non-reproductive ones. With a little thought, it can be seen that subsidies between age groups are actually more nearly fair, than subsidies based on marital status or gender preference, or even employers, who tend to hire different age groups in different industries. On the other hand, if interest-free borrowing between age cohorts is permitted, there must be some agency or special court to safeguard that particular feature from being gamed. All of these complexities are vexing because they introduce bureaucracy where none existed; it is simply a consequence of using individual ownership of accounts to attract deposits which nevertheless must occasionally be pooled later. Because these borrowings are mainly intended to smooth out awkward features of the plan, every effort should be made to avoid charging interest on these loans. However, if gaming of the system is part of the result, interest may have to be charged.Proposal 16: Where two groups (by age or other distinguishing features) can be identified as consistently in deficit or surplus -- internal borrowing at reduced rates may be permitted between such groups. Borrowing for other purposes (such as transition costs) shall be by issuing special purpose bonds. These bonds may also be used to make multi-year intra-family gifts, such as grandparents for grandchildren, or children for elderly parents.
Proposal 17: A reasonably small number of escrowed accounts within a funded account may be established for such purposes as may be necessary, particularly for transition and catastrophe funding. Where escrowed accounts are established, both parties to an agreement must sign, for the designation to be enforceable. (2606)Escrowed Subaccounts. Both Obamacare and Health Savings Accounts are presently expected to terminate when Medicare begins, at roughly age 65. Nevertheless, we are talking about lifetime coverage, where we have a rough calculation of the cost ($325,000) and the Medicare data is the most accurate set, against which to make validity comparisons. We want to start with $325,000 at the expected date of death, spend some of it in roughly 20 installments, and see how much is left for the earlier years of an average life. Then, we repeat the process in layers down to age 25 and hope the remainder comes out close to zero. There are several things missing from this, most notably how to get the money out of the fund, but let's start with this much, in isolation for the Medicare age bracket, age 65-85. We are going to assume a single-premium payment at age 65, which both life expectancy and inflation in the future will increase in a predictable manner, and changes in health and health care eventually reduce healthcare costs, not increase them. Not everyone would agree to the last assumption, but this is not the place to argue the point.
We know:
(a) The average cost of Medicare per year ($10,900)
(b) How many years the beneficiaries on average are in the age group (18).
(c) Therefore, we know how much of the $325,000 to set aside for Medicare ($196,200),
(d) And know how much a single premium at age 65 would have to be, in order to cover it. ($196,000 apiece)
(e) We thus know how much all the working-age groups (combined as age 25 to 65, 60% of the population) must set aside, in advance for their own health care costs, when they reach Medicare age ($196,000 apiece).
(f) And by subtraction therefore how much is left for personal healthcare within age 25 to 65 ($128,800).
(g)We can be pretty certain average Medicare costs will exceed those of anyone younger, setting a maximum cost for any age.
(h) All of this calculation ignores the payroll deductions for Medicare and premiums. Since this is nearly half of the cost, it changes the conclusions considerably, depending on how you treat these points. During the transition phase, several approaches may be necessary. Furthermore, the size of accumulated debt service is unknown, or what the alternative plans are, for it.
Shifts in the age composition of the population produce large changes in total national costs, but should by themselves not change average individual costs. What they will do is increase the proportion of the population on Medicare, thereby paradoxically making both Obamacare and Health Savings Accounts relatively less expensive. Obamacare can calculate its future costs with the information provided so far. But the Health Savings Account must still adjust its future costs downward for whatever income is produced by investments. We don't yet know how much each working person must contribute each year, because we haven't, up to this point, yet offered an assumption about the interest rate they must produce. We should construct a table of the outcome of what seem like reasonably possible income results. There are four relevant outcomes to consider at each level: the high, the low, and the average. Plus, a comparison with what Obamacare would cost. But there are two Medicare cost compartments: the cost from age 25 to 64, and the cost from 65-85 advancing slowly toward a future life expectancy of 91-93. These two calculations are necessary for displaying the relative costs of Medicare and also Obamacare.
Children's Healthcare. Someone is sure to notice the apportionment for children is based on income rather than expenses. The formula can be adjusted to make that true for any age bracket, and a political decision must be made about where to apply an assessment if income is inadequate; we made it, here. We have repeatedly emphasized that if investment income does not match the revenue requirement, at least it supplies more money that would be there without it. Somewhat to our surprise, it comes pretty close, and we have exhausted our ability to supply more. Any further shortfalls must be addressed by more conventional methods of cost-cutting, borrowing, or increased saving. In particular, attention is directed to the yearly deposit of $3300 from age 25-65, which is what the framers of the HSA enabling act set as a limit, somewhat arbitrarily.
Privatize Medicare? And finally but reluctantly, the figures include provision for phasing out Medicare, which everyone treats as a political third rail, untouchable. But gradually as I worked through this analysis, I came to the conclusion that uproar about medical costs would not likely come to an end until the Medicare deficit was somehow addressed. I believe we cannot keep increasing the proportion of the population on Medicare, paying for it with fifty-cent dollars, and pretending the problem does not exist. So it certainly is possible to balance these books by continuing our present approach to Medicare. But it would be a sad opportunity, lost.
In summary, we have concocted a guess of the outer limit of what the American public is willing to afford for lifetime health coverage ($3300 per person per year, from age 26 to 65), and added an estimate of compound income of 8% from passive investing, to derive an estimate of how much we can afford. From that, we subtract the cost of privatizing Medicare if our politicians have the courage for that ($98,000 -196,000) and thus derive an estimate of how much is available for health care of the rest of the population ($128,000). Because of the longer time spans available for compound income, at 8% it would cost more out-of-pocket to finance the $128,000 than the $196,000; it would actually be financially better to include it. The non-investment cost, on average, would only be $ 148,000 per lifetime, for an expense which otherwise almost insurmountably crowds out everything else in the national budget. It might be $98,000 less because of Medicare payments, or it might prove to be more, depending on interest rates and scientific progress. Believe it or not, that could be a wide improvement over the present trajectory.
That's how it seems at first when you approach the topic of multi-year health insurance. But there are several exciting additions when you really get into it. It plods along, and then it explodes.
Healthcare, A Much Simplified Overview
Let me say at the beginning, what could be repeated in a summary: The present healthcare dilemma has three interlocked parts, scientific, financial, and political. The scientific component is capsulized by three symbolic life expectancies: in 1900: age 47, today: age 83, and fifty years from now: age 100. We're living a lot longer, and soon expect the population to divide into thirds (one third getting educated, one third retired, and one third working to support the whole population. It probably won't work very well. Most health reforms amount to finding some way to shift income from the working third to the other two thirds.
The main scientific problem in the past was to avoid dying too young. But the problem in the far future will be living too long, running out of savings. Right now we can imagine having both problems, and few can guess which problem to fear. Maybe there is enough money for one of those two life terminations, but we don't have enough money for both of them, for everyone. We would have to give up something else, like national defense. Let's try to use the same money twice, if we can.
Finance. The payment systems need to be more interchangeable for alternative uses. But be careful. This could seemingly lead to merging Medicare and Social Security (someday) into one interchangeable program. Interchangeability of funds might plausibly seek to be at the family level instead of over-reaching to the level of demographic groups of whole thirds of the population. We do need to devise ways to transfer from one stage of a person's life to another, Saving for a Rainy Day, as it were. Some solutions will inevitably turn into problems. Proposals to integrate all health care into one vertical single-payer medical system would likely clash with more useful integration of Medicare and Social Security. These arguments can possibly wait for a later time, but only if we recognize they remain undecided. Generally speaking, they translate into recognizing that it is easier to shift money than people. Governments regard such as shifting with indifference, but we train children from birth to be possessive about their own money. And we elect politicians to see the difference.
Both the insurance spread-the-risk approach and the government pooling process skirt the difficulty there is not enough money to cover both possibilities for everyone. Either to borrow or insure postpones repayment for a while, that's about all. Meanwhile, healthcare costs are subject to more sudden changes in greater ranges than the economy as a whole.
Finally, let's see if we can put these shifts to work, and get some extra money from investment income, with compound interest working its magic over the whole expanse.
Politics. Meanwhile, we move toward a time when voters who earn money aren't sick, and the sick voters don't earn money. But they all have a vote. Already, we conduct transfers of money on a scale people may rebel against. It must become their own money, in their own accounts, spent later on themselves -- rather than forced transfers between demographic groups. At most, we might try extending that to the family unit, and even that should be kept as voluntary as possible.
|
Constitutional equal justice tends to make political solutions resemble one-size fits all.
|
So that's the general nature of our problems. Healthcare does become less expensive in the long run, even though more expensive in the short run. And through recent advances of financial management, Health Savings Accounts can generate surprising amounts of extra money on their own, overall helping with the other problems. The abstruse issue of inflation also arises here, where you might not expect it, because if trillions of dollars eventually migrate into passive investments through Health Savings Accounts, the elderly will hold shareholder voting rights they would be unwilling to surrender. The course of further inflation, the main concern of the elderly, would shift toward the hands of savers, away from borrowers. Unfortunately, what the proper balance is, isn't yet clear.
Flies in the Ointment
The reader will please excuse my round-about way of explaining the essence of an idea by skipping past one serious issue, and then returning to it. What you have just read is a succinct, perhaps overly succinct, description of the main elements of the lifetime HSA idea. Where I don't have precise data, I approximate it within the ballpark, assuming it can be sharpened up later. What has been deliberately omitted from the foregoing description, is the possibility that someone will get sick and spend some money. That's not just possible, it's certain. When you spend money on healthcare, you can replenish the fund, but you can't replace the income it would have earned if you hadn't spent it. You can slide past that difficulty by double-funding it, but then you would go to the other extreme and over-count it. The concepts involved are pretty simple, but the arithmetic gets pretty complicated because it will change over time. A monitoring agency must be charged with making objective annual mid-course corrections within boundaries set by Congress.
