6 Volumes
Constitutional Era
American history between the Revolution and the approach of the Civil War, was dominated by the Constitutional Convention in Philadelphia in 1787. Background rumbling was from the French Revolution. The War of 1812 was merely an embarrassment.
Health Reform: Children Playing With Matches
Health Reform: Changing the Insurance Model
At 18% of GDP, health care is too big to be revised in one step. We advise collecting interest on the revenue, using modified Health Savings Accounts. After that, the obvious next steps would trigger as much reform as we could handle in a decade.
Second Edition, Greater Savings.
The book, Health Savings Account: Planning for Prosperity is here revised, making N-HSA a completed intermediate step. Whether to go faster to Retired Life is left undecided until it becomes clearer what reception earlier steps receive. There is a difficult transition ahead of any of these proposals. On the other hand, transition must be accomplished, so Congress may prefer more speculation about destination.
Handbook for Health Savings Accounts
New volume 2015-07-07 23:31:01 description
Consolidated Health Reform Volume
To unjumble topics
(1) Obamacare: Spare Parts for a Book
Maybe these should have been included, but it was decided to leave them out.
Health Reform: Seen On the Mass Media
Both political parties in the 2008 election promised to revise healthcare financing and delivery; the nation was restless. It had been restless since a Republican Congress swept Newt Gingrich to Speaker in 1994. It soon swept him back out of power, but its ability to surprise reappeared in 2010 with Republican Senator Scott Brown's election to Edward Kennedy's seat, and then there was the 2012 Republican Congressional landslide, -- but on the other hand there was President Obama's 2012 re-election. One electoral mandate after another, often sending opposite signals. Only a King is allowed to be capricious, nations are described as undecided. When Democrat Barack Obama won his first election in 2008, a concrete proposal was eagerly awaited because it seemed likely to be radical; it disappointed because it merely overpromised. He neglected the iron rule for leadership: underpromise but overdeliver. In order to retain a free hand, the working elements of Obamacare were never concisely stated; in America, that is usually a misjudgment. After enactment, details can no longer escape systematic examination for what they are, and what they omit. We got rid of our King more than two hundred years ago. Capricious behavior is out of fashion. Over-deliver, that's the thing.
Political strategists calculate sweeping changes have the best chance of approval immediately after a new president takes office. But for the Affordable Care Act, that slogan may still have been true but mis-timed; since overly brief sequencing gave interest groups responsible for Obama's election undue influence over the proposal, with an undue sense of mandate from the elections they won. The resulting legislation, the Affordable Care Act, is heavily slanted toward rewarding the base, and the base expected a reward. With its momentum up, organized Labor, blacks and Hispanics displayed impatience about mitigating features the rest of the nation objected to. As Lyndon Johnson once said, the majority of Americans are non-black and non-poor. Political misjudgment increasingly characterizes Obamacare, which at first seemed so smart about politics..
Thousands of pages of uncoordinated proposals had emerged from four congressional committees in 2010, confusing the public about what the basic proposal was, and making it uncomfortably obvious that the congressmen themselves had neither written nor properly digested it. It was announced as a proposal to expand coverage to the whole population, uncharacteristically saving the resulting cost by eliminating waste and overutilization in medical care. That appealed to the public. But without more explanation about how these goals would be achievable, in fact, whether the premises were accurate, the public could not see how to program expansion and cost reduction were consistent, or how these two thousand pages made them so. Universal health insurance was said to be mandated, but in fact, it doesn't say so. What it says is everyone has a choice between insurance and a small tax. Anyone with a pencil knew what to do next.
Furthermore, the public could not see what urgency justified delivering a stack of paper to congressional authorizing committees in the morning and demanding an affirmative vote in the afternoon of the same day. Consequently, the conviction took hold that what was proposed would end up being a massive cut in Medicare benefits to pay for it. Soon after the voluminous bills were released, the Congressional Budget Office (CBO) further undermined trust in the proposal by announcing its assessment that it would add a trillion dollars to health costs in ten years, but still would only extend new insurance to about half of the uninsured population. That didn't sound like universal coverage at no added cost, at all. Furthermore, the CBO had credibility, in fact, was the only credible agency that had actually studied this massive legislation. The President immediately appeared on television, endlessly repeating the promise that the extra cost would not add one dime to the public debt. Therefore, fear of large impending Medicare cuts had to be entirely plausible if you believed anything the man said. The public uproar about an implausible idea thus became general before members of Congress had time to read it or devise soothing explanations; their floundering upset the public even more.
To rescue the deteriorating situation, the President attempted to go directly to the public with weeks of daily speeches. On one Sunday he appeared personally on five television talk shows. Naturally many speeches were ghost-written, containing misstatements or exaggerations, with the result that the harried President next resorted to heated oratory that would have been excessive even on the campaign trail. He was criticized as using rabble-rousing, undignified for a sitting President. Failing into a "trust me" approach, he actually was left with the difficult choice of withdrawing the proposal or being seen to ram it through Congress on a party-line vote. Party-line enactments of controversial legislation tend to justify the opposition party into repealing a controversial law just as soon as they return to power.
With the public bewildered as to what the proposal really was, enacting something certain to be reversed was even more unappealing. The alternative, a humiliating withdrawal of the proposal, seemed intolerable to its strongest supporters in the base. But reversal did not seem unreasonable to independent voters, who had wondered all along why there was such haste. The nation was fighting two international wars, both of them going bad, and was in the deepest economic recession since 1937. What's the hurry with this healthcare thing? It was a reasonable question, and the President did not help himself by darkly accusing opponents of delaying tactics.
* * *
In this analysis, the following three sections address 1) the proposal and its own flaws, particularly the savage strategy for getting enacted. 2) The growing consequences of flaws in health financing which had long pre-existed Obamacare and 3) An improved proposal, not so much radical, as extensive. For a century, conservative proposals of all sorts have been incremental, creating opportunities for mid-course corrections. Often denounced as hesitant and timid, a grand strategy often takes more time than a pitched battle, but usually advances farther and more enduringly.
Chicago Sauce on an Arkansas Turkey
Presumably, the proposers of affordable health coverage considered the approach of making it affordable through making it cheaper. Unfortunately, "affordable for every American" is so expansive that some people, somewhere, would require extra subsidy no matter how much prices were cut. Obamacare's supporters would be bitter to discover a two-class system, with them in second class. It did not take long to see how unpopular cutting existing programs would be, first with providers and then with provides. And then Obama advisors must have developed a greater understanding that existing internal hospital cost-shifting meant: Medicare was already subsidizing Medicaid, while the private sector had really been subsidizing the indigent care that Medicaid excluded. The savings to government costs (of universal coverage) were not going to be nearly as much as had been imagined.
So, a subsidy program was required. In addition, ensuring illegal immigrants during high unemployment was seriously unpopular, particularly in border states like Texas, where uncompensated care was already hard to manage. So we can easily imagine how the proposal emerged as: "Affordable health coverage for all Americans (legal residents only) achieved by giving cash subsidies ("refundable tax credits") to lower income groups, and expanding Medicaid coverage above its former income threshold". That wouldn't be a catchy political slogan, but it would be precise.
Such patchwork necessarily made it harder to comprehend. Somewhere in its evolution someone also seems to have determined to rescue Medicare from its impending bankruptcy -- while we are at it, let's fix Medicare. However both ideas, universal coverage and restructuring Medicare solvency, would be expensive; combining them might make the package unsupportably expensive in a recession, but it might also create more opportunity for major progress.
 Affordable health coverage for all Americans (legal residents only) was to be achieved by giving cash subsidies ("refundable tax credits") to lower income groups while expanding Medicaid coverage limits to include them. A universal mandate for coverage, (but only our way, or the highway.) 
|
| Obamacare Capsulized |
The Obama administration seemed to follow the same path. Modifying the pathway to a Budget Reconciliation Committee added the novel advantage of avoiding the Senate's 60-vote anti-filibuster rule, thus requiring only a simple majority to pass the Senate when it returned. It still needed 60 votes in the Senate to prevent a filibuster on the initial round, so the original Senate contribution to the conference committee had to contain a lot of goodies, just to get to the conference committee -- in order to be dropped.
In the flurries of lobbying activity, hospital advocates have suggested uninsured patients just appeared at hospital accident rooms, effectively causing other patients to subsidize them. That was somewhat true, but extending the idea to a claim the government was already paying for all indigent care, was a stretch because hospital cost-shifting was laying most of the cost on the private sector. To go further and proclaim that including indigent care under the insurance coverage umbrella would thus be cost-free, did really strain the facts. How could it be cost-free and still cost a zillion dollars? Right from the start, this proposal was making itself hard to defend.
|
The sound-bite is: the Obama health reform proposal of 2009 will extend affordable health insurance to poor Americans (citizen), and save Medicare from ruin by cutting costs. Because this still won't pay the bill, the rest of the nation must get less coverage for more cost.
|
So, at the end of September 2009, the country confronted multiple thousand-page bills from the House of Representatives containing wide assortments of liberal ideas, and a more conservative Senate proposal from Senator Baucus (D, Montana) representing the views of the Democratic caucus within the Senate Finance Committee. The British magazine The Economist promptly snorted; Senator Baucus' bill was "Half a loaf, half-baked." Since laws passed by strict party votes are in danger of prompt reversal when the other party next gains majority control, Senator Baucus had been struggling to achieve some Republican support but apparently decided bipartisanship was not worth the delay. In any event, the Senate's assignment was to get past a filibuster; the real zingers could come from Nancy Pelosi's House bill. Andy Stern the labor leader, had appeared on a television show offering no arguments at all, merely demanding a vote be taken instantly, presumably before public support eroded. Moderate House Representatives are characteristically most concerned with being turned out of office after passing a controversial proposal because they face election every two years. The much more liberal leadership of the House, with seniority because of their safe gerrymandered seats, are however more likely to honor extreme partisan demands. With a safe Democratic majority of the House, a few moderates could be spared to "vote their conscience".
Because the Senate thinks of itself as the sensible, deliberative body, oversight of law remains with its originating committee, to preserve the connection to the "intent of Congress". Because Medicare and Medicaid are amendments to the Social Security Act, the Senate Finance Committee has maintained jurisdiction over these three social benefit programs. A "unified budget" made it easier to shift one program's surplus to cover another's deficit. In the House, with turnover every two years, continuing oversight is mostly assumed by the Appropriations Committee, on the grounds that this is the only committee which reviews every ongoing program, every session. But the realities of the program mix with the quirks of the Senate, and for over forty years whatever the Finance Committee says about Medicare, pretty much goes. During the fall of 2009, this group of old colleagues could be seen on C-Span, gently joshing each other, and even more genially suggesting their disagreements. Each member of Finance belongs to several other committees, but on Medicare, they know their stuff and have a loyal staff to remind them of what they have forgotten. They considered 550 amendments to Obamacare, and stubbornly defended the right of each committee member of either party to be heard courteously, in spite of what must have been a wild frenzy of pressure by unions and other partisans, to be done with it. Their patient labors turned up one issue that party leaders -- especially the Governors -- probably wish they had left alone.
|
Blow away the smoke. Obamacare is about fixing Medicaid without admitting who, or what, caused it to need fixing.
|
| The nut of the matter. |
The fifty Medicaid programs are a big mess. They are run by state governments with Federal provision of at least 57% of the funds, and in some cases over 80%. Some states offer eligibility to those with incomes at only half of the poverty level, others go to several times the poverty level. Their tendency is to use the HMO model of healthcare delivery, but it is an individual state option. Minority groups absolutely hate HMO. The fraud level in Medicaid is by far the largest in the whole government. The quality of care is uneven, but it is always going to be somewhat substandard since it pays well below cost and deals with high-crime populations, amid uncomprehending chronic poverty. It attempts to deal with the deplorable psychiatric inpatient problem, which is in its present condition because of bungled regulation. Medicaid under-reimbursement is the main cause of hospital cost shifting, which causes still other distortions. And so on. If you search for an explanation of the bizarre statistics on infant mortality, the ranking of U.S. "health care quality" as 19th in the world, etc, the explanation is to be found right here. To the extent that statistics are not rigged in order to make certain countries look good, the poor rank of American healthcare reflects the sadly underfunded Medicaid programs.
Even the medical profession is largely unaware of Medicaid issues because most members of mainstream medicine have long stopped accepting membership in the program, in part because of its laughable reimbursement, but more importantly, the HMO organizational model makes it impractical to treat an occasional poor person free of charge and skip the paperwork. It, therefore, is sometimes true that some Medicaid physicians see nothing else. And finally, hear this: Senator Grassley muttered that 90% of the cost of Obamacare is aimed at fixing Medicaid, and no Democrat on the committee corrected him. When you get down to it, Obamacare is a very expensive program for making Medicaid what it ought to be, and definitely isn't. Originally confined to Maternal and Infant Care, its money is largely spent on nursing homes. This would make a perfectly plausible explanation for why it has been so hard to see what the new proposal is all about -- it's about fixing the old mess which state and federal governments created, while at the same time hoping to extend a similar program to the rest of the country later, as a "single payer" system. Senate Finance has a difficult tap dance with this one, but they have put their heads down and are plodding on.
|
Eighty percent of the cost is devoted to fixing the flaws of Medicaid.
|
| Senator Grassley |
Many unexpected developments are still possible in an on-going debate, but it seems timely to examine the Obama proposal as presently visible at half time, so to speak. What is so far proposed of consequence, and what problems would be cured?
Employer Mandates. First, nearly universal health coverage hopes to be achieved by mandates, making it illegal not to be covered, imposing fines for non-compliance. It does not seem extreme to predict a rise in the fines to a level where they support the rise in costs they provoke. That would serve the initial problem of pacifying the public during the early going, but ultimately justifying the Supreme Court assessment that it was a tax, not a penalty. Unfortunately for this idea, Justice Roberts stated in his opinion that the fact that the penalty was so low proved it was a tax. If the penalty tax was raised enough, it would prove it was not a tax, and therefore the universal mandate would become unconstitutional because the rest of the Court had already agreed that the Commerce Clause did not support it. Chief Justice Marshall once opined that "The power to tax is the power to destroy" which generates the justification that only a small tax is safely small enough to be a tax and not a penalty. It follows that while the Constitution permits the Federal Government to tax for revenue, it is not an enumerated power to tax in order to coerce or destroy. Justice Roberts may have been tipped off, but if not it was a shrewd guess.
Obamacare closes the safety valve that just about every poor person has long been eligible for Medicaid, but few of them actually join it until they get into a hospital and the social worker signs them up. The true antagonism of poor people to "Welfare medical treatment" has yet to surface into public view. Mandates are always unpopular, but back in Washington two competing ideas for mandates once headed for a conference committee. Because of the tax preference for the purchase of health insurance by employers, we still have a largely employer-based system, defining for poor people what normal health care looks like. As hospitals (responding to the shift of Medicaid costs to Medicare which they are forced to make) have increasingly shifted the costs of indigent care onto employer-based insurance, those employers who participate are increasingly anxious to make their competitors stop evading "their share". Unfortunately for this proposition, the non-participating employers never agreed to subsidize someone else, and do not feel bound by any moral strictures surrounding the demand of big business that their competitors are obliged to share a burden which big business decided to assume for its income tax benefit. If you doubt that small business and big business are competitors, just ask yourself what small retail businesses probably think of Amazon and Walmart. Then ask yourself whether very many small businesses benefit from ERISA.
Since almost all interstate employers already buy insurance for their employees under the coverage of the ERISA law, representatives of large employer groups want their competitors, especially foreign-owned, to experience equal expense. Big employers would thus be pleased with an employer mandate: employers who do not provide employee health benefits would be fined. Big employers are not so much threatened by little ones, as anxious to avoid government regulations which ultimately favor smallness as a preferred business model. By contrast, small employers are resistant to the employer mandate, amplifying the political perspective that increased cost would particularly hurt new employment in the present recession. Small employers enjoy and would hate to lose, the reputation of being the largest source of new jobs in our economy. Employer mandate might indeed ensure some uninsured people but the remaining uninsured would be unaffected. An employer mandate solves some purposes of big business but probably injures small business to a degree offsetting the cost-shifting argument. So, although an employer mandate was on the table, Senator Baucus proposed the individual mandate which Representative Pete Stark of Berkely, California had been advocating for years. That is, every person found without health insurance would be fined. Recall now, that Chief Justice Roberts introduced the qualification that the fine must remain small to be called a tax. Presumably, compliance would be even less than the widely-evaded mandate for automobile liability insurance.
One cannot leave the subject of mandates without the impression that there is some poorly understood connection with the Henry Kaiser income tax preference for employers who provide employee health insurance. Almost nothing can illustrate the intensity of warfare between big business and small business than this. Large employers definitely do not want to share this benefit with their smaller competitors, and definitely, do not want to say so in public. To the rest of the public, big business is taking the wrong side of the fairness argument, to say nothing of the Constitutional argument about equal treatment. But there is no other source visible for the seventy-year defense of the indefensible which has long convinced Congress that the tax inequity is politically impregnable, and cui bono will have to suffice. As long as this remains the case, there is some hope that some Congressman will be willing to fight it out.Individual mandate creates a somewhat different political problem of what to do about recalcitrants who are both sick and uninsured, who must now fear punishment as much as their illness when they appear for treatment. They are unlikely to forget which congressman voted to create the vexing outcome of fearing-to-seek-treatment. The Congressional Budget Office summed it all up: we started with forty million uninsureds, but it is most likely we will be left with thirty million uninsured (and now resentful) persons, including 7 million who are in jail, an equal number of mentally retarded or disturbed, and 11 million illegal immigrants. The very vocal remainder is hard to classify and hard to count. But the CBO is probably right, it's hard to see how insurance reform of any description will get the number much below 30 million.
|
Give the tax exemption to everyone, or give it to no one.
|
A second difficulty with the individual mandate is that it exposes the long-standing inequity in the Henry Kaiser tax law. The main reason we continue a largely employer-based system is that purchase cost is effectively reduced by the tax discount when an employer buys it for an employee. Self-employed or unemployed persons do not now receive this tax-discount. For seventy years it has been desirable to extend this tax exemption to everyone equally, both for fairness, and to create portability mitigating the pain of pre-existing condition exclusions. Pre-existing condition exclusion always existed, but it is the linkage to portability between jobs that makes it such a wide-spread issue. But the employer-based system might lose its main reason to continue, so that particular consequence has yet to be addressed. Inverting the traditional relationship between being sickly and paying higher insurance premiums has never sounded completely plausible, but we are now going to see what happens if we try it that way. Additionally, the political consequence of not equalizing the tax preference would get worse. Compelling millions to buy individual insurance, while at the same time denying them everyone else's tax exemption for it -- is not likely to survive long once it gets public attention.
Give tax exemption to everyone or give it to no one, or give it for a lesser amount, but give the same thing to everyone if you hope for re-election. While tax equity is not in the current legislation, it might as well be, and the CBO should be asked to score it as part of the eventual cost. And finally, no mandate in sight during a recession would insure illegal immigrants, who are a large part of the uninsured problem in certain regions. It is reported that sixty percent of uninsured persons are concentrated in Florida and the four states bordering Hispanic America, a fact that ten senators and several dozen congressmen are sure to notice. Proponents of amnesty for illegals have undoubtedly thought about this matter. Opponents of amnesty are apt to see immigration reform as just a way to cloak the costs of Obamacare as an unrelated issue.
Now turn to the other main objective of reform legislation, to reduce the high costs of medical care. The poster child of this objective, possibly the central issue agitating many politicians, is the approaching bankruptcy of Medicare. To skip over technicalities, accumulated subsidies of fifty years of Medicare recipients have created unfunded liabilities that make Medicare the largest single debtor on the planet, unless someone wants to compete with $250 billion a year. If you think about it, Medicare would have no debts at all if it were self-supporting. Until something is changed, the fifty percent subsidy of Medicare by borrowing from general tax revenues is steadily making the problem worse. The understanding of the public is just beginning to realize that Medicare is so heavily subsidized, and this is probably the main source of its popularity. Ignoring how this growing debt was created, it is accompanied by fifty years of promises to every citizen about what they are entitled to. Perhaps it was believed that an uproar over reducing Medicare benefits could be softened by burying it in a nationwide reduction of all healthcare costs, but half the cost of Medicare is a pretty big nut to bury, and fifty years of accumulated debt is just about impossible to hide.
In fact, such expansiveness provokes more suspicion that something is being slipped in by the back door. In angry town meetings which frightened congressmen, held during the August 2009 recess, one speaker after another went to the microphone and said something like, "I have excellent health insurance and I wish everybody else had it, too." Following which, something was immediately said equivalent to, "But don't you dare take my good coverage away from me to give it to someone else!" And not invariably, but often enough to make it emphatic, some would add, "I voted for you in the past, but I'd never vote for you, again." No doubt, every one of those congressmen was asking himself how the party leaders could have got him into such a fix. Why don't we try something else? Senator Baucus offered to pay for reform by putting a tax on health care providers, but every worried citizen quickly saw that taxing providers will raise costs, not lower them. Credibility is waning.
|
The Affordable Care Act would cost a trillion dollars, and still, leave 5% of the population without insurance.
|
| The Congressional Budget Office |
An adage is getting hardened: Increasing access to subsidized health care is not compatible with cutting costs, and won't even produce universal coverage. It is increasingly difficult for presidential oratory to reverse that opinion. The Congressional Budget Office has not pronounced the Obama plan to be an unachievable goal, but after examining an enormous pile of studies, it amounts to that. They simply said it would cost a trillion dollars, and would still leave 5% of the population uninsured. In one sentence, the CBO probably killed a lot of strategies.
Still, the Obama administration gamely plunges ahead, seemingly forgetting that defeat of the Clinton health plan was followed by a mass eviction of incumbent congressmen; by their analysis it wasn't a bad plan that made trouble, it was failure to pass the bad plan, which it must be recalled was a universal HMO system. The Clintons avoided public defeat by pulling that legislation away without a floor vote. But at least they did escape the backlash against what would then have been a ruinously unpopular program. It is not unrealistic to surmise that Obama would never have been elected to a first term if Clinton had not backed away from his version of healthcare reform. Right or wrong, some Democratic congressmen are certainly toying with that heretical idea.
For one thing, the public has always been bewildered by the need for such a rush, such a collision. We are now fighting wars and struggling with the worst depression since 1930. All of those major projects are going poorly. Why in the world would we believe that reforming health care is our major priority, right now?
The following section closes the discussion of the main features of the Obama plan and ignores thousands of pages of legislation not yet implemented. The law is mainly made up of earmarks, boondoggles, and in consequence -- the usual contents of an annual budget reconciliation act produced at Thanksgiving or the day before Christmas. We hear nothing about tort reform, which at most will produce a study or a pilot program. Nor the public option, which Senator Baucus said cannot pass the Senate, and about which former Senator Dole said he heard, but scarcely would believe, that the Public Option was just a smokescreen intended to distract the public while the rest of the bill slipped past the uproar of Public Option getting defeated. The fate of the expensive but inconsequential computerized medical record would once have depended on the precarious health of Senator Byrd of Virginia, who had long held a stranglehold on government computer procurements, but which now mainly perplexes us as to what to do with it. Blue-sky yarns about the value of the Electronic Medical Record abound. But except for large group practices which do seem to need it, most doctors see EMR as an expensive way to add two hours a day to their already overloaded workload and badly compromise patient privacy in the process.
How to spend
------------------------------------------------------------------------------------------------------- Throughout this discussion of the design of Health Savings Accounts, lifetime version, we have attempted to follow the underlying design of what we already do. That is, parents usually pay for children, old folks usually pay out of savings. So, once the money is in the Account, we try to imagine how it is now usually disbursed for healthcare, and even occasionally what the sources of it are. Our general choice is to follow established patterns where we can. Nevertheless, we favor debit cards in place of insurance claims forms, for all outpatient claims which fail to trigger the re-insurance deductible. Paying 10% for someone to pay your bills for you, is just unacceptable.Children almost always have their medical bills paid by their parents or their parents' insurance. Where to place the upper limit on childhood is a puzzle, but recent law has included children up to age 26 on their parents' health insurance. Since that seems to meet general approval, we adopt it, although it might be wise to allow emancipated children to opt out. Regulations on the use of parents' HSAs for their children are a little unclear, but we assume they would be easily changed if they conflict with reasonable practice. That parents-pay-for children system does complicate a smooth estimation of the future growth of the parent's Account, however, particularly in the event of a divorce of two parents with such accounts. It also interferes somewhat in the child's future right to claim compounded growth, so there is a brief temptation to give it to all three at once. However, the deposit was only one deposit.