Double Counting.The lifetime Health Savings Account is in three parts: for children, for wage-earning years, and Medicare. For Medicare, the funding is fairly adequate, because the money is saved up in an escrow account, unspent while the buy-out price accumulates. In fact, it could be 50% over-accumulated by continuing the payroll deduction and premiums. Once you are ready to transfer the funds for the buy-out, you can decide whether you need to accumulate the payroll deductions and Medicare premiums. My guess is that at first, it would work without such supplements, but eventually, longevity would increase, new diseases and new treatments would appear, and risks of a cash shortage would then appear. Accordingly, continuing the payroll deduction and premiums would be one possible way to accumulate reserves for unexpectedly high sickness costs. If that method is chosen, some protections must be built in, to protect the reserve from being diverted to other uses..
The same might be true of Grandpa's grandchild insurance, which in a sense is borrowed from an adjustment in Medicare rates. The childhood costs are also fairly small. The only real example of double-counting which remains is in the wage-earning group from age 21 to 66. That issue could be visualized in two segments.
From age 21 to age 45, health costs of working people are not significantly higher than for children, except for obstetrics and gynecology. Even those two items are partly covered by splitting apart the obstetrical costs between mother and child, now artificially combined in contrived family insurance plans. Aside from this issue, the health costs of young adults are not greatly different from adolescent costs. From age 45 to 66, however, the cost curve gradually rises until older adult costs begin to match the Medicare costs (with terminal illness removed). It is this subset of one group which likely would create the greatest cost resulting in double-counting the investment income, and replacing the medical expenditures. Furthermore, this is also the arena of greatest cost-shifting, and therefore, may I say it, obscurity in the data. Nevertheless, the shortfall of middle-aged sickness costs has boundaries constraining it. The annual costs surely cannot be greater than the first year of Medicare, for example, and the earning power is at a peak at this time of life. The greatest medical advances have fortuitously concentrated in this group. The costs are likely to decline, as science concentrates on the four or five main diseases of maturity (diabetes, cancer, Alzheimer's, and Parkinsonism). There is also the special issue of the ability to delay some costs a few years until Medicare has the responsibility to pay for it.
It seems possible the data already exists to cope with the costs of these matters, but at an extreme, they should be covered by doubling premiums for the twenty years in question. Doubling $365 a year should provide a $365 cushion in escrow for contingencies. Since this is the peak earning period of life, and still remains well below average health insurance premiums, it seems to have the greatest fairness. Transition costs, the other great unknown, are beyond my capability to predict, and I simply don't do it. During the transition, the opportunity would exist to devote special research to this topic, and at least see if it turns up any crippling issues. I hope not, and I doubt it, but the potential has to be acknowledged. In the meantime, it would look as though the good ol' standard issue Health Savings Account is a little safer bet. It reduces costs, but not as much as the various methods of capturing the upswing of compound interest, at its far end.
Black Swans. There's a possibility that things will go in quite the opposite direction. The stock market has been going up at a rate of 12% for a century. Why does the investor only get 5% to spend? Inflation is clear enough, but why not 9%? In a sense, this apportionment is traditional, tracing back to investing endowments for colleges or museums. If the stock market has a black swan and drops 50%, are you going to close the doors of the college until the market recovers? One conceivable strategy for this event would be to accumulate a cash reserve to be used during the dark days of depression. However, this has inflation dangers, and it is impossible to say how much it should be because if you keep 50% in reserve, you might as well say you are only realizing 6% overall during a 12% rise. So, the alternative wisdom urges an investment of 60% in stocks (at 12%) and 40% in bonds (at 4.5%), allowing you to keep the doors of the college open in both an inflation and deflation when the numbers will suddenly change. So, a 60/40 investment ratio became traditional in investment circles, reinforced by saving the neck of many investment managers. But just a minute.
We are investing in our own health care, not for a college. If revenue declines for several years, it doesn't matter nearly so much for a young person if his income dips, only to recover in later years. The fundamental argument underpinning 60/40 is weakened considerably. If the market is headed for 12% in the long run, why not just ride out the dips and peaks? There's no good reply to this challenge, except an innate conservatism when you are managing other people's money. Very well, why don't we just lean in that direction? Surely a ten-year-old child can ride it out, even if a 70-year-old has to be more cautious. Consequently, you begin to see more and more investment managers leaning toward 80/20 or even 90/10 mixture of stocks (12%) and bonds (4%). When your clientele is of many mixed ages, such as pooled Health Savings Accounts are likely to be, perhaps the younger ones would be well served to get 6% or 7% income, while the older ones play it safe with 4%. This line of reasoning is likely to be more widely heard as uncertainty about middle-man costs gets more wide-spread. If the investment manager is suspected of taking 2-3% of the reserve as a kick-back, or just profit margin, it becomes a more pointed argument that brokerage accounts are not pooled investment funds at all, but rather an open market between a buyer and a seller. If the stock market takes a black swan dive, you can be sure the 4% reserve will not be used to buffer the losses of the investor, in the present arrangement of things.
If the projected investment return is high enough, no investment contingency is worth discussing. In this book, we only wish to point out that a 6.5% lifetime return is more than ample to cover lifetime health costs, plus a wide contingency reserve. That is particularly true if you remember the bulk of costs come later in life. A return of 6.5% does not seem at all inconceivable, if you look at Ibbotson's data for Twentieth-century asset returns, and read John Bogle's books on saving passive transaction costs on total-market index funds. At the same time, I am mindful of all those potentates who blithely accepted 17% projected returns on pension funds a few years ago, and now look at them. We are double-counting the reduced medical costs of the future, which we cannot know with precision, and warn that you must keep an eye on them. But there is such a wide swing between present premiums and any conceivable escalation of $365 a year, that it seems worthy of serious investigation.
The Premium of Catastrophic Coverage. You have to feel sorry for the owners of an insurance company which sells catastrophic health insurance. It has long been defined as high-deductible coverage, but nowadays everything has a high deductible and an upper benefit level which is not mentioned much. The was a time when a well-functioning market was maintained by the adage that the higher the deductible, the lower the premium. It was often called "Excess major medical coverage", and entirely used as reinsurance. Under the circumstances of the Affordable Care Act, high deductible policies hide the subsidies they make and receive and do their best to avoid quoting a price unless the customer is in the office and has his pen in his hand. The Affordable Care Act made it clear it would like nothing better than to have Catastrophic insurance disappear in disgrace. As a matter of fact, ever since the McCarran Fergusson Act, it is a question whether any insurance may be regulated under the Federal, as opposed to State, government. The United States Supreme Court has an opportunity to address these vexing issues in King v. Burwell , and we await its decision with eagerness.
Spending Rules--Same Purpose As Escrow Accounts
Useful features are buried in the spending-rule idea. A portfolio would never go to zero if spending is held below a certain level; an endowment on auto-pilot. This magic number was once 3%, now is thought to be 4%. In trust funds for irresponsible "trust fund babies", spending rules are particularly common. In taxable circumstances, it is a vexing complication for non-profit institutions that federal tax rules require minimum annual distributions of 5%, somewhat more than a taxable account can sustain indefinitely, at least according to present theory, and assuming present costs. Every effort should be made to reduce middle-man costs, and the present rate of progress is encouraging. As long as medical progress continues to depend on a top level of talent, efforts to attack the cost of care itself may prove counter-productive.
In my opinion, a spending rule is pretty much the same as a budget, and the same goals can be accomplished with an escrow account, permitting no expenditures at all until a certain date, and then only for a stated purpose. And furthermore, there can be several spending rules, just as there are several lines in a budget. There surely ought to be both a discretionary spending rule and an inflation spending rule, for example, since inflation is beyond citizen control. As a practical matter, planning will generally mean 5% discretionary, and 3% inflation, for a total of 8%. Until recently, it was generally assumed if the Federal Reserve instituted, or Congress mandated, an inflation target of 2%, it would mean 2% was dependable because the Fed had unlimited power to print money. However, in 2015 the inflation rate is 1.5%, in spite of heroic efforts to use "Quantitative Easing" to bring it to 2% by buying two or more trillion dollars worth of bonds. Inflation has remained at 1.5%, resulting in much wringing of hands. So spending rules help establish responsibility for deviations.
It is not useful to engage in political arguments over why this is so, it must be adjusted for. The consequence is we have an Inflation Spending Rule of 3% and actual inflation of 1.5%, leading to a national inflation surplus of 1.5%. If a Health Savings Account has an Inflation Spending Rule of 3% only because that is what we have seen in the past century, our inflation is 1.5% under budget, which could easily be misinterpreted as an extra 1.5% to spend. When we figure out what this means, we can puzzle what to do with it, but until that happens, no spending allowed. Another precaution would be to have two spending rules, totaling 8%, only 5% of which is actually spendable. If we create special escrow funds for buying out Medicare or passing to our grandchildren -- the same thing.
|
If you don't limit yourself, Others will limit you.
|
| Spending Rules |
In the case of Health Savings Accounts, a spending rule of 6.5% within an investment yielding a net of 9%, is a special case, but a good one. The central purpose of the whole HSA idea is to lower the effective cost of medical care, by generating funds to pay for it. The more income generated, the lower the effective price of medical care, so why impose a spending rule? In fact, a spending rule for an HSA does not reduce the income, it only delays the spending of it, because either the funding account gets exhausted by the time of death, or it is rolled over into an IRA. Either way, there is no final end to HSA spending, only postponements. When spending is postponed, it eventually earns more income; the ultimate effect is more availability for health care. If a cash shortage forces the HSA to curtail health spending, the bills must be paid from other sources, usually taxable ones. So even in this situation, there is more health spending power ultimately generated, but it is generated by not spending tax-sheltered money. It could even be argued that diseases later in life tend to be more serious. Indeed, if a spending rule is under consideration for an HSA, it could be voluntary as long as there is no way to game it. Unfortunately, that can lead to coercion for someone's own good, always a dubious idea.