In some ways, it is easier to have both parents contribute to the child's one-time initial deposit, in order to have longer for their compounding to continue, and to have the child's account begin with their contributions. This makes a $150 contribution at birth become $300, and you really can't keep responding to problems that way, without destroying the universal appeal of the plan. However, it is easier to imagine acceptance of double contribution with a later rebate of half of it, than to imagine a single contribution later cut in half. Perhaps it is easier to give people their choice of the two approaches, but it certainly muddles future projections. We opt for double contributions, with an optional rebate of the half at the child's 26th birthday, if the parents have had a falling out. With double contributions, there should always be a small surplus in the child's account, whereas sharing even minimal deficits is apt to cause more trouble in an already strained marriage. Double deposits as a default, single deposits as an option. Optional rebate at child's age 26.
Immediately we must expect an outcry about poor mothers who can't afford it. But every other proposal suggests a government subsidy for this purpose, and so do we. The ultimate savings to the government of putting up $150 per baby, would be enormous, but they would not be totally realized until the child was forty, and the government would be "loaning" the expenses in the meantime. An important reservation is the health expenses of the indigent are usually higher than average, obscured by the fact that many of them are not paid.
Grandparents. Children are repaying a debt to their parents, which parents frequently forgive; the parents initially pay it out of their own accounts. With the elderly, there are often no children or grandchildren; the elderly either have some savings, or they are indigent. Where there are descendants, they are not always willing to back the defaults of the elderly. If they bought out Medicare (with roughly $40,000, adjusted) after attaining age 65, they will, in summary, stop paying Medicare premiums, pay outpatient costs with a credit card, and their catastrophic insurance will pay the hospital an updated (we hope) version of the Diagnosis Related Groups (DRG) for inpatients. To adjust for contingencies the insurance might make a deposit in the patient's HSAccount for other medical costs (ambulances, for example), which the patient pays by credit card. Emergency care may well fall into this ambiguous category. The catastrophic insurance company is expected to have negotiated reasonable charges with the hospital, and to defend the patient against unreasonable ones. Rent-seeking in the outpatient area is more the patient's responsibility to detect, to object to, and to negotiate below a certain amount. Generally, the principle sought is to assume no responsibility for recognized overcharges, unless they have been agreed to in advance of the service.Working people, age 26-65, and/or their employers. At present, much of the health care of working people are voluntarily paid for by employers. Therefore, it is their choice what to do about a diminishing cost, absorbed in this system by their employees. Since the source of most of this windfall is an investment in the stock of their companies, perhaps everyone will benefit. Time alone will answer that issue, and perhaps it is too early to be making decisions about it. So for the moment we abstain from the fairness issue and do not greatly object to a gradual adoption of the HSAccounts for Lifetime Health Insurance, which is inherent in making it voluntary. However, it is clear that the employees are often spending for what they formerly got free, and as a beginning might well be gratified to have a roll-over of their Flexible Spending Accounts into Lifetime Health Savings Accounts. That would require the passage of no law, and perhaps ought to be requested politely. A surrender of industry's stance against income tax equity on health expenses would be nice, even though the Editorial Page of the Wall Street Journal cautions restraint in this effort, even restraint of the Tea Party members of the Republican Congress. I'm afraid I disagree on this significant point, which seems to put me to the right of the Tea Party.
That would seem to leave working-age people paying for themselves, their children, maybe their parents, and the indigents. Before that, for many of them, it was once all free. With that description, it is natural to expect some grumbling. But the cost to them is only a fraction of the former cost to the nation, and they get a great deal more control over an important part of their lives. It must be obvious that the old way was too expensive to continue, and it won't continue long. If for no other reason, unions will demand that everyone else feel some pain. Working-age people will end up with a bill of thirty or forty dollars a month, an undisturbed medical system, and no more yearly health insurance premiums. The employer has the employee health insurance cost gradually lifted from his back, and know very well that he will be pressed to spend some part of it for employee costs. Let him pay some into the HSAccounts, particularly during the early transition stage, when there will be very little investment "cushion".
And finally, it must be pointed out the federal government has been supporting a lot of this cost for nearly fifty years, but their instinct is to hide it. Fifty percent of Medicare costs are paid for with general tax money, quite effectively concealed in the budget term "Transfers from the General Account". Borrowing from foreigners is largely traceable to this source, and no one can be sure what will happen to world finance if it stops. Because this fifty percent subsidy would have to be extended to every citizen if we adopted a Single Payer system, even extreme liberals hesitate to press that solution, or imaginary solution to our problems. For now, leave it alone, and see how things are progressing.
Premiums and payroll taxes* Catastrophic Insurance= Debit Cards* Revised DRG= Personal funds* Direct Marketing= Internal loans* Escrow funds* Federal Reserve monitoring and midcourse adjustment. Deliberate overfunding of HSA*Data Sources for Health Care
OTHER REVENUE PROVIDERS WITH POTENTIALLY USEFUL MEDICAL DATA, MOSTLY UNUSED
Although some research discoveries are stumbled on by accident, most of the important ones derive from asking the right questions. If you don't ask the right question, you can wander around in a laboratory white coat for a lifetime without discovering much that is worth knowing. We already have huge stores of data, much of it in electronic form, about the health system. It mostly comes from people paying bills:
Health Insurance
Health Savings Accounts
Payroll deductions for Medicare
Medicare premiums
Military Medical Systems
Veterans Administration
Government subsidies to Hospitals
Medicaid (50-70% Federal)
Social Security
Life Insurance
Premium Investment Income
Cash payments (weak source)
Unclassified Remainder
To summarize the data sources already in existence raises questions of privacy and overwhelming government intrusion into the lives of citizens. That might well be a threat in forty or fifty years, but the disaster of the Health Insurance Exchanges trying to use a small particle of this data is reassuring, in a discouraging sort of way. These systems were originally devised to ask questions of no great relevance to national health costs, so they pose no great temptation to a wandering medical snooper. But they almost always have to meet some sort of an annual budget, so the answer to the question we are now asking is mostly available to everybody, on the Internet. It should be comparatively easy to learn, with adequate accuracy, how much is being spent on what kind of person, right now. If the total comes anywhere near 18% of GDP, we have as much detail as we need for this book to defend the conclusions it draws. We can tell the gross amounts, and by dividing by 350 million, get the average per person costs. Apportionment by age is somewhat less precise, but the numbers are so large, age stratification can be fairly accurately estimated. Let's start with a question we think we know the answer to.
Direct Marketing of Health Insurance?
New blog 2014-01-07 21:29:34 contentsWelcome to Welfare
|
Percent of Their Hospital Cost Reimbursed: Medicaid 70%, Medicare 106%, Private Insurance 150%, Uninsured 400% (?)
|
| Hospital Cost Shifting |
There's lots more; in politics there always is. The Pew Foundation, which now includes public opinion polling in its tasks, has pointed out 80% of the public does not share the polarization now so blatantly agitating the political class. Hence, some commentators have questioned the prevailing opinion of gerrymandering as the main source of it. These observers point to a worldwide decline in party affiliation; "independence" of party affiliation is claimed by nearly half of American voters when asked. Perhaps we have things backward, and gerrymandering is merely one effort, along with growing dependence on financial contributions by wealthy donors, to rescue party power. Television (and especially the Internet) prompts the voter to hang back before making decisions, hoping to decide something without pressure from party leaders. The growing tendency to vote straight party ballots is not taken by a few commentators as evidence of true voter wishes, but rather as evidence of the futility of resisting a two-party system. Some sophisticated observers feel straight ballots result from plurality ("first past the post") counting of votes, but this (unfortunate) trend seems more likely to be stimulated by (too) early voting by mail.
Since a two-party system favors moderate candidates over extremist ones, it may not be a bad system, but rather a good system adjusting to circumstances. A hidden cause of the present crisis in health care financing comes from the Medicaid programs, run by the states, but mostly (and inadequately) financed by federal taxes. A two-party system disciplines the nominating process by raising doubts about the ability of extremists to win the general election. Consequently, the final two candidates are often so similar the chance of a loser bolting the process, becomes small. In a proportional voting process, splinter parties cannot be silenced in the primaries, because political deals take place after the election when the public has become irrelevant to the voting outcome. Threats of public disaffection are therefore disregarded. This hidden feature went unrecognized at the Constitutional Convention, as indeed was the whole party apparatus. But it has to be counted as one of our greatest strengths, placing a much higher value on unity than dogma. If you follow this reasoning, you would have to conclude the present level of divisiveness will not persist. Because each generation has to learn its own lessons, it may recur, but it will not persist.
Nursing homes were not originally included in the 1965 legislation, but most states receive strong pressure to pay for elderly indigents in nursing homes, stranded by running out of savings. Perhaps it would be a good thing to include nursing home coverage in a reform bill, but nursing homes bear too much resemblance to work-houses to generate much demand to be in one. In variable degree, the circumvention has grown up of paying for nursing homes with money intended for hospitals but necessarily underpaying the hospitals. The hospitals make up the deficit by overcharging for outpatient services, as everybody will recognize who has been charged for the same service, both as an inpatient and an outpatient. By prevailing estimates, the Medicaid programs only pay hospitals about 70% of their actual costs. Hospitals escape insolvency to a minor degree by raising reimbursement demands on Medicare (to about 106% of costs) and more appreciably through private insurance (to something approaching 150% of costs). Teaching hospitals have some opportunity to raid funds intended for indirect research overhead, for resident stipends, and for disproportionate shares of an indigent, "self-pay" patients. Various accounting tricks account for the rest. For example, the transfer of schools of nursing from hospitals to universities has emboldened universities to seek the equivalent of traditional hospital reimbursement schemes, merely and mostly triggering new arenas for dispute, because the hospitals had hoped to profit from the transfer. Since Medicare somewhat overpays hospitals for its own patients, in recognition of the underpayment by states for indigents, current jargon blames the "government programs" for underfunding hospitals. A better summary of the situation is: Medicaid under-reimbursement is the largest source of hospital financing problems, but other problems are less resistant to change. That's pretty significant, in view of the Obamacare plan to put millions of uninsured into Medicaid, some of whom never asked to be insured at all, and most of whom have no previous experience with "welfare", so they need to start reading some books by Charles Dickens.

|
| Governor Christie of New Jersey |
The outcome of all this is nursing homes are in effect supported by Blue Cross and other private insurers of younger people, raising premiums to employer groups and individuals by something estimated like $900-1500 a year per subscriber. That's because Medicare is busy subsidizing Medicaid's hospital patients, the main source of hospital deficits. Because this juggling lacks straight-forwardness, results are inefficient; only about 42% of hospitals actually break even. As might be expected, knowledgeable employer Human Resources departments and hospital administrations know about and object to this system. They are cooperating with Obamacare more than might be otherwise expected, probably in the hope this cost-shifting can be adjusted more in their favor when it is less in the public eye. Mandating all employers to participate would, of course, increase the base of people sharing this exaction, but would ultimately link corporation treasuries to government deficits. The dream of the service unions would be to use this excuse to mandate the unionization of hospital employees. Governor Christie of New Jersey quickly saw a way to split the Union movement into public and private compartments through this. "Every time they get a raise, you get a tax increase," he told the unions of the private sector.
The participation of physicians in the Obamacare effort is riven by their own politics. For surgeons, the premiums for Malpractice insurance can sometimes run to $200,000 a year. An appalling proportion of obstetricians have been sued by their patients, to the point where women have no doctor to deliver their babies in certain parts of the country. For doctors in this high-risk category, relief from the plaintiff lawyers is the most pressing of all problems. On the other hand, many physician specialties have almost no malpractice risk and are much more exercised about the SGR reimbursement freeze, which has been in effect since the administration of Lyndon Johnson and has been severely undermined by inflation ever since then. With physician ranks divided by two different priorities, the way is open to promise both and reward neither.
|
The powers not delegated to the United States by the Constitution, nor prohibited by it to the States, are reserved to the States respectively, or to the people.
|
| Tenth Amendment |
Urban-rural differences remain important in health care. Senators Baucus, Grassley and Snowe come from sparsely settled states. Former Senator Daschle is from South Dakota; there are perhaps twenty states potentially in this category. With a sparse population, it is difficult to develop sufficient insurance business for the law of large numbers to establish actuarial safety; these states need to combine into regional areas to reduce the competitive size of their loss reserves. On the other hand, populous states like New York, California, etc. are often adamantly opposed to regional groupings, for opposite reasons. These population disparities create differing attitudes about modifying the 1945 McCarran Ferguson Act, which limits federal insurance regulation and enables state regulation, thereby making it difficult for small states to agree to interstate health insurance sales and portability. The fact that large employers have already achieved this freedom through ERISA also makes them unwilling to see the problem or waste political capital achieving it for others. And thereby diminishes the power of low-population states to resist national healthcare insurance, which is their natural position.
And finally, Obamacare raises some questions about judicial remedies. Certain Op-Ed commentators have raised a question of the constitutionality of federal mandates or pre-emptions of state laws, depending on how they are phrased. The U.S. Constitution was only narrowly ratified in 1789, in large part because the states were fearful of the federal government getting bigger and more powerful than necessary. In response to this strong feeling, the Tenth Amendment reinforces in no ambiguous words, that anything not specifically assigned to the national government is to be in the province of the state or local governments. If ever there was original intent, it was that one.
REFERENCES
| Never Enough: America's Limitless Welfare State | amazon |
Co-Insurance (2)
New blog 2013-07-01 16:26:04 contentsIt's a convenience for the insurance company perhaps since it reduces the insurance cost by 20% and is easily figured on the back of a salesman's envelope. Therefore it helps in the three-way negotiation between the employer, the insurance company, and the union. The union calculates how much income tax the employees save by how much income is split between the "fringe benefits" (non-taxable) and the "pay packet" (taxable), and the negotiations shift around these offsets, usually at the end of grueling collective bargaining.
It was once explained to me that Co-pay was very popular with negotiators for unions and management because it was easy to calculate the total cost of it for an entire self-insured corporation. If a proposed budget for the employees was known, and the budget for health benefits was agreed, the arithmetic was easy. If the company has a 20% co-pay, it can reduce the company's total insurance cost by 20%, and if it doesn't come out right, you can negotiate 18% or 22% or whatever. Late at night when these negotiations characteristically get serious, the cost of the offer and counter-offer can be quickly calculated. By contrast, if a deductible is proposed, you have to know how many people use the program, how often they would get sick per year, and even so the calculation is difficult, requiring actuaries or at least accountants. So, the explanation ran, everybody, likes co-pay, and everybody hates deductibles. The insurance people present especially like co-pay, because there will soon be a demand to add it to the package as second insurance, and the premiums for that are also easily quoted, up or down as the negotiations proceed. When it got to involve Medicare and Medicaid, the Congressmen were in essentially the same position of only wanting to know what bulk costs of the whole program would be. In short, co-pay is easy to "score". But the best that can be said for it is, it's just another short-term benefit for which long-term costs are increased because there are diminished incentives for the third-party to hold them back. Just kick the can down the road.
It has never seemed completely credible that anyone would base expensive decisions on considerations so trivial, but you never know. Having invented Medical Savings Accounts with John McClaughry in 1980, for me the mysterious resistance to high deductibles has never seemed adequately explained. Negotiators must easily see that two (or three) insurance policies will be more expensive to administer than just one. They must immediately acknowledge that being 100% insured will increase costs by making the beneficiary ignore the cost, and they are probably willing to accept (off the record) the American Actuary Association's estimate that costs are thereby increased 30%. That much alone would free up about 5% of the Gross Domestic Product since we are currently spending 18% of GDP on Health care. There has almost seemed no point to go on that wages could be increased by diverting this wasted money to the pay packet, to say nothing of the frustration many doctors feel at having no idea of the true cost of what they order, and hence little interest in making the number smaller. Obviously, if true costs are concealed, they go up. This blinding of the doctor to true costs is what makes cost-shifting easy to do without criticism. The absence of a pool of deductibles makes it impossible to generate compound interest, and that in turn makes it less practical to consider "portability" of health insurance from one employer to the next. It is at the very root of fictitious costs for medical care of all sorts, which somehow seem to the advantage of many participants in the health field. Eliminating co-pay would result in a small saving, and it probably would result in a big saving in healthcare costs. The aggregate national savings would be astonishing. Health Savings Accounts are slow to be adopted, not because they fail to save money, but because state laws have imposed mandatory insurance benefits for small-cost items, apparently passed for the main purpose of undermining deductibles.
Most people initially resist the idea of a high deductible on the ground that poor people can't afford it. When it is explained that what is intended is basically to give the poor the money to pay for it, most resistance disappears. A more correct description is that some method is constructed to give them the money, but in a way that allows them to spend money left over from healthcare, for something else they want to buy. The ability to buy something else is not the same as wasting it, and safeguards are only prudent. Retirement is the use most commonly considered. Because interest rates are being suppressed by the Federal Reserve, this proposal may be somewhat retarded for a year or two, until interest rates return to normal levels. Addition of an inflation-protection feature (like TIPS) might well enhance its attractiveness. Ultimately, the first step would be to eliminate Co-pays. Completely and permanently.
Cost to Charge Ratio (2)
of the community when all is said and done, this system is designed to keep indirect costs within reasonable boundaries. If that aggregate is spoken of as a single product, its costs can be grouped together as company-wide costs. In the case of Apple, the main costs outside direct production costs are research and development, marketing and administration. In the case of hospitals, in addition to direct production costs, there is usually less marketing cost than a manufacturer would experience and considerably more charity. By calculating the variation of prices to costs among different products, it is possible to see which particular product is carrying the burden, and which product is being subsidized. In the case of hospitals, this analysis would permit an outside opinion to form about the fairness of such cross-subsidy, which is most commonly motivated by local competition. The neighbor hospital has some expensive gizmo and we don't; we buy a gizmo to keep up with them and subsidize its cost by overcharging for everything else. Decades ago there was a rage for establishing planning commissions to determine how many gizmos a community needs, but it was largely dropped because of bickering about what is normal business flexibility in every industry. It is now generally agreed that hospitals should have the business latitude to make these choices themselves, and suffer the consequences if unrelated prices get pushed out of line by cross-subsidies of excessive expansion.Indirect costs are a much harder matter to judge. Some administrators are paid too much, some renovations are excessive, some charity is really poor debt collection; but if these things are passed off to insurance companies, who pass them off to the public, they can unduly escalate. Direct costs are whatever they are, but indirect costs are more a matter of opinion. Some insight can be gained by measuring the ratios of direct to indirect costs, and then making a national comparison of those ratios with peer institutions, a process that is hampered by the traditional regulation by states instead of nationally. Since the cost of health care has long been rising faster than the cost of living, the suspicion is fostered that insurance companies put up less price resistance than a marketplace without them would. Since the cost of major illness is often beyond the means of its victims, insurance does seem to be called for, and the higher the cost the more that is true. For more than seventy-five years, health insurance has been in the middle, between the party who wants lower prices, and the party who wants higher ones. That may well have been a bad decision, requiring some experimentation with a return toward "indemnity insurance" and away from "service benefits". That is, the insurance pays money to the patient, and the patient then pays the bill. An indemnity system protects the insurance company from cost overruns, and this at least removes the pressure for the insurance company and the hospital to collude against the patients' financial interest. Once a suspicion arises that there could be some degree of collusion between the two, it is possible to see that using insurers to police a hospital's indirect costs may be something to discourage. Alternatively, it might be possible to apply patient copayment to the indirect, but not the direct, hospital costs. At the moment, copayments have little or no effect on patient utilization, but the selective application of them might be worth at least a pilot study, to see if they could dampen prices better than they affect service volume. A copayment of 20% of the indirect cost component of a patient's bill would certainly draw attention. Even a 1% copayment would dramatize the point.
Hospital prices have been inflated far too much, and far too irregularly, to serve as cost signals. In order to minimize the true cost of charity care, the services more heavily used by the indigent have had their indirect costs minimized by cost-shifting them away to better-reimbursed departments; it is a perfectly natural thing to do. Poorly utilized departments are subsidized by better-reimbursed ones; so what else is new? To assign a fixed ratio of charges to costs would greatly hamper the flexibility needed to keep the institution from failing. But without some understood relationship between the posted, stated price and its true cost, the hospital doctors are quite unable to design a cost-effective treatment strategy. Knowing very well the lack of relationship between prices and costs, the doctors freely admit they disregard the prices entirely. While allegiance to what is scientifically best is not completely bad, it is not necessary to be so blind to the economics of the various alternatives. In time, it will lead to the design of model treatment strategies by committees. That is not itself a bad thing, except for the way it undermines individual thinking by the professional who is closest to the specifics of a case. That is a debilitating thing; a bad thing if you wish. It certainly lessens the potential for minimizing the cost of care, which is the flag it is flying. Some way must be found to improve the usefulness of prices as a guide to costs, an imperative which is otherwise certain to lead to the use of some degree of force to achieve it. And that would be a really bad thing.
from the for the Hospitals tend to be either for-profit corporations like Apple or nonprofit corporations with a different accounting system. It may help a little to know that for-profit corporations are measured by their profitability, while nonprofits are measured by the increase (or decrease) in their assets compared with last year. Items enclosed on a balance sheet with parentheses have always gone in an (unfavorable) direction. Increases (or decreases) in assets are intended to include gifts and variations in stock market prices. However, increases (or decreases) in assets like fine art don't count at all. Sometimes that can be highly misleading, as when the Barnes Art Collection increased in value by billions of dollars. Other assets, like buildings and equipment, are measured by depreciation, which is not always parallel to market prices. There is a movement favoring "mark-to-market", but investment firms are particularly opposed to marking to market, because temporary drops in market price are sometimes unrealistic, only requiring a little time to recover, a phenomenon sometimes seen in endowment funds, as well. Conventional measures of success, like the profit margin and the increase in net assets for nonprofits, are generally useful. But they can also conceal many traps. The most prominent one is to introduce these concepts when someone questions why everything costs so much as if to imply that it is unlikely that a hospital could be overcharging when it is only generating a 2% profit.
The ten dollar aspirin tablet is usually introduced at this point in the discussion, balanced by descriptions of accident room patients who try to pay nothing at all. The discussion is now one of cost-shifting. It must be obvious that the cost to charge ratio is well over a thousand percent for the aspirin, whereas Apple probably is less than a hundred percent for everything they sell you. Perhaps not, perhaps it is over a thousand percent for a number of retail items. In any event, the problem for the hospital customer is he has no way of telling what is being given free to bring the overall cost to charges down to 5%. That is, he is given no role in choosing the charity he is supporting, but he knows it varies widely between hospitals. He has to have some trust that the institution is behaving in a responsible way, which is difficult when he sees new and glistening hospital interiors or reads of seven-figure executives. Perhaps it is a little unfair to blame the trustees for avoiding embarrassing questions with no particular justification, but it does not seem unfair to ask that the hospital cost accountant prepare meaningful reports to both the management and the trustees. To the management first, to allow them time to look into oddities in the reports before having to answer for them. But no matter how it is handled, the cost accountant should be made more central than he usually is.
Every item ought to be assigned a cost to charge ratio, both inclusive and exclusive of overhead costs. It is usual to include overhead by a so-called step-down process since overhead must be paid and it generates no charges at all, only costs. But to include it in the net cost to charge ratio is potentially to bury one of the things you are trying to discover: is the overhead excessive? Having determined that point, it may be legitimate to re-include overhead in the "net" calculation of the cost to charges. Hence the suggestion of reporting it both ways. No one doubts the books balance; the items of expenditure include most of the costs. The essential issue is whether this is all pretty expedient, whether too much frivolous expenditure is being permitted by shifting its cost to certain profit centers. When this cost to charge system is compared among other hospitals or other years in the same hospital, it is possible to recognize the unusual items or departments quickly. However, the beginning trustee or utilization reviewer may need to have the costs and charges stripped out and aggregated, to highlight the highly deviant figures for ready appraisal. Consequently, it may be necessary for the insurance company to require reports of certain items, structured in that way. Other such reports may be needed to identify overpaid employees, or overstaffed departments, usually as patients and dollars per employee, compared with other institutions. Ultimately, it may even be necessary to establish norms, but that begins to resemble micromanaged cost control, when peer pressure may be all that is required.
Executive Summary, continued
continues the inequity of denying the same tax exemption to everyone because of the nature of employment, and would be very hard to defend in open public debate, but even equalization will fail to adjust historical disparities in premiums upon transition to universal coverage (because of resistance to rebalancing the pay-packets). Secondly, service benefit compromises which might be tolerated in a private system become dubious within a government mandated one. And thirdly, businesses have outgrown their 20th Century role as a rescuer of vital community service, and now often regard health costs as a growing burden to company competitiveness, which stockholders must be induced to accept. Businesses themselves may be changing perspective and beginning to see the advantages of employee-selected and employee-owned portable health insurance. They may have come to see that employer-basing drove them toward selecting a one-year term model, rather than a lifetime whole-life model, and the employee-owned model is portable between jobs, and able to pay much of its own cost by compounding investment income. Many of the present complaints grow from discontinuity, while continuous coverage greatly reduces the expensive patchwork of multiple insurance forms, pre-existing conditions, uncoordinated successive insurance plans -- and is able to generate investment income, besides. The easiest way to become adjusted to a billing and information system is to avoid frequent changes in the companies running them. Forcing insurance companies to maintain a nationally uniform system is a disruptive way to get there, reduces innovation and competition. Beyond a certain point, people will rebel.