If a portfolio generates 8% but only spends 5%, there's a safety factor of 3%, almost exactly matching the long-term effect of inflation. We hope moreover, the inflation issue is addressed by using the theory that inflation of expenses should match inflation of revenue, but you never can be sure of it. It is, in fact, more likely they won't match. A spending rule increases the power to shift surplus revenue to years of high medical cost, which will be later years, and will, by compounding, actually increase the total amount of it. This consequence is not necessarily obvious. The spending rule guards another easily forgotten thought: the purpose of an HSA is not to pay for every cent of health care. It is meant to pay for as much of it, as it can. It is likely, to invent an example, to encourage skipping cosmetic surgery, so there will be money enough for cancer surgery at a later time.
The purpose of this soliloquy is to justify the establishment of escrow accounts within Savings Accounts, to keep the fund from wandering from its purposes, or at least to recognize it early if it does. There should be a Medicare buy-out escrow fund, with a suggested budget calculated to make it come out right. And a Grandparent's escrow fund, and Permanent Investment Escrow fund, budgeted to pay for a future lifetime of care, alerting the owner how much it is below budget. These escrow funds are intended to be flexible but intended to serve their purpose. HSA Account managers are encouraged to use them and to explain them. By making certain escrows mandatory and uniform, big data monitoring is facilitated. Other government access should be minimized.
Escrow Accounts for Future Needs.
One of the important advantages of Health Savings Accounts over historical health insurance lies in the contrasting sacrifices you must make if you can't afford everything. Traditional health insurance ("first dollar coverage") paid for the small things, but if you ran out of money, you had to sacrifice some big things. The Health Savings approach is to provide money for the big things first and sacrifice little things if you must. That's the essential philosophy, and it has become exaggerated by increased longevity. We need to add a simple way to by-pass small expenses and save money for later. That's the reasoning behind adding escrow accounts to high-deductible insurance.
Think about it: when a subscriber faces a medical expense costing more than his account balance, he has three choices. He could forego the medical service, he could pay cash out of pocket, or he could borrow the money. Sometimes he will have enough money in the account, but saves it for some later purpose; in that case, he might be both a borrower and an investor at the same time. When it comes time to pay off his loans, that obligation should have a higher priority than investing new money, since otherwise, the subscriber is investing on margin. Margin investing is generally a bad idea, but it can be made less risky through using an escrow account. That's a designated-purpose account, which is more difficult to invade. So, he may divide his account into three escrow accounts, and the managers may decide they need even more. It becomes inflexible if it can never be invaded, but it shouldn't be easy and paying cash or tax-unsheltered money is always better if you can.
Borrowing Escrow. It's wise to pay off debts early, so the program should require its permission to do anything else with a new deposit. Not all managers of HSA will advance overdrafts, but some will, probably at rather high-interest rates. More commonly other subscribers will have surplus money they would like to lend like a credit union, because deposits up to their annual limit are tax deductible, and they would be reluctant to pay the taxes to redeem them.
|
If you will need it later, Set it Aside, Now.
|
| Escrow Subaccounts |
It's possible to imagine gaming such arrangements of differing tax liability, so Congress must decide what circumstances permit it. With insurance, considerable pooling of resources happens without tax consequences, but when bank accounts are individually owned, pooling is not allowed without legal provision. Depositing unencumbered money in the escrow account is the same as investing it, except its presence indicates availability for loans in certain circumstances. Nevertheless, it is inevitable that gaps between the two curves, revenue, and expense, will develop, even though the hills eventually exceed the valleys.
My suggestion is to limit structural borrowing at low-interest rates to smoothing out the valleys characteristic of entire age levels, rather than provide individual banking arrangements between subscribers. Over time, these variations will standardize. And since the accounts will collectively grow, the quirks will eventually stabilize the investment accounts, possibly even augmenting income. However, if a surplus or deficit is exhausted, it should not be perpetuated with outside financing. The accounts operate under the principle that they come out right at the end. It, therefore, ought to be possible to adjust age-determined structural imbalances in bulk, while attempts by subscribers to game such variations should be countered by modifying interest rates.Wholesale buyouts have their advantages, but piecemeal buy-outs are better.
Proposal 5: Congress is urged to permit pooling (at low interest) between the accounts of an age group inconsistent surplus, -- and other age groups in consistently deficit status,-- occasioned by persistent divergences between revenue and medical withdrawals at differing ages. If there are other imbalances created by differential depositing, they should be corrected by adjusting internal interest rates. (2735)Medicare Escrow. There are a number of reasons why some people would want to buy their way out of Medicare, whereas others would become terrified at any mention of changes in their Medicare plan. The incentive for the government to permit Medicare buy-outs would lie in ridding itself of its deficit financing, with secondary borrowing from foreign nations. And the advantage for the plan itself is providing a cushion for a transition to lifetime accounts, ultimately a better cushion for revenue misjudgments.
By noting the average annual cost of Medicare, the number of Medicare beneficiaries, and the average longevity of subscribers, the average lifetime Medicare costs of Medicare can be calculated. Assuming inflation to affect both revenue and healthcare expenses equally, inflation is ignored. Then, with various compound investment assumptions, a range of future income can be estimated. All of this can be estimated as requiring a lump-sum payment of $60,000 at the 65th birthday in order to make a fair exchange for the Medicare entitlement and guessed at $80,000 if accrued debts are serviced. However, the individual would have paid about half of that with previous payroll deductions during his working life (a quarter of the total), and by buying out of it at age 65, would be relieved of Medicare premiums which amount to another half of what is left, or a quarter of the total cost. However, that complexity of description eventually leaves half of the total to be made up by Federal subsidy from the taxpayers because loans must be repaid. It's complicated because every revenue source available has been tapped.
The biggest issue is a foreign debt to be paid back for financing Medicare deficits in past years. Consequently, in order to put a stop to further borrowing, the buyout price must be raised. Obviously, if a past debt is serviced, more contribution is needed. Unfortunately, information about prior indebtedness is not readily available, so the entirety is here guessed to require a single-payment premium of $80,000 at the 65th birthday, for a full Medicare buyout. If the entire Medicare program, past and present, is to be paid off, they're very likely will have to be a tradeoff between increased revenue from HSA deposits and diminished service of foreign debts. As a guess, the elasticity of HSA revenue of $3350 per year, from age 26 to 66, has already more than reached its limit. For the moment, we have accepted the present Congressional limit, which was presumably rather arbitrary. While it is possible to imagine this arbitrary limit could be made to stretch to cover lifetime health costs, more likely it will only cover a portion. But to cover the Medicare unfunded debts of half the past century in addition to current costs, will require some new concept, as yet undevised, and a good deal more information than is presently public.
"All-other" Escrow. It is difficult to foresee which escrows will prove so popular they will require limits, and which others will be so unattractive they will require minimums. Moreover, it can be anticipated some people will wish to use account surplus as an estate-planning tool, while others will have no estate. A provision in law directing the uses of account surplus at death may thus appeal to the majority of subscribers, but actually may be highly unsuitable for the majority. Therefore, while it seems harmless to provide a vehicle for such individualization, too much should not be expected of it.
To most readers, these sums will seem prodigious, and indeed they are. Few people at present are in a position to consider them. We can pray for some relief from scientists, from the economy, and from demographics, because downsizing Medicare is a growing requirement, provoking even more drastic remedies if we sweep it under the rug. We need, first, to make Medicare more modular so it can be downsized in pieces, instead of all-or-none. In time, we need to downsize it and use the pieces to fund protracted retirement costs. The long-term goal, for the scientists, the politicians, and the patients, is to make it unnecessary to spend so much money on health. Beyond that, the funding of retirement has no logical limit. This long-term vision of our future must first become commonplace in our culture so we will seize every chance opportunity to advance it in fact.
Using Escrows to Estimate Cost Risks(1)
The general thesis of this proposal is we can make better guesses about the future than we think we can, just as long as we remain aware they are guesses. In the past, that approach has made some blunders, like the sun revolving around the earth, or Columbus badly underestimating the width of the oceans. And so the world divides itself into "failure-avoiders" and "success-seekers", each contemptuous of the other. Those divisions are not likely to change much.
The proposed approach is to estimate how much we must save to achieve a distant goal, subtract it from the amount we can stretch ourselves to save, and see if what's left, is a realistic number. If you envision atom bomb attacks and climate catastrophes, the answer is No. But if you confine yourself to the question at hand, the answer might well be Yes. So as long as we confine ourselves to a voluntary approach, the nation will hold itself together if someone is wrong.
Let us repeat the basic assumption, that for practical purposes, all money is derived from the working age group, 21-66, and everything else is essentially borrowed. That is, the health costs of children under age 21 are supported by their parents, and those over 66, by savings. In addition to this basic division, about 10% of the population are unable to support themselves because of disabilities, prison and related matters--and must be subsidized. All of these side issues are slowly improving, but in this analysis we must ignore them, or at least treat them as a general category. We are now about to consolidate children and elderly people into one group.
That is made possible by the happenstance that our birthrate is 2.1 children per mother, which comes out to be one grandparent per grandchild. There are all manner of exceptions, like trans-gender people, divorces, polygamy and what have you. Our purpose is not to be comprehensively respectful, but to estimate quantities. And one grandchild per grandparent suffices for that. If each grandparent is financially linked to one grandchild, the others are a matter of pooling more with less. All newborn health costs are the responsibility of someone else, usually the father, increasingly the mother. This proposal suggests that we make health costs the responsibility of the grandparent generation, since Medicare has already made the grandparents the responsibility of government. We do this because Medicare is increasingly becoming a burden we cannot sustain. The public does not seem willing to listen to this, and so politicians are unwilling to bring it up. But Medicare is unsustainable in its present form, and therefore is absolutely destined to change. When we eventually face facts, I believe it will seem rational to combine the health costs of the two groups, so I propose we start the ball rolling by taking advantage of it sooner rather than too late. We can come back to this later, but let me briefly step up to the soap box:
We are launched on a demonstration model to the effect that compound interest income can greatly reduce the effective cost of healthcare. It is the nature of compound interest curve to turn upward the longer they extend. Therefore, we would greatly enjoy substituting lifetime compounding for annual premiums, and the greater the longevity the better. However, lifetime healthcare funding is greatly hampered by the rather high costs of the first year of life. People would almost have to live to be two hundred years old to make up for that high cost at the beginning of life, would have to inherit several thousand dollars, and would have to have rich parents instead of nearly insolvent ones. It is almost impossible to overstate the hampering effect of the high costs of the first year of life. So, we propose that grandpa transfer some of his excess Medicare funds to a grandchild, overfund Medicare a little to make room for the cost, and use Health Savings Account transfers as the vehicle for it. That adds at least 21 years to the compounding of 21 to 66, and it could potentially add the years 66 to 83, our present life expectancy. If we can somehow transform 44 years of compounding to a full 83 years, the financial consequence would be astounding. We are talking about lifetime health care, supported by a third of a lifetime of savings, if that much. No wonder the actuaries are wringing their hands.
Using Escrow to Estimate Health Costs (2)
Because so many people's circumstances are so different, we offer two ways for Grandpa to transfer one grandchild's health care to one grandchild, and skip any description of pooled transfers of the rest.
Grandpa can either transfer a lump sum single-payment upon the birth of the lucky grandchild or through his will if that is more suitable. Alternatively, the Health Savings Account of one generation can transfer $365 yearly to the grandchild's escrow account, which is set aside for grandchild to buy his way out of Medicare -- if he later chooses -- at the 66th birthday. Grandpa will only do this for 21 years, after which it is the child's own responsibility. According to my math, that will pay for the estimated costs of Medicare, stop the foreign borrowing to pay for deficits, and perhaps make a dent in the accumulated foreign debts.
What it won't do is pay for the grandchild's health costs if they escalate out of control between now and then, or if Medicare is forced to add on all manner of deductibles, copayments, taxes and other out-of-pocket exceptions to pay for cost escalation. His catastrophic health insurance is supposed to protect against that, and within limits, it will. But at the present time, catastrophic health insurance has been so jumbled that you cannot get a salesman to make an average quote for publication. It will only become possible to make sensible judgments after the United States Supreme Court has made a final judgment, or if Congress assembles a sufficient majority to clarify the situation. As matters stand right now, there is no need for excess coverage, and the money in the escrow account should be released to an Individual Retirement Account (IRA). The amounts of accumulated funds in HSAs are illustrated in accompanying tables, grouped in multiples of $365 contributions. For very high-cost over-runs, catastrophic health insurance would normally be an alternative to consider.
But that -- encompassing childhood costs and Medicare buy-out -- is only half of the proposal. The rest has to do with the age group 21-66, which is now tangled in the courts, under King v. Burwell and I cannot go further.
Lifetime Health Insurance: Monitoring the Data
The longer we wait to make drastic changes, the more difficult they become, more proof of benefit will be demanded. In the proposed case of switching health insurance from term insurance to whole-life, a century of insurance development contributed insights. But remember, the past fifty years have seen plenty of dissatisfaction come to the surface, only to be dashed by a (generally correct) opinion that the old system was working better than the proposed one would.
Health Cost Monitor Center. This time, let's start in advance with establishing a monitor center, and locate it near other public data centers. Turf issues are inevitable, but bowling teams can break them down. With attention to the issue, an interagency technical center could develop into a useful employment center, attracting superior people with vastly enhanced opportunities for personal advancement. If the center is large enough and sufficiently diversified, it will resist abuse by tyrants.
|
By waiting fifty years, we now have big data. But we could have had answers, fifty years ago.
|
| Perfect is the Enemy of Good Enough |
Conversely, in a population as large as ours, enough people of younger ages will inquiring minds; the problem is to establish the right leadership, and the right opportunity so we can still estimate in advance what difference our proposals make to costs at almost any age. At least then, the public could judge what is actually happening, instead of relying on the pronouncements of political candidates. Half of hospital cost experience already resides in Medicare data, the last years of life are well documented, and the first years of life are fairly predictable for these purposes. So we start the data with pretty good anchors and a panoramic overview of costs. With at least a stated goal of offering suggested prices for lifetime planning, but not necessarily universal ones, we should be able to cope with a voluntary system.
Footnote: An experience forty years ago makes me quite serious about this monitoring issue. While I was on another mission, I discovered Medicare and Social Security are on the same campus in Baltimore, with their computers a hundred yards apart. So I proposed to the chief statistician, that the Medicare computers already contained the date and coded diagnosis of every Medicare recipient who had, let's say, a particular operation for particular cancer. At the same time and in the same location, the Social Security computers contain the date of everybody's death; the Social Security number links the two. So, why not merge one data set into the other, and produce a running report of how long people seem to be living, on average, after receiving a particular treatment or operation -- and how it seems to be changing, over time. (Length of survival = date of death minus date of the procedure) He merely smiled at the suggestion, and I correctly surmised he had no intention of going any further with it. This time, I resolved to write a book, to see if that might have more effect.
Let's ponder about some of the uncertainties which can only result in guesses at the moment, but which in time can be more precise, and provide the material for mid-course corrections:
|
Considering the sums involved, We don't watch public money very carefully.
|
| You Cannot Have Too Much Data |
Transition Calculations. Let's say we have politicians with the skill to persuade the public to phase out Medicare in order to put an end to the foreign borrowing of half its costs and persuade enough beneficiaries to do so by buying themselves out of the program. It has been our extrapolation that this could be done with a single payment of $80,000 at age 66, having earned an income of 6% since age 30. The cost would compare favorably with present payroll deductions for Medicare, although of course, you can't spend it on two different things; the present premium costs of Medicare provide a roughly equal amount. That provides a price goal, for the beneficiary to make a last-minute decision whether to go ahead with the buy-out. And during the years of accumulating the wherewithal in an escrow fund, it presents a distant steady goal. In addition, we also must recognize that a large foreign debt has been obligated to pay for shortfalls of years now past.
The size of the debt is unclear, but we estimate about an additional $80,000 would pay it off. If the numbers come out wrong, the debt payment could be shrugged off, the way the Chinese Imperial government did a century ago, and the way the Greek government wants to do at present. For argument sake, let us assume that debt to be $80,000, but we are unsure how to pay it. (If I sound like Lyndon Johnson, it is because I am dealing with the same topic.) If these numbers approach any kind of accuracy, the process of buy-out could begin, voluntarily, delaying the choice until the 66th birthday. If there is significant interest in the idea, these numbers could be sharpened, but there would always remain some guesswork. Some additional protection of the gamble could be provided by adding a catastrophic insurance policy. In the long run, this whole buy-out idea would be strengthened by migrating the center of care to a nearby retirement village and using the hospital system only for tertiary care. Obviously, it is intended that the proposed monitoring center would be actively involved, and not merely act passively collecting data without designing some large-scale experiments, also obviously voluntary.
Somehow, a large and well-respected health monitoring system could perform a significant service by participating in more demonstration programs, since so often Congress must resort to trying something because it seems like a good idea. Such an approach needs some discreet professional guidance since obviously, Congress would be reluctant to hand over power, simply because some bureaucrat had gone to graduate school or present the Congressional opposition with an opportunity to get rid of them by assigning unwelcome proposals to a protracted study they did not need. Nevertheless, a few well-designed demonstration programs might be a useful way to make some decisions which are currently only based on hunches. It seems likely the kind of monitoring agency needed, would only have the desired outcome if the first Director of it was a strong and highly talented professional, preferably with a distinguished reputation for an impartial examination of the evidence.
That particular function stresses innovative ideas, starting from their beginning. A limited amount of that is badly needed, but sensitivities must be respected. The main function of a monitoring agency is to provide reliable reports to Congress that a developing program is, or is not, on schedule, or is or is not producing the intended effects at a promised cost. Congress is busy, and it is often in a hurry. It needs to be told that something unexpected is happening, or that something expected is not happening before the news media starts to get excited. And somehow it needs to be a welcome friend to the departmental auditors, who will greatly resent an outside body finding something which has been overlooked. As the saying goes, it needs to have some money in the bank before it opens its mouth.
Cost is the Big Issue, But Here's Another
In the calculation of A Dollar a Day, it is assumed Congress will permit Health Savings Accounts to purchase the catastrophic, low-cost high-deductible health insurance which pools the risk and acts as a fail-safe insurer of last resort. In a sense, catastrophic insurance through HSA substitutes for a limitation of out-of-pocket expenditures by the subscriber, and incidentally gives income tax exemption to everybody, not just employees of big companies. It also assumes the President will sign such a law, although that may have to wait for a new election if the matter cannot be compromised. No doubt, any president would be heavily influenced by the attitude of big business. The reader is reminded Henry J.Kaiser started this issue in 1944 as a wartime expedient, but the rest of big business has followed his lead, protecting its own tax write-off. For eighty years, this relic of World War II has been quietly but fiercely defended, along with the very large corporate tax reduction which is implicit.
Unfortunately, the negotiations between employer representatives and the administrators of the Affordable Care Act have remained secret, and a resolution of the position of employer-donated insurance has been delayed for two years. The probably motives of big business are clear enough, however, because very large corporate tax write-offs are at stake. Our proposal in this book is to compensate employers with a reduction in the world's highest corporate tax, which has been shown by the Irish government's experience to destabilize international currencies if it is done too rapidly. Adding to the transition awkwardness is the effect of disrupting patients and providers who are already engaged in transactions. Accordingly, there are cogent arguments for transitional accommodations.
Proposal 24 :Congress is urged to consider permitting employers to include catastrophic coverage as a fringe benefit, regardless of other modifications, and to continue coverage after terminations of employment until it is no longer required. Employees without catastrophic coverage may purchase it independently, and carriers will be required to coordinate successive policies in such a way that the employee runs no added risk during transitions.