But among the opportunities neglected by mandated universal-coverage at community-rated seem to be: Opportunities for coordinated compound interest to finance coordinated lifetime systems; opportunity to coordinate insurance company information barriers at least enough to eliminate the need for up to three insurance forms to pay for one medical service completely; an opportunity to re-examine the technicalities of traditional patient cost-sharing, thereby downgrading or eliminating ineffective co-pay, but expanding much preferable deductibles buffered by Health Savings Accounts. In the past, many compromises were made to accommodate the highly untraditional insurance concept of service benefits, including bungled but laudable transitions to reimbursement by diagnosis-related groupings. It would be a great mistake, however, to equate this hospital approach with system-wide elimination of fee-for-service. Information systems and cost accounting based on item charges are highly developed and cumbersome to replace; no system outside the acute care hospital has more than experimented with other approaches. It would seem far simpler to modify insurance design to isolate two billing approaches (itemization and capitation) and force them to include, side by side, both office-based care and inpatient services using the same hospital cost accounting data to establish reimbursements. Mandated universal systems can facilitate some of these things, but the real test of democracy is to achieve them without resorting to force.
All of the foregoing areas of omission from the Affordable Care Act should be regarded as areas where improvements in the health administrative system might be possible for either political party to espouse. Therefore, if both parties might agree on some of them, progress might continue even though there is another acrimony in the background. The list of other approaches opened up to examine is probably longer than the average reader has the patience to read, but it includes Last-year of Life escrow, and gradual dispersal of the physical centers of health delivery away from tertiary centers, not toward them. More modest goals and timetables for computerizing physician notes would greatly reduce transition costs for providers. Centralized statistics might thereby be lessened, but the quality of care need not be. The savings from digitizing physician office notes have been greatly overstated, and mostly apply to physician practice aggregates, which inherently magnify communication and record-keeping costs.
Although health reform is now portrayed as a settled decision, the debate which preceded it never anticipated a 50% swing in cost difference between Obamacare and its insurance alternatives. At this time of national financial turmoil, such savings might actually exceed 5% of Gross Domestic Product, thus providing appreciable funds for other urgencies. It seems incredible that such an equilibrium would escape re-examination.
PRIORITIES NOT EXPLORED: Every reformer must choose priorities, but cannot escape criticism for other roads not taken. The chosen highest priority of ensuring everyone with community-wide premiums must also now demonstrate it was achievable without injuring the quality of care. It must also be demonstrated that the commendable goal of spreading expenses widely did not require so much complexity and inflexibility that the delivery system could not keep up with scientific advances. Even if all that can be achieved, the question will remain whether the time and effort might have been better applied to solve a myriad of other healthcare problems which have less to do with insurance. Other problems undiscussed in this paper might have included the financial abandonment of inpatient psychiatry, the unnecessary diversion of non-emergencies into hospital accident rooms in order to retain control of the system within acute care hospitals, unprioritized expenses encouraged by internal hospital cost-shifting, and distorted state budgets encouraged by complex shifting of underfunded hospital Medicaid costs to other payers, especially Medicare. By burying medical costs within insurance, physicians directed to use less expensive methods are denied truly useful information about the cost of components. (That is, not about posted charges, but about what is the true cost.) Item costs are the central signals used, and the present attack on the fee for service offers no substitute signals. The nursing profession is distracted by clerical functions, and its training programs transferred out of hospitals into less meaningful college environments, by reimbursement bundling. The medical profession has seen its overhead costs inflated by compliance with questionable reimbursement requirements, effectively impoverishing primary care, and overcompensating procedural alternatives which can more easily transfer overhead to the hospital. The serious issue of "Job Lock" raised by the earlier Clinton proposal is an inherent component of employer basing, probably continuing as long as employer basing does, and possibly as long as the Tenth Amendment does. The tax inequities for self-employed and small-business employed persons are stubbornly continued, as will be exposed when premiums stabilize. Many of these issues have insurance features because insurance is the dominant method of payment, but they are not considered here as direct consequences of the insurance model. While this list could be extended, its present extent already strains the limits of what can be coherently grouped by sources and causes. This paper confines a critical analysis of those insurance issues where solutions are proposed.
and Generally empowers non-physician administrative control through reimbursement as a means to control rather than assist the higher goal of widespread good medical care.Introduction, continued
Almost three years after the President presented 2500 pages of the proposed health law to Congress for approval, the commentary is hampered because important rules are still unissued. If the program eventually works well, criticism and proposed alternatives may well be set aside. But if enough voters become upset during the early stages of implementation, there will be no escape from the review of other options. To some people alternatives of any sort would seem premature, but here they grow from a preliminary perception that this enormous program has wandered from identifying the basic problem, and thus failed to concentrate on a coherent remedy for solving it.
At its root, the Affordable Care Act is, quite rightly, an insurance reform. Reform of a system is considered to be failing because healthcare costs were rising alarmingly and many citizens had no insurance to buffer them from it. The bulk of citizens did have insurance, and their indifference to cost was considered a cause of the escalation. It was therefore elected to make health insurance universally mandatory and uniform, with government subsidies for those who could not afford it. A unified system would eliminate enough inefficiency to pay for itself, and while some individuals would see higher costs, average lifetime health costs would decline overall, as the peaks and valleys of lifetime costs level out. Governmental control of the insurance system would thereby put it in a position to ignore the nationwide indifference to costs, while its evident power to ration would make rationing unnecessary. More than this was, of course, promised during political campaigns, and more were probably secretly hoped for. But this short summary intends to make the best case for what was offered and will be accepted as the basis for analysis in this paper. If less than the best case makes an appearance, it will be noticed.
Insurance reform is expected to change something, so it seems fair to criticize the Affordable Care Act for accepting three major questionable aspects of the old system, as well as two innovations of its own. Much of this critique will focus on the new problems making the old problems worse, possibly bringing other old problems to the surface, as well. Criticism without offering a substitute is useless, so this paper re-examines Health Savings Accounts in this new environment and finds it actually makes that alternative more attractive. Combined with a repeal of the present tax preference for employer-controlled coverage, these two reforms might be sufficient alternative, with a more gradual beginning. However, the reader is asked to consider the far more ambitious proposal for lifetime, individually owned health policies, universally mandated if you please, with the potential for internally generated investment income to pay for substantial parts of its cost. And the reader is asked to look beyond insurance reform as the way to reduce medical costs without rationing, with the example of moving the center of medical care (physician offices) away from the acute care hospital campus, toward the concentrations of most illness (retirement villages). This latter would largely consist of removing obstacles to where the system seemingly wants to go, anyway. Several other non-insurance reforms are presented in sketchy form, with the urging that most of their seemingly insurance-related features are merely a reflection of present predominant payment routing through insurance, a feature now found in almost anything medical. When they rise to a level embedded in law, they may, of course, require legislative attention to reverse them.
The difficulties it should first correct are distortions of medical care imposed by existing insurance-like financing, searching for a way to conduct a pre-payment system. High costs and failure to include everyone are important issues. But they were only two of many distortions emerging from an employer-based, tax-preferenced, prepayment system. It had been awkwardly forced into an ill-suited term-insurance format long before the present Administration took office. The national clamor of dissatisfaction did not originate out of a united voice of the uninsured population demanding more free coverage, nor was individual cost constraints a central problem for the insured public; rather, clamor mostly originated with third-parties imagining that soaring aggregate costs could be constrained by cost-shifting them, and actuaries endorsing the delusion. Fundamental sources of unrest are to be found in limitations of one-year term insurance itself when applied to a pre-payment process for lifetime expenses -- further complicated by accidentally employer-basing it. Both of these distortions were seriously amplified by uneven bestowal of tax preference, also by accident. The number of small claims is too large to support the claims-processing cost. The size of the premium pool is too small to permit so much free care to be hidden within it because the average premium must not preclude the middle class from affording it. The cost of young and old dependents is rising, the cost of the employee who pays the bill is shrinking, but they are mostly the same people at different ages. The result was unaffordable delivery cost throughout a century of progressively vanishing disease. The health beneficiaries of this process were the patients, with longevity increased by three decades. The financial beneficiaries are also easy to identify. Just count the growing number of non-professionals who are making a living serving it.
On top of all this, a host of new problems are now predictable from additionally striving for universal insurance coverage. In the long history of insurance, there are no precedents to follow, for eliminating market-set prices as a benchmark for insurance reimbursement. The relevant test of whether insurance reform is successful in the end, rests on whether these and other distortions can be improved, ultimately leading to better, less expensive medical care for everyone who needs it, as distinguished from insurance for everyone, payment from no one. Three historic flaws in the existing system might be about to become four. Ominously, present indications are that Obamacare will not only raise aggregate costs appreciably but that at least half of the formerly uninsured population will discover Medicaid coverage was not their idea of an improvement. Unless Medicaid can be significantly and rapidly improved, four problems will become five. The great bulk of problems to be addressed have scarcely been comprehended by non-medical people. For example, no attempt has been made to reconcile more expensive care with more "affordable" care, which would appear to be its opposite. Very likely, medical care difficulties will continue to rankle, no matter how universally Obamacare manages to extend some sort of insurance coverage at a community rate. This time around, the public must insist on a more informed appraisal of the many consequences, of which political consequences are the least important.
------------------------------------------------------------------------------------------ That might sound fair, but it certainly contained political dynamite. Americans prefer individual insurance policies to generational transfers because they distrust the promises of politicians. Americans would surely prefer to own their own policies and take them to their next job if they could. It's not clear that individual health insurance policies are impossible, but they would be difficult to achieve unless they were greatly simplified. One of the great advantages of the Health Savings Account approach is that it would make individual policies a feasible option. It is thus worth a moment to consider the difficulties of employer-basing any kind of health insurance, before going on to the difficulties of present forms of health insurance, regardless of where it is based.
In Summary
In Brief Summary. Suggestions for American healthcare reform are made, embracing the full potential of unencumbered Health Savings Accounts, and changing the physical center of healthcare delivery while turning some of the incentives of reimbursement in a better direction. Unfortunately, most of the intent of the suggested changes to the system cannot be appreciated without understanding the history and economics of health insurance, and the complexities of the modern health delivery system. An attempt to capsulize these matters is mixed among the proposed solutions to them in outline. They come from a physician with decades of practice behind him, fifteen of them before Medicare was created. No claim is made of lack of bias. The more important suggestions are:
A. INSURANCE REVISION
..1. Health Savings Accounts, linked to debit cards, reinsurance, investment vehicles, and marketing. ..2. Elimination of Co-pay, but increase of deductibles. ..3. Equalized tax-exemptions (for health) for all citizens, regardless of employer. ..4. Reduction of employer domination of employee health insurance choices. ..5. Increased deductibles for elective admissions to the hospital (or decreased deductibles for emergencies).B. REIMBURSEMENT REVISION
..6. Revised ambitions for computerized medical records. ..7. Substitution of market-based prices for hospital cost-accounting in DRG calculations and patient bills.C. ACCOUNTING REVISIONS AND APPEALS
..8. Establish a nation-wide appeals mechanism for both beneficiaries and providers. ..9. Independent negotiation and payment for aggregated hospital indirect costs. ..10. Inter-institutional comparisons of charge-to-cost ratios, indirect costs shifts, and indirect costs.(D. LONG-TERM: INDIVIDUALLY OWNED AND SELECTED WHOLE-LIFE FUNDING)
..(11.) Payment of Last year-of-life costs from an escrow to Medicare, beginning last-year-of life pre-funding...(12.) Gradual substitution of whole-life health insurance for term-life health insurance, beginning with first year-of-life post-funding.
..(13.) Encourage migration of office medicine toward the campus of retirement communities. As a beginning, charge some agency with discovering obstacles to moving (independently competing) physician offices to the campuses of Retirement Communities.
What Obamacare Should Say But Doesn't
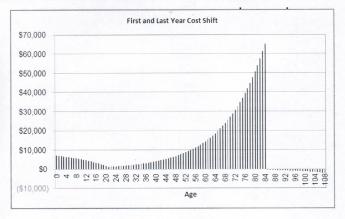
|
1a. TAX EQUITY. All tax exemptions stimulate overuse because they amount to a discount. For example, federal tax exemptions now mainly extend to two consumer purchases: health insurance and home mortgages. We currently have national crises in both at the same time. The tax-subsidized home-mortgage housing bubble played a major role in the 2007 financial panic, while tax-subsidized health care threatens to lead health costs into a second unsupportable bubble. Higher education seems to be going the same way, and it becomes difficult to imagine what would result if two or three of these bubbles merge. The expression "Children playing with matches" comes to mind. Giving a tax advantage to one group but not to its competitors is essentially just a variant, containing the paradoxical advantage that the competitors will object to it if they can't extend it to themselves.
Giving a tax subsidy to employees but not to self-employed or unemployed persons nevertheless created a uniquely American system of employer-based health insurance, and lobbying now perpetuates this rather odd system. Noting the allegedly temporary origins of this tax quirk (as a wartime expedient) merely dramatizes its lack of justification for seventy years afterward. It should not be necessary to describe collateral damage like job lock and internal hospital cost shifting. The issue of equal justice alone should be enough to justify the abolition of this unfairness. To mandate individual coverage but differentially exclude large subpopulations from tax exemption, is to invite a Supreme Court case. And since such a law has been passed, the sooner a damage case is granted certiorari , the better. To achieve equity, it does not matter whether tax exemption is given to everyone, denied to everyone, or limited to part of the cost (reducing the exemption for some, partly extending it to those who do not have it). Any choice between these three would make it equitable, although gradual elimination would be better, still.
|
If health insurance is mandated, its tax treatment must be uniform.
|
| Hidden Cost |
Once the tax is equalized, this proposal clears away the main obstacle to
1b. INDIVIDUAL OWNERSHIP OF HEALTH INSURANCE POLICIES, already proposed in Congress; but seemingly without hope of adoption. Determined opposition from the current owners of "self-insured" groups, the employers, or the unions who have acquired this function from employers. Since most such arrangements are de facto "administrative services only", insurer protests of higher administrative costs for individual ownership are often just relics of ancient combat between Blue Cross and commercial insurers.
Regardless of the internal structuring of incentives, healthcare reform cannot be permanently settled without individual ownership. It must be understood, however, that eliminating the tax preference could be resisted at first by patients who acquire it, because of fear the eliminated tax would in some way be shifted to them. That need not be true if consideration is given to the relative size of the losers and gainers. Since the membership of group policies greatly outnumber individual policyholders, the redistributed revenue cost of tax equity would be considerably smaller than 50/50. The CBO should provide a sliding scale estimate for negotiating purposes.
1c. ENCOURAGE WIDE-SPREAD DIRECT MARKETING OF HEALTH INSURANCE. Since Health Savings Accounts and Catastrophic High-Deductible Health Insurance are libertarian ideas without religious overtones, it is uncomfortable to advocate them as mandatory, even passing laws to that effect. However, the libertarian doctrine does not seem to preclude creating incentives for universal adoption. This doctrinal attitude imposes slower adoption than mandating them, although a better product result from more trial and error as the idea spreads. Therefore, readers may be surprised to see me advocate electronic insurance exchanges as a way to speed up trial and error spread of the idea's adoption. It is a way of preserving the flexibility of deductibles, benefits, alternative uses of surpluses, and vendor arrangements. It is also a way of narrowing the conflict with the Tenth Amendment, combining state regulation with inter-state marketing. If multiple alternative details prove necessary, direct computer marketing would be a quick way to discover what the permissible alternatives would be. Finally, the widespread examples of other interstate marketing can be employed to search out how to convert marketing from intra-state to interstate, rather than assume certain commerce is inherently (and permanently) interstate or inherently within-state.
An accidental feature of Health Savings Accounts is that the account can be growing for a number of years before the re-insurance feature is frequently needed. Indeed, young people may need a certain form of reinsurance protection and a different form as they grow older. The important feature is to have permanently stable savings vehicle in place while different forms of re-insurance are proving themselves. It seems heresy to say so, but we might even discover niches of the marketplace where first-dollar coverage or service benefits have some useful temporary role.
|
The States Are in the Road
|
1d. PRE-EMPT STATE LAWS WHICH INHIBIT CATASTROPHIC COVERAGE. State mandated benefits now severely limit high-deductible insurance in many states, and are the main reason Health Savings Accounts have been slow to spread. The provisions of ERISA shield employer-based health insurance from the unfortunate health coverage mandates in question. ERISA could not have been successful without this pre-emption, so unions and management unite in absolute concern to isolate ERISA from congressional meddling, although for different reasons.
1e. REVISIT McCarran FERGUSON ACT . This act effectively makes the "business" of insurance the only major industry restricted to the state rather than federal control. It should be amended to permit the sale and portability of health insurance policies across state borders and interchangeability of individual policies when people change state residence, thus greatly increasing competition and reducing prices. Once more, present law discriminates in favor of the employees of interstate corporations, who are also exempted by ERISA.
1f. MANDATE DISPLAY OF DIRECT COST MULTIPLES NEXT TO PRICES (FEDERAL PROGRAMS ONLY) (whenever prices are displayed, as in bills, price lists, etc.) FOR ITEMS COVERED BY HEALTH INSURANCE. Some high mark-ups are justified, but the public has a right to criticize them. This would not prohibit, but would considerably hamper, cost-shifting. It should be presented to provider groups as forestalling the prohibition of cost-shifting because of abuse. For this and other reasons, it would enhance provider competition.
1g. REIMBURSE HOSPITALS ONLY ON RECEIPT OF ASSURED POST-DISCHARGE HANDOVER OF MEDICAL RESPONSIBILITY (FEDERAL PROGRAMS ONLY). Unfortunately, hospitals do need increased incentive to improve post-discharge communication, which now increasingly occurs on a Saturday. Payment by diagnosis, otherwise a seemingly attractive idea, results mostly in sequestration of medical charts within the accounting department. That's undesirable at any time, but is most destructive at the vulnerable moment of hand-over.
1h. Similarly, REIMBURSE HOSPITALS FOR LAB WORK ON THE LAST DAY OF HOSPITALIZATION ONLY AFTER DEMONSTRATION IT HAS BEEN REPORTED TO A RESPONSIBLE PHYSICIAN. Such lab work, frequently obtained within hours of discharge, is sometimes overlooked and may even be unobtainable for the previously mentioned reasons, which in this case also apply to the hospital's own physicians.
1i. RESTORE ORIGINAL FORM OF PROFESSIONAL STANDARDS REVIEW ORGANIZATIONS (PSRO). These physician organizations effectively regulated many issues which are now the subject of the complaint. They were lobbied into ineffectiveness in 1980, and together with "Maricopa", essentially turned medical oversight over to insurance companies who thus receive no physician advice except from their own employees.
|
Treat liabilities like debts. And transfers from the general fund as liabilities.
|
| Accounting, for Congressmen |
1j. ENCOURAGE THE ESTABLISHMENT OF REGIONAL BACKUPS FOR AMBULANCES DRAWN OUT OF AREA. At present, ambulances are limited to going to the nearest hospital, rather than to the hospital of patient preference. The main justification for such behavior is the possibility that a second call might come while the ambulance was in a distant area. Fire departments have long solved this problem by shifting reserve vehicles into an overstrained area, to cover that area while the home vehicle is temporarily unavailable. In some areas, a reserve vehicle backup might require additional ambulances, but mostly it requires a mobile phone network. In areas of extreme distances between ambulances, the main need would be to relax regulations which exclude volunteer vehicles from serving that function. In densely settled urban areas, we now have the preposterous situation of mothers in active labor being stranded at the wrong hospital, only a few blocks away from the obstetrician who has their records. When such situations are repeatedly encountered, the current IRS exemption from financial reporting should be rescinded from the ambulance sponsor.
1k. As a general principle, when a service, device or drug is used in both the inpatient area and the outpatient one has its price exposed to regular market forces in the outpatient arena, the same price should be applied to it in the inpatient arena. It would be sensible to add a (separately negotiated) inpatient overhead adjuster reimbursement which generally applies to inpatients, and a second adjuster for the emergency room. There will be some services which are totally unique to inpatients or emergency rooms, which will have to be treated as outliers. In this way, a mutually reinforcing restraint is placed on such dual-use items -- with the market holding down outpatient costs, and the DRG ultimately holding down inpatient/emergency costs including outliers. As a general rule, the overhead cost-multiple established for dual-use should apply to the single-use items of either in-patient or out-patient. The key to all of these balancing limits is to permit open competition between hospital emergency services and private competitors, and an absolute prohibition of linkages between providers and emergency vehicle operators. After a brief trial, all such price constraints should be exposed to re-negotiation with an eye toward establishing transparent regional norms.
|
The Supreme Court Needs Help, Too
|
2. LEGISLATE OVER-RIDE OF 1982 MARICOPA CASE. This unfortunate U.S.Supreme Court 4-3 decision was never tried and upholds only a motion of summary judgment about a per se violation. It prohibits physician groups from agreeing on lower prices and has been taken to mean physicians are excluded from exercising control of HMOs and Managed Care. It also perpetuates the notion of individual competitors in a profession which is rapidly acquiring larger groupings as units of competition. By some quirk, the full tape recording of the 1982 U.S. Supreme Court arguments can be heard on the Internet. It is "above this author's pay grade" to know whether it would be better to ask the Supreme Court to review its earlier decision, or to make legislative changes in the antitrust law which would somehow result in a better outcome.
Strange Interlude
Once a bill is signed by the President after enactment by both houses of Congress, it is normal procedure for the Executive branch to devise regulations (with the force of law) to implement its intent. Commonly, this process uncovers unintentional flaws in the statute, which is then returned to Congress for "technical" amendments. When there is a politically divided government however, suspicions can be instinctive in the Supreme Court that regulations or technical amendments might be written to conflict with the original will of Congress. Before matters get to that point, however, differences between House and Senate versions must be reconciled, and then identical reconciliations must be agreed by both houses. In the case of the Affordable Care Act, widely differing versions between the two houses were tolerated or even encouraged, but the House version was withdrawn in order to jam through an identical version of the Senate bill in its place. This did avoid the need for reconciliation. However, the maneuver was so hurried it required more than average corner-cutting, and potentially had to accept some un-removable booby traps in the surviving Senate version.

|
| Republican Senator Scott Brown |
A situation of this complexity would be difficult under any circumstances. But the Senate required a supermajority of 60 to evade a filibuster of the reconciliation. The Democrats had a bare sixty, including some with deep reservations which could only be pacified by accepting unwelcome provisions. And, it included at least two Senators in poor health. Consequently, differing Obamacare bills had been passed while there was a safe Democratic majority in the House of Representatives, but only one-vote Democratic filibuster control in the Senate. Democratic Senator Edward Kennedy then died, and an elected Republican, Scott Brown, replaced him. With Democratic Senator Richard Byrd in poor health the original plan to cherry-pick a clever administration hybrid out of differing versions in front of the House-Senate conference committee, became unfeasible, if not dangerous. About the only option seemingly available to the Democratic floor leaders was to adopt one version or the other and then achieve consent for an identical bill from the other house. The Senate version was chosen to survive and be forced through the House in a matter of hours, even though almost no Congressman had read it; and this behavior was conducted under full television coverage by C-Span. Television viewers probably did not have enough information to understand why things were being handled so roughly, but it added to a public distaste for the brutal tactics they could readily observe the leadership had been applying. Although it has been useful to blame excessive partisanship for this mess, it would not be difficult to name a dozen majority leaders in the past who might have surmounted such difficulties with more instinctive ease.
|
| Democratic Senator Richard Byrd |
The Republicans were given no face-saving consideration in any of these matters and reacted with outrage. The obedient Democrats were humiliated by the public watching their abject subjugation. As one consequence, the November 2112 election administered a heavy defeat to the Democrats, while sending a large contingent of freshmen Republican Congressmen with what they considered to be a strong public mandate to disrupt or even repeal Obamacare. Most of these new Congressmen belonged to the "Tea Party", had little experience with the "inside baseball" of Congress, and found they disliked the environment. Many of them had the inclination to repeal this one Act, followed by resigning from Congress after a single two-year term. Their fury at discovering the legislative straight-jacket they were in, must have contributed greatly to the polarization which was already notable. Naturally, the White House bureaucrats destined to write the Obamacare regulations were watching, dismayed by the prospect of claiming controversial opinions to be the "will of Congress". At this writing, it seems likely at least some regulations will come under consideration by the U.S. Supreme Court, for failing to follow the intent of Congress, for following an unconstitutional intent, or for failing to implement statutory sections of the law at all. Therefore, it would not be surprising to find some regulations which were then written, contained some "booby traps" for the Supreme Court. All of this would seem to predict epic contests between Chief Justice Roberts and President Obama, both of them constitutional strategists.
Meanwhile, many Republicans and some Democrats are calling for the President to postpone implementation, ostensibly until the enrollment computers are fully functional, but really hoping to get past the November 2014 elections. The approaching State of the Union address might have been an opportunity to blow the trumpet of compromise. But Barack Obama has proved to be an unusually stubborn person, and the prospect of facing an opposition majority in Congress does not seem to bother him. If he chooses to tough it out, perhaps we can finally learn exactly what he had in mind for the Law. If it is of any consequence to him, he had managed to get this far without fully revealing what he was trying to achieve. Almost before Senators Kennedy and Byrd died, the Tea Party gained control of the House, and Obama was forced to work his own way out of a hodge-podge.
A major tactical part of this strange interlude grew out of what lawyers and courts call "Standing". The Supreme Court, in particular, is rigid in refusing to hear a case where no one has been injured. Anxious to avoid hypothetical arguments more properly the province of the Legislative Branch, the Court insists on hearing real cases of injury by one party against another. When a new law has not yet been completely implemented, there is likely to be an interval when no one can claim he has been injured by it. That is, no one at all has "Standing". As we will see in a minute, various state governments took the position that the law injured them by invading what the Constitution declared was the province of the several states. And therefore, the states had been injured by the law, even though no insurance policies had been issued. It will be noted the Court's decision in the case confined itself to this argument. Obviously, it reserves the right to take up the case a second time, after millions of people acquire standing, and the Court can choose which argument, by which person with Standing, it chooses to hear.
Cost Effect of Increasing Longevity
Since healthcare is more expensive in older people, Medicare costs should rise in the future, right? Well, actually that could be disputed. Medicare costs may rise as a result of new and more expensive treatments, but increasing longevity by itself can lower costs. Since it surprises most people to hear it, follow the logic carefully.
It costs about $171,000 per lifetime to run Medicare or about $13,000 per year at a life expectancy of 78. That's the figure of the census bureau all right, but it's the life expectancy at birth. Life expectancy for a person age 65 is in the 80s, so the average yearly Medicare cost is closer to $5000. If we look ahead a few years, it is easily possible to foresee a life expectancy of 91. That would be a yearly cost of around $6000. But you would have to pay medical bills for an extra few years so costs wouldn't go down, right? There are three possibilities.
One possibility is that the costs of the elderly are mostly terminal care costs. Since you only die once, increasing longevity may mean that you typically increase the length of being old but healthy, followed by a single terminal illness. In that case, average yearly costs should go down with increasing longevity. Another possibility is that living six or so years longer just gives you the time to run up more bills for more illnesses. You might have time for two fatal illnesses, from one of which you recover. There's still a third possibility. A lot of people in their late fifties may store up illnesses as a backlog which emerges while Medicare begins paying the bills but gradually subsides. What does the data show?
The data shows that aggregate costs are slowly growing at a rate well below 6%, so if your savings are growing at 6%, you are gaining on it as you get older. If you invest $85,000 at 6% on your 65th birthday, Medicare will consume the whole amount by age 78. But on the other hand, if you invest $40,000 at age 65, Medicare will only consume it (half as much, notice) by the age of 91. It should certainly be clear that Medicare costs are growing considerably more slowly than 6%. They are growing, but a shrewd investor could certainly beat them. And since the Federal Reserve targets a deliberate annual 2% inflation of the currency, Medicare costs net of inflation are growing considerably slower than 4% a year, for whatever reason. If Medicare costs should rise, or if the economy worsens, there's probably a tipping point where increased longevity becomes a bad thing for your financial health. But we haven't reached that point, yet.
If some young math genius invests $310 every year at 6% from age 25 to age 65, he could buy out his Medicare entitlement for $50,000. When life expectancy was 78, he could have bought it out for $85,000. Pre-payment would have cost $520 per year, 25 to 65, at 6%. If some enlightened government would stop collecting Medicare premiums and Medicare payroll deductions, our math genius could have it for half the price. And the government? They could stop borrowing from the Chinese, an amount equal to half the cost of the program, so it's a win-win situation, right? Maybe it's even better than another sustainable growth factor.
What Part of Medicare Gets Paid?
Unthinkingly, many people believe Medicare completely pays all medical costs for 44 million eligible recipients. Not by a long shot. In the first place, many medical costs are ineligible for Medicare reimbursement; the largest is nursing home care. About 5 million recipients are "dual eligible", which means they get both Medicare and Medicaid coverage, and then state Medicaid programs do pay for nursing homes to a variable degree. The federal government excludes "custodial" care, but to some degree does pay for "skilled nursing care" , so the nursing home matter often seems ambiguous, and becomes the source of some resentment.
Beyond that, patients are responsible for annual cash deductibles, hospital daily deductibles and about 20% co-insurance, all of which are really Medicare-related. The 20% coinsurance was allegedly meant to generate cost concern by demanding patients "have some skin in the game", but the great majority of patients promptly took out a second, co-insurance, coverage, so any cost restraint has long been eliminated for them. They have to pay a second insurance administrative cost, plus its profit margin, however. A 20% co-payment isn't enough to influence behavior, while the ability to budget retirement costs is more important to elderly people on a fixed income. They soon see the foolishness of buying a 20% insurance to cover a 20% discount on the first insurance, but the reaction is not that it's stupid, but rather, that Medicare is stupid. Furthermore, if the individual has Major Medical Insurance coverage, some additional odds, ends and outliers are covered, but with with a third insurance layer of cost and profit added. Once it was discovered that insurance profitability was also enhanced by a great many people neglecting to file a Major Medical claim form, the incentive of the insurance industry to protest the situation was effectively smothered. In summary, by addressing the total costs of the elderly rather than Medicare alone, we can claim the elimination of this triple insurance cost, which somehow escaped the attention of the designers of Obamacare for their scheme. In fact, it can be suspected that many advocates of "single payer" are imagining the elimination of this duplication.
In addition, the Medicare patient pays premiums, which amount to a quarter of Medicare cost, and derived from young working person from age 25 to 65, the 2.9% payroll deduction contributes another quarter. We can't both collect it, and still assume it as a cost for the taxpayer to assume. The remaining 50% of the Medicare cost results in a deficit, paid for with debt, largely owed to the Chinese. There's a lot of rounding error and approximation in the reports, but the impression is gained that the U.S. government doesn't pay very much of Medicare costs at all, except for its administrative costs and the debt service. But in fact until those debts are finally settled, no one can say how much the government pays for Medicare.
Since our present purpose is not to pay the costs but to approximate them for discussion of alternatives, rounded-off costs, are perfectly adequate. Approximations only contribute serious errors, if applied in different ways to different payment systems. The individual and his employer are now paying somewhat more than half of Medicare costs, which are perhaps 70% of the total medical costs of the elderly, and the remaining 30-40% is a government obligation whose ultimate settlement is not yet determined. It's not easy (impossible?) to say what we might be paying if these costs were borne by a new financing arrangement. Most economists say the employer contribution is adjusted in fact by lowering wages by an equal amount, and that in turn is recouped in part by income taxes. Furthermore, the Chinese loaned us the money with the expectation of being repaid, so there are outstanding debts from the past which must be figured into the calculation.
Under these circumstances, it seems appropriate to start with a way to pay the total program costs of Medicare. We'll start with that, making a mental note that there's probably 25% (?) more, and try to cope with these other leads and lags, by trying to offset them during the transition, or just by letting the Government Accounting Office figure out the rest. Medicare program costs are a known quantity for use in a program re-design, while other unknowns are for others to conjure with.
Congressional Hearing: Health Savings Accounts
Thank you for asking me to describe Health Savings Accounts. In five minutes, I will try to make four points.
HEALTH SAVINGS ACCOUNTS, OLD STYLE.
Thirty years ago, John McClaughry of Vermont and I devised the Health Savings Accounts you may be familiar with, and millions of people have tried them with satisfaction. It has been reported that they can reduce healthcare costs by as much as 30%.
They consist of two ways to pay for Healthcare. Essentially, one is an individual investment account, rather like an IRA, or Individual Retirement Account. The subscriber usually uses a special bank credit card and receives an income tax deduction if the money is spent on healthcare. The account is individually owned, as an incentive to be frugal and shop wisely, because whatever money is left over he may keep in a regular IRA. He needs to deposit into the account, only such money as he requires for healthcare, depositing less if he has been frugal in the past. If he deposits more than he spends, he gets it back with interest. These healthcare expenditures are usually office or outpatient expenses, subject to shopping around as vigorously as he chooses.The second form of payment comes from a high-deductible health insurance policy. This policy is ordinarily used for hospital inpatient expenses where the patient has very little ability to choose or to shop, and where payments are usually lump-sums derived from a system called DRG (Diagnosis Related Groups). This has proved to be an effective cost restraint.
Right now, if you don't have an old-style HSA, you probably can't get one. Recent regulations forbid new accounts for persons over the age of thirty, the accounts are only partly tax-deductible, and existing accounts end when Medicare begins. These are artificial, and I hope temporary, barriers which could be swept away in an afternoon of Congress.
HEALTH SAVINGS ACCOUNTS, NEW STYLE. (Lifetime Health Savings Accounts)
To these two original building blocks, I now propose to add two new ones. They both probably require legislation, and they may even need to be considered in separate committees of Congress..
One new feature to Health Savings Accounts is a lifetime, or whole-life, policies substituted for present one-year term formats. Not only would that save marketing costs, and permit permanent funding. Obviously, lifetime policies must somehow be portable between states.Lifetime health savings accounts have the surprising ability on paper at least, to pay for most of the healthcare costs by themselves. True, the McCarran Ferguson Act is in the way, and maybe even the Tenth Amendment. But major reductions of healthcare costs are too important to ignore, without first examining work-arounds.
The second is passive investing , a Wall Street term for eliminating churning and stock picking by using total-market index funds. This system promises to return 12% per year to the investor, but I quote John Bogle that the financial system extracts 85% of the return before the investor gets it, just as it does in many 401(k) plans. This battle of fees needs to be fought out because, in the case of healthcare, thirty extra years of longevity have greatly increased the return available for disorders of old age, which predominate. In thirty years at only 7%, money will have three doublings, or multiply eight times. You could lose half of it in a stock market crash, and still, have 400% of what you started with.
Examples
First Example, single payment of relatively small deductible. The smallest deductible in the Obamacare Insurance Exchanges is $1250. If a deposit in the HSA is made at age 26 to cover this contingency but never used, it should rise to $10,000 if invested in U.S. Treasuries at 3.7% -- by age 85. That won't get you where you want to go, but it may be the least that can be afforded.
Second Example, single payment of $6300.The the largest deductible in the Obamacare Exchanges is $6300. A single deposit of this size at age 26 will reach $10,000 at age 40. At that point, we can hope that 10% is generally available in the marketplace, and thus would reach $24,000 at age 65. An IRA of $24,000 will start paying pensions at the minimum distribution rate of $960 a year. In a sense, that's not a bad investment of $6300, but everything has to go smoothly (in health as well as finances) for 39 years to achieve it. The point of these first two examples is to demonstrate that HSA is probably not able to overcome current abnormally low short-term interest rates enough to be used solely as a place to park small deductible reserves. At $10,000, it becomes feasible, and when interest rates return to normal levels, it may again be feasible for small savers.
Third Example, single payment of $10,000 (deductible reserve of $6300, plus $3700 cash), at birth. This cash contribution at birth will not only match the $10,000 minimum demanded by brokers for unrestricted investment (i.e. for eligibility for 10% long-term investment return), with an added bonus of reducing premiums for paying a higher deductible. Now, this one is far less accessible, but it illustrates some important points.
At one time, a $25,000 deductible health insurance policy was available for an annual premium of $100; but while times have changed, it still remains true, the higher the deductible, the lower the premium may be. Secondly, the lower the premium, the more is left for investment. This deposit, if placed in an IRA at age 26 at a 10% income rate, would generate a fund of $411,000 at age 65, making possible an annual pension of $15,000. Quite a contrast! The third feature is that starting the compounded income at birth instead of 26 adds nearly four doublings to its investment horizon. The ultimate consequence would be a comfortable retirement fund of $60,000 a year. What's mainly standing in the road of this windfall, is all the current dissension about the place of the family in American life. If it is the parent's duty to supply healthcare for their children from the moment of conception, then the cost is an obligation and should confer ownership of the benefits. If the child didn't ask to be born, his costs are his own and, while the parents may make a gift or a loan, the benefits are the child. And if there is a divorce or illegitimacy, the support costs are probably the determining factor. Quite obviously, we are at quite a distance from a basis for settling this issue. If you throw in the costs of an abortion subtracted from the cost of being born, you go off on another tangent, one you probably never return from.
Should we treat Obstetrics and Pediatrics as a loan from parents to a child?After all, the insurance location of Maternal/Childhood Coverage Could Add 26 Years of Compounding and solve several problems which are now beyond the scope of this book. It seems like a problem which could be reserved for a later time since lifetime coverage can be addressed without it, no matter if it would be simpler to include it. This is a book about healthcare finance, with every incentive to avoid thorny society problems. However, a collision occurs when we attempt to include the rather considerable costs of obstetrics and/or abortion, and the comparatively minor medical costs of children under the age of 26. The goal is not so much to protect against these costs, as to add 26 years of compounded investment income to the calculations, and the problem is that our society has not completely decided whose financial responsibility such costs belong to. Judges make expedient decisions in divorces and illegitimacy; but issues like this, for them to stick, must really be made by society in general. For purposes of long-term prediction, we will, therefore, assume that a child is responsible for his own birth and subsequent medical costs and that someone else in the family is responsible for reimbursing the child. Treating costs as the infant's responsibility is something of a fiction, like pretending each child has a trust fund to pay everybody back at age 26, but it will have to serve.
At the moment, everybody does have some mechanism for paying Obstetrical costs, even while that mechanism is only to rely on charity. The costs have already been assigned to someone. For the most part, Obstetrics is now part of the parents' health insurance policy. It must be admitted that the true costs are not readily available since the whole matter is tangled in internal cost-shifting by hospitals and insurance policies. However, they are determinable by someone, and eight thousand dollars seems adequate. Two hundred dollars a year seems right for average childhood costs from birth to age 26 but obviously, better data would improve the precision. We take a guess at $8200 for obstetrics and pediatrics combined or $5200 for pediatrics alone. At 10% investment income, the fund would overtake the pediatrics in 26 years, and possibly allow the fund to break even on the Obstetrical costs over the 26 years. For a while at least, policies like this should allow the managers to gain experience; if the investment pays the medical costs, then enough of the obstetrics will be double-paid by existing sources to make the whole experiment escape insolvency A pilot study of four or five years, in four or five states, might clarify the issues. After that, it should be possible to establish profitable levels for the package. Somewhere mixed up in this are the inordinately concentrated malpractice costs of obstetricians. We look longingly toward the Chief Justice and the Judicial Council to rationalize this wasteful situation, and then for the ensuing savings at 10% for 26 years to get most Health Savings Accounts off to a profitable level by age 26. This complicated sentence structure may seem a round-about way to streamline transaction costs for HSA brokers, but something like that will have to be done to reduce transaction costs, which are probably roughly equitable in the first and second examples. But nevertheless, costs must be reduced because of the tremendous jump in gains in the third example is too attractive to be ignored. In summary, in this discussion, we regard the initial high obstetrical costs and the low pediatric costs which follow, as a wash. We can come back later and tinker with details. But the important point at the moment is to stress that we can garner 26 years at 10% compounded investment income, by simply declaring them to be manageable break-even costs.
Fifth Example: Deductible Reserve, Generous Returns, for Twenty-Six Additional Years. All of this begins to merge with the idea of lifetime health insurance, which is the subject of the next Chapter. So we need to add at least one new idea, which is whole-life health insurance. We end this term-insurance line of thought with the stockbroker's hard-nosed assessment that he can't make a profit with this idea unless he starts with a $10,000 nest egg, or else charges hidden fees. The first $6300 gets provided by Obamacare's discovery they can't make health insurance work without a $6300 deductible. Matching that is my own assertion that no one should risk using $6300 deductibles unless he can see some source for the money, whether it is a government subsidy or his own personal savings, of enough ready cash to cover one year's deductible. Even so, we have to find another $3700 to get to the safe harbor of ten percent. If such a thing as $10,000 deductible became available, it would close this gap without borrowing, because higher deductibles make lower premiums possible, and eventually you break even. But right now, the individual has to borrow $3700 to make this work. Because the new father and mother are young, they are going to have to pay a higher interest rate, and we might as well assume a loan-rate of 10%. But it's 10% on $3700 of it, which makes the whole fund eligible for a 10% return. In round numbers, that's $1000 minus $370, or a net gain of $630 a year; reducing the loan balance to $3100 the second year, $2500 the next, etc., You would have to be working with real Obstetrical costs to know how much it would cost, but this is the general idea behind calling the initial cost a wash.. Now, where does that leave us, with essentially $10,000 to prime the pump, and starting with a growing income of $1000?
Well, it leaves us with $80,000 at age 26, and literally millions at age 65. The numbers are so generous we see no need for precision. We can now see a clear path from a cash contribution you must make, to quite enough money to pay all average lifetime medical costs by the age of 65. All medical costs, so no 6% payroll deduction, no premiums, become a possibility. And with enough extra cash emerging from the calculation to make it unnecessary to use a calculator to be reassuring. Only by getting another 26 years of income does it become possible, but it does make it unnecessary to have quite so many assets when you start being a capitalist at birth.
As a footnote, we find it unnecessary to tell bankers how to smooth out repayment of $10,000 from people who are pretty much guaranteed to have millions before they die; it's what bankers do for a living and they are good at it. But there is one other risk inherent in this discussion: the risk that any particular individual could get very sick several times. In some circles, the solution to that contingency would be called "reinsurance", and in other circles, it implies "subsidy". But, otherwise, this system has only one remaining difficulty. It would take 80 years to prove itself. That might seem like a great handicap, until it gets compared with the risk of taking on too many complex tasks, too rapidly. One of the great advantages of taking this approach is that its several steps force major readjustments to be gradual.
Blue Sky Flying for Congress: What to Do With Money Which Health Savings Accounts Drop in Your Lap
Let's be clear about our role. It is to suggest four or five main ways to rearrange health financing, so enormous sums are available to reduce health costs. Once the money is available, only Congress can decide what to do with it. In fact, my prediction is anything else would be brushed aside as an amateur suggestion. Nevertheless, I have given the matter some thought, and offer my ideas. They begin with leaving the practice of medicine alone, on the grounds that the public will not support any major intrusion into what they consider their private affairs. And my suggestions end with the opinion a change such as I propose can only be done once in a century. So please get it right if you do it.
Starting Young, and Playing With Numbers. The power of compounding is brought out by starting really young, possibly even at birth with a gift from parents. At 10%, money doubles in seven years; at 7%, it doubles in ten. In 65 years there are eight doublings at 10%, six doublings at 7%. The real power of compounding comes at the end of the series. The last three doublings were added in the past century. It makes them eight times as valuable to us as to our grandparents. So, something slow, gradual and unnoticed, creeps up on us before opening an entirely new set of possibilities.The Debts of Our Parents. We started by showing it would likely be feasible to assemble $80,000 by the 65th birthday, and that much money on average, would likely pay for Medicare because the relative values will not change unrecognizably in thirty years. Remember, Medicare is spending $11,000 a year on the average Medicare recipient, for roughly 20 years, or roughly $200,000 during a 20-year lifetime after 65. If you start with a nest egg, sickness will slowly wear it down. At the same time, you do make a certain return on your nest egg. The goal is to build the egg up when you are working, so you have something to spare between the interest you make on your nest egg, and the annual cost of the illness. Eventually, the sicknesses win the race, but your task was to stretch things out as long as you can. Eventually, a few people will have to resort to dipping into the last-year-of-life fund (see below), and if things go badly wrong maybe we can only pay fifty cents on the dollar. There is this contingency provision, but it will not be infinite.
Eight times as valuable to us as to our grandparents.Three doublings added. We divide the roughly 85 years of life into three compartments: (1) Children from birth to age 25, whose health expenses are a debt they owe their parents. (2) Working people, from age 25 to 65, who essentially generate all the wealth of society. (3) And over 65, when working income ceases, and living costs are paid from savings generated earlier in life. There are forty years to earn, preceded by 25 years of being supported, and followed by 20 years of living on savings. That's why so much of this book pivots around ages 25, 65, and 85. If you learn it from your parents, you get a head start. If you must learn it for yourself, mostly it's all gone before you react.
Learn from your elders, get a Head Start.If You Learn for Yourself, mostly it's gone. Working backward from $80,000 at age 65, you need to start with only $200 at birth with 10% working for you or $1,000 at birth with 7%. What's the significance? If you make a lump-sum payment of $80,000 on your 65th birthday, the lump sum generates what we now assume is the lifetime average cost of Medicare. Translating $200 at birth into $80,000 in 65 years is definitely possible. Figuring out how to translate the money earned into what the average person will spend 65 years later, is too complicated to be precise, but we have learned you always underestimate the change in such a long period. We always underestimate the change, but the cost of it cannot exceed the money we will have. Paradoxically, that may be a little easier. Remember, the stock market averaged 12.7% during the past century, but here we only project a 10% return to an investor, therefore few would dispute results of this financial magnitude are a reasonable goal. I'm not entirely sure what we are predicting, but perhaps it is an invisible limit to the rate of inflation a viable economy can withstand. No gold or silver standard, but perhaps the velocity of money standard. Maintaining a future goal of 3% inflation during the next century, for example, seems entirely within the power of one person, the Chairman of the Federal Reserve. He may fail, and the world economy flies apart, but if it holds together, something like this velocity will have to continue, even if we all are commuting to Jupiter for lunch. The final conclusion would be unchanged: a comparatively minor investment at birth could be fairly comfortably projected to pay for average Medicare costs, half a century from now. You might even get all of Medicare for a single $200 payment; now that's really a bargain. Even $1100 (at 7%) is still a trivial price for retirement with unlimited health care. But remember, we are not promising to pay for it all, just some big chunk that presently isn't paid for. During major inflations such as Germany, Russia and China had, the individual nation disintegrates but eventually catches back up with the rest of the world. Our whole financial system seems to have been stabilized by some such notion for the past four or five centuries.
Let's examine the concern, which isn't entirely fanciful. Since earning power starts to disappear around age 65, there will inevitably be some people who throw themselves on the mercy of Society with no hope of paying their substantial medical costs. My suggestion is we anticipate this contingency by initially excluding payment for healthcare in the last year of life, which as I have said many times, comes to everyone. Because nearly everyone who dies, is on Medicare, we have pretty good data about the cost of the last year of life. Setting aside the funds to pay for it would allow us to add the cost to our estate or insurance. For those who have somehow escaped pre-payment however, this remains the last final debt and a fairly substantial one. Segregating this debt as the last unpaid one, allows for the people who fall through the cracks, to fall through this one, last. Whether we make this deficit into an unfunded debt of society, or a pre-funded responsibility of a benign society's natural obligations to its citizens, or a debt of society to its medical institutions -- makes only a rhetorical difference. The problem has been concentrated in a single focus, where it can be dealt with as generously (or as tight-fisted), as we choose to appear in the eyes of the world. As envisioned, all other debts are paid before this one, so to some people, it will seem like a contribution to the Community Chest, while others will treat it like highway robbery by welshers and ne'er do wells. But at least we have provided for what we all acknowledge is inevitable.
We estimate compounding will add more revenue, roughly matching the costs of robust stragglers who live from 85 to 91. That is, the growing costs of the elderly are like a longer neck on a giraffe -- rather than a bigger belly on a hippopotamus. Average costs actually go down a little after 85. We assume a fair number of them will be healthy during most of the extra longevity, with heavy terminal care costs merely shifted to 91 instead of 85. We started at age 65, with 65 years of health costs already paid; we paid down the estimated costs of twenty years, and the interest on the remainder pays five more. We get there with money left over, we haven't diverted the premiums from Medicare, and we still have to pay for that last year of life. Except we let Medicare calculate the average cost from the people who decline this gamble, and the fund reimburses the hospital or whatever, for average terminal care costs -- during what is only then recognized to have been the last year of life. If the money from fund surplus isn't enough, the agency can look at raiding the Medicare payroll deduction pool. And there can always be recourse to liberalizing or restricting enrollments, to age groups which experience shows will either enhance or restrict the growth of the fund, as predictions come closer to actual costs. And finally, the last recourse is to have the patient pay for some of his own costs, himself, by re-instituting Medicare premiums. Those who feel, paying for all of the healthcare with investment income was always a pipe-dream, will feel vindicated. But all this book ever claimed was it would reduce these costs by an unknowable amount, which is nevertheless a worthwhile amount.