Commentary: Catastrophic coverage is ordinarily much cheaper than current policies provided by employers, and therefore the corporate tax abatement will be less. Negotiations about corporate tax reductions may wish to take this into account, as well as compensating wage rises for affected employees. Because of the massive number of employees involved, transitions should be voluntary where ever possible.
When costs are better understood, the cost to the individual subscriber should be less. Unfortunately, the rhetoric cadence of "a dollar a day" will have to be sacrificed, because average costs may well be reduced below that figure. While the current employees of big business would nominally be paying for this change, increasing use of Health Savings Accounts would have the result of reducing their total health costs, as well.
Employers who currently provide health fringe benefits could well prove to be the heaviest losers. Negotiators for corporate tax reduction should remember this; it has the effect of describing much of our corporate tax revenues, as eventually paying for a considerable amount of health care.
Paying for the Healthcare of Children
It has been said by others that eventually healthcare will shrink down to paying for the first year of life, and the last one. Right up to that final moment, medical payments must somehow evolve in two opposite directions. We might just as well imagine two complimentary payment systems immediately because the two persisting methodologies could eventually conflict unless planned for. Paying in advance is fundamentally cheaper than paying after the service is rendered because there is no potential for default in payment.
The two methods even result in different aggregate prices; in one case you pay to borrow, while in the other you get paid to loan the money. Dual systems are a fair amount of trouble; remember how long it took gasoline filling stations to adjust to credit cards versus cash. When gas prices eventually got high enough, they just charged everybody a single price, again. This isn't just lower middle-class stubbornness. Dual payment systems slow you down, and profit is generated from repeated rapid transactions. The buyer wants the goods and the seller wants the money. The profit comes from doing exchanges as fast and often as you can manage them.
In a well designed lifetime scheme, with balances successively transferred from one pidgeon-hole to another, it becomes possible to maintain a positive balance for years at a time (thereby reducing final prices, because the income from compound interest keeps rising toward its far end). That was a discovery of the ancient Greeks, but sometimes Benjamin Franklin seems like the only person to have noticed.
|
The last year of life is more expensive, But the first year of life may cause more financial pain.
|
However, In real-life health costs, there is one intractable exception. Because obstetrics can be costly, particularly the high costs of prematurity and congenital abnormalities, the first year of life averages $10,500, or 3% of present total health costs. It, therefore, results in pricing which many young parents cannot afford, in spite of insurance overcharges to catch up later. And thereby a multi-year stretch of interest income is jumbled up, often lost entirely. It gets worse: childhood costs from birth to age 21 average 8% of lifetime healthcare. Please notice: Single-year term insurance premiums always rise to a much higher level than a lifetime, or whole-life, premium costs, because of internal float compounds in whole-life. Modern medicine has also resulted in rising lifetime costs, with only this obstetrical exception. Someone surely would have figured this out, except excessive taxation of corporations created a motive not to notice the effect on tax exempted expenditures.
This problem obviously could be approached by borrowing or subsidizing. Someone might even envision a complicated process of transferring obstetrical costs to the grandparents for thirty-five years, then transferring the costs back to the parent generation. Since we are describing a cradle-to-grave scheme, it seems much better to imagine a single person's costs eventually becoming unified. Grandparents do in fact share continuous protoplasm with grandchildren, but before that was recognized, the courts had decided a new life begins when a baby's ears reach the sunlight. Stare decisis beats biology, almost every time. A society which already has a high divorce rate and plenty of other family upheavals probably feel better suited to the principle of "Every ship on its own bottom." -- except for this financing issue. For childless couples and parentless children, some kind of pooling is possibly more appealing, and the complexities of modern life may eventually lead that way.
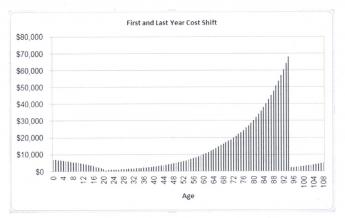
|
In the meantime, lawyers, who see a great deal of human weakness, are probably better suited to suggest a methodology for transferring average birth costs between generations, and back, although a voluntary process seems more flexible. It would seem grandparents are often most likely to be in a position to leave a few thousand dollars to grandchildren in their wills, and age thirty-five to forty seems the time when competing costs are at a lifetime low, making that the best time to pay it back.
Some grandparents are destitute, however, and some parents are basketball stars. There are surely generalizations with many exceptions. The process is happily simplified by a birth rate of 2.1 children per couple, which is also 1:1 at the grandparent/grandchild level and our Society has an unspoken wish to increase the birth rate if it could afford it. For legal default purposes, matrilineal rather than patrilineal descent may be more workable. But -- if every grandparent willed an appropriate amount to some grandchild's account, it would work out (with a small balancing pool), creating a small incentive for the intermediate generation to have more children.
The answer to this dilemma probably lies in revising the estate-resolution process, making HSA-to-HSA transfers largely automatic within families, devising a common law of special exceptions and adjustments, and creating a pooling system for special cases which defy simple-minded equity. A large proportion of grandparents have an indisputable defined obligation, and a large proportion of grandchildren have an indisputable entitlement. The difficult problems reside in the exceptions and require a Court of Equity to decide them. We leave it to others to fill in the details because there could be many ways to accomplish this, and some people have strong preferences. The basics of this situation are the grandparents with surplus funds are likely to die later, but they are still likely to die, close to the age when newborns are appearing on the scene.
When you get down to it, the problem isn't hard if you want to solve it. By arranging lifetime deposits in advance, a large number of grandparents could die with an HSA surplus of appropriate size. A large number of children will be born without a standard-issue family and need the money. After the standard-issue cases have been automatically settled, these outliers can be referred to a Court of Equity charged with doing their best. After a few years of this, the results can be referred back to a Committee of Congress to revise the rules.
A basic fact stands out: most newborn children create a healthcare deficit averaging 8% of $350,000, or $29,000, by the time they reach age 21. Most young parents have difficulty funding so much, and so all lifetime schemes face failure unless something unconventional is done to help it. A dozen more or less legitimate objections can be imagined, but seem worth sacrificing to make lifetime healthcare supportable. The main alternative is to pour enormous sums into the government pool, and then redistribute them. I am uneasy about letting the government get deeply mixed into something so personal. So, speaking as a great-grandfather myself, about all that leaves as a potential source of funds, is grandpa, and even grandpas sometimes have an aversion to long hair and rock music.
Multi-year Issues
Lifetime Health Savings Accounts (L-HSA) would differ from ordinary HSA in two major ways, and the first is obvious from the name. In addition to meeting each medical cost as it comes along, or at most managing each year's health costs, the lifetime Health Savings Account would try to project whole lifetimes of medical costs, and make much greater use of compound income on long-term invested reserves. The difference in net income would be quite considerable. The concept seeks new ways to finance the whole bundle more efficiently; one of which is that health expenses are increasingly crowded toward the end of life, preceded by many years of good health, which can build up unused reserves and earn rising rates of income on them. Since the expanded proposal requires major legislation to make it work, it must be presented here in concept form only, for Congress to think about and possibly modify extensively.
This proposal does not claim to be ready for immediate implementation. It is presented to promote the necessary legal (and attitudinal) changes first needed to implement its value. And frankly, a change this large in 18% of GDP is really best phased in gradually, starting with those who feel adventurous. Experience has already shown HSA is most popular with the age group 30-40. By the time the timidest among us have joined up, the transition will have become more predictable. As a first step, let's add another early proposal for the present Congress to consider:
Proposal 17b. Tax-exempt Hospitals Should be Required to Accept the DRG method of payment for inpatients from any Insurer, although the age-adjusted rates should be negotiable based on a percentage surcharge to Medicare rates. The DRG should be gradually restructured, using a reduced SNOMED code instead of enlarged ICDA code, and designed to be used as a Google-like search engine on hospital computers rather than numerical look-ups, except for very common hospital diagnoses.Overfunding and Pooling. Lifetime Health Savings Accounts, besides being multi-year rather than annual, are unique in a second way : they overfund their goal at first, counting on mid-course corrections to whittle down toward the somewhat secondary goal of precision -- amounting to, "spending your last dime, on the last day of your life". To avoid surprising people with a funding shortfall after they retire, we encourage deliberate over-estimates, to be cut down later and eventually added to retirement income. For the same reason, it is important to have attractive ways for subscribers to spend such surpluses, to blunt suspicions the surpluses might be confiscated if allowed to grow. An acknowledged goal of ending with more money than you need runs somewhat against public instincts and is only feasible if surpluses can be balanced with pleasing alternatives.
Saving for yourself within individual accounts is more tolerable than saving for impersonal groups within pooled insurance categories, but nevertheless must constantly defend itself against the administrative urge to pool. Pooling should only be permitted as a patient option, which creates an incentive to pay higher dividends for it. It also eases the concern about confiscation by making it more cumbersome; very likely, inflation is a realistically greater concern. The menace of rising health cost at the end of life induces more tolerance of pooling in older people, whereas small early contributions compound more visibly if pooling is delayed. Young people must be taught the instinctive belief it gets cheaper if you don't spend it. The overall design of Lifetime HSAs is to save more than seems needed, but provide generous alternative spending options, particularly the advantage of pooling later in life. Because it may be difficult to distinguish whether underfunded accounts were caused by bad luck or improvidence, the ability to "buy in" to a series of single-premium steps should, both create penalties for tardy payment, as well as incentive rewards for pooling them. This point should become clear after a few examples.