Whoops, Medicare is Subsidized. A major explanation for the astounding bargain in Medicare funding can be traced to a 50% subsidy of Medicare by the Federal government, which is then borrowed from foreigners with no serious provision forever paying it back. Medicare is: about half paid for by recipients, about a quarter paid for by payroll deductions from younger working people, and about a quarter paid for by premium payments from Medicare beneficiaries, collected by reducing their Social Security checks.A quarter paid in advance, a quarter paid at the time of service, and half of it a subsidy from the taxpayers at large. No wonder Medicare is popular; everybody likes to get a dollar for fifty cents. But the Chinese might be astonished to hear Medicare described as self-funded, sort of ignoring the repayment of their loan.
|
America's Big Benevolent Gamble.
|
| Billions for Research |
That's indeed how much it will cost if you do it all by raising revenue. You can also do some of it by cutting costs, where fortunately we are well along on a uniquely American way to do things. No one else has the money to do it our way, so everyone else tries to cut costs by turning out the light bulbs. But without saying a word, notice how we have united in what the rest of the world thinks is madness.
|
Americans Unite, Others Think It's Madness.
|
| Eliminate Costs by Eliminating Disease |
Consider a moment, how difficult it is to say how much medical care will cost. Remember, a dollar in 1913 is now called a penny, and today's dollar is very likely to be called only a penny in 2114. We long ago went off the gold standard, and money is only a computer notation. Looking back, it is remarkable how smoothly we glided along, deliberately inflating the currency 3% a year, and listening to assurances this was the optimum way to handle monetary aggregates. Even more remarkable still is to hear the Chairman of the Federal Reserve ruminating we don't have enough inflation. It took a thousand years to get used to metal coins, several centuries to get used to paper money, and almost a century to get used to being off the gold standard. The political task of convincing the whole world that inflation is a good thing sounds very close to starting a world-wide civil war.So, here is a plan for paying for healthcare, which is nothing if not flexible. If we start running out of money too early, we just don't pay our foreign debt, that's all. Doing it overtly is probably to propose a change in our entire culture so it would be done by inflation, a dime on a dollar.But we now have more than a million people over the age of 100. They got cough drops as a baby for a penny, and now hardly blink when a bottle of cough medicine costs several dollars. But instead of that, they are likely to get an antibiotic which was not even invented in 1913, retail cost perhaps forty dollars when it was invented, and now can be bought for less than a dollar. If they got pneumonia in 1935, they probably died of it, no matter how much was spent for the 1935 medicine, so how do you figure that? Or someone who got tuberculosis and spent five years in a sanatorium, who today would be given fifty dollars worth of antibiotics. The problems a statistician is faced with are impossibly daunting.
The current practice, which reaches the calculation of $325,000 for lifetime medical costs, is to take today's health costs and today's health predictions, and adjust the average health care experience for it, both backward and forwards. Every step of this process can be defended in detail. But the fact is, average lifetime health cost of someone born today is only the wildest of guesses, no matter what kind of insurance is in force, or who happens to be President of the United States. The cost of drugs and equipment go through a cycle of high at first, then cheaper, then they vanish as useless. But adjusting the overall cost of materials and services when only a faint guess can be made about healthcare and disease content, can be utterly hopeless, or it can be quite precise. Unfortunately, even its probable degree of future precision is a wild guess. It's a wonderful century to be living in unless you are a healthcare analyst. The only safe way to make a prediction is to make a guess that is too high and count on public gratitude that it actually wasn't much higher than you predicted. But to guarantee a particular average outcome, which an insurance actuary is asked to do, will be impossible for quite a few decades.
If that isn't enough, we inflate some more until we can stop running up foreign debt.
If that isn't enough, we cut costs, inflate some more, and reduce the quality of health care.
And if that isn't adequate, we put a stop to funding biological research, by letting foreigners try their luck at it. Americans would be particularly loathed to do that because it represents a confession we were wrong about our boast to put an end to the disease.
This four-step process is absolutely mind-boggling to me, absolutely unspeakable, although the Chairman of the Federal Reserve is able to hint around about it. To me, it is so repellant that absolutely no circumstances would allow me to endorse it, and my hope is that just the mention of it will be enough to stir up the newspapers and the Congress. Stir them up, that is, to take some of the harsher measures which are necessary to withstand such suggestions. Meanwhile, we have the satisfaction of generating some compound income on the premiums, which will make the direst eventuality, to be not quite as bad as otherwise.
To keep track of how we are doing, the alternative I propose is to create a semi-permanent agency with adequate resources to oversee the transition and release honest white papers about how it is going, judge how it must be modified. After that, no doubt, a blue-ribbon oversight board must be appointed with power to suggest to Congress what needs to be modified. The blue-ribbon approach is to designate a couple of dozen private institutions to send one representative, and to rotate the appointees among a smaller board than the number of institutions which nominate one. Let's say, twenty positions among thirty institutions, rotating on a three-year cycle, to minimize overlap with Congressional elections. No doubt, that would produce an annual flood of half a dozen books a year by board members, agitating a process which is ultimately decided by elected Congressional representatives.
Former Foreward to Saving for a Rainy
George Ross Fisher, MD
Philadelphia
January, 2015
three intended as part of a larger volume about the Affordable Care Act of 2010, commonly called Obamacare. However, that episode is vexed with unexpected developments, so I set the longer version aside lest it gets longer. This slimmer one concentrates on what I would offer in place of the ACA, or at least parts of it. I fully expect any criticism of an American President's plan to be greeted with, "OK, wise guy, what would you suggest that's better? " So, here it is.It's the Health Savings Account, in two forms, single-year and multi-year. The 1981 single-year version works pretty well, but the passage of time suggests a dozen or more tweaks, which are explained individually. The original version has often demonstrated a 30% cost reduction among several million early-adopters. So perhaps if we polish a few rough spots, the 30% savings will spread even further. Whether it spreads any faster will depend on national politics.
Meanwhile, in searching for more ways to cut cost, I discovered less expensive variations of Health Savings Accounts can be developed on a lifetime model. Lifetime insurance makes it possible to eliminate costs like covering gall bladder removal in people whose gall bladder has already been removed. That's the idea which started me down this path. Even more important, however, it soon provided a framework for combining several advances like whole-life insurance, passive investing, direct-pay insurance and eventually, even some Constitutional reconsiderations. Adding complexity worries me because although some people will quit trying to understand complexity, and just adopt it because it works, other people will reject it, just because it sounds confusing. As it gets more complicated, it also must get more paternalistic; opinions differ on whether it is an advantage. There are enough Americans who won't accept anything unless they understand every word of it so their carefulness will keep it slowed down. Even that has its advantage: a careful approach upsets fewer apple carts.
No doubt the two versions of Health Savings Accounts could be described in fewer pages. But greater density can hinder comprehension, seldom helps it for fast readers. Furthermore, presenting an alternative without a critique would leave the reader uncertain whether I believe the Affordable Care Reform presently goes too far, or not far enough. (In fact, both things are true, because it seems so likely both government and business employers will abandon the patient in pursuit of other agendas.) At the same time, the Affordable Care Act seems politically unsustainable. It costs too much. It needs more balance between benevolence and fiscal prudence, and it certainly needs more restraint to both sides protesting the other will ruin us. Of course, we must do what we can for the poor. But we also need to stop promising more than we can deliver. In the very long run, it won't be politicians, it will be scientists who seriously reduce the cost of disease for everyone, by eliminating diseases. Until that happy day arrives, we need to maintain a lowered tension of aspirations. When government and business operate as partners, that's nice, but somehow it doesn't sound like a level playing field for the rest of us. But having business and government at odds with each other would fit anybody's description of unsustainable.
The Affordable Care Act contains at least two innovative ideas which I certainly endorse. The idea of direct payment of insurance from client to the insurance company (replacing employers as absentee brokers), is good since it reduces the temptation for financial intermediaries to abuse the role of umpires. Rent-seeking is the technical term for this, I believe. Most office and outpatient claims could easily be paid by a bank credit card, streamlining the slow and expensive claims processing approach. Sadly, we may never know the full benefits of direct payment, because public dismay at the fumbling introduction of computerized insurance exchanges could poison direct-pay indefinitely. And secondly, to go on with my diplomatic message, the ACA use of a "cap" on out-of-pocket payment seems like a simple, clever way to avoid adding another costly layer of reinsurance. The system already requires three levels of insurance (basic, supplementary, and major medical) to pay simple claims completely; it doesn't need more layers, it needs fewer. These two features, translated as -- more business efficiency, and less mission-creep -- could easily be allied with Health Savings Accounts, which in the past brought financial pragmatism to several million Americans, voluntarily. Remember, this country responds poorly to almost anything containing the word "mandatory".
However, two points of agreement are not enough innovation to balance the remaining unevenness. I regret how the Affordable Care Act continues to push the square peg of "service benefits" into the round hole of casualty insurance. That sort of incompatible mixture befuddled things for a century, and I look for little good to come of it. Except for helpless hospital inpatients with a tube in their nose, service benefits generate rent-seeking, because service benefits blur the boundaries and create loopholes. Later on, we describe the confusion and exploitation created by service benefits (renamed Diagnosis-Related Groups) as a method of reimbursement. If sharpened and refocused, they could ease the problem of negotiating prices with people too sick to cope with finances. But the wide implementation of that inpatient approach without vigilant pilot testing has resulted in chaos in outpatient pricing. Even dropping DRG and returning to the old system would now pose a daunting risk, for one main reason. The DRG system has made hospital outpatient prices -- totally meaningless, and bewildering to patients who encounter two widely different prices for the same thing in the same institution. As a goal, the techniques of service benefits should be revised for inpatients, but eliminated for outpatients, who are generally alert for bargains. Two systems of payments perhaps, but reaching roughly the same price. As it happens, this uproar is not the fault of Obamacare, nor is its remedy inherent in Health Savings Accounts. But neither system of reimbursement can function without understanding what hospitals are all about.
The Health Savings Account is a mixture of two approaches which more accurately reflect the natural expectations of consumers. It's a mixture of cash payments with insurance coverage. It can be viewed as cash with insurance standing behind it, or it can be viewed as insurance with cash to fill in its gaps. It's definitely a step away from One Size Fits All. That may make a problem for Congress to decide which committee has jurisdiction, but in practice, it is more useful to address the larger issue, which is making the customer happy. The tendency should be resisted to specify by law that one system is to be used for inpatients, and the other for outpatients, for example. That's the way it mainly works out of course, but there are plenty of exceptions. My friends in administrative positions will have to forgive me for saying no one really likes uniformity -- except administrators. What has evolved is failing to appreciate the difference between a marginally better choice for everybody, and a clearly better choice for a majority. We have democracy all right, but there are many cases where multiple choice is more suitable than the majority rule. Admittedly, individually owned accounts create technical difficulty for cross-subsidy of expensive items, and I thoroughly understand the nation's attachment to pooled insurance as a way to subsidize the poor and helpless. But other patients have special problems, too. An unwarranted affection for simplification leads to this kind of outcome.
Perhaps we do start to wander off the topic, which is saving money for healthcare. In a larger sense, it is only a small part of another larger problem, which is how to fix an engine, while the motor is still running. Neither one of the larger topics, however, is the main mission of this book, so let's restate what it is.
Regardless of chapter markings, there are only two topics: regular Health Savings Accounts, as they exist today. And Lifetime Health Savings Accounts, as I hope they will evolve, tomorrow.
George Ross Fisher, MD
Philadelphia
January, 2015
Supreme Court Rescues Obamacare, June 26, 2015

|
| Obamcare |
The case of King v. Burwell was argued before the United States Supreme Court March 4, 2015, and the decision was reported June 26, 2015. In a clear victory for President Obama, the Court held that it was not the intent of Congress that a phrase in the statute, even though repeated six times, should be the final meaning of the law. Someday a participant in the writing of the law will come forward and tell the story of how the words got into the statute in the first place, but at the moment all we know is the words are there, and the law is unworkable if they remain. Just about everyone would agree these two statements are true. Furthermore, it is clear only Congress could change them, and Congress has changed parties since they were originally written; so they probably cannot be changed at all before new elections are held, unless the President agrees with Congress to do it. There is a third possibility: Congress and the President could make private agreements about what they would compromise on and present a friendly adjustment. Whether that was tried and failed, or whether it was not tried at all, is unclear. So, the Supreme Court did what it never wants to do, it changed the law.
Since millions of citizens had watched (on C-Span) the legislation, dropped on the desks of astounded Congressmen, with no opportunity permitted to debate or amend it. Indeed, even to read most of it before it was voted on, the public is inclined to take the Court's word for it, that...
"The Affordable Care Act contains more than a few examples of inartful drafting".Whether the clause in question was accidental or not, is a matter of opinion. The clause in dispute reads, and is repeated six times, as
Tax credits "shall be allowed" for any "applicable taxpayer", but only if the taxpayer has been enrolled in an insurance plan through"an Exchange established by the State under [42 U/S.C., pp18031]" pp36B(b)-(c)Some idea of the Court's historic position is given in a few quotes:
"In a democracy, the power to make the law rests with those chosen by the people. Our role is more confined--"to say what the law is."--Marbury v. Madison, 1 Cranch 137, 177 (1803)In the end, three conservative Justices, Scalia, Thomas, and Alito found there was no reason to change the language of the statute as ambiguous, and four liberal Justices, Ginsburg, Breyer, Sotomayer, and Kagan found there was. The two swing Justices, Kennedy and Roberts, joined the liberals in finding the statute ambiguous, for a final vote of 6-3."Oftentimes the meaning--or ambiguity--of certain words or phrases may only become evident when placed in context."--Brown and Williamson, 529 U.S. at 132.
"Reliance on context and structure in statutory interpretation is a 'subtle business, calling for great wariness lest what professes to be mere rendering becomes creation and attempted interpretation of legislation becomes legislation itself.'-- Palmer v. Massachusetts U.S. 79,83 (1939)
Judging from the global circumstances, it is probably fair to conclude that ambiguity was probably not the only issue involved, and it was probably inartful for the Court to establish a precedent that such a restructured role for the Court was either necessary or desirable. The history of Canada's use of this device to coerce provinces into joining the national health system was well known in Canada at the time. And the McCarran Ferguson Act has restricted insurance administration to a State level for seventy years. Both of these examples would seem to have provided a sounder basis for the Court to interfere in what really seems like pretty clear language in the law.
Hamlet Speaks His Mind
Hamlet may have been speaking of his mother, or his significant other, Ophelia. And Justice Anton Scalia in his dissent may have been speaking of Health Secretaries Burwell and Sibelius, or the six Justices who took the other side of the Burwell case. But anyone who knows his Shakespeare recognizes the outrage in his voice when he repeatedly intoned "Frailty, thy name is..." several times, changing only the name of the person into the fault he is deploring. He goes on for 21 printed pages, but his summary suffices:
Today's opinion changes the usual rules of statutory interpretation for the sake of the Affordable Care Act. That, alas, is not a novelty. In National Federation of Independent Business v. Sibelius, 567 U.S., this Court revised major components of the statute in order to save them from unconstitutionality. The Act that Congress passed provides that every individual "shall" maintain insurance or pay a "penalty." 26 U.S.C. pp5000A. This Court, however, saw that the Commerce Clause does not authorize a federal mandate to buy health insurance. So it rewrote the mandate-cum-penalty as a tax. 567 U.S. at__(principal opinion) (slip op., at 15-45) The Act that Congress passed also requires every State to accept an expansion of its Medicaid program, or else risk losing all Medicaid funding. 42 U.S.C. (principal opinion) (slip op., at 45-58). Having transformed two major parts of the law, the Court today has turned its attention to a third. The Act that Congress passed makes tax credits available only on an "Exchange established by the State." This Court, however, concludes that this limitation would prevent the rest of the Act from working as well as hoped. So it rewrites the law to make tax credits available everywhere. We should start calling this law SCOTUS-Care.Perhaps the Patient Protection and Affordable Care Act will attain the enduring status of the Social Security Act or the Taft-Hartley Act; perhaps not. But this Court's two decisions on the Act will surely be remembered through the years. The somersaults of statutory interpretation they have performed ("penalty" means tax, "further [Medicaid] payments to the State" means only incremental Medicaid payments to the State, "established by the State" means not established by the State) will be cited by litigants endlessly, to the confusion of honest jurisprudence. And the cases will publish forever the discouraging truth that the Supreme Court of the United States favors some laws over others and is prepared to do whatever it takes to uphold and assist its favorites.
I dissent.
Deeper Detail: Extending the Investor's Return, Simplifying His Role
-------------------------------------------------------------------------------------------Start by looking at what happens if you increase the interest rate from 5% to 12%, or if you lengthen life expectancy from age 65 to age 93. Stretch the limits to see what stress will do. For example, increasing the interest rate to the edge of believable gets your balance to a couple of million dollars amazingly quickly, while lengthening the time period (for that interest rate to work) even further enhances that gain. The combination of the two easily escalates the investment above twenty million. Because we are only trying to get to $350,000, reaching it suddenly seems believable.
The combination of extra time plus extra interest rate holds out a theoretical promise of paying for a lengthening lifetime of medical care, in spite of medical cost inflation. Present realities don't quite stretch that far, but finding some way to reach that level is not hard to imagine. In fact, it gets the calculation to giddy amounts so quickly it engenders suspicion, to which one answer is, we probably don't need anything like twenty million. The actuaries at Michigan Blue Cross, verified by the Medicare agency, estimate average lifetime health costs to be around $350,000 per lifetime. That's just a guess, of course, but increasing interest rates and life expectancy just a little could reach that minimum requirement. How do we go about it, and how far dare we go?
Some very credible theories sometimes disappoint us. Remember, our whole currency is based on the notion of the Federal Reserve "targeting" inflation at 2%, but in spite of spending trillions of dollars, they sometimes seem unable to achieve that target. We had better not count on schemes which require the Federal Reserve to target interest rates, because sometimes, they can't. On the other hand, if a vast army of smart people set about to nibble at various small increases in interest rates and longevity, perhaps they can make serious progress.
One person who does have practical control of the interest rate an investor receives is his own broker. For a full century, Rogen Ibbotson has published the returns on various investments, and they don't vary a great deal. Common stock produces a return of between 10% and 12.7% in spite of wars and depressions; if you stand back a few feet, the graph is pretty close to a straight line. If you search carefully, a number of brokerages offer Health Savings Accounts which produce no interest at all -- to the investor -- for the first ten years. Try earning 2% during inflation of 2%, and see what it gets you. In ten years, that approaches a haircut of nearly 100%, explained by the small size of the accounts, and by the fact that experienced customers who know better, just look for other vendors. Since the number of Health Savings Accounts has quickly grown to be more than ten million, it's time for some consumer protection. The prospective future size of these accounts should command much greater market power, quite soon. After all, passive investment should mainly involve the purchase of blocks of index funds, with annual fees of less than a tenth of a percent. Most of this haircutting is explained by the uncertainties of introducing the Affordable Care Act during a recession, and taking six years to get to the point of a Supreme Court Test to see if its regulations are legal and workable.
That's the Theory. If Necessary, Settle for Less. The rest of this section is devoted to rearranging healthcare payments in ways which could -- regardless of rough predictions -- outdistance guesses about future health costs. When the mind-boggling effects are verified, skeptics are invited to cut them in half, or three quarters, and yet achieve roughly the same result. The purpose is not to construct a formula, but to demonstrate the power of an idea. Like all such proposals, this one has the power to turn us into children, playing with matches. By the way, borrowing money to pay bills will conversely only make the burden worse, as we experience with the current "Pay as you go" method. By reversing the borrowing approach we double the improvement from investment, in the sense we stop doing it one way and also start doing the other. In the days when health insurance started, there was no other way possible. The reversal of this system has only recently become plausible, because life expectancy has recently increased so much, and passive investing has put the innovation within most people's reach. The environment has indeed changed, but don't take matters further than the new situation warrants.
Average life expectancy is now 83 years, was 47 in the year 1900; it would not be surprising if life expectancy reached 93 in another 93 years. The main uncertainty lies in our individual future attainment of average life expectancy, which we will never know, but probably could guess with a 10% error. When the future is thus so uncertain, we can display several examples at different levels, in order to keep reminding the reader that precision is neither possible nor necessary, in order to reach many safe conclusions about the average future. Except for one unusual thing: this particular trick is likely to get even better in the future because people will live longer. Even so, it is better to do a conservative thing with a radical idea.
Reduced to essentials for this purpose, today's average newborn is going to have 9.3 opportunities to double his money at seven percent return and would have 13.3 doublings at ten percent. Notice the double-bump: as the interest rate increases, it doubles more often, as well as enjoying a higher rate. If you care, that's essentially why compound interest grows so unexpectedly fast. This double widening will account for some very surprising results, and it largely creeps up on us, unawares. Because we don't know the precise longevity ahead, and we don't know the interest rate achievable, there is a widening variance between any two estimates. So wide, in fact, it is pointless to achieve precision. Whatever it is, it's going to be a lot.
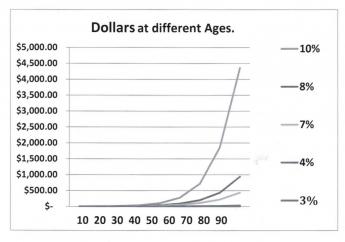
|
| One Dollar: Lifetime Compound Interest, at Different Rates |
Start with a newborn, and give him one dollar. At age 93, he should have between $200 (@7%) and $10,000 (@10%), entirely dependent on the interest rate. That's a big swing. What it suggests is we should work very hard to raise that interest rate, even just a little bit, no matter how we intend to use the money when we are 93, to pay off accumulated lifetime healthcare debts. Don't let anyone tell you it doesn't matter whether interest rates are 7% or 12.7%, because it matters a lot. And by the way, don't kid yourself that a credit card charge doesn't matter if it is 12% or 6%. Call it greed if that pleases you; these small differences are profoundly important.
------------------------------------------------------------------ If that lesson has been absorbed, here's another:
In the last fifty or so years, American life expectancy has increased by thirty years. That's enough extra time for three extra doublings at seven percent, right? So, 2,4,8. Whatever amount of money the average person would have had when he died in 1900, is now expected to be eight times as much when he now dies thirty years later in life. And even if he loses half of it in some stock market crash, he will still retain four times as much as he formerly would have had, at the earlier death date. The reason increased longevity might rescue us from our own improvidence is the doubling rate starts soaring upward at about the time it gets extended by improved longevity. In particular, look at the family of curves. Its yield turns sharply upward for interest rates between 5% and 10%, and every extra tenth of a percent boosts it appreciably.
Now, hear this. In the past century, inflation has averaged 3%, and small-capitalization common stock averaged 12.7%, give or take 3%, or one standard deviation (One standard deviation includes 2/3 of all the variation in a year.) Some people advocate continuing with 3% inflation, many do not. The bottom line: many things have changed, in health, in longevity, and in stock market transaction costs. Those things may have seemed to change very little, but with the simple multipliers we have pointed out, conclusions become appreciably magnified. Meanwhile, the Federal Reserve Chairman says she is targeting an annual inflation rate of 2% of the money in circulation; the actual increase in the past century was 3%. If you do nothing at 3%, your money will be all gone in thirty-three years. If you stay in cash at 2%, it will take fifty years to be all gone.
But if you work at things just a little, you can take advantage of the progressive widening of two curves: three percent for inflation stays pretty flat, but seven percent for investment income starts to soar. Up to 7%, there is a reasonable choice between stocks and bonds; but if you need more than 7% you must invest in stocks. Future inflation and future stock returns may remain at 3 and 7, forever, or they may get tinkered with. But the 3% and 7% curves are getting further apart with every year of increasing longevity. Some people will get lucky or take inordinate risks, and for them, the 10% investment curve might widen from a 3% inflation curve, a whole lot faster. But every single tenth of a percent net improvement will cast a long shadow.
But never, ever forget the reverse: a 7% investment rate will grow vastly faster than 4% will, but if people allow this windfall to be taxed or swindled, the proposal you are reading will fall far short of its promise. Our economy operates between a relatively flat 3% and a sharply rising 4-5%. In other words, it wouldn't have to rise much above 3% inflation rate to be starting to spiral out of control. Our Federal Reserve is well aware of this, but the public isn't. A sudden international economic tidal wave could easily push inflation out of control, in our country just as much as Greece or Portugal. As developing nations grow more prosperous, our Federal Reserve controls a progressively smaller proportion of international currency. Therefore, we could do less to stem a crisis that we have done in the past.
To summarize, on the revenue side of the ledger, we note the arithmetic that a single deposit of about $55 in a Health Savings Account in 1923 might have grown to about $350,000 by today, in the year 2015, because the stock market did achieve more than 10% return. There is considerable attractiveness to the alternative of extending HSA limits down to the age of birth, and up to the date of death. It's really up to Congress to do it. If the past century's market had grown at merely 6.5% instead of 10%, the $55 would now only be $18,000, so we would already be past the tipping point on rates. In plain language, by using a 10% example, $55 could have reached the sum now presently thought by statisticians -- to be the total health expenditure for a lifetime. But by accepting a 6.5% return, however, the same investment would have fallen short of enough money for the purpose. Like the municipalities that gambled on their pension fund returns, that sort of trap must be avoided. Things are not entirely hopeless, because 6.5% would remain adequate if our hypothetical newborn had started with $100, still within a conceivable range for subsidies. But the point to be made provides only a razor-thin margin between buying a Rolls Royce, and buying a motorbike. If you get it right on interest rates and longevity, the cost of the purchase is relatively insignificant. That's the central point of the first two graphs. For some people, it would inevitably lead to investing nothing at all, for personal reasons. Some of the poor will have to be subsidized, some of the timid will have to be prodded. This is more of a research problem than you would guess: a round-about approach is to eliminate the diseases which cost so much, choosing between research to do it, or rationing to do it. Right now we have a choice; if we delay, the only remaining choice would be rationing.
Commentary.This discussion is, again, mainly to show the reader the enormous power and complexity of compound interest, which most people under-appreciate, as well as the additional power added by extending life expectancy by thirty years this century, and the surprising boost of passive investment income toward 10% by financial transaction technology. Many conclusions can be drawn, including possibly the conclusion that this proposal leaves too narrow a margin of safety to pay for everything. The conclusion I prefer to reach is that this structure is almost good enough, but requires some additional innovation to be safe enough. That line of reasoning will be pursued in Chapter Fxxx.Revenue growing at 10% will relentlessly grow faster than expenses at 3%. As experience has shown, it is next to impossible to switch health care to the public sector and still expect investment returns at private sector levels. Repayment of overseas debt does not affect actual domestic health expenditures, but it indirectly affects the value of the dollar, greatly. Without all its recognized weaknesses, a fairly safe description of present data would be that enormous savings in the healthcare system are possible, but only to the degree, we contain next century's medical cost inflation closer to 2% than to 10%. The simplest way to retain revenue at 10% growth is by anchoring the price leaders within the private sector. The hardest way to do it would be to try to achieve private sector profits, inside the public sector. This chapter describes a middle way. Better than alternatives, perhaps, but nothing miraculous. For the full whammy, you will have to read chapters Three and Four.
Cost, One of Two Basic Numbers. Blue Cross of Michigan and two federal agencies put their own data through a formula which created a hypothetical average subscriber's cost for a lifetime at today's prices. The agencies produced a lifetime cost estimate of around $300,000. That's not what we actually spent because so much of medical care has changed, but at such a steady rate that it justifies the assumption, it will continue into the next century. So, although the calculation comes closer to approximating the next century, than what was seen in the last century, it really provides no miraculous method to anticipate future changes in diseases or longevity, either. Inflation and investment returns are assumed to be level, and longevity is assumed to level off. So be warned. This proposal, particularly with merely an annual horizon, proposes a method to pay for a lot of otherwise unfunded medical care. The proposal to pay for all of it began to arise when its full revenue potential began to emerge, rather than the other way around. If the more ambitious second proposed project ever works in full, it must expect decades of transition. Perhaps that's just as well, considering the recent examples we have had of being in too big a hurry. Rather surprisingly, the remaining problem appears mainly a matter of 10-15% of revenue, but all such projection is fraught with uncertainty.
Revenue, The Other Problem. The foregoing describes where we got our number for future lifetime medical costs; someone else did it. Our other number is $132,000, which is our figure for average lifetime revenue devoted to healthcare. That's the current limit ($3300 per year of working life) which the Congress itself applied to deposits in Health Savings Accounts. No doubt, the number was envisioned as the absolute limit of what the average person could afford, and as such seems entirely plausible. You'd have to be rich to afford more than that, and if you weren't rich, you would struggle to afford so much. To summarize the process, the number was selected as the limit of what we can afford. If it turns out we can't afford it, this proposal must somehow be supplemented. The provision made for that predicament is we will then have to jettison one or two major expenses, the repayment of our foreign debts for past deficits in healthcare entitlements, or the privatization of Medicare. That would leave us considerably short of paying for lifetime health costs, but it might actually be more politically palatable. It's far better than sacrificing medical care quality, at least, which to me is an unthinkable alternative, just when we were coming within sight of eliminating the diseases which require so much of it.
Lifetime Healthcare, Using Health Savings Accounts (1)
Can it be done? What would it cost? Since no one can predict future healthcare costs, no one knows how to pay for them. Conclusions like that over-state the difficulty. It's fairly easy to predict minimum available revenue, and fairly good cost extrapolations already exist. Payment feasibility can amount to comparing "no more than" with "no less than". With luck, we can judge the relative probability of success among payment proposals. Since that still sounds like a scam, what follows is step-by-step. We apologize to actuaries and mathematicians, who may find simplified explanations tiresome.
Medical Costs. We use someone else's estimate of present costs and the foreseeable rate of growth. Blue Cross of Michigan, confirmed by federal agencies, estimates the average lifetime cost in America today roughly approximates $350,000 for a male, and about 10% more for females, using the year 2000 dollars. An 83-year overall lifespan necessarily includes history and prediction. The gender difference rests mainly on women's somewhat longer life expectancy, as well as the statistical convention of attributing all obstetrical costs to the mother; it's likely to be a stable ratio. A million dollars for a family of three is pretty daunting. Because there have been so many changes in medical care in the past century, likely to be repeated in the next century as well, $350,000 must be considered a soft number. Most extrapolation errors will arise from it, so an analysis reduces to this question: How close could we come to cover a $350,000 cost, without distorting medical care? To simplify the explanation, the cost goal is reckoned in the year 2000 dollars, so inflation and other adjustments are taken from revenue, to make them match. Inflation has remained steady at 3% in the past century, so 3% per year is accepted for the future in this analysis. Medical inflation is somewhat different; greater than 3% in the past, recently diminished. Only revenue projections are discussed, with costs taken as a given. It isn't perfect, but it can serve as a base for mid-course corrections, providing a margin for error is adequate.
Revenue, per average person. It is easier to estimate future bulk numbers for the whole nation than to predict an individual's future cost. Therefore, our approach is to take national costs, divide them by the population, and concentrate final analysis into a hypothetical "average" person. Since the goal is to compare average costs with average revenue, it is important to avoid using revenue as a basis for costs. The temptation is great, however, because of the well-known tendency of costs to rise to the level of available funding. To the extent possible, such behavioral adjustments are reserved for "dynamic scoring."
Other Data Points. Longevity has risen by 30 years in the past century but is now relatively stable at age 83. Where practical, we have extended calculations to 93, which seems a reasonable guess for where longevity might go in the coming century. How much an average person could or would be likely to accept as a personal expenditure is hard to say, just as it is hard to say how much cost the country would be willing to pay for subsidies to the poor. There is a temptation to use present costs as a surrogate because there is so much uproar about them, but that approach has too much circularity to its logic. After all, the public is complaining. So, whenever practical, we have presented a family of curves which permit the reader to choose between alternatives. The final data point is the maximum achievable interest rate, a matter of enough complexity to require special discussion, which follows after voicing an opinion about the medical future underlying this subject.
The medical side of it. There is fair reason to believe most or all late-developing diseases might originate in the dozen or so complete genes in the mitochondria of cells. These genes are only inherited through the mother and probably originated in the plant kingdom. So the conquest of our currently most expensive diseases -- diabetes, cancer, Alzheimer's disease, Parkinson's disease, and arteriosclerosis -- during the next century -- is not a totally unreasonable prediction. Furthermore, new cure discoveries, while generally expensive at first, eventually become cheap. Mix it all together, and while the costs of the next century may at times be towering, it seems entirely conceivable healthcare payments could become self-sustaining without financial intervention, a century from now. If we generate the means to get to that point, curiously we should give some credit to financiers, like Warren Buffett and John Bogle. If that sounds confusing, read on.
What passive investment income for a Health Savings Account is generally achievable? Essentially, this proposal advocates saving in advance instead of paying after the fact (often called "Pay as you go.") That translates into being paid interest instead of being charged interest. For this, we steer the reader toward investing his savings as much as possible in an HSA (Health Savings Account), rather than an IRA (Individual Retirement Account), or a 401(k) plan, the employer-based equivalent to IRA. There's nothing the matter with these other tax shelters; they are just not as good as an HSA. The only qualified American savings plan to contain a tax shelter on both deposits and withdrawals is the HSA, and even its tax shelter on withdrawals is limited to approved medical expenditures. The Canadian savings plans do have this dual advantage, but in every other qualified American plan, it is necessary to reduce either the deposit or the withdrawal by its estimated taxes at different ages. All graphical representations of IRAs and 401(k)s likewise require a mental adjustment for taxes. In amounts, this large, taxes make a vital difference. After-tax savings vehicles are necessarily less generous, and are not discussed.
So far, so good. Probably the greatest reluctance this proposal will encounter will come from an almost absolute need to invest the HSA in common stocks, which many people sincerely feel is a form of gambling. But to reflect on history for a moment, it took over a century for Americans to overcome their resistance to banks, which are now found on practically every street corner. Pioneer families were obedient to Shakespeare's, "neither a lender nor a borrower is," which indeed remains pretty good advice in most circumstances. But banks were also the foundation of the Industrial Revolution, and their process could also be called a form of gambling. Modern index funds are a far cry from 19th Century mining and railroad stocks. Their risks, while not totally eliminated have been tamed, so the modern economy really has no savings vehicle quite as safe for those who must live in the real world. At this particular moment in time, almost no stock is as risky as bonds, and in Europe cash in the mattress can lose 50% of its value in a month, responding to central-bank changes in currency rates. True, approximately every thirty years stocks fall almost as much, but modern investment has ways of coping with the "black swan" risk, by somewhat sacrificing some of the investment return. Every company eventually comes to an end in about a century, and the only real safety comes from wide diversification of risks substituting for agility in jumping among them. The current total-market index fund model allows for investment in the whole economy at once, counting on remorseless market pressure to purge the index of failing companies, while constantly adding new ones who are succeeding. Holding several thousand successful stocks at once is the new definition of safety. Meanwhile, the new definition of success is moderate but relentless growth, from low costs and low taxes.
John C. Bogle of Philadelphia probably did not invent the notion you can't beat the index (he means the stock market averages like Dow Jones, Standard, and Poor, Russell, etc.), but he certainly evangelized the idea. Let's explain. When you finally overcome the idea of getting rich by out-performing the stock market, the idea reverses itself. The entire stock market is a proxy for the whole economy, and although some people do get rich faster than the stock market grows, hardly anybody gets appreciably richer than the index in the stock market without using leverage , and leverage is only for gamblers who can disguise the nature of their leverage.
Professor Roger Ibbotson of Yale has compiled extensive data for the previous century and demonstrates how relentlessly the American equity stock market has grown quite linearly, varying by asset class but largely disregarding stock market crashes, or numerous wars large and small. While small stocks have grown at a rate of 12.7% per year over the past century, safer Blue chip stocks have consistently grown at about 11%. With big computers, we can see investors in stocks have only received a return of 8%, which sometimes implies the financial industry is absorbing 3% for its expenses and profits. That may not be a fair comment since a considerable portion of the 11% must be invested in lower-yielding bonds to protect against periodic black swan disasters like 1929 and 2008; this point is expanded later. Vanguard, Bogle's fund, reduces overhead cost by matching his portfolio to the index and letting it run indefinitely, a process known as passive investing, which at least minimizes taxes and expenses. Perhaps, over time, ways can be found to widen the investor's lifetime return to more than 8%, but for the time being one must be satisfied with 8%, and 11% remains the ultimate goal for the far future. Warren Buffett does better than that by buying whole insurance companies and leveraging with their cash float; that's not exactly possible for other people. To rephrase the whole business, a total-market index fund offers the 8% current safe limit to passive investing, within a bumpy unsafe 11% world. Furthermore, the 8% contains steady 3% inflation, so investors better not count on more than 5% spendable return. A disappointingly low five percent, relatively safe, after-tax and after-inflation, return. What will that achieve toward paying an average lifetime cost of $350,000? Remember, this is compounded , which has a magic of its own.
Table xxx plots how $400 will grow in response to compounding, starting at birth and ending at 83 to 93 years, at 5% to 12% compound investment return. We've already described why 83, 93, and 5% were chosen, but why $400? It's a personal guess, shown at the bottom of a family of curves which go up to 12%, the current maximum. It represents the amount I guess would be privately regarded as within almost everyone's reach, and if lost wouldn't financially cripple them forever. It would admittedly have to come as a government subsidy for handicapped people who could never support themselves. And since it would be at birth, it would have to seem bearable to young parents. Also included in this family of curves, are 12% (the limit of growth in the stock market over the past century) and other 1% levels down to 5%, so the effect of taxes, overhead, inflation, and bond protection against stock crashes, can be judged. Note in particular how the curves widen around age 60, exposing the new opportunity created by the 30-year increase in longevity during the past century. The consequence of every improvement in the investment return is multiplied appreciably after you reach that bend in the curve. In my personal opinion, this growth is both staggeringly large, but disappointingly inadequate to pay for all future health care with enough margin to justify committing the whole country to risk it. It will pay for a big chunk of it, however.
Another central point of the graph, however, is that a lifetime of investing a relatively small amount -- at reasonably achievable interest rate -- has apparently come within our grasp. In my view, however, we have to do better than this. We have to tweak this basic idea enough to generate more than $400 at birth. Although prosperous people could use it to make a large reduction in their lifetime medical costs, there is not enough room for error, to permit the nation to risk so much for millions of people with only a marginal income. In the following sections, we apply a variety of other variations to convert an attractive idea into a widely useful one.
************* Compound interest always surprises people with its power, and in this example, 5% just about makes the goal. There's not much room for error or contingencies. All of the known factors are conservatively estimated, and it passes the test. What isn't covered is the unknown factor, the atom wars, a stock market collapse, an invasion from Argentina. To be on the safe side, we had better not count on this approach to pay for all of the health care. Just a big chunk, like 25%, does seem feasible. In the immediately following section, we examine the first "technical" problem. The first year of life is just as expensive as the last year of life, and you can't dip into savings.
Basic Coverage: Three Big Problems, No Little Ones

|
| Columbus and the Egg |
Let's summarize. We started with the classical Health Saving Account (C-HSA), which may need a little updating, but appeals to millions of frugal people as a simple way to avoid the tangles of present-day healthcare financing. The law hasn't changed much, but used by millions of subscribers has turned up many surprising features, all good ones. Deliberately overfunding them has unexpectedly useful results, for example, in providing retirement income if you have been lucky with your health.
On that foundation then was devised New Health Savings Accounts (N-HSA), combining six more innovations, each of which is easy to explain, but in combination utterly transform the basic design. The extended longevity of the 21st Century makes compound interest in passive investing into a powerful investment tool and is used to reduce healthcare costs to the consumer, markedly. Secondly, improved healthcare for the working years has unbalanced the employer-based model, so sickness costs are getting crowded into retirement years. For this, the accounts permit extraction of the first year and last years of life, transferring their heavy costs to the working generation where employment-basing still makes sense. And so on. With very little new legislation, most of this package is ready to go.
Lifetime Health Savings Accounts (L-HSA), patterned on a whole-life model. L-HSA won't work without some new legislation to edge around recent regulations and some outmoded premises. Multi-year coverage is cheaper but requires a longer commitment, so it needs to be precisely designed. Starting fresh, it directly addresses a host of problems hiding behind a century of habit. Its flexibility accepts a range of designs, stretching from self-insurance out of a bank's safe deposit box, stretching all the way to letting life insurance companies run everything.
We conclude insurance of every sort "shares the risk" for expensive problems but generates extra expense when little problems get insured that don't need to be. Little medical problems swamp the fixed overhead of insurance unnecessarily. When you only insure essentials -- as true catastrophic insurance does -- it costs far less than insuring everything. So, here's an outline of a major variation, adding features, one by one. It's a Health Savings Account, on steroids.
Proposal 25A: Let's combine the high cost of the first year of life with the really high-cost last year of life, as a basic foundation of minimum health insurance.The dual combination could surely include everyone. What I am technically trying to achieve, I admit it, is to combine one life situation, which sometimes generates a surplus it can't use, with another situation, where every baby creates a difficult debt for someone else to pay. And whereas 100% of the population experiences birth and life at the two ends of life, there is ancient uneasiness about sharing liabilities outside of families, and even, how far the boundaries of families will stretch. Ancient fear of violating obsolete family boundaries sometimes hinders useful proposals. Because of increased longevity, grandparents are now real people, not just a picture on the wall. And by no means are they all senile.
A sly feature of all this is, people still alive are willing enough to overfund the costs of the terminal care lying ahead of them, but few still alive have their own birth costs on their minds, even if they were never paid. That lopsided initial generation might generate sizeable reserves for a circular program, if we imaginatively link accounting between generations, carrying those birth costs forward. Another unrecognized feature is the costs of these first and last years of every life are in fact both paid in retrospect, and often not by the patient.
Furthermore, most of the heavy expenses of both ends of life are created within a hospital, which often delays final billing until the issue of responsibility is settled, creating blind spots in which final responsibility is unclear. Nevertheless, the hospital aggregates many services in a total hospital bill, so bulk payments by diagnosis or even by age, are tempting but as yet crudely perfected. When all these matters finally get standardized, reimbursement from one insurance entity to another should become commonplace. The final transaction in both end-of-life insurance as well as the beginning of- life insurance easily and more naturally evolves into who reimburses some other entity who (temporarily) paid the bills.That's about all, there is to say about the funds' flow, which should become very simple, but come in larger lumps. At such esoteric levels, no one cares whose money it is, so long as it gets paid. At the local patient level, family transfer issues can be troublesome. It can be recalled we have gone into detail about grandparent/grandchild transfers in the section on New Health Savings Accounts, and indeed it emerges as the main innovation of that effort. Still earlier, we described the compound interest hidden in the background, paying for a great deal of it. As an aside, most people will eventually find it is desirable to use overfunded accounts as a basis for tax-sheltered retirement costs, and will therefore often die with a small surplus, which is the basis for closing the loop between generations. That may take time to evolve.
Proposal 25B: And then, add catastrophic coverage regardless of age, less the cost of overlaps. Title: Tri-Challenge Basic Coverage.Here's the universal catastrophic coverage we promised in the first chapter, minus the first and last years of life overlaps.
Overlaps. One passing word about overlaps. Reducing overlaps is one of the main mechanisms for reducing costs, but the insurance entities will fight fiercely over who gets the reductions. For example, what about a six months old child who dies with an expensive hospital bill? My suggestion is that the beginning of life insurance pays first, the end of life insurer pays second, and then the catastrophic insurer pays for the balance. This gives the savings to the catastrophic carrier, but most of the cost is given to grandpa, who is dead, and anyway, most of it is investment income, leading to fewer complaints.
We thus design the basic coverage to include two universally-unavoidable costs, plus the universally-inescapable risk of unpayable health costs at all ages in-between. It is clearly superior to less universal, and more unaffordable, coverages.
Proposal 25C: Require the unused birth coverage to be transferred, either at the time of death or optionally at other times, to either a designated grandchild by inheritance or to a designated pool of unassigned third-generation recipients. The grandchild's Health Savings Account would begin at birth, capturing 21 extra years of compound interest, compared with employer-based insurance.The purpose of beginning an HSA at birth is to add 21 years to the compounding while staying within the laws of perpetuities.
A 1:1 ratio of national grandparents to national grandchildren do exist, but so do multi-children families, no-children families, unmarried families, divorces, etc. There is definitely a need for a pool within which, mis-matched funds are administered.
The childhood transfer feature adds about $28,000 to the coverage, but it would only require $42 a year (added to the last year of life premiums, at 6.5% interest compounded from one year of age). Because catch-up transition at age 40 would require $200 annual contribution to catch up with newborns, rising to $28,000 for someone aged 65, it might be better to add $25, or so, at birth to reduce the even greater cost of late joiners (over age 40) to the plan. They must be enticed, however, because they are the ones closest to activating the transfers, and hence are the most important support to enlist to an innovation.
Proposal 25D: This is voluntary Tri-Challenge Basic Coverage. Whether to make it mandatory, whether to subsidize it for the poor, and whether to replace Obamacare with it -- are political decisions, not questions of insurance design.This coverage probably approaches half of the entire health costs of the nation, depending on how you treat the cost of prison inmates, the unemployable and illegal immigrants. If science should ever succeed in eliminating every major disease and therefore every other cost of healthcare, 18% of present costs would very likely persist. And in fact, the cost of prisoners, mentally retarded and illegals show no signs of changing much, either.
They are costs most likely to be permanent, but what we spend on the rest will depend on where we place the limits on "Catastrophic" care insurance. That cost depends on the size of the deductible, and the upper limit of coverage. You can readily predict the debate: the higher the deductible, the lower the premium, so the out of pocket cost depends on the deductible, too. But while controversy would remain, the great beauty of this design is the lessened political resistance from every voter who would likely benefit, which is 100%.
There is no escaping these realities, and in the meantime, the rest of health costs will dwindle down to the cost of birth and death, which change their nature very slowly. Therefore, although it is not traditional in the health insurance field, I propose it has long seemed an entirely natural thing, for the costs of childbirth to be an obligation of some other generation, usually but not always of the same family.
The problem is indeed complicated by the unusual concentration of malpractice claims in obstetrics, as well as the marginal finances of parents at this stage of their careers. But the hidden effect is to create more, or less, valuable babies, depending on how you judge the impact of emotions versus supply and demand. It was almost an unknown issue a century ago.
Any resistance to this proposal is thus likely to be more instinctive than rational since we have had so many generations of channeling such issues within the family unit. The relatively trivial cost of funding children's health care through 104 years of compound interest does generate a temptation to overfund the program, which if necessary can be frustrated by requiring one or more zero balances per lifetime. That is particularly true in this particular instance when compound interest could generate almost any amount of leveraged money at the death of a grandparent, simply by increasing the modest amount impounded at the grandparent's birth, and waiting long enough for it to grow. People in charge of managing the currency are then drawn into the discussion. Indeed, the relatively confiscatory level of estate taxes (60-70%) is a sign our society is not comfortable with perpetuities, although available remedies are fairly simple. Indeed some states also levy inheritance taxes on the recipients as well as the donor's estate taxes.
Whatever the traditional resistance, it's permanently true that the costs of the first year of life will always greatly exceed what a newborn is able to pay. And therefore it surely follows that this obstacle has hindered health financing for a very long time. There must be some mechanism for inter-generational transfer of funds, or life cannot continue. At present, it's called a family, and families are under strain. Conditions of modern life have evolved to the point where interference with some generational transfers will cause more suffering than the relaxation of such attitudes. There will be resistance, but it must be persuaded to reconsider its position and bilateral compromise must result.
Warning: Start Saving While You are Young. Health Costs for the first year of life are reportedly 3% of the total, and while the last year of life (15%) is worse, those costs laid on young families are particularly disruptive because of still higher costs later if neglected. At best they compete with college, housing, and automobile costs, and probably reduce the birth rate of the middle class. The enclosed graph shows a family of curves based on subsequent investment income from different invested external-contribution levels at birth, to help readers judge how much surplus might likely be generated at the end of a lifetime of average costs. Our goal is to estimate the cost of overfunding grandpa's health costs at birth, so there would remain an incentive for him to spend wisely, but still generate enough surplus to fund a grandchild's juvenile health costs. That is, to estimate the cost of transferring the obligation of grandchild costs from parents to grandparents. But it must ultimately be recognized that the full consequences of such a basic change, are unpredictable.
First, however, we must determine the size of grandchildren's costs. 3% of all costs ($10,500) for the first year of the child's life sounds plausible. But 5% of costs from the first birthday cake to the 21st birthday ($17,200) sounds surprisingly high and needs to be challenged if only to defend it properly from rapidly escalating educational costs. That's one of the great advantages of starting with a demonstration project; you can see where the bills are coming from. But that's mostly a quibble, because even $17,000 is manageable, and the legal boundary of age 21 is strongly defended.
Let's take just a moment to examine the laws of perpetuities, which mostly focus on intergenerational inheritance. Established about three hundred years ago as common law, they permit transfers for 21 years after the birth of the last person to be alive at the time of the bequest. I'm not a lawyer, but those do not seem like a handicap for what is proposed.