Proposal 17c: Where two groups, by age or other distinguishing features, can be identified and matched, as permanently in revenue/expense deficit, or surplus, internal borrowing at reduced rates may be permitted between the two groups to the extent they consistently match. Borrowing for other purposes (such as transition costs) shall be by issuing special purpose bonds. These bonds may also be used to make multi-year intra-family gifts, such as grandparents for grandchildren, or children for elderly parents.Smoothing Out the Curve. There is a considerable difference between individual bad luck with health, and mismatches between average costs of different age groups. Let's explain. An individual can have a bad auto accident and run up big bills; as much as possible, the age group should smooth out health costs by pooling within the age cohort to pay the bill. On the other hand, compound investment income follows one curve, while illnesses predominate in bulges on a different curve. It isn't bad luck that concentrates obstetrical and child care costs into a certain age range, it is biology. No amount of pooling within the age cohort can smooth out such a systemic cost bulge, so the reproductive age group will have to borrow money (collectively) from the non-reproductive ones.
With a little thought, it can be seen that subsidies between age groups are actually more nearly fair, than subsidies based on marital status or gender preference, or even employers, who tend to hire different age groups in different industries, and can accordingly game their health costs in various ways. On the other hand, if interest-free borrowing between age cohorts is permitted, there must be some agency or special court to safeguard that particular feature from being gamed. All of these complexities are vexing because they introduce bureaucracy where none existed; it is simply a consequence of using individual ownership of accounts to attract deposits which nevertheless must occasionally be pooled, later. Because these borrowings are mainly intended to smooth out awkward features of the plan, every effort should be made to avoid charging interest on these loans or bonds. However, if gaming of the system is part of the result, heightened interest may have to be charged. Using bonds to borrow between age groups is probably cheaper than constant bookkeeping, and more reassuring about the political risk.
Proposal 17d: A reasonably small number of escrowed accounts within a funded account may be established for such purposes as may be necessary, particularly for transition and catastrophe funding. Where escrowed accounts are established, both parties to an agreement must sign, for the designation to be enforceable. (2606)
Escrowed Subaccounts. Buying Out of Medicare.Both Obamacare and Health Savings Accounts are presently expected to terminate when Medicare begins, at roughly age 65. Nevertheless, we are on the subject of lifetime coverage, where we have a rough calculation of the cost ($350,000) and the Medicare data is the most accurate set, against which to make validity comparisons. We want to start with $350,000 at the expected date of death, spend some of it in roughly 20 installments, and see how much is left for the earlier years of an average life. Then, we repeat the process in layers down to age 21 and hope the remainder comes out close to zero. There are several things missing from this, most notably how to get the money out of the fund, but let's start with this much, in isolation for the Medicare age bracket, age 66-85, more or less. For simplicity, we are going to assume a single-premium payment at age 66, which both life expectancy and inflation in the future will increase in a predictable manner, while changes in health and health care eventually reduce healthcare costs, not increase them. Not everyone would agree to the last assumption, but this is not the place to argue.
We know:
(a) The average cost of Medicare per year ($10,900)
(b) How many years the beneficiaries on average are in the age group (18).
(c) Therefore, we know how much of the $350,000 to set aside for Medicare ($196,200),
(d) And know how much a single premium at age 65 would have to be, in order to cover it. ($196,000 apiece)
(e) We thus know how much all the working-age groups (combined as age 21 to 66, 60% of the population) must accumulate, in advance for their own health care costs, when they reach Medicare age($196,000 apiece).
(f) And by subtraction therefore how much is left for personal healthcare within ages 21 to 66 ($128,800).
(g) We can be pretty certain average Medicare costs will exceed those of anyone younger, setting a maximum cost for any age.
Shifts in the age composition of the population will produce very large changes in total national costs in any given year, but should by themselves not change the average lifetime costs. What they may do soon is increase the proportion of the population on Medicare, thereby paradoxically making both Obamacare and Health Savings Accounts relatively less expensive. Obamacare can predict its future costs with information already available. But the Health Savings Account must still adjust its net future costs for whatever income is produced by investments. We don't yet know is how much each working person must contribute each year, because we haven't, up to this point, yet offered an assumption about the interest rate they must produce. Let's construct a table of the outcome of what seems like reasonable income results. There are four relevant outcomes to consider at each level: the high, the low, and the average. Plus, a comparison with what Obamacare would cost. But there are two Medicare costs: the cost from age 21 to 66, and the cost from 67-85, advancing slowly toward a future life expectancy of perhaps 91-93. These two estimations are necessary for displaying the relative costs of Medicare and also Obamacare.
Someone is sure to notice the apportionment for children is based on income rather than expenses. The formula can be adjusted to make that true for any age bracket, and a political decision must be made about where to levy assessments if income is inadequate; we made it, here. We have repeatedly emphasized that if investment income does not match the revenue requirement, at least it supplies more money that would be there, without it. Somewhat to our surprise, it comes pretty close, and we have exhausted our ability to supply more. Any further shortfalls must be addressed by more conventional methods of cost-cutting, borrowing, or increased saving. In particular, attention is directed to the yearly deposit of $3300 from age 25-65, which is what the framers of the HSA enabling act set as a limit, perhaps arbitrarily.
And finally but reluctantly, the figures include provision for phasing out Medicare, which everyone treats as a political third rail, untouchable. But gradually as I worked through this analysis, I came to the conclusion that uproar about medical costs is never likely to come to an end until the Medicare deficit is somehow addressed. I believe we cannot keep increasing the proportion of the population on Medicare, paying for it with fifty-cent dollars, and pretending the problem does not exist. So it certainly is possible to balance these books by continuing our present approach to Medicare for a while. But it would be a sad opportunity, lost. In summary, we have concocted a guess of the outer limit of what the American public is willing to afford for lifetime health coverage ($3350 per person per year, from age 21 to 66), and added an estimate of compound income of 6% from passive investing, to derive an estimate of how much we can afford. From that, we subtract the cost of privatizing Medicare if our politicians find the courage for that ($196,000) and thus derive an estimate of how much is available for health care of the rest of the population ($128,000).
No doubt, data from the Obamacare program will soon reveal some information, but it will derive from a non-representative sample group. It would seem dangerous at this point to use data from that source to make a judgment about the soundness of this one. Because of the longer time spans available for compound income, at 6% it would actually cost more out-of-pocket to finance the $128,000 than the $196,000; it would actually be financially better to do it. The non-investment cost would only be small, for an expense which otherwise seems almost insurmountably crowding out everything else in the national budget.
What remains is to see if it is possible to finance the average healthcare of younger people with a budget of $128,000. All told, we could foresee a limit of a dollar a day for life, but that would assume using all of the revenue-enhancements together. If for no other reason, a slow transition would make this unrealistic.
Public Misconceptions
(Healthcare for Citizen Lobbyists)
There are a few other ideas about the cost of medical care, which I would say are widely held, but the truth of which seems dubious. In fact, I would characterize them as misconceptions. If misconceptions are held long enough, they eventually work their way into the tax code.
Is Preventive Medicine Always and Everywhere Less Expensive? As heads nod vigorously in support of prevention, please notice in general usage it suggests several different things. The overall implication is that small interventions for everyone are less expensive to society; less expensive, that is than large expenses for the few who get the disease. That is clearly not invariably the case, and unfortunately, in a compulsory insurance world, it may seldom be the case. The point is not that preventive care is a bad thing, because it is often a very good thing, even by far the very best thing. It's just not necessarily cheaper.
Take for example a tetanus toxoid booster, which ten years ago cost less than a dollar for the material. Recently in preparation for a vacation trip, I was charged $85 dollars by my corner drugstore, just for the material. If you do the math, $85.00 times millions of Americans is a far greater sum than the present aggregate cost of Americans actually contracting tetanus, especially following the advice to have a booster shot every ten years. This becomes more certain if one adds in the cost of administration. The vaccine is quite effective, Americans had almost no cases in the Far Eastern Theater in World War II. The British who did not vaccinate routinely had large numbers of often fatal cases. Furthermore, even if the tetanus patient survives, the disease is hideously painful. Is it better to immunize routinely? Yes, it is. Is it cheaper? I'm not entirely sure, because I have no access to the production costs of tetanus toxoid. But it certainly seems likely it isn't cheaper. Malpractice costs, which are a different issue entirely, complicate this opinion.
|
Better, yes. Cheaper? No.
|
| Preventive Medicine |
Something, probably malpractice liability, has transformed an effective preventive procedure from clearly cost-effective to -- probably not cheaper for a nation which no longer has horses on the streets, but still has horses on farms and ranches. This is presently mostly a malpractice liability problem for the vaccine maker, not a preventive care issue. Take another well-known example. In the case of smallpox vaccination, it is now clearly more expensive to vaccinate everyone in the world than to treat the few actual cases. The waffle currently being employed is to limit vaccination to countries where there are still a few cases, hoping thereby to eradicate the disease from the planet.
Over and over, an examination of individual vaccinations shows the answer to be: better, yes, cheaper, no; with the ultimate answer depending on accounting tricks in the calculation of cost, cost inflation because of third-party payment, and related perplexities. To be measured about it, excessive profitability of some preventive measures could act as a stimulant for finally calling off prevention, by taking on a briefly more expensive campaign to achieve final eradication. Somewhere in this issue is the whisper that "natural" gene diversity of any sort must never be totally eliminated, a viewpoint which even the diversity philosopher William James never openly extended to include virulent diseases.
Routine cervical Pap tests, routine annual physical examinations, routine colonoscopies and a host of other routines are in general open to questioning as to cost-effectiveness. The issue is likely to increase rather than go away. Much of the current denunciation of "Cadillac" health insurance plans focus on the elaborate prevention programs enjoyed by Wall Street executives, college professors, industrial unions, and other privileged health insurance classes. A more useful approach to a borderline issue might focus on removing such items from health insurance benefit packages, particularly those whose cost is subsidized, either directly or by income tax deductions. Those preventive measures which demonstrate cost-effectiveness can have their subsidy restored, or be grouped together into a category which must compete for eligible access to limited funds.