The pool would also pay for multiple children in a family or those newborns who do not have a willing grandparent. I never met any of my four grandparents, so I don't know if they would have been willing or not. As the father of fourteen living children, one of my two grandfathers would surely have wanted some adjustments. If it becomes an issue, the government could easily afford to donate the $7 yearly required to avoid the issue. During the early transition phase, it might possibly be necessary to have government backup if temporary mismatches appear, eventually repaid by adjusting the initial cash deposits. It happens the birthrate is 2.1 per mother, which easily matches one-half per grandparent, greatly relieving but not eliminating the occasional mismatches. It would seem a fairly simple task to charge 1:1 (grandparent to child) for the first three or four years, and gradually re-adjust if more precise data becomes available. It could even be possible to pay for the child-generation completely, but this is not entirely desirable. It should not require dynamic scoring to understand that making healthcare free would increase its cost.
|
Not everything which is desirable to do is desirable to do in a big hurry.
|
If desired, the 1.6% salary withholding for Medicare can be reduced, relieving working people and their employers of about one-quarter of Medicare costs. The tax inequity between employees and self-employed should be eliminated anyway, but this somewhat reduces the disparity. The doughnut hole was a good idea, but it is part of copayments which are a bad idea. It should be self-evident that making hospital insurance free but doctor payment subject to Part B premium, creates unmanageable distortions. Many healthcare financing problems are like the fable of Columbus and the egg -- once explained, anybody can do it. Nevertheless, it would seem much better to proceed slowly according to a defined plan, using demonstration projects and experimental trials, mid-course adjustments, and careful monitoring. Because not everything which is desirable to do is desirable to do in a big hurry.
Finally, someone does need to calculate the cost of adding catastrophic stop-loss insurance to birth-and-death insurance. It isn't possible for an insurance outsider to calculate the overlaps between the two types of insurance, which are probably considerable. But, particularly if there is a lot of overlap making it relatively cheap, that combination would constitute the kind of basic insurance which covers what everyone needs, and very few would be able to fabricate. If you linked it to a more sensible diagnosis related code, as a basis for DRG for inpatients, and firm association with market-based outpatient costs, you might get a firm basic package. It then only requires a relative value index for items which do not overlap, and a firm rule that the same items be charged the same amount, for helpless inpatients and not-so-helpless outpatients.
What are vital but uncovered by this basic package are new scientific discoveries, so self-evidently essential they create temptations to exact extortionate prices. I'd say it would be shooting yourself in the foot to go hard on such discoveries for their first few years. Overall, that which is left uncovered by this hybrid tri-insurance may be hated for its commercial motives, but nevertheless remains something we clearly want to encourage. Managing costs of that sort ought to be left to the Food and Drug Administration, the Patent Office and competition. And silently endured by insurance.
Lifetime Healthcare, Using Health Savings Accounts (3)
Let's return for the moment to the difference between what a total market index earns (11%) and what just about every foundation and endowment earns (8%). That 3% difference is so large it has a major effect on what an HSA can provide. If 3% represented what the financial industry imposed as a middle-man cost, it would be an outrage we should work to change. However, it likely has a more benign explanation with standard available protections. Remember, there are two cycles recognized in the stock market, one of which is the daily or weekly volatility which can be ignored by long-term investors. For a century it has had a standard deviation of about three percent, conventionally referred to as if "risk" can be represented as one standard deviation in amount.
However, that is not the risk most long-term investors fear. Roughly following a 30-year cycle, although don't count on that, it has recently been termed a "black swan" risk, of 30-50% volatility. Such disturbances usually last a couple of years and can be utterly disruptive to foundations and nonprofits who meet payroll to keep their doors open. The market has always recovered in a few months or years, but meanwhile, how can you function?
Available solutions vary but generally come down to a choice between a contingency reserve, and a "balanced" portfolio of stocks and bonds, usually in 60/40 ratio. Since bonds generally return about 5% instead of the blue-chip stock average of 10%, the nominal return on a balanced portfolio is reduced from 10% to 8%; the real return after inflation is further reduced from 8% to 5%. However, in the case of a lifetime HSA, the lifetime at risk of a black swan crash stretches from birth to age 66, much longer than 30 years. We suggest the after-inflation bond content of the portfolio should grow 2% a year from age 43 to 66 when the eventual bond content of the portfolio should roughly equal the required lump-sum payment to Medicare. Once the disbursement is made, the remaining portfolio can return to 100% stocks.
It could still fund a Medicare buy-out without disturbing the rest of the investment program if by bad luck the time for a buy-out coincides with a bear market. If there is no bear market, the cost of this safety measure can be shrugged off as just the price of safety, because it also permits the extra risk of 43 years of a 100% stock portfolio. The overall effect -- 43 years of 100% stocks ignoring the risk in the background of a black swan -- is to increase the portfolio's overall total return from 5% to 6%, as well as mostly guaranteeing the fund will be undisturbed by black swans at just the wrong time. This safety assumes no withdrawals from the fund except this one, so no amount of volatility needs to be considered except volatility at the one moment of liquefying a portion to buy out of Medicare. That's individual black swan risk; the black swan risk for the entire population is otherwise practically certain to afflict someone at some time within a 66-year interval. The tiny proportion of people wealthy enough to weather the storm with outside funds can elect not to do it at any time up to the 43rd birthday. However, they should probably be required to fund their own contingency arrangement, because for a poor person to neglect safety is a risk of unraveling the scheme they should not run. Remember for a moment the scheme promises to cost $xxxx for the avoidance of lifetime costs of $350,000, and thus is entitled to insist on reasonable protective rules if someone wants to share the benefits.
Lifetime Healthcare, Using Health Savings Accounts (4)
At the time this book is written, newspapers report 12 million people to have Health Savings Accounts. Unfortunately, newspapers also report the Affordable Care Act ("Obamacare") is awaiting the Supreme Court decision as to its Constitutionality. Like the rest of the healthcare world, we must wait to see how the decision affects the financing. At the hearing, Justice Alito hinted the effective date of the decision might be delayed longer than the decision itself. Therefore I decided to proceed with a discussion of really radical health insurance reform, necessarily treating working-age people as a later add-on. The whole matter of paying for healthcare amounts to shifting resources from people who are able to work, to paying for people who are too sick to work. Insurance is one way to accomplish it but is the ideal way for only some of it. For one thing, insurance has proved to be remarkably expensive. It involves a major shift of funds from those who can work, to those who can't, but administrative income from the transfers somehow gets dissipated. We can do better than that, by hundreds of millions of dollars.
Furthermore, the financial strain has overwhelmed the political obstacles. To speak of Medicare as a political "third rail" is no longer tolerable. It is the job of politicians to persuade the elderly that no one wants to ruin their entitlement, shorten their lives, or ration their care. Protection from all that would be strengthened, not weakened, by making the system sustainable. And the time is long past for believing the government will protect the funds better than having the money within one's own possession. At the other age extreme, the parents of children will do a better job of protecting the kids, than treating the whole age group as if it were in a child-care center. Mind you, there must exist a fail-safe or catastrophic, health insurance against legitimately huge medical expenses, plus a system of oversight for overcharging. But the first level of price resistance must rest with the patient's family, who have an avenue of appeal if they are bullied. We need an appeal mechanism, not a system of regulators. We need catastrophic insurance, not first-dollar coverage. With these two basics in place, the next level of a decision must be restored to the patient's family. While of course, frugal shopping is useful, the main decision a family must make is whether to spend their funds now or save them for a later rainy day. A public education program might well prove useful, reinforcing but not supplanting the advice of a family physician. By improving the investment choices of the administrators of Health Savings Accounts, the investment experience of the whole country would be enhanced by educating the public in personal investment. That would be an invisible advantage of an enlightened HSA investment service; the visible part would be to set realistic goals and then achieve them. Assuming legal or legislative clearance, the total lifetime cost would be one single payment at the birth of $2200 (invested @ 6% compounded), in addition to whatever it turns out Obamacare charges for coverage from age 22 to 66.
In return for that, Medicare could stop borrowing 50% of its costs from foreigners, and each individual would cover the cost of one child per subscriber, up to age 21. (Remember, the present birthrate is 2.1 children per mother.) That is, individuals with children would get coverage for one designated child from birth up to age 21, for $220, which would be a bargain price for what is now 8% of lifetime medical costs, or $25,000. The government would get a far larger benefit of 50% of Medicare costs for one person. That would be a far more attractive part of the bargain, paying for coverage worth $82,500, for $2000. Although this would be a bargain package for many subscribers, it would only be of tangible value to those who had children. Very likely, it would be a futile selling opportunity, whose only virtue from the presentation is to illustrate how we already start with solvency instead of subsidy. Subsidy -- and advantage to working people -- comes later, when compound interest makes the other, more customer-attractive, features vastly cheaper to provide. For that, we must await the Supreme Court's decision, followed by bipartisan debate and eventually, election results.
So, that's sort of a disappointment until we begin to envision what some regulatory changes could make, in addition. Remember, unless there is a change in the law, one-quarter of Medicare's cost is supplied by payroll deductions from working people, and one quarter from the premiums paid by Medicare subscribers. Therefore, this proposal would only pay for half of the cost of Medicare, the rest being the elimination of the present deficit spending. If a system of voluntary Medicare buy-outs could be established, these costs would disappear, and both working people, as well as present Medicare subscribers, would be appreciably better off financially. At first, only the adventurous first-adopters would take the bargain, but even that slow beginning would allow a new program to get started, picking up more timid subscribers gradually. The whole population would now be offered a voluntary bargain. The next legislative step with significance would be to provide for an overfunded Medicare buy-out, which with a lump sum payment gives the customer a Medicare buy-out plus the surplus, which goes to cover the first 21 years of medical cost for a designated grandchild. Where does this extra money come from?
Taxing the Working Generation We won't know the realities of financing Obamacare for quite some time to come, but we can estimate how painful the revenue effect would be for working people, in addition to their Obamacare costs. For an extra $5 a month, from age 22 to 66, a small tax on working people would generate (with 6% compound interest) an extra pool of $xxxxx by age 66. That would seem easily adequate to supplant the $2220 pump priming at birth we postulated at the beginning of this section. Since it is paying for subsidies to the poor as well as the well-off, it probably should be discounted by a third or even a half. So, if that seems insufficient margin, it could be raised in incremental amounts of $5 per month, depending on how much saving could be effected in Obamacare costs, which at present we do not know. Nevertheless, the numbers inspire reasonable confidence that this general approach is at least worth a demonstration project. At present, the main uncertainty revolves around the consistent ability to generate a 6% return through index funds, including adequate provision for the "black swan" sort of recession every few decades.Since John McClaughry and I were the two originators of Health Savings Accounts in 1981, we obviously are pleased with the notion that so many fellow citizens see our idea as the main alternative to comprehensive government involvement. The previous few chapters outline how I think the HSA can be stretched to finance and reduce the cost of all medical care, how its segmentation would assist a stepwise transition to it, and how it would essentially leave the scientific details to scientists while leaving more decision-making to the patient. Having once been in charge of the Professional Standards Review Organization in my area, I am completely satisfied that professional self-governance can quickly control abuses if there must be an iron fist hidden somewhere inside this velvet glove. Doctors are generally no more interested in administration than Senators are, or that executives of unrelated businesses once were; but doctors are disciplined and bright, which is the main qualification. I share Senator Wallace Bennett's view that a small but adequate minority can be found to do the work, although overstaffing will seldom prove a problem.Technicalities of Transition Once transfers from the "grandparent" HSA to the "grandchild" one are working smoothly, the working-generation contribution can be eased by up to 8% (the cost of children). Furthermore, if the option of buying-out Medicare is made legal and feasible, it should no longer be necessary to deduct Medicare withholdings from paychecks; prior payments might be open to a negotiated rebate. That should eventually reduce the price of lifetime coverage but unfortunately might make any remaining gaps less appealing for poor people until the entire life cycle gets into operation. Looking ahead, considerable premium costs would be less necessary and are therefore up for consideration in the new scheme.
Repealing Obamacare's present prohibition of Catastrophic Health Insurance after age 30 is certain to be very popular, and should be an early priority, leaving extra room for compromise after the removal of childhood costs. All Obamacare policies are high-deductible, but their premiums have been raised to cover the uninsured. Once this funding concept has proven itself, that should be less necessary. Since the HSA covers everyone who wants it and anticipates subsidies for those who cannot afford it, a compromise phase-in should be possible. How much real re-insurance would then cost is probably fairly well known to its recent insurers, although recent uproars will probably make new bidders rather protective. In this sense, public opinion is important to the price which would be demanded. As far as a subsidy to the poor is concerned, Obamacare originally anticipated hospitals would be able to lower their prices if everyone became insured and internal cost-shifting would stop; this would provide a test of that hope. Really serious planning may have to be deferred until a concerted effort is made to clarify the extent of internal hospital cost-shifting; one hopes this is already underway. If the approaching Judicial outcome produces a mixture of priorities which cannot be balanced, there will just have to be a later Congressional action to balance it. Since it can be anticipated that the piecemeal introduction of lifetime coverage will seem attractive to many, perhaps there will be several opportunities to get things more optimal. Transition into a new system must coincide with a transition out of the old one. Unfortunately, just the fear of deadlock could slow smooth advancement.
Health Savings Accounts were originally designed to replace employer-based health insurance, but millions of subscribers would be relatively satisfied with either one. Like any one-size-fits-all solution, each will seem uncongenial to some people, who should be left free to make a choice. By leaving enrollment voluntary, institutions can gradually expand or contract to adjust to demand. I have an enduring but blurred memory of the chaos which ensued in 1966 when Lyndon Johnson on television invited old folks to start sending the government their medical bills when it was soon discovered Medicare did not even have a listed telephone number. A vacant supermarket was found in Camp Hill, Pennsylvania, to store the unopened mailbags of Medicare claims, floor to ceiling.
All the HSA needs, to integrate almost any reasonable working-person health insurance into lifetime coverage, is a reliable stream of enough money to function. Starting at age 21, this money would link the roll-over money from the "grandparent's" surplus Medicare funds after death to the newborn's new HSA. Judging from this untried analysis, the likely limiting step would appear in the organization of the proposed Medicare "buy-out" program, since infirm old folks in the last years of life would have little incentive to switch. In fact, demographic mismatches might appear between any two segments of a lifetime program. Therefore, a contingency fund to cover these anticipated shortfalls, especially for the first year of life, would probably have to be regarded as the main hindrance to smooth start-up. From my talks at public meetings, I detect that elderly people have accepted Medicare as a fact of their lives, and are surprisingly indifferent to the Obamacare commotion. They even express the unlikelihood that anyone could ever change the present entitlement, in time to make a personal difference to them. This attitude must be gradually persuaded to yield, and then secondarily reflected by their elected representatives. A surplus is welcome at any juncture; it is the shortages which will hurt. The key to a smooth transition is to devise the right incentives, well in advance of the uproar.
Healthcare Financing, Up to Medicare Age
We have just estimated the lifetime healthcare cost of people up to age 65 as $128,000. That estimate was largely derived from guessing the limit of what people could afford for a lifetime of healthcare ($325,000), and observing you can't spend more than you have, indefinitely. From the total was subtracted the present known cost of Medicare, leaving the younger people with a healthcare budget of $128,000 from birth to 65.We then calculate how much compound income could be derived from $128,000 at 8%, recognizing it would arrive in yearly limits of the Health Savings Account Law of $3300 per year, from age 26 to 65. We calculate under two assumptions, with and without privatizing Medicare, and in two other assumptions, average life expectancy of 83 (the present figure) and life expectancy of 93 (the projected life expectancy). Curiously, the longer life expectancy has a lower projected cost, probably because it does not include the treatment costs of whatever lengthens life expectancy by ten years. But it does include the extra revenue from the lengthened period of compound interest on reserves.
It is most unfortunately true that present law prohibits paying for high-deductible insurance which is mandated to accompany a Health Savings Account. By striking a single sentence of the law, the injustice of unequal tax deductability for employer-paid insurance would disappear, but for the moment this feature must simply be accepted. First, let's define it. A high deductible could be as little as $1250 per year, or as high as $6000 for family plans. Its top limit, however, is simpler. It need not be higher than $10,900, the average cost of Medicare, since average young people will almost always cost less than the elderly. Furthermore, let's state the great virtue of high-deductibles: the higher the deductible, the lower the premium. As a consequence, the sellers of high-deductible Catastrophic healthcare insurance are very reluctant to advertise or even quote over the telephone, what their typical annual premium would cost, particularly when pre-existing condition riders are forbidden. This last feature creates an incentive to search for group memberships, higher premiums, younger clients, higher deductibles and lower ceilings. A longer waiting period for insurance to take effect might be a partial solution. As would rebates for longer subscriptions without claims. Obamacare has withdrawn its pure Catastrophic coverage in favor of paying subsidies for higher premiums to fairly high income groups. Increasingly, it is difficult to obtain this type of coverage without either being in a group or having a personal interview. With a change of party control in Congess, this would be a very good time to hold hearings on the problem. In the meantime, for discussion purposes, we use the hypothetical limits of $5000 deductible with an $11,000 maximum limit, for a premium of $1000 annual premium. Probably no policy exactly matches this example, but the difficulties could be ironed out by agreed rebates, or guaranteed issue, after 5 years of policy-holding. All of this does increase the administrative costs of what started out to be an ultra-lowcost product.
This approximation would consume $39,000 of a $128,000 budget, allowing $3300 annually to be deposited in the account. With compound income at 8%, this would purchase $xxxx worth of deductibles and outpatient costs over the 39 years of coverage, and including childhood costs. Except for unusual medical circumstances in the first few years, this should suffice. Indeed, after the first five or ten years, the fund would grow to the point where additional savings could be derived from less expensive fail-safe insurance policies, or even smaller deposits into the fund.
Pit Stop: Some Features Regular HSA and Lifetime HSA Have in Common
This book was primarily written to explain the difference between regular Health Savings Accounts and Lifetime Health Savings Accounts. The first is available right now although in somewhat crippled form, and the second requires enabling legislation to become available in a year or two. Naturally, the emphasis is on differences between them. They have several features in common however, based on obscure quirks in law which are vital for the reader to understand. So at the risk of a little repetition, let's review the DRG, the Flexible Spending Account, and the income tax deduction.
The Income Tax Deduction, for Employees Only. Seventy or more years ago, wartime wage freezes interfered with moving steel workers to the West Coast, so as a temporary war measure, fringe benefits were not considered taxable income. Big business and big labor never allowed this situation to be rectified, so in time it became the principle basis for employer-based health insurance. Employees got a tax deduction but self-employed and unemployed people did not. Much was made of this unfairness, but it never was changed.
Meanwhile, no one called attention to the fact that big business was getting an income tax deduction, too, which amounted to fifty percent in state and federal corporate income tax. Added to the fifteen to thirty percent deduction for the employee, this indefensible inequity became the main financing method for the American health system. And it was the main pressure behind the Clinton Health Plan, as well as the Affordable Care Act, or Obamacare. Like a smiling Cheshire cat, big business hardly said a word about it.
The DRG Diagnosis-Related Groups were a group of two hundred payment groups, used to pay for Medicare's hospital in-patient costs, and widely imitated because Medicare payments are half of the hospital revenue. They replaced nearly a million specific diagnoses, so they were extremely crude approximations. More important, they replaced fee-for-service billing. It no longer mattered how long you remained in the hospital or what services you received, hospitals were paid by the DRG. Being essentially meaningless lumps of diagnoses, their translation into money was easily manipulated, eventually resulting in a 2% profit margin, spread around rather unevenly. Many hospitals lost money, which was easy to do in a 2% inflation. Consequently, hospitals shifted their costs internally to exaggerate the effect that the Emergency room generated a 15% profit, and the out-patient area, formerly the domain of physician offices, became an extension of the hospital and had a 30% profit. The distorting effect and the consequent uproar is easily imagined.
The Flexible Spending Account. Essentially the same as an HSA or Health Savings Account, the FSA had one major difference. At the end of the year, any unspent money was returned, in what was soon called "Use it or Lose it." A large number of health-related luxuries, like prescription sunglasses, were consequently purchased in order to get some value out of the system; many people dropped the policy. However, they were heavily sponsored by Employers and Health Insurers, so were widely adopted. If the law could be changed to permit unused surplus to be "rolled over" to future years, essentially millions of employees would find themselves with what amounted to Health Savings Accounts. This would appear to be a gift by employers to employees, but gradually the terms of agreements changed. Much of the money sacrificed at the end of the year is effectively now the employees' own money, as a result of employee participation in the premiums, and in co-payments for the benefits.
There are many other quirks and unfairnesses in the existing employer-based system, particularly as they disadvantage non-employees. But in a very simple paragraph of reforms to these three, the Health Savings Account would emerge as a major reform, whether the one-year term or lifetime. A cleanup of the diagnostic code underlying DRG is badly needed, income taxes should be leveled for everyone regardless of the type of employer, and rolling over the year-end surplus of Flexible Spending Accounts would give a big boost to HSA enrollment.
That's all, the rest is in this book. Making healthcare cheaper is a bigger project, so let's return to where we were. We were about to talk about passive investment.
Disadvantages of Lifetime Health Care
So, right off, what are the disadvantages of lifetime coverage? They would seem to be:
1. At the moment, persons receiving Medicare are excluded from starting Health Savings Accounts. During the debate about Obamacare, seniors were therefore remarkably uninterested in two topics which didn't affect them: Obamacare and Health Savings Accounts. Very few seem to realize that Medicare is 50% subsidized by the federal taxpayer, and therefore few realize they are quite right to be uneasy Medicare might be "robbed" to pay for Obamacare. No politician is comfortable discussing this issue, for fear his party will be blamed for injuring a perfectly blissful status quo. Naturally, everybody likes buying a dollar for fifty cents, and everybody likes to imagine payroll deductions and premiums create an impregnable entitlement. The sad truth is the 50% subsidy, paid for by borrowing from foreigners, practically guarantees Medicare will be eyed as a victim, using the "fairness" argument. Seniors on Medicare, of which I am one, should be immediately in favor of a proposal which forestalls such pressure. Unfortunately, right now every one of them is looking toward the sunset, gambling on outliving a threat they hope will go away.
2. The computer revolution, which makes lifetime health insurance even imaginable, has severely impacted the investment community. It is still difficult to foresee which branch of the existing financial community would be natural allies, or natural enemies, of Health Savings Accounts. A remarkably large segment of the investment community already has HSAs for their personal affairs, and the banking community sees a chance that Bank Debit Cards could displace the huge industry of insurance claims processing. Meanwhile, insurers remain uncertain whether HSAs are a new revenue source or a threat to existing lines of business. The Dodd-Frank legislation is so large and complex it confuses everyone about net winners and losers. Investment advisors have been hit hard by the recession, and are forced to charge $250 per trade when their competitors charge $7.50 for the same service. Just about everybody in the HSA business is uncertain whether HSAs are insurance policies with an attached savings account, or whether they are investment vehicles with stop-loss insurance attached. Things are tough when lobbyists don't even know which committee to lobby. It takes time for HSAs to achieve profitable size, so industry leadership hangs back to see what they look like when bigger.
3. There are lots of small advantages, but one big disadvantage. The transition from one system to another takes a long time, perhaps a lifetime for some.
How can we navigate a transition that might take a century to complete?
Transition Strategy. The general answer to the long transition period lies in providing more than one method to close the transition gaps. Start from both ends, and then find one or more methods to break into the middle. If life insurance saves money, use some of it to overfund parts of the system as an incentive. When you find people are gaming the system, drop the feature which permits it. If some goal is accepted to speed up the transition, calculate what it is worth to accomplish it, and limit the feature as the transition speeds up. The method proposed in the ****previous**** chapter will certainly work out, but a newborn baby will be a Medicare recipient before children's insurance is complete for everyone. The rest of us have already lost some years for compounding, while some of us are already on Medicare and are, as they say, entitled. Therefore, we propose two additional ways of getting to the goal. Reducing the cost of healthcare is one, to be taken up in Chapter ****. That one works for everyone's finances at any age.The other method, which suits people of working age, is the present topic. It has two possible solutions, the issuance of special revenue bonds, and offering inducements for dropping Medicare. In the present environment, just using Medicare as a transfer vehicle is unthinkably unwise, politically. Reducing Medicare can only be brought up as a voluntary exchange, long into the future when the financial attractiveness of the HSA approach is so well established it has no political downside. It can be used to pay for non-medical retirement costs after HSAs demonstrate they can comfortably cover medical ones. At that point, it would no longer have the stigma of "robbing" Medicare but might be politically acceptable as making some use of unspendable double coverage.