The inference is strong that unrestrained substitution of community prevention for patient treatment escalates costs rather considerably, and -- at the least -- needs to demonstrate more cost-effectiveness before subsidy is extended. While self-interest is a possibility if only physicians are consulted, total reliance on bean-counters could eliminate benevolent judgment entirely. Community cost effectiveness is a ratio, and both sides must be fairly argued. Don't forget many people quietly recognize the need for gigantic cost-shifting between age groups. Spending money on young workers to pay for shots is one way to shift the cost of elderly illness, backward to the employer they no longer work for. It can be a pretty expensive way to do it.
In the final analysis, without some form of patient participation in the cost, this issue is probably unsolvable. To launch a host of double-blind clinical trials to find out the truth will lead to answers of some sort, which will quickly be undermined by price/cost confusion, leading to increasingly futile regulation. Including preventive costs in the deductible at least allows public participation in the decisions and true balance to begin; which is to say, even universal preventive care admiration cannot be adequately assessed except in the presence of a substantial open market for the product.
Much "preventive" care is really "early detection" or "early management". That's entirely different. When the goal changes so subtly, it is often not possible to judge what is worthwhile, except by placing some price on pain and suffering. The abuse by the trial bar of the monetization of pain and suffering in the malpractice field, ought to be a gentle reminder of that. Preventive colonoscopy has clearly caused a decline in deaths from colon cancer; that's a medical judgment and a transitional one. Whether the cost of catching those cancers early was cost-effective is largely a matter of colonoscopy cost, and on digging into it, will be found to be as much an anesthesia issue as a colonoscopist one. In any event, it is not one where the opinion of insurance reviewers should be decisive. If the litigation industry moves to make an omission of prevention a new source of action, it will surely be a sign it is a past time, to caution the public about the direction of things.
 Average Hospital Profit Margins: Inpatient 2%, Accident Room 15%, Satellite Clinics 30%
|
| Payment By Diagnosis |
Outpatient is Not Necessarily Cheaper Than Inpatient For the Same Problem. Medicare provides half of the hospital revenue; the other half is often dragged into a uniform approach. The reimbursement mostly has nothing to do with the itemized bills hospitals send and may have little to do with production costs. The DRG (Diagnosis-Related Groups) system for reimbursing hospitals for inpatients is thus not directly based on specific costs in the inpatient area. It is related to clustered diagnoses lumped into a DRG group, and then assumes overpayments will eventually balance underpayments within individual hospitals.
That last point, depending on the Law of Large Numbers, is questionable, and especially so in small hospitals. When two million diagnoses are condensed into 200 Diagnosis groups, group uniformity just has to be uneven. Reimbursement means repayment, but this interposed step often interferes with that definition. Someone in the past fifty years discovered the reimbursement step was an excellent choke point. Manipulating the reimbursement rates without changing the service is a handy place to choose winners and losers; it's largely out of sight of the people who would recognize it for what it is. Furthermore, for various DRG groups, or for all of them, it becomes possible to construct a fairly tight rationing system for inpatient costs.
The degree to which actual production costs match a particular DRG reimbursement rate is blurred by inevitable imprecision in the DRG code construction. It is impossible to squash a couple of million diagnoses into two hundred code numbers without imprecision. It works both ways, of course. The coders back at the hospital will seek weaknesses out, experimentally. A grossly generalized code is placed in the hands of hospital employees, resulting in a system which suits both sides of the transaction, but is one which ought to be abolished, on both sides, by computerizing the process. At least, computers could avoid the issue of mistranslating the doctors' English into code.
The overall outcome with Medicare is an average 2% profit margin on inpatients during a 2% national inflation. This is far too tight to expect it to come out precisely right for everybody. And in fact, inflation has averaged 3% for a century but is 1.6% right now. The Federal Reserve Chairman desperately tries to raise it, but it just won't go up. If you don't think this is a serious issue, just reflect that our gold-less currency is supported by a 2% inflation target which the Federal Reserve is proving unable to maintain.
For technical reasons, the same forced loss is not true of outpatient and emergency services, which usually use Chargemaster values. Emergency services are said to approximate 15% profit margins, and outpatient services, 30%. It is therefore difficult to believe anyone would start anywhere but the profit margin, and work backward to managing the institution. In consequence, the buyer's intermediary has stolen the pricing process from the seller. Without the need to communicate one word, prices rise to the level of available payment and then stop there. But let's not be too specific in our suspicions. Some incentive to direct patients to the emergency and outpatient areas must develop, and is acted upon in the pricing. It just doesn't have to be so confusing and so high-handed.
Any assumption by the public that outpatient care is cheaper than inpatient hospital care is likely to be quite misleading. Short of driving the hospital out of business, revenue in this system is whatever the insurance intermediary chooses to make it. There was a time when the intermediary was Blue Cross, and behind them, big business. Nowadays, it is Medicare, but Obamacare probably aspires to the turf.
Let's test the reasoning by using different data. Because hospital inpatient care is reimbursed at roughly 106% of overall cost, while hospital outpatient care is reimbursed at roughly 150%, hospitals are impelled to favor outpatient care, no matter which type of care happens to have the cheapest production cost, the best medical outcomes, or enjoys the greatest comforts. Instead, the rates and ratios are ultimately determined by magazine articles and newspaper editorials. At some level within the government, a political system responds to what it thinks is public opinion, vox populi est vox Dei. No matter what their personal feelings may be, hospital management encounters more quarrelsomeness on wages in the inpatient area, less resistance in the outpatient and home care programs. So, true costs must actually rise in the outpatient area, sooner or later, following the financial incentives. Personnel shortages follow, as does friction between hospitals and office-based physicians. The process is circular, but the origin of favoring outpatient care over inpatient care was primarily driven by some accountant reading a magazine article.
A highly similar attitude underlies the hubbub for salaried physicians rather than fee-for-service. It's a short-cut to a forty-hour week, and following that, to a doctor shortage. And following that, to enlarged medical school budgets. If anyone imagines that will save money, the reasoning is obscure.
Everybody can guess what it costs to wash a couple of sheets and buy a couple of TV dinners. Everyone fundamentally understands Society's need to transfer medical costs from the sick population to the well population. Nothing known about hotel prices justifies a 50% difference in price between inpatient and outpatient care, all else being equal. The room price mainly supports overhead costs which are unrelated to direct patient care, so those fixed costs are like migratory birds, settling to roost where it's quiet. Remember, it doesn't cost driving the system, it is now profit margins.
The Return of a Discharged Hospital Patient Within 30 Days is not Necessarily a Sign of Bad Care. Rather, it reflects the fact that hospital inpatient reimbursement is entirely based on the bulk number of admissions, not the sum of itemized ingredients. Having undermined fee for service, Medicare must resort to taxing the whole admission.
Early re-admission can, of course, be a sign of premature discharge or careless coordination with the home physician. But these issues are so remote from the basic reason for admission, that bulk punishment is unlikely to change the criticized behavior. That behavior may mean a convalescent center is convenient to a hospital, making it reasonable to move the patient without much loss of continuity of care; and treating his return to the acute facility becomes a matter of small consequence. It is also a matter of cost accounting; when you claim a hundred dollar hotel cost to be worth thousands of dollars, many distortions are inevitable. If a hospital essentially shuts down on weekends, for example, there actually might be better care available somewhere else.
Imposing a penalty for returns to the hospital post-discharge has certainly changed behavior, but it is far from clear whether institutions are better as a result. Without a detailed study of longitudinal effects and costs, this threat is no more than an untested experiment. Without access to accounting practices, doctors assume the penalty for a high re-admission rate merely affirms that hospital insurance reimbursement by DRG is solely dependent on the discharge diagnosis, therefore bears little relation to the quality of care. Given a particular diagnosis, reimbursement is totally independent of any other cost. When all you have is a hammer, everything looks like a nail to the DRG.
The legitimate reasons for re-admission to the hospital are many and varied. Collectively, they could well constitute a general attitude on the part of a particular hospital that it is reasonable to send many patients home a little early in order to achieve greater overall cost savings -- in spite of sustaining a few re-admissions. But this is somewhat beside the point. The insurance companies accept the fallacy that favoring readmission is the only way a hospital can increase reimbursement under a DRG system. This is merely a debater's trick of redefining the issue, from true cost to reimbursement amount. More or fewer tests, longer or shorter stays have no effect, but readmission can double reimbursement. Consequently, re-admission has been stigmatized as invariably signifying careless treatment, justifying a penalty reduction of overall reimbursement. This is high-handed, indeed. It would require a research project to determine which of the alleged motives is actually operational.
The Doughnut Hole: Deductibles versus Copayments. To understand why the doughnut hole is a good idea, you have to understand why copay is a flawed idea. In both cases, the purpose is to make the patient responsible for some of the cost in order to restrain abuse. As the expression goes, you want the patient to have some skin in the game. The question is how to do it; the doughnut has not been widely tried, but the copayment approach is very familiar: charge the patient 20% of the cost, in cash.
This co-pay idea finds great favor with management and labor in negotiations because the premium savings are immediately known. If the copayment is 10%, then employer cost will be decreased by 10%; if it is 50%, the cost is reduced by 50%. In midnight bargaining sessions, such simplicity is much appreciated. However, the doughnut hole was not devised to make negotiations simpler for group insurance, it was devised to inhibit reckless spending, theoretically unleashed once the initial deductible has been satisfied.
Health insurance companies also like both co-pay and doughnuts for questionable reasons. Both offer an opportunity to sell two insurance policies as two pieces of the same patient encounter, adding up to 100% coverage, but eliminating the patient's skin in the game. Doubling the marketing and administrative fees seems like an advantage only to an insurance intermediary, while it totally undermines the incentive of restraining patient overuse. In practice, having two insurances for every charge has led to mysterious delays in payment of the second one, even though they are often administered by the same company. Physicians and other providers hate the system, not only because it involves two insurance claims processes per claim, but because it often makes it impossible to calculate the residual after insurance, i.e., patient cash responsibility, until months after the service has been rendered. Patients often take this long silence to imply payment in full, and disputes with the provider are common. Long ago, older physicians warned the younger ones, "Always collect your fees while the tears are hot."