Special Bond Sales. The safer approach is, therefore, to issue bonds to smooth out bumps in what is in some respects an equity investment. To match present cultural patterns, it should be recognized that working parents now fully assume the medical costs for their children, but have only a moral liability for the medical costs of their retired parents. Therefore, our culture might accept bond indentures with similar structure, but in one of the cases resist an identical bond issuance which differs significantly from accepted local patterns. In fact, it is difficult to imagine enacting any proposal which does not generally respect societal patterns. An important feature would be to start HSAs at an early age, adding as much as 26 years to the duration available for compounding. At 10%, that would be almost four doublings of the investment, and a fairly good start toward the initial goal of $80,000 in the account by age 65, while still starting with relatively small investments in childhood. True, a bond issue would have the interest to pay, but since the interest payment stays within a family it might be designed to seem less burdensome than taxes. It is a curiosity that U.S. Treasury bonds are entirely general obligations, unlike state bonds. There may be a good reason why federal bonds for specific projects are agency bonds, but someone else will have to explain it. The two purposes for which special bond issues might be considered are: respect for society's wishes with regard to parent/child discipline, divorce and illegitimacy issues; and to smooth out gaps in coverage necessitated by nonlinear relationships between revenue and expenses at different ages.
As a practical demonstration of the superiority of equity investing over zero-sum fixed income, an invisible psychological value cannot be overstated. If our nation expects for longer longevities to rely increasingly on investments rather than salaries, it must broaden its experience with sensible risks. Whether we like the idea or not, we are collectively taking long strides toward a rentier culture, where our main hope of advancement lies in greater willingness to understand and buffer the reasons for market volatility. One of the features of even this attenuated risk-taking is to recognize that a few people will start their investing at the bottom of a dip, while most will start at the top of a peak. The long-term result will smooth it out, but some people are destined by the luck of their birthday to make more profit in an equity market, than others. And some people are destined by the timing of their illnesses to end up with less money in the account than others, too. It may not seem fair, but tampering with investment cycles will not improve it. By establishing a system of buy-ins, both as a transition step and also for late-comers, the opportunity of market-timing is created. Almost nothing is more discredited as an investment strategy than market-timing by amateurs, but it probably cannot be completely avoided here, and will probably exaggerate the differences in account size achieved by members of the same age cohort. Somehow, the attitude must be made general, that nobody can make anything at all in the accounts if we return to annual premiums; all extra money in these accounts is "found" money. The books will not balance completely at all stages, so it becomes a political question whether to forgive the difference (as Lyndon Johnson did in 1965) or to define it as a subsidy (as Barack Obama seems to be planning for his start-up insurance system.) Perhaps in accounting for residual medical costs at the end of life, a way can be found to equalize outcomes, but it seems unwise to tamper directly with such large amounts which are mainly responding to the world's inherent volatility.Proposal 16 :Congress should authorize special limited-use bond issues (or Federal agency bond issues) for two Health Savings Account purposes: to fund accounts of late age at enrollment within the transitional stage who have difficulty attaining self-sustaining status; and to create a permanent bridge between age groups which are in chronic deficit and age groups which are in permanent surplus, to the extent that such particular age disparities remain in balance. In both of these cases, it is calculated the accounts will eventually come into permanent balance after a full transition has taken place within current demographic trends.
Comment: With the passage of time, it should be possible to identify age groups (for example, the first five years of enrollment) which will eventually come into balance with other age groups which permanently generate a surplus. Knowing aggregate lifetime coverage will itself bring these two groups into permanent balance, it is sensible to borrow from one and loan to the other during early transitions, at minimal interest rates. Having provided for eventual coverage of these secular risks, it becomes more reasonable to extend favorable rates to them during early transition. When the slots are fully loaded, so to speak, there will always be secular fund imbalance between age groups, where market rates are always needed to cover the overall plan design. The intent of these two interest rate levels is to distinguish between a transitional phase which is temporary, leading to an equilibrium loan imbalance which is a natural part of the design.
There are several other serious matters. They will be briefly noted, and then an omnibus solution presented, the IIOO. Let's answer one inevitable jibe immediately: How can poor folks afford this? Answer: They have to be subsidized, that's all, just as they are in every other proposal including Obamacare. It's important to face this because neglecting it is the route by which every deficit has been incurred, every budget unbalanced. People who spend other people's money on healthcare characteristically have higher than average health costs themselves. But the novel discovery is Health Savings Accounts have generally proved to reduce costs by 30%. When both approaches operate at the same time, results are not reliably predicted but can be monitored. Miscalculations usually result in debts, dropped options and dropped amenities. A politically appointed board would be wise to refuse an assignment to address this, unless contingency instructions are clear, and remain out of their hands. When Congress eventually discovers how to put a ceiling on the national debt, effective answers to this related issue may become more apparent.
Transition from Term Most transition problems (shifting from one-year coverage to lifetime coverage) have to do with whether you are a child, whether your children are gone and forgotten, or whether you are supporting everybody else in your family. As the saying goes, how you stand will depend on where you sit. The unique borrowing problem here, is complete transition takes so long, groups will differ significantly on whether to unify forward (child to grandparent) or backward (grandparent to child), until it can be worked out how to borrow as a child and borrow for a time as a grandparent, depending on particular situations. What's to be avoided is intergenerational borrowing as groups; we've tried that. The benefits of invested premiums are obvious to all groups, but the arrangements must be debated thoroughly in order to avoid just kicking the can down the road. Almost any arrangement would suffice for a brief transition, but this transition would take so long it would amount to a Constitutional Convention when it was over. The eventual goal is to place the cost burden largely on working people age 26-75 since that is the only age group in direct contact with the national economy. The tricky part is to utilize other age groups during the transition -- and then slowly work out of it. Don't forget a third generation will intervene -- their own children, as well as their parents and grandchildren. The whole construction is a job for actuaries, but the modern use of index funds put on the table the potential of a diversified investment, absolutely without stock-picking, at favorable rates of interest, allowing room for cyclicity of the economy. America seems to need increased fertility, and the compound income might make it possible, but if it is not carefully examined, it might act as an inducement for women to delay their first child even longer than they presently do. As long as you don't get overwhelmed by too many transition issues at once, almost any intergenerational problem would be eased by generating more revenue. At ten percent, money compounds to double itself every seven years, and the resulting sums can boggle the mind. But if they are not planned for, the extra money will either vanish or induce people to act like a deer frozen in the headlights.
Making ten or twelve percent on safe investments may seem impossible to those who have recently lost thirty percent on the stock market, and of course, it is not guaranteed. That is why lifetime health insurance based on fixed income securities cannot be presented as guaranteeing payments for future services; only equity securities (stocks) can do that, and even they, mostly don't succeed in real terms, or net of inflation. Lifetime health insurance should only promise to supply a substantial portion of future health costs, and has little hope of doing so except for two possibilities. If the taxpayers would stand for it, you might deliberately overfund the accounts; since they won't, it is necessary to induce some to do it voluntarily and shrug your shoulders at those who don't. That probably won't work, either, so we are left dependent on our scientists to reduce or eliminate medical costs. They are willing enough to try, but of course, they can's guarantee. You can gamble on its happening, or you can wait until it is a sure thing. We are decades into fiat currency without the semblance of backing by monetary metals and must feel our way. However, the bright side of our present financial system is that transaction costs are steadily declining for reasonably safe passive investing. Professor Ibbotson has demonstrated that total market averages have been remarkably steady for asset classes over the past eighty years, and probably will safely remain so for another century, but that's another assumption which might go wrong. When you get down to it, you either go ahead or you don't. That's all. Investing in the total domestic stock market of America, the investment is guaranteed by the full faith and credit of America, just as surely as if invested in U.S. Treasury Bonds, and it pays a little better in return for its increased volatility.
Still another question comes from people who rightly believe there is no free lunch: Where does the extra money come from? A fast answer is that it comes from correcting a blunder of long standing, called the "pay as you go" system. To some extent, this problem began with the original Blue Cross plans of the 1920s, but it was elevated to its present stature by the Medicare and Medicaid proposals of 1965. By the pay/go approach, this year's premium money is spent for this year's sick people, not the people who paid the premiums. That ruse helped get the program started, but it means current unspent premium money is quickly gone, and thus it means no compound interest or investment income is generated by rather huge revenue collections in the future. Since health expenses rise with advancing age, a great deal of floating premium money might be invested for many decades, if only it had not already been spent. Actual projections are surprisingly large, but I would prefer that others announce their calculations, employing the motto of "Underpromise, but over-perform."
Other substantial sources of reserves exist, nevertheless. Health Savings Accounts now in operation are reporting 30% savings; since it is unlikely this record can be maintained with inpatients, who are generally older, overall savings may well turn out to be closer to 15%. Inflation helped a lot to pay off the original startup costs of 1965, but at least nominally it is true the debt has been paid. We are now free to invest that ancient transition cost, so to speak, as long as we don't try to spend the same money twice. But there is considerable squeamishness about the public sector acquiring equity in the private sector, so Treasury bonds are about the only public sector investment the public will easily allow. Investment experts are however almost unanimous in feeling that equities provide greater long-term income (see graphs by Ibbottson) and security against inflation. On the other hand, if private individuals invest in common equity with index funds, less resistance is encountered. Any way you look at it, some investment income is better than no income, and for long-term investment, equity is better than debt. For political purposes, it would seem best to restrict investments to U.S. companies, and index funds are less controversial (i.e. "gambling with my money") for most small investors than actively managed funds, because the savings mostly come from reduced investment expenses. John Bogle is telling the world that 85% of most total return is diverted back to the financial industry, and this is one way to rebalance that. Fifty percent of investors would do better than average, fifty percent would do worse because of broad diversification, but not much worse, because total index diversification is fast approaching a maximum. Meanwhile, compound interest would be at work, and most people would be astonished to learn how large the long-term appreciation would grow. Tax-free, diversified, and long-term.
Finally, the question arises: how can you tell whether income from this source would equal the terminal care costs of fifty years from now? You can't, of course, you can't. But this transfer and invest scheme would generate a whole lot of money that presently isn't being generated. If it isn't enough, we will have to do something in addition. The monitor and mid-course correction system are expected to detect when more money is required to balance the books, and therefore more money will have to be invested in the Health Savings Accounts. If savings are insufficient, either subsidies or borrowing will have to be resorted to. Experts sometimes will be wrong, so revenue should be raised somewhat higher than the experts think we need. And if it all goes wrong, if we have an atomic war or an expensive cure for cancer, there is always the national debt. Which is where we began, isn't it.
Independent and Impartial Oversight Organization. (IIOO)After reviewing the complexities, it seems best to create an oversight body with more time and expertise that can be expected of representatives who are subject to periodic election. However, Congress must make it clear that it retains ultimate authority to break from the normal routine, occasionally concentrating its attention on conflicts between expert opinion and public opinion.
Working backward, a mixed public/private system needs an official backer of last resort, a function which cannot be delegated, and an experienced crisis management team in place with the authority to act within defined limits, most of the time. The last resort has to be the full credit of the United States, just as unfortunately it now is with Medicare. What's mainly needed is a sort of Federal Reserve in the very narrow sense of an independent management team, under the direct governance of a Board whose composition is half public, half private. To be useful, it needs a monitoring authority provided by a mandate from Congress, a comparatively limited amount of regulatory authority of its own, intentionally limited by adequate board representation from all stakeholders. The Board needs to be constantly told what is going on, and it needs general authority and trust to act in an emergency. Many proposals require a system of mid-course corrections particularly in the first decade of operation, at the same time the Board must not usurp Congressional authority.
Congress, on the other hand, must have the restraint of private oversight by technical experts who can appeal to the public, to make very certain it does not feel it has a new piggy bank. Corruption is one thing; misjudgments are quite another. Once in a while, we manage to construct such an agency.
Beware the Middle-man: Common Stock Index Fund Earnings are Not the Same as Investor Returns.
There's quite a lot to passive investing if you mean running an Index fund. The rewards of this hired complexity can nevertheless be lost by carelessness in choosing an expensive middle-man. Or even by having a reliable agent who works for an organization, remorselessly devoted to its own income maximization -- in the middle. Or having a small reliable agency bought out by a corporate raider with entirely different goals from the ones you thought you selected. But if your long-term common stock index results approach 10% total return, at least you have passed the first test. As my mother repeatedly told her granddaughters: Don't marry the first man who asks you.
Asset Allocation Managing the funds of a Health Savings Account has important similarity to managing a pension or endowment fund. An important distinction: healthcare imposes random cash requirements on an HSA, compared with the steady, predictable cash requirements of an endowment fund. After the Health Savings Account has matured to a steady state, its fund balance becomes predictable, just as cash balances in a big bank eventually do. Nevertheless, the HSA is probably destined to require larger cash reserves while maturing, and the second period of the volatility after age fifty, when more serious illnesses get more frequent. On top of that, when a securities crash comes along, it may take as long as two years for the market average to stop falling, and as long as three years to recover. That's by contrast with normal ripples in the markets, where 90% of important gains or losses are made in 10% of time periods. The rest of the time the market dawdles.
If most "dips" are followed by recoveries, why not just wait it out? Here, almost all organizations have the same problem of "meeting the payroll". The uproar of being late with a payroll must be experienced to be believed. While most employees will quietly accept a short, reasonable delay, the few who are stretched by a brief interruption for any reason, can be very vocal. The financial management of any fund faces the same issue and is very reluctant to repeat it. All of them face the possibility of some sudden decline in the value of the portfolio when at first it would be general opinion it is wiser to avoid selling from the portfolio and wait for a quick recovery. Reserve portfolios are set aside for sudden cash requirements, of course, but human nature induces most people to wait and hope for better times. In more tangible terms, it is generally the business of the investment manager to cope with a lot of small waves, but only the Board of Directors can decide to liquidate the whole reserve. In for-profit situations, there is also a question of paying taxes.
Conventional advice is to maintain a portfolio of 60% stocks, 40% bonds, with the cash flow from the bonds intended to bridge the gaps. Since bonds pay less than stocks, the overall portfolio yield is lowered. If interest rates are unusually low, it may be the bond component which is itself the risk, but at least in theory, mixed assets "balance the risk." As a consequence, an 8% steady yield from an endowment or pension fund is the best performance many professionals expect, with most funds even happy to achieve 7.5%. But happiness is relative. We have just demonstrated the first step in how a 10% total return can turn into 4%. You're already down to 7.5%.
Buying Out Your Medicare?
The public is vaguely aware there is a problem with Medicare indebtedness, but for the most part, this issue is swept aside, for fear agitation might injure the chances of funding healthcare for those of working age. The size of this debt is not well known but can be guessed at by realizing Medicare costs are 50% borrowed. The current CMS data show a line for contributions from the general fund, equalling 50% of the total. Because cost accounting for government accounts has its special features, inter-agency transfers are referred to as assets. It's a debt, all right, and a large part of it is owed to the Chinese. For whatever reason, Treasury debt is entirely "general obligation", so it is not usually possible to tell from Treasury debt, how much is assigned to particular debts. They would have to be totaled from Medicare annual reports, which are not generally available for much of the past. So we don't -- right now -- know how much we owe foreigners for Medicare debts, but it is considerable, very likely going back to the days when deficits began to appear. That gives me a choice: I can keep quiet about the subject, or I can conjecture. I choose to conjecture.
Some, maybe all, of the transfer from general taxes in the latest year to Medicare, was borrowed. Medicare started in 1965, but during the early years, the receipts from payroll deductions were larger than the expenses of the Medicare program. But when the program was fully underway, it ran a deficit. For how many years, and for what amounts, is only a guess. But I assume guessing the debt to be equal to a full year of Medicare expense, is large enough to make the point I wish to make, but may well be larger. For present purposes, let us assume the existing debt is equal to a full year's cost of Medicare, which we do know is 549.1 billion dollars. This guess is selected for illustration because it is large enough to cause alarm, but is probably on the small side. I hope it will provoke some official figure to be released, and sincerely hope my own proves to be too large..
Because, if it proves close to the guess, it presents a future problem for paying off the debt, which would actually be worse than the healthcare cost now under such heavy debate. The past indebtedness is currently not under debate and is still getting worse. The public, including my colleagues in the medical profession, often point to Medicare with admiration. Since everybody likes a dollar for fifty cents, that's perfectly natural. And so it is also perfectly natural for elected officials to treat the matter of replacing Medicare as if it were the "third rail of politics." Just touch it and you'll be dead. That's also fair play until it is proposed the whole medical system of the country be covered with a "Single Payer System", which is a fancy way of proposing everything should be funded like Medicare; and that's just too much.
So I propose, discomfiting friend and foe alike, that we buy our way out of this problem by allowing the public to buy its way out of Medicare. One by one, as they approach the 65th birthday, they should have the opportunity to relinquish Medicare, by depositing $80,000 in a Health Savings Account. Assuming 10% compound income return (see Chapter Four), $40,000 should generate $433,000 by the age of 91, which I assume to be the average longevity in a few years. By taking a guess at the size of the debt, the remaining $40,000 would throw off an additional $433,000 for paying it off. With 25 million Medicare recipients paying that much, let's hope it is more than adequate right now, although it will clearly become inadequate if we delay. These numbers ought to seem like a bargain to the public, and they certainly would seem like a bargain to the government. If there is any other proposal for managing this debt, we have yet to hear it. That's probably because of "third rail" concern, but unfortunately, it may also reflect there is no other solution to talk about.
Issues and Problems In the first place, $40,000 at 10% will only yield $202,000 by age 83, the present average longevity. It will slowly grow, as will the medical expenses from 83 to 91. The debt is already too conjectural to justify more precision, but a decade or so is not unusual for oriental negotiations. Sooner or later, we must expect this progressive longevity to flatten out, and make the problem harder to solve.
In the second place for a long time to come, people arriving at their 65th birthday will have a history of payroll deductions when they were young. This will eventually dwindle down, but it begins as a quarter of Medicare costs and must be returned as part of the buy-out. Meanwhile, persons older than 65 will have fulfilled their payroll deduction, and are paying annual premiums, which also equal a quarter of Medicare costs. This seems to be approximately prorated, so only the payroll deduction is owed these people during the transition.
And to go on, there will surely be medical developments. Some of them may raise costs, some lower them, and all of them summarized by a hoped-for cure for cancer, which may raise costs or lower them, more likely raising them before eliminating them. Once the discovery is made and announced, its price will be known, and appropriate adjustments demanded. For this and a host of similar issues, only a scientific body with the power to adjust prices can be expected to make the appropriate response with mid-course corrections. Given the present affection of the public for subsidized Medicare, it appears likely, voluntary buy-outs will be a slow and protracted process. They should provide ample time for basing reasonable adjustments to what would be mainly favorable developments.
Deductibles Too High?
In 1981, John McClaughry and I devised the Health Savings Account, and in 1996 it became law, in 2003 permanently. It features a high-deductible health policy, linked to a tax-exempt savings account. One of the purposes of the savings account was to contain enough ready cash to cover the deductible. Since there have been recent reports of public unhappiness with the high deductible of almost all Obamacare policies, I suggest the participants open up Health Savings Accounts in addition to their insurance. An amount equal to the deductible can probably be deposited since the current top limit is $3250 per year. Very likely, only one deposit would be necessary until a second major illness made its appearance, and all deposits are tax-deductible. They accumulate compound interest if unused, and usually, a debit card is provided for other medical expenses, once the balance to reach one deductible has been reached. At this point, a second tax shelter is available for medical expenses--the only qualified pension program to offer both front-end and back-end deductions.Double tax deductions are common in Canada, but Health Savings Accounts are the only available American plans which provide this. Furthermore, you can't lose money on them. If you should be so lucky as to reach age 66 without using the deductible, it turns into an ordinary IRA for retirement income. By that time, many people would find the compound interest had greatly multiplied the original deposit.
As a bit of history, 14.5 million people have these accounts already, containing several billion in deposits. Among employer-based insured, 31% have these accounts, and 41% made no withdrawals in a year. One New York bank manages 900,000 accounts.
The Health Savings Account was devised as a money-saving device for Catastrophic health insurance. That is, for high-deductible policies, which happened to have the feature that the higher the deductible, the lower the premium. But although Obamacare has higher premiums to pay for extra features, there is no reason why the Health Savings Account could not be used in conjunction with Obamacare.
Most people don't have $3000 in savings lying around so they may have to make smaller deposits over time, to build up to the deductible level. Most banks and brokerages don't welcome the expense of handling small deposits so you may have to accumulate $3000 independently, and there may be an unexpected squeeze. But every program has to start somewhere, and it may be inevitable that some people are a little too late for this one. But millions of people have already found out about Health Savings Accounts, so it's a real thing when you are ready.
George Ross Fisher MD
Philadelphia PA
32 Blogs
Health Reform: Seen On the Mass Media
New blog 2014-01-15 00:55:29 description
Chicago Sauce on an Arkansas Turkey
The sound-bite is: the Obama health reform proposal of 2009 will extend affordable health insurance to every American (citizen), and save Medicare from ruin by cutting costs. Review of the proposal suggested he should press the reset button.
How to spend
New blog 2014-03-25 23:46:45 description
Data Sources for Health Care
REVENUE PROVIDERS WITH POTENTIALLY USEFUL MEDICAL DATA, MOSTLY UNUSED
Direct Marketing of Health Insurance?
Remote and undeveloped regions of the country traditionally sell insurance through local brokers. Increasingly, some insurance companies sell their products directly to the consumer, a process greatly simplified by the use of computers. Costs are lower with direct marketing, but it requires a customer who knows what he wants and is confident about prices.
Welcome to Welfare
New blog 2014-06-24 18:42:35 description
Co-Insurance (2)
New blog 2013-07-01 16:26:04 description
Cost to Charge Ratio (2)
New blog 2013-07-17 19:12:46 description
Executive Summary, continued
New blog 2013-06-13 17:45:19 description
Introduction, continued
New blog 2013-06-14 19:33:13 description
In Summary
Suggestions are made for introducing competition, internally funded compound interest, patient cost sharing, and insurance restructuring into Obamacare.
What Obamacare Should Say But Doesn't
Here are ten healthcare finance reforms, superior to Obamacare. By far the easiest and most effective is equalizing the tax exemption, now only enjoyed by big employer groups.
Strange Interlude
 Obamacare was signed into law March 23, 2010, to go into effect January 1, 2014. During the 33-month interval, the Executive Branch produced thousands of pages of regulations, still too incomplete for full understanding. To its opponents, this protracted semi-secrecy was a hunker-down response to the overwhelming Republican Congressional victory in 2012, and the disastrous failure of the electronic insurance enrollment system in late 2013.
Obamacare was signed into law March 23, 2010, to go into effect January 1, 2014. During the 33-month interval, the Executive Branch produced thousands of pages of regulations, still too incomplete for full understanding. To its opponents, this protracted semi-secrecy was a hunker-down response to the overwhelming Republican Congressional victory in 2012, and the disastrous failure of the electronic insurance enrollment system in late 2013.
Cost Effect of Increasing Longevity
If average Medicare costs are treated as a single-premium cost at age 65, invested premiums will actually outgrow increasing costs.
What Part of Medicare Gets Paid?
New blog 2014-08-11 00:45:52 description
Congressional Hearing: Health Savings Accounts
Health Savings Accounts have dual payment systems, cash, and insurance. The new style adds passive investing in a lifetime instead of an annual model.
Examples
New blog 2014-12-03 19:20:48 description
Blue Sky Flying for Congress: What to Do With Money Which Health Savings Accounts Drop in Your Lap
New blog 2014-11-11 00:33:45 description
Former Foreward to Saving for a Rainy
New blog 2015-01-15 19:26:18 description
Supreme Court Rescues Obamacare, June 26, 2015
Hamlet Speaks His Mind
New blog 2015-06-25 19:24:16 description
Deeper Detail: Extending the Investor's Return, Simplifying His Role
New blog 2015-06-05 00:10:43 description
Lifetime Healthcare, Using Health Savings Accounts (1)
New blog 2015-03-06 01:37:12 description
Basic Coverage: Three Big Problems, No Little Ones
New blog 2015-03-10 20:34:33 description
Lifetime Healthcare, Using Health Savings Accounts (3)
New blog 2015-03-11 19:51:17 description
Lifetime Healthcare, Using Health Savings Accounts (4)
New blog 2015-03-13 21:34:27 description
Healthcare Financing, Up to Medicare Age
New blog 2014-12-29 00:14:24 description
Pit Stop: Some Features Regular HSA and Lifetime HSA Have in Common
Both types of Health Savings Accounts, the Regular and the Lifetime, contain some important modifications of existing health insurance.
Disadvantages of Lifetime Health Care
Disadvantages? What disadvantages?
Beware the Middle-man: Common Stock Index Fund Earnings are Not the Same as Investor Returns.
Investing is only part of running an endowment.
Buying Out Your Medicare?
New blog 2014-11-26 19:40:08 description