It has long been a mystery why hospital bills take so long to go through the system; at one time, protracting the interest float seemed a plausible motive. However, the persistence of delayed processing during a period of near-zero interest rates makes this motive unlikely. It now occurs to me that the reimbursement of health insurance costs by the business employer is related to corporate tax payments, and hence to the quarterly tax system. Using the puzzling model of a monthly bank statement for online reporting would have some logic, but great confusion, attached to the bank statement approach for group payment utility. But in the end, I really do not understand why health insurance reimbursement or even reporting to the patient, should take so many months, and cause so much difficulty. Recently, the major insurance companies have started to imitate banks by putting the monthly statement continuously online on the Internet. If doctors find a way to be notified, the billing cycle could be speeded up considerably, and even the deplorable custom of demanding cash in advance may abate. The intermediaries probably won't do it, so it is a business opportunity for some software company, and a minor convenience for the group billing clerk.
So, the idea of a doughnut hole was born, after empirical observation about what was owed on two levels, one for small common claims, and another for big ones. Formerly, the patient either paid cash in full or was insured in full, so arriving at the Paradise of full coverage is purchased in cash within the first deductible. Unfortunately, once that last threshold was crossed, the sky became the limit. Some way really had to be found to distinguish between extravagant over-use, and the use of highly expensive drugs, particularly those still under patent protection. The idea was generated that if the two levels of the doughnut hole were calculated from actual claims data, there might often be a clear separation of minor illnesses from major ones. Since the patient would ordinarily be uncertain how far he was from triggering the doughnut hole, the restraint of abuse might carry over, even into areas where the facts were not as feared.
It is too early to judge the relative effectiveness of the two different patient-responsibility approaches, but it is not too early to watch politicians pander to confusion caused by an innovative but unfamiliar approach, while the insurance administrators simplify their own task by applying a general rule, instead of tailoring it to the service or drug. And by the way, the patients who complain so bitterly about a novel insurance innovation, are deprived by the donut hole of a way to maintain "first-dollar" coverage, which is a major cause of the cost inflations they also complain so much about. Some people think they can fix any problem just by loudly complaining about it. Perhaps, in a politicized situation, it works; but it doesn't fool anyone.
Plan Design. The insurance industry, particularly the actuaries working in that area, have long and sophisticated experience with the considerations leading to upper and lower limits, exclusions and exceptions. Legislative committees would be wise to solicit advice on these matters, which ordinarily have little political content. However, the advisers from the insurance world have an eye to bidding on later contracts to advise and administer these plans. They are not immune to the temptation to advise the inclusion of provisions which invisibly slant the contract toward a particular bidder, and failing that, they look for ways to make things easier, or more profitable, for whichever insurance company does get the contract. The doughnut hole is a recent example of these incentives in action; no member of any congressional committee was able to explain the doughnut for a television audience, so it was ridiculed. The outcome has been a race between politicians to see who could most quickly figure out a way to reduce the size of the hole. The idea that the size of the hole was intended to be an automatic adjustment to experience, seems to have been totally lost in the shuffle. Asking industry experts for advice is fine, but it would be well to ask for such advice from several other sources, too.
Fee-for-Service Billing. In recent years, a number of my colleagues have taken up the idea that fee-for-service billing is a bad thing, possibly the root of all evil. Just about everyone who says this, is himself working for a salary; and I suspect it is a pre-fabricated argument to justify that method of payment. The obvious retort is that if you do more work, you ought to be paid more. The pre-fabricated Q and A goes on to reply, this is how doctors "game" the system, by embroidering a little. I suppose that is occasionally the case, but the conversation seems so stereotyped, I take it to be a soft-spoken way of accusing me of being a crook, so I usually explode with some ill-considered counter-attack. My basic position is that the patient has considerable responsibility to act protectively on his own behalf. That is unfortunately often undermined by excessive or poorly-designed health insurance. Nobody washes a rental car, because that's considered to be the responsibility of the car rental agency. A more serious flaw in the argument that we should eliminate the fee for service, was taught me in Canada.
When Canada adopted socialized medicine, I was asked to go there by my medical society, to see what it was all about. That put me in conversation with a number of Canadian hospital administrators, and the conversation skipped around among common topics. Since I was interested in cost-accounting as the source of much of our problems, I asked how they managed. Well, as soon as paying for hospital care became a provincial responsibility, they stopped preparing itemized bills. Consequently, it immediately became impossible to tell how much anything cost. The administrator knew what he bought, and he paid the bills for the hospital. But how much was spent on gall bladder surgery or obstetrics, he wouldn't be in a position to know.
So I took up the same subject with the Canadian doctors, who reported the same problem in a different form. Given a choice of surgical treatment or a medical one for the same condition, they simply did not know which one was cheaper. After a while, the hospital charges were abandoned as a method of telling what costs more, and eventually, no effort was made to determine comparative prices at all. There's no sense in an American getting smug about this, because manipulation of the DRG soon divorced hospital billing charges from having any relation to underlying costs, and American doctors soon gave up any effort to use billing as a guide to treatment choices. We organize task forces to generate "typical" bills from time to time, but these standardized cost analyses are a crude and expensive substitute for the immediacy of a particular patient's bill.
My friends in the Legal Profession make a sort of similar complaint. The advent of cheap computers created the concept of "billable hours", in which some fictional average price is fixed to a two-minute phone consultation. In the old days, my friends tell me, they always would have a conference with the client, just before sending a bill. The client was asked how much he thought the services were worth to him, and often the figure was higher than the actual bill. In the cases where the conjectured price was lower, the attorney had an opportunity to explain the cleverness of his maneuvers, or the time-consuming effort required to develop the evidence. A senior attorney told me that never in his life did he send a bill for more than the client agreed to pay, and he was a happier man for it. Naturally, the bills were higher when the attorney won the case than when he lost it, which is definitely not the case when a hospital is unsuccessful in a cancer cure. Similarly, you might think bills would be higher if the patient lived than if he died, but income maximization always takes the higher choice. So the absence of this face-to-face discussion is a regrettable one in medical care, as well.
Martin Feldstein Does It Again: Eliminate Tacit Tax Exemption for 70% of Workers Denied To the Rest
Headlines in the Wall Street Journal announced collapse of Congressional healthcare reform. In the same edition, a small short article buried in its depths described a possibly major step toward its reform. Martin Feldstein calmly observed, a tax exemption for healthcare insurance of 2.9% really amounts to a wage increase whose elimination might go a long way toward paying for the eighty-year mess Henry J. Kaiser had created. (In fact, it was effectively taxable income of 4%.)
It was all so simple: healthcare extended longevity, created thirty years of new retirement cost. In turn, exempting the premium for healthcare became a tax-exempt increase in wages -- for the 70% of employees getting insurance as a gift. Maybe not at first, but wages adjust to expect it during eighty years. Social Security could not cope with an extra thirty years, so SSA was going broke, while health insurance was actually the main cause of increased longevity.
But notice how unused Health Savings Accounts automatically turn into retirement accounts (IRAs) for Medicare recipients. So if you are lucky and prudent with healthcare, or if you overfund an HSA, unused healthcare money makes a reappearance in retirement funds where it belongs. If you have used up the money, you have probably been sick, and maybe won't need so much for a shortened retirement. Increasingly, expensive healthcare hits the elderly hardest, so there are many years during which compound interest overcomes inflation. At the rate things are going, retirement may become four times as expensive as Medicare, so let's consider that future.
Medicare doesn't save its withholdings, it uses "pay as you go" and spends the money on other things, like battleships. Therefore, to make any use of this windfall, it is necessary to save it, invest it, and use it for retirement. Just doing that much might redirect the other 30% of the withheld tax to its intended purpose. So the economic effect would be considerable, just by stirring around in that corner of it.
14 Blogs
Waiting for Roberts
Some ruminations about health financing, written while we wait for the Supreme Court to announce its decision on v.
Better, but More Complicated: Lifetime HSAs
Start with a Health Savings Account (a tax-exempt IRA with catastrophic insurance backup, payable only for Healthcare). Add a concept: add other age groups, like working people (26-65) who indirectly pay almost all health costs and children. We try to integrate this pattern into a lifetime health insurance design:
Obstetrics and Pediatrics through age 25 are really special loans from parents to children, usually not repaid.
Medicare, on the other hand, owes an unpaid debt for their 50% subsidy. Failure to recognize the subsidy tempts the public to extend it with "Single payer" disasters. Public education is the first, and rather major, a step toward fixing this before it ruins us.
(www.philadelphia-reflections.com/blog/2606.htm)
Healthcare, A Much Simplified Overview
Flies in the Ointment
New blog 2015-06-22 20:58:14 description
Spending Rules--Same Purpose As Escrow Accounts
Invisibly, a corporate spending rule is a way to increase the size of the reserve fund.
Escrow Accounts for Future Needs.
Within a Health Savings Account, it is necessary to have some nest eggs that the subscriber can touch, but he would rather not. And other accounts which are borrowed, which ought to be paid off, first. That's just the way life is, of course, but it's better to keep escrow accounts, to indicate different designated purposes.
Using Escrows to Estimate Cost Risks(1)
New blog 2015-06-24 22:19:01 description
Using Escrow to Estimate Health Costs (2)
New blog 2015-06-24 23:51:23 description
Lifetime Health Insurance: Monitoring the Data
Cost is the Big Issue, But Here's Another
Ne
Paying for the Healthcare of Children
New blog 2015-02-18 20:16:10 description
Multi-year Issues
New blog 2015-06-20 17:45:55 description
Martin Feldstein Does It Again: Eliminate Tacit Tax Exemption for 70% of Workers Denied To the Rest
The Henry Kaiser tax exemption for health would pay toward Social Security, indirectly paying for retirement, which health insurance prolonged.